Treatment patterns and outcomes for patients with unresectable stage III and metastatic melanoma in the USA
Abstract
Aim: To describe treatment patterns and outcomes of patients with unresectable stage III and metastatic/stage IV melanoma. Materials & methods: An observational retrospective chart review of patients diagnosed with advanced melanoma before 1 November 2015 who initiated a new line of therapy (LOT) from 1 January 2015 to 31 May 2016. Results: Among 487 patients, ipilimumab monotherapy (27.5%) was the most common first line of therapy (1LOT) in 2015, surpassed by nivolumab monotherapy (21.5%) in 2016. 12-month survival was ≥80.1%; proportions were highest forpatients treated with nivolumab + ipilimumab (86.6%). All treatments relatively well tolerated in real-world setting and adverse events were consistent with the previously reported safety profiles. Conclusion: This study provides important insights into real-world advanced melanoma treatment patterns and demonstrates encouraging treatment safety and patient survival data.
Melanoma of the skin is the fifth leading cancer in the USA in terms of estimated new cases and deaths [1]. As of June 2018, there were an estimated 91,270 new cases in the year 2018, accounting for 5.3% of all new cancer cases in the US and an estimated 9320 deaths, accounting for 1.5% of all cancer deaths [1].
The treatment landscape for advanced melanoma has significantly changed with the US FDA approvals of ipilimumab (Yervoy®, Bristol-Myers Squibb, NY, USA; approved 25 March 2011) [2], vemurafenib (Zelboraf®, Genentech, CA, USA; 17 August 2011) [3], dabrafenib (Tafinlar®, Novartis, Basal, Switzerland; 29 May 2013) [4], trametinib (Mekinist®, Novartis, Basel, Switzerland; 29 May 2013) [5], pembrolizumab (Keytruda®, Merck, NJ, USA; 4 September 2014) [6] and nivolumab (Opdivo®, Bristol-Myers Squibb, NY, USA; 22 December 2014) [7]. The FDA later approved ipilimumab in combination with nivolumab on 30 September 2015 [7] and cobimetinib (Cotellic®, Genentech, CA, USA) in combination with vemurafenib on 10 November 2015 [8]. On 27 June 2018, the FDA approved encorafenib and binimetinib (Braftovi® and Mektovi®, Array BioPharma, Inc., CO, USA). In recent years, the use of combination regimens have become common, with data demonstrating even greater increases in progression-free survival (PFS) and overall survival (OS) [9]. Results of several randomized controlled trials have shown that nivolumab in combination with ipilimumab resulted in significantly longer PFS and OS than ipilimumab alone in both BRAF mutant and wild-type melanoma [10]. Dabrafenib in combination with trametinib has also been shown to be superior to both dabrafenib alone and vemurafenib alone in improving OS in patients with BRAF V600E or V600K mutations [11–15].
With advancements in drug therapies, physicians now have access to multiple treatment options for advanced melanoma. While there are some data that characterize the treatment patterns and survival of patients with advanced melanoma in the pre-immuno-oncology era [16–18], these were focused on a single treatment or from a period prior to combination therapies. There is little real-world data that cover all currently approved therapies with more clinical detail than is available in administrative database analyses.
In this study, our primary focus was to assess treatment patterns, including treatment regimen selection as well as time to initiation of therapy and duration of therapy, in patients with advanced melanoma. Additionally, we describe the use of biomarker testing, assess OS and PFS, and examine the time to grade and duration of treatment-related adverse events (AEs).
Methods
Study design
This was an observational, retrospective, multisite and noninterventional study that collected real-world data from medical records of patients diagnosed with advanced melanoma treated at community or academic cancer centers in the USA. Patients were assigned treatment cohorts based on first-line biologic treatment: ipilimumab monotherapy, nivolumab monotherapy, nivolumab + ipilimumab, pembrolizumab monotherapy, dabrafenib + trametinib or other. The study was sponsor-blinded so that the physicians and patients remained anonymous to the source of study funding and vice versa. A chart review design was necessary to gain a deeper understanding of patients’ underlying clinical characteristics. Extracting data directly from the charts allowed for the collection of Eastern Cooperative Oncology Group (ECOG) status, BMI, mutation status, disease staging, disease progression and rationale for initiation and discontinuation of treatment. It also allowed for better identification of AEs that may not have required treatment. The target population included a random sample of patients with advanced (unresectable stage III or metastatic/stage IV) melanoma who were diagnosed prior to 1 November 2015 and received treatment for advanced melanoma from 1 January 2015 to 31 May 2016, irrespective of date of diagnosis of unresectable stage III or metastatic/stage IV melanoma. The index study period (1 January 2015 to 31 May 2016) was chosen to capture treatment patterns with outcomes observed by line of therapy (LOT), which occurred after the FDA approval of nivolumab for the treatment of advanced melanoma in 2015. This allowed for the collection of a minimum 6 months of patient follow-up data.
Clinical data were sourced from patient medical records and reflected the period from diagnosis of advanced melanoma (irrespective of unresectable or metastatic diagnosis) to the most recent visit. Month and year of last office or clinic visit were used to ensure that a representative sample of patients with advanced melanoma was enrolled within the study period.
Physicians (medical oncologists and hematologists/oncologists) were responsible for identifying eligible patients who met the inclusion criteria. From this pool of eligible patients, instructions were provided to randomly select eligible patients based on the date of initiation of index treatment within the study inclusion period (1 January 2015–31 May 2016), using random month/year generator assigned each physician/site. The process was repeated for each additional patient enrolled.
Physicians used uniform case report forms (CRFs) to extract information including patient demographics, clinical and disease characteristics, treatment patterns, treatment-related AEs and clinical outcomes.
Study population
Inclusion criteria were adults aged 18 years or older with a diagnosis of unresectable stage III or metastatic/stage IV melanoma prior to 1 November 2015, and initiation of a new LOT for advanced melanoma during the index period between 1 January 2015 and 31 May 2016, irrespective of diagnosis date. The lines of therapy were restricted to immunotherapies or targeted therapies for the treatment of advanced melanoma. Start and stop dates for each line of therapy were identified in the patient medical chart. The 1LOT was the first immunotherapy or targeted therapy given; the 2LOT was the second immunotherapy or targeted therapy – among others. ‘Other’ therapies are treatments outside of the five immunotherapies or targeted therapies of interest and are defined in results section. Complete medical history from date of diagnosis through most recent or current therapy (defined as end of data collection period) was required for medical chart extraction. Patients were excluded if they were previously enrolled in a cancer treatment-related clinical trial.
Study outcomes
The primary outcomes included assessment of treatment patterns and clinical outcomes. Treatment patterns encompassed the year of treatment initiation, number of LOTs received, agent prescribed and rationale for treatment initiation and discontinuation. Additionally, time to initiation of each LOT (time from stage III/stage IV diagnosis to 1LOT, or time from last dose of 1LOT to first dose of 2LOT), duration of treatment (time from first dose to last recorded dose) and treatment sequence were analyzed. OS and PFS were measured from date of first recorded therapy dose during study period to date of melanoma-related death or progression, respectively. Additional outcomes included occurrence of grade III or IV AEs related to first LOT (1LOT). The proportion of patients that experienced an AE, mean number of AEs per patient and duration of AEs were assessed.
Statistical analysis
Patient demographics, clinical characteristics, treatment patterns and AE occurrence were reported using descriptive statistics; categorical statistics were described as frequency and proportion of the patient cohort, while continuous statistics were summarized as mean and standard deviation. OS and PFS were estimated descriptively using the Kaplan–Meier product limit method. Patients were censored at death, confirmed lost to follow-up or end of study, whichever occurred first. All analysis was conducted using SAS v9.4 (SAS Institute Inc., NC, USA).
Ethics
This study was conducted in accordance with International Society for Pharmacoepidemiology (ISPE) Guidelines for Good Epidemiology Practices and Applicable Regulatory Requirements. The study received approval from New England Institutional Review Board on 11 January 2017.
