Second-line rituximab–bendamustine versus rituximab–gemcitabine–oxaliplatin in diffuse large B-cell lymphoma in the real world
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Despite long-term responses to first-line immunochemotherapy, many patients with diffuse large B-cell lymphoma (DLBCL) have relapsed/refractory disease. Second-line treatment options are available. However, a large proportion of patients are ineligible for transplantation/intensive therapy. Patients & methods: This observational study of 702 patients in the USA, who used second-line therapies for relapsed/refractory DLBCL, evaluated treatment patterns and overall survival (OS). The study focused on the OS outcome of patients receiving second-line rituximab–bendamustine or rituximab–gemcitabine–oxaliplatin. Results & conclusion: Rituximab–bendamustine and rituximab–gemcitabine–oxaliplatin were received by 4.6 and 1.4% of patients, respectively (N = 42/702). Median and 1-year OS rates were similar between regimens. Many of the 200 different treatment regimens observed in second line were modified versions of National Comprehensive Cancer Network regimens.
Diffuse large B-cell lymphoma (DLBCL) is the most common subtype of non-Hodgkin lymphoma (NHL), representing 30−58% of all cases [1,2]. DLBCL is an aggressive form of NHL. Patients have a poor prognosis, and without treatment will typically die within weeks or months of diagnosis [3]. Rituximab, an anti-CD20 monoclonal antibody, has proven efficacy and a tolerable safety profile in CD20-positive DLBCL [4]. In combination with other drugs, rituximab has been approved as first-line standard of care for several types of NHL [5,6]. In particular, R-CHOP (rituximab plus cyclophosphamide, doxorubicin, vincristine and prednisone) is the current standard of care for previously untreated DLBCL, both in Europe [5] and in the USA [6]. Although 60% of patients treated with R-CHOP achieve long-term responses, approximately 20–25% of patients will eventually relapse or 10–15% will exhibit refractory disease within the first 2–3 years following immunochemotherapy [7]. Life expectancy is reduced in patients with previously treated relapsed/refractory DLBCL, and most patients die within 2 years [7].
Current treatment options for relapsed/refractory DLBCL are limited and present a therapeutic challenge, as tumors can exploit multiple escape mechanisms to evade the immune system [8,9]; a more personalized treatment strategy is thus required. Although high-dose chemotherapy followed by autologous stem-cell transplantation (ASCT) is the standard of care for chemosensitive patients aged <70 years with relapsed/refractory DLBCL [5], only around half of patients are eligible for this treatment approach [10]. Currently, there is no standard of care for patients with relapsed/refractory DLBCL who are ineligible for ASCT; however, a broad spectrum of therapeutic options are available [5,6]. There are few data on the patterns of second-line therapies currently used in routine clinical practice in patients with relapsed/refractory DLBCL. The real-world outcomes associated with these second-line treatments are also not clear, particularly for patients not suitable for ASCT and intensive therapy.
Rituximab–bendamustine (R–benda) and rituximab–gemcitabine–oxaliplatin (R–GemOx) are two regimens with proven efficacy and safety for patients not eligible for ASCT [11,12]. R–benda and R–GemOx can usually be administered easily as an outpatient [13,14]; data regarding real-world outcomes using these regimens are limited.
This retrospective, real-world observational study, set in the USA, aimed to evaluate treatment patterns, as well as overall survival (OS), in patients with DLBCL who received second-line R–benda or second-line R–GemOx.
Patients & methods
Data source & study sample
Electronic medical records and the raw oncology domain dataset were extracted from the US Veterans Health Administration database.
Inclusion criteria
Patients (veterans) with a diagnosis of NHL were initially identified from the database. This group was further screened to include only those with an indicator for complete chart extraction in the raw oncology domain and with at least 1 month of follow-up time. The final sample included patients diagnosed with DLBCL between 2004 and 2016 who received both first- and second-line therapy. Patients who initiated second-line therapy were assumed to have relapsed/refractory DLBCL (i.e., either progressed following first-line therapy [relapsed] or did not respond to first-line therapy [refractory]). Of this sample, survival outcomes were analyzed in patients receiving R–benda or R–GemOx.
Exclusion criteria
Patients with T-cell/histiocyte-rich large B-cell lymphoma, plasmablastic lymphoma, large B-cell (plasmablastic) lymphoma arising from human herpesvirus 8-associated multicentric Castleman disease or primary effusion lymphoma were excluded. Patients with other malignancies prior to first DLBCL diagnosis were also excluded.
This study was conducted in accordance with the Declaration of Helsinki, Good Clinical Practice guidelines and all applicable local laws and regulations. The study protocol and its amendments, and other study-related materials, were approved by institutional review boards/ethics committees. The institutional review board granted a waiver of informed consent for this database study.
