Modeling of implementation of the new Organ Procurement and Transplantation Network/United Network for Organ Sharing policy for patients with hepatocellular carcinoma
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To simulate effects of the new Organ Procurement and Transplantation Network/United Network for Organ Sharing policy on the patients’ characteristics and post orthotopic liver transplantation (OLT) outcome. Materials & methods: The United Network for Organ Sharing database was used to identify patients with hepatocellular carcinoma who were listed for OLT 2002–2014. All patients (actual group) versus simulated group with new 6-month delay in assigning Model for End-Stage Liver Disease score exception and Model for End-Stage Liver Disease exception cap of 34 were compared. Results & conclusion: With the new policy, 7,745 (30.4%) of the transplanted patients would have received a delayed transplantation or not be transplanted. The simulated group also showed significantly higher mean overall survival after OLT (p < 0.002) and received more locoreginal treatments (p < 0.001).
Despite the results of locoregional therapies and surgical resection, orthotopic liver transplantation (OLT) remains the curative option for patients with unresectable hepatocellular carcinoma (HCC) [1,2].
The United Network for Organ Sharing (UNOS)/the Organ Procurement and Transplantation Network (OPTN) was created as a consequence of NOTA (1984), and data have been captured since 1987 to ensure fair allocation and distribution of liver transplants [3]. Once an HCC patient is listed in a regional transplantation list, the patient will experience a variable wait time before receiving liver transplant, depending on the Model for End-Stage Liver Disease (MELD) score and geographic region in which he is listed [4]. Multiple recent studies showed that HCC patients had a lower dropout rate from the waiting list, decreased risk of waitlist mortality and increased odds of transplant compared with non-HCC patients [5–7]; therefore, it was recommended to set a higher HCC exception score as a cut-off or delay HCC MELD exception score assignment [7,8]. Thus, UNOS recently amended the liver transplant allocation policy for HCC patients [9]. Based on new criteria, the maximum value of MELD exception scores have been capped at 34 since October 2015, and HCC patients have been assigned their biological or native MELD scores only 6 months following listing, as opposed to being assigned points immediately [9].
The purpose of the new policy is to provide a better balance in liver transplant opportunities between candidates with HCC exceptions and those with allocation priority based on calculated MELD score, but possible effects of the new changes in enrollment criteria have not been simulated in a large-scale population-based study. Thus, this study aimed to investigate the effects of the new OPTN/UNOS policy on outcome, receivers’ characteristics, survival and locoregional therapy (LRT) rates.
Patients & methods
Study design & ethics
For this Health Insurance Portability and Accountability Act-compliant study, UNOS Organ Procurement and Transplantation Network (OPTN) Standard Transplant Analysis and Research data files were obtained under institutional review board approval.
Study population
The most recently updated UNOS database was used to identify patients with HCC who were listed for OLT between February 2002 and December 2014 and transplanted up to September 2015. The UNOS database includes data on waitlisted candidates, transplant recipients and donors in the USA, submitted to the system by the institutes which are members of the OPTN and has been described elsewhere [10]. The UNOS database has been implemented since 2002 and a minimum of 2 years was considered for this observation.
All patients, listed in the current UNOS database based on the old policy, were first analyzed as the actual group. The old criteria are as follows: OLT candidates with HCC, within Milan Criteria, (and downstaged to Milan criteria) listed for OLT from January 2002 to December 2014, transplanted up to September 2015, only patients with sufficient data on waitlist dates and duration, mean MELD score cutoff criteria for liver transplant determined by year and region.
Any conventional trans-arterial chemoembolization or drug eluting bead trans-arterial chemoembolization, Y90 radioembolization (Y90-RE), radiofrequency, chemical ablation, cryoablation and microwave ablation postdiagnosis and prior to transplant were defined as bridging LRT.
As the second step, the same patient population data were used to model the outcome of the new policy, as the simulated group. Mean biological and exception MELD scores for transplanted patients were first used and then stratified by region and year of transplant. Then, the new MELD exception point cap of 34 was applied to all patients with new MELD exception scores. In addition, a 6-month delay of exception point allocation was implemented by assigning the biological MELD score of all HCC patients during the first 6 months postlisting. If the patient was still within Milan criteria after 6 months, the patient was given a MELD score of 28 which was subsequently increased every 3 months up to the maximum score of 34.
By comparing both groups, this study examined if the new policy changes had an effect on the population who would eventually receive liver transplantation. The study flowchart is shown in Figure 1. After implementation of both the MELD score cap and the 6-month delay in HCC MELD exception points, a total of 7745 patients who received OLT would not have qualified under the new policy in the same timeframe. Only 1773 patients would still have received liver transplant under the new policy. This population was considered as simulated group and compared with the actual group under the old criteria.

Figure 1. The study flow chart.
The compared groups, actual and simulated groups, are marked by *.
HCC: Hepatocellular carcinoma; LT: MELD: Model for End-Stage Liver Disease; OLT: Orthotopic liver transplantation; UNOS: United Network for Organ Sharing.