Results
Patient characteristics
A total of 166 physicians were screened for participation in the study, of which 45 physicians provided data. A total of 487 patients were assigned to six treatment cohorts from 45 participating ‘across all treatment groups, median follow-up time from start of 1LOT was 14.1 months (IQR: 11.0–20.3 months). Median follow-up was shortest in the nivolumab group (12.1 months [IQR: 10.6–14.5]) and longest in the dabrafenib + trametinib group (15.7 months [IQR: 11.8–19.7])’. The average age varied by 11 years between cohorts (57.1 years in nivolumab + ipilimumab vs 68.3 years in nivolumab) but the difference was not statistically significant (Table 1). A slight male preponderance was noted across cohorts (range: 50.0–66.7%), with the highest percentage in the nivolumab + ipilimumab cohort and the majority of patients were white (range: 91.6–97.1%).
| Baseline characteristics | Ipi Mono (n = 106) | Nivo Mono (n = 69) | Nivo + Ipi (n = 60) | Pembro Mono (n = 95) | Dab + Tram (n = 84) | Other (n = 73) |
|---|---|---|---|---|---|---|
| Age (years), mean (SD) | 60.9 (11.4) | 68.3 (12.2) | 57.1 (11.3) | 62.6 (13.5) | 62.6 (12.6) | 64.9 (14.0) |
| Vital status: alive, n (%) | 78 (73.6) | 55 (79.7) | 50 (83.3) | 73 (76.8) | 61 (72.6) | 48 (65.8) |
| Male, n (%) | 59 (55.7) | 37 (53.6) | 40 (66.7) | 51 (53.7) | 42 (50.0) | 41 (56.2) |
| Race, n (%): | ||||||
| – White | 100 (94.3) | 67 (97.1) | 58 (96.7) | 87 (91.6) | 77 (91.7) | 69 (94.5) |
| – Black or African American | 4 (3.8) | 1 (1.4) | 1 (1.7) | 5 (5.3) | 2 (2.4) | – |
| – Asian | 2 (1.9) | – | – | 3 (3.2) | 5 (6.0) | 2 (2.7) |
| – American Indian/Alaska Native | – | – | 1 (1.7) | – | – | 1 (1.4) |
| – Native Hawaiian/Other Pacific Islander | – | 1 (1.4) | – | – | – | 1 (1.4) |
| BMI, mean (SD) | 26.0 (3.9) | 25.8 (3.4) | 28.1 (5.1) | 26.0 (4.1) | 27.4 (5.6) | 26.7 (4.9) |
| Charlson Comorbidity Index, mean (SD) | 0.4 (0.8) | 0.5 (1.0) | 0.5 (0.8) | 0.8 (1.2) | 0.8 (1.1) | 0.9 (1.4) |
| Current primary major medical insurance, n (%): | ||||||
| – Private insurance† | 64 (60.4) | 43 (62.3) | 51 (85.0) | 40 (42.1) | 42 (50.0) | 36 (49.3) |
| – Government insurance‡ | 41 (38.7) | 26 (37.7) | 9 (15.0) | 51 (53.7) | 39 (46.4) | 36 (49.3) |
| – Uninsured/unknown§ | 1 (0.9) | 0 (0.00) | 0 (0.00) | 4 (4.2) | 3 (3.6) | 1 (1.4) |
| Diagnosed at early stage, n (%) | 24 (22.6) | 14 (20.3) | 30 (50.0) | 20 (21.1) | 32 (38.1) | 22 (30.1) |
| Advanced stage, n (%): | ||||||
| – IIIB | 2 (1.9) | 1 (1.4) | 1 (1.7) | – | – | – |
| – IIIC | 8 (7.5) | 3 (4.3) | – | 7 (7.4) | 1 (1.2) | 4 (5.5) |
| – IV | 96 (90.6) | 65 (94.2) | 59 (98.3) | 88 (92.6) | 83 (98.8) | 69 (94.5) |
| Presence of distant metastasis, n (%) | 96 (90.6) | 65 (94.2) | 59 (98.3) | 88 (92.6) | 83 (98.8) | 69 (94.5) |
| Metastases at diagnosis, n (%): | ||||||
| – Bone | 14 (13.2) | 16 (23.2) | 11 (18.3) | 14 (14.7) | 24 (28.6) | 17 (23.3) |
| – Brain | 10 (9.4) | 6 (8.7) | 3 (5.0) | 12 (12.6) | 8 (9.5) | 10 (13.7) |
| – Distant skin | 18 (17.0) | 10 (14.5) | 8 (13.3) | 13 (13.7) | 12 (14.3) | 8 (11.0) |
| – Liver | 33 (31.1) | 19 (27.5) | 21 (35.0) | 33 (34.7) | 37 (44.0) | 18 (24.7) |
| – Lymph nodes | 42 (39.6) | 23 (33.3) | 37 (61.7) | 33 (34.7) | 39 (46.4) | 32 (43.8) |
| – Lung | 68 (64.2) | 53 (76.8) | 45 (75.0) | 61 (64.2) | 59 (70.2) | 48 (65.8) |
| – Other | 2 (1.9) | – | 2 (3.3) | 5 (5.3) | 6 (7.1) | 3 (4.1) |
| ECOG score at advanced diagnosis, n (%): | ||||||
| – 0 | 27 (25.5) | 26 (37.7) | 22 (36.7) | 18 (18.9) | 16 (19.0) | 22 (30.1) |
| – 1 | 64 (60.4) | 35 (50.7) | 34 (56.7) | 64 (67.4) | 60 (71.4) | 31 (42.5) |
| – 2 | 14 (13.2) | 8 (11.6) | 3 (5.0) | 10 (10.5) | 8 (9.5) | 20 (27.4) |
| – 3 | 1 (0.9) | – | 1 (1.7) | 2 (2.1) | – | – |
| – Not assessed/unknown | – | – | – | 1 (1.1) | – | – |
| LDH result, n (%): | ||||||
| – Elevated | 42 (39.6) | 32 (46.4) | 28 (46.7) | 43 (45.3) | 51 (60.7) | 30 (41.1) |
| – Normal | 55 (51.9) | 33 (47.8) | 27 (45.0) | 42 (44.2) | 30 (35.7) | 28 (38.4) |
| – Not assessed/unknown | 9 (8.5) | 4 (5.8) | 5 (8.3) | 10 (10.5) | 3 (3.6) | 15 (20.5) |
| PD-L1 result, n (%): | ||||||
| – Positive | 21 (19.8) | 23 (33.3) | 14 (23.3) | 39 (41.1) | 14 (16.7) | 7 (9.6) |
| – Negative | 30 (28.3) | 7 (10.1) | 21 (35.0) | 6 (6.3) | 17 (20.2) | 23 (31.5) |
| – Not tested | 55 (51.9) | 39 (56.5) | 25 (41.7) | 50 (52.6) | 53 (63.1) | 43 (58.9) |
| Started 1LOT post PD-L1 test, n (%) | 51 (48.1) | 29 (42.0) | 35 (58.3) | 45 (47.4) | 31 (36.9) | 30 (41.1) |
| BRAF result, n (%): | ||||||
| – Positive | 17 (16.0) | 7 (10.1) | 10 (16.9) | 19 (20.0) | 84 (100.0) | 56 (76.7) |
| – Negative | 80 (75.5) | 53 (76.8) | 49 (83.1) | 68 (71.6) | – | 11 (15.1) |
| – Not tested | 9 (8.5) | 9 (13.0) | 1 (1.7) | 8 (8.4) | – | 6 (8.2) |
| Follow-up from advanced diagnosis, mean (SD), months | 16.2 (7.6) | 13 (6.4) | 14.5 (5.2) | 16.5 (7.5) | 15.6 (5.7) | 15.8 (7.0) |
The table shows baseline demographic and clinical characteristics by 1LOT. Patients were primarily white, with a slight majority male. Although most patients were diagnosed with late stage disease, the ECOG scores were relatively low (0, 1). PD-L1 testing was not as common as BRAF testing.
†Private insurance: Health maintenance organization, preferred provider organization and traditional fee for service.
‡Government insurance: Medicare, Medigap, Medicaid, State Funded, Veterans Affairs.
§Uninsured: Indigent/No pay.
(-): 0; BMI: Body mass index; BRAF: B-Raf proto-oncogene; Dab + Tram: Dabrafenib + Trametinib; ECOG: Eastern Cooperative Oncology Group; Ipi: Ipilimumab; LDH: Lactic acid dehydrogenase; Mono: Monotherapy; Nivo: Nivolumab; Nivo + Ipi: Nivolumab + Ipilimumab; PD-L1: Programmed death ligand 1; Pembro: Pembrolizumab; SD: Standard deviation.
Charlson Comorbidity Index scores were similar across cohorts (range: 0.4–0.9). An ECOG score of 0 was common in patients treated with nivolumab (37.7%) and nivolumab + ipilimumab (36.7%); however, most patients had an ECOG score of 1. The majority of patients in the ipilimumab, nivolumab, nivolumab + ipilimumab and dabrafenib + trametinib cohorts reported having private health insurance; whereas, most patients in the pembrolizumab cohort had government-sponsored health insurance.
