Negative pressure wound therapy in total hip and knee arthroplasty: a meta-analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To assess the efficiency and safety of negative pressure wound therapy (NPWT) in the total hip and knee arthroplasty, we conducted a meta-analysis from randomized controlled trials. Methods: Potential academic articles were identified from the Cochrane Library, PubMed, Embase, Springer and ScienceDirect. Secondary sources were identified from the references of the included literature. RevMan 5.1 was used to analyze the pooled data. Results: Six randomized controlled trials met the inclusion criteria. Meta-analysis showed more superficial surgical site infection and blisters in patients with total knee arthroplasty. There were no significant differences between two groups in total infection and total complications. Conclusion: NPWT decreased the incidence of superficial surgical site infection. More blisters were noticed in patients with NPWT after total knee arthroplasty.
Total hip and knee arthroplasties (THA and TKA, respectively) are effective procedures to treat advanced stages of knee and hip osteoarthritis. Wound complications, especially the surgical site infection (SSI), are substantial problems. Although the rate of infection is relatively low (0.2–2.3%) [1], serious infection could require extra medical interventions and result in unsatisfactory outcomes [2]. Besides, extra money will cost for infections including surgical intervention, more tests and longer ward care. A recent retrospective study reported that infection significantly increased the cost of infection after total joint arthroplasty. Compared with the mean €7200 for a normal total joint arthroplasty, extra €12,800 were needed for debridement, antibiotics and implant retention treatment, and €44,600 for a two-stage revision [3]. Complex procedures also caused increased risk of heterotopic ossification after THA [4], high rate of joint dislocation [5].
Negative pressure wound therapy (NPWT) induces macro and micro deformation, improving wound healing. Besides that, NPWT decreases the accumulation of hematoma and seroma, producing a dryer wound, and with less chance of healing complication and infection. NPWT was reported to improve more formation of granulation and hasten wound closure by increasing blood flow, saturation of oxygen and stimulating angiogenesis [6]. NPWT has been proposed for closed wounds to provide a clean, dry wound environment in the immediate postoperative period [7]. Howell et al. performed a randomized clinical trial (RCT) to evaluate the effect of NPWT on intact postoperative wound after TKA. They found more blisters in the NPWT group than standard dressing group (63 vs 12%) [8]. Therefore, they stopped their study early on the behalf of safety and did not suggest its routine use in primary TKA. However, the device used in this study was an old version and modern devices were invented later. Promising effect of NPWT was showed in THA with significant reduction of seromas (44 vs 90%) in the closed wounds confirmed by ultrasound [9]. Recently, several studies demonstrated that NPWT was applied in total ankle arthroplasty [10], and TKA and THA [11–14]. The clinical effect of the application of NPWT in THA and TKA remains controversial.
Therefore, we conducted a large sample meta-analysis to evaluate the efficiency and safety of NPWT in THA and TKA from RCTs. Based on our clinical experience, we hypothesized that the NPWT can reduce SSI and perform differently for TKA and THA.
Materials & methods
Literature & search strategy
The meta-analysis was performed according to the prioritized reported items for systematic review and meta-analysis (PRISMA guidelines). The electronic databases, including PubMed, Cochrane CENTRAL, ScienceDirect and Embase were searched to identify the studies evaluating NPWT in THA or TKA from the inception of electronic databases to November 2018. Structured search strategies were used in combination, according to Boolean logic: ‘negative pressure’, ‘arthroplasty or replacement’, ‘wound’ and ‘infection’. In addition, manual research of reference list was conducted for other potential included trials. The meta-analysis was based on acknowledged guidelines of the prioritized reported items for systematic review and meta-analysis.
Inclusion & exclusion criteria
Studies were considered eligible for inclusion if they satisfy the following criteria: population: patients treated with THA or TKA; intervention: NPWT, control: conventional dressing; outcome measures, one or more of the following outcomes were reported: SSI, reoperation, complications and other outcomes; and, study design: published RCTs.
We excluded articles that were studies without controlled groups; articles without available full-text versions; and no available outcomes data.
Data extraction & outcome measures
Two of the reviewers independently reviewed and extracted information from the identified studies including first author name, publication year, country, sample size, intervention characteristics and outcome measures. The major outcomes we concerned included SSI, wound complications (other than infection) and reoperation.
Quality assessment
The quality assessment of the randomized trial was conducted using the Cochrane Collaboration. The literature quality was evaluated separately by two reviewers. Consensus was reached through consultation for divergence.
Data analysis & statistical methods
The RevMan 5.1 (The Cochrane Collaboration, Oxford, UK) was used for analyzing the pooled data. Heterogeneity was estimated by the p-value and I2 based on the standard χ2 test. If there was significant heterogeneity (I2 >50%, p < 0.1), a random-effects model was used for data analysis. When no significant heterogeneity was found (I2 <50%, p > 0.1), a fixed-effects model was used for the data analysis. In cases of significant heterogeneity, a subgroup analysis was performed to investigate the sources. The mean differences and 95% CIs were determined for continuous outcomes. Dichotomous data were calculated by the odds ratio (OR) and 95% CIs.
