A better strategy using barbed sutures for wound closure in total knee arthroplasty
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: The purpose of this study was to conduct a meta-analysis to systematically compare the clinical outcomes between knee barbed sutures (KBS) and knee traditional sutures (KTS) for wound closure in total knee arthroplasty (TKA). Method: This study retrieved potential academic articles comparing the clinical outcomes between KBS and KTS in TKA from the MEDLINE database, the PubMed database, the EMBASE database and the Cochrane Library. The reference articles for the identified studies were carefully reviewed to ensure that all available documents were represented in the study. Results: A total of 14 articles (eight randomized controlled trials [RCTs], six non-RCTs) were involved in our study. The overall participants of barbed Sutures group were 1255, whereas it was 1247 in the traditional sutures. Our meta-analysis showed that KBS is preferable for wound closure of TKA as its shorter lower total cost (weighted mean difference [WMD] = -276.281, 95% CI = -480.281 to -72.280; p = 0.008) and wound closure time (WMD = -4.895,95% CI = -6.105 to -3.685; p < 0.001). However, there was no difference in any complications (p = 0.572), wound complications (p = 0.550), superficial infection (p = 0.918), deep infection (p = 0.654), wound dehiscence (p = 0.649), suture abscess (p = 0.939), arthrofibrosis (p = 0.970), needle sticks (p = 0.158), suture breakage (p = 0.371) and knee society scores (KSS; p = 0.073). Conclusion: The use of KBS in TKA is associated with significantly shortened wound closure times and total closure cost without increased risk of intraoperative needle sticks and suture breakage and postoperative incision complications. Given the relevant possible biases in our study, adequately powered and more RCTs with long-term follow-up are needed to compare the efficacy and safety between KBS and KTS.
The dynamic state of the healthcare system and new healthcare policies, with medical technology as well as the aging population, have focused on the increasing numbers of knee arthroplasties (KA) [1]. The rate of KA has increased from 3.2 to 5.1 per 10,000 people [2]. The tremendous increase in the number of KA requires the reduction of complications, the shortened operation time and the improved postoperative function [3]. Suture type has been deemed to be a time consuming and a considerable part of the surgery [4]. In addition, the quality of sutures is crucial to withstand forces during the early exercise of the knee joint [5]. Recently, barbed suturing that are bidirectional in nature, has been introduced for edges of soft tissue wounds in gynecologic and plastic surgical fields due to its multiple advantages including shorter closure time, less material used, improved watertight closure and less infection-related complications [6–9]. However, the evaluation of overall primary outcomes in knee arthroplasty reconstruction conducted by Campbell et al. [10] showed that a higher superficial infection rate using barbed sutures (3.2 vs 11.8 %; p = 0.001). Gililland et al. [11] retrospectively compared two closure techniques in primary total knee arthroplasty (TKA) and found the similar time, cost and closure-related problem rate between the barbed and conventional group. In brief, various studies have shown mixed results [12,13]. Although, previous studies have been performed to explicit the safety and efficiency of the barbed suturing, the conclusion still remains unclear [14–17]. Therefore, the quantitative meta-analysis was examined to certify whether there is a difference in benefits with barbed suture and conventional sutures in TKA.
Materials & methods
PRISMA [18], the abbreviation for Preferred Reporting Items for Systematic Reviews and Meta-Analyses, was used as the guidelines.
Data sources & searches
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) was used to conduct our study. We sought to systematically and comprehensively retrieve all studies comparing the outcomes of knee barbed sutures (KBS) versus knee traditional sutures (KTS) in TKA through EMBASE, PubMed, MEDLINE and the Cochrane Library of Controlled Trial from the date of barbed suture was first used to close wound in operation by McKenzie in 1967 [19] to December 20, 2018. Since Complex search strategies were performed by using ‘barbed’ or ‘knotless’ or ‘quill’ and ‘total knee arthroplasty’ or ‘total joint arthroplasty’ or ‘total knee replacement’ or ‘total joint replacement’ as our search terms and keywords. All references for identified reports (including original studies, review papers, systematic reviews and meta-analyses) were checked to search for trials that were not included in our electronic search.
Inclusion & exclusion criteria
Studies were included if they met the following preplanned criteria in accordance with PICOS: population: limited to the TKA population; intervention: used strictly KBS; comparison: using KBS and KTS in the TKA; outcome measures: one or more of the intraoperative or following outcomes were reported: the total cost for suture, the total time of closure and operation, KSS (Knee Society Score), the number of any complications, wound complications, superficial infection, deep infection, wound dehiscence, suture abscess, arthrofibrosis and needle sticks, and suture breakage; an official published full-text English-written randomized controlled trials (RCTs) or non-RCTs. The exclusion criteria were as follows: conference or commentary articles and letter to the editor; observational studies and animal trials; unclear patient characteristics and outcome data; case reports and case series; non-English language publications.
Data extraction
Preplanned data elements were extracted independently by two observers, WQX and YZ, including basic data (author, publication time, age), study characteristics (trial type, postoperative follow-up time) and outcomes (the total cost for suture, the total time of closure and operation, KSS, the number of any complications, wound complications, superficial infection, deep infection, wound dehiscence, suture abscess, arthrofibrosis and needle sticks, suture breakage) in a tabular format and in a standardized form. The third investigator (X.Y.Y.) reviewed the data for accuracy and completeness, and he was simultaneously responsible for verifying and contacting authors in the event that data were incomplete or disagreement occurred in the process of data extraction.
Statistical analysis
Comparison of the outcomes of KBS versus KTS in TKA was analyzed by using standard software (Stata version 12.0 statistical software; Stata Corp LP, TX, USA). When I2 >50%, the data were considered with obvious heterogeneity, therefore, a meta-analysis was conducted using a random effects model according to the Cochrane Handbook for Systematic Reviews of Interventions (version 5.1.0). Otherwise, the fixed effect model was performed. p < 0.05 was considered statistically significant between the two groups. For categorical variable outcomes (any complications, wound complications, superficial infection, deep infection, wound dehiscence, suture abscess, arthrofibrosis, needle sticks and suture breakage), a risk difference (RD) or relative ratio (RR) with 95% confidence interval (CIs) was calculated for the assessment. The results of the continuous outcomes (the total cost for suture, KSS and the total time of closure) were expressed as the mean difference (MD) with 95% CIs.
Results
Search results & study characteristics
Initially, 113 articles were identified by searching electronic databases and other sources, then 44 articles were removed by preliminary screening and duplicate article detection. Finally, 14 articles satisfied the inclusion and exclusion criteria for this research. Full texts and references were carefully read. Other details are shown in the flow chart (Figure 1).

Quality assessment & risk of bias assessment
The literature quality evaluation was conducted separately by two reviewers. The study scores of all non-RCTs assessed by the methodological index for nonrandomized studies (MINORS) are shown in Table 1. The quality and applicability of each RCT included in our study were evaluated by using Cochrane’s Collaboration’s tool [20], Figure 2A and B contain more details of the quality assessment for RCTs.