Measurement of second-line therapy
Lines of therapy were identified from the start/end dates of agents, based on an algorithm adapted from previously published algorithms [15,16]. Lines of therapy were measured from the initial DLBCL diagnosis and not from the diagnosis of relapsed/refractory disease. Initiation of second-line therapy corresponded to the initiation date of a drug not included in first-line, or reinitiation of first-line agent(s) after a gap of >120 days. The second-line regimen was defined as those agents used in the 42 days after second-line therapy was initiated.
Data analysis
Patient characteristics, median OS and 1-year OS, were compared between patients with DLBCL who received second-line R–benda or second-line R–GemOx. The OS from the initiation of second-line therapy was calculated using Kaplan–Meier methodology and univariate/multivariate Cox regression. Surviving patients were censored at the data cut-off date (31 December 2017). A multivariate Cox regression model was adjusted for risk factors that were selected based on results of univariate models and clinical significance, including patient age, cancer stage, first-line regimen, abnormal LDH or hemoglobin 6 months before second-line treatment initiation.
Results
Overall study sample characteristics
Of 2600 patients with DLBCL identified that satisfied the study inclusion criteria, 702 received second-line therapy and were included in the final analysis (Figure 1). A total of 12 regimens were used by ≥10 patients per regimen, which included 345/702 (49%) of the patient population (Table 1). The remaining 188 regimens were used by <10 patients/regimen (357/702 [51%]; Table 1). All National Comprehensive Cancer Network (NCCN)-recommended regimens [6] were among the 12 commonly used (≥10 patients/regimen) regimens. Of these 12 regimens, rituximab plus ifosfamide, carboplatin and etoposide (R-ICE) (77/702 [11.0%]) and R-CHOP (75/702 [10.7%]) were the most commonly used. Many of the less common regimens were modified versions of the recommended regimens.
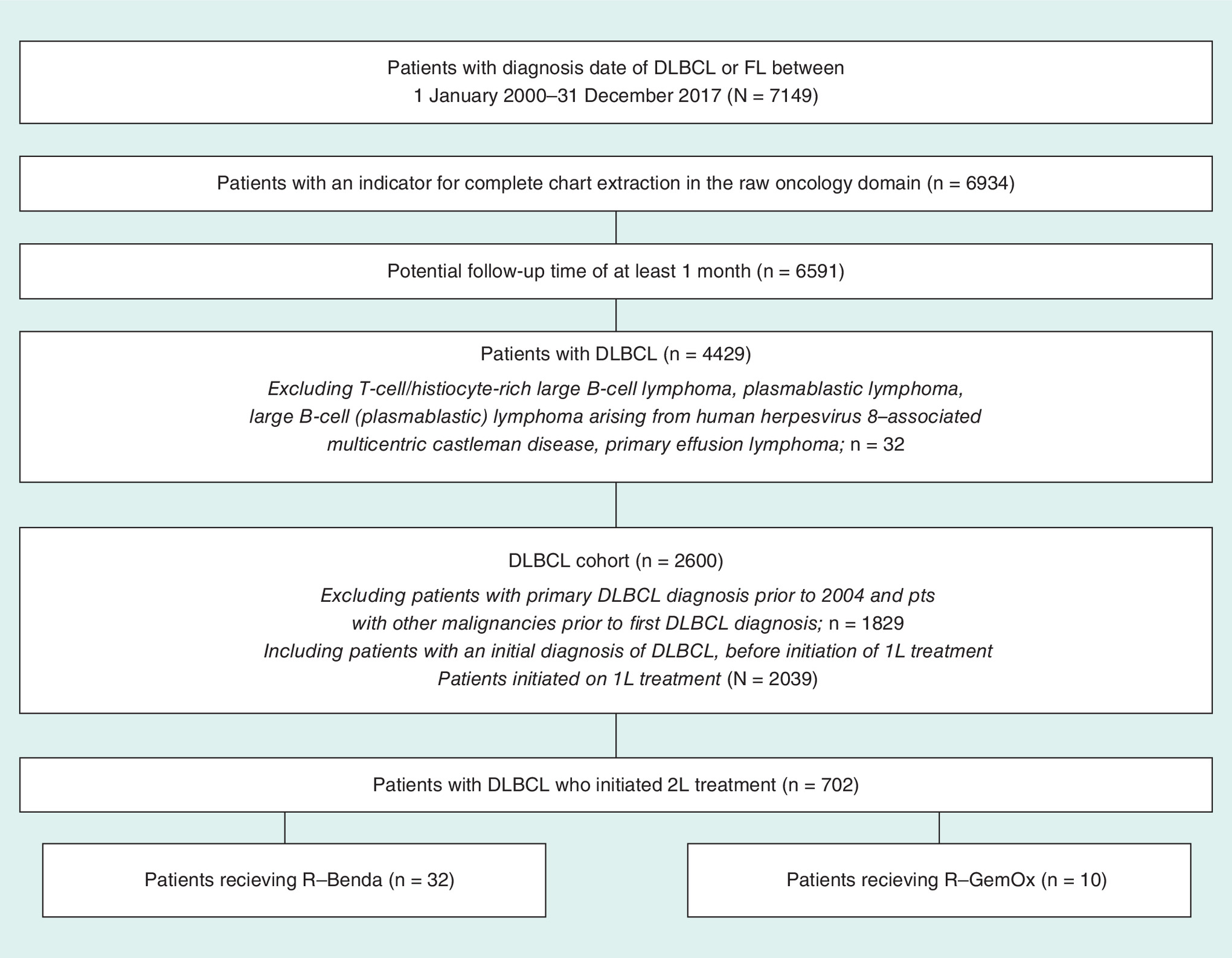
Figure 1. Patient flow.