Results
Search results
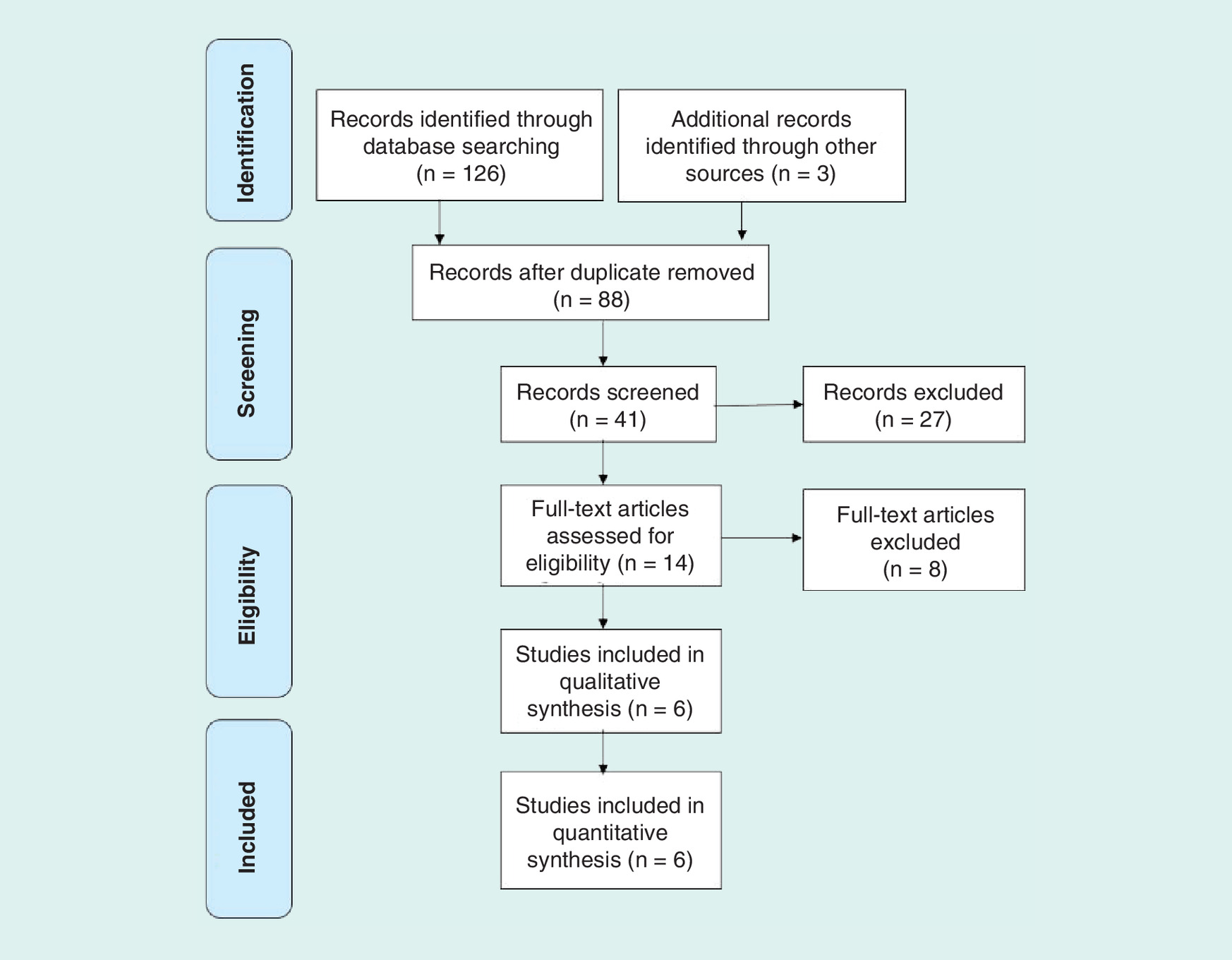
A total of 129 reports were identified as potentially relevant literature reports. By scanning title and abstract, 115 reports were excluded according to the eligibility criteria. Eight reports are eliminated after browsing the full text. Eventually, six RCTs were eligible for data extraction and meta-analysis. The searching process is shown in Figure 1.
