Osimertinib in first-line treatment of advanced EGFR-mutated non-small-cell lung cancer: a cost–effectiveness analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Osimertinib improves progression-free survival in first-line EGFR mutation–positive non-small-cell lung cancer. Materials & methods: A Markov cohort model including costs, utilities and disutilities, was conducted to estimate quality-adjusted life-year (QALY) and incremental cost–effectiveness ratio when treating with osimertinib versus standard first-line tyrosine kinase inhibitors (TKIs). Results: Osimertinib presented higher QALYs (0.61) compared with standard EGFR–TKIs (0.42). Osimertinib costs were €83,258.99, in comparison with €29,209.45 for the standard EGFR–TKIs. An incremental cost–effectiveness ratio of €273,895.36/QALY was obtained for osimertinib. Conclusion: Osimertinib was more effective in terms of QALYs gained than comparators (erlotinib–gefitinib). However, to obtain a cost–effectiveness alternative, a discount greater than 60% in osimertinib acquisition cost is required.
Epidermal growth factor receptor (EGFR) mutations are the most usual oncogenic mutation in patients with non-small-cell lung cancer (NSCLC) with adenocarcinoma. Detection of EGFR mutations are found in about 10–15% of Western patients and 30–35% of Asian patients [1]. In Spain, the mutation detection rate in advanced NSCLC patients was found to be 11.6% in the REASON study (82.6% presenting in-frame deletions in exon 19 and 17.4% presenting L858R mutation in exon 21) [2]. The first-generation EGFR-tyrosine kinase inhibitors (TKIs) gefitinib and erlotinib are highly active against cancers with two EGFR common sensitizing mutations (in-frame deletions in exon 19 or L858R mutation in exon 21) [1].
Nevertheless, more than half of the patients with NSCLC with EGFR-activating mutations develop tumor resistance despite the initial beneficial response to first-generation TKIs (erlotinib and gefitinib), generally 9 to 14 months after treatment initiation target [3–8]. Disease progression while on therapy with first-generation EGFR–TKIs is associated with a T790M acquired mutation in the EGFR gene. Consequently, T790M resistance mutation reduces binding of first and second-generation EGFR–TKIs to the target receptor and forces a change of treatment [9–11]. Osimertinib is an oral, third generation, irreversible EGFR–TKI that is currently employed in NSCLC EGFR T790M resistance mutations, with successful results [11–14]. Additionally, FLAURA study has demonstrated the clinical benefit of osimertinib in EGFR-TKI-sensitizing mutations [15]. In FLAURA study, the median progression-free survival (PFS) in patients with untreated EGFR mutated NSCLC was demonstrated to be significantly longer with osimertinib than with standard first-line EGFR–TKIs (18.9 vs 10.2 months) with a similar safety profile and lower rates of serious adverse events [15].
To date, only two prior studies have been published evaluating the cost–effectiveness of osimertinib [16,17]. A decision analytic model analysis over a 10-year time horizon has been published evaluating the cost–effectiveness of osimertinib in first-line EGFR-positive NSCLC [17]. Another cost–effectiveness analysis containing a probabilistic Markov model has been published recently, comparing osimertinib versus the first-generation employed EGFR–TKI in Canada [16]. Therefore, a complete Markov pharmacoeconomic model analysis in a European country with a public healthcare system including a deterministic and a probabilistic model of osimertinib in first-line EGFR positive NSCLC adenocarcinoma could provide extremely valuable information for medical decision makers to facilitate the optimization of healthcare resources in Europe. The aim of this study is to evaluate the incremental cost–effectiveness ratio (ICER) of osimertinib versus standard EGFR–TKIs (erlotinib and gefitinib), in order to determine which is the most efficient drug in first line.
Materials & methods
Cost–effectiveness analysis (CEA): Markov model
Design & perspective analysis
A Markov model was adopted to estimate the costs, the quality-adjusted life-years (QALYs) and ICER of two different treatment strategies (osimertinib vs standard EGFR–TKIs) in two hypothetical cohorts of patients with EGFR-positive sensitizing mutations advanced NSCLC. The model was developed from the Spanish National Health System perspective. The threshold for determining whether a strategy is cost effective was €24,000/QALY [18]. All the costs were estimated in euros (€) 2018, and a discount rate of 3% was used for costs and effects throughout the model. The Markov model was developed in Microsoft Excel 2011 (Microsoft Corp., WA, USA), using a 15-year time horizon. The results were presented in terms of costs (€), QALYs gained and ICER.
Markov model structure
The model included three mutually exclusive health states: stable disease (SD), progressive disease (PD) and death. Each health state was associated with costs, health effects and the probability of moving to any other state. The structure and transitions allowed in the model are shown in Figure 1. Initially, all patients were on SD and received one of the two treatment strategies. On each 28-day simulation cycle, the hypothetical cohort of patients could remain on SD, experience PD or death. Patients in SD continued treatment with the initial TKIs until progression occurred. When progression occurred, patients were changed to a second-line regimen. After PD occurred, patients could remain in this state or die. PD was simulated until all patients died. Death of patients from any cause were included in this state.
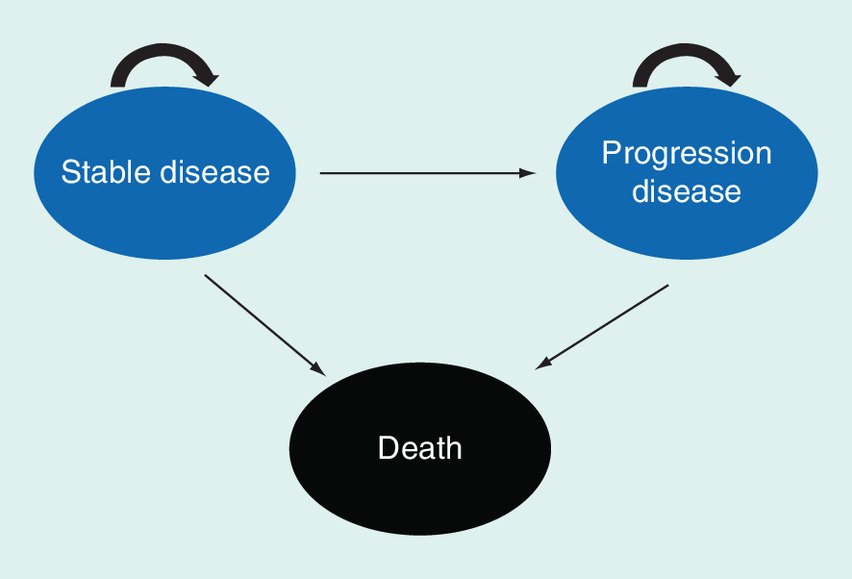
Figure 1. Structure of the Markov model.
