Treatment of gynecological malignancies: long-term follow-up of health-related quality of life and healthcare costs
Abstract
Aim: To assess long-term health-related quality of life (HRQoL) and treatment-related costs in gynecological cancer patients, and to compare HRQoL between cancer types and to age-standardized general female population. Materials & methods: A prospective 8–10-year follow-up of 218 patients treated in Helsinki University Hospital in 2002–2004. Results: The most common malignancies were uterine, ovarian and cervical cancers. The mean HRQoL scores were 0.880 (baseline), 0.885 (6 months) and 0.884 for survivors in the end of the study. Depression, vitality and sexual activity were impaired at baseline but improved during follow-up. Total secondary healthcare costs during the follow-up averaged EUR 41342. Conclusion: The long-term HRQoL of surviving gynecological cancer patients was good and similar to that of age-standardized general female population.
More than every third individual in the Western World is diagnosed with cancer during their lifetime [1]. Around 170 million years of healthy life were lost worldwide due to cancer in 2008, and 23.6 million new cases of cancer are expected per year by 2030 [2]. The number of cancer survivors will increase as cancer treatments improve. On the other hand, years lived with impaired health-related quality of life (HRQoL) will also increase and costs of treatment escalate [2]. Knowledge of the long-term HRQoL and costs of treatment of cancer patients is essential and will affect a growing population of patients and physicians in the future.
Of gynecological malignancies, uterine cancer is the most common in Western countries as screening programs have curtailed the incidence of cervical cancer. Ovarian cancer is the second most common, and other gynecological cancers (vulvar, vaginal, tubal, gestational trophoblastic) are markedly rarer [2–5]. In Finland (a population of 5.5 million), 1600–1700 gynecological malignancies are diagnosed yearly (1675 in 2014). In 2014, 835 (50%) of these were of uterine, 421 (25%) of ovarian and 174 (10%) of cervical origin [1,6]. These add up to a yearly incidence of 30.1 cases of uterine, 15.2 cases of ovarian and 6.3 cases of cervical cancer per 100,000 Finnish women which is similar to the corresponding incidences for example in the USA (32.3, 13.2 and 7.8) [3].
The therapy of gynecological cancers varies from laparotomy and laparoscopic or robotic surgery to adjuvant radiation, chemotherapy, hormonal therapies and/or other pharmaceutical therapies depending on the type and classification of the malignancy. In the USA, just under 10% of all hysterectomies are carried out due to a malignancy [7]. In Finland, this rate is similar (886 out of 6000 hysterectomies/year [14.8%]) [6].
Both encouraging [8–13] and distressing [14–16] HRQoL results of patients treated for gynecological malignancies have been reported. Sexual activity seems to be the HRQoL aspect that is affected for the longest [10,17,18]. Adjuvant radiotherapy affects HRQoL negatively regarding both bowel [11,19] and bladder function as well as sexual activity [20]. Whether different surgical techniques differ regarding their (cost–) effectiveness, is contradictory [21,22]. Because cancer treatments increase life-years, treatment has often been deemed worthwhile independent of its costs. However, in addition to life expectancy, also the HRQoL is important and it has often been poorly taken into account in cost–effectiveness studies [23–25].
Original long-term HRQoL data of gynecological patients are rare [26]. The aim of this study is to assess the long-term HRQoL and treatment-related costs in patients treated for a gynecological malignancy in a publicly funded, real-world secondary healthcare setting. This information on the development of HRQoL and costs over time after treatment in such a setting should be of interest and useful even though the study design, with no suitable comparators to the treatments given, does not allow proper cost–effectiveness analyses to be carried out.
Materials & methods
As a part of a large, prospective, observational HRQoL and cost study 812 women entering scheduled operative treatment in the Department of Obstetrics and Gynaecology of the Helsinki University Hospital between November 2002 and December 2004 filled in the 15D HRQoL questionnaire. Data on those having benign conditions have been reported earlier [27]. For this long-term follow-up study, 218 patients with any gynecological malignancy and having answered the baseline and 6-month follow-up questionnaires were included. In addition, they answered the 15D HRQoL survey 8–10 years after treatment. All patients received treatment according to the standard clinical treatment protocol used in the hospital at that time. In-between group analyses were done between women with different cancer types and between different types of surgery in order to find out whether these would show a different kind of association with HRQoL.
The 15D is a generic, standardized and self-administered HRQoL instrument that can be used both as a profile and as a single index score measure. The questionnaire includes 15 dimensions: mobility, vision, hearing, breathing, sleeping, eating, speech, excretion, usual activities, mental function, discomfort and symptoms, depression, distress, vitality and sexual activity, with five levels on each. The single index score (15D score), representing the overall HRQoL, on a 0–1 scale (1 = full health, 0 = being dead) and the dimension level values from 1 (= no problems) to 0 (= being dead), are calculated from the questionnaire by using a set of population-based preference or utility weights [28,29]. The minimum clinically important change or difference in the 15D score is estimated to be ±0.015 [30]. The 15D has previously been used and validated extensively in different types of cancer. A recent six-country study ranked the 15D first among the most frequently used generic HRQoL instruments in sensitivity and construct validity in the disease area of cancer [31–34].
To obtain knowledge on how the HRQoL of the study patients differed from that of the general female population, the HRQoL of women at baseline and at follow-ups was compared with that of the age-standardized general female population of the same living area (Helsinki and Uusimaa Hospital District, Finland). At baseline and at 6 months, the population data came from the National Health 2000 Health Examination Survey (Health 2000) [35]. The target population of Health 2000 consisted of individuals aged 18 or over, including people living in institutions. The Survey used a stratified two-stage cluster sampling design. First, mainland Finland was divided into five geographical strata, one of them being the Helsinki and Uusimaa Hospital District. Within each stratum, 16 clusters (health center areas) were selected as the first stage of sampling. The sample size for each cluster was proportional to its target population. At the second stage of sampling, the actual persons (observations) were selected from the computerized population register using systematic random sampling.