Study characteristics & risk of bias assessment
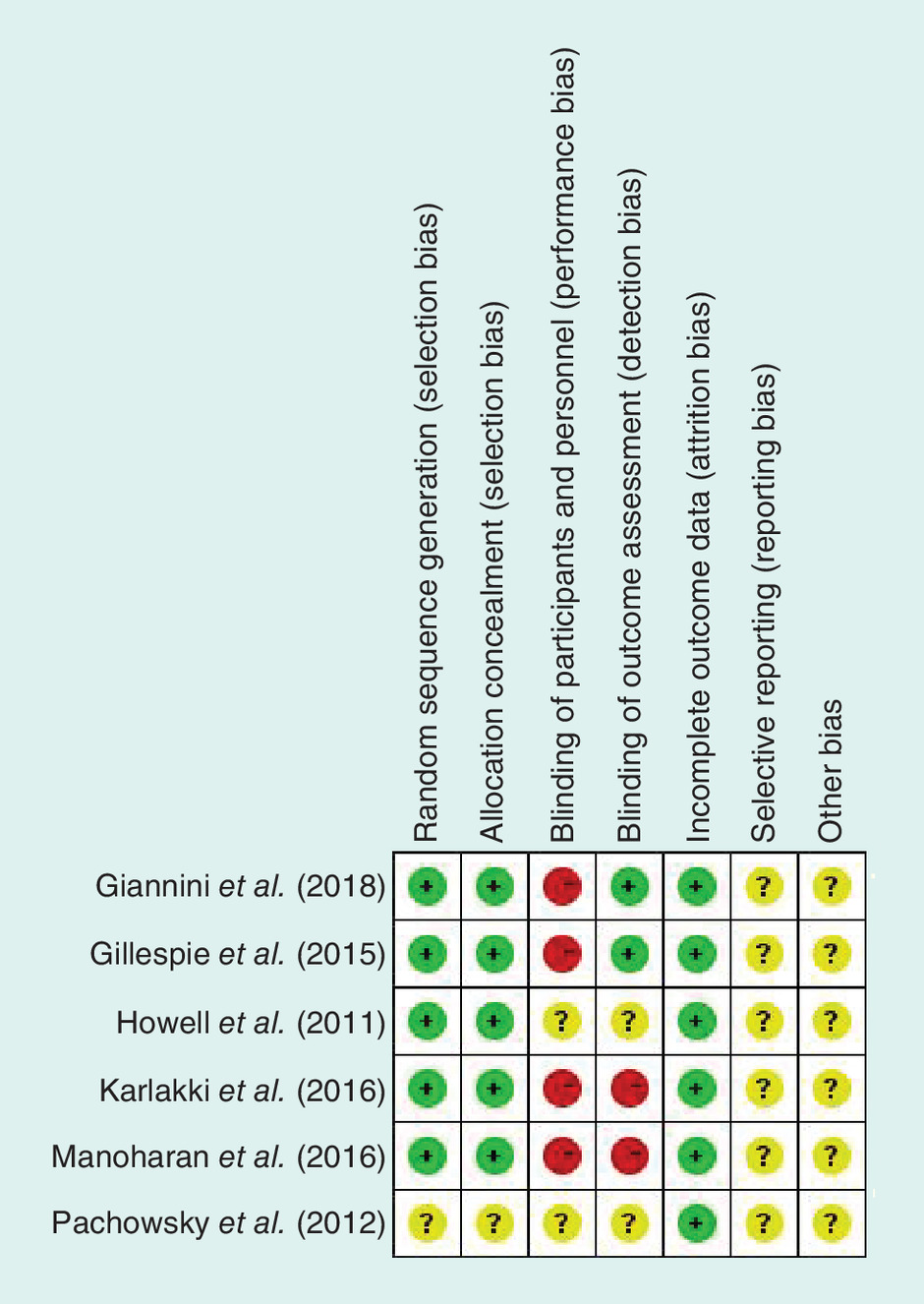
Demographic information of included studies was summarized in Table 1 with statistically similar baseline between both groups. Two studies reported primary TKA [8,15], two studies reported primary THA [9,16] and one study reported primary TKA and THA [17]. Revisions of TKA and THA were performed in one study [12]. The data were pooled only from the randomized part in study by Manoharan et al. [15]. Sample size was from 9 to 107, including 320 cases in NPWT group and 339 patients in control group. Two major devices were applied with variable negative pressure of 80 or 125 mmHg. The duration of negative pressure ranged from 2 to 8 days. Details of the methodological quality of the included RCTs were illustrated in the Figure 2.
