Patient characteristics and bleeding events in nonvalvular atrial fibrillation patients treated with apixaban or vitamin K antagonists: real-world evidence from Italian administrative databases
Abstract
Aim: This study aimed to evaluate the risk of major bleeding among two cohorts of nonvalvular atrial fibrillation patients newly initiating a vitamin K antagonist (VKA) or apixaban in a real-world setting in Italy. Patients & methods: A retrospective study using a large administrative database of Italian local health units was performed, using data from ten local health units and patients were included from the date of new initiation of apixaban or VKAs from January 2012 to June 2015. Results: Risk of major bleeding was calculated using an adjusted Cox regression model. Compared with VKA, apixaban had a significantly lower risk of major bleeding (hazard ratio = 0.44 [95% CI: 0.12–0.97]). Conclusion: In this analysis, apixaban was associated with a lower risk of major bleeding compared with VKA.
International guidelines on atrial fibrillation (AF) management suggest that important advances in pharmacologic therapy have occurred in the last decade, particularly with regard to oral anticoagulants (OACs) for stroke prevention in patients with nonvalvular AF (NVAF) [1,2].
OACs currently available in Italy for NVAF include vitamin K antagonists (VKAs) and novel direct OACs (NOACs), such as dabigatran, rivaroxaban, apixaban and edoxaban. The use of any OAC is guided by international and national criteria and described in professional guidelines [1,2]. This guidance balances the risk of stroke as well as bleeding using OAC therapy and as such OAC treatment is recommended for high-stroke risk patients (i.e., those with ≥2 stroke risk factors) and not recommended to AF patients without additional stroke risk factors [3].
In some countries, there are national, regional and local restrictions on the prescription of NOACs. Currently, with regard to the prescription of NOACs under the Italian National Health Service (Servizio Sanitario Nazionale [SSN]), the Italian Drugs Agency (Agenzia Italiana del Farmaco [AIFA]) has made their provision conditional on prescription by authorized specialists who are required to fill in an e-form (web-based) for the therapeutic plan (TP), which helps to identify patients eligible for NOACs [4–6]. The application of the rules of the TP in routine clinical practice by physicians is not well known [7], but according to the TP, a patient can only be prescribed an NOAC if they are at an increased risk of bleeding based on fulfilling at least one of the following criteria: both CHA2DS2-VASc (score for AF stroke risk) ≥ 1 and HAS-BLED (score for major bleeding risk) > 3; or additionally if they have a Time in Therapeutic Range < 70%; or international normalized ratio (INR) monitoring difficulties.
In order to understand AF management in Italy, this study aims to describe patient characteristics and to evaluate the risk of major bleeding between two cohorts of NVAF patients newly initiating a VKA or apixaban in a real-world setting in Italy.
Patients & methods
Study source
The study was conducted using a large administrative and laboratory database of ten Italian local health units (LHUs), geographically distributed throughout Italy. In particular, the following databases were used: the Beneficiaries’ database, which contains all demographic data for patients (deaths included); the Outpatients and Inpatients Pharmaceuticals Prescription database, which contains all drugs supplied for patients, including the Anatomical-Therapeutic-Chemical (ATC) code of the drugs dispensed, the number of units per package, the dose and the unit cost per pack for each drug purchased for the patient; the Hospital Discharge database, which contains all hospitalization data for patients, with the primary and secondary discharge diagnosis codes classified according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM); and the Outpatient Specialist Services database, which contains all information about laboratory assessments, diagnostic tests and visit requests for patients and the dates on which these were performed. A patient code, available in each database, allows electronic linkage between all databases. To guarantee patient privacy, an anonymous univocal numeric code was assigned to each subject included in the study. No personally identifiable information related to patients were provided to the authors. According to the Italian guidelines regarding the conduct of observational studies [8], established by the Italian Drug Agency, ‘Agenzia Italiana del Farmaco – AIFA’ on 20 March 2008, the local Ethics Committee of each participating LHU approved the study. Informed consent was not obtained, since it is not required when using encrypted retrospective information for research purposes.
Cohort definition
This study was a retrospective cohort study from 1 January 2012 to 31 December 2015 (study period) that included all beneficiaries within each LHU aged ≥18 years with an NVAF diagnosis (ICD-9-CM code: 427.31), who received a first prescription (index date, ID) of apixaban (ATC code: B01AF02) or VKA (only warfarin, ATC code: B01AA03). The characterization period was defined as the 1-year period prior to the ID used to ascertain patient demographic and clinical characteristics. All patients included in the analysis were followed until treatment regimen change (discontinuation or switch), leaving the database, death or end of follow-up period.
