Positive deviance approaches to improving vaccination coverage rates within healthcare systems: a systematic review
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Our objective was to systematically review the use of the positive deviance approach to identify strategies to improve vaccination coverage rates. Materials & methods: We searched English language articles in Medline, Embase, Cochrane Library, CINAHL and PsycINFO without any date restrictions on 4 October 2017. We compiled a list of all strategies and evaluated the quality of these studies using the QATSDD tool. Results: After a review of 241 citations, we included eight studies. These studies focused on a wide variety of vaccines and settings. Core strategies that support vaccine uptake include the importance of tailoring and targeting in both messaging and delivery of vaccines and tracking delivery of vaccines. Patient and provider education, reminders, feedback loops, community collaborations, immunization registries and use of a medical home were also identified as other strategies. Conclusion: Our findings highlight several useful core strategies, which can be used to promote vaccination coverage. PROSPERO: CRD42017078221.
Vaccination is one of the most effective strategies which is known to decrease rates of morbidity and mortality. Despite the availability of many effective vaccines with low rates of adverse effects, the rates of vaccination have not met their national or international targets for some vaccines [1]. Randomized clinical trials have provided evidence of the efficacy of selected strategies in specific settings, but practical, efficient strategies that are effective in diverse, complex settings, are difficult to identify. Positive deviance studies provide insight into strategies that have been used with success in real-world settings, and thus may offer one approach to improve rates of vaccination.
The positive deviance approach is based on the principle that there are individuals (or organizations), who consistently demonstrate a high level of performance compared with their peers [2–4]. These high performers, who face the same constraints as their peers, may possess knowledge and strategies that can help others improve. The steps in the positive deviance approach include: identification of ‘positive deviants’ or high performers, in-depth study of high performers using qualitative methods to generate testable hypothesis about supporting and enabling strategies that allow them to succeed, and testing these hypotheses in a larger representative sample [2]. Some conceptualizations include a fourth stage, in other words, dissemination [3]. Positive deviance has been successfully applied to address diverse problems including reducing childhood malnutrition [5] and improving care after myocardial infarction [6]. Although a systematic review found an increase in the number of positive deviance studies in healthcare in recent years [2], very few studies focused on vaccination. Our objective was to systematically review the application of the positive deviance approach to identifying strategies to improve vaccination coverage rates. We aimed to describe the stages of the positive deviance approach used, determine what types of strategies were identified and assess the quality of its application.
Materials & methods
Search strategy
We searched English language articles in Medline, Embase, Cochrane Library, CINAHL and PsycINFO without any date restrictions on 4 October 2017. We also searched the references of included studies to find additional studies. An outline of the search strategy for PubMed is shown in the protocol, which is attached as an appendix. It was modified and adapted for various databases. Additional searches were carried out by manually reviewing the reference lists of included studies.
Systematic review registration
We carried out a systematic review according to a prespecified protocol. The protocol was registered at PROSPERO (CRD42017078221). Details of the search are available from the protocol. We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist for reporting the results [7].
Eligibility criteria & participants
We included studies of any design (e.g., qualitative, quantitative and mixed method) without any restrictions on study design, if the study has reported on the use of positive deviance approaches for vaccination among children and adults. We excluded narrative reviews and studies that did not use the positive deviance approach or address the outcome of vaccination.
Interventions
We used a broad definition of the positive deviance approach, which relied on the definition in the primary studies. Positive deviance approaches may have different names (e.g., bright star) and all such studies were eligible for inclusion. We did not limit ourselves to high performers but also evaluated studies that reported on low-performing providers and health systems.
Outcomes
We conducted a qualitative synthesis of data to identify potentially effective strategies for improving vaccination coverage using the positive deviance approach. We also attempted to determine the quality of such studies.
Data extraction
Studies were selected for inclusion based on the review of titles and abstracts that were exported into a web-based data management repository (www.rayyan.qcri.org) [8]. Articles, titles and abstracts were screened by two authors independently for potentially eligible articles. Any discordance between the authors over the eligibility of any article were resolved by reference to the full text, and all discrepancies were resolved by agreement after rechecking the source papers, further discussion among the reviewers, and full consensus prior to inclusion. Two reviewers were independently involved in all stages of study selection, data extraction and quality assessment. We extracted data on all relevant outcomes for each of the research questions, including that relating to study design, the location of the study, the study characteristics and the stages of the positive deviance approach. We extracted data on the major themes onto an iterative framework that listed the various strategies used to improve vaccination rates as a part of positive deviance approach. We also evaluated data on the results of the risk of bias assessment.
Quality assessment
We used the 16-item QATSDD tool [9], scored on a Likert scale of 1–4 to evaluate the risk of bias. This tool shows good reliability and validity in the quality assessment when studies included in the systematic review have diverse study designs.
Data synthesis
All data were extracted into a prespecified Excel data sheet. We compiled all strategies for improving vaccination coverage and created an organizing framework of strategies using thematic analysis. We did not conduct a separate analysis of strategies identified by high performers to low performers because the primary studies did not report the data to enable such comparisons. We extracted the strategies as reported in the results section of each study and compiled a list of all strategies identified with examples. The core strategies identified represent a compilation of successful strategies identified in studies that included both high- and low-performing sites and high-performing sites only.
