Multi-gene assays: effect on chemotherapy use, toxicity and cost in estrogen receptor-positive early stage breast cancer
Abstract
Aim: To assess multi-gene assay (MGA) effects on chemotherapy use, toxicities, recurrences, and costs in estrogen receptor-positive early breast cancer. Methods: Meta-analysis performed using data from public databases. Results: Studies included 12,202 women. Relative to no testing, chemotherapy use was higher with 12-gene and 70-gene and lower with PAM50 (commercial) and 21-gene MGAs. Overall, 1643 distant recurrences occurred with no testing, declining by 231 (21-gene), 121 (70-gene), 54 (12-gene) and 94 (PAM50); only the 21-gene assay resulted in no risk of increasing the number of distant recurrences. Relative to ‘no testing’, total cost of care declined only with 21-gene MGA. Conclusion: MGAs differ in chemotherapy use and related outcomes for women with estrogen receptor-positive early breast cancer.
The conventional approach to selecting adjuvant chemotherapy for women with estrogen receptor-positive (ER+) early stage breast cancer is to consider tumor size (pT1-pT3, >0.5 cm), nodal status (pN0 or pN1mi) and results of a multi-gene assay (MGA) [1,2]. Decisions guided by MGAs may potentially spare some patients from the toxic effects that are associated with chemotherapy (e.g., secondary cancers, neurotoxicity and cardiotoxicity) [3–7], while also identifying patients who are most likely to benefit from chemotherapy (i.e., those who are at high risk of distant recurrence). For example, when considering the results from MGAs, low scores could result in a lower rate of chemotherapy use, while high scores could result in higher rate of chemotherapy use.
The most recent (2018) NCCN Guidelines® recognize several MGAs for consideration of adjuvant systemic chemotherapy, including the 21-gene Recurrence Score® test (Oncotype DX Breast Recurrence Score®, Genomic Health, Inc., CA, USA), the 70-gene signature using microarray technology (MammaPrint®, Agendia, CA, USA), the commercial PAM50 risk of recurrence (ROR; Prosigna®, NanoString Technologies, Inc., WA, USA) and the 12-gene molecular score (EndoPredict®, Myriad Genetics, UT, USA) [2]. All four assays have been validated in studies that satisfy Simon Category B study quality for prognosis-only assays [8]. Additionally, the results of a retrospective analysis of the National Surgical Adjuvant Breast and Bowel Project (NASBP) B-20 randomized trial also found that high 21-gene Recurrence Score results predicted benefit of the addition of chemotherapy to endocrine therapy on the rate of distant recurrence [9], satisfying Simon Category B study quality for a predictive assay, and the 21-gene assay is recognized as predictive of recurrence risk in the NCCN guidelines in node-negative breast cancer [2]. The most recent NCCN Guidelines also strongly consider use of the 21-gene test in node-negative, hormone receptor-positive, HER2-negative disease [2]. The randomized, controlled Microarray In Node negative Disease may Avoid ChemoTherapy (MINDACT) trial of the 70-gene assay revealed different rates in distant recurrence when women were stratified by clinical risk and genomic risk [10].
Comparative differences across MGAs on chemotherapy utilization and effects on risks of toxicities, medical resource use or costs have not been systematically studied. The primary aim of this study was to summarize the available literature on use of chemotherapy by MGA (21-gene, 70-gene, 12-gene and PAM50 [commercial]) results score (low, intermediate or high) based on a systematic review and meta-analysis to assess the proportions of women experiencing distant recurrence and on chemotherapy-related toxicity and adverse events and costs.
Methods
The study was a cost–effectiveness analysis, using decision-theoretical principles, from the perspective of a third-party US payer. We applied the principles described by the joint International Society for Pharmacoeconomics and Outcomes Research and Society for Medical Decision Making (ISPOR-SMDM) Task Force guidelines for Modeling Good Research Practices [11], and the Second Panel on Cost–Effectiveness in Health and Medicine [12]. The overall study design is shown in Figure 1.

Figure 1. Study design.
ER: Estrogen receptor; ISPOR-SMDM: International Society for Pharmacoeconomics and Outcomes Research-Society for Medical Decision Making; MGAs: Multi-gene assay.
We summarized effects of MGAs on distant recurrence as reported from randomized trials and registries, and commonly cited in other assessments. The incidence of acute care visits (emergency department visits and hospitalizations) and secondary cancer following chemotherapy were based on reports of registries and records of a large regional US health plan (Humana, KY, USA). Costs of chemotherapy regimens and supportive care were based on 2018 published price indices [13]. Past prices, when applicable, were brought into current US dollars (2018), using Personal Health Care Expenditure deflator developed by the Centers for Medicare and Medicaid Services [14].
Multi-gene assays
Four MGAs were used in the analysis: the 70-gene signature test, PAM50 (commercial) ROR, the 12-gene molecular score and the 21-gene Recurrence Score test. Interpretation of results for ROR in patient with node-negative status, per the instructions for the individual MGAs, are as follows: 21-gene Recurrence Score result: low risk (<18), intermediate risk (18–30) and high risk (≥31); 70-gene score result: low risk and high risk; PAM50 ROR result: low risk (0–40), intermediate risk (41–60) and high risk (61–100) and 12-gene result: low risk (<3.3287) and high risk (>3.3287) [2,15].
Effects of MGA testing on chemotherapy use
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for undertaking a systematic review of published literature on use of chemotherapy, stratified by MGA result (e.g., a score of low, intermediate or high risk; or a score of low or high risk) [16]. The PICO criteria, search terms and strategy are detailed in Supplementary Table 1. We assessed study quality according to the methods set out in the Cochrane Handbook for Systematic Reviews of Interventions, and the Cochrane tool for assessing risk of bias [17]. We graded each study for low, high or unclear bias, per Cochrane's definitions.
Studies of the effects of MGA testing on chemotherapy use were summarized using meta-analysis regression, adjusting for study differences by study year, academic setting, country, tumor size and grade. A systematic computerized search of electronic databases including PubMed, Embase, Google Scholar and Cochrane Library up to May 2018 was carried out. The search used the following keywords: ‘12-gene’; ‘21-gene’; ‘70-gene’; ‘breast cancer’; ‘clinical utility’; ‘decision impact’; ‘EndoPredict’; ‘EPClin’; ‘MammaPrint’; ‘Oncotype’; ‘PAM50’; ‘Recurrence Score’; ‘Prosigna’; and ‘ROR’. We searched each citation using the Web of Science Core Collection to identify other studies that may be eligible for inclusion.
Eligible studies had to meet the following inclusion criteria: conducted in patients with early stage breast cancer; met at least one of the following filters: ‘clinical study’; ‘clinical trial’; ‘clinical trial: Phase IV’; ‘comparative study’; ‘controlled clinical trial’; ‘evaluation study’; ‘meta-analysis’; ‘observational study’; ‘randomized controlled trial’; had chemotherapy use data based on actual patients and not hypothetical case studies; had data on the proportion of actual patients who would be recommended to have chemotherapy prior to MGA testing and on recommended or actual use of chemotherapy after MGA testing and articles were written in English. We excluded studies that compared current use of chemotherapy after testing with historical patterns of chemotherapy published in the literature.