The majority of patients were diagnosed at a late stage (range: 50.0–79.7%); most had stage IV at diagnosis. The most common sites for metastases were lung, lymph nodes and liver. There was one patient with a prior history of breast cancer, and one patient with prior history of prostate cancer. Less than half of patients were tested for PD-L1 expression; a third of patients treated with nivolumab and 41.1% of those treated with pembrolizumab tested positive for PD-L1 expression. The majority of patients were tested for BRAF mutations, but not all who were tested positive received a BRAF inhibitor. Of those BRAF positive, 43.5% initiated 1LOT treatment with dabrafenib + trametinib.
Treatment patterns
Of the 487 patients, 21.8% initiated 1LOT with ipilimumab, followed by 19.5% on pembrolizumab and 17.2% on dabrafenib + trametinib (Figure 1). The most common 1LOT in 2016 was nivolumab monotherapy (21.5%) (Figure 1). Of the 111 patients with BRAF mutations who initiated 2LOT, 29.7% received pembrolizumab, 25.2% nivolumab and 15.3% an ‘other’ type of treatment. The most common 1LOT and 2LOT treatments in the ‘other’ cohort were vemurafenib (n = 40), temozolomide (n = 15), dacarbazine (n = 7) and vemurafenib + cobimetinib (n = 7). The most commonly used 2LOT in 2016 was pembrolizumab monotherapy (29.2%). Of those who received 1LOT ipilimumab monotherapy, 28.3% received 2LOT, most commonly nivolumab monotherapy and pembrolizumab monotherapy (both 40.0%; Figures 2 & 3). Of patients who received 1LOT nivolumab monotherapy, 11.6% received 2LOT, most commonly an ‘other’ treatment (37.5%). Of patients receiving 1LOT nivolumab + ipilimumab treatment, only 8.3% received 2LOT, most of whom received an ‘other’ treatment (60.0%; Figures 2 & 3) . A total of 13 patients continued to 3LOT treatment. Of the 193 patients that tested BRAF positive, 68 (35.2%) moved to 2LOT, most commonly pembrolizumab (29.4%) and nivolumab (23.5%). There were 91 patients who initiated BRAF + MEK combination treatment (dabrafenib + trametinib or vemurafenib + cobemetinib), of whom nine (9.9%) progressed to a 2LOT during the study period. Gaps between the lines of therapy where noted but it is unclear if these gaps were intended as washout periods or due to other reasons.
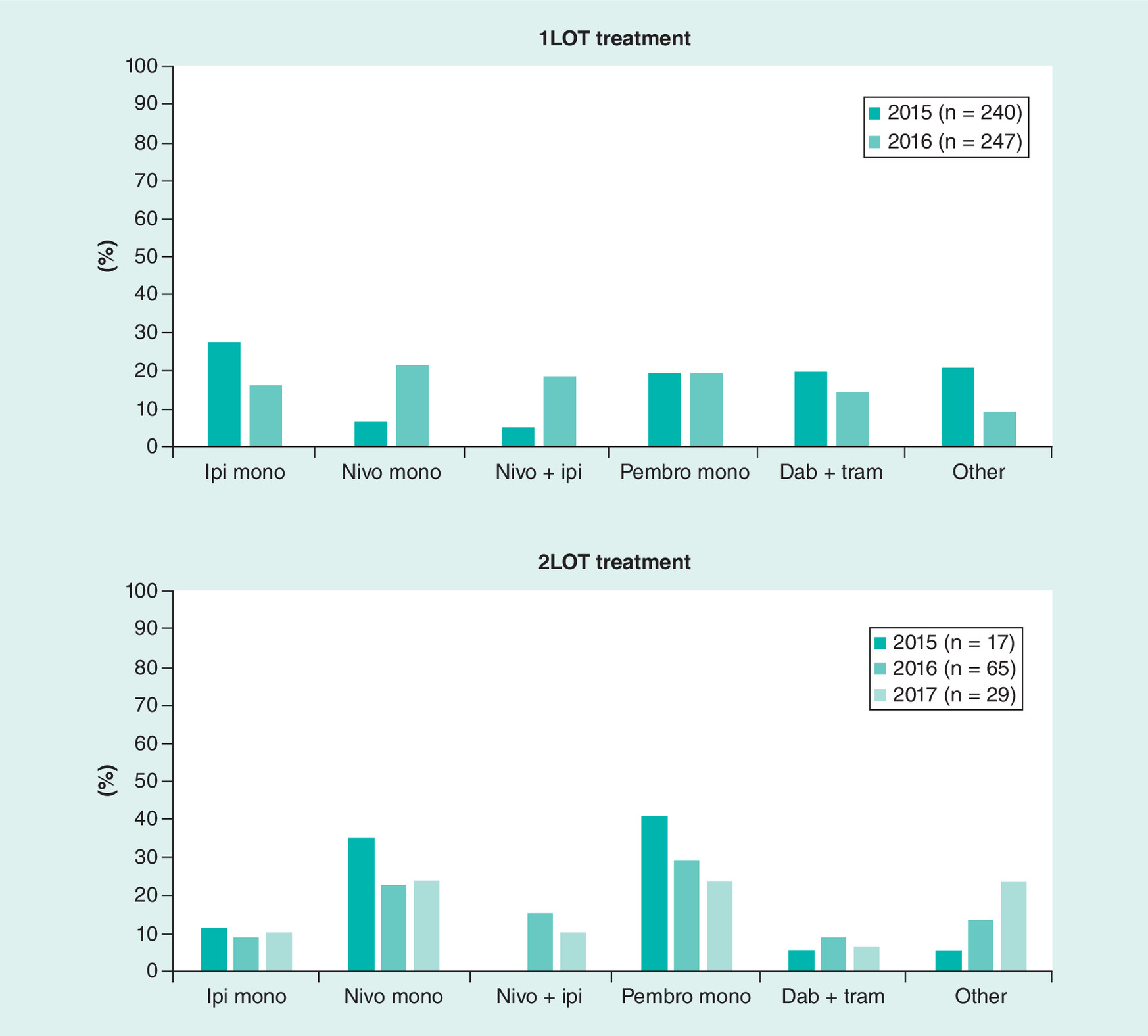
Figure 1. Distribution of therapies used as first line of therapy (1LOT) by treatment year.
The top graph shows what percentage of patients in the cohort initiated the indicated treatment as 1LOT. Use of ipilimumab monotherapy as 1LOT became less common in 2016, while use of combination nivolumab + ipilimumab was more common in 2016 compared with previous year. The lower graph represents trends in use of treatments as 2LOT from 2015 to 2017. Only the ‘other’ cohort showed an increase in percent of patients from 2015–2017.
Other = treatments outside of the five treatments of interest (primarily, vemurafenib, temozolomide, dacarbazine and vemurafenib + cobimetinib).
1LOT: First line of therapy; 2LOT: Second line of therapy; Dab + Tram: Dabrafenib + Trametinib; Ipi: Ipilimumab; Mono: Monotherapy; Nivo: Nivolumab; Nivo + Ipi: Nivolumab + Ipilimumab; Pembro: Pembrolizumab.
