To what extent can the chosen blood pressure measurement technique affect the outcomes of an observational survey?
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: We analyzed to what extent measurement protocol influenced individual blood pressure (BP) and achievement of treatment target in patients with coronary heart disease. Methods: In a subsample of Czech EUROASPIRE III–V survey participants (n = 913), we compared the per-protocol BP measurement (by automated oscillometric device OMRON at the beginning of survey procedure) with control auscultatory measurement (by physician during interview). Results: Per-protocol approach produced significantly (p < 0.0001) higher BP values (by 9/6 mmHg in median) than auscultatory measurements and led to markedly higher proportion of patients over target BP (less than 140/90 mmHg; 59.3 vs 34.9% [p < 0.0001], per-protocol vs auscultatory technique, respectively). Conclusion: Per-protocol oscillometric technique was not equivalent to conventional auscultatory measurement and seriously over-rated the real nonachievement of BP target in observational surveys.
Since 1994, a series of cardiovascular prevention Guidelines [1–6] defined treatment targets for appropriate blood pressure (BP) control and regularly updated this recommendation in light of available data from interventional trials. It has been repeatedly reported that control of BP remains unsatisfactory. Indeed, 45–55% of secondary prevention patients exceeded recommended BP targets across EUROASPIRE I–V (1995–2017) [7–10]. These unsatisfactory results somewhat disagree with constantly growing availability or prescription rate of antihypertensive drugs and also with visible improvements in other parts of secondary prevention practice (for example, control of hypercholesterolemia) [7–10]. In the present study, we aimed to investigate whether at least part of these unsatisfactory results cannot be attributed to a chosen protocol of BP measurements in EUROASPIRE surveys.
Individual BP represents rather variable entity and its assessment might be biased by several ways. In EUROASPIRE, an automated oscillometric technique was chosen for BP measurement with an intention to standardize the measurements across study centers and across each EURASPIRE surveys and this decision seems to agree with recommendation for office BP measurement in daily clinical practice – auscultatory and oscillometric measurements can be used for any decision-making if appropriately validated [11]. However, concordance of both techniques has been disputed, even when both measurements were taken simultaneously [12–14]. Moreover, in EUROASPIRE protocol, BP measurement was scheduled generally at the beginning of clinical visit. However for the patient, the survey procedure represents more than less unfamiliar situation, rather different from routine clinical visit. The ‘white coat’ effect could be probably more accented than during usual office BP measurement. In our opinion, the interview with physician, realized as a part of the EUROASPIRE protocol (and similar to usual office visit) represents a chance for patient to have time to calm down.
Thus, main purpose of our study was to compare individual BP values and corresponding achievement of treatment target (prevalence of uncontrolled hypertension) by these two different modalities (i.e., automated oscillometric BP at the beginning of the study visit vs auscultatory measurement during interview) in stable coronary heart disease patients. In a subset of patients, we also tested individual differences in BP control if additional BP registration modalities (professional oscillometric sphygmomanometer and unattended automated oscillometric device) were used.
Methods
All procedures performed in this study were in accordance with the principles of Good Clinical Practice and ethical standards formulated in the 1964 Declaration of Helsinki and its later amendments. The study protocol was approved by the local Ethics Committee of the University Hospital in Pilsen. Written informed consent was obtained from all participants included in the study. Data were stored and evaluated under the provisions of the Czech Data Protection Act and General Data Protection Regulation direction of the European Committee.
Design & study population
The study represents a secondary analysis of EUROASPIRE survey data from the Czech Republic, a cross-sectional analysis of three pooled independent cohorts (EUROASPIRE III, IV and V examined in 2006–2007, 2012–2013 and 2016–2017) of patients with stable manifest coronary heart disease (CHD), in other words, baseline examination was done at least 6 months after its first manifestation. Patients aged less than 80 years and hospitalized for any of the following discharge diagnosis were retrospectively identified from hospital records. The diagnoses included: first coronary artery bypass grafting, first percutaneous transluminal coronary angioplasty and acute myocardial infarction or ischemia. Recruitment of patients started with the most recent hospital record and proceeded backward until the required sample of 600 subjects in each campaign (EUROASPIRE III, IV and V) was achieved. These patients were invited for an interview/clinical examination and responders (77.3% of the initially identified pool of patients) were included in the survey. All three campaigns of the EUROASPIRE survey were conducted in the same two centers in the Czech Republic: University Hospital in Pilsen and Department of Cardiology, Institute for Clinical and Experimental Medicine in Prague under almost identical protocol. Each interview/clinical examination took place 6–24 months after the qualifying index event. For the purpose of present analysis, we used a subsample of 913 subjects (65.6% of total sample). This subsample covers all subjects from EUROASPIRE III plus those who were interviewed in Pilsen center in the course of EUROASPIRE IV and V (serial BP measurements, necessary for this subanalysis was done only in one of both Czech centers of this project).
Data collection
The standard protocol of EUROASPIRE (EA) survey was followed as described elsewhere [9,15]. Information on personal and demographic characteristics, personal and family history of CHD, lifestyle and pharmacotherapy were obtained. Height and weight were measured in light indoor clothes without shoes using SECA 701 scales and measuring stick (SECA, Hamburg, Germany). Waist circumference was measured using a tape measure. Breath carbon monoxide was measured by a SMOKERLYSER device (Bedfont Scientific, Upchurch, UK) to verify smoking status (with 10 ppm of breath carbon monoxide as the cut-off point). Venous blood samples were drawn after at least 12 h of overnight fast. Laboratory examinations included estimation of total and HDL cholesterol, triglycerides (TG) and glucose, and were performed in the central study laboratory of the respective EUROASPIRE survey [9,15]. LDL cholesterol was calculated using the Friedewald equation, in other words, LDL = total cholesterol – HDL – (TG/2.22) (all in mmol/l). Symptoms of depression and/or anxiety was ascertained using standardized self-reported Hospital Anxiety and Depression Scale (HADS) questionnaire (validated Czech version) [16].