All investigators had access to the research literature and to the data-extraction report form. Data extraction was carried out independently by one investigator (J Hornberger) and verified by another (M Turner). Discordant cases were reviewed and resolved (L Hochheiser). The extracted data fields include first author's name, year of publication, years of data collection, country, setting (academic, community, both), design (single-arm pre/post, 2-arm concurrent), number of patients, age (mean or median), MGA used and mean tumor size. We also extracted information on the proportion of patients by nodal status (node negative, micrometastases), tumor size <2 cm, tumor grade (I, II, III), ER+, PR+, MGA risk status (low, intermediate or high; and low or high), and recommended chemotherapy without (or before) and with (or after) MGA testing and stratified by risk category. Patients with node-positive status were excluded from the analyses.
Relative reduction in distant recurrence
The relative reduction of distant recurrence with chemotherapy was stratified by risk group for each MGA. We used data published on the relative reduction of 10-year distant recurrence when feasible. This approach was possible for results of the 12-gene, PAM50 and 21-gene tests. The relative reduction for results of the 70-gene test was available for only the past 5 years, and we extrapolated with an exponential hazard rate to 10 years.
The relative reduction of distant recurrence with chemotherapy by 21-gene Recurrence Score risk group was based on Paik et al. [9]. The reduction was 0% if low risk, 36% if intermediate risk and 79% if high risk. The Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) meta-analysis provided commonly cited rates for distant recurrence that were used in assessment of the 12-gene and PAM50 ROR scores [18]. The relative reduction was set to 30% for all risk groups [19]. For the 70-gene test, we utilized published results from the MINDACT trial, which provided 5-year rate of distant metastasis-free survival (DMFS) for patients who had discordant clinical risk as assessed by Adjuvant! Online (www.adjuvantonline.com) and genomic risk by 70-gene signature score and were subsequently randomized to receive chemotherapy or no chemotherapy, based on the results of either clinical or genomic risk [10]. In MINDACT, the relative risk of chemotherapy on 5-year DMFS for clinical high risk and the 70-gene score low-risk result was 0.69 (95% CI: 0.39–1.21; p = 0.193). The relative risk of chemotherapy on 5-year DMFS for clinical low risk and 70-gene score high-risk result was 1.09 (95% CI: 0.54–2.19; p = 0.815) [10]. Evidence on the rate of chemotherapy if clinical and 70-gene risk results were both high or were both low was not reported. In the absence of evidence for the effect of chemotherapy in concordant cases, we generalized the effect of the discordant patients to the respective 70-gene signature score risk result. In other words, we assume 0% benefit of chemotherapy if the 70-gene score result indicated low risk and 31% benefit if it indicated high risk (‘31%’ calculated as the inverse 0.69 relative risk reduction × 100).
Rate of acute care visits following adjuvant chemotherapy
There are many available adjuvant chemotherapy regimens; however, our analysis included the following based on the availability of utilization and adverse event data from Ruddy et al., in which records of 8621 women with early stage breast cancer from the OptumLabs Data Warehouse (OLDW) were used to assess hospitalizations and emergency department visits over 2 years in patients receiving four contemporary adjuvant chemotherapy regimens between 2008 and 2014 [20]: doxorubicin + cyclophosphamide; doxorubicin + cyclophosphamide, followed or preceded by docetaxel or paclitaxel; doxorubicin + cyclophosphamide, concurrent with docetaxel or paclitaxel; docetaxel + cyclophosphamide (TC); dose-dense doxorubicin + cyclophosphamide + paclitaxel; and cyclophosphamide, methotrexate, with 5-flourauracil. The OLDW contains more than 100 million privately insured and Medicare Advantage enrollees throughout the US, medical claims for professionals and facility claims for individuals enrolled in the medical health plans. The study involved analysis of pre-existing, de-identified data that underwent approval by the Mayo Clinic Institutional Review Board. We additionally explored the published literature for the most contemporary reports by large US health plans on use of these regimens and regimen-specific incidence of toxicities and secondary cancers.
To determine the rate of acute care visits following adjuvant chemotherapy, from Ruddy et al. we extracted the average rates and ranges for sensitivity analyses (95% CIs) of acute care visits per 100 patients adjusted by age, race, region, surgery type, year of chemotherapy start and number of chronic conditions. Data from the OLDW found 55% of patients received docetaxel + cyclophosphamide, 35% received doxorubicin + cyclophosphamide followed or preceded by docetaxel or paclitaxel, 7% received doxorubicin + cyclophosphamide concurrent with docetaxel or paclitaxtel and 4% received doxorubicin + cyclophosphamide (Supplementary Table 2). The model utilized an average rate of 43% for emergency department visits and 23% for hospitalizations within 24 months of chemotherapy initiation (Supplementary Table 3).
Rate of secondary cancers following adjuvant chemotherapy
Rosenstock et al. accessed records of 92,110 women with early breast cancer from the SEER–Medicare and the Texas Cancer Registry–Medicare linked databases [21]. We extracted their estimates of 8-year cumulative incidence of acute myelogenous leukemia (AML) and myelodysplastic syndrome (MDS). From the SEER database, the incidence of AML/MDS at 8 years was 1.13% with docetaxel + cyclophosphamide, compared with 3.14% with doxorubicin + cyclophosphamide, 2.39% with doxorubicin + cyclophosphamide followed or preceded by docetaxel or paclitaxel and 2.39% with doxorubicin + cyclophosphamide concurrent with docetaxel or paclitaxel. The average 8-year incidence was 1.73% when we applied the distribution of chemotherapy use from OLDW; the rate without chemotherapy was 1.56%.
Costs
Unit cost of each drug was based on national fee schedules [13]. Use and unit costs of anti-emetics and supportive growth factors were based on data from large regional health plan [22]. The cost of acute care visits was estimated to be US$1180 without chemotherapy and US$5447 with chemotherapy, for a net difference of US$4267 [23–26]. The average net 8-year incidence of AML/MDS resulting from chemotherapy for early stage breast cancer was 1 in 590 who receive chemotherapy, and the associated direct medical cost is US$40,000 for MDS and US$227,287 for AML [27,28]. Cost of distant recurrence included traditional chemotherapy for relapsed disease based on SEER-Medicare costs [19], the additional cost of using CDK4/6 inhibitors [28] and cost of terminal phase case care [29–33].
Analysis
Descriptive statistics were produced on all variables extracted from the published studies of the effect of MGAs on the proportion of patients recommended/assigned chemotherapy. See Supplementary Material for details on meta-analyses conducted to assess the change in use of chemotherapy based on test and risk class.
The effects of MGA on chemotherapy use were added to an existing decision-analytical framework of the effect over 25 years of MGA guided-treatment decisions on a cohort of patients’ incidence of distant recurrence, chemotherapy toxicities, secondary cancers and on direct medical costs [22]. The cumulative incidence of distant recurrence was estimated using state-transition modeling, accounting for censoring due to death from any cause. The cumulative incidence of secondary cancers was estimated using a separate state-transition model, also accounting for censoring due to death. The rate of acute care visits in the first 2 years due to chemotherapy was based on frequency methods. The primary end point of the analysis included proportion of chemotherapy use with MGA. Secondary end points included distant recurrence, the number of patients with chemotherapy related acute care visits, the rate of secondary cancers, and care related to chemotherapy, acute care visits and disease progression. Assumptions for base case values, range, distributions and all data sources are shown in Table 1. Outcomes and costs are computed for a 2 million-member US health plan. Sensitivity analysis (deterministic and multivariable probabilistic) were performed. Bayesian 95% CIs were estimated for the effect of MGAs on avoidance of distant recurrence relative to no testing. All future costs and outcomes were discounted at a fixed annual rate of 3% [11]. Meta-analysis of studies of MGA use were conducted using StataIC 15.2 (STATACORP, LLC, TX, USA). The decision-analytical model was constructed in Microsoft® Excel® 2016 MSO, using proprietary Visual Basic for Applications routines for sensitivity analyses.
