Factors associated with delay in presentation among patients for oral cancer
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This study aimed to determine factors that influence delay in presentation among oral cancer patients. Materials & methods: A cross-sectional study with 128 Oral cancer patients receiving treatment from the Hospital of Stomatology, at Jilin University, in China, was conducted. Results: A total of 78 patients delayed seeking treatment for more than 3 weeks after noticing symptoms of oral anomaly. Patients who were male, farmers (Odds ratio [OR] = 2.617; 95% CI: 1.90–3.64), or currently smoking (OR = 4.651; 95% CI: 1.21–9.46), were more likely to delay. Patients alerted to the problem at a physical exam had much lower risk of delay than patients who discovered the disease independently (OR = 0.029; 95% CI: 0.01–0.30). Higher coping style scores (OR = 0.747; 95% CI: 0.47–1.18) and oral cancer knowledge scores (OR = 0.886; 95% CI: 0.60–2.01) were significantly correlated with shorter delays. Conclusion: Delay in presentation may be achieved through regular oral health screening and improved public education about factors influencing delay.
Oral cancer is the sixth most common form of cancer worldwide [1]. It includes some kinds of neoplasms inside the mouth and tumors on the lips, tongue, gums, hard and soft palates, salivary glands, tonsils, oropharynx, nasopharynx and hypopharynx [2]. The diagnosis of malignant oral cavity tumors results in profound and lasting physical and psychological effects on patients [3]. These consequences usually comprise possible health and quality of life-related impairments (for example, affecting articulation, chewing, swallowing and physical appearance) [4], as well as potential psychological impacts including changes to perceived autonomy and greater proneness toward depression or anxiety [5,6].
Despite advances in treatment of oral cancer in recent years, the 5-year survival rate has not improved notably [7,8]. Early oral malignant lesions are usually asymptomatic. Obvious symptoms such as ulceration, pain, unexplained bleeding or a mass [9], only present in late stages of malignancy, which means that most oral cancers have developed to the advanced stage by the time the patient visits the clinic. Late presentation is an important issue as advanced disease requires more radical treatment and is associated with poorer prognosis [10]. Schrijvers et al. [11] propose that survival rates could be improved by up to 30% if people consult a doctor in a timely way during the early stages. Increased knowledge of risk factors and the symptoms of oral cancer remains the most effective method to control the morbidity and mortality associated with this disease [12]. Patients presenting with cancer at an advanced stage might immensely increase distress levels for themselves and their families, while also worsening health-related quality of life outcomes and survival rates after therapy [13]. Therefore, in order to prevent late presentations, it is significant to identify the factors associated with such delays.
Patient delay was defined in our study as the time taken by patients to first seek professional advice after becoming aware of abnormal symptoms. Patients were deemed to have delayed if more than 3 weeks had passed between first symptoms detection and seeking professional medical help. According to public health promotion literature, it is recommended that patients experiencing potentially malignant oral symptoms for 2 weeks should seek professional medical opinion. The 3-week timespan included in our study allows extra time to make an appointment to see a dentist.
Some factors have been reported to be associated with the delay in presentation of oral cancer, including sociodemographic variables [14], patients’ health-related behaviors (such as smoking or alcohol consumption) [15], date of first symptom, date of first seeing a dentist or the method they found out about their problem [16]. In addition, a recent study found significant relationships between active coping style and delay in presentation [17]. Another study showed that the best way to improve delay in presentation was through improved knowledge of the oral cancer risk factors [18]. Investigating the factors associated with patient delay has important implications for those at risk of suffering from oral cancer. The objective of this study is to describe delay in presentation among patients with oral cancer province of Jilin in China, and to identify factors associated with this delay, so as to provide evidence of the need for a program for delay prevention among patients. It is hypothesized that delay in presentation will not be predicted by the sociodemographic characteristics of the patient, help-seeking behaviors, approach to seeking treatment for their oral health difficulties or knowledge of the oral cancer and coping style.
Material & methods
Participants
Convenience sampling was used to recruit participants for this study. The Department of Oral and Maxillofacial Surgery in the Hospital of Stomatology, at the University of Jilin in China was selected as the setting for data collection. Recruitment took place and the study was conducted between April of 2018 and March of 2019. Patients were eligible to take part in the study if they were aged 18 or older and were pathologically diagnosed with oral cancer. Doctors were involved in deciding whether or not patients were included. Patients with mental disorders and either recurrent oral cancer or oral cancer that was concomitant with other cancerous tumors were excluded. The investigators visited the cancer ward to carry out the interviews. Each interview took approximately 15 to 20 min and was conducted in a private room.
Ethics approval
This study protocol was approved by the research ethics committee of the institution where recruitment took place (permission number 1, dated 9 April 2018). All patients gave the written informed consent to participate, according to the Declaration of Helsinki, before taking part in the study.