BP measurement modalities
In all BP measurement modalities, BP was measured in a sitting position and after at least 10 min rest, the patient should sat with the right arm on the table (the cuff should be in the same horizontal level, as patient's heart), palm facing upward and uncross his/her legs. Standardized adult cuff (16 × 30 cm) was used for patients with arm-circumference 22–32 cm, while an oversized cuff (16 × 36 cm) for those with arm-circumference larger than 32 cm. The cuff was applied to the upper arm so that the bottom edge of the cuff was positioned 1–2 cm above the elbow joint and the center of the bladder was over the brachial artery.
We use five different modalities of BP measurement (Figure 1): First, ‘per-protocol’ measurement was performed according to the defined EUROASPIRE survey methodology, in other words, at the very beginning of survey procedures (namely before taking blood sample) by study nurse. An automated oscillometric device was used (OMRON M5-I in EUROASPIRE III, while OMRON M6 in EUROASPIRE IV and V, OMRON Corp., Kyoto, Japan). BP readings were obtained at least twice with 5 min apart, but if the difference between both values exceeded 10 mmHg, repeated readings were realized (for the purpose of present analysis average of last two readings was used). Second measurement was realized by physician during interview at least 30 min after ‘per-protocol’ measurement. In the second BP measurement, we used auscultatory device (standard mercury sphygmomanometer with 2 mm of mercury precision in EUROASPIRE III and IV or NISSEI DM-3000 electronic sphygmomanometer [NISSEI, Tokyo, Japan] in EUROASPIRE V). The same approach as in ‘per-protocol’ BP measurement regarding number and BP values used for analysis was applied. Additional three BP measurement modalities were realized only in subsets patients. First, in a random subsample (named ‘cohort 2’) we repeated automated oscillometric measurement, similarly as in ‘per-protocol’ measurement and by the same study nurse, but at the end of the survey procedures. Second, in EUROASPIRE V survey we performed another oscillometric measurement using hybrid NISSEI DM-3000 device (which also enable to switch for oscillometric mode) obtained by (the same) physician during an interview (this subsample is marked ‘cohort 3’). Last BP measurement modality (done in ‘cohort 3’ again) represents unattended automated oscillometric (uAO) measurement using BPTru device (model BPM 200, BpTRU Medical Devices, Coquitlam [BC], Canada). It was set to measure BP six-times in 1-min intervals, while the patient had been seated alone in a separate room. The BPM 200 model of BPTru skips the first measurement and calculates the mean of the second to the sixth measurement.

Figure 1. Blood pressure measurement modalities.
*by study nurse; **by physician during interview. All measurements were performed at least twice, after at least 5 min rest with appropriate cuff placed.
BP: Blood pressure.
Data management
BP values were compared intra-individually across all five BP measurement modalities (Figure 1). Descriptive statistics (means, medians and frequencies) and conventional statistical methods (Wilcoxon's paired test and Spearman's correlation) were used. We also tested whether any covariate might influence the intra-individual difference between per-protocol and auscultatory technique, by means of multiple step-wise logistic regression. For this purpose, conventional risk factors were dichotomized using cut-off points proposed by the 5th Joint European Guidelines for Cardiovascular Prevention [5]. Raised BP (failure to achieve BP target values) was defined as systolic BP ≥140 mmHg and/or diastolic BP ≥90 mmHg (irrespective of diabetes). HADS score for depression or anxiety ≥8 points was categorized as respective mood disorder present. Statistical analysis was performed using STATISTICA 8 (StatSoft, Inc., OK, USA) and STATA 8 (STATA Corp LP, TX, USA). The p-values < 0.05 were considered significant.
Results
The study sample consisted of 913 patients (725 males and 188 females) with manifest coronary heart disease, mean age 63.6 (± SD 9.3) years. Baseline parameters are listed in Table 1 (first column, i.e., cohort 1).
| Parameter | Cohort 1¶ | Cohort 2# | Cohort 3†† |
|---|---|---|---|
| n | 913 | 295 | 202 |
| Age (years) | 63.6 (9.3) | 64.7 (9.2) | 64.8 (9.4) |
| Age ≥65 years (%) | 45.8 | 54.2 | 55.0 |
| Gender (% of males) | 79.4 | 81.4 | 81.2 |
| Current smoking (%) | 19.7 | 17.6 | 22.8 |
| Body mass index (kg/m2) | 29.6 (4.7) | 29.7 (4.4) | 30.0 (4.9) |
| Body mass index ≥30 kg/m2 (%) | 41.7 | 44.8 | 44.6 |
| Waist circumference (cm) | 105.0 (12.4) | 107.1 (11.5) | 109.0 (12.9) |
| Increased waist circumference (%)† | 65.5 | 75.6 | 78.7 |
| LDL cholesterol [mmol/l] | 2.44 (0.94) | 2.26 (0.84.6) | 1.91 (0.79) |
| LDL ≥1.8 mmol/l (%) | 78.7 | 68.7 | 46.0 |
| Fasting glucose (mmol/l) | 6.81 (2.42) | 6.68 (2.17) | 6.36 (2.26) |
| Diabetes mellitus (%)‡ | 40.3 | 35.9 | 33.7 |
| Antihypertensive treatment (%) | 96.3 | 98.0 | 93.6 |
| Treatment with betablockers (%) | 85.5 | 83.7 | 77.7 |
| Treatment with ACEi or ARB (%) | 77.0 | 81.0 | 76.2 |
| Anxiety score by HADS (points) | 4.7 (3.6) | 4.8 (3.7) | 4.6 (3.4) |
| Depression score by HADS (points) | 4.9 (3.6) | 4.9 (3.5) | 4.9 (3.3) |
| Anxiety (%)§ | 18.9 | 20.3 | 19.3 |
| depression (%)§ | 22.6 | 23.1 | 21.3 |
The numbers in italic cannot be calculated between columns, since they are overlaps among then (i.e. cohort 2 is a part of cohort 1).