Markov model health states.
Treatment alternatives
Each cohort was treated with osimertinib (at a dose of 80 mg once daily) or a standard oral EGFR–TKI (gefitinib at a dose of 250 mg once daily or erlotinib at a dose of 150 mg once daily), according to FLAURA clinical trial [15].
Transitional probability data
Transition rates between different states were estimated based on progression of disease and survival values estimated from FLAURA clinical trial [15]. The method of Guyot et al. was employed to recreate the patient level data [19]. Due to the short follow-up of FLAURA trial, Overall survival (OS) and PFS were not fully observed, therefore, results were extrapolated by using survival functions. In order to determine the most appropriate parametric survival curve, a goodness-of-fit analysis was conducted based on the best fit model among gamma, log-logistic, Weibull, lognormal, Gompertz, exponential, Royston–Parmar, generalized F and generalized gamma parametric distributions. These analyses were assessed using parametric plots, long-term projections and statistical tests (Akaike Information Criterion [AIC] and Bayesian Information Criterion [BIC]) (Supplementary Figure 1 & 2 and Supplementary Table 1). We used visual inspection of the Kaplan-Meier curves, goodness-of-fit statistics and clinical plausibility to determine the optimal parametric distribution with the best fit. The OS data is still immature (only complete in 25%). For this reason, a single parametric model (gamma) has been selected for all the treatment arms.
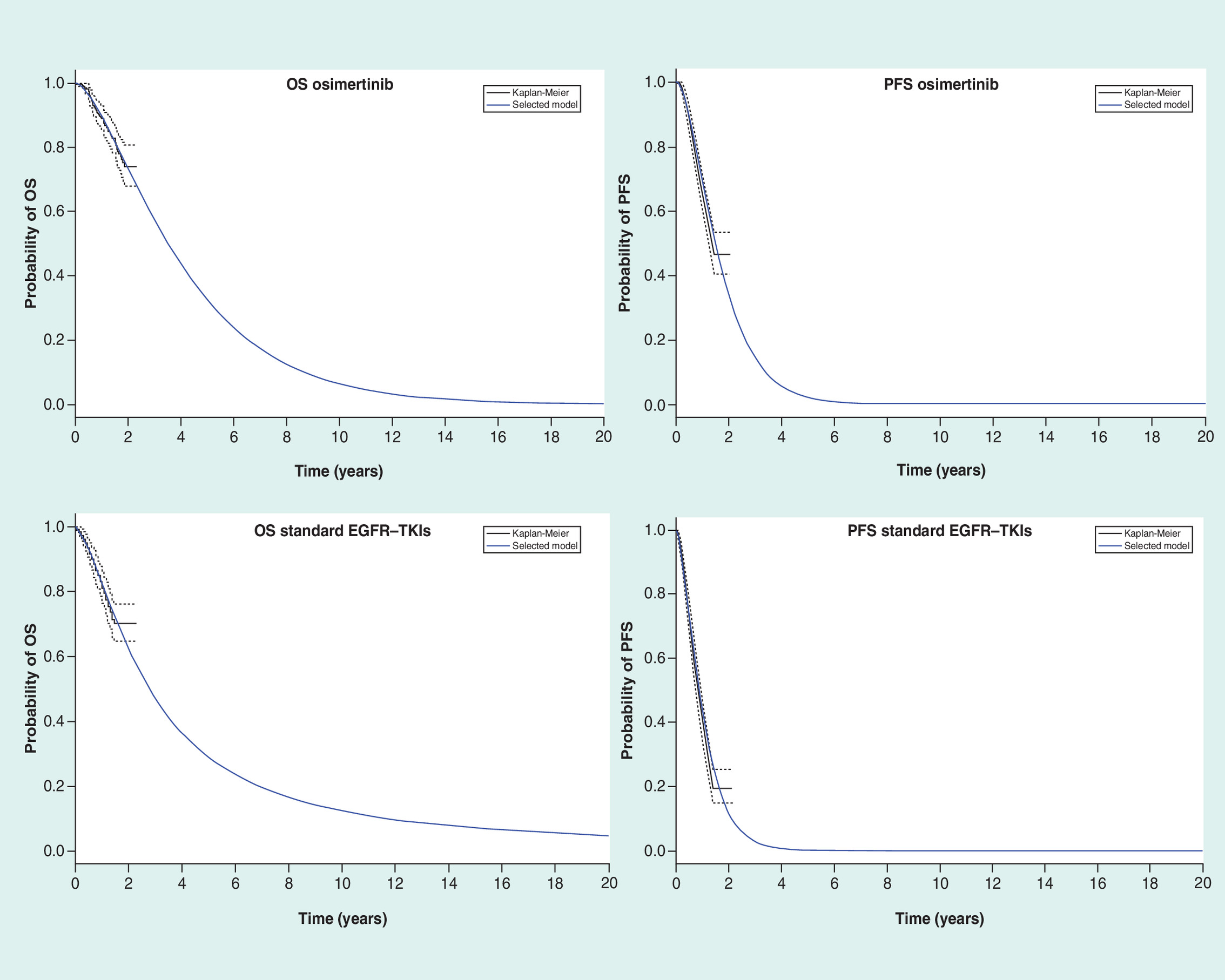
Figure 2. Overall survival and progression-free survival Kaplan–Meier plot and selected fitted curves.
OS: Overall survival; PFS: Progression-free survival; TKI: Tyrosine-kinase inhibitor.
Transition probabilities from SD and PD to death were obtained based on OS and PFS as shown in Figure 2. Finally, the difference between the OS and PFS curves was employed to calculate the probability of the patient remaining on PD state.