Findings
Systematic search
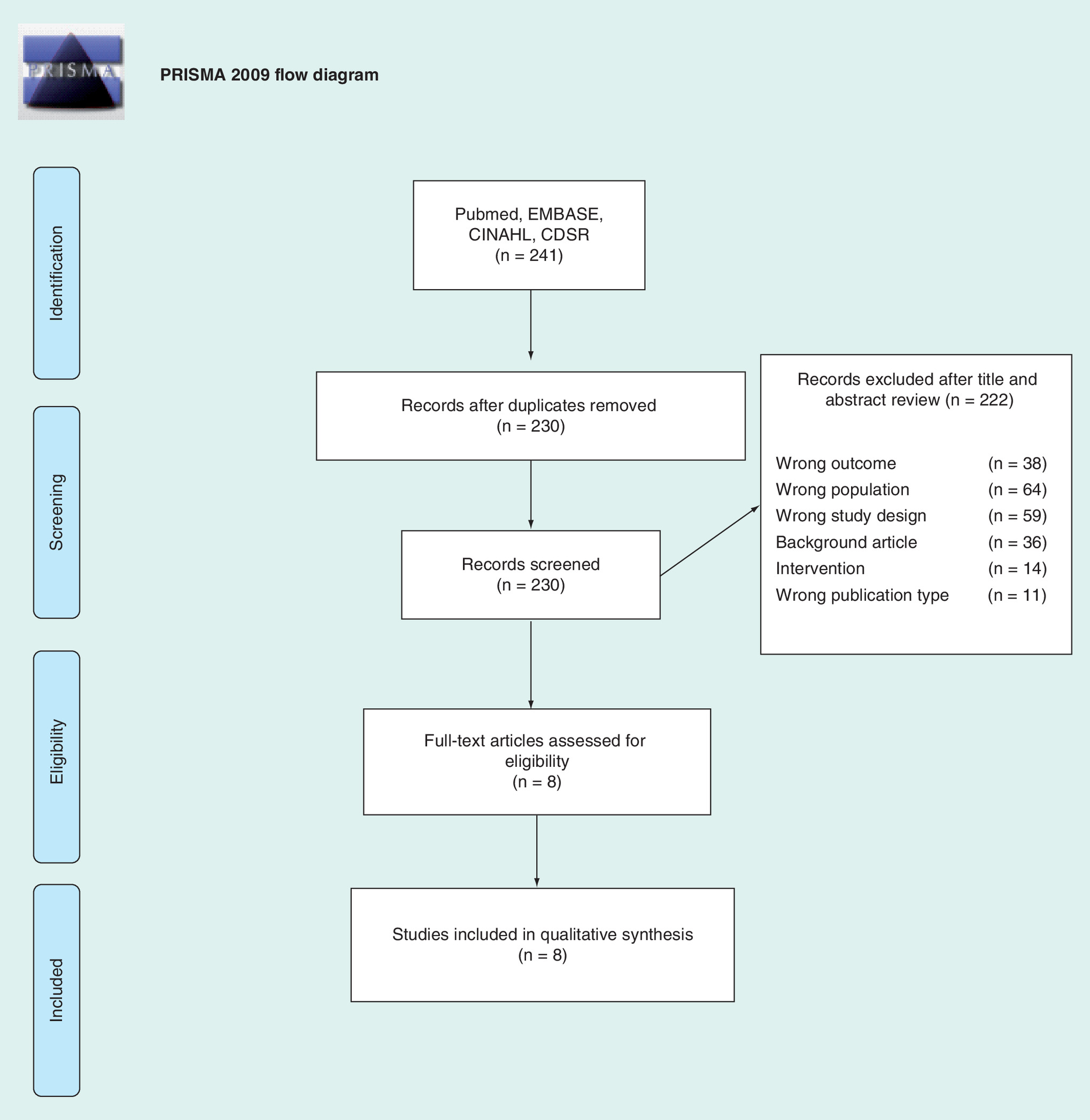
We screened 241 citations and identified eight studies that were eligible for inclusion [10–17]. The process of study selection is shown in Figure 1. The baseline characteristics of the studies are shown in Table 1. Five studies were conducted in the USA [10,11,15–17], two studies in Africa [12,13] and one study in the UK [14]. Similarly, differences in vaccine characteristics (number of doses required, seasonality, response to epidemic, availability) also resulted in differences between studies. The settings varied, from evaluating programs in practice sites [14,17], public vaccination clinics [10], to evaluating programs at district levels [12], local health departments [11] and health plans [15]. These studies evaluated a range of vaccines including H1N1 vaccination among school children [10,11], Diphtheria pertussis and tetanus vaccination [12,13], influenza vaccination [14], human papilloma virus (HPV) vaccination [15] and vaccination for children diptheria pertussis tetanus (DTP)/diptheria tetanus acellular pertussis (DTaP), polio, measles mumps rubella (MMR), Hib, HepB [17]. All studies identified positive deviants and generated hypotheses about how such deviants succeed, although not all studies used an objective performance measure to identify high performers [10–17]. We did not identify any studies that tested hypotheses quantitatively or addressed the dissemination stage of the positive deviance approach.