†
≥102 in males or ≥88 in females.
‡
Fasting glycaemia ≥7 mmol/l and/or antidiabetic treatment.
§
≥8 points by relevant HADS score.
¶
Total sample (all patients had ‘per-protocol’ oscillometric and auscultatory blood pressure measurement.
#
Subample of patients measured repeatedly (at the end of survey visit with automated oscillometric device (similarly as per-protocol measurement).
††
Subsample of patients measured repeatedly with another automated oscillometric devices (NISSEI DM-3000 and BPTru BPM 200).
ACEi: Angiotensin converting enzyme inhibitor; ARB: Angiotension II receptor blocker; HADS: Hospital anxiety-depression scale.
Comparison of per-protocol & control auscultatory measurements
We compared automatic oscillometric measurement assessed at the very beginning of survey procedures with auscultatory measurement realized by physician during interview with patients; full sample (cohort 1) was used for this analysis. Per-protocol oscillometric BP was significantly higher than standard auscultatory technique, with median intra-individual difference between the both methods 9/6 mmHg (Table 2, top panel & Figure 2, panels A). Despite the fact that BPs were significantly correlated, the linearity and tightness of this association were relatively poor (Figure 2, panels B). Moreover, the differences between both methods were not symmetrically distributed either for systolic or for diastolic BP (see Bland–Altman plots, panels C of Figure 2). Use of oscillometric (per-protocol) technique over-rated prevalence of inappropriate BP control (defined as systolic BP ≥140 mmHg and/or diastolic BP ≥140 mmHg) by more than 24% (≈ 59 vs 35%), compared with auscultatory technique.
| BP measurement modalities | 1st measurement | 2nd measurement | p-value |
|---|---|---|---|
| Cohort 1 (n = 913): | |||
| Per-protocol§ vs auscultatory physicians measurement¶ | |||
| – BP technique | Oscillometric§ | Auscultatory¶ | |
| – Systolic BP (SD) | 142.5 (19.5) | 132.1 (17.2) | <0.0001 |
| – Diastolic BP (SD) | 85.1 (11.4) | 78.1 (10.2) | <0.0001 |
| – Patients over BP target values (%)† | 59.3 | 34.9 | <0.0001 |
| – Median SBP difference (interquartile range)‡ | – | 9 (3 to 17) | – |
| – Median DBP difference (interquartile range)‡ | – | 6 (1 to 12) | – |
| Cohort 2 (n = 295): | |||
| Per-protocol§ vs repeated oscillometric measurement# | |||
| – BP technique | Oscillometric§ | Oscillometric# | |
| – Systolic BP (SD) | 141.5 (18.9) | 139.6 (20.6) | 0.041 |
| – Diastolic BP (SD) | 85.6 (11.1) | 82.0 (10.2) | <0.0001 |
| – Patients over BP target values (%)† | 57.3 | 52.2 | 0.079 |
| – Median SBP difference (interquartile range)‡ | – | 3 (-5 to 11) | – |
| – Median DBP difference (interquartile range)‡ | – | 4 (-2 to 9) | – |
| Cohort 3 (n = 202): | |||
| Per-protocol§ vs professional oscillometric device†† | |||
| – BP technique | Oscillometric§ | Oscillometric†† | |
| – Systolic BP (SD) | 138.9 (16.8) | 130.4 (17.6) | <0.0001 |
| – Diastolic BP (SD) | 86.5 (10.3) | 76.6 (11.4) | <0.0001 |
| – Patients over BP target values (%)† | 57.3 | 34.2 | <0.0001 |
| – Median SBP difference (interquartile range)‡ | – | 8 (1 to 16) | |
| – Median DBP difference (interquartile range)‡ | – | 10 (5 to 15) | |
| Auscultatory¶ vs professional oscillometric device†† | |||
| – BP technique | Auscultatory¶ | Oscillometric†† | |
| – Systolic BP (SD) | 126.8 (15.5) | 130.4 (17.6) | <0.0001 |
| – Diastolic BP (SD) | 75.8 (10.8) | 76.6 (11.4) | 0.063 |
| – Patients over BP target values (%)† | 22.3 | 34.2 | <0.0001 |
| – Median SBP difference (interquartile range)‡ | -3 (-10 to 3) | ||
| – Median DBP difference (interquartile range)‡ | 0 (-5 to 3) | ||
| Per-protocol§ vs automated unattended measurement‡‡ | |||
| – BP technique | Oscillometric§ | uAO‡‡ | |
| – Systolic BP (SD) | 138.9 (16.8) | 123.2 (17.3) | <0.0001 |
| – Diastolic BP (SD) | 86.5 (10.3) | 75.0 (10.2) | <0.0001 |
| – Patients over BP target values (%)† | 58.4 | 22.3 | <0.0001 |
| – Median SBP difference (interquartile range)‡, †† | – | 13 (8 to 25) | |
| – Median DBP difference (interquartile range)‡ | – | 12 (7 to 16) | |
| Auscultatory¶ vs automated unattended measurement‡‡ | |||
| – BP technique | Auscultatory¶ | uAO‡‡ | |
| – Systolic BP (SD) | 126.8 (15.5) | 123.2 (17.3) | 0.002 |
| – Diastolic BP (SD) | 75.8 (10.8) | 75.0 (10.2) | 0.174 |
| – Patients over BP target values (%)† | 22.3 | 22.3 | 0.99 |
| – Median SBP difference (interquartile range)‡ | 4 (-5 to 11) | ||
| – Median DBP difference (interquartile range)‡ | 0 (-4 to 6) | ||
The p-value by Wilcoxon's paired test or χ2 test.
†
SBP ≥140 and/or DBP ≥ 90 mmHg.
‡
1st minus 2nd measurement.
§
Automated oscillometric device (OMRON) at the beginning of survey procedures by research nurse (as defined by protocol of EUROASPIRE surveys).