| Quality assessment for nonrandomized trials | Eickmann et al. (2010) | Gililland et al. (2012) | Patel et al. (2012) | Campbell et al. (2014) | Maheshwari et al. (2014) | Zhang et al. (2016) |
|---|---|---|---|---|---|---|
| A clearly stated aim | 2 | 2 | 2 | 2 | 2 | 2 |
| Inclusion of consecutive patients | 2 | 2 | 2 | 2 | 2 | 2 |
| Prospective data collection | 0 | 0 | 0 | 2 | 0 | 0 |
| Endpoints appropriate to the aim of the study | 2 | 2 | 2 | 2 | 2 | 2 |
| Unbiased assessment of the study endpoint | 2 | 2 | 2 | 2 | 2 | 2 |
| A follow-up period appropriate to the aims of study | 2 | 2 | 2 | 2 | 2 | 2 |
| Less than 5% loss to follow-up | 2 | 2 | 2 | 2 | 2 | 2 |
| Prospective calculation of the sample size | 0 | 0 | 0 | 0 | 0 | 0 |
| An adequate control group | 2 | 2 | 2 | 2 | 2 | 2 |
| Contemporary groups | 2 | 2 | 2 | 2 | 2 | 2 |
| Baseline equivalence of groups | 2 | 2 | 2 | 2 | 2 | 2 |
| Adequate statistical analysis | 2 | 2 | 2 | 2 | 2 | 2 |
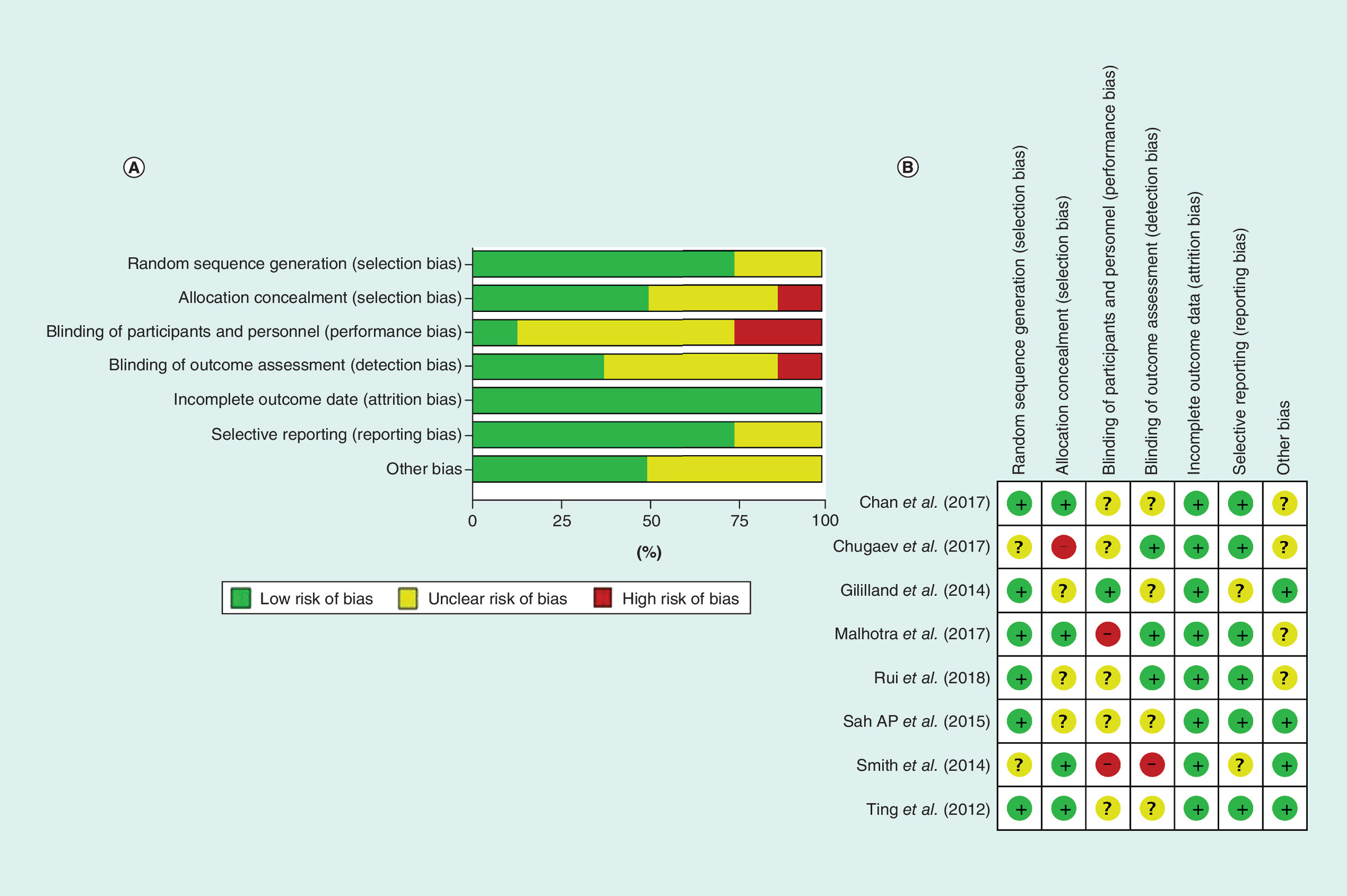
Figure 2. Quality assessment of randomized trials.
(A) A risk of bias graph for randomized controlled trials. (B) A risk of bias summary for randomized controlled trials.
Study & patient characteristics
A total of 14 articles (eight RCTs [21–28] and six non-RCTs [29–34]) published between 2010 and 2018 were included in the analysis and involved 2464 patients (1255 were treated with KBS and 1247 with KTS). Among them, Smith et al. [26] conduct a study included an RCT and a retrospective study. The patients with simultaneous bilateral total knee replacement were included in two studies (Rui et al. [35] and Sah et al. [25]) that KTS was used on one side and KBS were used on the other side. The demographic characteristics and details of the method of placement and suture type for a knee replacement of the two groups are summarized as shown in Tables 2 & 3, respectively. Table 4 refers to the details of inclusion criteria and exclusion criteria of placement for knee arthroplasty.
| Study | Year | Design | Country | Follow-up | Sample (N) | Age (mean) | Gender ratio (M/F) | BMI | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| BC | TC | BC | TC | BC | TC | BC | TC | |||||
| Eickmann et al. (2010) | 2010 | RCS | America | 3 m | 90 | 88 | 67.6y | 68 | 32/54 | 23/56 | NA | NA |
| Gililland et al. (2012) | 2012 | RCS | America | 1.5 m | 98 | 85 | 61 | 63 | 32/66 | 30/55 | 32 | 33 |
| Patel et al. (2012) | 2012 | RCS | America | NA | 23 | 130 | NA | NA | NA | NA | NA | NA |
| Ting et al. (2012) | 2012 | RCT | America | 3 m | 17 | 18 | 64 | 63 | NA | NA | 32 | 32 |
| Campbell et al. (2014) | 2014 | n-RCT | America | 12 m | 169 | 247 | 65.3 | 67.6 | 37/132 | 68/185 | NA | NA |
| Gililland et al. (2014) | 2014 | RCT | America | 1.5 m | 191 | 203 | 64 | 63 | 77/144 | 77/126 | 33 | 33 |
| Maheshwari et al. (2014) | 2014 | RCS | America | 6 m | 115 | 75 | 65 | 61 | 22/93 | 16/59 | 34 | 34 |
| Smith et al. (2014) | 2014 | RCT | America | NA | 10 | 8 | 59.2 | 70.6 | 5/5 | 3/5 | 33.7 | 30.1 |
| Sah AP et al. (2015) | 2015 | RCT | America | 12 m | 50 | 50 | 68 | 68 | 21/29 | 21/29 | 30 | 30 |
| Zhang et al. (2016) | 2016 | RCT | China | 3 m | 68 | 48 | 65.3 | 64.4 | 10/58 | 7/41 | NA | NA |
| Chugaev et al. (2017) | 2017 | RCT | Russian | 3 m | 200 | 102 | NA | NA | NA | NA | NA | NA |
| Chan et al. (2017) | 2017 | RCT | China | 3 m | 55 | 54 | 70.5 | 70.4 | 9/46 | 7/47 | 26.8 | 26.5 |
| Malhotra et al. (2017) | 2017 | RCT | India | 12 m | 80 | 90 | 63.1 | 60 | 21/59 | 20/70 | NA | NA |
| Rui et al. (2018) | 2018 | RCT | China | 1 m | 38 | 38 | 60.11 | 60.11 | 8/30 | 8/30 | 26.76 | 26.76 |
BC: Barbed closure; BMI (kg/m2): Body mass index (kg/m2); m: Month or months; N: Total number of observations; NA: Not mentioned; n-RCT: Nonrandomized prospective study; RCS: Retrospective study; RCT: Randomized controlled trial; TC: Traditional closure; y: Year or years.