| Parameter | Base-case value | Range | Distribution | Data source(s) | Ref. | |
|---|---|---|---|---|---|---|
| Low | High | |||||
| Population size | 2,000,000 | 878,728 | 4,552,033 | LogNormal | Assumption | |
| Incidence of pN0, ER+, HER2−ESBC (per 100,000 women) | 52 | 48 | 55 | Normal | American Cancer Society, Howlader | [34,35] |
| Growth rate of population | 0.70% | 0.30% | 1.00% | Normal | The World Bank | [36] |
| Costs | ||||||
| Chemotherapy drugs, adjuvant | US$4297 | US$3958 | US$4666 | LogNormal | Fee schedules† | |
| Supportive care, adjuvant | US$10,986 | US$10,119 | US$11,928 | LogNormal | Fee schedules† | |
| Chemotherapy administration, adjuvant | US$1159 | US$1067 | US$1258 | LogNormal | Fee schedules† | |
| Hospitalizations | US$22,000 | US$18,663 | US$25,933 | LogNormal | Blumen, Rashid, Hurvitz, Wong | [23,26] |
| Emergency department visits | US$800 | US$679 | US$943 | LogNormal | Blumen, Rashid, Hurwitz, Wong | [23,26] |
| AML | US$227,287 | US$163,570 | US$315,824 | LogNormal | Irish, Pan | [27,28] |
| Myelodysplastic syndrome | US$46,000 | US$39,023 | US$54,224 | LogNormal | Irish, Pan | [27,28] |
| Chemotherapy drugs after recurrence – CDK4/6i | US$60,000 | US$55,263 | US$65,143 | LogNormal | Howard | [37] |
| Chemotherapy drugs after recurrence – non-CDK4/6i | US$56,333 | US$54,510 | US$58,217 | LogNormal | Chandler | [19] |
| Terminal phase care, breast-cancer specific mortality | US$80,000 | US$73,684 | US$86,858 | LogNormal | Chastek, Chandler | [19,29] |
| Terminal phase care, non-breast-cancer specific mortality | US$10,000 | US$9210 | US$10,857 | LogNormal | Chastek | [29] |
| Probability of breast-cancer specific mortality after recurrence | 0.9 | 0.86 | 0.95 | Kim, Ren, Tsuji, Zeichner | [30,31,32,33] | |
| Ratio of acute care visits, chemotherapy vs no chemotherapy | 0.22 | 0.21 | 0.22 | Beta | Enright | [38] |
| Incidence of events | ||||||
| − Hospitalizations, with chemotherapy | 0.23 | 0.2 | 0.27 | LogNormal | Ruddy | [20] |
| − Emergency department visits, with chemotherapy | 0.43 | 0.42 | 0.44 | LogNormal | Ruddy | [20] |
| − AML, no chemotherapy | 0.59 | 0.49 | 0.67 | Normal | Rosenstock | [21] |
| Myelodysplastic syndrome, no chemotherapy | 1.56 | 1.36 | 1.72 | Normal | Rosenstock | [21] |
| Relative risk if chemotherapy | ||||||
| − AML | 1.35 | 1.24 | 1.46 | LogNormal | Rosenstock | [21] |
| − Myelodysplastic syndrome | 1.72 | 1.58 | 1.87 | LogNormal | Rosenstock | [21] |
| Probability of recurrence if no chemotherapy (10 year) | ||||||
| 21-gene Recurrence Score | ||||||
| − Low risk | 7% | 5% | 9% | Beta | Paik | [9] |
| − Intermediate risk | 11% | 9% | 13% | Beta | Paik | [9] |
| − High risk | 30% | 28% | 32% | Beta | Paik | [9] |
| PAM50 (commercial) ROR | ||||||
| − Low | 7% | 5% | 9% | Beta | EBCTCG | [18] |
| − Intermediate risk | 5% | 3% | 7% | Beta | EBCTCG | [18] |
| − High risk | 30% | 28% | 32% | Beta | EBCTCG | [18] |
| 12-gene risk score | ||||||
| − Low risk | 7% | 5% | 9% | Beta | EBCTCG | [18] |
| − High risk | 15% | 13% | 17% | Beta | EBCTCG | [18] |
| 70-gene signature risk score | ||||||
| − Low risk | 7% | 5% | 9% | Beta | Cardoso | [10] |
| − High risk | 14% | 12% | 16% | Beta | Cardoso | [10] |
| Relative ROR (chemotherapy vs no chemotherapy) | ||||||
| 21-gene recurrence score | ||||||
| − Low risk | -0.31 | -0.36 | -0.27 | Normal | Paik | [9] |
| − Intermediate risk | 0.39 | 0.34 | 0.43 | Normal | Paik | [9] |
| − High risk | 0.74 | 0.69 | 0.78 | Normal | Paik | [9] |
| PAM50 (commercial) ROR | ||||||
| − Low risk | 0.3 | 0.25 | 0.34 | Normal | EBCTCG | [18] |
| − Intermediate risk | 0.3 | 0.25 | 0.34 | Normal | EBCTCG | [18] |
| − High risk | 0.3 | 0.25 | 0.34 | Normal | EBCTCG | [18] |
| 12-gene risk score | ||||||
| − Low risk | 0.3 | 0.25 | 0.34 | Normal | EBCTCG | [18] |
| − High risk | 0.3 | 0.25 | 0.34 | Normal | EBCTCG | [18] |
| 70-gene signature risk score | ||||||
| − Low risk | 0 | -0.05 | 0.04 | Normal | Cardoso | [10] |
| − High risk | 0.31 | 0.26 | 0.35 | Normal | Cardoso | [10] |
| Fixed annual time discount rate | 3% | 0% | 5% | Uniform | Caro | [11] |
†Redbook (WAC/AWP), CMS fee schedule (ASP), VAFSS, NADAC.
ASP: Average sales price; AML: Acute myelogenous leukemia; AWP: Average wholesale price; CMS: Centers for Medicare & Medicaid Services; EBCTCG: Early Breast Cancer Trialists’ Collaborative Group; ER+: Estrogen receptor-positive; ESBC: Early stage breast cancer; HER2-: Human epidermal growth factor receptor-negative; NADAC: National Average Drug Acquisition Cost; pN0: No regional lymph node metastasis identified histologically; ROR: Risk of recurrence; VAFSS: Veterans Affairs Federal Supply Schedule Service; WAC: Wholesale average cost.
Results
Meta-analysis of decision impact
The electronic literature searches identified a total of 43 papers. Twelve papers were omitted because they lacked sufficient information about chemotherapy use stratified by risk group. We extracted detailed information from the final 31 papers (Figure 2; Supplementary Table 4). Studies included 12,202 women with recurrence score results using the 21-gene (n = 10,501, 86% [25 studies]), 70-gene (n = 960, 8% [2 studies]), PAM50 (n = 592, 5% [3 studies]) and 12-gene (n = 149, 1% [1 study]) assays. The mean cohort age was 55.7 years (standard deviation [SD] 4.7 years). Across all studies, tumor size was <2 cm in 68% (SD 13%) of women, and tumor was grade I in 22% (SD 10%) of women and grade II in 59% (SD 10%) of women. 84% of tumors (SD 7%) were PR+.

Figure 2. Systematic literature search.
CT: Chemotherapy; EP: EndoPredict; ER+: Estrogen receptor-positive; ESBC: Early stage breast cancer; MGA: Multi-gene assay; MMP: MammaPrint; ROR: Risk of recurrence; RS: Recurrence Score.