Measures
Information collected using the general information questionnaire included sociodemographic data about the participants (age, gender, marital status, education level, employment, monthly income), health-related behaviors (smoking status, drinking status, health insurance, use of dentures, place of residence and residence status) as well as information about their approach to seeking treatment for their oral health difficulties (date of first symptom, date of first seeing a dentist and how they found out about their problem).
The previously validated HUMPHRIS Oral Cancer Knowledge Scale (HOCKS) [19] was used to assess participants’ knowledge of oral cancer. Some items about UK oral cancer epidemiology were excluded. Two HOCKS subscales were used, including 13 items for assessing knowledge of risk factors and eight questions for assessing signs of oral cancer. All of the items have only dichotomized responses (‘true’ or ‘false’). The scores range from 0 to 21, with higher scores representing a more accurate knowledge level. In the present study, the Cronbach’s alpha coefficient of HOCKS was 0.826.
The coping styles were measured using the Chinese version of the Medical Coping Style Questionnaire (MCSQ) [20]. The scale was originally developed by Feifel et al. [21] and includes three dimensions: confrontation (8 items), resignation (7 items) and avoidance (5 items). Each of the dimensions utilizes a 4-point Likert-type scale, ranging from ‘1 = never’ to ‘4 = always’. The total scores range from 20 to 80. The more often a response was given, the higher the related factor score. The Chinese version of the MCSQ has established validity and reliability and is widely used in Chinese studies [22]. In the present study, the Cronbach’s alpha coefficients of the three dimensions of the MCSQ were 0.816, 0.782 and 0.796, respectively.
Statistical analysis
Analyses were performed using the Statistical Package for the Social Sciences (IBM SPSS Statistics for Windows, NY, USA, version 22.0), and the Kolmogorov–Smirnov test was applied to validate the hypothesis of normality for study variables (p > 0.05). For categorical variables, data are presented using numbers and percentages, while continuous variables are represented as means and standard deviations (SD). Delay time is expressed using median and interquartile range. Univariate logistic regression was used to determine differences between the study variables and patient delay. The patient delay (>3 weeks) or no delay (<3 weeks) was analyzed as a dependent variable and factors significantly related to patient delay were then entered into a multifactor logistic regression analysis to test their significance. All analyses were two-tailed, and p-value <0.05 was considered statistically significant.