Cost estimation
Only direct medical costs were calculated (drugs, disease management, adverse events [AE] and second-line treatment). The cost of erlotinib, gefitinib and osimertinib were calculated according to the officially notified listed prices ([drug price - 7.5% official discount in Spain] × Value added tax [VAT]) (Table 1) [20,21]. Disease management costs were estimated according to an expert panel's advice. Disease management cost per patient and cycle was calculated multiplying the cost of healthcare resources employed by the unit cost of each resource consumed over a 15-year time horizon.
| Management of non-small-cell lung cancer | Cost per 28-day cycle and patient | Ref. |
|---|---|---|
| – Erlotinib/gefitinib | €1,836,48 | [20,21] |
| – Osimertinib | €5447.36 | |
| Second-line cost of osimertinib | €9294 | [20,21] |
| – Scheme (29% of total patients) | ||
| – EGFR–TKI scheme erlotinib/gefitinib (21%) | ||
| – Platinum-based chemotherapy schemes (36%) | ||
| – Non platinum-based chemotherapy schemes (35%) | ||
| – Others therapies (8%) | ||
| Second-line cost of standard EGFR–TKIs | €15,310 | [20,21] |
| – Scheme (47% of total patients) | ||
| – EGFR–TKI scheme treated with osimertinib (46%) | ||
| – Platinum-based chemotherapy schemes (13%) | ||
| – Non platinum-based chemotherapy schemes (12%) | ||
| – Others therapies (4%) | ||
| Grade III–IV adverse events | Median cost/cycle | [23] |
| – Diarrhea | €924.11 | |
| – Decreased appetite | €1375.31 | |
| – Dry skin | €26.2 | |
| – Paronychia | €341.41 | |
| – Stomatitis grade 3 | €2,332.14 | |
| – Stomatitis grade 4 | €5,325.7 | |
| – Pruritus | €341.41 | |
| – Fatigue | €106.78 | |
| – Anemia | €992.22 | |
| – Vomiting | €681.51 | |
| – Rash | €341.41 | |
| – AAT elevation grade 3 | €559.91 | |
| – AAT elevation grade 4 | €1799.09 | |
| – AAT elevation | €559.91 | |
| Utilities scenario | Value | [24] |
| – On treatment with no side effects | 0.84 | |
| – Diarrhea | 0.32 | |
| – Vomiting | 0.25 | |
| – Rash | 0.15 | |
| – Stomatitis | 0.25 | |
| – Dry skin | 0.15 | |
| – Decreased appetite | 0.41 | |
| – Paronychia | 0.15 | |
| – Anemia | 0.41 | |
| – Fatigue | 0.41 | |
| – Disease progression | 0.17 |
TKI: Tyrosine-kinase inhibitor.
The second-line therapy regimens were obtained from Supplementary Table 3 of FLAURA study [15] as is shown in Table 1. In osimertinib second-line arm, 21% of the patients were re-challenged with standard EGFR–TKI (erlotinib–gefitinib), 36% with platinum-based chemotherapy, 35% with non-platinum-based chemotherapy and 8% with other therapies (PD-1/PD-L1, anti-VEGF and others targeted therapies). In standard EGFR–TKIs second-line arm, 46% of the patients were treated with another EGFR–TKI including osimertinib, 13% with platinum-based chemotherapy, 12% with non-platinum-based chemotherapy and 4% with others therapies (PD-1/PD-L1, anti-VEGF and others targeted therapies). To calculate second-line costs, patients were assumed to have a body height of 170 cm and a weight of 70 kg, resulting in a body surface area of 1.73 m2. As PFS second-line treatment curves were not available in FLAURA clinical trial, we employed AURA3 clinical trial PFS2 curves to calculate second-line treatment duration [14]. We estimated the Area under the curve (AUC) in the PFS AURA3 trial curve comparing osimertinib versus platinum-pemetrexed in NSCLC patients who had disease progression after first-line EGFR–TKI therapy to obtain second-line treatment duration. We employed Guyot et al. method to simulate the best survival curve [19]. In order to obtain the best adjusting method, this survival curve was fitted with a Weibull distribution.
Unit costs were obtained from an official database published in Spain [22]. Side effects management costs in Spain (Table 1) were obtained from an internal database [23]. Adverse effect (grade III–IV events) frequencies associated with osimertinib and gefitinib–erlotinib treatments were obtained from FLAURA study [15]. Model costs are presented in Euros (€) 2018 (Table 1).
Utilities estimation
Health state utility inputs and disutility values for the base case were obtained from recent data published from UK [24]. Different utilities values were applied considering the different health states (SD and PD) and are summarized in Table 1. A health utility of zero was applied to the health state of death.
Disutilities estimation
Only disutility values associated with grade III–IV were addressed. To calculate the disutility values associated with grade III–IV in SD, disutilities parameters of each AE extracted from Nafees et al. was multiplied by the relative frequency of the corresponding event obtained from FLAURA trial to calculate a weighted average disutility value for each event profile. Disutility values calculated for each grade III–IV AE were subtracted from utility values while patients remained in SD.
Univariate sensitivity analysis
A deterministic univariate sensitivity analysis (DUSA) was performed to address the uncertainty of the ICER estimated value. In DUSA a single parameter in the model (drug costs, utilities or discounts) was modified to examine the effect on the ICER result. Drug costs were modified in three different ranges (±20%, ±40% and ±60%). Utilities values were varied in a range of ±15%. The 2008 utility value (0.473) in progression disease employed in previous article of quality of life [25], was used in order to determine if the ICER value is modificated. Discount values in the DUSA model were varied in a percentage of 0 and 6%.
Probabilistic sensitivity analysis
A probabilistic sensitivity analysis (PSA) was conducted to assess the uncertainty of the estimated results in the DUSA. The analysis was performed using 10,000 Monte Carlo simulations. Different parameters (side effects managements costs, disease management cost, second-line treatment costs, acquisition drug costs, utilities and transition probabilities) of the model were varied to determine the robustness of the model. In addition, the PSA was employed to obtain acceptability curves, showing the probability of each alternative being cost-effective across a range of possible values of willingness to pay for an additional QALY [26].
According to the characteristics of each variable, different types of probability distributions were employed to variate the model parameters [27]. Gamma distributions were applied for costs, beta for utilities and Dirichlet distributions for transition probabilities.
Results
Under base-case assumptions, the total QALYs were 0.61 and 0.42, for osimertinib and standard EGFR–TKIs, respectively. Osimertinib provided a 0.20 increase in QALYs compared with the standard EGFR–TKIs. For osimertinib arm, the mean costs of the intervention were €83,258.99 discounted over the 15-years horizon, in comparison with the €29,209.45 for the standard EGFR–TKIs. These costs and QALY values yielded an incremental ICER of €273,895.36/QALY for osimertinib compared with standard EGFR–TKIs. The results of the baseline scenario analysis are shown in Table 2. Additionally, the net gain in life-years (LYG) in osimertinib group compared with standard EGFR–TKI group was 0.25 (1.05 life-years vs 0.80 life-years for osimertinib and standard EGFR–TKIs, respectively).
| Variable | Strategy | |
|---|---|---|
| Standard EGFR–TKIs | Osimertinib | |
| Total cost/pt | €29,209.45 | €83,258.99 |
| – Treatment cost/pt | €19,214.00 | €74,651.43 |
| – Disease management/pt | €2307.05 | €2638.15 |
| – Adverse events costs/pt | €35.30 | €55.01 |
| – 2L cost /pt | €7653.10 | €5914.40 |
| QALY gained /pt | 0.42 | 0.61 |
| ICER (€/QALY) Osimertinib vs Erlotinib–Gefitinib | €273,895.36/QALY | |
2L: Second-line pt: patient; ICER: Incremental cost–effectiveness ratio; QALY: Quality-adjusted life year; TKI: Tyrosine-kinase inhibitor.