Patients were excluded if they had a prior prescription of the index OAC; had a record indicating valvular AF (ICD-9-CM codes: 394.0, 394.1, 394.2, 394.9, 396.0, 396.1, 396.8, 396.9, 424.0, 745.xx, V42.2, V43.3 for mitral stenosis or artificial heart valves) at any time during the study period; had a record indicating venous thromboembolism (ICD-9-CM codes: 451-453, 671.3, 671.4, 671.9 for deep vein thrombosis; or ICD-9-CM codes: 415.1, 673.2, 673.8 for pulmonary embolism) during the characterization period and including ID; had a record of knee or hip replacement (V43.64, V43.65) 6 weeks before and including the ID; had more than one OAC (apixaban or VKA) exposure, which started on the same date or subsequent OAC exposures after the first.
Patients were classified into two groups according to anticoagulant therapies received at ID: VKA and apixaban.
Variable definitions
Data on age, gender and the prevalence of selected comorbidities were obtained during the characterization period for each patient in the study cohort.
History of stroke risk factors such as hypertension (ICD-9-CM codes: 401-405), diabetes mellitus (ICD-9-CM code: 250), congestive heart failure (ICD-9-CM code: 428), arterial embolism (ICD-9-CM codes: 444-445), stroke or transient ischemic attack (ICD-9-CM codes: 430-436), previous bleeding events and gastrointestinal ulceration (ICD-9-CM codes: 531-533) and kidney disease (ICD-9-CM codes: 582-585) on or ever prior to ID were also evaluated.
Comorbidities were measured using the Charlson Comorbidity Index (CCI) [9]. The CCI score in classes (0/1–2/3–4/5+) was calculated for each patient by summing points related to the comorbidities reported in Supplementary Table 1. Comorbidities were defined based on discharge diagnoses (ICD-9-CM codes) recorded on, or ever prior to the ID and pharmaceutical prescriptions (ATC codes; used as a proxy for diagnosis) recorded in the characterization period. The CCI score reflects a patient’s overall health status.
The patients’ stroke and bleeding risk were calculated using CHA2DS2-VASc and HAS-BLED scores, respectively [1,10–12].
The CHA2DS2-VASc score in classes (from 0 to 9) was calculated for each patient by summing points related to the risk score components reported in Supplementary Table 2. Risk score components were defined based on records of diagnosis (ICD-9-CM codes) or prescriptions for specific drugs (ATC codes; used as a proxy for diagnosis).
The HAS-BLED score in classes (from 0 to 7) was calculated for each patient by summing points related to the risk score components reported in Supplementary Table 3. Risk score components were defined based on records of diagnosis (ICD-9-CM codes) or prescriptions for specific drugs (ATC codes; used as a proxy for diagnosis).
The primary end point was the first impatient admission for major bleeding, including gastrointestinal bleeding, intracranial bleeding and bleeding from other sites. ICD-9-CM codes are given in Table 1.
| Primary outcome | ICD-9-CM codes cohort (n, %) |
|---|---|
| Gastrointestinal bleeding | 456.0, 456.20, 530.82, 531.0x, 531.2x, 531.4x, 531.6x, 532.0x, 532.2x, 532.4x, 532.6x, 533.0x, 533.2x, 533.4x, 533.6x, 534.0x, 534.2x, 534.4x, 534.6x, 535.01, 535.11, 535.21, 535.31, 535.41, 535.51, 535.61, 537.83, 562.02, 562.03, 562.12, 562.13, 568.81, 569.3, 569.85, 578.x; Procedure Code: 44.43 |
| Intracranial bleeding | 430.xx, 431.xx, 432.0, 432.1, 432.9, 852.0x, 852.2x, 852.4x, 853.0x |
| Bleeding from other sites | 285.1, 360.43, 362.43, 362.81, 363.61, 363.62, 363.72, 364.41, 372.72, 374.81, 376.32, 377.42, 379.23, 423.0x, 596.7x, 599.7x, 602.1x, 620.1, 621.4, 626.2, 626.5, 626.7, 626.8, 626.9, 719.1x, 782.7, 784.7, 784.8, 786.3x, 958.2, 997.02, 998.11; Procedure code: 99.04 |
Outcomes were identified using primary or secondary diagnosis/procedure on inpatient claims.
ICM-9-CM: International Classification of Disease, Ninth Edition, Clinical Modification.
Statistical analysis
Continuous variables were reported as mean and standard deviation (±SD) and compared using the t-test for independent samples, whereas categorical variables were expressed as numbers and percentages and compared using the Chi-square test. The covariate balance was assessed also using standardized differences.