Outcome definition
The main studied outcomes were HCC progression beyond transplant criteria and death with the secondary outcome of need for LRT. The occurrence and the date of death were either obtained from data reported by the transplant centers completed by data from the USA and the OPTN or extracted from online social security death index resources.
Statistical analysis
Statistical analysis and data management were carried out using JMP statistical software version 20.0 (SAS In., NC, USA). Chi-square test and Fisher exact probability were used for comparison of categorical variables, while independent t-test was applied to compare the continuous variables. The outcome of actual and simulated groups was compared using a Kaplan–Meier estimation and Log-rank test. Effects of different variables were independently assessed by the Cox proportional hazards model. Similar statistical analysis was performed for subgroups of HCC patients stratified based on LRT status. For statistical analysis, bridging LRTs were categorized as TACE (conventional trans-arterial chemoembolization and drug eluting bead trans-arterial chemoembolization), RFA, or other groups (including cryoablation, microwave ablation, chemical ablation or Y90-RE). A p-value of less than 0.05 is considered significant.
Results
Population characteristics
Out of 37,870 HCC patients who were granted MELD exception points during the study period, 25,476 (67.3%) patients actually received OLT. When the new policy criteria were applied, a total of 17,731 HCC patients would have received OLT and 7745 (30.4%) currently transplanted patients would have had delayed transplantation or not listed for transplant in the same timeframe (Figure 1).
The baseline demographic characteristics of the both groups’ population are presented in Table 1. There were no significant differences in age, gender and ethnicity between the comparison groups. However, significantly higher index tumor size is noted in the simulated group compared with the actual group at the time of transplant, with a mean size of tumor 3.7 cm versus 2.6 cm (p < 0.001). Significantly higher BMI was observed in the simulated group compared with the actual group (mean BMI of 28.8 vs 26.5 kg/m2; p < 0.001). The median wait time was not statistically different between two groups (p = 0.055).
| Variables | Mean (SD)/groups | Actual group (n = 25,476) | Simulated group (n = 17,731) | p-value |
|---|---|---|---|---|
| Age at OLT | Mean (SD) | 58.17 (6.14) | 57.11 (7.67) | 0.320 |
| Donor Age | Mean (SD) | 45.72 (8.56) | 43.89 (9.22) | 0.758 |
| Gender | – Male | – 77.4% | – 75.2% | 0.773 |
| – Female | – 22.6% | – 24.8% | ||
| Donor gender | – Male | – 60.3% | – 61.9% | 0.331 |
| – Female | – 39.7% | – 38.1% | ||
| Ethnicity | – White | – 70.2% | – 68.9% | 0.09 |
| – Black | – 9.1% | – 13.5% | ||
| – Other | – 20.7% | – 17.6% | ||
| BMI | Mean | 26.5 | 28.8 | <0.001 |
| Donor BMI | Mean | 24.6 | 24.8 | 0.312 |
| Index tumor size | Mean | 2.6 cm | 3.7 cm | <0.001 |
| Etiology of HCC (%) | – Hepatitis B | – 30.7% | – 31.3% | 0.252 |
| – Hepatitis C | – 40.5% | – 38.1% | ||
| – Other | – 28.8% | – 30.6% | ||
| Median wait time (days) | Mean | 127.2 | – 167.9 | 0.055 |
| Warm ischemic time | – >30 min | 81.0% | – 82.7% | 0.261 |
| – ≤30 min | 19.0% | – 17.3% |
BMI: Body mass index; HCC: Hepatocellular carcinoma; OLT: Orthotopic liver transplantation; SD: Standard deviation.
Overall survival
The median overall survival (OS) in the simulated group was slightly, but significantly higher than in the actual group (98.9 vs 96.8 months; p = 0.002, Figure 2). Although the OS curves overlap during the first 38 months, but the actual and simulated groups curves diverge afterward (Figure 2).