| Study (year) | Location | Setting and context | Vaccine and target population | Positive deviant identification |
|---|---|---|---|---|
| Klaiman et al. (2013) | USA (nine states) | Local health departments’ public vaccination clinics (n = 13) of varying size, serving rural, suburban and urban communities across the USA | H1N1 (flu) | Review of National Association of County & City Health Officials Model Practices database and emergency preparedness conferences and research partners, recommendations from peers |
| Klaiman et al. (2014) | USA (nine states) | Local health departments’ school-based vaccination clinics (n = 13) of varying size, serving rural, suburban and urban communities across the USA | H1N1 (flu); School-aged children | Review of National Association of County & City Health Officials Model Practices database and emergency preparedness conferences and research partners, recommendations from peers |
| LaFond et al. (2015) | Ethiopia, Cameroon and Ghana | Immunization programs in 12 districts; part of ARISE project | DPT3/Penta 3 | Routine immunization coverage rates 2006 and 2010; compared improvers with those with steady coverage |
| Naimoli et al. (2008) | Sub-Saharan Africa | Six countries (Ghana, Rwanda, Malawi, Ethiopia, Mauritania, Cameroon) in sub-Saharan Africa | DPT3; Children under 5-year old, 1997–2002 | WHO/UNICEF estimates of DPT3 coverage, 1997–2002; included high, medium–high, medium–low and low performers |
| Newby et al. (2016) | UK (Coventry and Warwickshire) | Practices (n = 20) of varied size serving diverse population with regard to deprivation, age, race/ethnicity and rural versus urban setting | Flu; Individuals older than 65 years old, under 65 years old with chronic condition and pregnant women | Flu vaccination uptake rates, 2014; included practices with high (>75%) or low (<75%) uptake |
| Razouki et al. (2016) | VA system in the USA | Flu campaign at six VA medical centers of varied size across the USA | Flu; HCPs | HCP flu vaccination rates 2011–2013; included high performers (rates >70%) and low performers (<40%) |
| Ng et al. (2017) | USA (Northeast, West, Midwest) | Commercial and Medicaid HMO plans serving racially diverse urban and rural population across the USA | HPV; Female adolescents | HEDIS measure (% plan members who receive three doses of HPV between 9 and 13 years of age), 2013 |
| Wishner et al. (2005) | Pennsylvania, USA | Private pediatric (n = 9) and family practices (n = 1) participating in Pennsylvania Educating Physicians in their Communities (EPIC) Immunization Education Program; practices varied in size and setting (urban, suburban, town and rural) | DTP/DTaP, Polio, MMR, Hib, HepB; Children | CASA score of immunization up-to-dateness among 2-year olds, 2000–2001; included practices with above-average (≥87%) and average (60–85%) scores |
ARISE: African RI System Essential; CASA: Clinic assessment software application; DTaP: Diptheria tetanus acellular pertussis; DPT3: Diptheria pertussis tetanus; HCP: Healthcare provider; HEDIS: Healthcare effectiveness data information set; HMO: Health maintenance organization; HPV: Human papilloma virus; MMR: Measles mumps rubella; Penta 3: Pentavalent3; VA: Veterans affairs.
Quality assessment
The quality assessment of the included studies using the QATSDD tool [9] was variable with incomplete reporting of several data elements as shown in Table 2. Most studies stated their aims and objectives and described the research setting. Only four studies provided a rationale for sample size [10,11,13,14]. Details of the recruitment process were only available from four studies [14–17]. These reflect a limitation in the reporting of studies rather than a judgment of its quality. Although most studies outlined a process of identifying positive deviants, this was not sufficiently detailed. Two studies described this in more detail but selected positive deviants using a subjective approach. Most studies did not clearly describe the process of selecting positive deviants or include detailed questionnaires or interview guides [10,11]. Only the Naimoli study measured routine vaccination coverage that is considered one of the best approaches to measure effectiveness of a vaccination strategy.