2L: Second line; DLBCL: Diffuse large B-cell lymphoma; FL: Follicular lymphoma.
| Total N = 702 | |
|---|---|
| Treatment regimens used in ≥10 patients ( ± maintenance) | n (%) |
| – R-ICE | 77 (11.0) |
| – R-CHOP | 75 (10.7) |
| – Rituximab | 34 (4.8) |
| – R–benda | 32 (4.6) |
| – Methotrexate | 24 (3.4) |
| – R-ESHAP | 23 (3.3) |
| – R-DHAP/R-EPOCH/R-GDP | 18 (2.6) |
| – Cyclophosphamide + doxorubicin + rituximab + vinblastine + vincristine | 15 (2.1) |
| – R-CVP | 14 (2.0) |
| – Cyclophosphamide + etoposide + rituximab + vincristine | 13 (1.9) |
| – R–GemOx | 10 (1.4) |
| – Carmustine + cyclophosphamide + etoposide | 10 (1.4) |
| Other treatment regimens (<10 patients/regimen) | n (%) |
| – All NCCN guideline-recommended agents | 262 (37.3) |
| – Not all NCCN guideline-recommended agents | 95 (13.5) |
NCCN: National Comprehensive Cancer Network; R–benda: Rituximab + bendamustine; R-CHOP: Rituximab + cyclophosphamide + doxorubicin + vincristine + prednisone; R-CVP: Rituximab + cyclophosphamide + vincristine + prednisone; R-DHAP: Rituximab + dexamethasone + high-dose cytarabine + cisplatin; R-EPOCH: Rituximab + etoposide phosphate + prednisone + vincristine + cyclophosphamide + doxorubicin; R-ESHAP: Rituximab + etoposide + cytarabine + cisplatin + methylprednisolone; R-GDP: Rituximab + gemcitabine + dexamethasone + cisplatin; R–GemOx: Rituximab + gemcitabine + oxaliplatin; R-ICE: Rituximab + ifosfamide + carboplatin + etoposide.
Patients receiving second-line R–benda or R–GemOx
A total of 32/702 patients (4.6%) received R–benda and 10/702 patients (1.4%) received R–GemOx. Analysis of baseline characteristics identified numerical imbalances between R–benda and R–GemOx cohorts in terms of race, number of involved lymph nodes, B symptoms, Charlson Comorbidity Index score and abnormal lactate dehydrogenase results (Table 2). Median follow-up time after second-line treatment initiation was 11.3 months in the R–benda cohort and 11.7 months in the R–GemOx cohort, with median OS durations of 11 and 13 months, respectively (Figure 2). One-year OS rates were 50.0% (95% CI: 31.9–65.7%) with R–benda and 60.0% (95% CI: 25.3–82.7%) with R–GemOx. In univariate and multivariate analyses, administration of R-CHOP as first-line therapy versus other regimens was the only covariate with a significant effect on OS (Table 3). Treatment with R–GemOx or R–benda did not significantly affect OS (hazard ratio [HR]: 0.89; 95% CI: 0.38–2.08; p = 0.79; and HR: 0.68; 95% CI: 0.27–1.73; p = 0.42, respectively).