| Suture type | Barbed closure | Traditional closure | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Study | Year | Fascia | Subcutaneous | Subcuticular | Skin | Fascia | Subcutaneous | Subcuticular | Skin |
| Eickmann et al. | 2010 | Running#2Quill | Running #2Quill | Running#2Quill | Tissue adhesive | Interrupted1-0Vicryl | Interrupted1-0Vicryl | Interrupted1-0Vicryl | Tissue adhesive |
| Gililland et al. | 2012 | Running#2 Quill | Running #2 Quill | Running#2Quill | Staples | Interrupted#1Ethibond | Interrupted2-0 Monocryl | Interrupted2-0Monocryl | Staples |
| Patel et al. | 2012 | Interrupted1-0Vicryl | Running3.0V-Loc | Running3.0V-Loc | Staples | Interrupted 1-0 Vicryl | Interrupted 2-0 Vicryl | Interrupted 3.0 Biosyn | Staples |
| Ting et al. | 2012 | Running #2Quill | Running #2Quill | Running #2Quill | Tissue adhesive | Interrupted 1-0 Vicryl | Interrupted 2.0 Vicryl | Interrupted2-0Monocryl | Adhesive |
| Campbell et al. | 2014 | Interrupted #1 Maxon | Running2.0V-Loc | Unclear | Running3.0V-Loc | Interrupted #1 Maxon | Interrupted 2.0 Vicryl | Unclear | Staples |
| Gililland et al. | 2014 | Running #2 Quill | Running #2 Quill | Running #2 Quill | Staples | Interrupted#1Ethibond | Interrupted2-0Monocryl | Interrupted2-0Monocryl | Staples |
| Maheshwari et al. | 2014 | Running 2# Quill | Running 0# Quill | Unclear | Staples | Interrupted#1Ethibond | Interrupted 0-Vicryl | Unclear | Interrupted3-0Ethicon |
| Smith et al. | 2014 | Running #2 Quill | Running #2 Quill | Running #2 Quill | Unclear | Interrupted#1Ethibond | Interrupted 2.0 Vicryl | Running 3-0 Monocryl | Unclear |
| Sah AP et al. | 2015 | Running 2-0 Quill | Running 2-0 Quill | Running 2-0 Quill | Unclear | Interrupted 2-0 Vicryl | Running 2-0 Monocryl | Running 3-0 Monocryl | Unclear |
| Zhang et al. | 2016 | Running 2-0 Quill | Vicryl | Vicryl | Staples | Vicryl | Vicryl | Vicryl | Staples |
| Chugaev et al. | 2017 | Running 2-0 Quill | Running 2-0 Quill | Running 2-0 Quill | Staples | Interrupted 2-0 Vicryl | Unclear | Unclear | Staples |
| Chan et al. | 2017 | Interrupted #1 Maxon | Running 0# Quill | Running 0# Quill | Unclear | Interrupted 1-0 Vicryl | Interrupted#2Ethibond | Interrupted#2Ethibond | Unclear |
| Malhotra et al. | 2017 | Running 2-0 Quill | Interrupted 2.0 Vicryl | Interrupted 2.0 Vicryl | Unclear | interrupted #1 vicryl interrupted #5 ethibond | Interrupted 2.0 Vicryl | Interrupted 2.0 Vicryl | Interrupted 2.0 Vicryl |
| Rui et al. | 2018 | Running 2-0 Quill | interrupted #2-0 Vicryl | interrupted #2-0 Vicryl | Staples | interrupted #1 vicryl | Interrupted 2.0 Vicryl | Interrupted 2.0 Vicryl | Staples |
Note: V-Loc and Quill are the absorbable barbed materials for suture.
| Study | Design | The total knee arthroplasty | |
|---|---|---|---|
| Inclusion criteria | Exclusion criteria | ||
| Eickmann et al. (2010) | RCS | 1. The patients who performed the total knee arthroplasty with barbed or traditional closure | 1. Cases with secondary procedures (hardware removal, knee scope on the contralateral knee); 2. Revisions; 3. Unicondylar arthroplasties; 4. Cementless total knees |
| Gililland et al. (2012) | RCS | 1. The patients who performed the total knee arthroplasty with barbed or traditional closure | Unclear |
| Patel et al. (2012) | RCS | 1. The patients who performed the total knee arthroplasty with barbed or traditional closure | 1. All cases other than joint reconstruction cases like revision; 2. Different preoperative diagnosis, patient demographics, patient age |
| Campbell et al. (2014) | RCS | 1. The patients who performed the total knee arthroplasty with barbed or traditional closure aged >18 years; 2. Partial and total knee arthroplasties have similar infection rates and can be compared | 1. Revision knee arthroplasty; 2. Previous incision on the operated knee; 3.History of chronic dementia (b20/30 MMSE) |
| Maheshwari et al. (2014) | RCS | 1. The patients who performed the total knee arthroplasty with barbed or traditional closure | Unclear |
| Zhang et al. (2016) | RCS | 1. The patients with knee osteoarthritis who performed the unilateral total knee arthroplasty | Unclear |
| Ting et al. (2012) | RCT | 1. Degenerative arthritis of the hip or knee with a planned unilateral, primary THA or TKA | 1. Local skin conditions such as dermatitis, eczema, or psoriasis; 2. Osteomyelitis or previous intra-articular infection; 3. Inflammatory arthritis; 4. Connective tissue or vascular disorders or diseases that would adversely affect wound healing; 5. Renal insufficiency (dialysis); 6. Steroid dependence; 7. Malnourishment; 8. Metastatic cancer; 9. Other disease processes resulting in an immunocompromised state |
| Gililland et al. (2014) | RCT | 1. The patients who need to undergo a primary TKA; 2. Over 18 years old, 3. English speaking | 1. Prior surgical incision or scar in close proximity of the proposed incision (<2 cm) |
| Smith et al. (2014) | RCT | 1. The patients who need to undergo a primary TKA | 1. Revision arthroplasty |
| Sah AP et al. (2015) | RCT | 1. The patients who need to undergo simultaneous bilateral TKAs | 1. Prior surgical incisions in the area of the planned surgical approach |
| Chugaev et al. (2017) | RCT | 1. Patients with end-stage osteoarthritis requiring primary non-complex TKA | Unclear |
| Chan et al. (2017) | RCT | 1. Patients with osteoarthritis requiring primary TKA | 1. Revision arthroplasty; 2. Prior surgical incision; 3. Underlying dermatological disease affecting the surgical site; 4. Those who refused to consent |
| Malhotra et al. (2017) | RCT | 1. Unilateral primary total knee arthroplasty for osteoarthritis of knee where medial para-patellar approach was used | 1. Previous knee surgery; 2. Intra-articular infection; 3. Stiff knee in which V-Y plasty of quadriceps was done; 4. Any medical condition which compromises the wound healing, barring obesity and diabetes to get a realistic sampling |
| Rui et al. (2018) | RCT | 1. The patients who need to undergo simultaneous bilateral TKAs | 1. A prior surgical incision or scar near the proposed incision site; 2. Skin problems around the incision; 3. Due to the different surgical difficulties of the 2 sides, we could not make the difference in the incision length <1 cm; 4. The patient refused to enroll in the study |
RCT: Randomized controlled trial; RCS: Retrospective study; THA: Total hip arthroplasty; TKA: Total knee arthroplasty.
Post-procedural outcomes
Twelve outcomes were assessed with our meta-analysis: the total cost for suture, the total time of closure, KSS, any complications, wound complications, superficial infection, deep infection, wound dehiscence, suture abscess, arthrofibrosis, needle sticks and suture breakage.
The total cost for suture
Five articles mentioned the total cost for suture and data pooled by a random effects model to reveal that there was a significant difference in the total cost for suture between two groups (n = 648, WMD = -276.281, 95% CI = -480.281 to -72.280; p = 0.008, I2 = 98.5%; p < 0.01; Figure 3). The present meta-analysis demonstrates that KBS with a lower cost than KTS in TKA.

Figure 3. Forest plot on the assessment of the total cost for suture.
WMD: Weighted mean mifference.
The total time of closure
Nine articles mentioned the total time of closure and data pooled by a random effects model to reveal that there was a significant difference in the total time for suture between two groups (n = 1209, WMD = -4.895, 95% CI = -6.105 to -3.685; p < 0.001, I2 = 91.5%; p < 0.01; Figure 4). The present meta-analysis demonstrates that KBS with a lower time than KTS in TKA.

Figure 4. Forest plot on the assessment of the total time of closure.
WMD: Weighted mean difference.
Knee society scores
There were three articles mentioned post-operation KSS, no obvious heterogeneity was observed and data pooled by a fixed model was used to show that TBS with a higher KSS than KTS in TKA (n = 603, WMD = -1.634, 95% CI = -3.421 to -0.153; p = 0.073, I2 = 24.3%; p > 0.05, Figure 5).