To visualize how the risk of the study outcome evolved over time since ID, we calculated and displayed the cumulative incidence rate of major bleeding events at 3, 6, 9 and 12 months accounting for the competing risk of mortality.
As this is an observational study and the patients were not randomly assigned to each treatment group, in order to reduce selection bias, we used a propensity score analysis to balance the two different anticoagulant treatment groups on possible baseline confounders. First, a logistic regression model was used to predict treatment assignment by all observed baseline characteristics listed above. Patients were then grouped into strata determined by the quintiles of the estimated propensity score. A random sampling method was then used and, within each stratum, a subset of VKA cases was randomly chosen, so that the final sample size equaled that of the apixaban group [13]. As the standardized difference values decreased after propensity score adjustment but significant differences in patient characteristics still remained, we used an adjusted Cox proportional hazard regression to model time to first major bleeding event accounting for the competing risk of mortality. Because of a low number of events, backward covariate selection was used to achieve a parsimonious model. The proportional hazards assumption was not violated.
As results referring to less than four patients are potentially patient identifiable ‘Codice in materia di protezione dei dati personali (Code for protection of personal data; D.Lgs. 196/2003)’ [14] – they have been reported as not issuable (NI).
p-values ≤ 0.05 were considered to be statistically significant. All statistical analyses were performed using STATA SE, version 12.0. Data management was carried out using Microsoft SQL Server 2012.
Results
After applying inclusion and exclusion criteria, 9914 NVAF patients were enrolled (Figure 1).
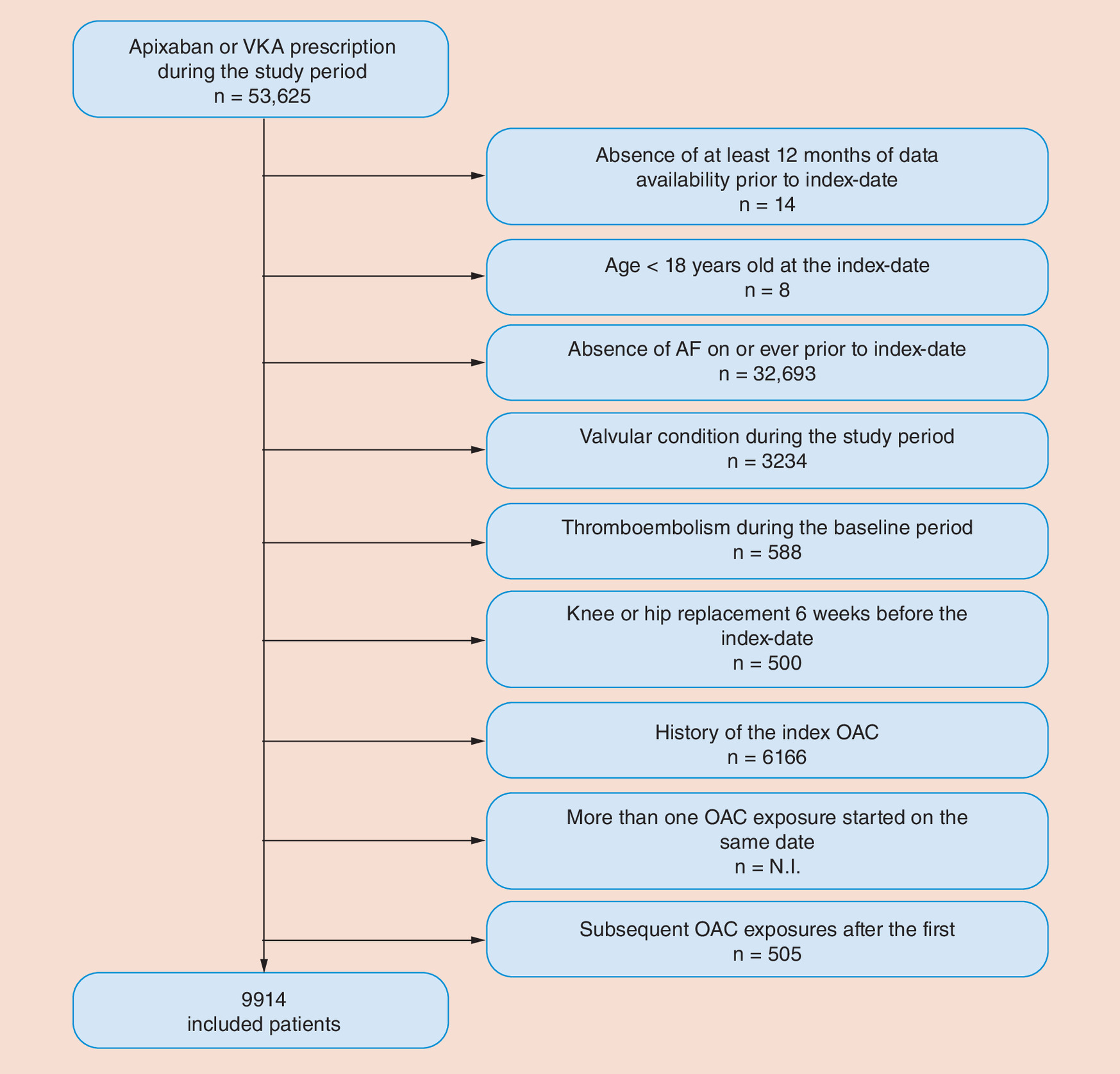
Figure 1. Flow chart of the inclusion/exclusion criteria.