¶
Standard auscultatory sphygmomanometer measured by physician during interview.
#
Automated oscillometric device (OMRON) at the end of survey procedures.
††
Automated oscillometric device (NISSEI) measured by physician during interview.
‡‡
uAO device (BPTru) at the end of survey procedures.
BP: Blood pressure; DBP: Diastolic blood pressure; SBP: Systolic blood pressure; SD: Standard deviation; uAO: Unattended automated oscillometric.
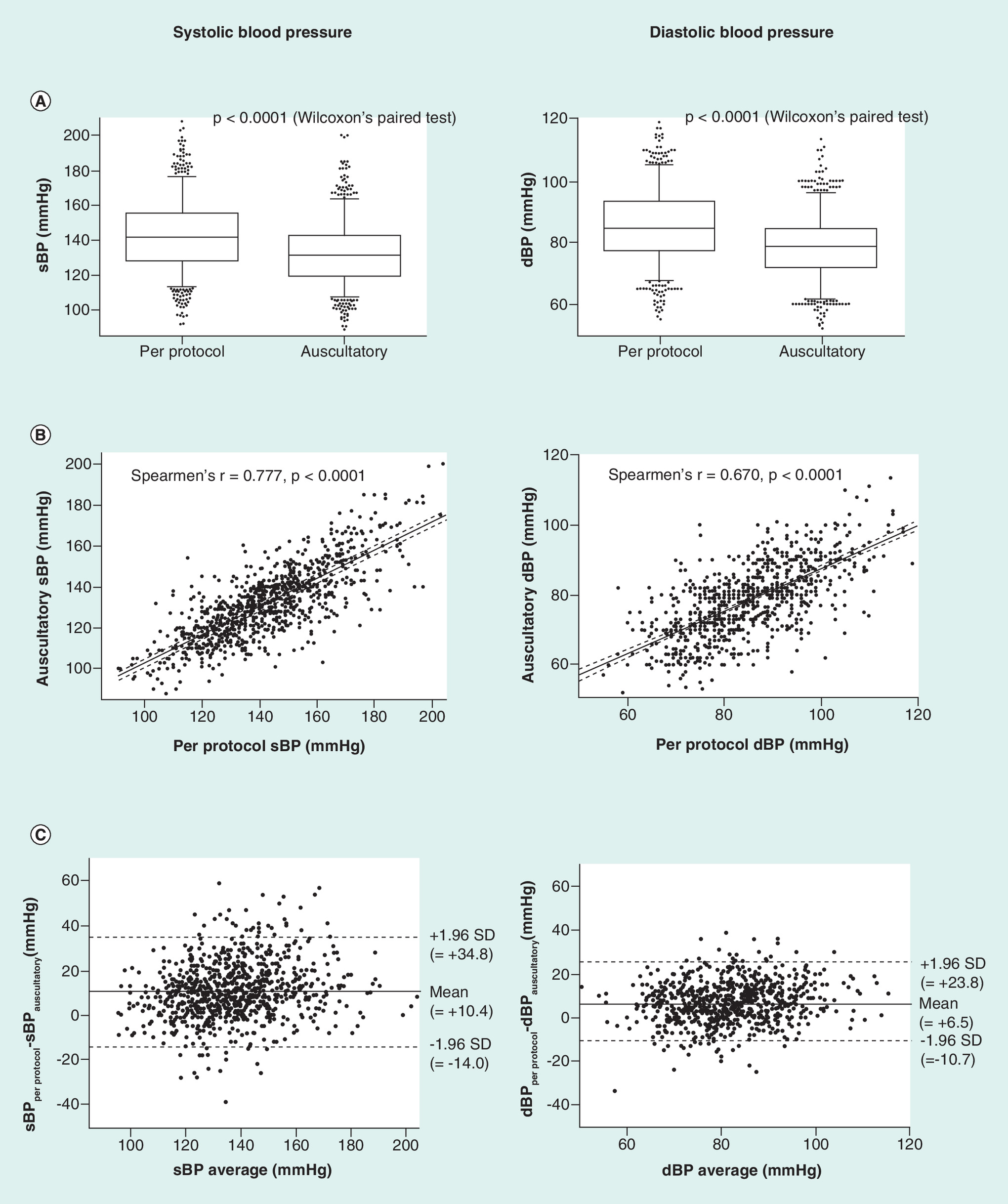
Figure 2. Per-protocol oscillometric and control auscultatory measurements, differences and correlations.
(A) Box whisker plots, (B) scatter plots and (C) bland-altman plots. n = 913 (cohort 1).
DBP: Diastolic blood pressure; SBP: Systolic blood pressure; SD: Standard deviation.
In a next step, we analyzed if any covariate (age, gender, current smoking, obesity, increased waist circumference, hypercholesterolemia, diabetes mellitus, anxiety, depression, treatment with specific drug classes, survey and center) may influence the difference between per-protocol and auscultatory BP value. In unifactorial analysis, we found that significant differences in either systolic or diastolic BP were found among age subgroups (11/8 vs 8/5 mmHg [p-values < 0.0001/<0.0001], in those aged ≥65 years vs <65 years, respectively) waist circumference categories (10/7 vs 8/5 [p- values 0.008/0.002], increased vs normal waist circumference, respectively) and survey (8/4 vs 11/6 vs 11/11 [p-values for trend < 0.0001/<0.0001], in EUROASPIRE III, IV and V, respectively). However, in multivariate analysis only age and current smoking group remained significant covariates of both, systolic and diastolic BP (see Supplementary Material for details). We also tested the potential effect of the observer (i.e., a physician who performed the auscultatory BP measurement). We did not find any significant influence of the observer on the established difference between per-protocol and auscultatory BP value, if adjusted for above-mentioned covariates (in multiple step-wise regression model; not in table). Moreover, since one observer was involved in all three surveys (EUROASPIRE III, IV and V), we used it as reference and compared with each of other observers, with no apparent effect again (see Supplementary Table).