| Characteristic | Second-line R–benda (n = 32) | Second-line R–GemOx (n = 10) | p-value† |
|---|---|---|---|
| Age, years: | |||
| – Mean ± SD | 65 ± 10 | 66 ± 6 | 0.59 |
| – Median (IQR) | 63 (60–69) | 64 (62–70) | – |
| Male, n (%) | 31 (96.9) | 10 (100.0) | 1.00 |
| Caucasian/White, n (%) | 25 (78.1) | 6 (60.0) | 0.41 |
| Refractory DLBCL‡, n (%) | 13 (40.6) | 4 (40.0) | 1.00 |
| Number of lymph nodes involved, n (%): | |||
| – 0 | 21 (65.6) | 5 (50.0) | 0.47 |
| – ≥1 | 10 (31.3) | 2 (20.0) | 0.70 |
| – Unknown/missing | 1 (3.1) | 3 (30.0) | 0.04 |
| Stage, n (%): | |||
| – I | 1 (3.1) | 1 (10.0) | 0.42 |
| – II | 5 (15.6) | 1 (10.0) | 1.00 |
| – III | 8 (25.0) | 2 (20.0) | 1.00 |
| – IV | 14 (43.8) | 4 (40.0) | 1.00 |
| – Unknown/missing | 4 (12.5) | 2 (20.0) | 0.62 |
| B symptoms, n (%): | |||
| – No | 19 (59.4) | 4 (40.0) | 0.47 |
| – Yes | 12 (37.5) | 3 (30.0) | 1.00 |
| – Unknown/missing | 1 (3.1) | 3 (30.0) | 0.04 |
| Charlson comorbidity index score: | |||
| – Mean ± SD | 3.9 ± 2.2 | 3.2 ± 1.9 | 0.37 |
| – Median (IQR) | 3 (2–6) | 2 (2–4) | |
| Patients with LDH test§, n (%): | 19 (59.4) | 4 (40.0) | 0.47 |
| – ≥1 abnormal result | 15 (46.9) | 3 (30.0) | 0.47 |
| Patients with hemoglobin test§, n (%): | 32 (100.0) | 8 (80.0) | 0.05 |
| – ≥1 abnormal result | 26 (81.3) | 5 (50.0) | 0.09 |
| First-line regimen R-CHOP, n (%) | 18 (56.3) | 6 (60.0) | 1.00 |
†
Statistical comparisons were conducted with Wilcoxon rank-sum tests for the continuous variables and Chi-square tests for the categorical variables.
‡
Refractory DLBCL was defined as <180 days between first-line end and second-line start.
§
In the baseline period.
DLBCL: Diffuse large B-cell lymphoma; IQR: Interquartile range; R–benda: Rituximab–bendamustine; R–GemOx: Rituximab–gemcitabine–oxaliplatin; SD: Standard deviation.

Figure 2. Overall survival from initiation of second-line therapy with rituximab–bendamustine or rituximab–gemcitabine–oxaliplatin in patients with diffuse large B-cell lymphoma.
OS: Overall survival; R–benda: Rituximab–bendamustine; R–GemOx: Rituximab–gemcitabine–oxaliplatin.
| Univariate Cox regression models | Multivariate Cox regression model† | |||
|---|---|---|---|---|
| HR (95% CI) | p-value | HR (95% CI) | p-value | |
| R–GemOx vs R–benda | 0.89 (0.38–2.08) | 0.79 | 0.68 (0.27–1.73) | 0.42 |
| Age (per year increase) | 1.04 (0.99–1.09) | 0.09 | 1.03 (0.98–1.08) | 0.28 |
| Refractory DLBCL (vs relapsed DLBCL)‡ | 1.02 (0.50–2.10) | 0.95 | – | – |
| With ≥1 lymph nodes involved (vs 0 nodes) | 0.85 (0.37–1.94) | 0.70 | – | – |
| Cancer stage IV (vs stage I–III) | 0.66 (0.31–1.39) | 0.27 | 0.65 (0.26–1.65) | 0.37 |
| Charlson comorbidity index (per point increase) | 1.01 (0.86–1.19) | 0.90 | – | – |
| Abnormal LDH§ (vs normal LDH) | 1.51 (0.74–3.09) | 0.26 | 1.74 (0.80–3.77) | 0.16 |
| Abnormal hemoglobin§ (vs normal hemoglobin) | 1.82 (0.76–4.36) | 0.18 | 1.73 (0.68–4.41) | 0.25 |
| First-line regimen R-CHOP (vs others) | 2.20 (1.00–4.84) | 0.05¶ | 2.49 (1.11–5.62) | 0.03¶ |
†
Model included all shown covariates (selected based on results of univariate models and clinical significance). Sex was not included among the potential predictors because 41/42 patients were male.
‡
Refractory DLBCL was defined as <180 days between first-line end and second-line start, and relapsed DLBCL was defined as ≥180 days between first-line end and second-line start.
§
Patients for whom a test was not ordered were assumed to have normal test results.
¶
Significant p-value.
DLBCL: Diffuse large B-cell lymphoma; HR: Hazard ratio; R–benda: Rituximab–bendamustine; R-CHOP: Rituximab plus cyclophosphamide, doxorubicin, vincristine and prednisone; R–GemOx: Rituximab–gemcitabine–oxaliplatin.