| Category | Klaiman et al. (2013) | Klaiman et al. (2014) | LaFond et al. (2015) | Naimoli et al. (2008) | Newby et al. (2016) | Razouki et al. (2016) | Ng et al. (2017) | Wishner et al. (2005) |
|---|---|---|---|---|---|---|---|---|
| Explicit theoretical framework | 2 | 2 | 2 | 2 | 0 | 1 | 0 | 1 |
| Stated aims/objectives | 1 | 1 | 2 | 3 | 3 | 3 | 3 | 1 |
| Clear description of research setting | 1 | 1 | 2 | 3 | 3 | 3 | 2 | 1 |
| Evidence of sample size considered in analysis | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 0 |
| Representative sample of target group of reasonable size | 1 | 1 | 1 | 2 | 2 | 2 | 0 | 0 |
| Description of procedure for data collection | 1 | 1 | 1 | 2 | 2 | 2 | 1 | 0 |
| Rationale for choice of data collection | 1 | 1 | 1 | 1 | 2 | 2 | 1 | 1 |
| Detailed recruitment data | 0 | 0 | 0 | 0 | 3 | 3 | 2 | 1 |
| Statistical assessment of reliability and validity | NA | NA | NA | NA | NA | NA | NA | NA |
| Fit between method of data collection and statistical analysis | NA | NA | NA | NA | NA | NA | NA | NA |
| Fit between research question and content of data collection tool | 1 | 1 | 2 | 2 | 3 | 2 | 2 | 1 |
| Fit between research question and method of analysis | 1 | 1 | 3 | 2 | 3 | 3 | 2 | 1 |
| Good justification for analytical method | 1 | 1 | 2 | 1 | 1 | 1 | 1 | 0 |
| Assessment of reliability of analytical process | 0 | 0 | 3 | 1 | 1 | 1 | 0 | 0 |
| Evidence of user involvement in design | 1 | 1 | 1 | 2 | 0 | 0 | 0 | 0 |
| Strengths and limitations critically discussed | 1 | 1 | 2 | 3 | 2 | 1 | 2 | 0 |
Data taken from [9].
0 = Not at all; 1 = Very slightly; 2 = Moderately; 3 = Complete.
NA: Not applicable.
Strategies & themes
The studies were conducted in heterogeneous settings with differences in contextual factors, system characteristics, vaccines of interest and the population targeted. However, despite these differences, several broad themes emerged. We characterized these themes as strategies and factors related to the process of vaccine delivery, supporting structural elements and contextual factors. We present a model of the potential relationship between these elements in Figure 2.
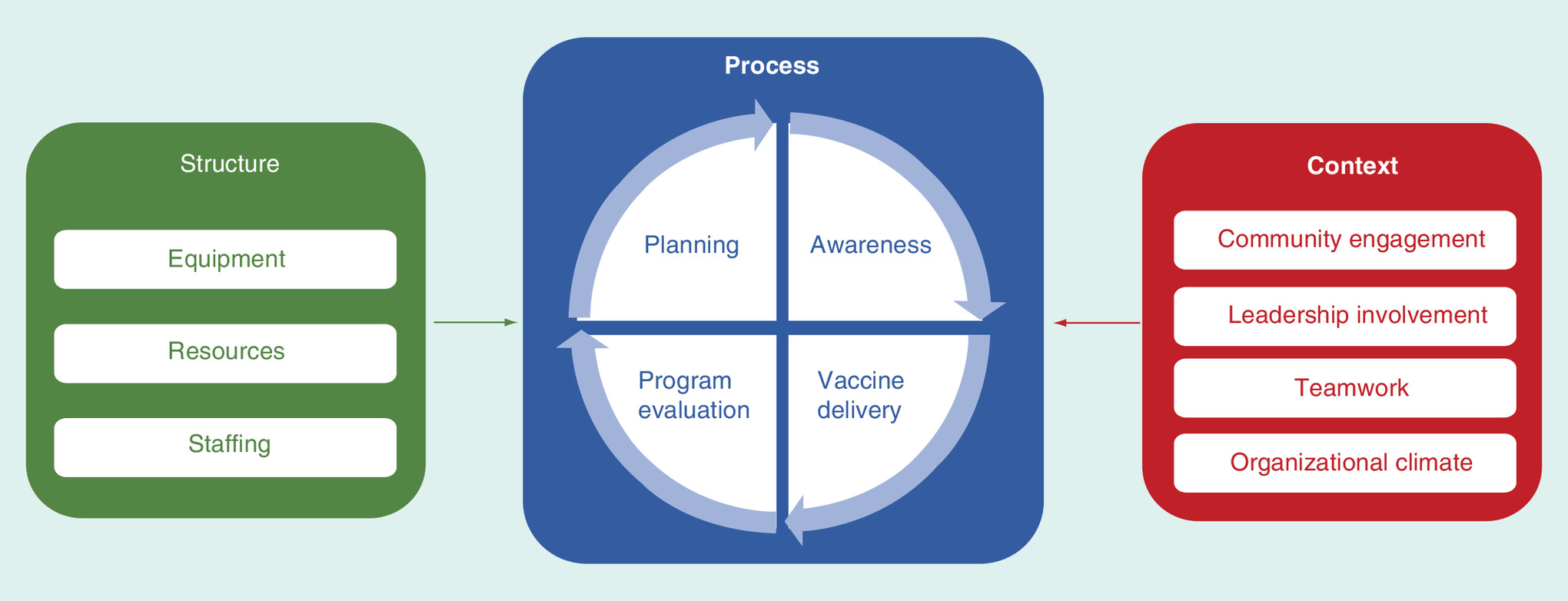
Key elements that characterize the process of vaccine delivery among high performers were found consistently across studies and can be categorized as: planning, raising awareness of vaccination, vaccine delivery and vaccine program evaluation as shown in Table 3. Many studies described collaborative planning with stakeholders and community partners as important to achieving successful vaccination programs. Approaches to increasing awareness and acceptance of vaccination among the target population included the need for tailored, targeted and deliberate messaging designed to overcome barriers to vaccination. Targeted communication is intended for a subgroup of participants based on participant characteristics shared by the group; whereas tailored communication is intended to reach one specific individual [18]. In the context of vaccine delivery, targeting refers to increasing the immunization level of the population by delivering vaccines to groups at the highest risk.