Results
A total of 140 cancer patients who met the inclusion criteria were invited to participate in this survey. Among all the retrieved questionnaires, 12 were invalid, leaving 128 (91.43%) included in the final analysis. The general characteristics of participants are presented in Table 1. Most of the patients with oral cancer were men (68.7%). Approximately half of the patients were between 18 and 45 years of age. A total of 75.8% of participants were married. It was found that 40.6% reported monthly income of 1000 to 3000 RMB. Farmers comprised the largest proportion of respondents. Additionally, 43.8% of participants current smoked.
| Variables | Characteristics of sample | |
|---|---|---|
| n | % | |
| Gender | ||
| – Males | 88 | 68.7 |
| – Females | 40 | 31.3 |
| Age group (years) | ||
| – 18–45 | 63 | 49.2 |
| – 45–60 | 40 | 31.3 |
| – ≥60 | 25 | 19.5 |
| Marital status | ||
| – Married | 97 | 75.8 |
| – Divorce | 6 | 4.7 |
| – Single | 25 | 19.5 |
| Education level | ||
| – Primary school | 14 | 10.9 |
| – Middle school | 54 | 42.2 |
| – High school | 27 | 21.1 |
| – ≥Graduate | 33 | 25.8 |
| Monthly income, RMB | ||
| – <1000 | 42 | 32.8 |
| – 1000–3000 | 52 | 40.6 |
| –3000–5000 | 25 | 19.6 |
| – >5000 | 9 | 7 |
| Employment | ||
| – Technician | 22 | 17.2 |
| – Farmer | 31 | 24.2 |
| – Worker | 25 | 19.5 |
| – Businessman | 4 | 3.1 |
| – Servicer | 5 | 3.9 |
| – Retiree | 15 | 11.7 |
| – Others | 26 | 20.3 |
| Smoking status | ||
| – Never smoked | 53 | 41.4 |
| – Stop smoking | 19 | 14.8 |
| – Currently smoking | 56 | 43.8 |
| – Place of residence | ||
| – Rural area | 52 | 40.6 |
| – City or town | 76 | 59.4 |
| Method of discovering difficulty | ||
| – Independently | 41 | 32 |
| – Pain | 66 | 51.6 |
| – Physical exam | 4 | 3.1 |
| – Others | 17 | 13.3 |
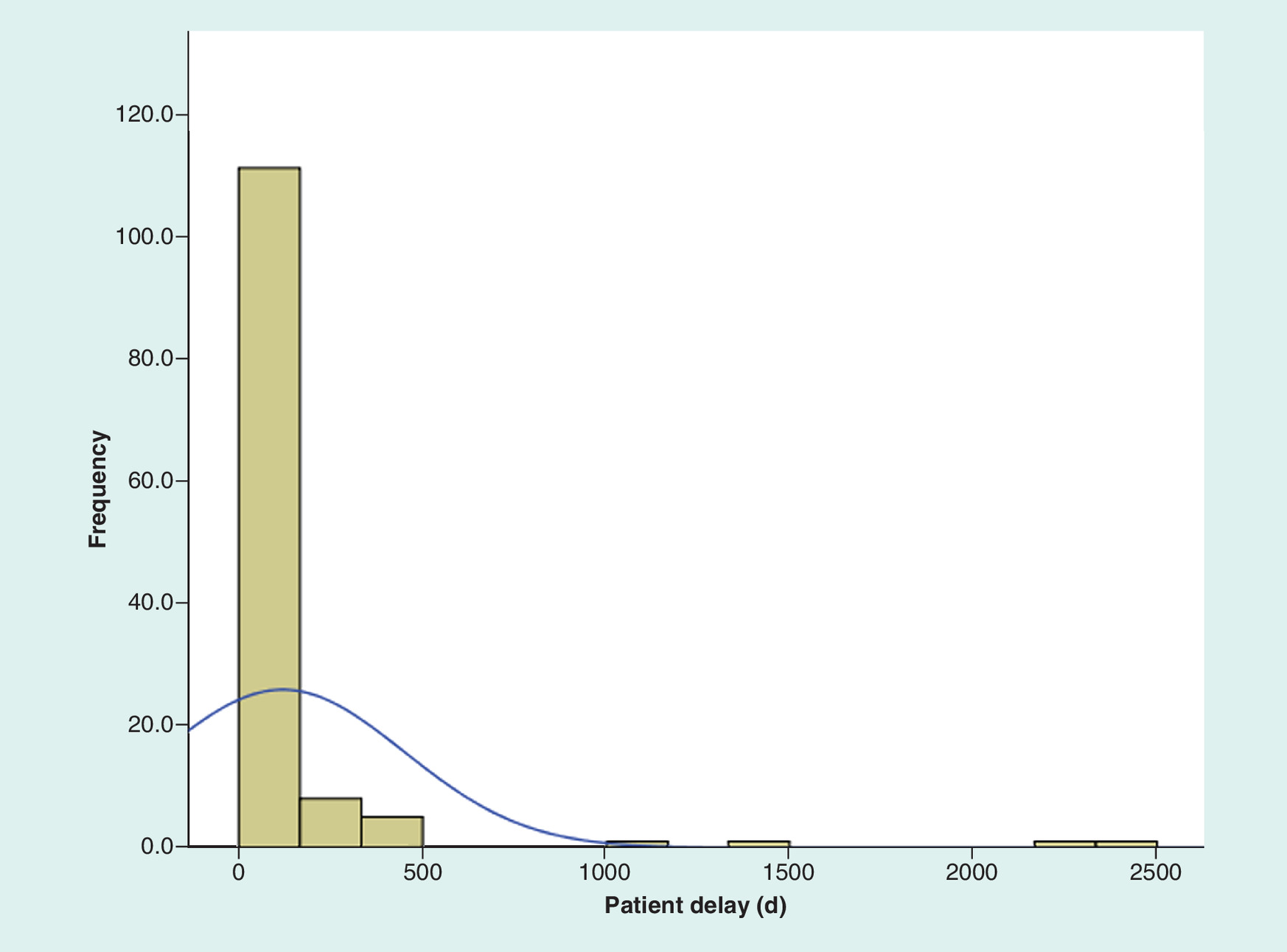
Regarding medical seeking information, 51.6% of participants found their abnormal oral symptoms as a result of experiencing pain, and the largest proportion of the sample reported to the regional center hospital when the symptom occurred. The mean score for oral cancer knowledge on the HOCKS was 10.19 (SD = 2.83). The mean score for coping style on the MCSQ was 45.11 (SD = 6.38). Figure 1 shows the distribution of delay in presentation and demonstrates the positive skew. The duration of patient delay ranged from 0 to more than 5 years. The median duration of delay in presentation was 30 days. Using the cutoff of more than 3 weeks, 78 participants (60.9%) were considered to have experienced prolonged patient delay and 50 participants (39.1%) did not delay in presentation.