| Study | Year | Country | Type (primary or revision) | Device | Age (year) | Sample | Follow | ||
|---|---|---|---|---|---|---|---|---|---|
| NPWT | Control | NPWT | Control | ||||||
| Howell et al. | 2011 | USA | TKA (primary) | (KCI) 125 mmHg, 2 days | NA | NA | 24 | 36 | 1 year |
| Pachowsky et al. | 2012 | Germany | THA (primary) | (KCI) 125 mmHg, 5 days | 66.2 ± 17.8 | 70.0 ± 11.0 | 9 | 10 | 10 days |
| Gillespie et al. | 2015 | Australia | THA (primary) | (PICO) 80 mmHg, 5 days | 63.8 ± 14.0 | 62.5 ± 12.4 | 35 | 35 | 6 weeks |
| Karlakki et al. | 2016 | UK | THA and TKA (primary) | (PICO) 80 mmHg, 7 days | 69.0 ± 9.0 | 69.2 ± 9.0 | 102 | 107 | 6 weeks |
| Manoharan et al. | 2016 | Australia | TKA (primary) | (KCI) 125 mmHg, 8 days | NA | NA | 21 | 21 | NA |
| Newma et al. | 2018 | USA | THA and TKA (revision) | (KCI) 125 mmHg, 2 days | 65 ± 11 | 65 ± 11 | 79 | 80 | 12 weeks |
| Giannini et al. | 2018 | UK | THA and TKA (revision) | (PICO) 80 mmHg, 7 days | 66.8 ± 11.5 | 66.0 ± 8.9 | 50 | 50 | 7 days |
KCI (Acelity company, TX, USA) and PICO (Smith & Nephew, Hull, UK, UK Prevena™ Incision Management System) were two kinds of negative pressure device.
NA: Not available; NPWT: Negative pressure wound therapy; THA: Total hip arthroplasty; TKA: Total knee arthroplasty.
Outcomes of meta-analysis
SSI was reported in three studies including deep incision infection in one study [8] and superficial infection in other two studies [16,17]. The organ or space infection was not counted in this study according to the function of NWPT on surgical incision. The incidence of total infection in NPWT group was 1.86% (3/161) while 6.18% (11/178) in control group. There was no significant difference between two groups in total infection (OR: 0.29; 95% CI: 0.08–1.05; p = 0.06) while less superficial infection in NPWT group (OR: 0.19; 95% CI: 0.04–0.90; p = 0.04). The deep incision infection was similar for NPWT group (1/24) and control group (1/36) in the only one study.