| Process | Ref. |
|---|---|
| Planning | |
| Advance planning necessary to optimize vaccine delivery Examples: Vaccine delivery locations and schedules, priority groups for vaccination, strategies to facilitate access and reach remote communities | [12] |
| High performers plan in collaboration with stakeholders | [11,12,16] |
| Awareness | |
| Message content should be tailored, targeted and deliberated to overcome vaccination barriers (Razouki, Klaiman, 2013, Ng) Examples: Counseling and motivational interviewing for vaccine decliners, use of default (‘you are due for your HPV vaccine’ rather than opt-in (‘would you like your HPV vaccine?’) communication strategy | [10,15,16] |
| Engage variety of people in delivering the message, including trusted, familiar individuals to make message more persuasive Examples: Use of community-centered health workers to deliver message, reference community organizations such as CDC or American Cancer Society in educational materials | [12,15,16] |
| Innovative and multimodal approach to deliver messages and reminders to target population Examples: Flashing road signs to inform residents of vaccination clinics; use of social media, websites, newspaper, radio and written materials to educate and increase patient awareness; reminders to patients via postcards, automated calls and birthday cards | [10,11,14,15,16] |
| Vaccine delivery | |
| Tailor the location, timing and/or vaccine delivery to maximize attendance of target population and make the vaccine convenient and easy to access Examples: Hold vaccine clinics for vulnerable populations in familiar buildings (shelters, senior centers), tailor vaccine clinic hours to target population, provide vaccination ‘opportunistically’ at any visit, use of standing orders to take vaccination out of physician’s hands, elimination of copays | [10,11,12,14,15,16] |
| Program evaluation | |
| Regular review and evaluation of vaccination program to assess needs, performance and problem-solving Examples: Regular team-oriented meetings with focus on problem solving, constructive discussion and peer learning; use of data for feedback and motivation | [11,12,15,16] |
| Identification and tracking of unvaccinated individuals to allow targeted messaging and vaccine delivery Examples: Identify ‘hotspots’ of refusers to target messaging. | [11,12,15,16] |
HPV: Human papilloma virus; CDC: Centers for Disease Control and Prevention.
Several studies described the benefits of engaging a variety of people in delivering this message, and particularly the value of including trusted and familiar individuals such as community health workers or well-known organizations to make the message more persuasive. Finally, most studies identified innovative and multimodal approaches to delivering vaccination-related messages and reminders to the target population as important features of high performers. Strategies to optimize the delivery of the vaccine used by high performers include tailoring clinic hours and locations to the needs of the target population, and policies to make vaccination a default option. Examples of this include use of standing orders and providing vaccination ‘opportunistically’ at any visit. Half of the studies described the use of regular program evaluation that often included efforts to identify and track unvaccinated individuals to inform future planning.
Structural elements such as staffing and vaccine supply are necessary, but not enough to distinguish improvers, according to LaFond et al. [12]. Such elements could include appropriately trained staff [12], dedicated staff toward vaccination campaigns [16] and/or enough staff or volunteers to ensure vaccination [10]. Other resources include ensuring the cold chain supply, an adequate and reliable vaccine supply, transportation and financing [12].
Identifying contextual factors and mechanisms (strategies) that lead to success is an overarching goal of positive deviance. While we did not parse out each strategy and theme and the context in which it worked well, the setting and context for each study is shown in Table 1. Three studies [10–12] used a realist evaluation to learn about the combinations of context and mechanisms that led select schools, health departments or districts to perform well. This enabled them to not only describe which approaches worked well but also in which contexts they did so. The remaining studies reviewed took different real-world approaches to doing that and achieved variable results in identifying interactions between context and strategies.
There were several contextual factors, including community engagement that were identified as important strategies in the included studies. Community engagement was an important factor noted by LaFond et al., who engaged a cadre of community health workers to ensure vaccine access for the community [11]. Klaiman et al. engaged the community to reach vulnerable populations and ensured that community providers supported the setting up and taking down of clinics [10]. Efforts at community engagement included establishing relationships with school authorities to set up clinics [11].
The role of leadership and organizational climate was identified as important to high-performing status in several studies [10,12,17]. There were several characteristics of leaders that ensured success. These included leadership styles which prioritized vaccination [14,16,17]. Some leaders administered the vaccine themselves, participated in skits promoting the vaccines and empowered vaccination campaigns via town hall meetings and larger events. The leaders at high-performing sites were noted to be tenacious, and a single leader was responsible for performance, as compared with fragmented leadership with no clear lead at low-performing sites [14]. Wishner et al. noted that there were a greater number of leaders with dominant managerial styles at above-average performing sites [17]. These leaders provided a clear vision and mobilized people to achieve this vision.