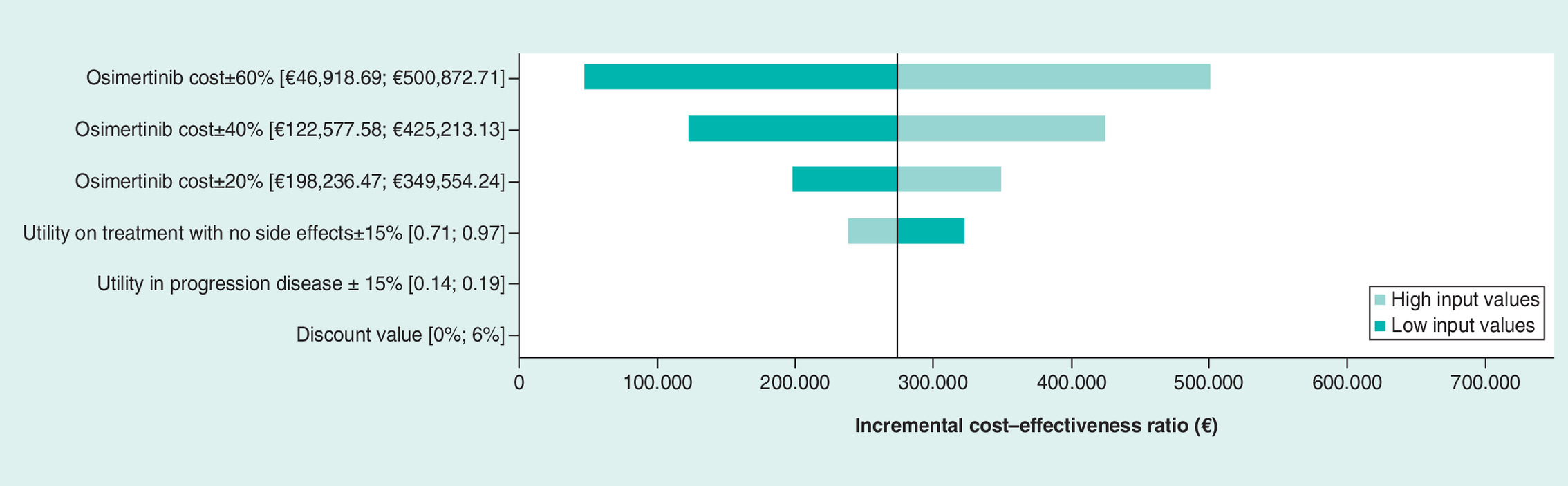
The DUSA showed significant changes in the ICER after modifying osimertinib costs, utilities and discount values as is shown in Tornado diagram (Figure 3) and Supplementary Table 2. Hence, the results of the DUSA showed that discounts greater than 60% in drug acquisition cost produced an ICER value below the threshold of 24,000€ per QALY gained fixed in Spain.
Furthermore, the PSA results were consistent with the base-case analyses. According to the cost–effectiveness plane shown in Figure 4, standard EGFR–TKIs were more effective and less costly in 62.28% of the iterations in the simulation. Only in 37.72% of the iterations, osimertinib was more effective and less costly than standard EGFR–TKIs.
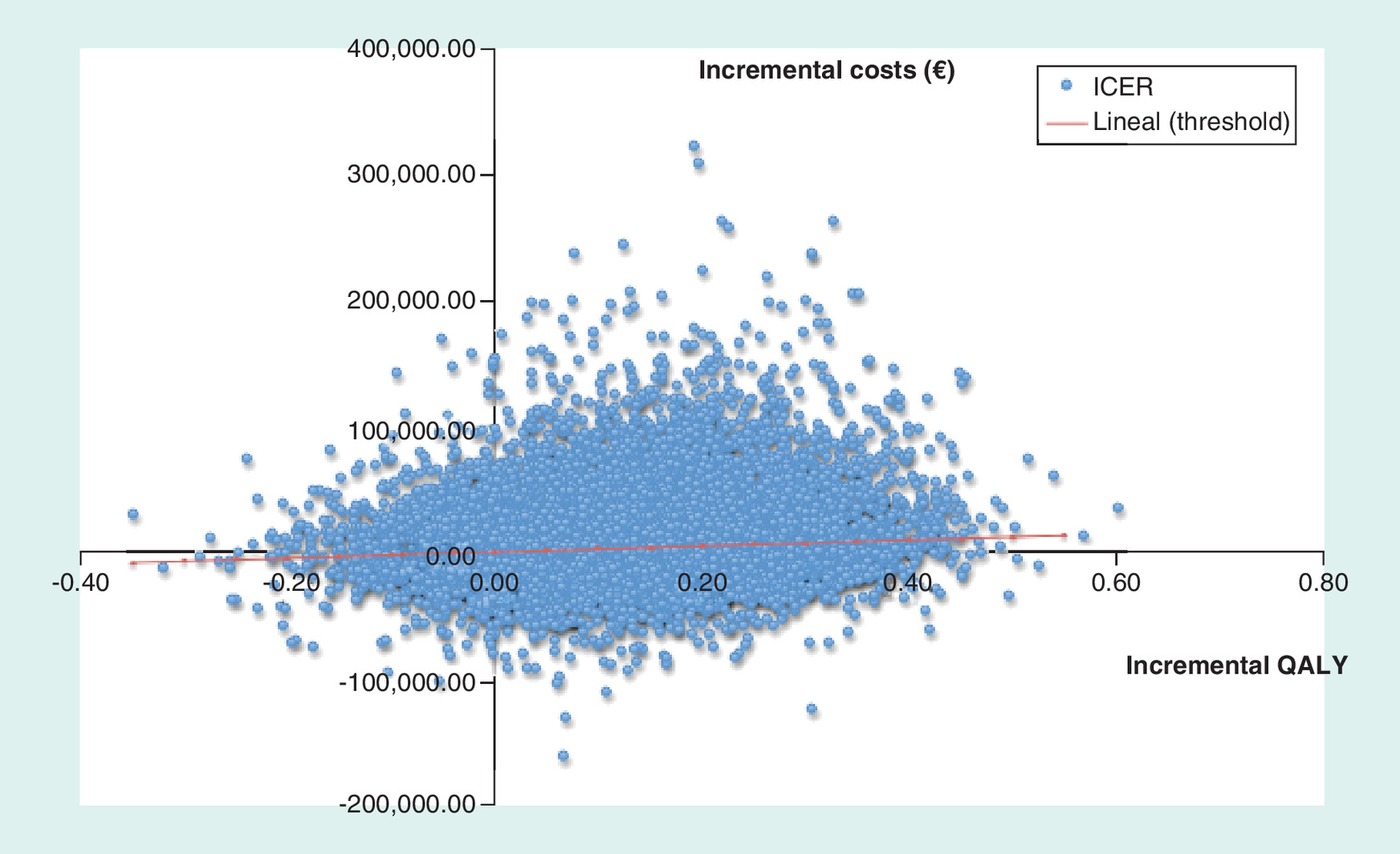
Figure 4. Scatter plot of Monte Carlo probabilistic sensitivity analysis for osimertinib versus first-line epidermal growth factor receptor-tyrosine kinase inhibitors (erlotinib–gefitinib).