Wound complications were reported in five studies. According to the number of patients who experienced wound complications, there were no significant difference between two groups (OR: 1.18; 95% CI: 0.21–6.60; p = 0.85). However, significant heterogeneity existed (I2 = 85% and p < 0.05). First, sensitivity analysis was performed by excluding the study involving revision arthroplasty and no significant difference was found between two groups (OR: 1.76; 95% CI: 0.25–12.26; p = 0.57; I2 = 80%; p < 0.05). Further subgroup analysis according to primary TKA or THA did not confirmed no significant difference of wound complications between NPWT and control group with significant heterogeneity in THA subgroup (OR: 0.40; 95% CI: 0.03–5.85; p = 0.50; I2 = 80%; p < 0.05) or TKA subgroup (OR: 1.96; 95% CI: 0.12–32.45; p = 0.64; I2 = 85%; p < 0.05, Figure 3). Analysis based on number of total wound complications showed similar results in both groups. Because blister or seroma was a major or the only wound complication in some studies, meta-analysis showed more blisters in NPWT group following TKA (OR: 14.77; 95% CI: 4.45–48.97, p < 0.05; I2 = 0%; p = 0.60) while similar incidence for THA subgroup (OR: 0.85; 95% CI: 0.08–8.76; p = 0.89; I2 = 63%, p = 0.07; Figure 4). The trends of all these outcomes were not changed significantly after excluding the data from study by Howell et al., in which an older device was used.
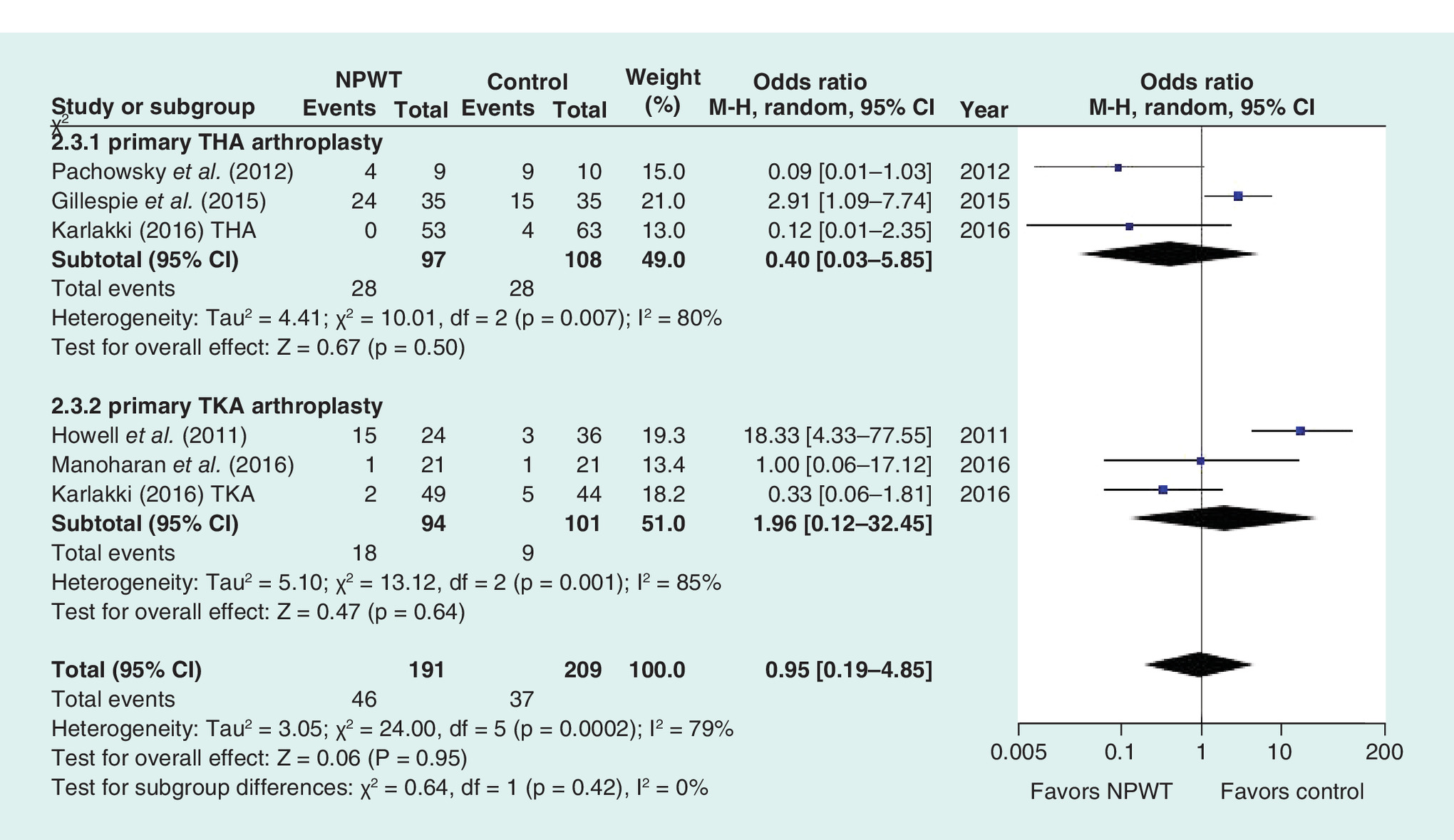
Figure 3. Forest plot showing total wound complications.
M-H: Mantel-Haenszel; NPWT: Negative pressure wound therapy; THA: Total hip arthroplasty; TKA: Total knee arthroplasty.
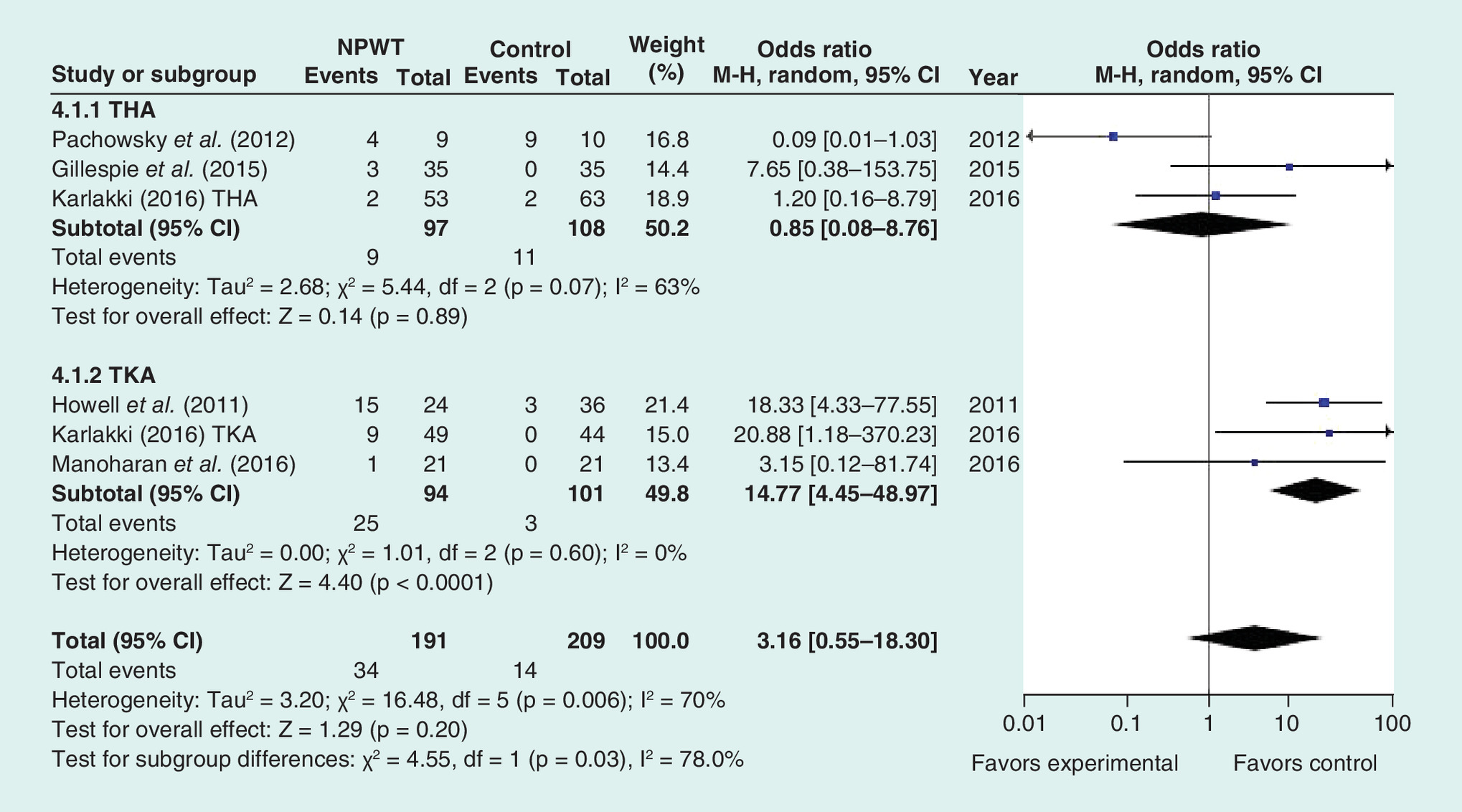
Figure 4. Forest plot showing wound blister.