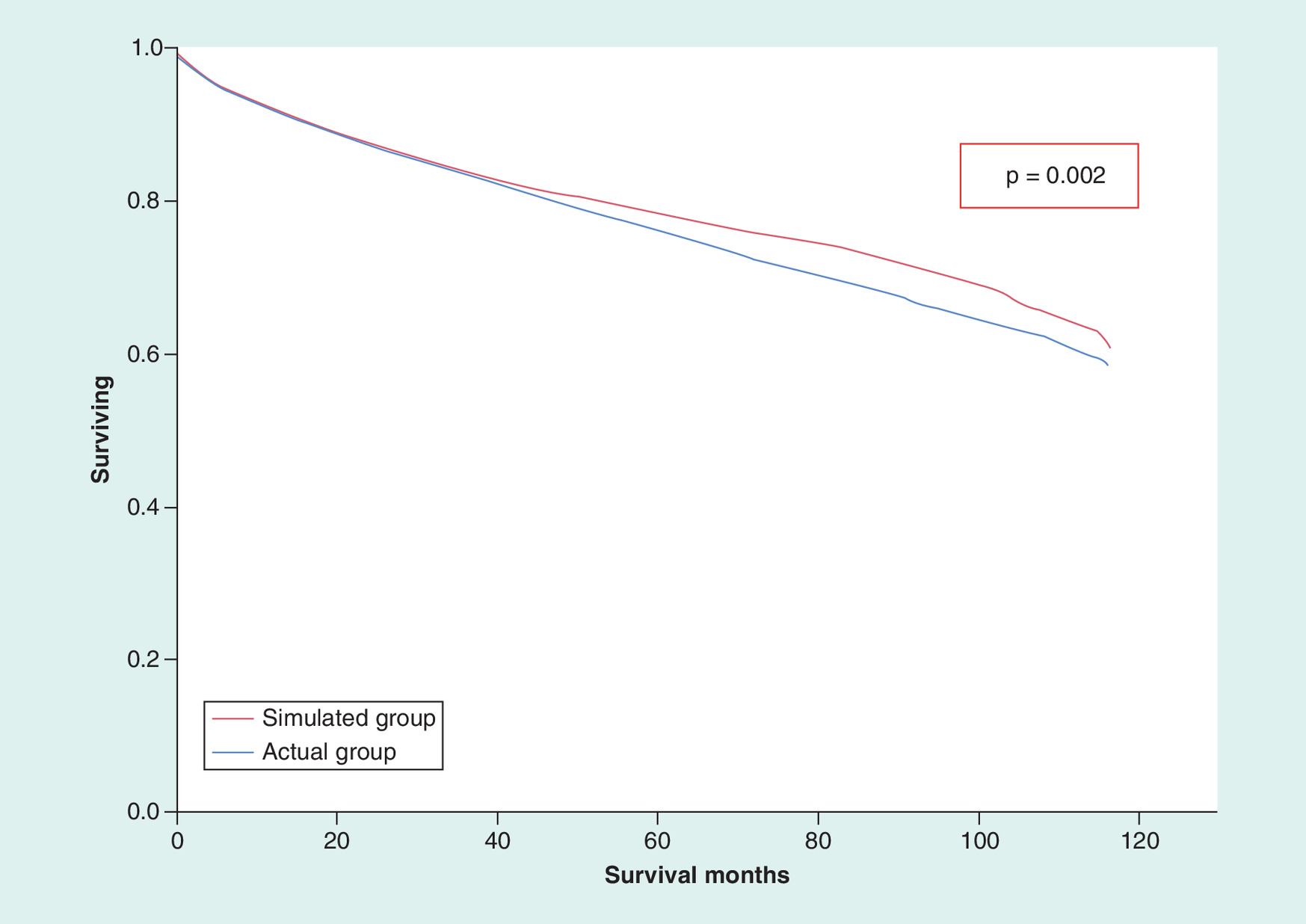
The median OS rate was not different between the actual and simulated groups at 1-year post-transplant (96.3 vs 97.7; p = 0.09). However, the OS was significantly higher in the simulated group at 5-year after OLT compared with the actual group (82.3 vs 78.5%; p < 0.001), and similarly 10-year post-OLT OS was significantly higher in the simulated group at 10-year post-OLT OS (68.9 vs 63.6%; p < 0.001).
The median OS rates from date of transplant in the actual and simulated groups are mapped out on Figure 3. Shift in color to blue suggests overall increase in OS by implementing of the new policy.