Proportion of chemotherapy use with MGA
Chemotherapy use using just clinicopathological features without MGA testing was 39.9% (n = 6,374; 95% CI: 39.5–40.4%) for low-risk women, 44.5% (n = 3,987; 95% CI: 44.0–45.1%) for intermediate-risk women and 50.0% (n = 1,841; 95% CI: 49.3–50.6%) for high-risk women (Figure 3A). Among all MGAs, chemotherapy use with MGA testing declined for patients identified as low risk and increased for patients identified as high risk. For two MGAs (12-gene and 70-gene assays), women were nearly evenly distributed between low and high risk (Figure 3B); fewer women were identified as high risk by the results of either the PAM50 or 21-gene assays. Unlike the results of the 12-gene and 70-gene assays, the PAM50 and 21-gene assays also include an intermediate risk group; use of chemotherapy was 40–45% among women in the intermediate-risk group.

Figure 3. Chemotherapy use before and after MGA testing.
(A) Probability of chemotherapy use before MGA testing, by risk group. (B) Probability of chemotherapy use after MGA testing, by MGA test. (C) Ratio of chemotherapy use with and without MGA testing, by MGA test.
CI: Confidence interval; MGA: Multi-gene assay.
Relative to no testing, significantly higher chemotherapy use was shown for patients who utilized the 70-gene assay (ratio 1.05; 95% CI: 1.01–1.11), no significant effect on chemotherapy use was shown for patients who utilized the 12-gene assay (ratio 0.94; 95% CI: 0.84–1.10) (Figure 3C) and a statistically significant reduction in chemotherapy use was shown for patients who utilized the PAM50 (ratio 0.88; 95% CI: 0.84–0.93) and 21-gene (ratio 0.76; 95% CI: 0.76–0.78) assays.
Distant recurrence
We show by MGA the rates of acute care use and distant recurrence, and the costs for chemotherapy use, management of distant recurrence, MGA testing, chemotherapy-related acute care and secondary cancers (Table 2). For a 2 million-member plan, no MGA testing results in 43% use of chemotherapy in 14,275 incident women, with an expected 1643 distant recurrences over 25 years. Chemotherapy-related acute care events with no MGA testing are expected in 5245 women (hospitalizations: 1836; emergency department visits: 3409). 484 secondary cancers are expected from chemotherapy.
| No testing | 12-gene assay | 70-gene assay | 21-gene assay | PAM50 (commercial) assay | |
|---|---|---|---|---|---|
| Chemotherapy use | 43% | 42% | 46% | 33% | 38% |
| Number of patients | |||||
| − Patient with recurrence | 1643 | 1589 | 1540 | 1412 | 1549 |
| − Hospitalization | 1836 | 1805 | 1903 | 1579 | 1702 |
| − Emergency department | 3409 | 3351 | 3534 | 2931 | 3160 |
| − AML | 122 | 121 | 123 | 118 | 120 |
| − Myelodysplastic syndrome | 363 | 360 | 368 | 343 | 106 |
| Cost (USD) | |||||
| − MGA test | − | $55,286,359 | $55,286,359 | $55,286,359 | $44,237,652 |
| − Recurrence | $310,996,430 | $300,829,022 | $291,580,009 | $267,254,154 | $293,230,449 |
| Chemotherapy-related | |||||
| − Chemotherapy regimen† | $101,260,408 | $98,425,117 | $107,336,033 | $77,970,514 | $89,109,159 |
| − Hospitalization | $40,394,736 | $39,705,419 | $41,871,844 | $34,732,489 | $37,440,520 |
| − Emergency department | $2,727,416 | $2,680,873 | $2,827,148 | $2,345,106 | $2,527,950 |
| − AML | $17,160,647 | $17,098,138 | $17,294,594 | $16,647,184 | $16,892,753 |
| − Myelodysplastic syndrome | $10,347,874 | $10,280,237 | $10,492,811 | $9,792,284 | $10,058,001 |
| Total cost | $482,887,510 | $524,305,166 | $526,688,797 | $464,028,091 | $493,496,484 |
| Difference relative to no testing | |||||
| − Chemotherapy use | -1% | +3% | -10% | -5% | |
| − Patients with recurrence | -54% | -103% | -231% | -94% | |
| − Total costs | +$41,417,655 | +$43,801,287 | -$18,859,420 | +$10,608,974 | |
†Includes chemotherapy drugs, administration and supportive care drugs.
AML: Acute myelogenous leukemia; MGA: Multi-gene assay; USD: United States dollar.
Distant recurrences show a decline with use of MGAs, sparing 54 women tested with the 12-gene assay (the lowest effect) to 231 women tested with 21-gene assay (the highest effect). In all, 1643 distant recurrences occurred with no testing. The number of distant recurrences relative to no testing avoided was 231 (95% CI: 80–663) with the 21-gene assay, 121 (95% CI: -180–585) with the 70-gene assay, 54 (95% CI: -294–480) with the 12-gene assay and 94 (95% CI: -198–610) with the PAM50 (commercial) assay. The 21-gene assay was the only MGA in which 100% of simulations reduced the number of distant recurrences relative to no testing (Supplementary Figure 1). The effect of MGAs on number of women experiencing chemotherapy-related acute care events and secondary cancers directly correlated with the effect on chemotherapy use. Hence, these events increased with use of the 70-gene assay, were unchanged with use of the 12-gene assay and decreased with use of the PAM50 and 21-gene assays.
Costs
The Medicare average sale price for all elements of doxorubicin + cyclophosphamide concurrent with docetaxel or paclitaxel was $3967, compared with $1799 for doxorubicin + cyclophosphamide, $1976 for doxorubicin + cyclophosphamide followed or preceded by docetaxel or paclitaxel and $2553 for docetaxel + cyclophosphamide (Supplementary Table 5). The average across all regimens was $7708. Intravenous administration cost was $1103, and cost of supportive products was $9731. Summing across all cost categories, the Medicare average cost of chemotherapy was $22,979, increasing to an average of $26,081 for non-Medicare combined costs.
The total cost of care with no MGA testing was $482.9M (average of $33,827 per woman), with 64% of costs related to management of disease recurrence (Table 2). Chemotherapy drugs, administration and supportive care accounted for 21% of costs.
Utilization of results from all MGAs except the 21-gene assay resulted in increased costs compared with no MGA testing, as shown in Table 2 and in Figure 4. The primary reasons for the observed increased costs is likely associated with the modest effects of utilization of results of the 12-gene, 70-gene and PAM50 assays on reducing chemotherapy use and recurrences. The net savings for 21-gene testing compared with no testing was $18.8M ($1321 per woman), whereas utilization of results of the 12-gene and 70-gene assays increased cost by more than $40M and by more than $10M with use of the PAM50 assay.

Figure 4. Difference in total costs between no testing and MGA testing, by MGA test.
Costs include costs of MGA testing, chemotherapy drug and administration, supportive care, chemotherapy-related acute care visits and secondary cancers and distant recurrences.
MGA: Multi-gene assay; USD: United States dollar.
Cost–effectiveness
When there exist multiple comparators, guidelines recommend the use of the cost–effectiveness plan (Figure 5), which reflects the set of potentially cost-effective strategies that dominate all other strategies directly [12]. In this analysis, the efficient frontier is defined by the line between no MGA testing and the 21-gene assay. Above the efficient frontier, all other comparators are dominated by either no MGA testing OR the 21-gene assay. The 21-gene assay is the only MGA, relative to no testing and all other MGAs, that simultaneously is cost-saving and reduces distant recurrences (i.e., referred to as ‘dominant’ to no MGA testing and to all alternative MGAs).