Discussion
Currently, there is no standard of care for patients with relapsed/refractory DLBCL who are ineligible for transplant. This study examined the use of second-line therapies for relapsed/refractory DLBCL in real-world clinical practice in the USA. A wide range of treatment (200 distinct therapy regimens) had been used in the 702 patients included in the analysis. Of the 12 regimens used in ≥10 patients, 11 were recommended by NCCN guidelines [6]. Second-line R-CHOP is not recommended in the NCCN guidelines. Despite this, we observed a high number of patients who were treated with second-line R-CHOP and modified regimens of R-CHOP that are outside of NCCN guidelines in the second-line setting. Alternatively, in the cases where first-line R-CHOP was not used, these patients may have received second-line R-CHOP. Many patients did not receive first-line R-CHOP; however, a small number of patients were rechallenged with second-line R-CHOP after progressing on first-line R-CHOP. Furthermore, these analyses include patients dating back to the year 2004, when fewer agents were available. In many cases, if patients experienced a good response to first-line R-CHOP, with a long duration of remission, they may have been challenged a second time with R-CHOP.
From the broad range of treatment regimens used in this patient cohort, we chose to focus on R–benda and R–GemOx as they are typically used in patients ineligible for ASCT, there have been no previous randomized, controlled trials of patients with relapsed/refractory DLBCL comparing these two regimens [11,12], and they can be administered in an outpatient setting [13,14]. R–benda has been studied previously in a prospective Phase II trial in patients with relapsed/refractory DLBCL who were considered ineligible for intensive salvage therapies [11,17]. While R–benda was an active combination in this setting, median OS was not reached because of the high number of censored data due to withdrawals from the study [17]. In a similar study [11], comparable efficacy with R–benda was demonstrated; however, OS was not reported. In the current analysis, median OS was 11 months with R–benda. A previous study of R–GemOx in patients with relapsed/refractory DLBCL showed a 5-year OS of 14% and a median OS of 11 months [12], which is comparable with the median OS of 13 months in the current analysis. Also in the current study, no statistical difference was found in 1-year OS or median OS between patients treated with second-line R–benda and second-line R–GemOx. Median OS was reached approximately 1 year after initiation of second-line therapy with both regimens.
Patients, who are either refractory or have received multiple lines of therapy, typically have a very poor prognosis. In this study, the proportion of patients with refractory disease was 40% for both treatment cohorts, which is consistent with that expected in the general DLBCL population that relapses after front-line therapy [7]. When comparing these real-world outcomes with interventional studies in this setting, it is important to note that the proportion of patients with refractory disease and the lines of therapy have a significant impact on expected outcomes. The current study specifically examined patients who received second-line therapy in the first relapse or refractory setting. Other clinical studies in this area typically have broader entry criteria; multiple prior lines of therapy are permitted and studies include variable proportions of primary, refractory patients. Therefore, outcomes may not be directly comparable. For example, response to therapies may differ depending on the proportion of primary refractory patients studied. Our data illustrate the vast range of second-line regimens currently used when patients relapse. Of the two regimens of interest, R–benda and R–GemOx, there appear to be no differences in OS. Together, these data highlight that there is still more to be done in this setting to achieve long-term remission for those patients ineligible for transplant in the first relapse setting.
The Scholar-1 study of pooled data, from two large randomized trials and two academic databases, provided seminal data on outcomes for patients with refractory DLBCL [18]. A median OS of 6.3 months was reported and outcomes were poor across patient subgroups and study cohorts. However, these data are not directly comparable with the current study as the populations examined and the eligibility criteria were different. Scholar-1 included patients who were refractory to second-line or later-line therapy or relapsed ≤12 months after ASCT, while the current study examined patients in the real-world setting who received second-line therapies.
The current study has several limitations. For example, of the 702 patients eligible for inclusion, only 32 were treated with R–benda and 10 with R–GemOx; the study may, therefore, be underpowered to detect small differences between the cohorts. There is also potential for overfitting the multivariate regression model. However, the multivariate analysis does provide insight into the potential modifying factors. An electronic medical record-based algorithm was used to identify lines of therapy and regimens; consequently, these data may not be as accurate as data collected from a clinical trial. Prognostic factors were selected a priori and were restricted to the variables available in the US Veterans Affairs database. International Prognostic Index, Follicular Lymphoma International Prognostic Index and International Prognostic Score were considered, but were not included due to high proportion of missing data (62.7, 96.0 and 95.6%, respectively). Eligibility criteria for ASCT are based on several clinical criteria and physician assessments that were not available in the Veterans Affairs database. Finally, the Veterans Affairs data includes mostly male veterans.
Overall the findings of this study reveal poor outcomes for patients with relapsed/refractory DLBCL treated with R–benda and R–GemOx. However, newer therapies such as chimeric antigen receptor T-cell therapies have shown promising outcomes in relapsed/refractory DLBCL as third-line or later therapies [19], providing hope for patients with this condition. The chimeric antigen receptor T-cell therapy, tisagenlecleucel, was approved for DLBCL in August 2017 and not available during the study period [20]. Polatuzumab vedotin in combination with bendamustine and a rituximab product is also now approved by the US FDA for adults with relapsed/refractory DLBCL after at least two prior therapies [21].