At 8–10 years, the population data came from the Health 2011 Health Examination Survey (Health 2011) [36]. The surviving participants of the Health 2000 were invited to participate in the Health 2011 as well, and the sample was supplemented with new invitees to achieve a representative sample at that point in time. A detailed description of the sampling in both surveys can be found elsewhere [37,38].
For this study, the female participants in the age range of the patients were selected from the Surveys (n = 800 from Health 2000 and n = 721 from Health 2011). These samples were then weighted to reflect the age distribution of patients at baseline/6 months (same sample) and 8–10 years, respectively
Healthcare costs comprised of costs of treatment of the malignant disease itself, surveillance visit costs and costs of treatment of cancer-related conditions. Costs were examined from the perspective of the secondary healthcare provider, and only direct costs were taken into account. Cost data were attained for the period of August 2002 to October 2012 from the Ecomed® clinical patient administration database (Datawell Ltd, Espoo, Finland). Costs were inflated to the 2012 price level by using the price index of public health services (Statistics Finland). Clinical consideration was used to assess which conditions were related to the malignancy (Online Resource 1).
Descriptive statistics are reported as means, standard deviations (SD), ranges and percentages. The statistical significance of the changes over time in the mean 15D scores and dimension level values was tested by paired samples t-test. The statistical significance of the difference in the mean 15D score and dimension level values between two unrelated groups was tested by independent samples t-test. Two-sided p-values < 0.05 were considered statistically significant. The data were analyzed using the SPSS for Windows statistical software version 22.0 (SPSS, Inc., IL, USA).
The study protocol was approved by the Ethics Committee of the Helsinki University Central Hospital (registration numbers 26/E6/02 and 195/13/03/03/2012).
Results
Patient characteristics
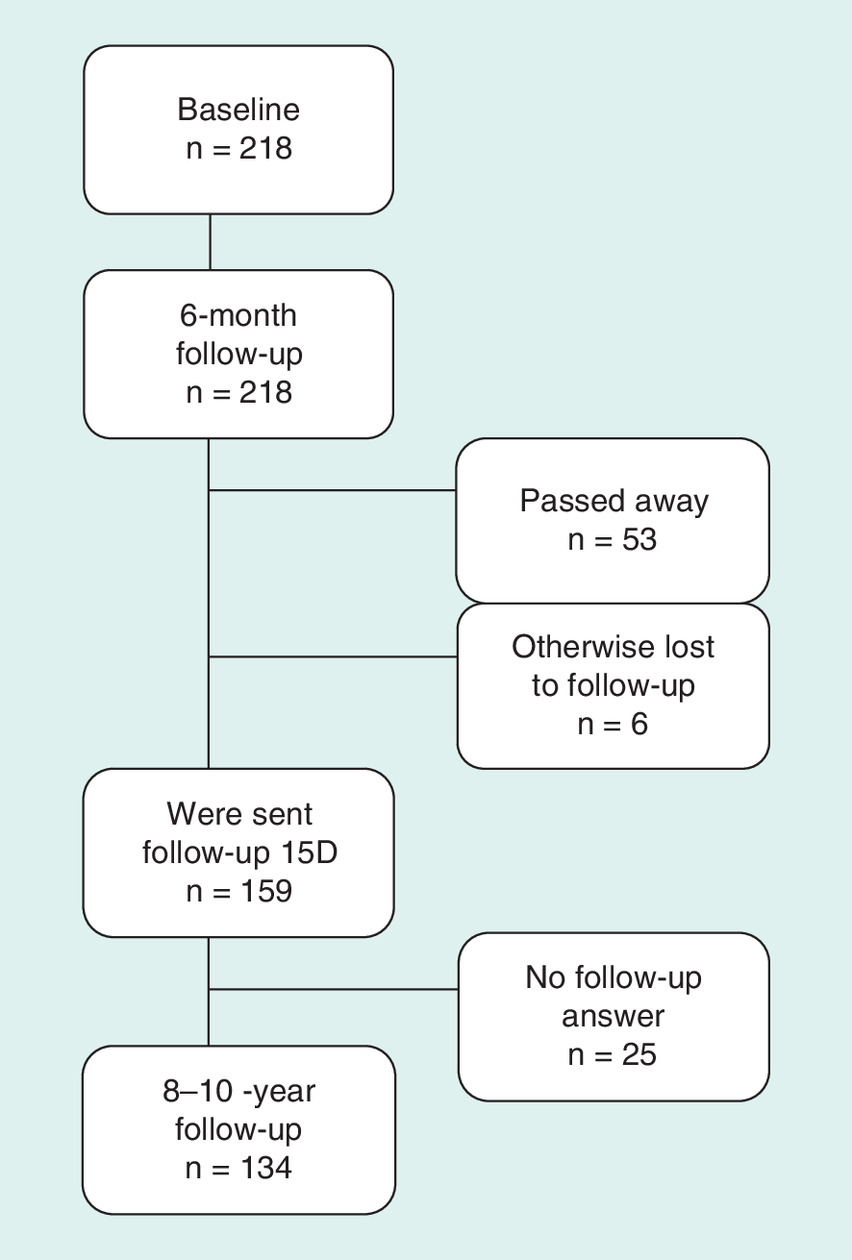
The mean age of the study patients at baseline was 60.1 (SD ± 12.9) years and at the long-term follow-up 68.4 (SD ± 12.2) years. By the average of 9.1 years (range 7.9–10.2 years) after treatment initiation, 53 of the original 218 patients (24%) had died, and six (2.8%) were otherwise lost to follow-up (moved to another part of the country or abroad). Of the remaining 159 patients, 134 (84%) answered the 15D questionnaire (Figure 1). The most common malignancies in the original 218 study patients were uterine (48%), ovarian (30%) and cervical cancer (8%). All patients had undergone demanding cancer treatments. Open surgical techniques were used in 164 (75%) patients and laparoscopic techniques in 35 (16%; Table 1).