Univariate logistic regression revealed that gender, age, education level, monthly income, employment, smoking status, place of residence, the method by which patients discovered their difficulty, oral cancer knowledge and coping style were significantly associated with patient delay in presentation for oral cancer. The results are shown in Table 2. In the multifactor logistic regression, we further found that there was a greater delay among patients who were male, farmers and had a history of smoking (Table 3). Patients who were farmers had a twofold higher risk of delay compared with those who were technicians (Odds ratio [OR] = 2.617; 95% CI: 1.90–3.64). Likewise, patients who had stopped smoking (OR = 3.742; 95% CI: 1.41–8.54) and those who were currently smoking (OR = 4.651; 95% CI: 1.21–9.46) had a higher risk of delay compared with the patients who had never smoked. Female patients had a lower risk of delay compared with male patients (OR = 0.044; 95% CI: 0.01–0.84). Patients whose difficulty had been discovered during a physical exam had a much lower risk of delay compared with patients who discovered the disease independently (OR = 0.029; 95% CI: 0.01–0.30). In addition, patients with higher coping style scores (OR = 0.747; 95% CI: 0.47–1.18) and higher oral cancer knowledge scores (OR = 0.886; 95% CI: 0.60–2.01) had a lower risk of delay.
| Variables | β | SE | p-value | OR | 95% CI | |
|---|---|---|---|---|---|---|
| Gender | 5.310 | 3.117 | 0.026 | 4.984 | 0.944 | 6.439 |
| Age | 9.792 | 5.066 | 0.034 | 6.753 | 5.450 | 8.032 |
| Education level | 7.252 | 2.373 | 0.040 | 6.745 | 1.043 | 10.040 |
| Monthly income | 1.407 | 2.560 | 0.037 | 6.844 | 3.447 | 7.978 |
| Employment | 3.438 | 1.078 | 0.006 | 9.536 | 1.052 | 17.344 |
| Smoking status | 1.076 | 1.434 | 0.019 | 7.924 | 2.320 | 10.329 |
| Place of residence | 2.118 | 1.468 | 0.009 | 6.817 | 3.091 | 7.973 |
| Method of discovering difficulty | 1.064 | 1.017 | 0.002 | 17.178 | 6.039 | 20.894 |
| Oral cancer knowledge | -0.262 | 0.104 | 0.012 | 0.770 | 0.628 | 0.943 |
| Coping style | 0.415 | 0.080 | 0.001 | 1.514 | 1.295 | 1.770 |
OR: Odds ratio; SE: Standard error.
| Variables | Delay n (%) | No delay n (%) | β | SE | p-value | OR | 95% CI | ||
|---|---|---|---|---|---|---|---|---|---|
| Gender | Males | 22 (17.19) | 18 (14.06) | — | — | — | 1.0 | — | — |
| Females | 30 (23.44) | 58 (45.31) | -3.120 | 1.506 | 0.038 | 0.044 | 0.01 | 0.84 | |
| Employment | Technician | 2 (1.56) | 29 (22.66) | — | — | — | 1.0 | — | — |
| Farmer | 9 (7.03) | 16 (12.50) | 9.477 | 2.590 | 0.004 | 2.617 | 1.90 | 3.64 | |
| Worker | 12 (9.38) | 10 (7.81) | 3.811 | 2.267 | 0.093 | 4.236 | 0.01 | 6.53 | |
| Businessman | 1 (0.78) | 3 (2.34) | -0.344 | 1.127 | 0.946 | 0.709 | 0.08 | 6.45 | |
| Servicer | 3 (2.34) | 2 (1.56) | 3.109 | 1.830 | 0.089 | 2.399 | 0.62 | 5.35 | |
| Retiree | 6 (4.69) | 9 (7.03) | 2.805 | 1.860 | 0.175 | 6.528 | 0.43 | 9.16 | |
| Others | 19 (14.84) | 7 (5.47) | 1.085 | 1.117 | 0.332 | 2.959 | 0.33 | 6.43 | |
| Smoking status | Never smoked | 28 (21.88) | 26 (20.31) | — | — | — | 1.0 | — | — |
| Stop smoking | 15 (11.72) | 41 (32.03) | 2.620 | 1.160 | 0.024 | 3.742 | 1.41 | 8.54 | |
| Currently smoking | 9 (7.03) | 9 (7.03) | 2.366 | 1.108 | 0.033 | 4.651 | 1.21 | 9.46 | |
| Method of discovering difficulty | Independently | 9 (7.03) | 32 (25) | — | — | — | 1.0 | — | — |
| Pain | 41 (32.03) | 25 (19.53) | -1.518 | 1.209 | 0.209 | 0.219 | 0.02 | 2.34 | |
| Physical exam | 0 (0) | 4 (3.13) | -3.531 | 1.185 | 0.003 | 0.029 | 0.01 | 0.30 | |
| Others | 2 (1.56) | 15 (11.72) | 7.882 | 11.097 | 0.987 | 12.804 | 0.01 | 24.12 | |
| Oral cancer knowledge | mean (SD) | 9.24 (2.65) | 11.58 (2.52) | -3.555 | 1.153 | 0.029 | 0.886 | 0.60 | 2.01 |
| Coping style | mean (SD) | 40.21 (5.0) | 48.46 (4.89) | -1.338 | 1.070 | 0.034 | 0.747 | 0.47 | 1.18 |
OR: Odds ratio; SD: Standard deviation.