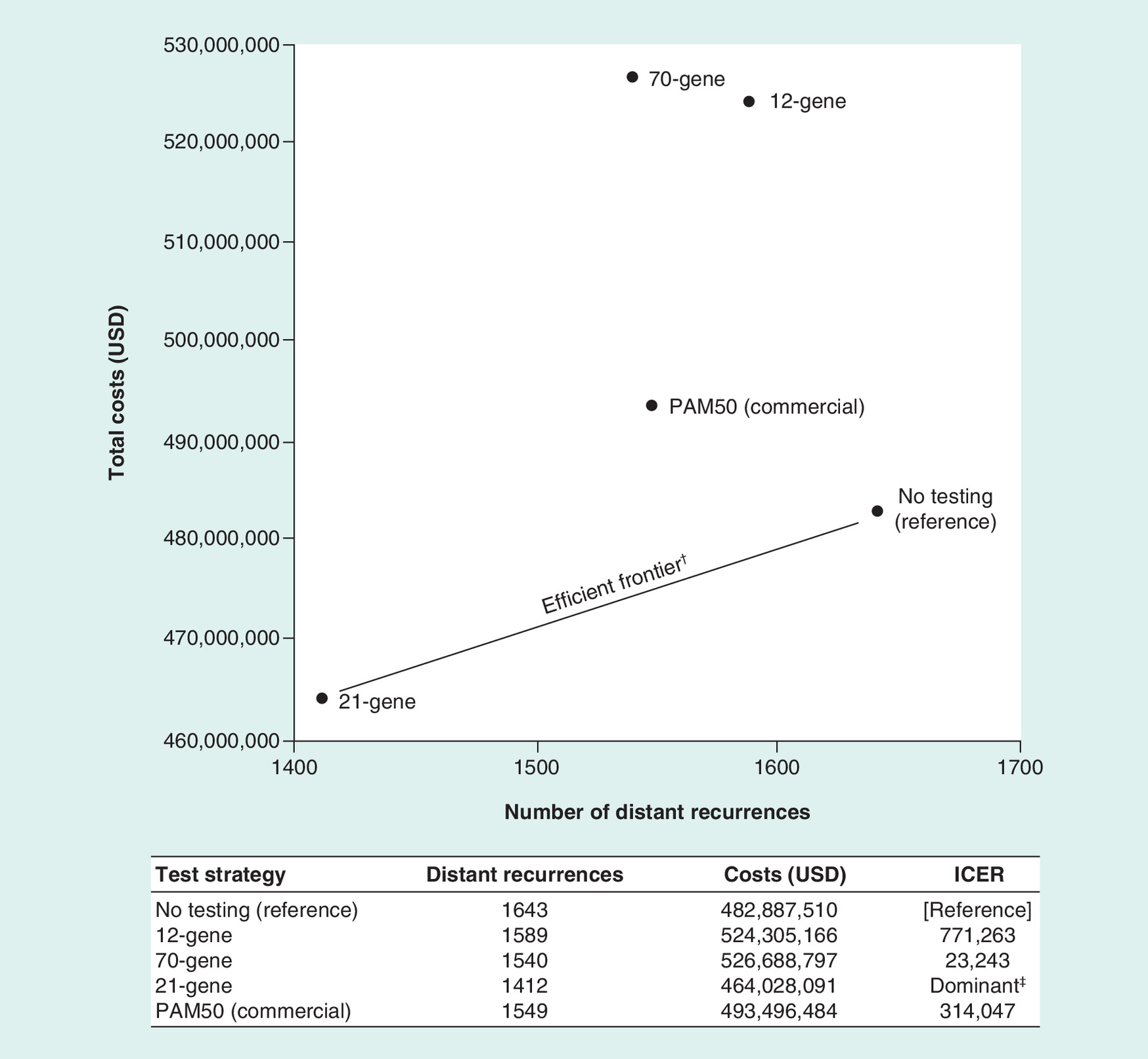
Figure 5. Cost–effectiveness plan: plot of total costs over distant recurrences.
†Efficient frontier: the set of potentially cost-effective strategies that dominate all other strategies directly. The 21-gene test is the only MGA relative to no testing and all other MGAs that simultaneously is cost-saving and reduces distant recurrences (i.e., dominant to no testing and to all alternative MGAs).
‡Dominant: cost-saving relative to no testing and reduces the number of distant recurrences.
ICER: Incremental cost–effectiveness ratio; MGA: Multi-gene assay; USD: United States dollar.
Sensitivity analysis
Deterministic sensitivity analysis showed that the total cost of care was most sensitive to estimates of the cost of MGA testing, the probability of recurrence and the effect of chemotherapy on reducing ROR (Supplementary Figure 2). With increased utilization of the 21-gene test, the proportion of patients receiving chemotherapy are reduced, and more savings accrue. The analyses also were highly sensitive to the cost of treatment for recurrences, cost of supportive care (Supplementary Table 6) and proportion of women tested whose insurance is commercial (Supplementary Table 7). By contrast, the distribution of type of chemotherapy and cost of chemotherapy administration were relatively noninfluential factors (Supplementary Table 8). Multivariable probabilistic sensitivity analysis revealed that only the 21-gene excluded the potential to increase rate of distant recurrence and excluded the potential to increase total costs (Supplementary Figure 1).
Discussion
This study represents a comparative effectiveness analysis (combining evidence from multiple primary and secondary sources of clinical, epidemiology and economic data) of four MGAs to assist women with node-negative, ER+ early stage breast cancer deciding on use of chemotherapy. The end points of the analysis include outcomes salient to the patient's decision-making, such as risk of distant recurrence, hospitalization and emergency room visits for toxicities and secondary cancer. We also examined the overall direct medical costs to a hypothetical 2 million-member health plan. The effect of an MGA on chemotherapy use was based on 31 observational studies performed in diverse settings that satisfied minimum inclusion criteria to draw causal inferences stratified by risk category.
While three of the MGAs demonstrated an increased use of chemotherapy relative to no testing, use of the 21-gene Recurrence Score demonstrated a decrease in chemotherapy utilization. Because the use of chemotherapy is so strongly associated with hospitalizations and emergency department visits in the first 2 years and secondary cancers over at least 8 years, chemotherapy reductions associated with utilization of results of 21-gene testing also reduced the incidence of these events. Based on analysis of the NSABP B-20 trial [9], which established the 21-gene Recurrence Score result as predictive of chemotherapy benefit [9], use of the Recurrence Score would likely resulted in fewer distant recurrences within 10 years of testing. From the perspective of total direct medical costs relative to no testing, three of the MGAs increased costs from $10.6M (PAM50 ROR assay) to $43.8M (70-gene assay) among a health plan with annual enrollment of 2 million members. By contrast, utilization of the 21-gene Recurrence Score result reduced total direct medical costs by $18.9M. In other words, the assay more accurately determines who does not benefit from chemotherapy; hence, physicians and patients can have more confidence in avoiding chemotherapy – as revealed in the change in clinical management studies – and in who will benefit from chemotherapy, which leads to fewer distant recurrences. The extensive sensitivity analyses reveal these findings were robust over a wide range of model inputs.