Two studies identified organization flexibility as an important feature of high performers. For example, Klaiman et al. noted the importance of flexibility in decision-making, staffing and clinic implementation [11]. Wishner et al. also noted that organizational climates that fostered a higher sense of responsibility among employees were associated with higher performance among small practices [17]. One study reported on team characteristics of high performers where team members worked together closely, had frequent communications, established close working relationships and were empowered to find solutions [16].
Discussion
Summary of findings
We found that a small but diverse group of positive deviance studies have been used to identify effective strategies for facilitating the uptake of vaccines. These studies focused on settings ranging from the clinic, community, public health organizations, health plans and national policy settings. Despite this diversity, we identified several core strategies and approaches that appear to support vaccine uptake in real-world settings. Such strategies may be helpful to organizations seeking to improve vaccination rates.
One of the key findings from these studies was the importance of tailoring and targeting in both messaging and delivery of vaccines as well as the importance of tracking delivery of vaccines. Targeted communication is intended for a subgroup of participants based on participant characteristics shared by the group; whereas tailored communication is intended to reach one specific individual. In the context of vaccine delivery, targeting also refers to increasing the immunization level of the population by delivering vaccines to groups at highest risk.
Our findings suggest the importance of patient and provider education, reminders, feedback loops, community collaborations, immunization registries and use of the medical home – a comprehensive patient or family-centered approach to primary care. Although the specific strategy used will depend on the local context, the findings from our review can be used to inform planning and implementation of efforts to improve vaccination. These findings are consistent with the understanding that there is rarely a ‘one-size-fits-all’ solution to complex problems such as increasing vaccination rates.
Comparison to other studies
There is a striking similarity on the types of strategies to support vaccination identified via the positive deviance approach and those proven to be effective in interventional studies. For example, our systematic review identified strategies comparable to those identified in a systematic review of 183 studies of interventions to improve vaccination among children, adolescents and adults in the USA [19]. That study categorized interventions under three headings: increasing community demand, enhancing access to vaccination services and provider-based interventions. There was evidence to support that community demand can be increased through client reminder or recall, the use of educational interventions, vaccination requirements for child care, school or college attendance. There was also evidence to support enhancing access to vaccination services through reduction of out of pocket costs, expanding access to healthcare settings and home visits and vaccinations in schools. Strong evidence supports the use of provider-based interventions including reminders to providers, assessment of and feedback to providers, and standing orders for vaccinations in adults. There is a striking similarity in the types of strategies to support vaccination identified via the positive deviance approach and those proven to be effective in interventional studies. This suggests that many of the strategies identified by studying high performers may in fact be effective despite the lack of quantitative hypothesis testing in these studies and supports the approach of positive deviance as an efficient means to identify effective real-world strategies. However, it is possible that some of the strategies used by high performers were informed by evidence generated from randomized controlled trials.
The set of interventions that were successful in our review is largely like those recommended by the CDC guidelines because they were likely informed by these guidelines or the underlying evidence. For example, many of the processes of vaccine delivery used by high performers (Table 3) included approaches outlined in the CDC Task Force on Community Preventative Services, such as prompts and reminders and reducing logistical barriers to vaccination. However, our study also identified novel contextual factors that are hypothesized to contribute to successful vaccination coverage, such as community engagement, teamwork, organizational climate and leadership characteristics, illustrating the potential value of the positive deviance approach.
Strengths & limitations
There are several strengths to the positive deviance approach. The strategies are practical, common sense and doable with the resources that most organizations have available. It is neither practical nor feasible to conduct a randomized controlled trial of each strategy or variation identified in these studies, but the approaches listed above provide a starting point for organizations to consider incorporating into their local approaches to vaccination. We also noted variation in the quality of studies which was anticipated. In addition, several of the studies lacked specificity or details on their approach. The process of identifying high performers via peers rather than by measures of actual performance is a limitation of some studies [10,11]. Very few studies involved multiple types of stakeholders (such as patients) or collect data at multiple levels. For example, the study on HPV vaccination collected data at only one level, interviewing medical directors and quality improvement staff of health plans [15]. We could not comment on the effectiveness of these strategies, or the value of dissemination since none of the studies quantitative conducted hypothesis testing or dissemination.
There are limitations to our review. Although we conducted a comprehensive search, it is possible that we may have missed few studies because the terminology used to describe positive deviants is somewhat inconsistent. We did not include non-English studies which may have biased our results. Few studies were conducted in the USA, which limits the generalizability of the findings from studies conducted in the UK or Africa to the USA where practice patterns are different. It is possible that we missed subsequent hypothesis testing studies, which may not be reported as such, or labeled as positive deviance studies. We cautiously consider these strategies to be potentially effective strategies for several reasons. Only one study reported vaccination as a measure of effectiveness. Furthermore, the findings from such qualitative studies should only be considered hypothesis generating and will require testing in larger samples to generate conclusive results on effectiveness.