M-H: Mantel-Haenszel; NPWT: Negative pressure wound therapy; THA: Total hip arthroplasty; TKA: Total knee arthroplasty.
Re-operations were reported in two studies. Howell et al. showed one deep SSI in each group and both patients needed re-surgery for irrigation, debridement and polyethylene liner exchange [8]. One patient in control group in the study by Manoharan et al. was provided an extra negative therapy because of persistent wound drainage [15]. Limited by primary surgery or revision, we did not pool these data together.
Discussion
Due to the promising pain relief and improvement of function of hip or knee joints, THAs and TKAs continue to increase rapidly across the worldwide. Wound problems will cause huge economic cost and impact patient’s quality of life. It is reported that more than 70% patients with wound complications were subsequently developed joint infections for THA or TKA [18]. The negative pressure therapy, which had perfect results in dealing open or chronic wound, was extended to arthroplasty [19]. The prophylactic use of NPWT after arthroplasty got support from several studies for patients who are at high risk for postoperative wound drainage [20].
Present meta-analysis pooled the results from RCTs and found that overall incidence of infection in NPWT group was 1.86% (3/161), which was less than that of 6.18% (11/178) in control group. Further analysis showed that NPWT only decreased the incidence of superficial SSI. Although the statistical p-value for deep infection was 0.06 while 0.04 for superficial site infection, we cannot draw a definitive conclusion because only three studies reported infection for TKA or THA, which weakened the confirming effect of NPWT on reducing infection. Besides, complexed comorbidities such as diabetes, obesity or smoking may influence the incidence of infection following THA or TKA [21,22]. Giannini et al. used the ASEPSIS score to quantitatively evaluate the severity of wound infection and found significantly higher ASEPSIS score of 10.5 in control group with more comorbidities than that of 5.4 in NPWT group [12]. Limited data of comorbidities could not be extracted for meta-analysis.
Except for definitive SSI, other wound complications were also reported in included studies. Present meta-analysis showed that NPWT do not decrease total complications in THA or TKA. Blisters were reported as the sole problems in some studies [8,9,12], and Howell did not suggest NPWT routine application in postoperative wound after primary TKA [8]. Friction of the negative dressing on intact skin was deemed as a reason for line blister formation. More comfortable devices have been designed and applied in knee arthroplasty after the one in study by Howell et al. Our results confirmed that more blisters were noticed in patients with NPWT following TKA while no difference following THA. Excluding the data from study by Howell did not change the situation. Relatively less soft tissue coverage of the knee than hip may lead to more blisters appeared following TKA. Besides, uncorrected procedure maybe another reason for more blisters [17].
Wound complications and related re-operations increase medical cost and length of hospitalization. Cooper et al. [23] and Newman et al. [11] showed lower re-operation rate in patients with NPWT. However, patients in their studies were following hip or knee revisions arthroplasty. And periprosthetic joint infection was one reason for revision in Newman’s study. Two included studies reported the patients received subsequent re-operation. Howell et al. stated that irrigation, debridement and polyethylene liner exchange were reported for one patient in each group [8]. One patient in control group was provided an NPWT because of persistent wound drainage in the other study [15]. More studies are needed to further assess the effect of NPWT on re-operation.
Several potential limitations should be noted: only six RCTs were included, all of which had a relatively small sample size; methodological weaknesses exist in studies, the performance bias existed in four studies while detection bias in two studies; some outcome parameters were not fully described so that we failed to perform a meta-analysis; different duration of NPWT may bring some bias.