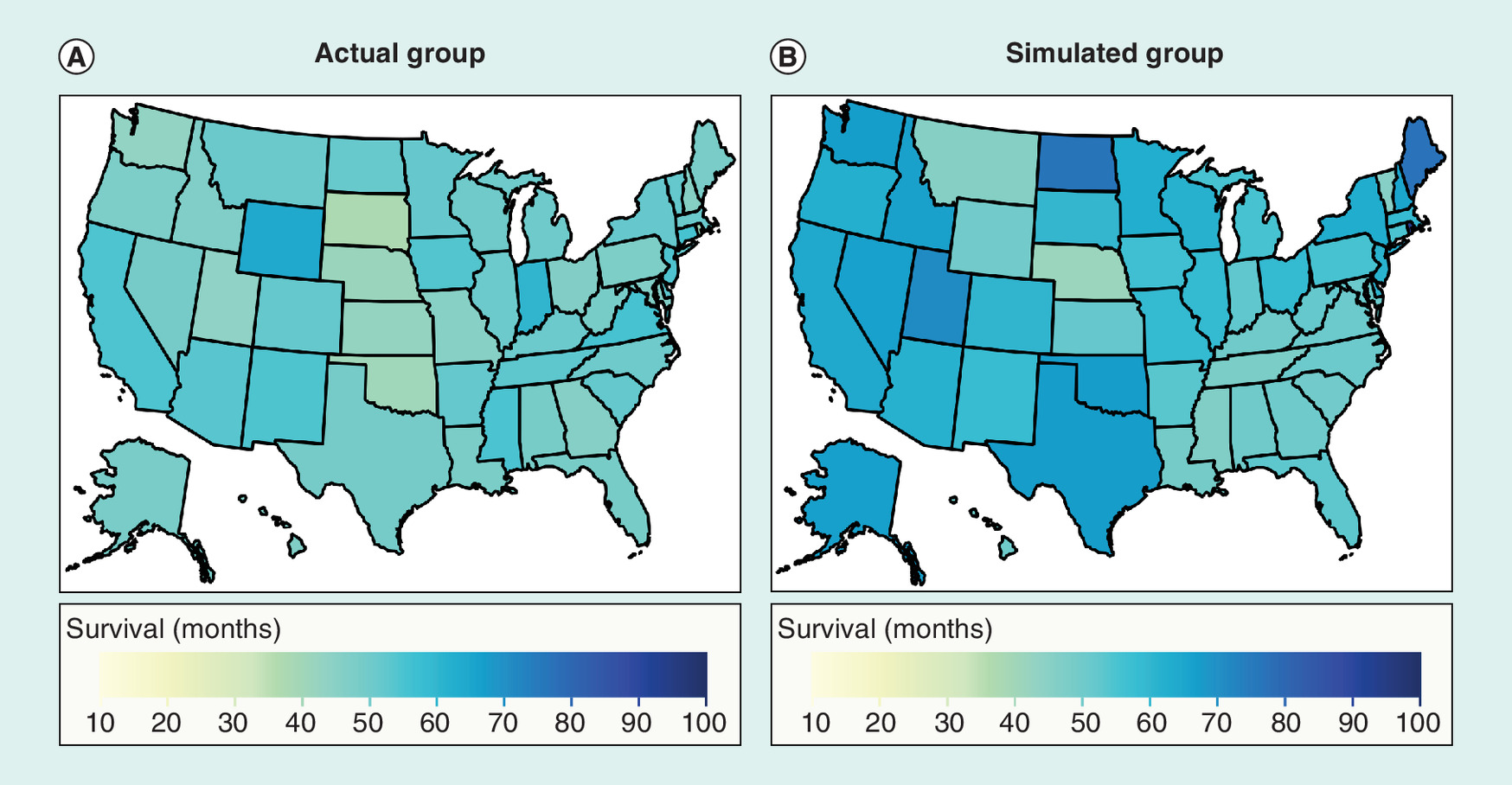
Figure 3. Median overall survival rates for the studied groups based on the states.
Mapping of the median overall survival rates for (A) actual and (B) simulated groups.
Bridging LRT & overall survival
Figure 4 demonstrates the rates of bridging LRT in both groups. The rate of bridging LRT was significantly higher in the simulated group, compared with the actual group (45.9 vs 36.0%; p = 0.007). As it is shown, the rate of TACE was increased more than other procedures, from 27.8 to 35.6%.
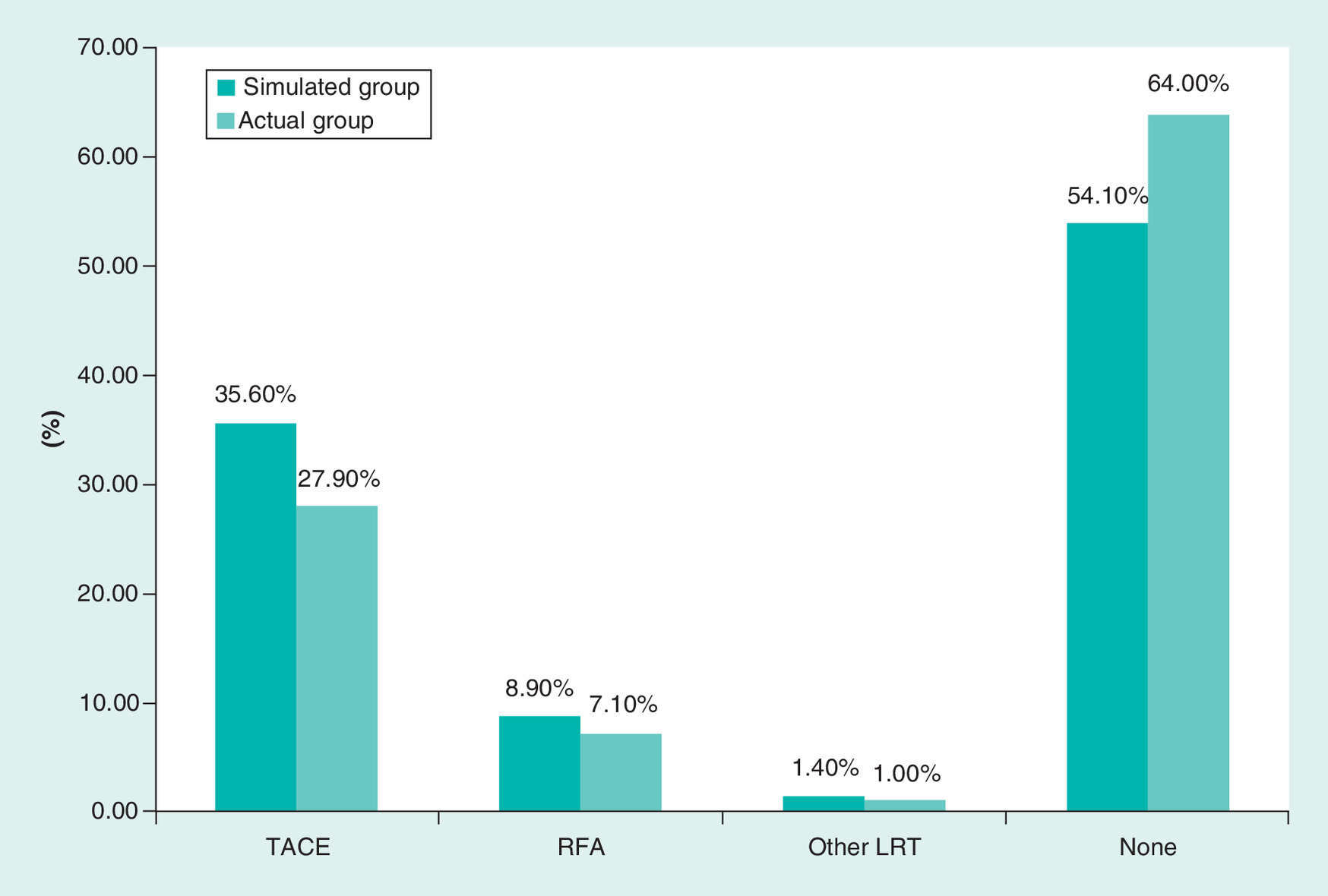
Figure 4. Frequency of bridging locoregional therapy in both actual and simulated groups.