Despite these limitations, there are several strengths to our review. We conducted a comprehensive search according to a prespecified protocol and included studies that addressed diverse approaches to vaccination. We were able to identify themes that are applicable in real-world settings and have face validity. These can be used to inform future strategies to improve vaccination.
Recommendations
Future studies should clearly define the approach used to identify positive deviants and should use objective measures of performance. Without an objective means of selecting high performers, the implications of the identified strategies are difficult to interpret and replicate. A recent study that sets forth criteria for assessing suitability of measures of hospital quality and safety as a good first step toward standardizing selection of indicators to use to select positive deviants could serve as a useful guide [20].
Success may be more broadly defined and conceptualized than simply high vaccination coverage rates when conducting such studies. It is possible that some of the parameters of ‘success’ identified in our review (minimizing disruption, costs, parental concerns) may be features of programs that effectively promote vaccination coverage.
Five studies included in our review included low performers [12–14,16,17]. Researchers should also consider including low performers to identify those characteristics that differentiate high performers from low performers, and also shed light on ineffective strategies.
Future studies, including systematic reviews, could also evaluate whether effective strategies that improve vaccination in randomized controlled trials are similar or dissimilar from those identified using the positive deviance approach.
Conclusion
We found that a small but diverse group of positive deviance studies has been used to identify effective strategies for facilitating the uptake of vaccines. Despite this diversity, and the variable quality of these studies we identified several core strategies and approaches that appear to support vaccine uptake in real-world settings. Such strategies may be helpful to organizations seeking to improve vaccination rates
Future perspective
The value of the positive deviance approach may be fully realized by including positive and negative deviants to determine which individual strategies or their combinations distinguish high from low performers. Larger studies which include collection of quantitative data are needed to test hypothesis regarding specific strategies and to understand the context in which vaccination strategies are effective.
•
Our systematic review shows that a small but diverse group of studies that applied the positive deviance approach identified several potentially effective strategies for facilitating the uptake of vaccines.
•
These strategies include tailoring and targeting in both messaging and delivery of vaccines and emphasize the importance of tracking delivery of vaccines.
•
Additional effective strategies identified by the positive deviance approach include patient and provider education, reminders, feedback loops, community collaborations, immunization registries and use of the medical home.
•
Although the specific strategy used will depend on the local context, the findings from our review can be used to inform planning and implementation of efforts to improve vaccination coverage.
Acknowledgments
The authors appreciate the help of Leah Goldman, who contributed to the development of the study protocol and data extraction and Calli Oleksy in preparing the manuscript for submission.
Author contributions
S Singh, K Fisher and KM Mazor contributed to the manuscript by planning the study and reviewing the literature and extracting the data. All the authors contributed to the assessment and interpretation of data. All the authors read, revised and approved the final version of the manuscript.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Data sharing statement
All relevant data are included in the manuscript. Additional data are available from the authors on request.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Feldstein LR, Mariat S, Gacic-Dobo M et al. Global routine vaccination coverage, 2016. MMWR Morb. Mortal. Wkly Rep. 66, 1252–1255 (2017).
2.
Baxter R, Taylor N, Kellar I et al. What methods are used to apply positive deviance within healthcare organisations? A systematic review. BMJ Qual. Saf. 25(3), 190–201 (2016).
•• This systematic review reports on key studies that have used the positive deviance method in healthcare systems.
3.
Bradley EH, Curry LA, Ramanadhan S et al. Research in action: using positive deviance to improve quality of health care. Implement. Sci. 4, 25 (2009).
4.
Lawton R, Taylor N, Clay-Williams R et al. Positive deviance: a different approach to achieving patient safety. BMJ Qual. Saf. 23(11), 880–883 (2014).
5.
Marsh DR, Schroeder DG, Dearden KA et al. The power of positive deviance. BMJ 329(7475), 1177–1179 (2004).
6.
Krumholz HM, Curry LA, Bradley EH. Survival after acute myocardial infarction (SAMI) study: the design and implementation of a positive deviance study. Am. Heart J. 162(6), 981–987.e9 (2011).
•• Important study that illustrates the success of the positive deviance approach in improving survival after myocardial infarction, which stimulated more research using this method.
7.
Moher D, Liberati A, Tetzlaff J et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 6(7), e1000097 (2009).
8.
Ouzzani M, Hammady H, Fedorowicz Z et al. Rayyan – a web and mobile app for systematic reviews. Syst. Rev. 5(1), 210 (2016).
9.
Sirriyeh R, Lawton R, Gardner P et al. Reviewing studies with diverse designs: the development and evaluation of a new tool. J. Eval. Clin. Pract. 18(4), 746–752 (2012).
10.
Klaiman T, O’Connell K, Stoto M. Local health department public vaccination clinic success during 2009 pH1N1. J. Public Health Manag. Pract. 19(4), E20–E26 (2013).