Conclusion
This real-world study showed heterogeneity in second-line therapy for DLBCL and highlights an unmet need for the treatment of relapsed/refractory DLBCL. Wide varieties of treatments are being administered as second-line treatment regimens in DLBCL, some of which are not recommended by NCCN. In this real-world analysis, a similar OS was observed in the two second-line treatment regimens studied, R–benda and R–GemOx. Further research using alternative sources of real-world data is warranted to determine whether these findings are reflected more widely.
•
There are few data on second treatment patterns for patients with relapsed/refractory diffuse large B-cell lymphoma (DLBCL) currently used in routine clinical practice.
•
We carried out a retrospective, real-world observational study, set in the USA, evaluating treatment patterns and overall survival (OS) in patients diagnosed with DLBCL between 2004 and 2016 who received second-line rituximab–bendamustine (R–benda) or second-line Rituximab–gemcitabine–oxaliplatin (R–GemOx).
•
A wide range of second-line treatment regimens (200 distinct therapy regimens) had been used in the 702 anonymized patients included in the analysis: 11 of the 12 regimens used by ≥10 patients/regimen were recommended by National Comprehensive Cancer Network guidelines (345/702 [49%]).
•
R-ICE (rituximab plus ifosfamide, carboplatin and etoposide; 77 [11.0%]) and R-CHOP (rituximab plus cyclophosphamide, doxorubicin, vincristine and prednisone; 75 [10.7%]) were the most commonly used regimens; 4.6% of patients received R–benda; 1.4% of patients received R–GemOx.
•
There was no statistical difference in 1-year OS rates (R–benda: 50.0% [95% CI: 31.9–65.7%]; R–GemOx: 60.0% [95% CI: 25.3–82.7%]) or median OS (R–benda: 11 months; R–GemOx: 13 months) between patients treated with second-line R–benda and second-line R–GemOx.
•
No statistical difference was found in OS with second-line R–GemOx compared with second-line R–benda in the univariate analysis (hazard ratio: 0.89; 95% CI: 0.38–2.08; p = 0.785) nor the multivariate analysis (hazard ratio: 0.68; 95% CI: 0.27–1.73; p = 0.424).
•
This real-world study highlights that a wide variety of treatments are being administered as second-line treatment regimens in DLBCL, some of which may not be recommended by National Comprehensive Cancer Network.
Financial & competing interests disclosure
This work was funded by F Hoffman-La Roche Ltd. R Ionescu-Ittu, A Guerin and S Shi are employees of Analysis Group and consultants to F Hoffman-La Roche Ltd. A Shang is an employee of F Hoffmann-La Roche Ltd. A Shang has ownership interests non-PLC in F Hoffman-La Roche Ltd. L Shi is a consultant to Intuitive Surgical, has ownership interests non-PLC in Bravo4Health and has received research funding from F Hoffmann-La Roche Ltd, Genentech Inc. and Chiasma. N Vander Velde and Y Lin declare no conflicts of interest. N Qayum was an employee of F Hoffmann-La Roche Ltd at the time of the study. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Third-party medical writing assistance under the direction of Raluca Ionescu-Ittu and Aijing Shang was provided by Rachel Hubbard, MSc and Russell Craddock, PhD MSc, of Gardiner–Caldwell Communications and was funded by F Hoffmann-La Roche Ltd.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. The institutional review board granted a waiver of informed consent for this database study.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest
1.
Swerdlow SH, Campo E, Harris NL (Eds). WHO Classification of Tumours. Vol. 2. WHO, Geneva, Switzerland, 223–237 (2014).
2.
Jaffe ES, Swerdlow SH, Vardiman JW. Chapter 5.13. Haematopoietic and Lymphoid Malignancies. In: WHO Classification of Tumours. Stewart BW, Wild CP (Eds). World Cancer Report 2014, Lyon, France (2014).
3.
Cultrera JL, Dahlia SM. Diffuse large B-cell lymphoma: current strategies and future directions. Cancer Control 19(3), 204–213 (2012).
• Reviews the current treatment protocols for diffuse large B-cell lymphoma (DLBCL) and the ongoing research focused on molecular diagnostics and prognostic factors, which aim to personalize treatment strategies.
4.
Casan JML, Wong J, Northcott MJ, Opat S. Anti-CD20 monoclonal antibodies: reviewing a revolution. Hum. Vaccin. Immunother. 14, 2820–2841 (2018).
5.
Tilly H, Gomes da Silva M, Vitolo U et al. ESMO Guidelines Committee. Diffuse large B-cell lymphoma (DLBCL): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 26(Suppl. 5), v116–v125 (2015).
6.
National Comprehensive Cancer Network. NCCN Guides for B-Cell Lymphomas. Version 1 (2019). www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf
7.