Changes of BP over time during survey procedures
Additional oscillometric BP measurement was done in a random subsample of 295 subjects (cohort 2), and we evaluated to what extent BP differ when registered at the very beginning (per-protocol) and at the end of survey procedures. Using the same device for both measurements (OMRON M6), BP somewhat decreased over time, giving median intra-individual difference 3/4 mmHg (Table 2). Spearman correlation coefficients were 0.70 (p < 0.0001) and 0.63 (p < 0.0001) for systolic and diastolic BP's, respectively. Also nonachievement of BP target was by repeated measurement oscillometric measurement (at the end) very similar to per-protocol rates (at the beginning), in other words, approximately 57 versus 52% (Table 2). In contrast, nonachievement of BP target was in this subsample only 28.5% (not in table), when auscultatory technique was used for definition.
Comparison of per-protocol or auscultatory measurements with other techniques
In a subset of 202 patients (cohort 3, EUROASPIRE V campaign), we performed additional BP readings using another two different devices. First, we compared per-protocol oscillometric readings (OMRON) versus another type of oscillometric device (NISSEI), the latter measurement was done during interview with the physician. NISSEI device measurements were 8/10 mmHg lower than per-protocol BP values (Table 2). In contrast, comparing NISSEI oscillometric readings with auscultatory readings (both performed at the interview with physician), the difference between both measurements was substantially lower (-3/0 mmHg, auscultatory minus NISSEI, Table 2). Also concordance of both techniques was better (Figure 3) than in per-protocol versus auscultatory comparison (Figure 2).
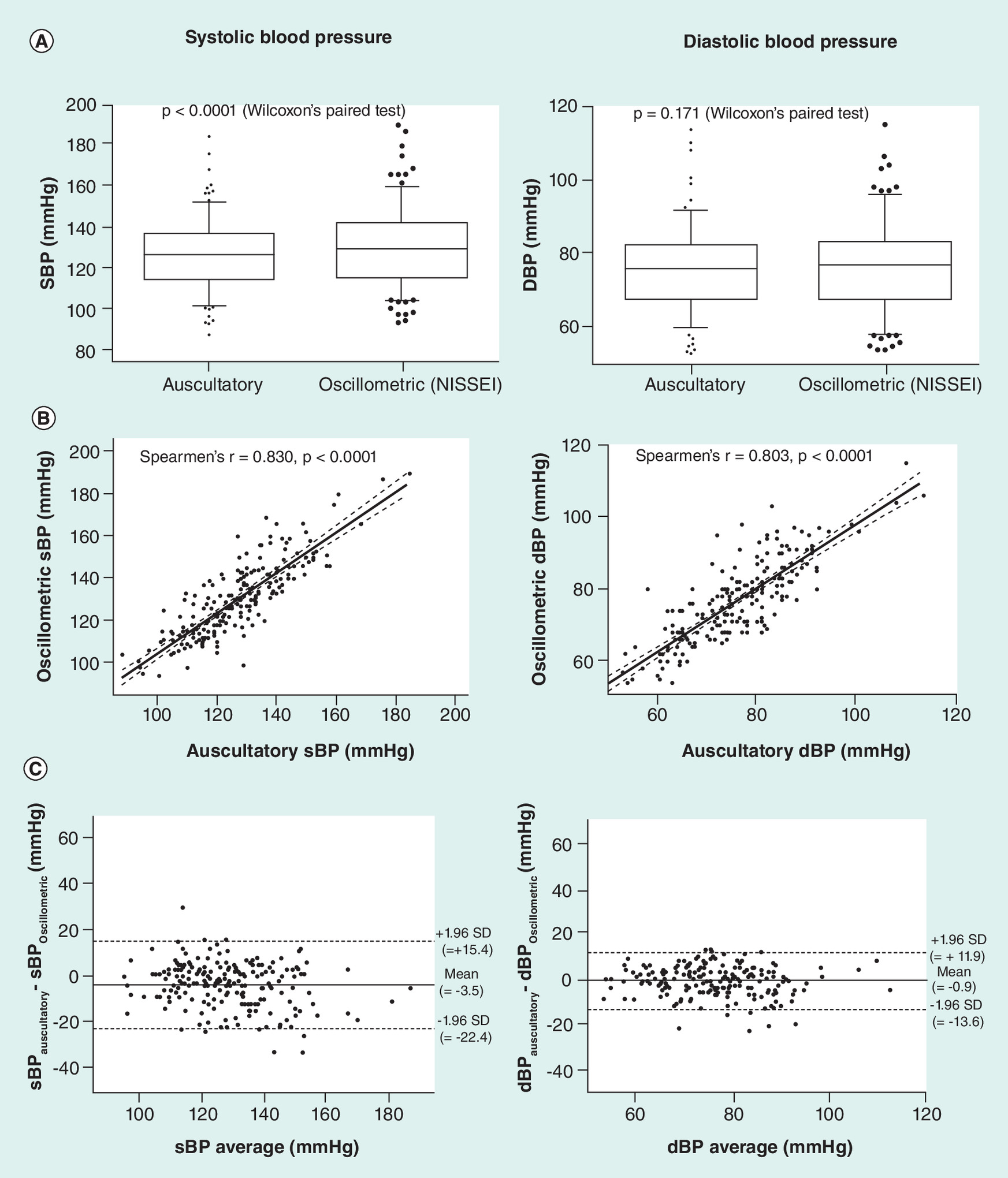
Figure 3. Auscultatory and another oscillometric device (NISSEI DM-3000) measurements, differences and correlations.
Box whisker plots, scatter plots and bland-altman plots.
n = 202 (cohort 3).
DBP: Diastolic blood pressure; SBP: Systolic blood pressure; SD: Standard deviation.