The current study comparing multiple MGAs with no testing includes three design features that bear noting. First, comparisons for the current analyses were based on a meta-analysis of studies that included actual women who underwent MGA testing (whereas many comparative effectiveness analyses are based on hypothetical patients). We excluded women who were not tested with an MGA based on choices made by the physician about whether to test, such as age, comorbidities or the patient/physician already having decided on use or nonuse of chemotherapy. Other comparative effectiveness studies have included this subset in their analyses [39–41], which may have resulted in mis-estimation of the effects of MGA testing on chemotherapy use because of selection bias. It is argued here that the effects of MGA testing must be assessed in women who receive the test, compared with appropriate controls, also referred to as a counterfactual [42,43]. Pre- and post-assessment of decision making is an accepted approach for evaluation of the impact of an intervention when randomization is neither feasible nor the norm [44]. We also introduced an approach to set a common baseline for use of chemotherapy across MGAs using multivariable regression, controlling for baseline characteristics, such as patient age, year of testing, tumor size, PR status and tumor grade. Relative changes in chemotherapy use by MGA were then computed to obtain unbiased estimates of the amount of chemotherapy utilized by MGA. Other sources of bias were explored as recommended by Hernan et al., to derive the most compelling inferences from observational databases [42]. Third, our drug-cost analyses included various fee schedules from commercial and government databases and accounted for the proportion of women who would be insured by each.
Results of the current study should be interpreted with caution considering the following limitations. First, studies varied in the quality of variable reporting, a not-uncommon challenge of extracting data from peer-review literature. Second, to estimate effect size, we excluded studies that failed to report baseline and change in use of chemotherapy by risk category. Historical controls were not used due to the significant baseline variations between studies, which would have yielded biased estimates, and the descriptive-only nature of noncomparative studies. Lastly, the effects on quality of life associated with use of chemotherapy were omitted that may not lead to hospitalizations. We also omitted extrapolating the effects of secondary cancers and distant recurrence on overall survival, and on quality of life. Finally, we omitted the ‘financial toxicity’ effects to women for out-of-pocket expenditures for chemotherapy and management of toxicities, which may exceed 5–10% of annual income [45,46] and the implications on women's labor-force participation [47,48]. The consequent bias of omitting these outcomes would likely be to underestimate the impact of the cost of the MGA including the costs of the non-21-gene MGAs.
The recently reported Trial Assigning Individualized Options for Treatment, or TAILORx, demonstrated that most women (70% or more) do not benefit from chemotherapy when using the 21-gene Recurrence Score test to guide treatment decisions [49], suggesting that even more patients may be able to avoid adjuvant chemotherapy without adversely effecting outcomes. Based on the results of TAILORx, the 21-gene test has been incorporated into the NCCN guidelines as the preferred test [2] and in the American Joint Committee on Cancer Staging pathological prognostic staging table [2,50]. As such, the results of the current analysis may represent an underestimate of the contemporary effect of the 21-gene test on chemotherapy use and associated cost-savings since the analysis was based on studies that were carried out pre-TAILORx. Further, following the publication of the TAILORx results, it is feasible that physicians and/or women who have been ambivalent about MGA testing in the past may gain increased confidence in testing, with the possibility that the use of chemotherapy may be reduced for women identified as having a low-risk and increase for women identified as having a high-risk 21-gene Recurrence Score result. Additional research will be important to document the impact of TAILORx results on adoption and use of chemotherapy.
Conclusion
In this simulation, rates of chemotherapy de-escalation were shown to differ by type of MGA utilized. The four MGAs affected rates of chemotherapy use differently, with subsequent differences in clinical outcomes and estimated healthcare utilization, demonstrating that the choice of test used carries implications for both the individual patient and for society.
The use of risk of recurrence score results from multi-gene assays (MGAs; 21-gene, 70-gene-12-gene and PAM50 [commercial] assays) on the impact on chemotherapy utilization in patients with estrogen receptor-positive early breast cancer was investigated.
A meta-analysis using data from published clinical trials and publicly available databases of actual patients was performed.
Overall, results from 12,202 patients were included in the analysis, the majority of whom (86.1%) utilized the 21-gene assay to determine recurrence risk.
Overall, utilization of chemotherapy was statistically significantly higher in patients who used the 70-gene assay, not significantly changed in patients who used the 12-gene assay, and statistically significantly reduced in patients who used the PAM50 and 21-gene assays, compared with no testing.
Distant recurrences showed a decline with use of all MGAs, with the greatest decline in patients who utilized the 21-gene assay, followed by the 70-gene, PAM50 and 12-gene assays.
Because of its predictive validation, only the 21-gene assay had a confidence interval that excluded the potential to increase rate of distant recurrence.
The effect of MGAs on the number of women who experienced chemotherapy-related acute care events and secondary cancers directly correlated with the effect on chemotherapy use (events increased with use of the 70-gene assay, were unchanged with use of the 12-gene assay and decreased with use of the PAM50 and 21-gene assays).
Relative to no testing, total cost of care declined only with use of the 21-gene assay.
In all, rates of chemotherapy de-escalation differ by type of MGA utilized and overall, reduced chemotherapy use was associated with avoidance of chemotherapy-related toxicities and secondary cancers, and substantial cost savings to health systems.
Supplementary data
To view the supplementary data that accompany this paperplease visit the journal website at: www.futuremedicine.com/doi/full/10.2217/cer-2018-0137
Author contributions
All authors were involved in the study concept and design; analyzed and interpreted the data, drafted or revised the manuscript for important intellectual content; and provided approval of the final version. J Hornberger and M Turner carried out data analyses. Data extraction was carried out by J Hornberger and verified by M Turner, and discordant cases were reviewed and resolved by L Hochheiser.
Financial & competing interests disclosure
Funding for this research was provided by Genomic Health, Inc. (Redwood City, CA, USA). L Hochheiser is a Consultant for Abbott (providing guidance and direction as part of a Payor Advisory Board) and has been a manuscript consultant to Genomic Health, Inc. J Hornberger and M Turner are full-time employees and stockholders of Genomic Health, Inc. G Lyman has the following disclosure: Leadership: Generex Biotechnology; Research Funding: Amgen (Inst), Hexal; Consulting or Advisory Role: G1 Therapeutics, Halozyme Therapeutics, Partners Healthcare, Hexal, Bristol-Myers Squibb, Helsinn Therapeutics, Amgen, Pfizer, Agendia, Genomic Health, Inc., Celldex (I), and Janssen (I).
Writing, editorial and graphics support for the development of this manuscript were provided by CodonMedical, an Ashfield Company, part of UDG Healthcare plc, funded by Genomic Health, Inc., Redwood City, CA, USA.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_file.docx)
- Download
- 381.57 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Giuliano AE, Edge SB, Hortobagyi GN. Eighth edition of the AJCC cancer staging manual: breast cancer. Ann. Surg. Oncol. 25(7), 1783–1785 (2018).
2.
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Breast Cancer V2.2018 (2018). www.nccn.org/professionals/physician_gls/pdf/breast.pdf.
• NCCN Guidelines v2.2018 provides recommendations for use of multi-gene assays in patients with early stage breast cancer.
3.
Swain SM, Whaley FS, Ewer MS. Congestive heart failure in patients treated with doxorubicin: a retrospective analysis of three trials. Cancer 97(11), 2869–2879 (2003).
4.
Ganz PA, Hussey MA, Moinpour CM et al. Late cardiac effects of adjuvant chemotherapy in breast cancer survivors treated on Southwest Oncology Group protocol s8897. J. Clin. Oncol. 26(8), 1223–1230 (2008).
5.