Sehn LH, Gascoyne RD. Diffuse large B-cell lymphoma: optimizing outcome in the context of clinical and biologic heterogeneity. Blood 125(1), 22–32 (2015).
• Highlights the importance of optimization of front-line therapy, as well as the development of more effective salvage strategies in patients with relapsed/refractory DLBCL.
8.
Kiyasu J, Miyoshi H, Hirata A et al. Expression of programmed cell death ligand 1 is associated with poor overall survival in patients with diffuse large B-cell lymphoma. Blood 126(19), 2193–2201 (2015).
9.
Georgiou K, Chen L, Berglund M et al. Genetic basis of PD-L1 overexpression in diffuse large B-cell lymphomas. Blood 127(24), 3026–3034 (2016).
10.
Sarkozy C, Sehn LH. Management of relapsed/refractory DLBCL. Best Pract. Res. Clin. Haematol. 31(3), 209–216 (2018).
• Reviews the incidence, outcome and management of relapsed and refractory DLBCL and examines novel agents in development.
11.
Ohmachi K, Niitsu N, Uchida T et al. Multicenter Phase II study of bendamustine plus rituximab in patients with relapsed or refractory diffuse large B-cell lymphoma. J. Clin. Oncol. 31(17), 2103–2109 (2013).
12.
Mounier N, El Gnaoui T, Tilly H et al. Rituximab plus gemcitabine and oxaliplatin in patients with refractory/relapsed diffuse large B-cell lymphoma who are not candidates for high-dose therapy. A Phase II Lymphoma Study Association trial. Haematologica 98(11), 1726–1731 (2013).
• This Phase II study examined the use of rituximab, gemcitabine and oxaliplatin in patients with refractory/relapsed B-cell lymphoma. An overall response rate of 61% was observed.
13.
El Gnaoui T, Tilly H, Mounier N et al. Rituximab plus gemcitabine and oxaliplatine (R–GemOx) in refractory/relapsed patients with diffuse large B-cell lymphoma (DLBCL) who are not candidates for high-dose therapy (HDT): a GELA study. J. Clin. Oncol. 28(15 Suppl.), 8011 (2010).
14.
Kleeberg UR, Linde H, Günther G, Tessen HW, Kersting M. Bendamustin–rituximab combination is a safe and effective, ambulatory treatment for elderly patients with chronic lymphocytic leukemia: retrospective real-world analysis by age from a German registry and review of the literature. Anticancer Res. 36(6), 2827–2838 (2016).
15.
Ramsey SD, Willke RJ, Glick H et al. Cost–effectiveness analysis alongside clinical trials II-An ISPOR Good Research Practices Task Force report. Value Health 18(2), 161–172 (2015).
16.
Seal BS, Sullivan SD, Ramsey S et al. Medical costs associated with use of systemic therapy in adults with colorectal cancer. J. Manag. Care Pharm. 19(6), 461–467 (2013).
• Aims to identify factors associated with higher total healthcare expenditures in patients with colorectal cancer receiving systemic therapy (biologic or chemotherapy). The study showed that healthcare costs are increasing considerably over time.
17.
Vacirca JL, Acs PI, Tabbara IA, Rosen PJ, Lee P, Lynam E. Bendamustine combined with rituximab for patients with relapsed or refractory diffuse large B cell lymphoma. Ann. Hematol. 93(3), 403–409 (2014).
• Examines the combination of bendamustine and rituximab in patients with relapsed and refractory DLBCL. The overall response rate was 45.8% (complete response, 15.3%; partial response, 30.5%).
18.
Crump M, Neelapu SS, Farooq U et al. Outcomes in refractory diffuse large B-cell lymphoma: results from the international SCHOLAR-1 study. Blood 130(16), 1800–1808 (2017).
19.
Neelapu SS, Locke FL, Bartlett NL et al. Axicabtagene ciloleucel CAR T-cell therapy in refractory large B-cell lymphoma. New Engl. J. Med. 377, 2531–2544 (2017).
20.
KYMRIAH (tisagenlecleucel) (2019). www.fda.gov/vaccines-blood-biologics/cellular-gene-therapy-products/kymriah-tisagenlecleucel
21.
POLIVY (polatuzumab vedotin) Highlights of prescribing information (2019). www.accessdata.fda.gov/drugsatfda_docs/label/2019/761121s000lbl.pdf
Information & Authors
Information
Published In
Pages: 1067 - 1075
PubMed: 31452397
Copyright
© 2019 Ionescu-Ittu et al. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 22 May 2019
Accepted: 1 August 2019
Published online: 27 August 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Second-line rituximab–bendamustine versus rituximab–gemcitabine–oxaliplatin in diffuse large B-cell lymphoma in the real world. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0062
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Lixia Ma, Yimeng Dou, Rui Liu, Teng Xu, Fan Yang, Peihao Zheng, Shaomei Feng, Yuelu Guo, Hui Shi, Fei Xue, Biping Deng, Xiaoyan Ke, Kai Hu, Efficacy and Safety of CART Cell Therapy in Aggressive B‐Cell Lymphomas Involving the Gastrointestinal Tract , Cancer Reports, 10.1002/cnr2.70083, 8, 1, (2025).