| Diagnosis at baseline | Number of patients | Treatment | Number of patients |
|---|---|---|---|
| Uterine (endometrial) cancer | 102 | AH + BSO | 135 |
| Uterine sarcoma | 2 | LH + BSO | 33 |
| Adjuvant chemotherapy | 12 | ||
| Ovarian cancer | 66 | Radical hysterectomy | 11 |
| Radiation | 5 | ||
| Cervical cancer | 17 | Laparotomy | 4 |
| Laparotomy, BSO | 4 | ||
| Tubal cancer | 9 | AH | 2 |
| Vulvar cancer | 5 | Laparoscopy | 2 |
| Vaginal cancer | 3 | Chemotherapy after cancer recurrence | 2 |
| Other* | 14 | Vulvectomy and excision of regional lymph nodes | 2 |
| Total | 218 | BSO | 1 |
| *Incl. e.g., peritoneal cancer, cancer of pelvic area | Laparotomy, USO | 1 | |
| Supravaginal hysterectomy + BSO | 1 | ||
| Excision of lesion of vulva or perineum | 1 | ||
| Open surgical techniques | 159 | Reoperation due to deep infection | 1 |
| Laparoscopic techniques | 35 | Reoperation for insufficiency of suture | 1 |
| Chemotherapy | 14 | Total | 218 |
| Radiation | 5 | ||
| Other | 5 | ||
| Total | 218 | ||
AH: Abdominal hysterectomy; BSO: Bilateral salpingo-oophorectomy; LH: Laparoscopic hysterectomy; USO: Unilateral salpingo-oophorectomy.
Comparison to the general population
Comparisons to the age-standardized general female population were made regarding both the mean 15D score and individual dimension level values. The mean 15D scores in the study population were similar at all follow-up time points and there were no statistically significant or clinically important differences; 0.880 (SD ± 0.087) at baseline, 0.885 (SD ± 0.092) at 6 months (general female population 0.889, SD ± 0.037), and among survivors at 8–10 years 0.884 (SD ± 0.104, general female population 0.888, SD ± 0.045; Figure 2).
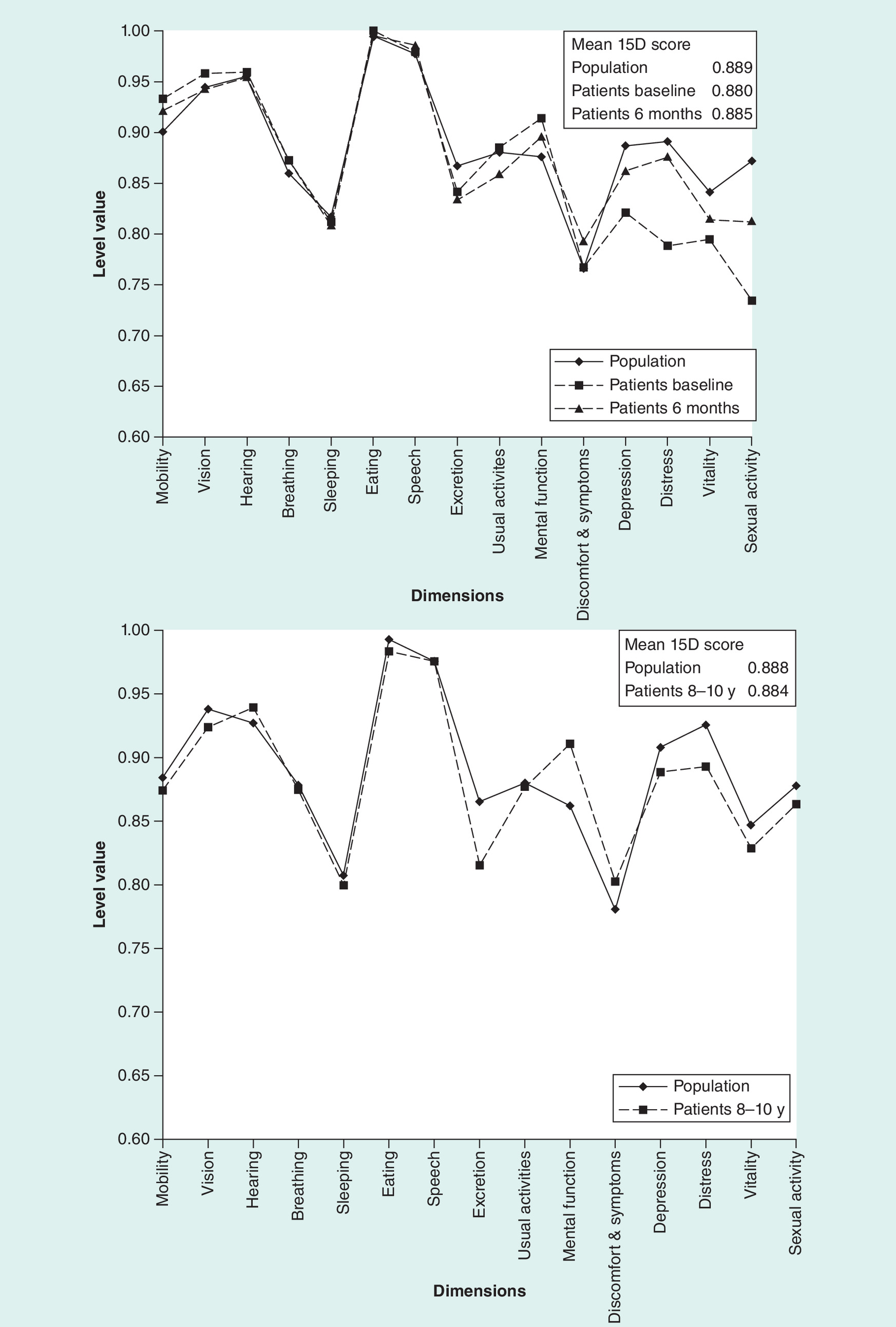
Compared with the age-standardized general female population, the study group was significantly (p < 0.05) worse off on the dimensions of depression, vitality and sexual activity both at baseline and at 6 months. The study group was also worse off on the dimension of distress at baseline and on the dimension of excretion at 6 months (p < 0.05). At baseline, the study patients were better off (p < 0.05) than the general female population on the dimensions of mental function and mobility and at 6 months on the dimension of discomfort and symptoms. When comparing the long-term follow-up measurements, the study patients were significantly better off (p < 0.05) on the dimension of mental function, but worse off on excretion and distress (Figure 2).