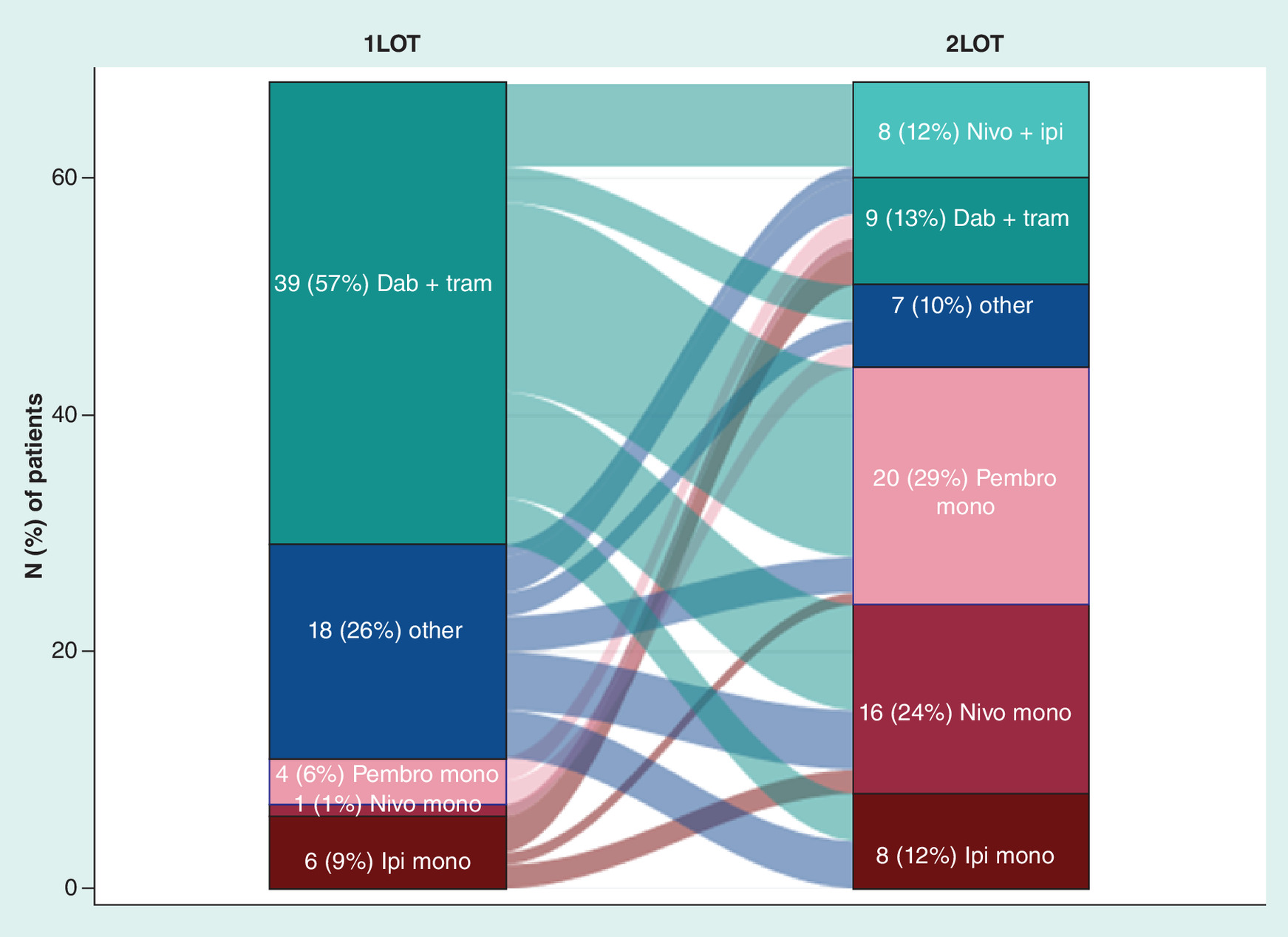
Figure 2. Treatment patterns of patients that initiated second line of therapy (BRAF mutation).
The Sankey diagram shows the flow of patients from 1LOT to 2LOT. The width of the lines is proportional to the number of patients. Of patients with a BRAF mutation who progressed to 2LOT, 57% initiated dabrafenib + trametinib, before moving to pembrolizumab, nivolumab + ipilimumab or nivolumab monotherapy, primarily.
1LOT: First line of therapy; 2LOT: Second line of therapy.
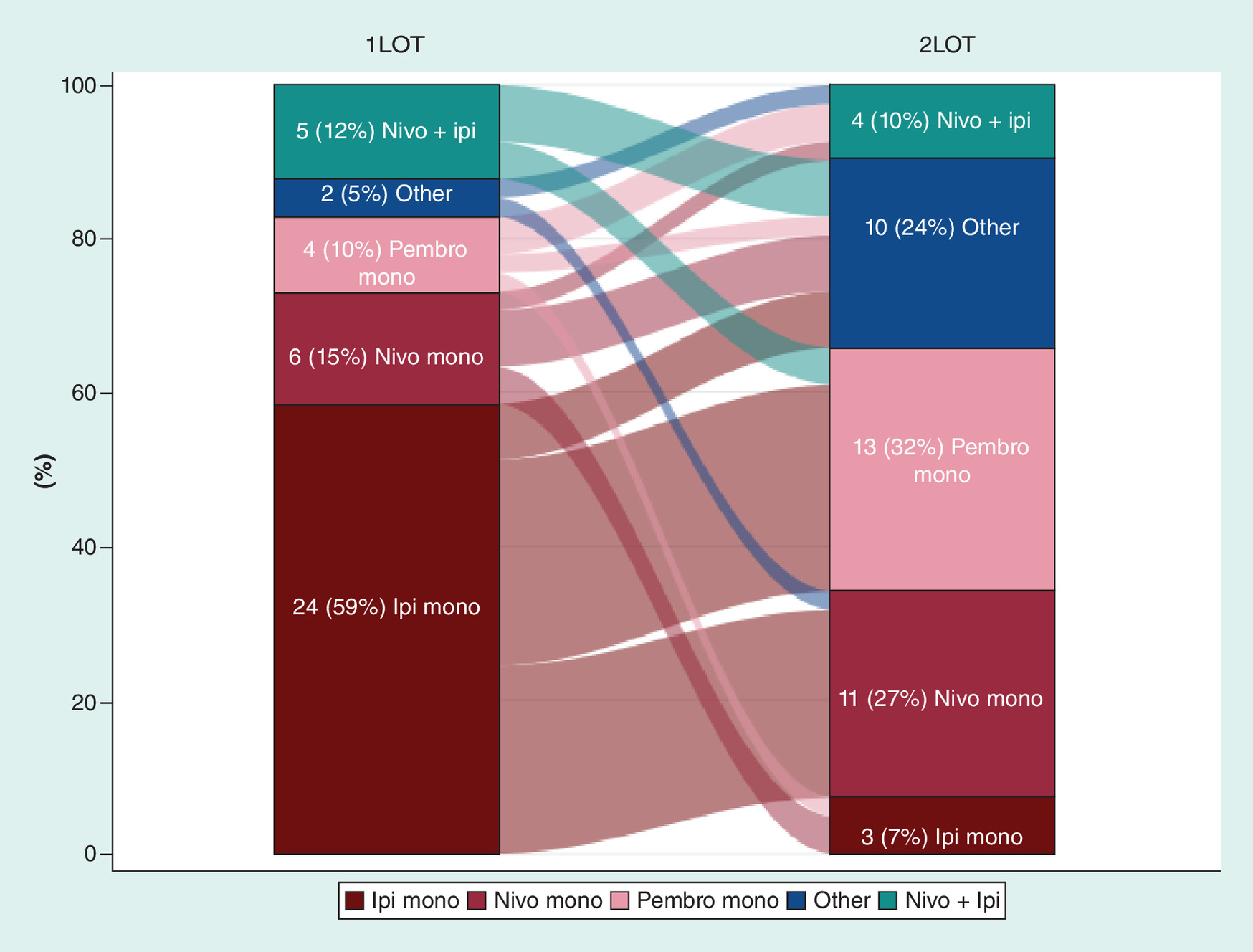
Figure 3. Treatment patterns of patients that initiated second line of therapy (wild-type BRAF).
The Sankey diagram shows the flow of patients from 1LOT to 2LOT. The width of the lines is proportional to the number of patients. Of patients with a BRAF mutation who progressed to 2LOT, 59% initiated ipilimumab monotherapy before moving on to pembrolizumab or nivolumab monotherapy, primarily.
1LOT: First line of therapy; 2LOT: Second line of therapy; Dab + Tram: Dabrafenib + Trametinib; Ipi: Ipilimumab; Mono: Monotherapy; Nivo: Nivolumab; Nivo + Ipi: Nivolumab + Ipilimumab; Pembro: Pembrolizumab.

Figure 4. Distribution of patients in study by first line of therapy.
The top box represents the total number of patients in the representative cohort of patients (N = 487). Lower boxes represent the number of patients who initiated the indicated treatment as first LOT.