Discussion
The aim of this study was to explore the factors associated with patient delay in presentation for oral cancer. We found a more than 3 weeks patient delay for 60.9% of oral cancers with potentially malignant oral symptoms, with a median length of delay of one month. This length of time was consistent with the findings of a previous study by Olesen et al. reporting on patients’ delay in seeking treatment in Iran [23]. In contrast, patient delay in seeking treatment for oral cancer symptoms was about 7 to 8 weeks in India [24]. In a study from Canada, the average delay was shown to be 12 weeks [25]. Early recognition is essential for purposes of improving survival rates, preserving oral function and enhancing overall esthetic and psychological outcomes.
It is uncertain whether gender is an associated factor for oral cancer patients’ delay in presentation. One study [26] showed that men demonstrated more delay than women. This result is similar to our conclusion. Paying more attention to oral health and potential lesions in this area for women may explain the greater delay among men. However, in another related study [27] investigating the association between delay in seeking treatment and psychological factors among 277 patients with cancer of the head and neck, the evidence indicated that gender was not related to patient delay in seeking medical help. Men are considered to be at high risk for oral cancer, and most of the patients in our study were men, so there may need to be more research conducted with women, in order to draw a conclusion about the impact of gender on delay time.
There seems to be an inseparable relationship between occupation and economic conditions. The economic status of people with higher social status is relatively better. The relationship between occupation and patient delay behavior warrants further investigation because this has been verified to be an influential factor in the study of patient delay [13,28]. Lower occupational social class was found by Llewellyn et al. [16] to be associated with longer patient delay, with higher morbidity and mortality in the more deprived people. Scott et al. [28] found that impoverished patients were less likely to find malignant lesions in the early stages, which further supports Llewellyn et al.’s[16] finding that patients with lower socioeconomic status were more likely to delay in seeking treatment help. The result of our study can be explained by the fact that the patient sample comes from the economically deprived population in the city of Changchun rather than the more prosperous coastal cities of China. After noticing the early symptoms, patients may attempt self-treatment due to economic constraints, which could account for their delay in seeking professional medical attention.
A total of 100 patients with squamous cell carcinoma of the oral cavity were examined in one study [29]. The result found that patient delay in seeking treatment was related to whether the patients were heavy smokers. Similarly, we also found in our study that risk of delay for patients who smoked either currently or in the past was much higher than for patients who had never smoked. However, another study [9] found that delay was inversely related to the amount of tobacco that patients smoked. The results in that case suggested that risk of delay was higher for those who smoked less tobacco. One reason for this latter finding may be that nonsmokers or light smokers realize their own low risk, causing them to mislabel symptoms as insignificant, thus leading to a delay in seeking professional advice. The relationship between delay and the amount of tobacco that patients smoked will be examined in our further study.
The method by which patients discovered their difficulty was associated with patient delay in presentation in our study. Regular physical examinations could significantly reduce patient delay in seeking treatment when problems arise. One study [9] investigated patients of an oral medicine clinic in Australia. Most participants reported that experiencing an ulcer, as a common initial symptom, had caused them to actively seek help. In contrast, the method by which patients discovered their symptoms was not found to have an association with patient delay in another study [16]. This could be because some of the early symptoms of oral cancer, such as ulcers or growths, are not uncommon in the oral cavity [9]. Alternatively, it may also be the case that the patients understand very little about the clinical manifestations of oral cancer [30]. Therefore, early and more widespread adoption of oral cavity screening and overall examinations for head cancer, have the potential to detect asymptomatic cancers at early stages and prompt those who show symptoms to consult a health care professional [31].
Medical seeking and sociodemographic variables can only explain patient delay in part. There was a general lack of knowledge about oral cancer among the participants in the current study, which proved the delay was associated with a lack of understanding of the symptoms of oral carcinoma and its risk factors. Other research [32] has also shown that patients with more accurate knowledge of oral cancer were unlikely to delay seeking help. Oral cancer knowledge is associated with a greater likelihood of seeking out oral cancer screening, thus promoting early detection. One qualitative study [9], which investigated oral cancer patients’ perceptions of their initial symptoms, found that approximately half of the participants interpreted common symptoms such as a pain or nonhealing ulcer, as something minor and rarely gave thought as to whether it might be oral cancer. One possible explanation, in the case of our study, is that most of the respondents had a low level of education and a lack of knowledge of early oral cancer symptoms, which led them to delay in seeking treatment. Thus, the best way to get patients to self-refer earlier may be through strengthening public education to improve knowledge of oral disease.