- Melina Sophie Kurte, Ann‐Cathrine Siefen, Florian Jakobs, Bastian von Tresckow, Hans Christian Reinhardt, Florian Kron, Cost‐effectiveness analysis of transplant‐ineligible relapsed or refractory diffuse large B‐cell lymphoma treatment options—Experience of the efficiency frontier approach, European Journal of Haematology, 10.1111/ejh.14095, 111, 6, (895-908), (2023).
- Ewa Paszkiewicz‐Kozik, Wojciech Michalski, Michał Taszner, Monika Mordak‐Domagała, Joanna Romejko‐Jarosińska, Wanda Knopińska‐Posłuszny, Jacek Najda, Anna Borawska, Monika Chełstowska, Monika Świerkowska, Anna Dąbrowska‐Iwanicka, Agata Malenda, Agnieszka Druzd‐Sitek, Robert Konecki, Beata Kumiega, Michał Osowiecki, Beata Ostrowska, Tomasz Szpila, Marcin Szymański, Łukasz Targoński, Katarzyna Domańska‐Czyż, Lidia Popławska, Sebastian Giebel, Andrzej Lange, Andrzej Pluta, Jan Maciej Zaucha, Grzegorz Rymkiewicz, Jan Walewski, Ofatumumab with iphosphamide, etoposide and cytarabine for patients with transplantation‐ineligible relapsed and refractory diffuse large B‐cell lymphoma, British Journal of Haematology, 10.1111/bjh.18166, 198, 1, (73-81), (2022).
- Samuli Tuominen, Kristiina Uusi-Rauva, Tea Blom, Sirkku Jyrkkiö, Kaisa Tuppurainen, Erika Alanne, Real-world Data on Diffuse Large B-Cell Lymphoma in 2010–2019: Usability of Large Data Sets of Finnish Hospital Data Lakes, Future Oncology, 10.2217/fon-2021-0806, 18, 9, (1103-1114), (2022).
- Zeyuan Wang, Xianting Ran, Siyu Qian, Huting Hou, Meng Dong, Shaoxuan Wu, Mengjie Ding, Yue Zhang, Xudong Zhang, Mingzhi Zhang, Qingjiang Chen, GPNMB promotes the progression of diffuse large B cell lymphoma via YAP1-mediated activation of the Wnt/β-catenin signaling pathway, Archives of Biochemistry and Biophysics, 10.1016/j.abb.2021.108998, 710, (108998), (2021).
- Marguerite Briand, Stephane Gerard, Martin Gauthier, Marie Garric, Zara Steinmeyer, Laurent Balardy, Impact of therapeutic management and geriatric evaluation on patient of eighty years and older with diffuse large B‐cell lymphoma on survival: A systematic review, European Journal of Haematology, 10.1111/ejh.13704, 108, 1, (3-17), (2021).
- Gena Kanas, Wenzhen Ge, Ruben G. W. Quek, Katie Keeven, Knar Nersesyan, undefined Jon E. Arnason, Epidemiology of diffuse large B-cell lymphoma (DLBCL) and follicular lymphoma (FL) in the United States and Western Europe: population-level projections for 2020–2025, Leukemia & Lymphoma, 10.1080/10428194.2021.1975188, 63, 1, (54-63), (2021).
- Leonard Jeff Harris, Kruti Patel, Michael Martin, Novel Therapies for Relapsed or Refractory Diffuse Large B-Cell Lymphoma, International Journal of Molecular Sciences, 10.3390/ijms21228553, 21, 22, (8553), (2020).
- Hsu-Chih Chien, Deborah Morreall, Vikas Patil, Kelli M Rasmussen, Chunyang Li, Christina M Yong, Zachary Burningham, Anthony Masaquel, Mary Halloran, Elisha De Long-Sieg, Mathias Schulz, Brian C Sauer, Ahmad S Halwani, Real-World Practice Patterns and Outcomes in Veterans with Relapsed/Refractory Diffuse Large B-Cell Lymphoma, Future Oncology, 10.2217/fon-2020-0522, 17, 4, (411-422), (2020).
- Emily C. Ayers, David Margolis, Daniel J. Landsburg, Real World Outcomes in Patients With Relapsed/Refractory Diffuse Large B-cell Lymphoma Receiving Palliative Intent Therapies, Clinical Lymphoma Myeloma and Leukemia, 10.1016/j.clml.2020.05.008, 20, 10, (661-667), (2020).