30 patients who were initially diagnosed at an early operable stage before progressing had received systemic adjuvant therapy, with the most common types being IFN-α (63.3%) followed by pegylated IFN-α (23.3%) and ipilimumab monotherapy (6.7%). The mean time to initiation of therapy from diagnosis to first dose was shortest for dabrafenib + trametinib (3.3 weeks) and longest for pembrolizumab monotherapy (8.9 weeks). The mean duration of treatment for 1LOT therapy was shortest for patients treated with ipilimumab monotherapy (29.8 weeks) and longest for patients treated with pembrolizumab monotherapy (56.5 weeks) and nivolumab + ipilimumab (51.4 weeks) (Table 2). The duration of 2LOT therapy was shortest for ipilimumab monotherapy (8.5 weeks) and longest for dabrafenib + trametinib (35.1 weeks).
| Variable description | Time (weeks), wean (SD) | |||||
|---|---|---|---|---|---|---|
| Ipi Mono | Nivo Mono | Nivo + Ipi | Pembro Mono | Dab + Tram | Other | |
| Time to 1LOT inititation | 5.4 (14.4) | 6.6 (13.0) | 5.1 (10.6) | 8.9 (20.7) | 3.3 (5.0) | 6.6 (13.1) |
| 1LOT treatment duration | 29.8 (32.2) | 45.5 (22.2) | 51.4 (25.5) | 56.5 (27.8) | 45.7 (18.5) | 44.1 (26.2) |
| Time to 2LOT initiation from end of 1LOT | 4.6 (4.4) | 12.9 (16.3) | 2.9 (2.7) | 14.0 (20.8) | 12.6 (14.5) | 14.7 (19.0) |
| 2LOT treatment duration | 8.5 (3.3) | 22.8 (16.6) | 28.8 (20.2) | 32.2 (21.9) | 35.1 (20.8) | 9.3 (6.7) |
| Time to 3LOT initiation from end of 2LOT | – | 22.6 (10.5) | – | 2.4 (1.0) | 2.1 (-) | 4.4 (2.1) |
| 3LOT treatment duration | – | 20.0 (6.3) | – | 11.8 (12.1) | 54.1 (0.0) | 11.9 (7.9) |
Patients initiated 1LOT in less than 9 weeks on average. The duration of treatment ranged from 29.8 to 56.5 weeks. For patients who initiated 2LOT, the time to initiation, from last dose of 1LOT treatment ranged from 2.7 to 20.8 weeks and duration of treatment ranged 8.5 to 35.1 weeks.
(-): 0; 1LOT: First line of therapy; 2LOT: Second line of therapy; 3LOT: Third line of therapy; Dab + Tram: Dabrafenib + Trametinib; Ipi: Ipilimumab; Mono: Monotherapy; Nivo: Nivolumab; Nivo + Ipi: Nivolumab + Ipilimumab; Pembro: Pembrolizumab; SD: Standard deviation.
The primary reasons for 1LOT treatment choice across all therapies were improved efficacy (64.7%) and demonstrated/documented survival benefit (46.2%). The primary reason for discontinuation across 1LOT therapies was disease progression (77.3%), which was also the most common reason for discontinuation of dabrafenib + trametinib (85.7%). Drug toxicity was a commonly cited reason for discontinuation of ipilimumab monotherapy. Reasons for 2LOT discontinuation were limited to disease progression, drug toxicity and administrative reasons.
PFS & OS
Progression-free survival
At 18 months after start of 1LOT, 72.2% of all patients had not progressed (Table 3). By the end of follow-up, only 118, out of 487 (24.2%) of patients had progressed (Supplementary Figure 1). Median PFS was not estimable because few patients had reached the event of interest. At 6 months post-1LOT therapy start, about 85% of patients across treatment groups had not progressed. The nivolumab + ipilimumab cohort had the highest percent of nonprogressed patients at 12 months (85.0%) and 18 months (82.7.0%) post-1LOT therapy start.
| Survival time | Ipi Mono | Nivo Mono | Nivo + Ipi | Pembro Mono | Dab + Tram | Other |
|---|---|---|---|---|---|---|
| Progression-free survival, % (95% CI) | ||||||
| 6 months | 85.8 (79.3–92.7) | 88.3 (81.0–96.3) | 93.3 (87.2–99.9) | 90.5 (84.8–96.6) | 92.8 (87.4–98.5) | 93.0 (87.3–99.1) |
| 12 months | 76.1 (68.3–84.7) | 83.6 (75.1–93.0) | 85.0 (76.4–94.5) | 82.6 (75.2–90.8) | 77.8 (69.3–87.4) | 80.4 (71.3–90.7) |
| 18 months | 70.0 (61.1–80.2) | 68.8 (50.6–93.5) | 82.7 (73.4–93.2) | 77.8 (69.3–87.4) | 72.7 (62.4–84.6) | 62.3 (49.5–78.3) |
| Overall survival, % (95% CI) | ||||||
| 6 months | 88.6 (82.7–94.9) | 87.0 (79.4–95.3) | 93.3 (87.2–99.9) | 92.6 (87.5–98.0) | 95.2 (90.8–99.9) | 93.2 (87.5–99.1) |
| 12 months | 77.6 (69.9–86.1) | 77.9 (68.2–89.1) | 86.6 (78.3–95.7) | 81.4 (73.8–89.8) | 79.5 (71.3–88.7) | 78.8 (69.7–89.0) |
| 18 months | 71.6 (62.8–81.7) | 77.9 (68.2–89.1) | 81.8 (70.4–95.0) | 74.0 (64.5–84.8) | 72.6 (63.0–83.7) | 65.0 (53.3–79.3) |
The progression free survival rate was highest at 6, 12 and 18 months for patients who initiated 1LOT with nivolumab + ipilimumab. The OS rate at 6 months was highest for patients who initiated 1LOT with nivolumab + ipilimumab; although, it was very similar to pembrolizumab and dabrafenib + trametinib. At 12 and 18 months OS was clearly higher for patients who initiated 1LOT with nivolumab + ipilimumab.
1LOT: First line of therapy; Dab + Tram: Dabrafenib + Trametinib; Ipi: Ipilimumab; Mono: Monotherapy; Nivo: Nivolumab; Nivo + Ipi: Nivolumab + Ipilimumab; OS: Overall survival; Pembro: Pembrolizumab.
Overall survival
At 18 months after start of 1LOT, 72.6% of patients were still alive (Table 3). By the end of follow-up, 25.1% of patients had died (Supplementary Figure 2). As a result, median OS was not estimable because few patients had reached the event of interest. At 12 months post-1LOT therapy start, the percent of patients still alive was highest in the nivolumab + ipilimumab group and lowest in patients treated with ipilimumab monotherapy. At 18 months, the percent of patients still alive was highest in the nivolumab + ipilimumab group and lowest in patients treated with ‘other’ therapy.
Adverse events
Of patients treated with 1LOT, 25.1% had a documented AE recorded in their chart. Patients treated with nivolumab monotherapy had the fewest documented AEs (11.6%), while patients on combination therapies had the highest number of documented AEs (Table 4). Across treatment cohorts, there was little variance in the average number of reported AEs per patient (range: 0.1–0.8 AEs). Rash, fatigue and diarrhea were the most commonly documented AEs for patients overall, but this varied by therapy. In general, few patients discontinued 1LOT due to AEs (9.0%).