Our research also demonstrated that coping style was related to patient delay in seeking care. The nature of this relationship will need to be further validated in future research, which we are planning to conduct. Research by Tromp et al. [27] was supportive of this premise, as their study demonstrated that patient delay was positively related to avoidance coping style, and patients who postponed medical seeking for longer periods of time made less use of the active coping style. This is in agreement with other research as well, as Lauver and Tak [33] found that patient delay was associated with avoidance coping style and patients who postponed the medical consultation for more than one month made less effort in seeking medical support. Thus, it seems essential to ensure that interventions be directed at decreasing negative coping styles and improving positive coping styles for oral cancer patients.
Several limitations of this study should be kept in mind when interpreting the current findings. First, this study used a cross-sectional design rather than a longitudinal one, a factor which prevents us from drawing any causal conclusions. Second, our study recruited convenience samples with oral cancer from only certain regions in China and, therefore, the findings cannot be used to make generalizations to other developed areas and countries. Third, this study used questionnaires to ask patients to recall early symptoms and when they appeared. The accuracy of this information is limited by patient recall and by the level of significance they attached to these symptoms.
Conclusion
Overall, our study demonstrates that lack of regular screening is associated with delay in presentation among oral cancer patients in our population. Similarly, negative coping style and lack of knowledge about oral cancer also seem to contribute toward this delay. These identified factors associated with it may be used in designing an intervention program for reducing patient delay. Specifically, the most feasible way to better inform the public about early symptoms of oral cancer, may be through regular screening of the oral mucosa with patients at greatest risk.
•
Oral cancer is the sixth most common form of cancer worldwide.
•
Patients presenting with cancer at an advanced stage might immensely increase distress levels for themselves, while also worsening quality of life outcomes and survival rates.
•
Patient delay was defined as the time taken by patients to first seek professional advice after becoming aware of abnormal symptoms.
•
A cross-sectional study was conducted between April of 2018 and March of 2019.
•
A total of 78 patients (60.9%) delayed seeking treatment for more than 3 weeks after noticing symptoms of oral anomaly.
•
Patients who were male, farmers, or currently smoking were more likely to delay in presentation.
•
Patients alerted to the problem at a physical exam had much lower risk of delay than patients who discovered the disease independently.
•
Higher coping style scores and oral cancer knowledge scores were significantly correlated with shorter delays.
•
Patient delay may be reduced through regular oral health screening and improved public education about factors influencing delay.
Author contributions
XY Zhang and LJ Bian were involved in the conception and design of the study, DL Liu, HM Dong and BY Zhang were involved in the drafting of the paper or revising it critically for intellectual content; Y Zhang and XY Zhang were involved in the analysis and interpretation of the data; YX Li and XL Wang were involved and in the final approval of the version to be published. All authors agree to be accountable for all aspects of the work.
Acknowledgments
We thank the authors of all of the included studies.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Hsu HW, Wall NR, Hsueh CT et al. Combination antiangiogenic therapy and radiation in head and neck cancers. Oral Oncol. 50, 19–26 (2014).
2.
Little JW, Falace DA, Miller CS, Rhodus NL. Dental Management of the Medically Compromised Patients (8th Edition). Mosby Co., St Louis, MO, USA, 475 (2013).
3.
Kessler PA, Bloch-Birkholz A, Leher A, Neukam FW, Wiltfang J. Evaluation of quality of life of patients with oral squamous cell carcinoma. Comparison of two treatment protocols in a prospective study. Radiother. Oncol. 70, 275 – 282 (2004).
•• Shows the quality of life of oral cancer survivors.
4.
So WK, Chan RJ, Chan DN et al. Quality-of-life among head and neck cancer survivors at one year after treatment–a systematic review. Eur. J. Cancer 48, 2391–2408 (2012).
•• Reports association between quality of life, coping styles in patients with oral cancer survivors.
5.
Horney DJ, Smith HE, McGurk M et al. Associations between quality of life, coping styles, optimism, and anxiety and depression in pretreatment patients with head and neck cancer. Head Neck 33, 65–71 (2011).
6.
Haisfield-Wolfe ME, McGuire DB, Krumm S. Perspectives on coping among patients with head and neck cancer receiving radiation. Oncol. Nurs. Forum 39, 249–257 (2012).
7.
Scott SE, Grunfeld EA, McGurk M. Patient's delay in oral cancer: a systematic review. Community Dent. Oral Epidemiol. 34, 337–343 (2010).
8.
Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J. Clin. 60, 277–300 (2010).
• Proves reason for delayed in oral cancer.
9.