HRQoL change analysis in study patients
Within the study group, an improvement from baseline to 6 months and 8–10 years was seen on the dimensions of depression, distress and sexual activity (p < 0.05; Table 2). However, between 6 months and 8–10 years, no statistically significant difference was noted indicating that the major improvement on the dimensions-mentioned above takes place during the first 6 months after treatment. Deterioration of mobility, vision, hearing and excretion was seen in the long-term (Table 2).
| Patient group | From baseline to 6 months | From baseline to 8–10 years | ||
|---|---|---|---|---|
| Improvement (p < 0.05) | Deterioration (p < 0.05) | Improvement (p < 0.05) | Deterioration (p < 0.05) | |
| Whole study group (n = 218) | Depression | Vision | Depression | Mobility |
| Distress | Usual activities | Distress | Vision | |
| Sexual activity | Sexual activity | Hearing | ||
| Excretion | ||||
| Ovary (n = 66) | Distress | Vision | Discomfort and symptoms | – |
| Sexual activity | Mental function | Depression | ||
| Distress | ||||
| Vitality | ||||
| Sexual activity | ||||
| Other (n = 152) | Speech | – | Depression | Mobility |
| Depression | Distress | |||
| Distress | Sexual activity | |||
| Vitality | ||||
| Sexual activity | ||||
| Open (n = 159) | Discomfort and symptoms | Vision | Discomfort and symptoms | Mobility |
| Depression | Usual activities | Distress | ||
| Distress | Sexual activity | |||
| Sexual activity | Depression | |||
| Laparoscopic (n = 35) | Distress | – | – | – |
At baseline, the mean HRQoL of ovarian cancer patients and that of patients with other types of cancer was similar. At 6 months, a statistically significant difference was observed in usual activities in favor of the nonovarian cancer patients. By contrast, at the long-term follow-up, the ovarian cancer group was better off on the dimensions of speech, discomfort and symptoms, and hearing (Table 3). Even though the other differences did not reach statistical significance, there was a clear tendency for the ovarian group to be worse off on many of the 15D dimensions at baseline and 6-months, but better off at 8–10 years compared with the nonovarian group (this is also true regarding the mean 15D score). In both groups, the dimensions of depression, distress and sexual activity improved over time (Table 2).
| Patient group | Statistically significant difference (p < 0.05) | ||
|---|---|---|---|
| Ovary (n = 66) vs other (n = 152) | *In favor of other | Baseline | – |
| **In favor of ovary | |||
| 6-month | Usual activities* | ||
| 8–10-year | Speech** | ||
| Discomfort and symptoms** | |||
| Hearing** | |||
| Baseline | Breathing* | ||
| Open (n = 159) vs laparoscopy (n = 35) | *In favor of laparoscopy | Usual activities* | |
| **In favor of open (none) | |||
| Discomfort and symptoms* | |||
| 15D score* | |||
| 6-month | Vision* | ||
| Breathing* | |||
| Excretion* | |||
| Usual activities* | |||
| Mental function* | |||
| 15D score* | |||
| 8–10-year | Mobility* | ||
| Vision* | |||
| Hearing* | |||
| Breathing* | |||
| 15D score* |
The patients that underwent open surgery (laparotomy) were significantly worse off than those treated laparoscopically throughout the follow-up, mainly on the physical dimensions (Table 3). Also, their mean 15D score was significantly (p < 0.05) lower both at baseline and in the short- and long-term follow-ups (baseline 0.874 vs 0.908; 6-month 0.880 vs 0.921; 10-year 0.877 vs 0.914). These differences are also clinically important. However, also in the open surgery group, discomfort and symptoms, depression, distress and sexual activity improved significantly during the long-term follow-up (Table 2). In the laparoscopically-treated patients, distress improved from baseline to the 6-month follow-up, but no other statistically significant changes were seen throughout the study period (Table 2).
Costs
The mean direct costs of all cancer-related treatments during the long-term follow-up were EUR 41 342 (95% CI: 34,513–48,743), which is equal to USD 51,110 with 2012 average currency exchange rate. A majority of the costs arose quickly after diagnosis. Almost half (48%) of the total costs accrued during the first 6 months and almost 60% of them by the 1-year follow-up. Over 80% of total costs accrued during the first 3 years of the almost 10-year follow-up (Figure 3).