N.I.: Not issuable; OAC: Oral anticoagulants; VKA: Vitamin K antagonist.
Among them, 1521 (15.3%) patients initiated apixaban and 8393 (84.7%) VKA. The demographic and baseline characteristics of the study population are shown in Table 2.
| Apixaban cohort (n, %) | VKA cohort (n, %) | p-value | Standardized differences | |
|---|---|---|---|---|
| Patients | 1521 | 8393 | ||
| Age at ID, median (min–max) | 79 (35–100) | 78 (20–104) | <0.001 | 0.185 |
| Gender, male | 749 (49.2) | 4390 (52.3) | 0.028 | -0.061 |
| History of stroke risk factors on or ever prior to ID | ||||
| – Stroke or transient ischemic attack | 242 (15.9) | 1263 (15.0) | 0.388 | 0.024 |
| – Thromboembolism | 9 (0.6) | 121 (1.4) | 0.007 | -0.085 |
| – Congestive heart failure | 1015 (66.7) | 5940 (70.8) | 0.002 | -0.087 |
| – Hypertension | 1461 (96.1) | 8026 (95.6) | 0.449 | 0.021 |
| – Diabetes | 359 (23.6) | 1943 (23.2) | 0.700 | 0.011 |
| History of events/conditions on or ever prior to ID | ||||
| – Gastrointestinal ulceration | 12 (0.8) | 15 (0.2) | <0.001 | 0.088 |
| – Gastrointestinal bleeding | 36 (2.4) | 48 (0.6) | <0.001 | 0.150 |
| – Intracranial bleeding | 20 (1.3) | 35 (0.4) | <0.001 | 0.097 |
| – Other bleeding | 65 (4.3) | 285 (3.4) | 0.088 | 0.046 |
| – Major bleeding events | 105 (6.9) | 344 (4.1) | <0.001 | 0.123 |
| Kidney disease prior to ID | ||||
| – Kidney failure | 74 (4.9) | 802 (9.6) | <0.001 | -0.182 |
| OAC history prior to ID | ||||
| – OAC-naive patients | 967 (63.6) | 8343 (99.4) | <0.001 | 1.039 |
ID: Index date; OAC: Oral anticoagulants; VKA: Vitamin K antagonist.
Among patients initiating VKA, the median age was 78 years. Patients in the VKA cohort were on average younger than the apixaban users (median age: 79 years; p < 0.001). The percentage of males was 49.2% among apixaban users and 52.3% among VKA users (p = 0.028). The standardized differences (SD) showed that VKA and apixaban cohorts differed in age, and having a history of gastrointestinal bleeding, major bleeding or kidney disease and also having an OAC history prior to ID (SD ≥ 0.1).
Apixaban patients were more likely to have a history of major bleeding (6.9 vs 4.1% of VKA; p < 0.001). The distribution of CCI scores for the included patients stratified according to index medication is presented in Table 3. More than 60% of patients in both cohorts had a CCI score of 1–2 (62.5 and 62.6% for apixaban and VKA cohort, respectively). Details on the distribution of patients according to the CHA2DS2-VASc and HAS-BLED scores are reported in Tables 4 and 5. The proportion of patients with high bleeding risk score (HAS-BLED ≥ 3) at baseline was 47.6% among apixaban users and 46.2% among VKA users (p = 0.009).
| Charlson Co-morbidity Index scores | Apixaban cohort (n, %) | VKA cohort (n, %) | p-value | Standardized differences |
|---|---|---|---|---|
| 0 | 151 (9.9) | 740 (8.8) | 0.458† | |
| 1–2 | 950 (62.5) | 5257 (62.6) | 0.025 | |
| 3–4 | 333 (21.9) | 1933 (23.0) | ||
| 5+ | 87 (5.7) | 463 (5.5) |
†Overall Chi-square test among different Charlson Comorbidity Index level groups.