ICER: Incremental cost–effectiveness ratio; QALY: Quality-adjusted life year.
Finally, the likelihood of osimertinib being considered cost effective was determined for a range of acceptability ratios, as shown in the acceptability curve. At the base-case scenario, there is a 42.94% probability of osimertinib being cost-effective at a threshold of €24.000/QALY (Figure 5).
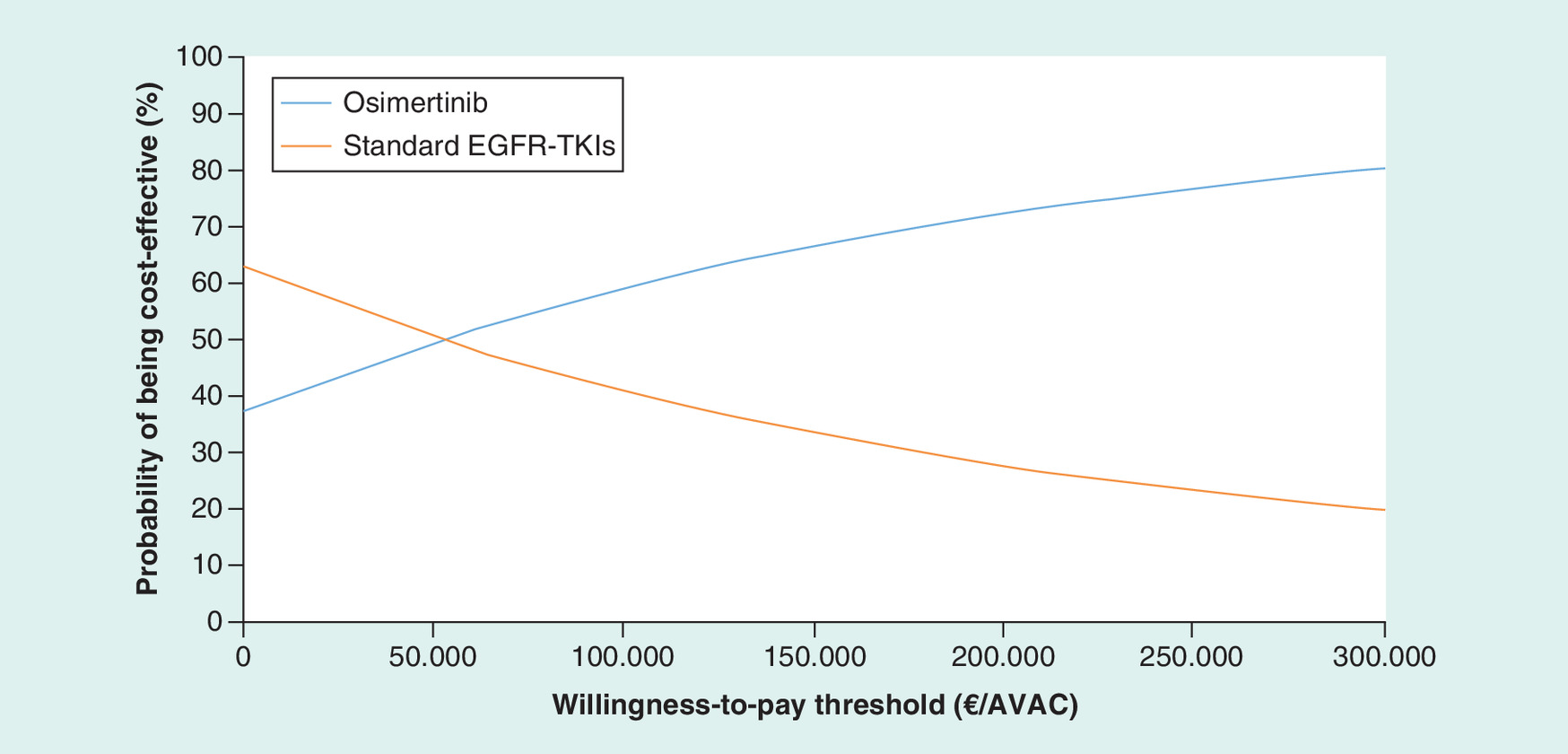
Figure 5. Cost–effectiveness acceptability curve osimertinib versus first-line epidermal growth factor receptor-tyrosine kinase inhibitors (erlotinib–gefitinib).
Graph plot willingness to pay scenario (x-axis) versus the likelihood in percentage that the treatment would be considered cost-effective (y-axis).
ICER: Incremental cost–effectiveness ratio; TKI: Tyrosine-kinase inhibitor.
Discussion
Recently, osimertinib has demonstrated a clinically meaningful benefit in patients with EGFR T790M mutation who have developed acquired resistance to TKIs [12–14]. Additionally, FLAURA study has demonstrated the clinical benefit of osimertinib in EGFR–TKI-sensitizing mutations. Therefore, we developed a complete cost–effectiveness analysis to compare osimertinib versus standard first-line EGFR–TKIs (erlotinib–gefitinib) in patients with previously untreated, EGFR mutation–positive advanced NSCLC, based on FLAURA study [15]. We demonstrated that osimertinib is considered more effective in comparison with standard TKIs in sensitizing EGFR mutations, in terms of QALYs gained (0.20). However, our study showed that osimertinib was not cost-effective compared with EGFR–TKIs because the ICER (€273,895.36/QALY) was higher than the commonly accepted threshold in Spain of €24,000/ QALY [18]. In addition, in our study, we established that discounts greater than 60% are crucial in the osimertinib acquisition costs to be considered a cost-effective alternative.