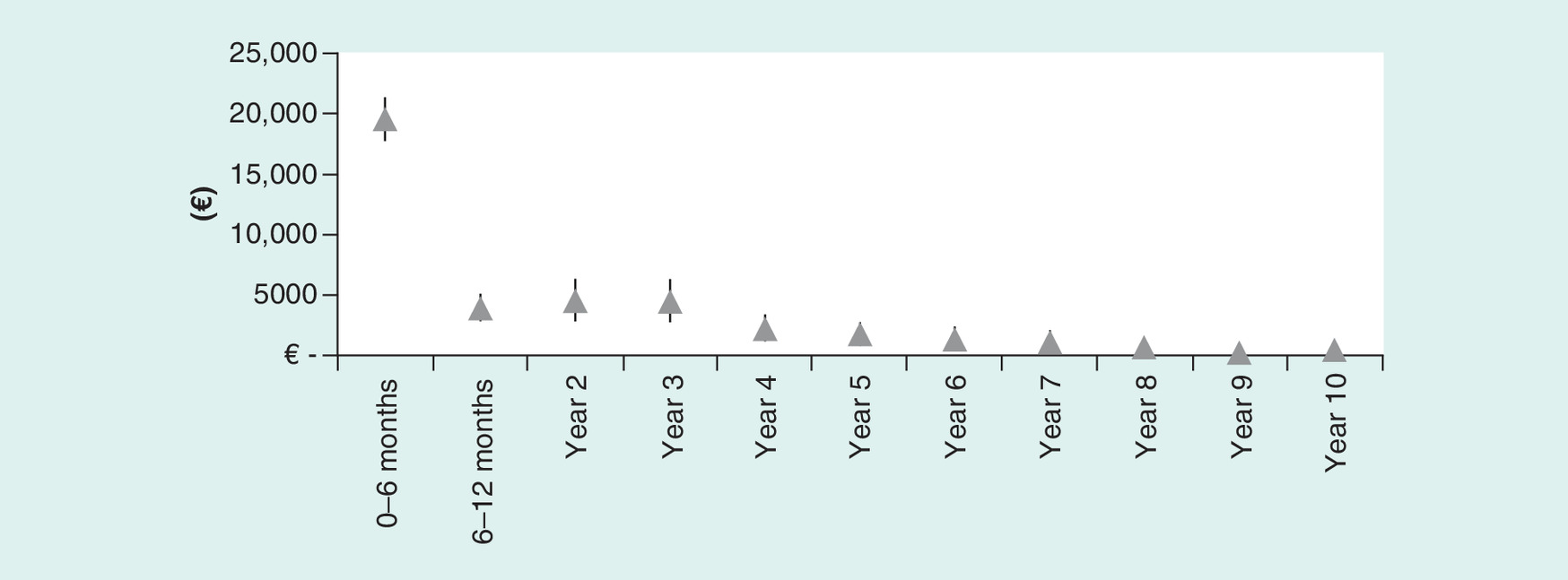
Figure 3. Costs by year.
Diagnoses taken into account when assessing costs.
Discussion
This study provides real-world information on long-term HRQoL and costs of gynecological cancer patients having undergone conventional clinical treatment. Given that the study group represents typical gynecological cancer patients regarding age and distribution of cancer types [39], and that the response rate was high, the results may be regarded as representative for any Western female population with a similar distribution of gynecological cancers. As cancer affects a large portion of the world population and as the incidence of cancer is rising, knowledge on the effects of cancer and cancer treatments on the HRQoL of patients is necessary.
As a whole, the mean HRQoL of patients in this study was high. As in previously published data with a shorter follow-up time (1–2 years) [8–11,19], our study showed that both the physical and mental recovery of patients after gynecological cancer treatment and heavy surgery is surprisingly good. Even though some studies have shown significant impairment especially in global and physical HRQoL scores during follow-ups varying from 1 month to 2.5 years [14,15], our study found very little deterioration in HRQoL. Thus, our study complements the findings of Dahl et al. in their systematic review (concerning mostly cervical cancer patients, follow-up of 2–27 years) [12] that survivors of the most common types of gynecological cancer do not have impaired HRQoL in the long-term. The same tendency of similar HRQoL of cancer patients compared with the general population has also been reported in malignancies of other organs [34,40]. Both according to the authors' own clinical experience and published data, the uncompromised HRQoL could be explained by cancer patients assigning a higher value to the same health state than women of the general population [41].
Even though the mean 15D score was similar at baseline and at the 6-month and 8–10-year follow-ups compared with the age-standardized general female population, the individual dimension scores varied. As also shown earlier, depression, vitality and sexual function were the most compromised [8,10,11,14,17,42]. Many previous studies have found mental aspects of HRQoL to improve quickly [8,10,11,14]. However, in a long-term (5-year) follow-up study of the HRQoL of gynecologic cancer patients, mental function remained compromised in the long term [42]. Our study showed all other aspects of mental function to improve already by the 6-month follow-up but distress persevered at the 8–10-year follow-up. In previous studies, the sexual well-being of patients has been reported to improve with time [8,10], even though not all patients had regained normal sexual function even after a 2- or 5-year follow-up [10,42]. In our study, the sexual activity score had improved markedly at 6-months and continued to improve up until the long-term follow-up. In previous studies, bowel symptoms have been reported to impair QoL of gynecological cancer patients during follow-up periods of 12–24 months [9,11,19]. Our study patients did not report such an impairment.
Surgery type has been reported not to affect HRQoL in gynecological cancer patients [9,10,21]. However, also differing findings have been reported. Laparoscopic surgery has been associated with improved QoL as well as cost savings due to shortened hospital stays and earlier return to normal activity as compared with open surgery [22]. Le et al. found bowel symptoms to be significantly increased in patients receiving whole pelvic radiotherapy and having undergone laparotomy as compared with those treated laparoscopically [11]. On the other hand, regarding bladder and sexual function of cervical cancer patients, Ditto et al. found adjuvant radiotherapy to affect the HRQoL more than the type of radical hysterectomy [20]. In addition to laparoscopy, also procedures for fertility preservation, sentinel lymph node mapping, and robotic and risk-reducing surgery might have advanced psychological, sexual and HRQoL outcomes and should be considered when making treatment decisions [43].
Our study showed markedly better HRQoL results both in the short- and long-term in patients treated by laparoscopy compared with laparotomy. However, our study setting is that of a normal clinical treatment protocol, and the indications of laparoscopy and laparotomy are different. Thus, at least some of the HRQoL difference in these groups may be explained by the difference in the severity of the disease between the patient groups. However, in the laparotomy group, the impaired HRQoL aspects were mainly physical and little difference was seen in the emotional or mental aspects of HRQoL.