Figure 5. Forest plot on the assessment of knee society scores.
WMD: Weighted mean difference.
Any complications & wound complications
Patients in both groups showed similar rates of any complications (KBS: n = 18/432; KTS: n = 32/380; RR = 0.767, 95% CI = 0.307–1.920; p = 0.572; Figure 6) and wound complications (KBS: n = 92/1036; KTS: n = 82/1027; RR = 0.861, 95% CI = 0.528–1.405; p = 0.550; Figure 7).
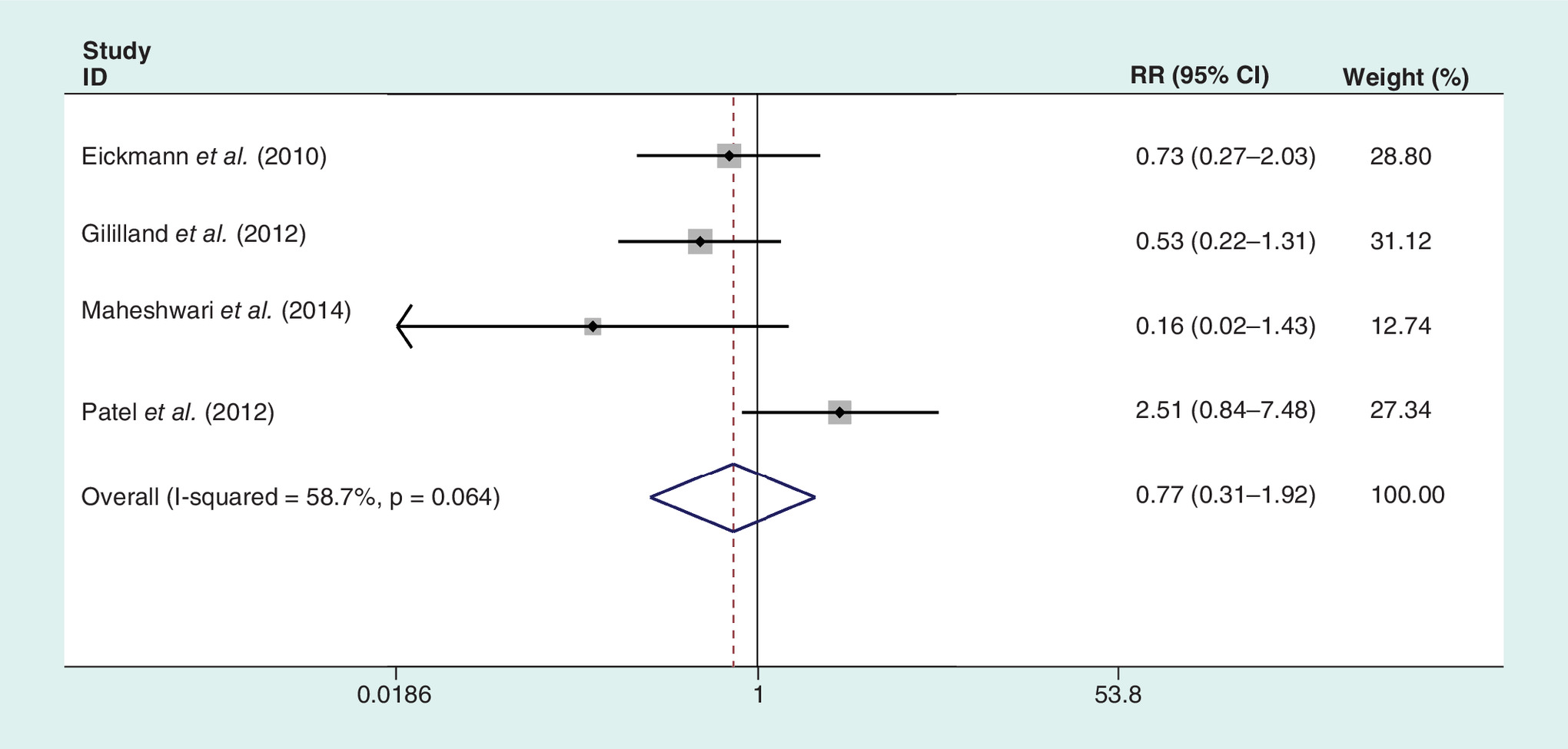
Figure 6. Forest plot on the assessment of any complications.
RR: Relative risk.
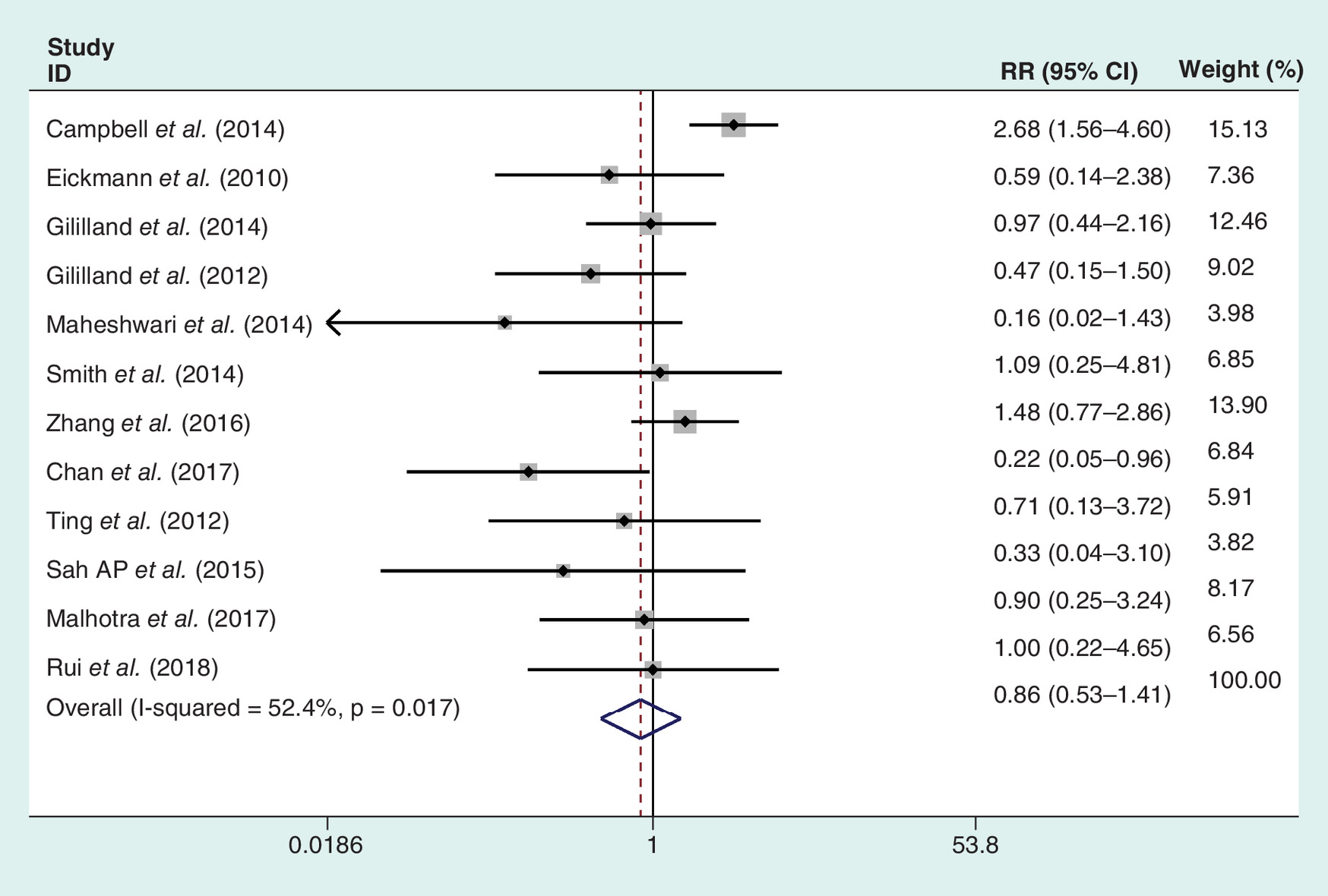
Figure 7. Forest plot on the assessment of wound complications.