LRT: Locoregional therapy; RFA: Radiofrequency; TACE: Trans-arterial chemoembolization.
Mean OS based on the type of LRT is shown in Table 2 for both actual and simulated groups. The mean OS of patients with LRT in the simulated group was higher than the actual group (p = 0.03). The mean OS of the patients without LRT was also significantly higher in the simulated group, compared with the actual group (p < 0.001).
| LRT status | Actual group (n = 25,476) | Simulated group (n = 17,731) | p-value |
|---|---|---|---|
| Mean OS (months) | Mean OS (months) | ||
| RFA | 98.4 | 100.1 | 0.03 |
| TACE | 97.3 | 98.8 | 0.03 |
| Other | 92.1 | 92.2 | 0.36 |
| No bridging LRT | 91.5 | 95.0 | <0.001 |
| Overall OS | 96.8 | 98.9 | 0.002 |
OS: Overall survival; LRT: Locoregional therapy; RFA: Radiofrequency ablation; TACE: Trans-arterial chemoembolization.
In the actual group, the median OS of the HCC patients with LRT was higher than the patients who did not have bridging LRT (94.2 vs 91.5 months, p < 0.001). The mean OS of the HCC patients who received RFA was 98.4 months, TACE 97.3 months and other LRT 92.1 months (p < 0.001; Figure 5A).
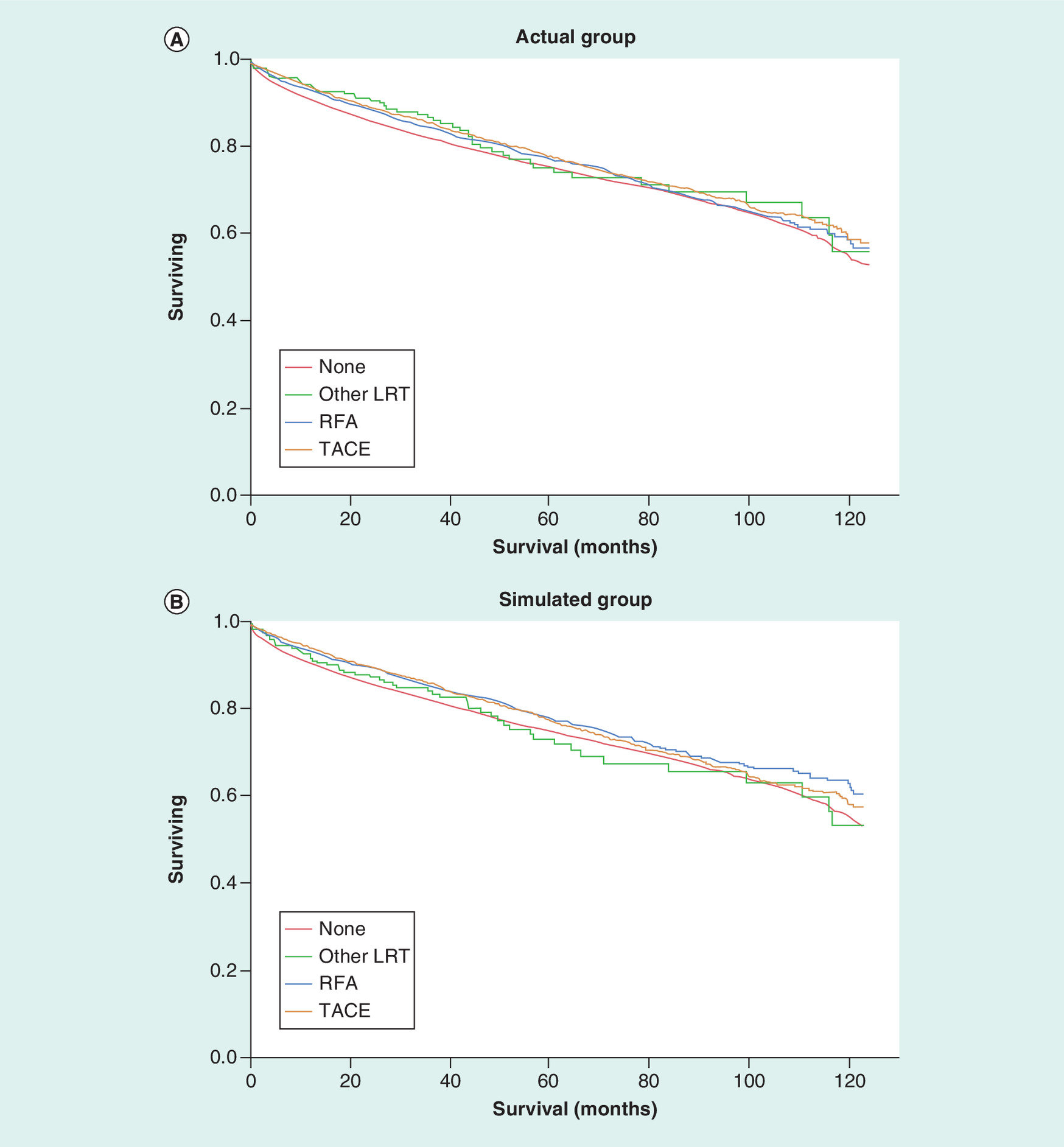
Figure 5. Cumulative survival curves of the studied groups.
Cumulative survival curves comparing hepatocellular carcinoma patients with pre-orthotopic liver transplantation LRT and without LRT in the actual group (A) and simulated group (B).
LRT: Locoregional therapy; RFA: Radiofrequency; TACE: Trans-arterial chemoembolization.
In the simulated group, the median OS of the HCC patients with pretransplant LRT was higher than the HCC patients who did not receive any bridging LRT (96.9 vs 95.0 months; p < 0.001). The mean OS of the HCC patients with RFA was 100.1 months, while the HCC patients with TACE showed median OS of 98.8 months. The patients with other types of LRT had mean OS of 92.2 months (p < 0.001; Figure 5B).
Discussion
Persistent advantage of HCC patients over non-HCC patients in receiving OLT has resulted in multiple adjustments in the MELD exception policy since 2002, with the most recent change in 2015, and new changes in the horizon. Simulating the new changes in the UNOS criteria in the current study demonstrated that 30.4% of transplanted HCC patients would have had approximately 6 months delayed or no allocation to OLT in the same timeframe. Previously, modeling of the new policy on Scientific Registry of Transplant Recipients data have similarly showed that 6-month delay before granting 28 exception points would yield a transplant rate of 44.2 for HCC patients compared with 33.9 for non-HCC candidates, with 6–9 months delay in OLT. This delay may create fairer access to OLT between HCC and non-HCC candidates and reduce the current disparity in transplant rate between these populations [7].