To date, only four different studies have compared the cost–effectiveness of osimertinib [16,17,28,29]. However, two of these studies are not comparable because they only compare osimertinib versus pemetrexed-platinum based chemotherapy in patients with demonstrated T790M mutation [28,29]. In the study published by Wu et al. [29] they estimated that osimertinib was not cost–effectiveness in the USA due to the high acquisition cost of osimertinib drug as we demonstrated. In addition, we can conclude that ICER value obtained (scenario 3 patients without metastasis) in USA by Wu et al. [29] is really approximate to ours with $222,030/QALY. In the recently published article by Aguiar et al. [17], the authors performed an innovative decision analytic-model over a 10-year time horizon to evaluate the cost–effectiveness of osimertinib from data collected from FLAURA study. The authors compared two different strategies: the first one comparing osimertinib in second-line in patients who harbor T790 mutation versus chemotherapy or immunotherapy in patients without this mutation; the second strategy they addressed in the aim of the study was similar to our purpose and consisted of the comparison of osimertinib in first-line continued by a standard second-line therapy at disease progression. The results obtained in the USA by Aguiar et al. are really in concordance with ours in Spain, obtaining an approximate ICER of $230.000/QALY, a QALY value for osimertinib of 2.12 and a 0.594 incremental number of QALY gained compared with the standard EGFR–TKIs (gefitinib–erlotinib–afatinib) in first line. However, in the study recently published by Aguiar et al., the authors only performed a DUSA over a 10-year time horizon. Generally, to reinforce the results obtained in the DUSA a PSA is frequently performed [30]. Therefore, in our study, the deterministic results obtained are complemented with a PSA to demonstrate the robustness of the ICER values obtained and to indicate accurately the osimertinib cost–effectiveness thresholds. Additionally, to improve the quality of the analysis, we changed the lifetime horizon in our study from the classical 10-year to a 15-year lifetime horizon analysis. Nonetheless, Aguiar et al. conclude that high cost of the drug makes osimertinib a not so cost-effective alternative, unlike the superior values of PFS or OS obtained.
To our knowledge, this is the first complete economic study in Europe to provide a direct comparison of osimertinib against the first-line standard of care (gefitinib–erlotinib) for the patients with EGFR mutated NSCLC. To reinforce our obtained results, another recently published Markov analysis by Ezeize et al. in Canada showed a similar non cost–effectiveness analysis with an incremental gain of 0.79 QALYs and an incremental ICER of 223.133$/QALY [16]. Therefore, our findings show that the choice of treatment in this study should be essentially determined by the drug acquisition cost. Considering the efficacy and the quality of life, osimertinib should be the treatment of choice. Osimertinib is expected to provide an incremental 0.20 QALYs gained in the study. However the acquisition cost was higher compared with the cost of standard EGFR–TKI, resulting in a difference of €55,437.43 per patient.
In addition, the acceptability curve of WTP obtained in our study shows a range of threshold values, as an aid for context-dependent decision making. We demonstrated that with standard WTP thresholds, osimertinib may be considered not cost-effective in Spain due to the high price of drug acquisition. Currently, the defined cost–effectiveness threshold in the Spanish setting is €24,000/QALY [18].
Nowadays, the establishment of different innovative purchasing algorithms such as pay-for-performance (P4P) are increasingly implemented in developed healthcare systems. These algorithms have demonstrated promoting improvements in healthcare quality and to reduce the acquisition costs of different innovative therapies [31,32]. To facilitate physician prescribing decision, different institutions such as European Society for Medical Oncology (ESMO) [33] or American Society of Clinical Oncology (ASCO) [34] have recently created pharmacoeconomic tools. Therefore, these results may be useful for health administrators and policy-makers in negotiations of prices with drug manufacturers, as also by the drug manufacturers themselves to consider reducing prices of this drug to encourage adoption of new generation of TKIs regimens.
There are some limitations in our study. First, common to all Markov models, there is the implicit uncertainty from combination of data from numerous sources and assumptions. Second, the result of the model could be impacted by the assumptions around curve extrapolation. Nonetheless, the algorithm used for extrapolation, Guyot et al. [19], provides excellent accuracy for the calculation of survival probabilities.
Thirdly, we only contemplate the payers' perspective of Spanish National Health System and not indirect costs (absenteeism, changes of individual productivity, unpaid assistance from a family member). In addition, the utility values considered in the model were extracted from a validated study published in the population of UK [24] but not from our own country, Spain, since these data were not available. The utility values of 0.17 assigned to disease progression could be lower than the utility values obtained in 2008 by Nafees et al. (0.473) [25]. This difference is due to the change of methodology employed to calculate these utilities values. In Nafees et al. study 2008 [25] authors employed a standard gamble method, while in 2017 study a time-trade-off method was employed by the authors [24]. Different authors as Stiggelbout et al. [35] conclude that these two methods are not equal estimating utility values, therefore producing the time-trade-off method lower utilities values. In order to determine the influence of utility values in definitive ICER results in our model, we included the 2008 utility value employed in Nafees et al. study (0.473) [25] in the DUSA, to determine if the ICER value is modificated by different utility values and we concluded that there was no difference (€273,895.36 vs. €264,691.25) Fourth, individual data from erlotinib and gefitinib patients cannot be extracted from the supplementary data of the FLAURA study, therefore a combined arm is evaluated in this study. Fifth, when disease progression while on therapy with first-generation EGFR-TKI, a second generation TKI, afatinib, is normally prescribed [36]. However, we did not include an afatinib arm in the economic analysis, because in the FLAURA study a direct comparison between afatinib and osimertinib is not evaluated.
Conclusion
From Spanish National Health System perspective, treatment with osimertinib was more effective in terms of QALYs gained than treatment with standard EGFR–TKIs erlotinib–gefitinib. However, osimertinib has been proved not to be a cost-effective alternative in first-line therapy for advanced EGFR-mutated NSCLC patients, compared with erlotinib-gefitinib due to the high acquisition costs of the drug. Additionally, our study could also be applied to other TKIs treatments with similar efficacy rates that become available in the future.
•
In FLAURA study, the median progression-free survival in patients with untreated EGFR mutated non-small-cell lung cancer was demonstrated to be significantly longer with osimertinib than with standard first-line epidermal growth factor receptor-tyrosine kinase inhibitors (EGFR–TKIs) (18.9 vs 10.2 months).
•
Osimertinib presented higher quality-adjusted life years (QALYs) (0.61) compared with standard EGFR–TKIs (0.42).
•
Osimertinib total costs of the intervention were €83,258.99, in comparison with the €29,209.45 for the standard EGFR–TKIs.
•
An incremental cost–effectiveness ratio of €273,895.36/QALY was obtained for osimertinib compared with standard EGFR–TKIs.
•
From Spanish National Health System perspective, osimertinib has been proved not to be a cost-effective alternative in first-line therapy for advanced EGFR-mutated NSCLC patients, compared with erlotinib–gefitinib due to the high acquisition costs of the drug.