Conclusion
NPWT decreases the incidence of superficial SSI. More blisters were noticed on patients with NPWT after TKA. More high-quality RCTs are required due to the limited quality and data of the evidence currently available.
•
Total hip and knee arthroplasties (THA and TKA, respectively) are effective procedures to treat advanced stages of knee and hip osteoarthritis. Wound complications, especially the surgical site infection, are substantial problems.
•
Negative pressure wound therapy (NPWT) induces macro and micro deformation, improving wound healing. Besides that, NPWT decreases the accumulation of hematoma and seroma, producing a dryer wound and with less chance of healing complication and infection.
•
Recently, several published studies have reported on the oral application of NPWT in THA and TKA.
•
A meta-analysis was conducted to evaluate the efficiency and safety of NPWT in THA and TKA from randomized controlled trials.
•
PubMed, Cochrane CENTRAL, ScienceDirect and Embase searches (January 1966–November 2018) yielded 129 results; 6 studies were included for review.
•
Meta-analyses were conducted using a fixed-effects or random model that reported odds ratio or mean differences and 95% credible intervals.
•
More superficial surgical site infection and blisters were found in patients with TKA. There were no significant differences between two groups in total infection and total complications.
•
NPWT decreased the incidence of superficial surgical site infection. More blisters were noticed in patients with NPWT after TKA.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
References
1.
Ridgeway S, Wilson J, Charlet A, Kafatos G, Pearson A, Coello R. Infection of the surgical site after arthroplasty of the hip. J. Bone Joint Surg. Br. 87(6), 844–850 (2005).
2.
Andersson AE, Bergh I, Karlsson J, Nilsson K. Patients’ experiences of acquiring a deep surgical site infection: an interview study. Am. J. Infect. Control 38(9), 711–717 (2010).
3.
Puhto T, Puhto AP, Vielma M, Syrjala H. Infection triples the cost of a primary joint arthroplasty. Infect. Dis. (Lond.) 51(5), 348–355 (2019).
4.
Manrique J, Alijanipour P, Heller S, Dove M, Parvizi J. Increased risk of heterotopic ossification following revision hip arthroplasty for periprosthetic joint infection. Arch. Bone Jt Surg. 6(6), 486–491 (2018).
5.
McAlister IP, Perry KI, Mara KC, Hanssen AD, Berry DJ, Abdel MP. Two-stage revision of total hip arthroplasty for infection is associated with a high rate of dislocation. J. Bone Joint Surg. Am. 101(4), 322–329 (2019).
6.
Lambert KV, Hayes P, McCarthy M. Vacuum assisted closure: a review of development and current applications. Eur. J. Vasc. Endovasc. Surg. 29(3), 219–226 (2005).
7.
Gomoll AH, Lin A, Harris MB. Incisional vacuum-assisted closure therapy. J. Orthop. Trauma 20(10), 705–709 (2006).
8.
Howell RD, Hadley S, Strauss E, Pelham FR. Blister formation with negative pressure dressings after total knee arthroplasty. Curr. Orthop. Pract. 22(2), 176–179 (2011).
9.
Pachowsky M, Gusinde J, Klein A et al. Negative pressure wound therapy to prevent seromas and treat surgical incisions after total hip arthroplasty. Int. Orthop. 36(4), 719–722 (2012).
10.
Matsumoto T, Parekh SG. Use of negative pressure wound therapy on closed surgical incision after total ankle arthroplasty. Foot Ankle Int. 36(7), 787–794 (2015).
11.
Newman JM, Siqueira M, Klika AK, Molloy RM, Barsoum WK, Higuera CA. Use of closed incisional negative pressure wound therapy after revision total hip and knee arthroplasty in patients at high risk for infection: a prospective, randomized clinical trial. J. Arthroplasty 34(3), 554–559 (2019).
12.
Giannini S, Mazzotti A, Luciani D et al. Postoperative wound management with negative pressure wound therapy in knee and hip surgery: a randomised control trial. J. Wound Care 27(8), 520–525 (2018).
13.
Helito CP, Bueno DK, Giglio PN, Bonadio MB, Pecora JR, Demange MK. Negative-pressure wound therapy in the treatment of complex injuries after total knee arthroplasty. Acta Ortop. Bras. 25(2), 85–88 (2017).
14.
Miyahara HS, Serzedello FR, Ejnisman L, Lima A, Vicente J, Helito CP. Incisional negative-pressure wound therapy in revision total hip arthroplasty due to infection. Acta Ortop. Bras. 26(5), 300–304 (2018).
15.
Manoharan V, Grant AL, Harris AC, Hazratwala K, Wilkinson MP, McEwen PJ. Closed incision negative pressure wound therapy vs conventional dry dressings after primary knee arthroplasty: a randomized controlled study. J. Arthroplasty 31(11), 2487–2494 (2016).
16.