Rogers SN, Vedpathak SV, Lowe D. Reasons for delayed presentation in oral and oropharyngeal cancer: the patients perspective. Br. J. Oral Maxillofac. Surg. 49, 349–353 (2011).
10.
Rogers SN, Brown JS, Woolgar JA et al. Survival following primary surgery for oral cancer. Oral Oncol. 45, 201–211 (2009).
11.
Schrijvers CT, Mackenbach JP, Lutz JM, Quinn MJ, Coleman MP. Deprivation, stage at diagnosis and cancer survival. Int. J. Cancer 63, 324–329 (1995).
12.
Scully C. Challenges in predicting which oral mucosal potentially malignant disease will progress to neoplasia. Oral Dis. 20(1), 1–5 (2014).
13.
Rogers SN, Pabla R, McSorley A, Lowe D, Brown JS, Vaughan ED. An assessment of deprivation as a factor in the delays in presentation, diagnosis and treatment in patients with oral and oropharyngeal squamous cell carcinoma. Oral Oncol. 43(7), 648–655 (2007).
14.
Esmaelbeigi F, Hadji M, Harirchi I, Omranipour R, vand Rajabpour M, Zendehdel K. Factors affecting professional delay in diagnosis and treatment of oral cancer in Iran. Arch. Iran Med. 17(4), 253–257 (2014).
15.
Feng XF, Huang HT, Wang R. Analysis of delay in seeking medical treatment of oral cancer patients and its influencing factors. J. Oral Sci. Res. 32(7), 716–719 (2016).
16.
Llewellyn CD, Johnson NW, Warnakulasuriya S. Factors associated with delay in presentation among younger patients with oral cancer. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 97, 707–713 (2004).
17.
Facione NC, Miaskowski C, Dodd MJ, Paul SM. The self-reported likelihood of patient delay in breast cancer: new thoughts for early detection. Prev. Med. 34, 397–407 (2002).
18.
Noonan B. Understanding the reasons why patients delay seeking treatment for oral cancer symptoms from a primary health care professional: an integrative literature review. Eur. J. Oncol. Nurs. 18, 118–124 (2014).
19.
Humphris GM, Duncalf M, Holt D, Field EA. The experimental evaluation of an oral cancer information leaflet. Oral Oncol. 35, 575 (1999).
20.
Wang XD, Wang XL, Ma H. Manual of mental health rating scale. Chin. Mental Health 13, 124–127 (1999).
21.
Feifel H, Strack S, Na VT. Coping strategies and associated features of medically ill patients. Psychosom. Med. 49, 616–625 (1987).
22.
Shen XH, Jiang QJ. Report on application of Chinese version of MCMQ in 701 patients. Chin J. Behav. Med. 1, 22–24 (2000).
23.
Olesen F, Hansen RP, Vedsted P. Delay in diagnosis: the experience in Denmark. Br. J. Cancer 101, S5–S8 (2009).
24.
Srikanth Reddy B, Doshi D, Padma Reddy M, Kulkarni S, Gaffar A, Ram Reddy V. Oral cancer awareness and knowledge among dental patients in South India. J. Craniomaxillofac. Surg. 40, 521–524 (2012).
25.
Gao W, Guo CB. Factors related to delay in diagnosis of oral squamous cell carcinoma. China J. Oral Maxil. Surg. 67, 1015 (2009).
26.
Pitiphat W, Diehl SR, Laskaris G, Cartsos V, Douglass CW, Zavras AI. Factors associated with delay in the diagnosis of oral cancer. J. Dent. Res. 81, 192–197 (2002).
27.
Tromp DM, Brouha XD, De Leeuw JR, Hordijk GJ, Winnubst JA. Psychological factors and patient delay in patients with head and neck cancer. Eur. J. Cancer 40, 1509–1516 (2004).
28.
Scott S, McGurk M, Grunfeld E. Patient delay for potentially malignant oral symptoms. Eur. J. Oral Sci. 116, 141–147 (2008).
29.
Hollows P, McAndrew PG, Perini MG. Delays in the referral and treatment of oral squamous cell carcinoma. Br. Dent. J. 188, 262–265 (2000).
30.
Hertrampf K, Wenz HJ, Koller M, Wiltfang J. Public awareness about prevention and early detection of oral cancer: a population-based study in Northern Germany. J. Craniomaxillofac. Surg. 40, e82–e86 (2012).
31.
Gómez I, Warnakulasuriya S, Varela-Centelles PI et al. Is early diagnosis of oral cancer a feasible objective? Who is to blame for diagnostic delay? Oral Dis. 16, 333–342 (2010).
32.
Dost F, Do L, Farah CS. Knowledge of oral cancer risk factors amongst high-risk Australians: findings from the LESIONS programme. Aust. Dent. J. 61, 432–439 (2016).