| Variable description | Ipi Mono (n = 106) | Nivo Mono (n = 69) | Nivo + Ipi (n = 60) | Pembro Mono (n = 95) | Dab + Tram (n = 84) | Other (n = 73) |
|---|---|---|---|---|---|---|
| AEs related to 1L, n (%) | 22 (20.8) | 8 (11.6) | 25 (41.7) | 21 (22.1) | 25 (29.8) | 21 (28.8) |
| AEs per patient, mean (SD) | 0.4 (0.7) | 0.3 (0.6) | 0.1 (0.3) | 0.8 (1.1) | 0.3 (0.6) | 0.4 (0.7) |
| Rash: | ||||||
| – n (%) | 0 (0.00) | 1 (12.5) | 7 (28.0) | 1 (4.8) | 13 (52.0) | 7 (33.3) |
| – Duration, median (days) | 0.00 (0.00–0.00) | 44.0 (44.0–44.0) | 21.0 (14.0– 55.0) | 38.0 (38.0–38.0) | 31.0 (20.0–281.0) | 45.0 (14.0–254.0) |
| Fatigue: | ||||||
| – n (%) | 5 (22.7) | 3 (37.5) | 8 (32.0) | 6 (28.6) | 4 (16.0) | 1 (4.8) |
| – Duration, median (days) | 77.0 (44.0–96.0) | 98.0 (21.0–116.0) | 198.0 (104.5–345.0) | 288.0 (140.0–477.0) | 280.5 (113.5–407.5) | 42.0 (42.0–42.0) |
| Diarrhea, n (%): | 3 (13.6) | 1 (12.5) | 4 (16.0) | 5 (23.8) | 5 (20.0) | 6 (28.6) |
| – Duration, median (days) | 42.0 (21.0– 79.0) | 37.0 (37.0–37.0) | 18.0 (11.0–40.0) | 21.0 (7.0–27.0) | 24.0 (17.0–28.0) | 18.5 (5.0– 54.0) |
| Arthritis, n (%): | 4 (18.2) | 1 (12.5) | 3 (12.0) | 4 (19.0) | 1 (4.0) | 0 (0.00) |
| – Duration, median (days) | 260.5 (176.0–277.5) | 273.0 (273.0–273.0) | 385.0 (217.0–595.0) | 178.5 (47.0–315.0) | 278.0 (278.0–278.0) | 0.00 (0.00–0.00) |
| Colitis, n (%): | 5 (22.7) | 0 (0.00) | 4 (16.0) | 1 (4.8) | 1 (4.0) | 1 (4.8) |
| – Duration, median (days) | 18.0 (14.0–19.0) | 0.00 (0.00–0.00) | 17.5 (9.0–24.5) | 29.0 (29.0–29.0) | 278.0 (278.0– 278.0) | 88.0 (88.0–88.0) |
| Autoimmune thyroiditis, n (%): | 3 (13.6) | 1 (12.5) | 3 (12.0) | 3 (14.3) | 0 (0.00) | 0 (0.00) |
| – Duration, median (days) | 97.0 (20.0–255.0) | 43.0 (43.0–43.0) | 28.0 (28.0–31.0) | 43.0 (25.0–44.0) | 0.00 (0.00–0.00) | 0.00 (0.00–0.00) |
| Vomiting, n (%): | 0 (0.00) | 0 (0.00) | 1 (4.0) | 0 (0.00) | 2 (8.0) | 6 (28.6) |
| – Duration, median (days) | 0.00 (0.00–0.00) | 0.00 (0.00–0.00) | 3.0 (3.0–3.0) | 0.00 (0.00–0.00) | 33.0 (20.0–46.0) | 56.5 (2.0–72.0) |
| Pruritus, n (%): | 1 (4.5) | 0 (0.00) | 1 (4.0) | 3 (14.3) | 1 (4.0) | 2 (9.5) |
| – Duration, median (days) | 14.0 (14.0–14.0) | 0.00 (0.00–0.00) | 30.0 (30.0–30.0) | 91.0 (8.0–105.0) | 31.0 (31.0–31.0) | 24.5 (21.0–28.0) |
| Elevated LFTs, n (%): | 0 (0.00) | 0 (0.00) | 4 (16.0) | 0 (0.00) | 1 (4.0) | 2 (9.5) |
| – Duration, median (days) | 0.00 (0.00–0.00) | 0.00 (0.00–0.00) | 52.0 (21.5–228.0) | 0.00 (0.00–0.00) | 23.0 (23.0–23.0) | 17.5 (4.0–31.0) |
| Endocrinopathy, n (%): | 1 (4.5) | 0 (0.00) | 5 (20.0) | 0 (0.00) | 0 (0.00) | 0 (0.00) |
| – Duration, median (days) | 21.0 (21.0–21.0) | 0.00 (0.00–0.00) | 94.0 (42.0–217.0) | 0.00 (0.00–0.00) | 0.00 (0.00–0.00) | 0.00 (0.00–0.00) |
| Pneumonitis, n (%): | 2 (9.1) | 1 (12.5) | 1 (4.0) | 1 (4.8) | 0 (0.00) | 0 (0.00) |
| – Duration, median (days) | 22.0 (12.0–32.0) | 51.0 (51.0–51.0) | 42.0 (42.0–42.0) | 62.0 (62.0–62.0) | 0.00 (0.00–0.00) | 0.00 (0.00–0.00) |
| Dermatitis, n (%): | 0 (0.00) | 0 (0.00) | 1 (4.0) | 1 (4.8) | 1 (4.0) | 1 (4.8) |
| – Duration, median (days) | 0.00 (0.00–0.00) | 0.00 (0.00–0.00) | 21.0 (21.0–21.0) | 804.0 (804.0–804.0) | 211.0 (211.0–211.0) | 180.0 (180.0–180.0) |
| Hepatitis, n (%): | 1 (4.5) | 0 (0.00) | 1 (4.0) | 2 (9.5) | 0 (0.00) | 0 (0.00) |
| – Duration, median (days) | 28.0 (28.0–28.0) | 0.00 (0.00–0.00) | 154.0 (154.0–154.0) | 29.0 (25.0–33.0) | 0.00 (0.00–0.00) | 0.00 (0.00–0.00) |
Those AEs were more frequently documented which initiated treatment with nivolumab + ipilimumab as 1LOT; although, the average number of AEs was lowest for this cohort indicating a high number of AEs in small number of patients. The most common adverse events were rash, fatigue and diarrhea.
AE: Adverse event; Dab + Tram: Dabrafenib + Trametinib; Ipi: Ipilimumab; Mono: Monotherapy; Nivo: Nivolumab; Nivo + Ipi: Nivolumab + Ipilimumab; Pembro: Pembrolizumab; SD: Standard deviation; LFT: Liver function tests.
Discussion
Our findings showed that a wide range of therapies were used in the treatment of advanced melanoma from 2015 through 2016/2017 and were in line with treatment guidelines at the time [19]. The most common index treatment was ipilimumab monotherapy (21.8%), which is expected given that it was the first approved immunotherapy in this indication. The current treatment guidelines; however, recommend use of nivolumab + ipilimumab over ipilimumab monotherapy as 1LOT therapy [20], which was observed in the data. The use of ipilimumab monotherapy as 1LOT decreased significantly during the observation period; beginning in late 2015, the incidence of nivolumab monotherapy and nivolumab + ipilimumab as 1LOT increased. Interestingly, the use of dabrafenib + trametinib as 1LOT decreased around the same time. Very few patients (<3% for any therapy) had a change in dosing (i.e., delayed treatments, increase or decrease in dose amount), but the duration of therapy was longer than what has been reported in other studies [21,22]. Comparison is difficult; however, since these studies used claims data through 2012 and 2013, respectively, and only had data for ipilimumab and vemurafenib.
Patients included in the analysis were, on average, older than 60 years, which is consistent with disease epidemiology. The population was fairly evenly split between males and females, although a lower proportion of females received nivolumab + ipilimumab as 1LOT. Patients had few comorbid conditions. Most patients had private health insurance or government insurance, so access to medications was not a concern. There were few differences between the cohorts overall.
Efficacy was slightly higher than what has been observed in clinical trials [10,12,14,17,23–26]. Larkin et al. [10] showed median PFS of 6.9 months for nivolumab monotherapy, 11.5 months for nivolumab + ipilimumab and 2.9 months for ipilimumab monotherapy. Similarly, Flaherty et al. [11] showed median PFS of 9.8 months for dabrafenib + trametinib. Long et al. [12] showed median PFS of 9.3 months for dabrafenib + trametinib and 8.8 months for dabrafenib alone. In the two Phase III clinical trials of pembrolizumab, median PFS ranged from 2.7 to 5.5 months [27]. The differences in observed PFS and OS are likely due to the fact this patient population tended to be younger (62.7 years) and with good performance status (ECOG 0 or 1). Multiple treatment options with varied targets as effective and viable 2LOT options may have also contributed to longer survival times than in older clinical studies. It should also be noted that due to the relatively short observation window, there was a significant amount of right censoring in the survival analysis.
AEs were not frequently documented in the medical chart, indicating that a low number of patients experienced a reportable AE during treatment, particularly grade III or IV events. The most common AEs (rash, diarrhea, colitis and arthralgia) were consistent with the clinical trial data [10–14,23–26,28–30]; however, the proportion with a documented AE or serious AE (SAE) was lower. It is possible that common or expected AEs were not documented in the medical chart as part of routine practice and were therefore unreported in this chart review study. Nonetheless, it is reassuring that the rate of clinically significant toxicities in the real world, particularly with nivolumab + ipilimumab, is not greater than what has been reported in clinical trials.
Study strengths and limitations
The strengths of the study included the fact that retrospective chart reviews are an efficient, reliable and verifiable method of data collection. Medical charts are often the best sources of information for documentation of cancer treatments and clinical outcomes. This study filled a gap in existing knowledge of current treatment patterns and clinical outcomes among patients diagnosed with unresectable (stage III) and/or metastatic (stage IV) melanoma who have received 1LOT immunotherapy. The stratified random selection by invitation of study physicians, planned number and geographic distribution of physicians, and robust samples of patient chart data that were collected in this study provided a rich, detailed dataset for analyses and hypothesis generation.