RR: Relative risk.
Superficial infection & deep infection
There were eight and five articles containing results of the rates of superficial infection and deep infection in the KBS and KTS groups, respectively. The data were pooled and showed that there were no differences between the two groups in rates of superficial infection (RR = 0.918, 95% CI: 0.414–2.033; p = 0.918; Figure 8) and deep infection (RD = 0.003, 95% CI = -0.011–0.017; p = 0.654; Figure 9).

Figure 8. Forest plot on the assessment of superficial infection.
RR: Relative risk.
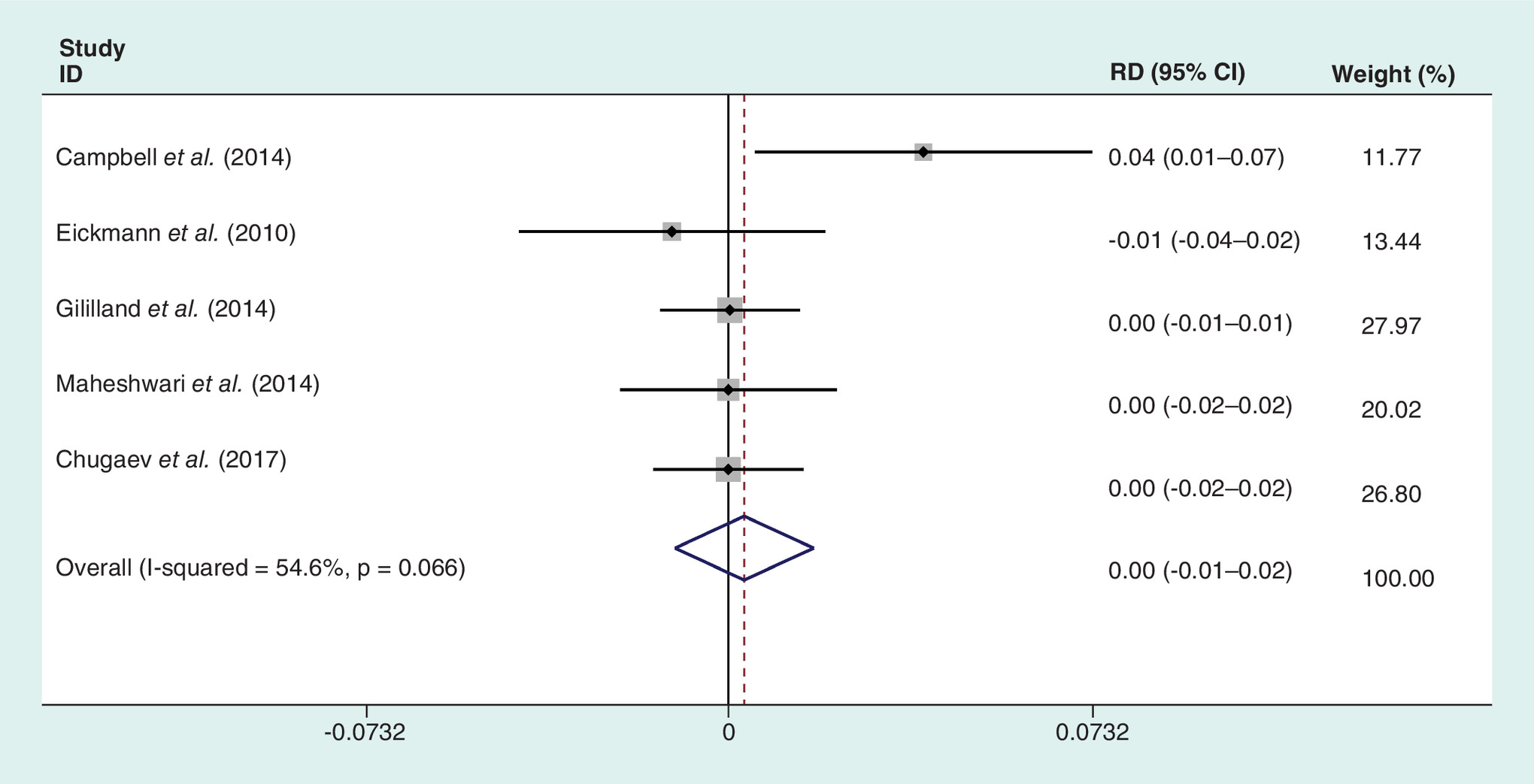
Figure 9. Forest plot on the assessment of deep infection.
RD: Rate difference.
Arthrofibrosis, wound dehiscence & stitch abscess
There were no differences between the two groups in rates of arthrofibrosis (RR = 1.014, 95% CI = 0.486–2.116, I2 = 0.00%; p = 0.970; Figure 10), wound dehiscence (RD = 0.005, 95% CI = -0.016–0.026, I2 = 41.7%; p = 0.649; Figure 11) and stitch abscess (RR = 1.023, 95% CI = 0.568–1.843, I2 = 33.7%; p = 0.939; Figure 12).
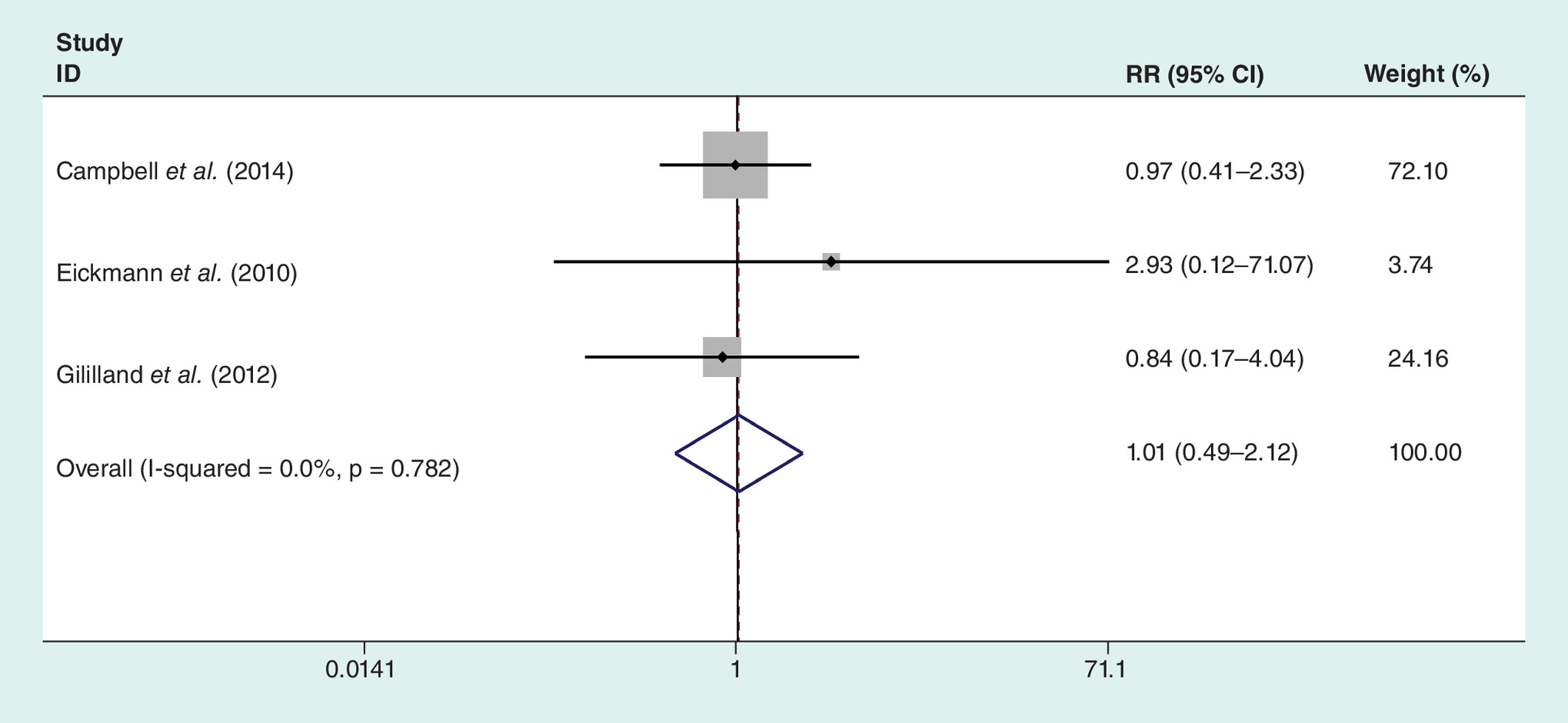
Figure 10. Forest plot on the assessment of arthrofibrosis.