Azim HA Jr, de Azambuja E, Colozza M, Bines J, Piccart MJ. Long-term toxic effects of adjuvant chemotherapy in breast cancer. Ann. Oncol. 22(9), 1939–1947 (2011).
6.
Smith RE, Bryant J, DeCillis A, Anderson S. National Surgical Adjuvant Breast and Bowel Project Experience. Acute myeloid leukemia and myelodysplastic syndrome after doxorubicin–cyclophosphamide adjuvant therapy for operable breast cancer: the National Surgical Adjuvant Breast and Bowel Project Experience. J. Clin. Oncol. 21(7), 1195–1204 (2003).
7.
Conroy SK, McDonald BC, Smith DJ et al. Alterations in brain structure and function in breast cancer survivors: effect of post-chemotherapy interval and relation to oxidative DNA damage. Breast Cancer Res. Treat. 137(2), 493–502 (2013).
8.
Simon RM, Paik S, Hayes DF. Use of archived specimens in evaluation of prognostic and predictive biomarkers. J. Natl Cancer Inst. 101(21), 1446–1452 (2009).
9.
Paik S, Tang G, Shak S et al. Gene expression and benefit of chemotherapy in women with node-negative, estrogen receptor-positive breast cancer. J. Clin. Oncol. 24(23), 3726–3734 (2006).
•• Provides validation of the 21-gene Recurrence Score result from a cohort of patients in the NSABP B-20 trial (i.e., shows that patients with high-risk scores derived benefit from adjuvant chemotherapy).
10.
Cardoso F, van't Veer LJ, Bogaerts J et al. 70-gene signature as an aid to treatment decisions in early-stage breast cancer. N. Engl. J. Med. 375(8), 717–729 (2016).
11.
Caro JJ, Briggs AH, Siebert U, Kuntz KM. Modeling good research practices-overview: A report of the ISPOR-SMDM Modeling Good Research Practices Task Force-1. Med. Decis. Making 32(5), 667–677 (2012).
12.
Neumann PJ, Sanders GD, Russell LB (Eds). Cost–Effectiveness in Health and Medicine (2nd Edition). Oxford University Press, Oxford, UK (2017).
13.
Levy J, Rosenberg M, Vanness D. A transparent and consistent approach to assess US outpatient drug costs for use in cost–effectiveness analyses. Value Health 21(6), 677–684 (2017).
14.
Dunn A, Grosse SD, Zuvekas SH. Adjusting health expenditures for inflation: a review of measures for health services research in the United States. Health Serv. Res. 53(1), 175–196 (2018).
15.
Martin M, Brase JC, Calvo L et al. Clinical validation of the EndoPredict test in node-positive, chemotherapy-treated ER+/HER2- breast cancer patients: results from the GEICAM 9906 trial. Breast Cancer Res. 16(2), R38 (2014).
16.
Moher D, Liberati A, Tetzlaff J, Altman DG. The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 8(5), 336–341 (2010).
17.
Higgins JPT, Green S (Eds). Cochrane Handbook for Systematic Reviews of Interventions Version 5.2. The Cochrane Collaboration (2017). www.handbook.cochrane.org.
18.
Early Breast Cancer Trialists’ Collaborative Group. Treatment of early breast cancer: A systematic overview of all available randomized trials of adjuvant endocrine and cytotoxic therapy volume 1: worldwide evidence 1985–1990. Oxford University Press, Oxford, UK (1990).
19.
Chandler Y, Schechter CB, Jayasekera J et al. Cost–effectiveness of gene expression profile testing in community practice. J. Clin. Oncol. 36(6), 554–562 (2018).
20.
Ruddy KJ, Van Houten HK, Sangaralingham LR et al. Impact of treatment regimen on acute care use during and after adjuvant chemotherapy for early-stage breast cancer. Breast Cancer Res. Treat. 164(3), 515–525 (2017).
•• Review of records from over 8000 women with early stage breast cancer in order to assess acute care use in patients receiving various chemotherapy regimens over a 24-month period.
21.
Rosenstock AS, Niu J, Giordano SH, Zhao H, Wolff AC, Chavez-Macgregor M. Acute myeloid leukemia and myelodysplastic syndrome after adjuvant chemotherapy: a population-based study among older breast cancer patients. Cancer 124(5), 899–906 (2018).
•• Determination of the risk of developing secondary cancers following adjuvant chemotherapy in patients with breast cancer.
22.
Hornberger BJ, Chien R, Krebs K, Hochheiser L. US insurance program's experience with a multigene assay for early-stage breast cancer. J. Oncol. Pract. 7(3 Suppl.), e38s–e45s (2011).
•• Assessement of the economic implication of the 21-gene assay in community practices from a US payer perspective.
23.
Wong W, Yim YM, Kim A et al. Assessment of costs associated with adverse events in patients with cancer. PLoS ONE 13(4), e0196007 (2018).
24.
Hurvitz S, Guerin A, Brammer M et al. Investigation of adverse-event-related costs for patients with metastatic breast cancer in a real-world setting. Oncologist 19(9), 901–908 (2014).
25.
Rashid N, Koh HA, Baca HC, Lin KJ, Malecha SE, Masaquel A. Economic burden related to chemotherapy-related adverse events in patients with metastatic breast cancer in an integrated healthcare system. Breast Cancer (Dove Med Press) 8, 173–181 (2016).
26.
Blumen H, Fitch K, Polkus V. Comparison of treatment costs for breast cancer, by tumor stage and type of service. Am. Health Drug Benefits 9(1), 23–32 (2016).
27.
Irish W, Ryan M, Gache L, Gunnarsson C, Bell T, Shapiro M. Acute myeloid leukemia: a retrospective claims analysis of resource utilization and expenditures for newly diagnosed patients from first-line induction to remission and relapse. Curr. Med. Res. Opin. 33(3), 519–527 (2017).
28.
Pan F, Peng S, Fleurence R, Linnehan JE, Knopf K, Kim E. Economic analysis of decitabine versus best supportive care in the treatment of intermediate- and high-risk myelodysplastic syndromes from a US payer perspective. Clin. Ther. 32(14), 2444–2456 (2010).
29.
Chastek BB, Harley C, Kallich J et al. Health care costs for patients with cancer at the end of life. J. Oncol. Pract. 8(6), 75s–80s (2012).
30.
Kim H, Choi DH, Park W et al. Prognostic factors for survivals from first relapse in breast cancer patients: analysis of deceased patients. Radiat. Oncol. J. 31(4), 222–227 (2013).
31.
Ren Z, Li Y, Shen T, Hameed O, Siegal GP, Wei S. Prognostic factors in advanced breast cancer: Race and receptor status are significant after development of metastasis. Pathol. Res. Pract. 212(1), 24–30 (2016).
32.
Tsuji W, Teramukai S, Ueno M, Toi M, Inamoto T. Prognostic factors for survival after first recurrence in breast cancer: a retrospective analysis of 252 recurrent cases at a single institution. Breast Cancer 21(1), 86–95 (2014).
33.
Zeichner SB, Ambros T, Zaravinos J et al. Defining the survival benchmark for breast cancer patients with systemic relapse. Breast Cancer (Auckl) 9, 9–17 (2015).
34.
American Cancer Society. Cancer Statitistics Center (2018). https://cancerstatisticscenter.cancer.org.
35.
Howlader N, Altekruse SF, Li CI et al. US incidence of breast cancer subtypes defined by joint hormone receptor and HER2 status. J. Natl Cancer Inst. 106(5), dju055 (2014).
36.
The World Bank. Population growth (annual %) (2018). https://data.worldbank.org/indicator/SP.POP.GROW.