Finally, we compared unattended automated oscillometric (uAO) device (BP Tru) with ‘per-protocol’ oscillometric and auscultatory measurement. Oscillometric per-protocol measurement was by 13/12 mmHg higher than the average of 5 reading from uAO device and over-rated prevalence of inappropriate BP more than twofold (58 vs 22%). Only auscultatory systolic measurements were higher than uAO-based values (with median difference 4/0 mmHg). Moreover, corresponding prevalence of BP ≥140/90 was the same using these two methods (Table 2). General concordance of both methods was relatively good (Figure 4).
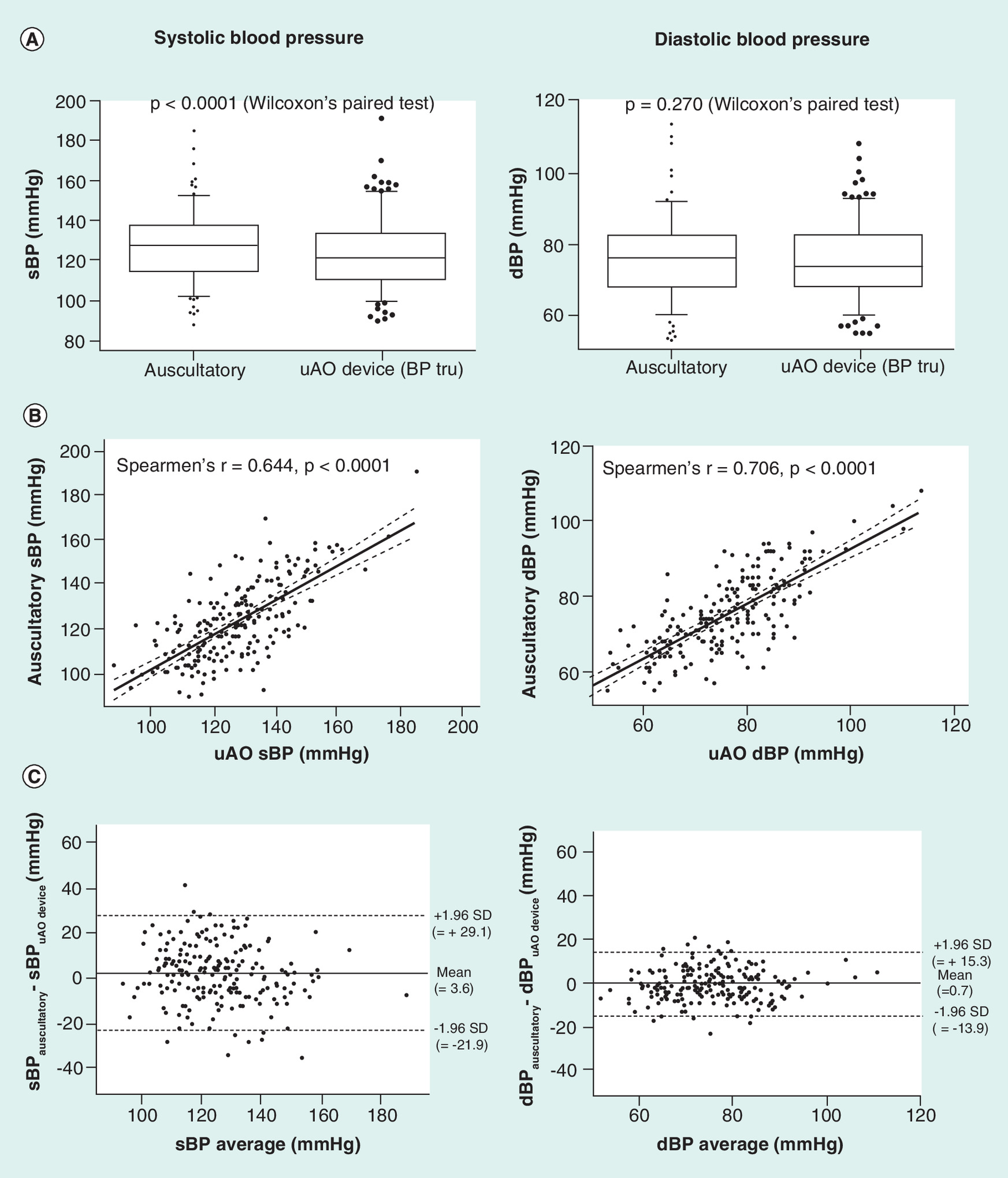
Figure 4. Auscultatory and unattended automated oscillometric device (BP Tru BPM 200) measurements, differences and correlations. (A) Box whisker plots, (B) scatter plots and (C) bland-altman plots.
n = 202 (cohort 3).
DBP: Diastolic blood pressure; SBP: Systolic blood pressure; SD: Standard deviation; uAO: Unattended automated oscillometric.
Discussion
The key finding of our study is that oscillometric and auscultatory techniques are not equivalent, at least if used in epidemiological surveys and set to coronary heart disease. Per-protocol oscillometric BP measurements were markedly higher (9/6 mmHg in median) and led to further 24% increase in prevalence of uncontrolled hypertension. All three EUROASPIRE surveys (III, IV and V) [9,15,17] elicited that control of hypertension to recommended BP target in cardiovascular patients in European countries remained rather unsatisfactory, and similar results we found in Czech patients [18]. In our subanalysis, proportion of those with per-protocol registered BP ≥140/90 mmHg was 62.5, 53.4 and 58.4% in 2006/07 (EA III), 2012/13 (EA IV) and 2016/17 (EA V), respectively (i.e., very poor). In contrast, using auscultatory-based BP, the corresponding proportions of patients over target BP were ‘only’ 42.7, 30.1 and 22.3% in the same samples. Thus, giving quite different message (i.e., control of hypertension is not so bad, and in addition, substantially improved over time). It is rather philosophic question which of these two conclusions is the true one. Indeed, the current Guidelines [11] recognized auscultatory-controlled and automated oscillometric devices as interchangeable and, the latter are extensively used for office BP estimation in clinical practice. On the other hand, the observed divergence between both techniques in achievement of treatment target seems to be unacceptable high and can lead not only to possible misinterpretation of an epidemiological survey (probably our case), but potentially also to incorrect clinical decision regarding management of hypertension.