It should be noted that the study results are projectable within the 95% confidence level to the population of melanoma-treating oncologists and the treatment of unresectable (stage III) and metastatic (stage IV) melanoma. Another limitation is that treatment patterns represent only the practices of physicians who agreed to participate in the study and may vary from nonresponding physicians (i.e., those who refused to participate in the study and/or those who failed to complete the patient case report forms on time). An exploratory analysis was conducted, stratifying patients by the physicians practice setting. Physicians were asked to self-report their clinic setting as Academic (12), Community (11) or Academic and Community (3); 19 sites did not self report. At least 66.7%of centers reported following treatment guidelines or protocols, regardless of setting. Use of immunotherapies was similar across all practice settings. It was noted that dabrafenib + trametinib was less common in academic only settings (66.7), and ipilimumab and nivolumab monotherapies were less common in academic and community-based settings. Academic and community-based settings were also more likely to interrupt drug dosing in response to AEs.
Patient characteristics not included in the data set such as income or other family-related variables may influence the prescribing behavior but cannot be accounted for. While the potential for missing data was considered during study design and steps were taken to address these issues before study implementation, introducing multidomain preventive strategies during the pilot testing and implementation phases of this study means that missing data may still occur. For example, the death of a patient might not always be included in the patient chart.
Because of the nature of this chart review study, all clinical outcomes could be influenced by measurement error.
It was not feasible to measure the overall response rate or duration of response due to the short observation window. Future research should allow for a longer follow-up to adequately observe the duration of response.
Conclusion
The results from this retrospective chart review provide insights into the care of patients with unresectable (stage III) and metastatic (stage IV) melanoma in the era of immunotherapy and targeted therapies. These results differ in some areas from clinical trial results, as our data represents actual clinical practice with broad selection criteria and no mandated study procedures or monitoring. Treatment selection evolved over the study period as new treatment options became available. Patient outcomes are much improved compared with historical data in this population, with the highest numerical PFS and OS being seen in patients who received nivolumab + ipilimumab combination. The rate of clinically significant (i.e., grade III to V) AEs reported in patient charts is in line with expectations. Future research should assess patient outcomes over a longer follow-up period.
Future perspective
Targeted therapies and immunotherapies are changing treatment patterns and improving outcomes for patients with unresectable stage III and stage IV melanoma. These treatments are still relatively new to the market and long term PFS and OS data is not yet available in a real-world setting. Additional follow-up assessing survival would be a benefit to patients and clinicians.
This study fills a gap in existing knowledge of current treatment patterns and clinical outcomes among patients diagnosed with unresectable (stage III) and/or metastatic (stage IV) melanoma who have received first line of therapy (1LOT) immunotherapy.
The most common 1LOT treatment in 2015 was ipilimumab (27.5%), which was surpassed by nivolumab (21.5%) in 2016.
A quarter of patients received 2LOT treatment; the most common were pembrolizumab monotherapy, nivolumab monotherapy, and ‘other’ therapy (e.g., vemurafenib monotherapy or combination therapy, temozolomide and dacarbazine).
Among BRAF-positive patients, more than a third received 2LOT, commonly pembrolizumab or nivolumab.
Across LOTs, improved efficacy and demonstrated/documented survival benefit were the primary reasons for treatment choice, while disease progression and drug toxicity were common reasons for treatment discontinuation.
By the end of follow-up, 27.8% of patients had progressed, with the nivolumab + ipilimumab cohort having the highest number of patients who had not progressed.
Over a quarter of patients had died by the end of study follow-up. Nivolumab + ipilimumab had the highest percent of survivors.
A quarter of patients treated with 1LOT had an adverse event (AE) documented in their chart and patients on combination therapy had the highest number of documented adverse events.
Although treatment selections evolved over the study period, treatment outcomes were much better than historical data and reflect real-world outcomes as opposed to more restricted clinical trials.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at:
https://www.futuremedicine.com/doi/suppl/10.2217/cer-2019-0003
Author contributions
A Tarhini, C Atzinger, K Gupte-Singh, C Macahilig and S Rao conceptualized the study. The methodology was overseen by A Tarhini, C Atzinger, K Gupte-Singh and C Macahilig. Formal analysis was done by C Johnson and C Atzinger. Investigation, writing of original draft, review and editing were done by all authors.
Financial & competing interests disclosure
This study was supported by Bristol-Myers Squibb (Princeton, NJ, USA). A Tarhini has disclosed a consulting or advisory role with Bristol-Myers Squibb and having received research funding from Bristol-Myers Squibb, Merck Sharp & Dohme, Amgen, Novartis, Incyte, and Prometheus Laboratories. A Tarhini has also disclosed a consulting or advisory role with Novartis, Genentech-Roche, Array Biopharma, NewLink Genetics, Incyte, HUYA, EMD Serono, Pfizer, Sanofi-Aventis and Regeneron. C Atzinger, C Johnson and C Macahilig serve as paid consultants for Bristol-Myers Squibb. K Gupte-Singh and S Rao are employees of Bristol-Myers Squibb. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
The writing of this manuscript was supported by Bristol-Myers Squibb.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations.
Supplementary Material
File (supplementary_figures.docx)
- Download
- 76.21 KB
References
Papers of special note have been highlighted as: • of interest
1.
National Cancer Institute. Surveillance, Epidemiology, and End Results Program. SEER stat fact sheets: melanoma of the skin (2018). https://seer.cancer.gov/statfacts/html/melan.html.
2.
Bristol-Myers Squibb. Yervoy (ipilimumab) package insert (2011). https://packageinserts.bms.com/pi/pi_yervoy.pdf.
3.
Genentech. Zelboraf (vemurafinib) package insert (2011). https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/202429s012lbl.pdf.
4.
Novartis. Tafinlar (dabrafenib) package insert (2013). https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/202806s002lbl.pdf.
5.
Novartis. Mekinist (trametinib) package insert (2013). https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/204114s001lbl.pdf.
6.
Merck. Keytruda (pembrolizumab) package insert (2014). https://www.merck.com/product/usa/pi_circulars/k/keytruda/keytruda_pi.pdf.
7.
Squib BM. Opdivo (Nivolumab) package insert (2014). https://packageinserts.bms.com/pi/pi_opdivo.pdf.
8.
Genentech. Cotellic (cobimetinib) package insert (2015). https://www.accessdata.fda.gov/drugsatfda_docs/label/2015/206192s000lbl.pdf.
9.
Sharma SP. A new standard of care for metastatic melanoma? Lancet Oncol. 16(1), e8 (2015).
10.
Larkin J, Chiarion-Sileni V, Gonzalez R et al. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N. Engl. J. Med. 373(1), 23–34 (2015).
• Demonstrates a clear survival benefit for combination therapy, while maintaining an acceptable tolerability profile.
11.
Flaherty KT, Infante JR, Daud A et al. Combined BRAF and MEK inhibition in melanoma with BRAF V600 mutations. N. Engl. J. Med. 367(18), 1694–1703 (2012).
12.
Long GV, Stroyakovskiy D, Gogas H et al. Combined BRAF and MEK inhibition versus BRAF inhibition alone in melanoma. N. Engl. J. Med. 371(20), 1877–1888 (2014).
13.
Long GV, Stroyakovskiy D, Gogas H et al. Dabrafenib and trametinib versus dabrafenib and placebo for Val600 BRAF-mutant melanoma: a multicentre, double-blind, Phase III randomised controlled trial. Lancet 386(9992), 444–451 (2015).
14.
Robert C, Karaszewska B, Schachter J et al. Improved overall survival in melanoma with combined dabrafenib and trametinib. N. Engl. J. Med. 372(1), 30–39 (2015).
15.
Long GV, Eroglu Z, Infante JR et al. Five-year overall survival (OS) update from a Phase II, open-label trial of dabrafenib (D) and trametinib (T) in patients (pts) with BRAF V600–mutant unresectable or metastatic melanoma (MM). J. Clin. Oncol. 35(15 Suppl.), 9505 (2017).
16.
Middleton MR, Dalle S, Claveau J et al. Real-world treatment practice in patients with advanced melanoma in the era before ipilimumab: results from the IMAGE study. Cancer Med. 5(7), 1436–1443 (2016).
17.
Uprety D, Bista A, Chennamadhavuni A et al. Survival trends among patients with metastatic melanoma in the pretargeted and the post-targeted era: a US population-based study. Melanoma Res. 28(1), 56–60 (2018).