Through the last two decades, an increasing number of HCC patients who are at an increased risk of progression to advanced cancer stages before developing a significant morbid/mortal cirrhotic liver disease have been listed for liver transplantation. Concern for this prompted the OPTN/UNOS to offer an exception score to promote better transplantation results and preserved post-transplantation outcomes by enrolling HCC patients during early stages [10,11] and lowering risk of dropout [12,13]. However, older policies did not allow adequate time to assess tumor biology and behavior and follow-up studies have shown that short HCC waiting times prior to liver transplant or HCC patients transplanted in short waiting-time regions have significantly higher risk of recurrence and decreased post-transplant survival [14,15] and supports at least 6 months of observation prior liver transplant [15,16]. Although our results indicated that the new policy would result in larger tumor size, this did not affect the outcome of transplantation as demonstrated by increased OS.
Our modeling revealed that the increased proportion of patients would have received LRT, particularly more pretransplant TACE, under the new policy. This is believed to be a consequence of larger tumor size and more advanced HCC by the time of transplantation under the new policy. To accommodate waiting time and control dropout rates, LRT plays an extremely important role for controlling tumor growth and keeping the tumor within the Milan criteria for liver transplantation. Prior studies in regions with long wait times for OLT have shown that HCC patients are often treated with LRT, including TACE, to control tumor burden [14] or downstage the HCC [17]. From the other end of the spectrum, several studies have also suggested that response to LRT could be utilized as a useful surrogate for tumor biology and can help select optimal transplant candidates [8,18,19].
Analysis of both old and new policies showed that having any bridging LRT conferred significant differences in OS, when compared with no bridging LRT HCC population under the new policy [20,21]. Our prior sociodemographic study demonstrated the HCC patients with longer wait times and pretransplant OLT had a longer OS [22]. Similar OS benefit post-LRT persisted in the new policy and to greater extent compared with the old policy.