The observed bias in BP measurements is not systematic and the large difference between both modalities seems to be attributable mainly to higher variability of per-protocol oscillometric technique (Figure 1A). Also limits of agreement between both techniques are relative broad (Figure 1C). The discordance of both techniques was generally independent from other patient's characteristics. For example, it was not higher in anxious patients, those with obesity, increased heart rate, etc. The only exception was the age of patients, when subjects aged 65 years or more had about twofold higher risk of having difference between both techniques (≥ +15 or ≥ +10 mmHg, for systolic or diastolic BP, respectively). In line with this finding, age-dependent higher variability of BP and consequent misclassification of hypertension were observed in other studies [19,20] and can be attributed to different properties of cardiovascular and autonomic nervous system in the elderly. We additionally tested the difference between both techniques also in regard to other characteristics. For example, no apparent between observers (physicians performing the auscultatory measurements) or between study centers (Pilsen/Prague) bias was found. And we obtained confirmatory results also if patients with atrial fibrillation were excluded.
In a subset of patients, we analyzed BP changes during survey visit and to what extent might be the per-protocol BP values influenced by unusual situation (participation in the study visit). Individual BP values, registered with the same oscillometric device (OMRON), but at the end of survey procedures, were somewhat lower than BP at the beginning (median intra-individual difference were 3/4 mmHg). However, the corresponding rate of achievement of target BP (140 mmHg) decreased only slightly (from ≈ 57 to 52%), being still far higher, than the same parameter, based on auscultatory measurement (≈ 29%). Therefore, the observed bias in BP values cannot be fully attributed to initial patient's stress.
More presumably, we should blame the device chosen for per-protocol BP measurement. Although this device (OMRON) is validated appropriately according to international standards [21], it was probably primary intended for (home) self-monitoring of BP. In the present analysis, we also compared per-protocol BP measured by OMRON with BP assessed using another oscillometric device NISSEI DM-3000 in a subgroup of patients. The concordance of both techniques in terms of target BP achievement was poor (57 vs 34%) again. However, when we compared NISSEI device with auscultatory measurement, we obtained more acceptable agreement. The logical explanation is that NISSEI oscillometric measurement was realized in the same time (i.e., during interview with physician) as auscultatory measurement. However, NISSEI device also enables to set maximal pressure of inflation (we used primary 160 mmHg and this pressure was further adjusted, if necessary) and generally, this device is primary intended for professional office BP measurements.
Last BP measurement modality tested was unattended automated oscillometric device (BP Tru). BP obtained by this device were not only markedly lower than per-protocol values, but also slightly lower (in systolic BP) than auscultatory measurements. The rate of adherence to target BP was for both modalities the same. On the other hand, despite that good concordance between conventional auscultatory technique and unattended automated oscillometric measurement was found in our analysis, we do not see any special advantage of the latter technique (which requires specific device, spatial adjustment of the medical office, is more time-consuming, etc), at least for routine practice.
Limitations
Our study had several limitations. It is necessary to stress that they are also other potential sources of bias in individual BP's, associated with study design. Our data are based on one single visit, realized for the purpose of observational survey. It can be presumed that registered BP (independently of used technique) may differ from usual BP assessed during regular clinical visit by patient's own physician.
Primary intention of our study was to demonstrate that different BP measurement techniques produce rather variable results, mainly in terms of average achievement of target BP in observational survey. Due to extensive program during study visit, each set of BP measurements (i.e., per-protocol, auscultatory, …) was not performed in the same time. Thus, our data cannot be used for entire validation across different BP techniques (which need different protocol). Moreover, because of indirect comparison of different methods, without having a ‘gold standard’ we are also not able to state, which BP is the ‘true one’ and which method is the ‘most exact’.
To simplify the message, we also used uniformly target BP lower than 140/90 mmHg. In fact, this target should be lower in diabetic patients [6].
Finally, due to inclusion criteria our sample includes relatively less-affected and long-term stable patients. As the interviews took place at least 6 months (median ≈ 1 year) after the qualifying cardiovascular event, the most severely ill patients deceased before the interview or did not respond because of their poor functional status.
Conclusion
Protocol of BP measurement may seriously bias results of studies dealing with hypertension control and relatively minor change of BP technique may completely alter results of an observational survey. We assume that the main reason for observed poor agreement was that per-protocol BP was registered using less appropriate device. Thus, any interpretation of observational surveys or interventional trial should be made with respect to used BP measurement technique.
Indeed, our study is not designed to answer the question, which method is the most accurate in terms of prediction of ‘hard’ cardiovascular outcomes (and we are not aware of any such evidence). On the other hand, the early concept of cardiovascular prevention started on presumption that BP values will be registered by auscultatory technique [1,2] and also underlying evidence, necessary for definition of BP targets from intervention trials, was based on auscultatory measurements (at least in ‘first generation’ of these studies). We think that similar approach should be used for basic decision making also in current everyday clinical practice, since the recommended principles of BP control in secondary prevention remained in last two decades more-than-less unchanged [2,6].
What is already known on this subject?
•
Current hypertension guidelines recognized automated oscillometric technique interchangeable with classical auscultatory measurement of blood pressure.
•
It has been demonstrated several times that various different techniques provided also intra-individually a different values.
What this study adds?
•
This analysis demonstrate that rather distinct change of blood measurement techniques leads to substantially different results in terms of blood pressure control.
•
Initial choice of blood measurement techniques may substantially influence the ‘general message’ of an observational survey.
Acknowledgments
The authors would like to acknowledge the cooperation of all investigators who also participated on the EUROASPIRE III–V surveys in Czech Republic over time (in alphabetical order): **V Adámková, **J Bělohoubek, *R Cífková, **M Galovcová, M Chocová, J Jeschke, P Karnosová, *A Krajčoviechová, H Rosolová, K Timoracká, J Vaněk, *P Wohlfahrt.