37.
Howard BDH, Chernew ME, Abdelgawad T, Smith GL, Sollano J, Grabowski DC. New anticancer drugs associated with large increases in costs and life expectancy. Health Aff. (Millwood) 35(9), 1581–1587 (2016).
38.
Enright K, Grunfeld E, Yun L et al. Population-based assessment of emergency room visits and hospitalizations among women receiving adjuvant chemotherapy for early breast cancer. J. Oncol. Pract. 11(2), 126–132 (2015).
39.
Ademuyiwa FO, Miller A, O'Connor T et al. The effects of oncotype DX recurrence scores on chemotherapy utilization in a multi-institutional breast cancer cohort. Breast Cancer Res. Treat. 126(3), 797–802 (2011).
40.
Hassett MJ, Silver SM, Hughes ME et al. Adoption of gene expression profile testing and association with use of chemotherapy among women with breast cancer. J. Clin. Oncol. 30(18), 2218–2226 (2012).
41.
Wang S-Y, Dang W, Richman I, Mougalian SS, Evans SB, Gross CP. Cost–effectiveness analyses of the 21-gene assay in breast cancer: systematic review and critical appraisal. J. Clin. Oncol. 36(16), 1619–1627 (2018).
42.
Hernán MA, Hernández-Díaz S, Robins JM. A structural approach to selection bias. Epidemiology 15(5), 615–625 (2004).
43.
Höfler M. Causal inference based on counterfactuals. BMC Med. Res. Methodol. 5, 28 (2005).
44.
Weber AM, van der Laan MJ, Petersen ML. Assumption trade-offs when choosing identification strategies for pre-post treatment effect estimation: an illustration of a community-based intervention in Madagascar. J. Causal Inference 3(1), 109–130 (2016).
45.
Ramsey SD, Bansal A, Fedorenko CR et al. Financial insolvency as a risk factor for early mortality among patients with cancer. J. Clin. Oncol. 34, 980–986 (2016).
46.
Jagsi R, Ward KC, Abrahamse PH et al. Unmet need for clinician engagement regarding financial toxicity after diagnosis of breast cancer. Cancer 124(18), 3668–3676 (2018).
47.
Ekenga CC, Pérez M, Margenthaler JA et al. Early-stage breast cancer and employment participation after 2 years of follow-up: a comparison with age-matched controls. Cancer 124(9), 2026–2035 (2018).
48.
Jagsi R, Abrahamse PH, Lee KL et al. Treatment decisions and employment of breast cancer patients: results of a population-based survey. Cancer 123(24), 4791–4799 (2017).
49.
Sparano JA, Gray RJ, Makower DF et al. Adjuvant chemotherapy guided by a 21-gene expression assay in breast cancer. N. Engl. J. Med. 379(2), 111–121 (2018).
•• Further validatation and refinement of the clinical usefulness of the 21-gene assay in a specified low-risk cohort of women with hormone-receptor–positive, HER2-negative, breast cancer enrolled in TAILORx.
50.
Plichta JK, Ren Y, Thomas SM et al. Implications for breast cancer restaging based on the 8th edition AJCC staging manual. Ann. Surg. (2018) (Epub ahead of print).
Information & Authors
Information
Published In
Copyright
© 2019 Lou Hochheiser.
History
Received: 29 November 2018
Accepted: 24 December 2018
Published online: 21 January 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Multi-gene assays: effect on chemotherapy use, toxicity and cost in estrogen receptor-positive early stage breast cancer. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0137
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Flora Nguyen Van Long, Brigitte Poirier, Christine Desbiens, Marjorie Perron, Claudie Paquet, Cathie Ouellet, Caroline Diorio, Julie Lemieux, Hermann Nabi, First versus second-generation molecular profiling tests: How both can guide decision-making in early-stage hormone-receptor positive breast cancers?, Cancer Treatment Reviews, 10.1016/j.ctrv.2025.102909, 135, (102909), (2025).
- Torsten O Nielsen, Samuel C Y Leung, Nazia Riaz, Anna M Mulligan, Zuzana Kos, Anita Bane, Timothy J Whelan, Ki67 assessment protocol as an integral biomarker for avoiding radiotherapy in the LUMINA breast cancer trial, Histopathology, 10.1111/his.15032, 83, 6, (903-911), (2023).
- Vladislav Berdunov, Ewan Laws, Gebra Cuyun Carter, Roger Luo, Christy Russell, Sara Campbell, Jeremy Force, Yara Abdou, The budget impact of utilizing the Oncotype DX Breast Recurrence Score test from a US healthcare payer perspective, Journal of Medical Economics, 10.1080/13696998.2023.2235943, 26, 1, (973-990), (2023).
- Giuseppe Curigliano, Fatima Cardoso, Michael Gnant, Nadia Harbeck, Judy King, Anne-Vibeke Laenkholm, Frédérique Penault-Llorca, Aleix Prat, PROCURE European consensus on breast cancer multigene signatures in early breast cancer management, npj Breast Cancer, 10.1038/s41523-023-00510-9, 9, 1, (2023).
- Laia Bernet, Pablo Fernández, David Hardisson, Núria Chic, Tomás Pascual, Firmas génicas en el cáncer de mama, Revista de Senología y Patología Mamaria, 10.1016/j.senol.2022.04.007, 35, (S67-S86), (2022).
- Henry L. Gomez, Juan E. Bargallo-Rocha, Roberto J. Billinghurst, Aníbal R. Núñez De Pierro, Federico A. Coló, Lisandro L. B. Gil, Carola Allemand, Ignacio L. McLean, Mauricio Lema-Medina, Fernando Herazo-Maya, Francisco J. Terrier, Raquel G. Cwilich, Mauricio Leon, Silvia G. Falcon, Roberto E. Castaño, Sergio C. Oliveira, Debbie M. Jakubowski, Calvin Chao, Practice-Changing Use of the 21-Gene Test for the Management of Patients With Early-Stage Breast Cancer in Latin America, JCO Global Oncology, 10.1200/GO.21.00008, 7, (1364-1373), (2021).
- André Mattar, Guilherme R. Fonseca, Murilo B. A. Romão, Jorge Y. Shida, Vilmar M. de Oliveira, Maria C. S. Bastos, Fabio Bagnoli, Jose F. Rinaldi, Monica M. Á. Stiepcich, Maria A. L. G. da Silva, Debbie M. Jakubowski, Calvin Chao, Sergio C. Oliveira, Luiz H. Gebrim, Substantial Reduction in Adjuvant Chemotherapy With the Use of the 21-Gene Test to Manage Early Breast Cancer in a Public Hospital in Brazil, JCO Global Oncology, 10.1200/GO.20.00609, 7, (1003-1011), (2021).
- Shuai Liu, Han Li, Qichen Zheng, Lu Yang, Meiyu Duan, Xin Feng, Fei Li, Lan Huang, Fengfeng Zhou, Survival Time Prediction of Breast Cancer Patients Using Feature Selection Algorithm Crystall, IEEE Access, 10.1109/ACCESS.2021.3054823, 9, (24433-24445), (2021).
- Yahiya Y. Syed, Oncotype DX Breast Recurrence Score®: A Review of its Use in Early-Stage Breast Cancer, Molecular Diagnosis & Therapy, 10.1007/s40291-020-00482-7, 24, 5, (621-632), (2020).
- Laura Dormer, Introducing Volume 9 of the Journal of Comparative Effectiveness Research , Journal of Comparative Effectiveness Research, 10.2217/cer-2019-0160, 9, 1, (1-5), (2019).