The changes in transplant policy did not impact 1-year post-transplant OS, and the long-term OS at 5-years and 10-years after transplant was only modest. A study comparing regions with short versus long waiting times prior to OLT has similarly shown that long waiting times is associated with a decreased risk of recurrence and increased post-transplant OS, and supports a minimum observation period before OLT [15]. Another observational study also suggested improved post-transplant OS in the patients with longer wait times [23]. This new policy may help to identify and prevent HCC patients who have a more aggressive tumor biology from dropping out of the list during the 6 months observation period before assigning MELD exception score, thus resulting in self-selection of patients with favorable tumor biology and improved chance of HCC disease-free post-transplant OS [24]. Concurrently, increased rates of LRT to prevent waitlist dropout while wait times could have helped to better characterize tumors by their response to LRT or remission after first LRT [20,21]. Furthermore, both old and new policies are permissive of any combination of class 5 lesions meeting Milan criteria, although the new policy does not address the lesions originally beyond Milan criteria and successfully downstaged [25]. An observation period with new policy would allow enough opportunity for reduction in tumor burden and downstaging by LRT, and may even bring HCC tumors outside of Milan criteria to within Milan criteria, and provide an observation period to determine tumor behavior [26].
One limitation is that this study is only simulating the new changes in the MELD exception criteria on the largest available transplant registry database in the USA and a follow-up longitudinal study is required to evaluate the real effect of new policy on rate of OLT, HCC patients drop-out rate and OS. The accuracy of this modeling in predicting OS could have improved by incorporating α-fetoprotein level, imaging characteristics (tumor size or number), tumor biology or post-LRT response. Furthermore, incorporation of Markov model or discrete event simulation with application of sensitivity analysis was impossible due to lack of required data, and a follow-up study from prospective data could analyze the socioeconomic impact of the new policy and increased utilization of the locoregional therapies.
In conclusion, this study showed that the new policy would have resulted in more equality in transplantation between HCC and non-HCC candidates, without affecting significantly the survival of transplanted patients, despite an approximately 6-months delay in waiting list time. Furthermore, this study highlights the importance of the role that LRT plays as a bridge to transplant in HCC patients under the new policy.
Future perspective
The policy could result in more equality in transplantation between HCC and non-HCC candidates. HCC patients would have significantly higher survival, despite an approximately 6-month delay in waiting list time. The number of HCC patients requiring LRT would increase.
•
When the new policy criteria were applied, a total of 17,731 hepatocellular carcinoma (HCC) patients would have received orthotopic liver transplantation (OLT) and 7,745 (30.4%) of currently transplanted patients would have been delayed or not allocated to transplant in the same time frame.
•
Median overall survival (OS) of patients who would have received transplant based on the new criteria was significantly higher than in the patients who were transplanted based on the old criteria.
•
The patients who would have been transplanted based on the new criteria had improved OS after the first 38 months.
•
OS was significantly higher in patients who would have been transplanted based on the new criteria at 5-years and 10-years post-OLT.
•
The rate of bridging locoregional therapy was significantly higher in the patients who would have been transplanted based on the new criteria.
•
Median OS was higher in HCC patients who received locoregional therapy as compared to HCC patients who did not receive locoregional therapy.
•
The new policy, which instituted a 6-month delay in assigning the model for end-stage liver disease (MELD) score exception and MELD exception cap of 34, would likely be associated with higher post-transplant OS, while providing more OLT equity between the HCC and non-HCC populations on the waiting list.
Financial & competing interests disclosure
M Strazzabosco has served on advisory boards for Bayer and Esiai/Merk. HS Kim served on Advisory boards for Boston Scientific and SIRTex. HS Kim is supported by the United States Department of Defense (CA160741). The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
References
1.
Fahrner R, Dondorf F, Ardelt M, Dittmar Y, Settmacher U, Rauchfuss F. Liver transplantation for hepatocellular carcinoma – factors influencing outcome and disease-free survival. World J. Gastroenterol. 21(42), 12071–12082 (2015).
2.
Kornberg A. Liver transplantation for hepatocellular carcinoma beyond milan criteria: multidisciplinary approach to improve outcome. ISRN Hepatol. 2014, 706945 (2014).
3.
UNOS. The United Network for Organ Sharing (2015). www.unos.org
4.
Hart A, Schladt DP, Zeglin J et al. Predicting outcomes on the liver transplant waiting list in the United States: accounting for large regional variation in organ availability and priority allocation points. Transplantation 100(10), 2153–2159 (2016).
5.
Washburn K, Edwards E, Harper A, Freeman R. Hepatocellular carcinoma patients are advantaged in the current liver transplant allocation system. Am. J. Transplant. 10(7), 1643–1648 (2010).
6.
Massie AB, Caffo B, Gentry SE et al. MELD exceptions and rates of waiting list outcomes. Am. J. Transplant. 11(11), 2362–2371 (2011).
7.
Heimbach JK, Hirose R, Stock PG et al. Delayed hepatocellular carcinoma model for end-stage liver disease exception score improves disparity in access to liver transplant in the United States. Hepatology 61(5), 1643–1650 (2015).
8.