RR: Relative risk.
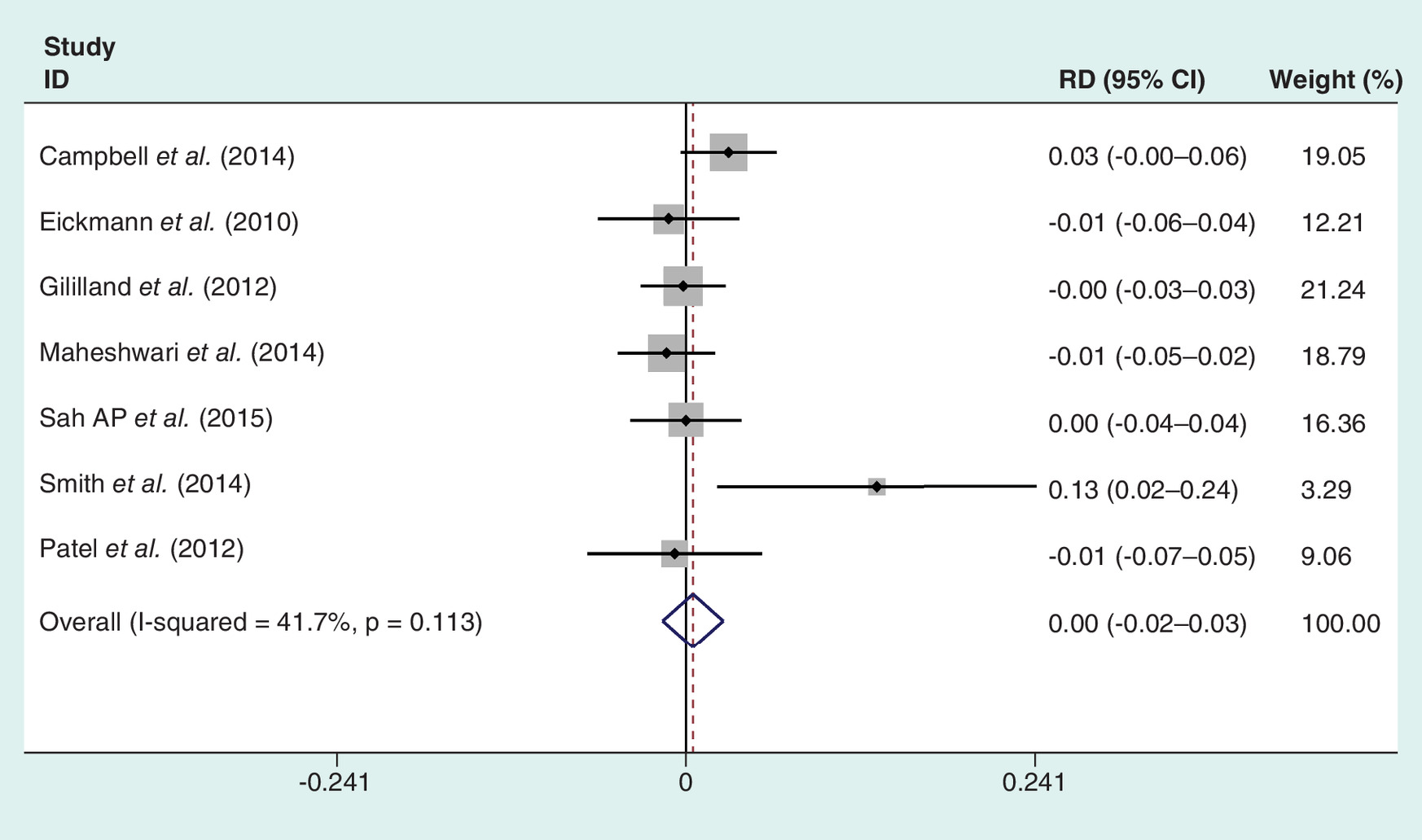
Figure 11. Forest plot on the assessment of wound dehiscence.
RR: Relative risk.

Figure 12. Forest plot on the assessment of stitch abscess.
RR: Relative risk.
Needle sticks & suture breakage
There were only three articles containing the specific results of needle sticks and suture breakage in the two groups. The random effects model showed that no significant difference was found in the result of needle sticks (RD = -0.023, 95% CI = -0.056–0.009, I2 = 55.8%; p = 0.158; Figure 13) and suture breakage between two groups (RD = 4.578, 95% CI = 0.163–128.289, I2 = 75.5%; p = 0.371; Figure 14).

Figure 13. Forest plot on the assessment of needle sticks.
RD: Rate difference.

Figure 14. Forest plot on the assessment of suture breakage.
RR: Relative risk.
Discussion
As the rate of TKA surgery continues to rise, it is particularly important to save cost–effectiveness while decreasing or maintaining current complication rates. Closing wound, which is an important part of arthroplasty, may cost considerable time and is crucial in remedying of wound and prevention of infection. Since KBS was first used to close wound in operation by McKenzie in 1967 [19], it has been adopted for use in many fields of surgical specialties due to be easy and speedy. Some surgeons supported that KBS leads to rapid wound closure and decrease the infection rate [36]. They explained that it can evenly distribute tension on the wound tissue to prevent knot-related ischemia and reduce complications. Nevertheless, there are some different voices emerging in other surgeons. They thought that KBS might lead to add the rate of the infectious complications in wound closure. Wright et al. showed that KBS increased the incidence of the extensor mechanism repair failure versus the traditional sutures [37]. It happens that there is a similar case that Helling et al. reported that suture suspension might gradually fail because of eversion of suture barbs or migration through tissues in barbed suture facial suspension [38]. They thought that eversion rates were higher than those reported in recent literature. So far, the application of KBS in the arthroplasty is still under debate.
Given for the debate related KBS, we performed a meta-analysis. we found that the total cost for suture and the total time of closure of KBS is statistically lower than the KTS. Similar with our findings, Zhang et al. [39] performed a meta-analysis involving nine articles and found that use of KBS in TKA reduces wound closures time and the total wound closure cost, which also corresponds to the results of Borzio et al. [40] and Meena et al. [41] The total cost of wound closure estimates was based upon the hospital cost of suture resource and operating room time. In the study of Stephens et al. [42] demonstrated that KBS was associated with 4 min less for the total time of closure than KTS in TKA, Similar results appeared that KBS could reduce the total time of closure by 40% in the study of Mansour et al. [43] Simultaneously, evaluation of the cost of operating room time was based on the average cost for material required and all of staff. The average cost of the operating room was USD 62/min (ranged from USD 22 to USD 133/min) in most hospitals of the USA [44]. Maheswari et al. [45] found that KBS was associated with a lower total cost for suture than KTS ($66.78 vs $82.59). In studies published in the recently, several reasons for shorter suture time and cost were outlined: barbed sutures could avoid a catastrophic failure of the entire length of the suture by holding the suture by barbs in place, even if one site breaks; barbed sutures is self-anchoring without any knots resulting in shorter suture time; although the materials of barbed closure are more expensive than those for KTS, a lower surgery time leads to a lower total cost; less number of individual sutures were used for closure.
As for other results, we found in KSS between KBS and KTS. Chan et al. [21] and Gililland et al. [36] both demonstrated no difference was found in KSS linked to the KBS group versus KTS. However, the available evidences are insufficient to draw a conclusion that the barbed sutures could have an increasing application in arthroplasty surgery. Further studies are needed to determine the safety and effectiveness of the widespread use of barbed suture in the multilayered closure of arthroplasty. Our study indicates that there is no obvious increase in the rates of the wound complications, which is similar to other studies. Borzio et al. [40] reported no significant higher rate of the wound complications in KBS group than KTS group by performing a meta-analysis. The same results also were given in the studies by Gilliand et al. [30] and Ting et al. [27]. Theoretically, although uneven pressure could appear on soft tissue owing to knots and result in ischemia, meanwhile adsorption of bulky knots may lead to local tissue infection, KBS shows more uniform tissue tension to decrease local ischemia, thereby reducing risk of wound complications. Unfortunately, there are some different viewpoints in recent literature. Campbell et al. held an opinion that barbed sutures had a higher incidence in wound infectious complications because the barbs could create nidi of infection. In addition, the recent articles found an interesting phenomenon that 12.5% barbed sutures breakage during operation. The possible reasons could be explained that: presence of stress riser at the barb, which weakens the suture causing it to break and the learning curve of freshman [23].