The prognosis of ovarian cancer is worse than that of other gynecological cancers (5-year survival rates are 43, 83 and 69% for ovarian, uterine and cervical cancer in the Finnish population, respectively [5]) and the diagnosis is often made at a later stage, which may be associated with poor overall health at the initiation of treatment. As a fourth of all gynecological cancers in Finland are treated in the study clinic, and we did not have any exclusion criteria, it is highly likely that the patient cohort is representative of the gynecological cancers in the country as a whole. In order to eliminate the possible bias caused by malignancies with an especially poor prognosis and tendency to recur, we also analyzed the HRQoL of ovarian cancer patients separately and compared the results to those of patients with other gynecological malignancies. The HRQoL of the patients with ovarian cancer could be expected to be worse than that of patients with other gynecological malignancies. However, this was not the case in our study. On the contrary, the mean 15D score was higher in the ovarian cancer group at the long-term follow-up than in those with nonovarian cancer suggesting, thus, that not even recurrence or ongoing adjuvant therapy markedly deteriorate the HRQoL of gynecological cancer patients. The lower survival rate of patients with ovarian cancer, however, can somewhat distort these results as it may be that the most morbid ovarian cancer patients die during the long-term follow-up. No difference between tumor groups was seen in the gynecologic cancer HRQoL study of Stafford and Judd either [42].
The mean total secondary care costs of gynecological cancer treatment in our patient material were EUR 41,342 (USD 51,110 with 2012 average currency exchange rate) during the 8–10-year follow-up. In ovarian cancer patients in Australia, mean direct medical costs have been reported to be AUD 31,958–50,945 at 2008 prices (USD 37,491–59,767 with 2008 average currency exchange rate) during a follow-up of 2.5 years [44]. In the USA, the mean inpatient costs of advanced ovarian cancer treatment were USD 21,914–33,678 at 2007 prices for the surgical period [25] and during a follow-up of 7 months USD 59,800–63,130 at 2010 prices [45]. Zakhari et al. reported median in-hospital charges per hysterectomy admission for uterine cancer in 2008–2012 to vary in the USA from USD 31,476 to 38,161 at current prices depending on whether a traditional laparoscopic or a robotic approach was used [46]. Ferrandina et al. from Italy reported mean DRG-based direct medical costs of EUR 22,200 (USD 25,003 with 2000–2007 average currency exchange rate) for cervical cancer patients during a minimum of 10-month follow-up [24].
The total costs in our study are, thus, slightly higher than what most of the prior studies have reported. This difference may be explained by our longer follow-up time as costs of shorter time periods (as seen in Figure 3) are similar to those reported previously. Also, differences in surgical procedures, pricing methods and cost items included could; however, affect total costs. As a marked proportion of costs accrue quickly after diagnosis, it seems that the surgical treatment of gynecological cancer patients is the major driver of total costs.
Strengths & limitations
Long-term HRQoL data of gynecological cancer patients are rare. The strength of this study is thus the acquisition of such original data in a real-world hospital environment using a conventional clinical treatment protocol. Also, the response rate in this study was high. Our goal was to depict the long-term real-world HRQoL of gynecological cancer patients as a group and the study was designed accordingly. Consequently, subgroup analysis comparing the HRQoL of women with different types of cancer and clinical features with each other is not possible. This can be seen as a limitation of the study. It should also be noted that the cost data only consist of direct costs to the hospital and that some uncertainty is always associated with the comparison of costs between different countries, different time periods and when different treatment conventions apply.
Conclusion
In conclusion, despite major surgery and demanding cancer treatments, the HRQoL of gynecological cancer patients is good and, in the long-term follow-up of 8–10 years the HRQoL of surviving patients similar to that of the age-standardized general female population. Both mental well-being and sexual activity were compromised at baseline but showed marked improvement already by the 6-month follow-up. Sexual activity continued to improve even up to the end of the study. Total secondary care costs of gynecological cancer treatment averaged EUR 41,342.
Future perspective
The incidence of cancer is rising and new, often expensive, treatments are developed. The number of cancer survivors is increasing and, on the other hand, years lived with possibly impaired HRQoL will rise. More weight will most likely be put not only on the survival of cancer patients but also on ensuring the best possible HRQoL for this patient group. As healthcare resources are not endless, more and more attention will need to be placed to the costs of care of cancer as well. A step in the right direction is to follow the developments of HRQoL and costs of treatments given. In the future, the number of proper cost–effectiveness studies on the treatment of malignancies will most likely increase as has already happened with benign disorders. In the future, the findings of these studies will probably be considered a nearly equally important aspect of treatment protocol development as pure clinical studies are considered today.
Although the incidence of cancer is rising and, thus, cancer treatments affect a growing proportion of patients and physicians, original long-term HRQoL data of gynecological cancer patients are rare.
The study assesses the long-term HRQoL and treatment-related costs in patients treated for a gynecological malignancy in a publicly funded, real-world secondary healthcare setting.
Despite major surgery and demanding cancer treatments, the HRQoL of gynecological cancer patients is good and similar to that of the age-standardized general female population in the long-term.
Depression, vitality and sexual activity were only temporarily impaired.
Of the total secondary care costs of a mean of EUR 41,342, almost half arose during the first 6 months and over 80% during the first 3 years after treatment initiation.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: www.futuremedicine.com/doi/full/10.2217/cer-2018-0125
Author contributions
K Pynnä, P Vuorela, P Aronen, A Leminen, H Sintonen, R Roine and P Räsänen participated in planning the study. T Vainiola gathered the data. K Pynnä, P Aronen and H Sintonen were responsible for data analysis and K Pynnä for most of the interpretation of the data and also responsible for drafting the manuscript. P Vuorela, A Leminen, H Sintonen, R Roine and P Räsänen acted as senior authors and consultants throughout the writing process and were responsible for revising the manuscript. All authors have approved of the final version to be published.