Gillespie BM, Rickard CM, Thalib L et al. Use of negative-pressure wound dressings to prevent surgical site complications after primary hip arthroplasty: a pilot RCT. Surg. Innov. 22(5), 488–495 (2015).
17.
Karlakki SL, Hamad AK, Whittall C, Graham NM, Banerjee RD, Kuiper JH. Incisional negative pressure wound therapy dressings (iNPWTd) in routine primary hip and knee arthroplasties: a randomised controlled trial. Bone Joint Res. 5(8), 328–337 (2016).
18.
Carroll K, Dowsey M, Choong P, Peel T. Risk factors for superficial wound complications in hip and knee arthroplasty. Clin. Microbiol. Infect. 20(2), 130–135 (2014).
19.
Karlakki S, Brem M, Giannini S, Khanduja V, Stannard J, Martin R. Negative pressure wound therapy for management of the surgical incision in orthopaedic surgery: a review of evidence and mechanisms for an emerging indication. Bone Joint Res. 2(12), 276–284 (2013).
20.
Siqueira MB, Ramanathan D, Klika AK, Higuera CA, Barsoum WK. Role of negative pressure wound therapy in total hip and knee arthroplasty. World J. Orthop. 7(1), 30–37 (2016).
21.
Song KH, Kim ES, Kim YK et al. Differences in the risk factors for surgical site infection between total hip arthroplasty and total knee arthroplasty in the Korean Nosocomial Infections Surveillance System (KONIS). Infect. Control Hosp. Epidemiol. 33(11), 1086–1093 (2012).
22.
Kopp SL, Berbari EF, Osmon DR et al. The impact of anesthetic management on surgical site infections in patients undergoing total knee or total hip arthroplasty. Anesth. Analg. 121(5), 1215–1221 (2015).
23.
Cooper HJ, Bas MA. Closed-incision negative-pressure therapy versus antimicrobial dressings after revision hip and knee surgery: a comparative study. J. Arthroplasty 31(5), 1047–1052 (2016).
Information & Authors
Information
Published In
Pages: 791 - 797
PubMed: 31397173
Copyright
© 2019 Future Medicine Ltd.
History
Received: 11 January 2019
Accepted: 15 May 2019
Published online: 9 August 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Negative pressure wound therapy in total hip and knee arthroplasty: a meta-analysis. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0009
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Andrew Pieri, Aisling Eves, Robert Thomas, Adam Critchley, Loraine Kalra, Henry Cain, Managing Drainless Mastectomy With Closed Incision Negative Pressure Wound Therapy Using Full-coverage Foam Dressings, Plastic and Reconstructive Surgery - Global Open, 10.1097/GOX.0000000000007056, 13, 11, (e7056), (2025).
- Josep M. Badia, Inés Rubio‐Pérez, Carlos Morales‐Pérez, José Bueno‐Lledó, Laura M. Rodríguez‐Lorenzo, Joan Sancho, Oliver Marín‐Peña, Susana López, Jaume Masià, José M. Balibrea, Closed‐Incision Negative Pressure Therapy: Scoping Review and Multidisciplinary Consensus Recommendations of the Spanish Observatory of Infection in Surgery, International Wound Journal, 10.1111/iwj.70750, 22, 10, (2025).
- Katherine A. Lygrisse, Greg Teo, Vivek Singh, Nishanth Muthusamy, Ran Schwarzkopf, Long William, Comparison of silver-embedded occlusive dressings and negative pressure wound therapy following total joint arthroplasty in high BMI patients: a randomized controlled trial, Archives of Orthopaedic and Trauma Surgery, 10.1007/s00402-022-04530-1, 143, 6, (2989-2995), (2022).
- Kareem G. Elhage, Mohamed E. Awad, Furqan B. Irfan, Joshua Lumbley, Gamal Mostafa, Khaled J. Saleh, Closed‐incision negative pressure therapy at −125 mmHg significantly reduces surgical site complications following total hip and knee arthroplasties: A stratified meta‐analysis of randomized controlled trials , Health Science Reports, 10.1002/hsr2.425, 5, 1, (2022).
- Ronald P. Silverman, John Apostolides, Abhishek Chatterjee, Anthony N. Dardano, Regina M. Fearmonti, Allen Gabriel, Robert T. Grant, Owen N. Johnson, Suresh Koneru, Anna A. Kuang, Andrea A. Moreira, Steven R. Sigalove, The use of closed incision negative pressure therapy for incision and surrounding soft tissue management: Expert panel consensus recommendations, International Wound Journal, 10.1111/iwj.13662, 19, 3, (643-655), (2021).
- Khaled M. Yaghmour, Fahad Siddique Hossain, Sujith Konan, Clinical and Health-Care Cost Analysis of Negative Pressure Dressing in Primary and Revision Total Knee Arthroplasty, Journal of Bone and Joint Surgery, 10.2106/JBJS.20.01254, 103, 6, (541-548), (2020).