Our study also had several limitations. First, the studies included in our research were not all RCTs, including eight RCTs, six non-RCTs which inevitably induced interviewer and recall bias. Second, the fact that individual patient data were not used in our study is one limitation of our meta-analysis. A further limitation is that the eligible studies varied in several aspects, including differences in study populations, basic comorbidities and treatment regimens. More importantly, surgeries classified as KTS and KBS included different methods for wound closure (Table 3), inducing significant heterogeneity in the total wound closure time and the total cost wound closure unavoidable.
Conclusion
The use of KBS in TKA is associated with significantly shortened wound closure times and total closure cost without increased risk of intraoperative needle sticks and suture breakage and postoperative incision complications. Given the relevant possible biases in our study, adequately powered and more RCTs with long-term follow-up are needed to compare the efficacy and safety between KBS and KTS.
•
This study retrieved potential academic articles comparing the clinical outcomes between knee barbed sutures (KBS) and knee traditional sutures (KTS) in total knee arthroplasty (TKA). A total of fourteen articles (eight RCTs, six- non-RCTs) were involved in our study.
•
The overall participants of barbed sutures group were 1255, whereas it was 1247 in the traditional sutures.
•
Our meta-analysis shows that KBS is preferable for wound closure of TKA as its shorter lower total cost (WMD = -276.281,95% CI = -480.281 to -72.280; p = 0.008) and wound closure time (WMD = -4.895,95% CI = -6.105 to -3.685; p < 0.001).
•
However, there was no difference in any complications (p = 0.572), wound complications (p = 0.550), superficial infection (p = 0.918), deep infection (p = 0.654), wound dehiscence (p = 0.649), suture abscess (p = 0.939), arthrofibrosis (p = 0.970), needle sticks (p = 0.158), suture breakage (p = 0.371) and knee society scores (p = 0.073).
Acknowledgments
We would like to show our gratitude to Y Yang, a student from Tianjin No.1 High School Grade 11, for helping the edit work. We also appreciate all of the authors included in our studies for obtaining these important yet controversial data.
Author contributions
X-Y Yang reviewed the data and contacted the authors; W-Q Xin and Y Zhao helped with data extraction; W-Q Xin designed the study; J Wu, Y-K Gao and H-Y Wang revised the article; and H Wang revised the manuscript after the first round review.
Financial & competing interests disclosure
Our work was supported by funding from the National Natural Science Foundation of China (no. 81570507, XYY), Project of the Natural Science Foundation of Tianjin City (grant no. 16JCZDJC35700) and Tianjin Science and Technology Projects in Key Areas of Traditional Chinese Medicine (2018001). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
1.
Kurtz SM, Ong KL, Lau E, Bozic KJ. Impact of the economic downturn on total joint replacement demand in the United States: updated projections to 2021. J. Bone Joint Surg. Am. 96(8), 624–630 (2014).
2.
Oleske DM, Bonafede MM, Jick S, Ji M, Hall JA. Electronic health databases for epidemiological research on joint replacements: considerations when making cross-national comparisons. Ann. Epidemiol. 24(9), 660–665 (2014).
3.
Doran JP, Zabinski SJ. Bundled payment initiatives for Medicare and non-Medicare total joint arthroplasty patients at a community hospital: bundles in the real world. J. Arthroplast. 30(3), 353–355 (2015).
4.
Elmallah RK, Khlopas A, Faour M et al. Economic evaluation of different suture closure methods: barbed versus traditional interrupted sutures. Ann. Transl. Med. 5(Suppl. 3), S26 (2017).
5.
Levine BR. CORR Insights([R]): is there an advantage to knotless barbed suture in TKA wound closure? A randomized trial in simultaneous bilateral TKAs. Clin. Orthop. Rel. Res. 473(6), 2028–2030 (2015).
6.
Nett M, Avelar R, Sheehan M, Cushner F. Water-tight knee arthrotomy closure: comparison of a novel single bidirectional barbed self-retaining running suture versus conventional interrupted sutures. J. Knee Surg. 24(1), 55–59 (2011).
7.
Vakil JJ, O’Reilly MP, Sutter EG et al. Knee arthrotomy repair with a continuous barbed suture: a biomechanical study. J. Arthroplast. 26(5), 710–713 (2011).
8.
Einarsson JI, Chavan NR, Suzuki Y et al. Use of bidirectional barbed suture in laparoscopic myomectomy: evaluation of perioperative outcomes, safety, and efficacy. J. Minim. Invasive Gynecol. 18(1), 92–95 (2011).
9.
Einarsson JI, Cohen SL, Gobern JM et al. Barbed versus standard suture: a randomized trial for laparoscopic vaginal cuff closure. J. Minim. Invasive Gynecol. 20(4), 492–498 (2013).
10.
Campbell AL, Patrick Jr DA, Liabaud B, Geller JA. Superficial wound closure complications with barbed sutures following knee arthroplasty. J. Arthroplast. 29(5), 966–969 (2014).
11.
Gililland JM, Anderson LA, Sun G, Erickson JA, Peters CL. Perioperative closure-related complication rates and cost analysis of barbed suture for closure in TKA. Clin. Orthop. Relat. Res. 470(1), 125–129 (2012).
12.
Ferrer-Marquez M, Belda-Lozano R, Soriano-Maldonado A. Use of barbed sutures in bariatric surgery. Review of the literature. Obes. Surg. 26(8), 1964–1969 (2016).
13.
Kaminer MS, Bogart M, Choi C, Wee SA. Long-term efficacy of anchored barbed sutures in the face and neck. Dermatol. Surg. 34(8), 1041–1047 (2008).
14.
Eickmann T, Quane E. Total knee arthroplasty closure with barbed sutures. J. Knee Surg. 23(3), 163–167 (2010).
15.
Stephens S, Politi J, Taylor BC. Evaluation of primary total knee arthroplasty incision closure with the use of continuous bidirectional barbed suture. Surg. Technol. Int. 21, 199–203 (2011).
16.
Patel RM, Cayo M, Patel A, Albarillo M, Puri L. Wound complications in joint arthroplasty: comparing traditional and modern methods of skin closure. Orthopedics 35(5), e641–e646 (2012).
17.
Shermak MA, Mallalieu J, Chang D. Barbed suture impact on wound closure in body contouring surgery. Plast. Reconstr. Surg. 126(5), 1735–1741 (2010).
18.
Yang Y, Zhou Y, Chi Y, Fan B, Chen Z. Characterization of soybean WRKY gene family and identification of soybean WRKY genes that promote resistance to soybean cyst nematode. Sci. Rep. 7(1), 17804 (2017).
19.
McKenzie AR. An experimental multiple barbed suture for the long flexor tendons of the palm and fingers. Preliminary report. J. Bone Joint Surg. Br. 49(3), 440–447 (1967).
20.
Cui L, Han Y, Zhang S, Liu X, Zhang J. Safety of stenting and endarterectomy for asymptomatic carotid artery stenosis: a meta-analysis of randomised controlled trials. Eur. J. Vasc. Endovasc. Surg. 55(5), 614–624 (2018).
21.
Chan VWK, Chan PK, Chiu KY, Yan CH, Ng FY. Does barbed suture lower cost and improve outcome in total knee arthroplasty? a randomized controlled trial. J. Arthroplast. 32(5), 1474–1477 (2017).
22.
Gililland J, Anderson LA, Barney JK, Ross HL, Pelt CE, Peters CL. Barbed versus standard sutures for closure in total knee arthroplasty: a multicenter prospective randomized trial. J. Arthroplast. 29, 135–138 (2014).
23.
Malhotra R, Jain V, Kumar V, Gautam D. Evaluation of running knotless barbed suture for capsular closure in primary total knee arthroplasty for osteoarthritis-a prospective randomized study. Int. Orthop. 41(10), 2061–2066 (2017).