Financial & competing interests disclosure
H Sintonen is the developer of the 15D and receives royalties from its electronic versions. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The study protocol was approved by the Ethics Committee of the Helsinki University Central Hospital (registration number 26/E6/02 and 195/13/03/03/2012) and, thus, the study was performed in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed written consent was obtained from all individual study participants. This included consent to include material pertaining to themselves, an acknowledgement that patients cannot be identified via the paper and that full anonymization was performed.
Supplementary Material
File (suppl_file.docx)
- Download
- 22.56 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
The WHO International Agency for Research on Cancer (2018). www.iarc.fr/index.php.
2.
Cancer Research UK (2018). www.cancerresearchuk.org/cancer-info/cancerstats/.
3.
Centers for Disease Control and Prevention (2018). www.cdc.gov/cancer/gynecologic/index.htm.
4.
Cancer Australia (2018). http://canceraustralia.gov.au/affected-cancer/cancer-types/gynaecological-cancers.
5.
Syöpäjärjestöt Finnish Cancer Association (2018). www.cancer.fi/.
6.
Finnish Cancer Register, Cancer Statistics of the National Institute of Health and Welfare (2018). www.cancer.fi/syoparekisteri/en/.
7.
Whiteman MK, Hillis SD, Jamieson DJ et al. Inpatient hysterectomy surveillance in the United States, 2000–2004. Am. J. Obstet. Gynecol. 198, 34.e1–34.e7 (2008).
8.
Ferrandina G, Petrillo M, Mantegna G et al. Evaluation of quality of life and emotional distress in endometrial cancer patients: a 2-year prospective, longitudinal study. Gynecol. Oncol. 133(3), 518–525 (2014).
• A 2-year follow-up of quality of life aspects of patients with endometrial cancer.
9.
Greimel E, Kristensen GB, van der Burg ME et al. Quality of life of advanced ovarian cancer patients in the randomized Phase III study comparing primary debulking surgery versus neo-adjuvant chemotherapy. Gynecol. Oncol. 131(2), 437–444 (2013).
10.
Carter J, Sonoda Y, Baser RE et al. A 2-year prospective study assessing the emotional, sexual, and quality of life concerns of women undergoing radical trachelectomy versus radical hysterectomy for treatment of early-stage cervical cancer. Gynecol. Oncol. 119(2), 358–365 (2010).
• A 2-year follow-up of the quality of life of cervical cancer patients.
11.
Le T, Menard C, Samant R et al. Longitudinal assessments of quality of life in endometrial cancer patients: effect of surgical approach and adjuvant radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 75(3), 795–802 (2009).
12.
Dahl L, Wittrup I, Væggemose U, Petersen LK, Blaakaer J. Life after gynecologic cancer – a review of patients quality of life, needs, and preferences in regard to follow-up. Int. J. Gynecol. Cancer 23(2), 227–234 (2013).
•• A systematic review on the quality of life and the needs and preferences during follow-up of gynecological cancer survivors.
13.
Lutgendorf SK, Shinn E, Carter J et al. Quality of life among long-term survivors of advanced stage ovarian cancer: a cross-sectional approach. Gynecol. Oncol. 146(1), 101–108 (2017).
• Quality of life of ovarian cancer patients eight years after treatment initiation.
14.
Minig L, Vélez JI, Trimble EL, Biffi R, Maggioni A, Jeffery DD. Changes in short-term health-related quality of life in women undergoing gynecologic oncologic laparotomy: an associated factor analysis. Support. Care Cancer 21(3), 715–726 (2013).
15.
Bjelic-Radisic V, Jensen PT, Vlasic KK et al. Quality of life characteristics in patients with cervical cancer. Eur. J. Cancer 48(16), 3009–3018 (2012).
• A 2-year follow-up of quality of life of patients with cervical cancer.
16.
Westin SN, Sun CC, Tung CS et al. Survivors of gynecologic malignancies: impact of treatment on health and well-being. J. Cancer Surviv. 10(2), 261–270 (2016).
•• A systematic stratified sample of the health concerns of gynecological cancer survivors.
17.
Hawighorst-Knapstein S, Fusshoeller C, Franz C et al. The impact of treatment for genital cancer on quality of life and body image – results of a prospective longitudinal 10-year study. Gynecol. Oncol. 94(2), 398–403 (2004).
18.
Grimm D, Hasenburg A, Eulenburg C et al. Sexual activity and function in patients with gynecological malignancies after completed treatment. Int. J. Gynecol. Cancer 25(6), 1134–1141 (2015).
19.
Yavas G, Dogan NU, Yavas C, Benzer N, Yuce D, Celik C. Prospective assessment of quality of life and psychological distress in patients with gynecologic malignancy: a 1-year prospective study. Int. J. Gynecol. Cancer 22(6), 1096–1101 (2012).
20.
Ditto A, Martinelli F, Borreani C et al. Quality of life and sexual, bladder, and intestinal dysfunctions after class III nerve-sparing and class II radical hysterectomies: a questionnaire-based study. Int. J. Gynecol. Cancer 19(5), 953–957 (2009).
21.
Bijen CB, Vermeulen KM, Mourits MJ et al. Cost–effectiveness of laparoscopy versus laparotomy in early stage endometrial cancer: a randomised trial. Gynecol. Oncol. 121(1), 76–82 (2011).
22.
Spirtos NM, Schlaerth JB, Gross GM, Spirtos TW, Schlaerth AC, Ballon SC. Cost and quality-of-life analyses of surgery for early endometrial cancer: laparotomy versus laparoscopy. Am. J. Obstet. Gynecol. 174(6), 1795–1799; discussion 1799-1800 (1996).