Second Department of Internal Medicine, Charles University, Pilsen. *Centre for Cardiovascular Prevention of the First Faculty of Medicine, Charles University and Thomayer's Hospital, Prague; **Department of Preventive Cardiology, Institute for Clinical and Experimental Medicine, Prague.
Financial & competing interests disclosure
The project was supported by the Health Development Agency of the Czech Ministry of Health (project 17-29520A), Specific Academic Research Project of Charles University (project SVV 260 393) and Charles University Research Fund (PROGRES, project Q39). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
File (suppl_file.docx)
- Download
- 17.43 KB
References
1.
Pyorala K, De Backer G, Graham I, Poole-Wilson P, Wood D. Prevention of coronary heart disease in clinical practice. Recommendations of the task force of the European Society of Cardiology, European Atherosclerosis Society and European Society of Hypertension. Eur. Heart J. 15(10), 1300–1331 (1994).
2.
Prevention of coronary heart disease in clinical practice. Recommendations of the Second Joint Task Force of European and other societies on coronary prevention. Eur. Heart J. 19(10), 1434–1503 (1998).
3.
De Backer G, Ambrosioni E, Borch-Johnsen K et al. European guidelines on cardiovascular disease prevention in clinical practice. Third Joint Task Force of European and Other Societies on Cardiovascular Disease Prevention in Clinical Practice. Eur. Heart J. 24(17), 1601–1610 (2003).
4.
Graham I, Atar D, Borch-Johnsen K et al. European guidelines on cardiovascular disease prevention in clinical practice: full text. Fourth Joint Task Force of the European Society of Cardiology and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of nine societies and by invited experts). Eur. J. Cardiovasc. Prev. Rehabil. 14(Suppl. 2), S1–113 (2007).
5.
Perk J, De Backer G, Gohlke H et al. European Guidelines on cardiovascular disease prevention in clinical practice (version 2012). The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts). Eur. Heart J. 33(13), 1635–1701 (2012).
6.
Piepoli MF, Hoes AW, Agewall S et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts): Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. J. Prev. Cardiol. 23(11), Np1–np96 (2016).
7.
EUROASPIRE. A European Society of Cardiology survey of secondary prevention of coronary heart disease: principal results. EUROASPIRE Study Group. European Action on Secondary Prevention through Intervention to Reduce Events. Eur. Heart J. 18(10), 1569–1582 (1997).
8.
Lifestyle and risk factor management and use of drug therapies in coronary patients from 15 countries; principal results from EUROASPIRE II Euro Heart Survey Programme. Eur. Heart J. EUROASPIRE II study Group. 22(7), 554–572 (2001).
9.
Kotseva K, Wood D, De Backer G, De Bacquer D, Pyorala K, Keil U. EUROASPIRE III: a survey on the lifestyle, risk factors and use of cardioprotective drug therapies in coronary patients from 22 European countries. Eur. J. Cardiovasc. Prev. Rehabil. 16(2), 121–137 (2009).
10.
Kotseva K, Wood D, De Bacquer D et al. EUROASPIRE IV: A European Society of Cardiology survey on the lifestyle, risk factor and therapeutic management of coronary patients from 24 European countries. Eur. J. Prev. Cardiol. 23(6), 636–648 (2015).
11.
Mancia G, Fagard R, Narkiewicz K et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur. Heart J. 34(28), 2159–2219 (2013).
12.
Landgraf J, Wishner SH, Kloner RA. Comparison of automated oscillometric versus auscultatory blood pressure measurement. Am. J. Cardiol. 106(3), 386–388 (2010).
13.
Heinemann M, Sellick K, Rickard C, Reynolds P, McGrail M. Automated versus manual blood pressure measurement: a randomized crossover trial. Int. J. Nurs. Pract. 14(4), 296–302 (2008).
14.
Raptis AE, Spring MW, Viberti G. Comparison of blood pressure measurement methods in adult diabetics. Lancet 349(9046), 175–176 (1997).
15.
Kotseva K, Wood D, De Bacquer D et al. EUROASPIRE IV: a European Society of Cardiology survey on the lifestyle, risk factor and therapeutic management of coronary patients from 24 European countries. Eur. J. Prev. Cardiol. 23(6), 636–648 (2016).
16.
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 67(6), 361–370 (1983).
17.
Kotseva K, De Backer G, De Bacquer D et al. Lifestyle and impact on cardiovascular risk factor control in coronary patients across 27 countries: Results from the European Society of Cardiology ESC-EORP EUROASPIRE V registry. Eur. J. Prev. Cardiol. 26(8), 824–835 (2019).
18.
Mayer OJ, Bruthans J, Timoracká K. The changes in cardiovascular prevention practice between 1995 and 2012 in the Czech Republic. A comparison of EUROASPIRE I, II, III and IV study. Cor. Vasa 56(2), e91–e97 (2013).
19.
Marshall T. Misleading measurements: modeling the effects of blood pressure misclassification in a United States population. Med. Decis. Making 26(6), 624–632 (2006).
20.
Tran NTT, Blizzard CL, Luong KN et al. Misclassification of blood pressure of Vietnamese adults when only a single measurement is used. J. Am. Soc. Hypertens. 12(9), 671–680 (2018).
21.
O'Brien E, Pickering T, Asmar R et al. Working Group on Blood Pressure Monitoring of the European Society of Hypertension International Protocol for validation of blood pressure measuring devices in adults. Blood Press. Monit. 7(1), 3–17 (2002).
Information & Authors
Information
Published In
Pages: 841 - 852
PubMed: 31475585
Copyright
© 2019 Future Medicine Ltd.
History
Received: 23 December 2018
Accepted: 17 May 2019
Published online: 2 September 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
To what extent can the chosen blood pressure measurement technique affect the outcomes of an observational survey?. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0149
Export citation
Select the citation format you wish to export for this article or chapter.