• Study reporting on the use of the positive deviance approach to support local vaccination efforts.
11.
Klaiman T, O’Connell K, Stoto MA. Learning from successful school-based vaccination clinics during 2009 pH1N1. J. Sch. Health 84(1), 63–69 (2014).
• Study reporting on the use of the positive deviance approach to support vaccination efforts in a school-based setting.
12.
LaFond A, Kanagat N, Steinglass R et al. Drivers of routine immunization coverage improvement in Africa: findings from district-level case studies. Health Policy Plan. 30(3), 298–308 (2015).
13.
Naimoli JF, Challa S, Schneidman M et al. Toward a grounded theory of why some immunization programmes in sub-Saharan Africa are more successful than others: a descriptive and exploratory assessment in six countries. Health Policy Plan. 23(6), 379–389 (2008).
14.
Newby KV, Parsons J, Brooks J et al. Identifying strategies to increase influenza vaccination in GP practices: a positive deviance approach. Family Prac. 33(3), 318–323 (2016).
• Study reporting on the use of the positive deviance approach to support vaccination efforts in practices in the UK.
15.
Ng JH, Sobel K, Roth L et al. Supporting human papillomavirus vaccination in adolescents: perspectives from commercial and medicaid health plans. J. Public Health Manag. Pract. 23(3), 283–290 (2017).
16.
Razouki Z, Knighton T, Martinello RA et al. Organizational factors associated with Health Care Provider (HCP) influenza campaigns in the Veterans health care system: a qualitative study. BMC Health Serv. Res. 16, 211 (2016).
17.
Wishner A, Aronson J, Kohrt A et al. Best practices: applying management analysis of excellence to immunization. J. Med. Pract. Manage. 20(5), 275–278 (2005).
18.
Kreuter MW, Wray RJ. Tailored and targeted health communication: strategies for enhancing information relevance. Am. J. Health Behav. 27(Suppl. 3), S227–S232 (2003).
19.
Briss PA, Rodewald LE, Hinman AR et al. Reviews of evidence regarding interventions to improve vaccination coverage in children, adolescents, and adults. The Task Force on Community Preventive Services. Am. J. Prev. Med. 18(Suppl. 1), 97–140 (2000).
20.
O’Hara JK, Grasic K, Gutacker N et al. Identifying positive deviants in healthcare quality and safety: a mixed methods study. J. R. Soc. Med. 111(8), 276–291 (2018).
Information & Authors
Information
Published In
Pages: 1055 - 1065
PubMed: 31580161
Copyright
© 2019 Future Medicine Ltd.
History
Received: 9 May 2019
Accepted: 5 August 2019
Published online: 3 October 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Positive deviance approaches to improving vaccination coverage rates within healthcare systems: a systematic review. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0056
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Mayumi Mizutani, Harumi Bando, Sofi Oktaviani, Naoko Nishitani, Junko Nishimura, Ritsuko Nishide, Susumu Tanimura, Global trends of positive deviance research in public health: A bibliometric analysis (1976–2024), Preventive Medicine Reports, 10.1016/j.pmedr.2025.103139, 56, (103139), (2025).
- Hyoseon Choi, Janghee Park, Sanghee Yeo, Seung-Joo Na, Hyojin Kwon, Physicians’ and Residents’ Well-Being in Ecological System: A Scoping Review of Positive Deviance Strategies, Healthcare, 10.3390/healthcare13151856, 13, 15, (1856), (2025).
- Mitchell A. M. Matthijssen, Mariëlle Cloin, Florian van Leeuwen, Ien van de Goor, Peter Achterberg, What made people (more) positive toward the COVID-19 vaccine? Exploring positive and negative deviance perspectives, BMC Public Health, 10.1186/s12889-024-21027-1, 25, 1, (2025).
- Ayelign Mengesha Kassie, Elizabeth Eakin, Biruk Beletew Abate, Aklilu Endalamaw, Anteneh Zewdie, Eskinder Wolka, Yibeltal Assefa, The use of positive deviance approach to improve health service delivery and quality of care: a scoping review, BMC Health Services Research, 10.1186/s12913-024-10850-2, 24, 1, (2024).
- Ayelign Mengesha Kassie, Elizabeth Eakin, Biruk Beletew Abate, Aklilu Endalamaw, Anteneh Zewdie, Eskinder Wolka, Yibeltal Assefa, Use of the positive deviance approach for healthcare system service improvement: a scoping review protocol, BMJ Open, 10.1136/bmjopen-2023-078809, 13, 12, (e078809), (2023).
- Ken Ing Cherng Ong, Jennifer Lisa Sakamoto, Masamine Jimba, Positive Deviance Leading and Coping with Social Change, The Palgrave Handbook of Global Social Change, 10.1007/978-3-030-87624-1_69-1, (1-12), (2023).
- Roisin O’Malley, Paul O’Connor, Caoimhe Madden, Sinéad Lydon, A systematic review of the use of positive deviance approaches in primary care, Family Practice, 10.1093/fampra/cmab152, 39, 3, (493-503), (2021).