•
A discount greater of 60% in osimertinib acquisition cost could produce an incremental cost–effectiveness ratio value below the established threshold of €24,000 per QALY gained in Spain to result a cost–effectiveness alternative.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: www.futuremedicine.com/doi/full/10.2217/cer-2019-0029
Author contributions
All the authors interpreted data, read and approved the final manuscript.
Financial & competing interests disclosure
Research grants from ISCIII PI17/02158 (JM), Juan Rodés research program ISCIII JR18/00050 (JM) and Rio Hortega CM 16/00223 (APC) from the Spanish government. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
{kind=link}
References
1.
Sharma SV, Bell DW, Settleman J, Haber DA. Epidermal growth factor receptor mutations in lung cancer. Nat. Rev. Cancer 7(3), 169–181 (2007).
2.
Esteban E, Majem M, Martinez Aguillo M et al. Prevalence of EGFR mutations in newly diagnosed locally advanced or metastatic non-small cell lung cancer Spanish patients and its association with histological subtypes and clinical features: the Spanish REASON study. Cancer Epidemiol. 39(3), 291–297 (2015).
3.
Jänne PA, Wang X, Socinski MA et al. Randomized Phase II trial of erlotinib alone or with carboplatin and paclitaxel in patients who were never or light former smokers with advanced lung adenocarcinoma: CALGB 30406 trial. J. Clin. Oncol. 30(17), 2063–2069 (2012).
4.
Rosell R, Moran T, Queralt C et al. Screening for epidermal growth factor receptor mutations in lung cancer. N. Engl. J. Med. 361(10), 958–967 (2009).
5.
Gao G, Ren S, Li A et al. Epidermal growth factor receptor-tyrosine kinase inhibitor therapy is effective as first-line treatment of advanced non-small-cell lung cancer with mutated EGFR: A meta-analysis from six Phase III randomized controlled trials. Int. J. Cancer 131(5), E822–E829 (2012).
6.
Maemondo M, Inoue A, Kobayashi K et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N. Engl. J. Med. 362(25), 2380–2388 (2010).
7.
Mitsudomi T, Morita S, Yatabe Y et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised Phase 3 trial. Lancet Oncol. 11(2), 121–128 (2010).
8.
Zhou C, Wu Y-L, Chen G et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, Phase 3 study. Lancet Oncol. 12(8), 735–742 (2011).
9.
Yun C-H, Mengwasser KE, Toms AV et al. The T790M mutation in EGFR kinase causes drug resistance by increasing the affinity for ATP. Proc. Natl Acad. Sci. USA 105(6), 2070–2075 (2008).
10.
Sos ML, Rode HB, Heynck S et al. Chemogenomic profiling provides insights into the limited activity of irreversible EGFR Inhibitors in tumor cells expressing the T790M EGFR resistance mutation. Cancer Res. 70(3), 868–874 (2010).
11.
Cross DAE, Ashton SE, Ghiorghiu S et al. AZD9291, an irreversible EGFR–TKI, overcomes T790M-mediated resistance to EGFR inhibitors in lung cancer. Cancer Discov. 4(9), 1046–1061 (2014).
12.
Goss G, Tsai C-M, Shepherd FA et al. Osimertinib for pretreated EGFR Thr790Met-positive advanced non-small-cell lung cancer (AURA2): a multicentre, open-label, single-arm, Phase 2 study. Lancet Oncol. 17(12), 1643–1652 (2016).
13.
Yang JC-H, Ahn M-J, Kim D-W et al. Osimertinib in pretreated T790M-positive advanced non-small-cell lung cancer: AURA Study Phase II extension component. J. Clin. Oncol. 35(12), 1288–1296 (2017).
14.
Mok TS, Wu Y-L, Ahn M-J et al. Osimertinib or platinum-pemetrexed in EGFR T790M-positive lung cancer. N. Engl. J. Med. 376(7), 629–640 (2017).
15.
Soria J-C, Ohe Y, Vansteenkiste J et al. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N. Engl. J. Med. 378(2), 113–125 (2018).
16.
Ezeife DA, Kirk V, Chew DS et al. Economic analysis of osimertinib in previously untreated EGFR-mutant advanced non-small cell lung cancer in Canada. Lung Cancer 125, 1–7 (2018).
17.
Aguiar PN, Haaland B, Park W, San Tan P, Del Giglio A, de Lima Lopes G. Cost–effectiveness of osimertinib in the first-line treatment of patients with EGFR-mutated advanced non-small cell lung cancer. JAMA Oncol. 4(8), 1080–1084 (2018).
18.
Vallejo-Torres L, García-Lorenzo B, Serrano-Aguilar P. Estimating a cost–effectiveness threshold for the Spanish NHS. Health Econ. 27(4), 746–761 (2018).
19.
Guyot P, Ades AE, Ouwens MJNM, Welton NJ. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan–Meier survival curves. BMC Med. Res. Methodol. 12, 9 (2012).
20.
Spanish Healthcare Ministry. Drug prices (2017). www.aemps.gob.es/cima/publico/home.html
21.
Spanish Healthcare Ministry. Official discounts in drug prices (2017). www.msssi.gob.es/profesionales/farmacia/pdf/DeduccionesJunio2017.pdf
22.
Departamento de Salud. ORDRE SLT/30/2013, de 20 de febrero, per la qual s'aproven els preus públics del Servei Catalá de la Salut. Orden SLT/30/2013, 20 Febrero, 2013. Diari Oficial de la Generalitat de Catalunya Núm 6323. Diari Oficial de la Generalitat de Catalunya. (2013).
23.
Martín Escudero V, Garcia del Muro X, Trigo J. Uso de los recursos y costes asociados con el manejo de los acontecimientos adversos asociado al uso de terapias dirigidas en el tratamiento del carcinoma de células renales metastásico en España. In: Jornadas de Economía de la Salud (2010).
24.
Nafees B, Lloyd AJ, Dewilde S, Rajan N, Lorenzo M. Health state utilities in non-small cell lung cancer: an international study. Asia Pac. J. Clin. Oncol. 13(5), e195–e203 (2017).
25.
Nafees B, Stafford M, Gavriel S, Bhalla S, Watkins J. Health state utilities for non-small-cell lung cancer. Health Qual. Life Outcomes 6, 84 (2008).
26.
Barton GR, Briggs AH, Fenwick EAL. Optimal cost–effectiveness decisions: the role of the cost–effectiveness acceptability curve (CEAC), the cost–effectiveness acceptability frontier (CEAF), and the expected value of perfection information (EVPI). Value Health 11(5), 886–897 (2008).
27.