33.
Lauver D, Tak Y. Optimism and coping with a breast cancer symptom. Nurs. Res. 44, 202–207 (1995).
Information & Authors
Information
Published In
Pages: 1003 - 1071
PubMed: 31290337
Copyright
© 2019 Future Medicine Ltd.
History
Received: 3 June 2019
Accepted: 27 June 2019
Published online: 10 July 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Factors associated with delay in presentation among patients for oral cancer. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0067
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Lidiane de Jesus Lisboa, Jean Carlos Zambrano Contreras, Valéria Souza Freitas, Influencia de la Raza/Color de Piel en los Retrasos en la Atención del Cáncer de Cavidad Oral en el Brasil: El Papel Mediador de la Geografía y la Gravedad Clínica, Revista Brasileira de Cancerologia, 10.32635/2176-9745.RBC.2026v72n3.5630ES, 72, 3, (e145630), (2026).
- Lidiane de Jesus Lisboa, Jean Carlos Zambrano Contreras, Valéria Souza Freitas, Ethnic-racial relationships within the healthcare service for the diagnosis and treatment of oral cavity cancer in Brazil, Revista Brasileira de Cancerologia, 10.32635/2176-9745.RBC.2026v72n3.5630EN, 72, 3, (e145630), (2026).
- Lidiane de Jesus Lisboa, Jean Carlos Zambrano Contreras, Valéria Souza Freitas, Influência da Raça/Cor da Pele nos Atrasos Assistenciais ao Câncer de Cavidade Oral no Brasil: O Papel Mediador da Geografia e da Gravidade Clínica, Revista Brasileira de Cancerologia, 10.32635/2176-9745.RBC.2026v72n3.5630, 72, 3, (2026).
- Sira Stanslaus Owibingire, Irene Kida Minja, Elison Nathaniel Simon, Daniela Elena Costea, Anne Nordrehaug Astrom, Assessing the covariates of delay in seeking health care among patients with oral and oropharyngeal squamous cell carcinoma in Tanzania, BMC Cancer, 10.1186/s12885-026-15572-8, (2026).
- Guru C. Sahu, Ravi Shankar, Hitesh R. Singhavi, Dipti Daga, Dharmendra K. Rai, Monika Gupta, Aseem Mishra, Delay in the diagnosis of oral cancer in India, time to focus toward capacity building of physicians: A prospective observational study, Indian Journal of Cancer, 10.4103/ijc.ijc_44_22, 62, 1, (128-134), (2025).
- Kafayat Aminu, Timothy Olukunle Aladelusi, Akinyele Olumuyiwa Adisa, Chiamaka Norah Ezeagu, Afeez Abolarinwa Salami, Jacob Njideka Nwafor, Peace Uwambaye, Jimoh Amzat, Julienne Murererehe, Semeeh Akinwale Omoleke, Mohammed Abdulaziz, Ruwan Duminda Jayasinghe, Kehinde Kazeem Kanmodi, Epidemiology, literacy, risk factors, and clinical status of oral cancer in East Africa: A scoping review, PLOS ONE, 10.1371/journal.pone.0317217, 20, 2, (e0317217), (2025).
- Omar A. Al-Karadsheh, Siraj J. Zabadi, Mahdi F. Waleed, Khadijeh A. Al-Abedalla, Najla S. Kasabreh, Ahmad A. Hamdan, Yazan M. Hassona, Dimitris N. Tatakis, Diagnostic delays of periodontitis and associated factors: a cross-sectional study, Clinical Oral Investigations, 10.1007/s00784-024-06075-6, 28, 12, (2024).
- Kehinde Kazeem Kanmodi, Afeez Abolarinwa Salami, Kamini Shah, Fatemeh Vida Zohoori, Lawrence Achilles Nnyanzi, The Types and Effectiveness of Mobile Health Applications Used in Improving Oral Cancer Knowledge: A Mixed Methods Systematic Review, Health Science Reports, 10.1002/hsr2.70171, 7, 11, (2024).
- Ayesha Irfan, Ayesha Fahim, Varda Jalil, Nasar Um Min Allah, Abeer Anjum, Remsha Mustafa, Habib Ahmad Qureshi, Fahim Haider Jafari, Muhammad Amber Fareed, Muhammad Sohail Zafar, Relationship of microvascular density and tumor-associated macrophages with orofacial squamous cell carcinoma progression, Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology, 10.1016/j.oooo.2024.06.013, 138, 4, (532-542), (2024).
- Yibing Tan, Xinglan Sun, Fengyin Qin, Yefeng Cai, Factors affecting stroke pre-hospital delay behavioral intention among community residents: A path analysis, Applied Nursing Research, 10.1016/j.apnr.2024.151820, 78, (151820), (2024).
- See more