24.
Salvi S, Ravetti JL, Arena G et al. Evaluation of RET gene rearrangement by fluorescence in situ hybridization in malignant mesothelioma. J. Thorac. Oncol. 13(1), e12–e14 (2018).
25.
Sah AP. Is There an advantage to knotless barbed suture in TKA wound closure? A randomized trial in simultaneous bilateral TKAs. Clin. Orthop. Rel. Res. 473(6), 2019–2027 (2015).
26.
Smith EL, DiSegna ST, Shukla PY, Matzkin EG. Barbed versus traditional sutures: closure time, cost, and wound related outcomes in total joint arthroplasty. J. Arthroplast. 29(2), 283–287 (2014).
27.
Ting NT, Moric MM, Della Valle CJ, Levine BR. Use of knotless suture for closure of total hip and knee arthroplasties: a prospective, randomized clinical trial. J. Arthroplast. 27(10), 1783–1788 (2012).
28.
Chugaev DV, Kornilov NN, Lasunskii SA. Bidirectional knotless barbed sutures during primary total knee arthroplasty: effective solution or new problem? Khirurgiia 12, 58–65 (2017).
29.
Eickmann T, Quane E. Total knee arthroplasty closure with barbed sutures. J. Knee Surg. 23(3), 163–167 (2010).
30.
Gililland JM, Anderson LA, Sun G, Erickson JA, Peters CL. Perioperative closure-related complication rates and cost analysis of barbed suture for closure in TKA. Clin. Orthop. Rel. Res. 470(1), 125–129 (2012).
31.
Patel RM, Cayo M, Patel A, Albarillo M, Puri L. Wound complications in joint arthroplasty: comparing traditional and modern methods of skin closure. Orthopedics 35(5), e641–e646 (2012).
32.
Campbell AL, Patrick Jr DA, Liabaud B, Geller JA. Superficial wound closure complications with barbed sutures following knee arthroplasty. J. Arthroplast. 29(5), 966–969 (2014).
33.
Maheshwari AV, Naziri Q, Wong A, Burko I, Mont MA, Rasquinha VJ. Barbed sutures in total knee arthroplasty: are these safe, efficacious, and cost-effective? J. Knee Surg. 28(2), 151–156 (2015).
34.
Zhang Z, Zhou YG, Lin F et al. Case–control study on the biodegradable barbed sutures in total knee arthroplasty. Zhongguo Gu Shang 29(9), 809–813 (2016).
35.
Li R, Ni M, Zhao J et al. A modified strategy using barbed sutures for wound closure in total joint arthroplasty: a prospective, randomized, double-blind, self-controlled clinical trial. Med. Sci. Monit. 24, 8401–8407 (2018).
36.
Gililland JM, Anderson LA, Barney JK, Ross HL, Pelt CE, Peters CL. Barbed versus standard sutures for closure in total knee arthroplasty: a multicenter prospective randomized trial. J. Arthroplasty 29(9 Suppl.), 135–138 (2014).
37.
Wright RC, Gillis CT, Yacoubian SV, Raven RB 3rd, Falkinstein Y, Yacoubian SV. Extensor mechanism repair failure with use of bidirectional barbed suture in total knee arthroplasty. J. Arthroplasty 27(7), 1413, e1411–e1414 (2012).
38.
Helling ER, Okpaku A, Wang PT, Levine RA. Complications of facial suspension sutures. Aesthet. Surg. J. 27(2), 155–161 (2007).
39.
Zhang W, Xue D, Yin H et al. Barbed versus traditional sutures for wound closure in knee arthroplasty: a systematic review and meta-analysis. Sci. Rep. 6, 19764 (2016).
40.
Borzio RW, Pivec R, Kapadia BH, Jauregui JJ, Maheshwari AV. Barbed sutures in total hip and knee arthroplasty: what is the evidence? A meta-analysis. Int. Orthop. 40(2), 225–231 (2016).
41.
Meena S, Gangary S, Sharma P, Chowdhury B. Barbed versus standard sutures in total knee arthroplasty: a meta-analysis. Eur. J. Orthop. Surg. Traumatol. 25(6), 1105–1110 (2015).
42.
Stephens S, Politi J, Taylor BC. Evaluation of primary total knee arthroplasty incision closure with the use of continuous bidirectional barbed suture. Surg. Technol. Int. 21, 199–203 (2011).
43.
Mansour A, Ballard R, Garg S, Baulesh D, Erickson M. The use of barbed sutures during scoliosis fusion wound closure: a quality improvement analysis. J. Pediatr. Orthop. 33(8), 786–790 (2013).
44.
Macario A. What does one minute of operating room time cost? J. Clin. Anesth. 22(4), 233–236 (2010).
45.
Shermak MA, Mallalieu J, Chang D. Barbed suture impact on wound closure in body contouring surgery. Plast. Reconstr. Surg. 126(5), 1735–1741 (2010).
Information & Authors
Information
Published In
Pages: 799 - 814
PubMed: 31359779
Copyright
© 2019 Future Medicine Ltd.
History
Received: 28 January 2019
Accepted: 15 May 2019
Published online: 30 July 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
A better strategy using barbed sutures for wound closure in total knee arthroplasty. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0019
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Changzhi Huang, Canhong Zhang, Shimin Zhang, Nanyi Xu, Lei Zhang, Jiuzao Lin, Xiaoyong Wang, Subcuticular suture achieves better esthetics, healing, and similar functional outcomes following unicompartmental knee arthroplasty: a single center retrospective comparative study, Frontiers in Medicine, 10.3389/fmed.2025.1708256, 12, (2026).
- Changzhi Huang, Nanyi Xu, Shimin Zhang, Jiuzao Lin, Xiaoyong Wang, Clinical outcomes of modified intradermal vs. traditional intermittent suture technique in total knee arthroplasty: a single-center retrospective study, Frontiers in Surgery, 10.3389/fsurg.2025.1655296, 12, (2025).
- Xianlin Gu, Qiong Guo, Qingwen Zhao, Guiyu Jiang, Yanjiao Shen, Youlin Long, Xin Chen, Yifei Lin, Jin Huang, Liang Du, Incidence and outcome characteristics of adverse event in surgery: an assessment based on systematic reviews of barbed suture, BMC Medical Research Methodology, 10.1186/s12874-025-02607-0, 25, 1, (2025).
- Pablo Sanz-Ruiz, José Ramón Caeiro-Rey, Juan Carlos Martínez-Pastor, José Luis Martín-Alguacil, Antonio Murcia-Asensio, Jesús Moreta, Consensus document on the management of wound closure in orthopaedic surgery, EFORT Open Reviews, 10.1530/EOR-24-0002, 10, 2, (82-94), (2025).
- Petra Baumann, Lourdes Hinojosa Sánchez, Núria Grané Garcia, Larisa Sologiuc, Amadeus Hornemann, Assessment of a novel unidirectional mid-term absorbable barbed suture versus a competitor barbed suture for vaginal cuff closure after gynaecology surgery, study protocol of a randomized controlled trial - BARHYSTER, BMC Surgery, 10.1186/s12893-024-02700-z, 25, 1, (2025).
- Mehmet Fevzi Cakmak, Levent Horoz, The Examination of the Benefits of the Usage of Barbed, Knotless Suture in Capsule Repair During Total Knee Arthroplasty: A Prospective, Double-Blind, Randomized Controlled Study, Indian Journal of Orthopaedics, 10.1007/s43465-023-00976-6, 57, 11, (1881-1890), (2023).
- Kelsey A. Rankin, David Gibson, Ran Schwarzkopf, Mary I. O’Connor, Daniel H. Wiznia, Operative Techniques to Reduce Hip and Knee Arthroplasty Complications in Morbidly Obese Patients, Arthroplasty Today, 10.1016/j.artd.2022.07.016, 17, (120-125), (2022).
- Changjiao Sun, Lianxu Chen, Ruiyong Du, Sha Wu, Qi Ma, Xu Cai, Barbed Sutures in Total Knee Arthroplasty: A Meta-analysis of Randomized-Controlled Trials, The Journal of Knee Surgery, 10.1055/s-0040-1710373, 34, 14, (1516-1526), (2020).