23.
Ashih H, Gustilo-Ashby T, Myers ER et al. Cost–effectiveness of treatment of early stage endometrial cancer. Gynecol. Oncol. 74(2), 208–216 (1999).
24.
Ferrandina G, Marcellusi A, Mennini FS, Petrillo M, Di Falco C, Scambia G. Hospital costs incurred by the Italian National Health Service for invasive cervical cancer. Gynecol. Oncol. 119(2), 243–249 (2010).
25.
Aletti GD, Podratz KC, Moriarty JP, Cliby WA, Long KH. Aggressive and complex surgery for advanced ovarian cancer: an economic analysis. Gynecol. Oncol. 112(1), 16–21 (2009).
26.
Pynnä K, Vuorela P, Lodenius L, Paavonen J, Roine RP, Räsänen P. Cost–effectiveness of hysterectomy for benign gynecological conditions: a systematic review. Acta Obstet. Gynecol. Scand. 93(3), 225–232 (2014).
27.
Taipale K, Leminen A, Räsänen P et al. Cost and health-related quality of life effects of hysterectomy in patients with benign uterine disorders. Acta Obstet. Gynecol. Scand. 88(12), 1402–1410 (2009).
28.
Sintonen H. The 15D instrument of health-related quality of life: properties and applications. Ann. Med. 33(5), 328–336 (2001).
29.
The 15D health-related quality of life (HRQoL) instrument (2018). www.15d-instrument.net/15D.
30.
Alanne S, Roine RP, Räsänen P, Vainiola T, Sintonen H. Estimating the minimum important change in the 15D scores. Qual. Life Res. 24(3), 599–606 (2015).
31.
Färkkilä N, Sintonen H, Saarto T et al. Health-related quality of life in colorectal cancer. Colorectal Dis. 15, e215–e222 (2013).
32.
Torvinen S, Färkkilä N, Sintonen H, Saarto T, Roine RP, Taari K. Health-related quality of life in prostate cancer. Acta Oncol. 52, 1094–1010 (2013).
33.
Loimu V, Mäkitie AA, Bäck LJ et al. Health-related quality of life of head and neck cancer patients with successful oncological treatment. Eur. Arch. Otorhinolaryngol. 272, 2415–2423 (2015).
34.
Richardson J, Iezzi A, Khan MA, Chen G, Maxwell A. Measuring the sensitivity and construct validity of 6 utility instruments in 7 disease areas. Med. Decis. Making 36(2), 147–159 (2016).
35.
Aromaa A, Koskinen S. Health and functional capacity in Finland. Baseline results of the Health 2000 Health Examination Survey. Helsinki, Finland (2004). www.julkari.fi/handle/10024/78534.
36.
Koskinen S, Lundqvist A, Ristoluoma N. Health, functional capacity and welfare in Finland in 2011. National Institute for Health and Welfare (THL), Report 68/2012. Helsinki, Finland (2012). www.julkari.fi/bitstream/handle/10024/90832/Rap068_2012_netti.pdf.
37.
Heistaro S. Methodology Report. Health 2000 Survey. Publications of the National Public Health Institute. Helsinki, Finland (2008). www.julkari.fi/handle/10024/78185.
38.
Lundqvist A, Mäki-Opas T. Health 2011 Survey – Methods. National Institute for Health and Welfare. Tampere, Finland (2016).
39.
The Association of the Nordic Cancer Registries (ANCR) (2018). www-dep.iarc.fr/NORDCAN/english/frame.asp.
40.
Herce Lopez J, Rollon Mayordomo A, Lozano Rosado R, Salazar Fernandez CI, Gallana S. Quality of life in long-term oral cancer survivors: a comparison with Spanish general population norms. J. Oral Maxillofac. Surg. 67(8), 1607 Tampere 1614 (2009).
41.
Feeny D, Krahn M, Prosser LA, Salomon JA. Valuing health outcomes. In: Cost–Effectiveness in Health and Medicine, Second Edition Neumann PJ, Sanders GD, Russell LB, Siegel JE, Ganiats TG (Eds). Oxford University Press, NY, USA 167–199 (2016).
42.
Stafford L, Judd F. Long-term quality of life in Australian women previously diagnosed with gynaecologic cancer. Support. Care Cancer 19 (12), 2047 (2011).
•• A 5-year follow-up of the quality of life of gynecological cancer patients.
43.
Carter J, Stabile C, Gunn A, Sonoda Y. The physical consequences of gynecologic cancer surgery and their impact on sexual, emotional, and quality of life issues. J. Sex Med. 10(Suppl. 1), 21–34 (2013).
44.
Gordon LG, Scuffham PA, Beesley VL et al. Medical costs and outcomes for Australian women with ovarian cancer: a patient-level analysis over 2.5 years. Int. J. Gynecol. Cancer 20(5), 757–765 (2010).
• A 2.5-year follow-up of medical costs and quality-adjusted life-years (survival adjusted by quality-of-life) of ovarian cancer patients.
45.
Forde GK, Chang J, Ziogas A, Tewari K, Bristow RE. Costs of treatment for elderly women with advanced ovarian cancer in a Medicare population. Gynecol. Oncol. 137(3), 479–484 (2015).
46.
Zakhari A, Czuzoj-Shulman N, Spence AR, Gotlieb WH, Abenhaim HA. Laparoscopic and robot-assisted hysterectomy for uterine cancer: a comparison of costs and complications. Am. J. Obstet. Gynecol. 213(5), 665.e1ee7 (2015).
Information & Authors
Information
Published In
Copyright
© 2019 Future Medicine Ltd.
History
Received: 15 November 2018
Accepted: 15 February 2019
Published online: 29 March 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Treatment of gynecological malignancies: long-term follow-up of health-related quality of life and healthcare costs. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0125
Export citation
Select the citation format you wish to export for this article or chapter.