Aalabaf-Sabaghi M. Decision modelling for health economic evaluation. J. Epidemiol. Community Health. 61(9), 839 (2007).
28.
Bertranou E, Bodnar C, Dansk V, Greystoke A, Large S, Dyer M. Cost–effectiveness of osimertinib in the UK for advanced EGFR-T790M non-small cell lung cancer. J. Med. Econ. 21(2), 113–121 (2018).
29.
Wu B, Gu X, Zhang Q. Cost–effectiveness of osimertinib for EGFR mutation-positive non-small cell lung cancer after progression following first-line EGFR–TKI therapy. J. Thorac. Oncol. 13(2), 184–193 (2018).
30.
Adalsteinsson E, Toumi M. Benefits of probabilistic sensitivity analysis – a review of NICE decisions. J. Mark. Access Health Policy 1, (2013).
31.
Epstein AM. Will pay for performance improve quality of care? The answer is in the details. N. Engl. J. Med. 367(19), 1852–1853 (2012).
32.
Sutton M, Nikolova S, Boaden R, Lester H, McDonald R, Roland M. Reduced mortality with hospital pay for performance in England. N. Engl. J. Med. 367(19), 1821–1828 (2012).
33.
Cherny NI, Sullivan R, Dafni U et al. ESMO – Magnitude of Clinical Benefit Scale V.1.0 questions and answers. ESMO Open 1(5), e000100 (2016).
34.
Schnipper LE, Davidson NE, Wollins DS et al. American Society of Clinical Oncology statement: a conceptual framework to assess the value of cancer treatment options. J. Clin. Oncol. 33(23), 2563–2577 (2015).
35.
Stiggelbout AM, Kiebert GM, Kievit J, Leer JW, Stoter G, de Haes JC. Utility assessment in cancer patients: adjustment of time tradeoff scores for the utility of life years and comparison with standard gamble scores. Med. Decis. Making 14(1), 82–90 (1994).
36.
Yang JC-H, Shih J-Y, Su W-C et al. Afatinib for patients with lung adenocarcinoma and epidermal growth factor receptor mutations (LUX-Lung 2): a Phase 2 trial. Lancet Oncol. 13(5), 539–548 (2012).
Information & Authors
Information
Published In
Pages: 853 - 863
PubMed: 31478399
Copyright
© 2019 Future Medicine Ltd.
History
Received: 19 February 2019
Accepted: 3 May 2019
Published online: 3 September 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Osimertinib in first-line treatment of advanced EGFR-mutated non-small-cell lung cancer: a cost–effectiveness analysis. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0029
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Nicola Perrotta, Adriana Coluccia, Francesca Rossi, Giulia Amato, Giacomo Polito, Pharmacoeconomic Analysis of Osimertinib Compared to Earlier‐Generation EGFR Inhibitors in EGFR ‐Mutated NSCLC : A Systematic Review , Cancer Medicine, 10.1002/cam4.72129, 15, 7, (2026).
- Li-Jung Elizabeth Ku, Jui-Hung Tsai, Li-Jun Chen, Szu-Chun Yang, Cost-effectiveness of lazertinib as first-line treatment in patients with EGFR -mutated advanced lung cancer , Therapeutic Advances in Medical Oncology, 10.1177/17588359241312143, 17, (2025).
- Angie Raad, Maria Rizzo, Katherine Appiah, Isabella Kearns, Luis Hernandez, Critical Examination of Modeling Approaches Used in Economic Evaluations of First-Line Treatments for Locally Advanced or Metastatic Non-Small Cell Lung Cancer Harboring Epidermal Growth Factor Receptor Mutations: A Systematic Literature Review, PharmacoEconomics, 10.1007/s40273-024-01362-2, 42, 5, (527-568), (2024).
- Rodrigo Motta-Guerrero, Alejandro Leon Garrido-Lecca, Virgilio E. Failoc-Rojas, Ana Calle-Villavicencio, Robert Villacorta-Carranza, Yesenia Huerta-Collado, Alicia Torres-Mera, Mario J. Valladares-Garrido, Víctor Rivera-Francia, Carlos Carracedo, Luis Raez, Effectiveness and safety of the bevacizumab and erlotinib combination versus erlotinib alone in EGFR mutant metastatic non-small-cell lung cancer: systematic review and meta-analysis, Frontiers in Oncology, 10.3389/fonc.2023.1335373, 13, (2024).
- Alejandro Vila Pérez, Emilio J. Alegre-del Rey, Silvia Fénix-Caballero, Zuzana Špacírová, Petra Rosado Varela, Antonio Olry de Labry Lima, Economic evaluation of adjuvant therapy with osimertinib in patients with early-stage non–small cell lung cancer and mutated EGFR, Supportive Care in Cancer, 10.1007/s00520-023-08239-8, 32, 1, (2023).
- Mousa Alali, Maher Saifo, Optimizing the Treatment for Advanced Non–Small-Cell Lung Cancer with Mutated Epidermal Growth Factor Receptor in Low-Income Countries: A Review, Journal of Immunotherapy and Precision Oncology, 10.36401/JIPO-22-29, 6, 3, (140-149), (2023).
- Yamin Shu, Yufeng Ding, Xucheng He, Yanxin Liu, Pan Wu, Qilin Zhang, Cost-effectiveness of osimertinib versus standard EGFR-TKI as first-line treatment for EGFR-mutated advanced non-small-cell lung cancer in China, Frontiers in Pharmacology, 10.3389/fphar.2022.920479, 13, (2022).
- Joo-Young Byun, Sun-Kyeong Park, Boon Peng Ng, Yi-Shao Liu, Chae-Rin Kim, Chanhyun Park, A systematic review of economic evaluations of tyrosine kinase inhibitors for non-small cell lung cancer (NSCLC), Expert Opinion on Pharmacotherapy, 10.1080/14656566.2022.2095203, 23, 11, (1247-1257), (2022).
- Haijing Guan, Chunping Wang, Chen Chen, Sheng Han, Zhigang Zhao, Cost-Effectiveness of 12 First-Line Treatments for Patients With Advanced EGFR Mutated NSCLC in the United Kingdom and China, Frontiers in Oncology, 10.3389/fonc.2022.819674, 12, (2022).
- Shahin Nargesi, Zeinab Dolatshahi, Aziz Rezapour, Vahid Alipour, Aghdas Souresrafil, Hiro Farabi, Seyed Arash Javadmoosavi, Mandana Safakhah, Najmeh Moradi, Cost-effectiveness of osimertinib in the treatment of advanced EGFR-mutated non-small cell lung cancer: a systematic review, Expert Review of Pharmacoeconomics & Outcomes Research, 10.1080/14737167.2022.2011721, 22, 4, (543-554), (2021).