• Compares overall survival between in the time frame before targeted therapies where available and immediately afterwards, demonstrating a clear survival benefit in the era of targeted therapies. It is limited by the few number of targeted and immunotherapies included.
18.
Cowey CL, Liu FX, Black-Shinn J et al. Pembrolizumab utilization and outcomes for advanced melanoma in US community oncology practices. J. Immunother. 41(2), 86–95 (2018).
• Demonstrates longer overall survival times in a real world setting, with results similar to our study.
19.
Coit DG, Thompson JA, Algazi A et al. Melanoma, Version 2.2016, NCCN Clinical Practice Guidelines in Oncology. J. Natl Compr. Canc. Netw. 14(4), 450–473 (2016).
20.
National Comprehensive Cancer Network. NCCN Guidelines – melanoma. NCCN Guidelines Version 2.2018 (2018).
21.
Ma Q, Chen YJ, Hines DM et al. Patterns of use of systemic therapies among patients with metastatic melanoma: a retrospective claims database analysis in the United States. J. Dermatolog. Treat. 28(6), 549–553 (2017).
• Represents one of the few analysis of real world data in patients with metastatic melanoma. The main findings on duration of treatment were similar to our findings. Its main limitation is that the observation window occurs prior to the availability of most immunotherapies studies in our research with the exception of ipilimumab monotherapy.
22.
Toy EL, Vekeman F, Lewis MC, Oglesby AK, Duh MS. Costs, resource utilization, and treatment patterns for patients with metastatic melanoma in a commercially insured setting. Curr. Med. Res. Opin. 31(8), 1561–1572 (2015).
23.
Hodi FS, O'Day SJ, Mcdermott DF et al. Improved survival with ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 363(8), 711–723 (2010).
24.
Postow MA, Chesney J, Pavlick AC et al. Nivolumab and ipilimumab versus ipilimumab in untreated melanoma. N. Engl. J. Med. 372(21), 2006–2017 (2015).
25.
Robert C, Long GV, Brady B et al. Nivolumab in previously untreated melanoma without BRAF mutation. N. Engl. J. Med. 372(4), 320–330 (2015).
26.
Robert C, Schachter J, Long GV et al. Pembrolizumab versus Ipilimumab in advanced melanoma. N. Engl. J. Med. 372(26), 2521–2532 (2015).
27.
Barone A, Hazarika M, Theoret MR et al. FDA approval summary: pembrolizumab for the treatment of patients with unresectable or metastatic melanoma. Clin. Cancer Res. 23(19), 5661–5665 (2017).
28.
Hodi FS, Chesney J, Pavlick AC et al. Combined nivolumab and ipilimumab versus ipilimumab alone in patients with advanced melanoma: 2-year overall survival outcomes in a multicentre, randomised, controlled, Phase II trial. Lancet Oncol. 17(11), 1558–1568 (2016).
29.
Ribas A, Puzanov I, Dummer R et al. Pembrolizumab versus investigator-choice chemotherapy for ipilimumab-refractory melanoma (KEYNOTE-002): a randomised, controlled, Phase II trial. Lancet Oncol. 16(8), 908–918 (2015).
30.
Weber JS, D'Angelo SP, Minor D et al. Nivolumab versus chemotherapy in patients with advanced melanoma who progressed after anti-CTLA-4 treatment (CheckMate 037): a randomised, controlled, open-label, Phase III trial. Lancet Oncol. 16(4), 375–384 (2015).
Information & Authors
Information
Published In
Copyright
© 2019 Future Medicine Ltd.
History
Received: 3 January 2019
Accepted: 13 February 2019
Published online: 5 March 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Treatment patterns and outcomes for patients with unresectable stage III and metastatic melanoma in the USA. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0003
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Miso Kim, Elizabeth M. Gaughan, Agueda Azpeitia, Aparna Rao, Maria L. Wei, Alexandra So, Xiaochen Zhong, Carola Berking, Ruixuan Jiang, Stéphane Dalle, Caroline Robert, Salma Alam, Tessa Davies, Dirk Debus, Marcin Dzienis, Sarah Danson, Ricky Frazer, Christoffer Gebhardt, Glenn Geidel, Jessica C. Hassel, Inga Hansen, Markus V. Heppt, Lina Hildebrandt, James Isaacs, Koung Jin Suh, Bhumsuk Keam, Yu Jung Kim, Thierry Lesimple, Phillipe Saiag, Ryan Weight, Alicia Delibes, Rosemarie Barnett, Clemens Krepler, Kavita Gandhi, Nawab Qizilbash, Irene Shui, Xiang-Lin Tan, Ryan J. Sullivan, Real-world treatment patterns in stage III and IV melanoma patients: insights from a global multi-center chart review study, Frontiers in Immunology, 10.3389/fimmu.2026.1813387, 17, (2026).
- Dweeti Nayak, Katherine G. Akers, Andrew M. Frederickson, Yves P.V. Mbous, Raquel Aguiar-Ibáñez, Systematic literature review of real-world evidence on overall survival in cancer patients before and after the approval of anti-PD-(L)1 therapy, Frontiers in Oncology, 10.3389/fonc.2025.1615795, 15, (2025).
- Namrata Bhadouria, Aftab Alam, Awaneet Kaur, Unraveling Skin Carcinoma: A Comprehensive Examination of Diagnosis, Treatment Strategies, and Emerging Therapeutic Avenues in Skin Cancer Management, Pharmaceutical Nanotechnology, 10.2174/0122117385282163240220072251, 13, 4, (648-664), (2025).
- John P. Garcia, Olivia A. Ho, Syed Ali Haider, Sahar Borna, Cesar A. Gomez-Cabello, Antonio Jorge Forte, Aaron C. Spaulding, Impact of Physician Specialty on Treatment Costs of Invasive Melanoma, Diseases, 10.3390/diseases12110284, 12, 11, (284), (2024).
- Ahmet Bozkurt, Aycan Sengul, Comparison of photon interaction coefficients for tumor compositions and healthy tissues simulated by Monte Carlo, Journal of Instrumentation, 10.1088/1748-0221/19/07/P07035, 19, 07, (P07035), (2024).
- Kalpana Mangal, Alankrita Madhur, Ishita Bansal, Sinonasal malignant melanoma- Diagnostically hidden Gem, IP Archives of Cytology and Histopathology Research, 10.18231/j.achr.2023.067, 8, 4, (292-295), (2024).
- Brian Ko, Kevin Tao, Lachlan Brennan, Swanand Rakhade, Cynthia X. Chan, Jee-Young Moone, Richard Zhu, Ariel Sher, Samuel Wang, Yadriel Bracero, Ben Fullerton, Beth McLellan, Larisa J. Geskin, Yvonne M. Saenger, Evaluating the efficacy of combination and single-agent immunotherapies in real-world patterns of disease progression and survival of metastatic melanoma patients, Melanoma Research, 10.1097/CMR.0000000000000945, 34, 2, (134-141), (2024).
- Dimitrios Bafaloukos, Panagiotis Kouzis, Panagiotis Gouveris, Ioannis Boukovinas, Konstantinos Kalbakis, Sofia Baka, Georgios Kyriakakis, Despoina Moschou, Aristea Molfeta, Stamatia Demiri, Dimitrios Mavroudis, Filio Spanoudi, Ioannis Dimitriadis, Helen Gogas, Real-world management practices and characteristics of patients with advanced melanoma initiated on immuno-oncology or targeted therapy in the first-line setting during the period 2015–2018 in Greece. The ‘SUMMER’ study: a retrospective multicenter chart review project, Melanoma Research, 10.1097/CMR.0000000000000949, 34, 2, (152-165), (2023).
- You Sung Nam, Martin J. Bullock, David Forner, Matthew H. Rigby, Martin Corsten, Jonathan R.B. Trites, S. Mark Taylor, A case report: Primary malignant melanoma of the glottic larynx – A very rare entity, Otolaryngology Case Reports, 10.1016/j.xocr.2023.100542, 28, (100542), (2023).
- Milica Markelić, Marija Mojić, Dijana Bovan, Sanja Jelača, Zorana Jović, Milica Purić, Djuro Koruga, Sanja Mijatović, Danijela Maksimović-Ivanić, Melanoma Cell Reprogramming and Awakening of Antitumor Immunity as a Fingerprint of Hyper-Harmonized Hydroxylated Fullerene Water Complex (3HFWC) and Hyperpolarized Light Application In Vivo, Nanomaterials, 10.3390/nano13030372, 13, 3, (372), (2023).