Parikh ND, Singal AG. Model for end-stage liver disease exception points for treatment-responsive hepatocellular carcinoma. Clin. Liver Dis. 7(5), 97–100 (2016).
9.
Network OPaT. Revised liver policy regarding HCC exception scores (2015). https://optn.transplant.hrsa.gov/news/revised-liver-policy-regarding-hcc-exception-scores/
10.
Mazzaferro V, Regalia E, Doci R et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N. Engl. J. Med. 334(11), 693–699 (1996).
11.
Toso C, Asthana S, Bigam DL, Shapiro AM, Kneteman NM. Reassessing selection criteria prior to liver transplantation for hepatocellular carcinoma utilizing the Scientific Registry of Transplant Recipients database. Hepatology 49(3), 832–838 (2009).
12.
Goldberg D, French B, Abt P, Feng S, Cameron AM. Increasing disparity in waitlist mortality rates with increased model for end-stage liver disease scores for candidates with hepatocellular carcinoma versus candidates without hepatocellular carcinoma. Liver Transpl. 18(4), 434–443 (2012).
13.
Toso C, Majno P, Berney T, Morel P, Mentha G, Combescure C. Validation of a dropout assessment model of candidates with/without hepatocellular carcinoma on a common liver transplant waiting list. Transpl. Int. 27(7), 686–695 (2014).
14.
Halazun KJ, Patzer RE, Rana AA et al. Standing the test of time: outcomes of a decade of prioritizing patients with hepatocellular carcinoma, results of the UNOS natural geographic experiment. Hepatology 60(6), 1957–1962 (2014).
15.
Terzi E, Ray Kim W, Sanchez W et al. Impact of multiple transarterial chemoembolization treatments on hepatocellular carcinoma for patients awaiting liver transplantation. Liver Transpl. 21(2), 248–257 (2015).
16.
Mehta N, H J, Harnois DM et al. Short waiting time predicts early recurrence of hepatocellular carcinoma after liver transplantation: a multicenter study supporting the “ablate and wait” principle. Hepatology 60, 446A (2014).
17.
Yao FY, Mehta N, Flemming J et al. Downstaging of hepatocellular cancer before liver transplant: long-term outcome compared with tumors within Milan criteria. Hepatology 61(6), 1968–1977 (2015).
18.
Mehta N, Dodge JL, Goel A, Roberts JP, Hirose R, Yao FY. Identification of liver transplant candidates with hepatocellular carcinoma and a very low dropout risk: implications for the current organ allocation policy. Liver Transpl. 19(12), 1343–1353 (2013).
19.
Kim YS, Lim HK, Rhim H, Lee WJ, Joh JW, Park CK. Recurrence of hepatocellular carcinoma after liver transplantation: patterns and prognostic factors based on clinical and radiologic features. AJR Am. J. Roentgenol. 189(2), 352–358 (2007).
20.
Xing M, Sakaria S, Dhanasekaran R et al. Bridging locoregional therapy prolongs survival in patients listed for liver transplant with hepatocellular carcinoma. Cardiovasc. Intervent. Radiol. 40(3), 410–420 (2017).
21.
Oligane HC, Xing M, Kim HS. Effect of bridging local-regional therapy on recurrence of hepatocellular carcinoma and survival after orthotopic liver transplantation. Radiology 282(3), 869–879 (2017).
22.
Magnetta MJ, Xing M, Zhang D, Kim HS. The effect of bridging locoregional therapy and sociodemographics on survival in hepatocellular carcinoma patients undergoing orthotopic liver transplantation: a United Network for Organ Sharing Population Study. J. Vasc. Interv. Radiol. 27(12), 1822–1828 (2016).
23.
Freeman RB, Jr., Steffick DE, Guidinger MK, Farmer DG, Berg CL, Merion RM. Liver and intestine transplantation in the United States, 1997-2006. Am. J. Transplant. 8(4 Pt 2), 958–976 (2008).
24.
Jadlowiec CC, Heimbach JK. Advances in how we prioritize liver allocation for hepatocellular carcinoma in the USA. Curr. Transpl. Rep. 3(4), 334–340 (2016).
25.
Yao FY, Xiao L, Bass NM, Kerlan R, Ascher NL, Roberts JP. Liver transplantation for hepatocellular carcinoma: validation of the UCSF-expanded criteria based on preoperative imaging. Am. J. Transplant. 7(11), 2587–2596 (2007).
26.
Elshamy M, Aucejo F, Menon KV, Eghtesad B. Hepatocellular carcinoma beyond Milan criteria: management and transplant selection criteria. World J. Hepatol. 8(21), 874–880 (2016).
Information & Authors
Information
Published In
Pages: 993 - 1002
PubMed: 31512955
Copyright
© 2019 Future Medicine Ltd.
History
Received: 22 December 2017
Accepted: 10 April 2018
Published online: 12 September 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Modeling of implementation of the new Organ Procurement and Transplantation Network/United Network for Organ Sharing policy for patients with hepatocellular carcinoma. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0076
Export citation
Select the citation format you wish to export for this article or chapter.