VKA: Vitamin K antagonist.
| CHA2DS2-VASc score at index date | Apixaban cohort (n, %) | VKA cohort (n, %) | p-value | Standardized differences |
|---|---|---|---|---|
| 0 | N.I. (-) | 25 (0.3) | 0.002† | -0.065 |
| 1 | 25 (1.6) | 195 (2.3) | ||
| 2 | 89 (5.9) | 731 (8.7) | ||
| 3 | 270 (17.8) | 1365 (16.3) | ||
| 4 | 448 (29.5) | 2273 (27.1) | ||
| 5 | 423 (27.8) | 2254 (26.9) | ||
| 6 | 162 (10.7) | 1034 (12.3) | ||
| 7 | 76 (5.0) | 407 (4.8) | ||
| 8 | 25 (1.6) | 104 (1.2) | ||
| 9 | N.I. (-) | 5 (0.1) |
†Overall Chi-square test among different CHA2DS2-VASc level groups.
N.I.: Not issuable; VKA: Vitamin K antagonist.
| HAS-BLED scores at index date | Apixaban cohort (n, %) | VKA cohort (n, %) | p-value | Standardized differences |
|---|---|---|---|---|
| 0 | 10 (0.7) | 75 (0.9) | 0.009† | |
| 1 | 93 (6.1) | 761 (9.1) | ||
| 2 | 693 (45.6) | 3678 (43.8) | -0.038 | |
| 3 | 590 (38.8) | 3154 (37.6) | ||
| 4 | 120 (7.9) | 670 (8.0) | ||
| 5 | 14 (0.9) | 53 (0.6) | ||
| 6 | N.I. (-) | N.I. (-) | ||
| 7 | 0 | N.I. (-) | ||
| 8 | 0 | 0 |
†Overall Chi-square test among different HAS-BLED level groups.
N.I.: Not issuable; VKA: Vitamin K antagonist.
The median follow-up was 10 months (min–max: 1–41 months) for patients treated with VKA and 4 months (min–max: 1–17 months) for patients treated with apixaban. The 1-year cumulative incidence of major bleeding (Figure 2) was 1.2% among apixaban initiators and 2.5% among VKA initiators.

Figure 2. Incidence of major bleeding: apixaban cohort versus vitamin K antagonist cohort.
VKA: Vitamin K antagonist.
Number of patients at risk (% with major bleeding) was: 859 (0.4%) and 6649 (0.8%) at 3 months, 530 (0.5%) and 5217 (1.5%) at 6 months, 283 (0.9%) and 4221 (2%) at 9 months, 114 (1.2%) and 3469 (2.5%) at 12 months for apixaban and VKA cohorts, respectively.
After performing the propensity score and the random selection within the strata, the number of patients included in the analysis was reduced to 3042. In the Cox proportional hazard regression analysis, the variables that entered into the model after the selection process were: age, gender, gastrointestinal ulceration, major bleeding events and type of anticoagulant treatment. Compared with VKA, apixaban had a significantly lower risk of major bleeding (hazard ratio = 0.44; 95% CI: 0.12-0.97; Table 6).
| Type of treatment | HR | 95% CI per HR | p-value | |
|---|---|---|---|---|
| VKA (reference) | 1.00 | |||
| Apixaban | 0.44 | 0.20 | 0.97 | 0.044 |
| Age | 1.04 | 1.00 | 1.09 | 0.035 |
| Gender (male) | 2.22 | 1.18 | 4.18 | 0.014 |
| Previous gastrointestinal ulceration | 7.51 | 1.76 | 31.96 | 0.006 |
| Previous major bleeding | 4.83 | 2.18 | 10.66 | <0.001 |
HR: Hazard ratio; VKA: Vitamin K antagonist.
Discussion
The use of NOACs has increased steadily following marketing approval; [15–18] however, their relative safety in NVAF patients in real-world clinical practice remains under evaluation. Existing studies on the real-world safety of NOACs have reported conflicting findings [19–23]. A recent systematic review and meta-analysis focused on the real-world safety of apixaban included 16 studies and reported a significant reduction in major bleeding as compared with warfarin (pooled relative risk [95% CI]: 0.62 [0.51, 0.75]). However, none of the included studies were based in Italy [24].
The current retrospective cohort study, therefore, analyzed administrative and laboratory databases from ten Italian LHUs to describe patient characteristics and to evaluate the risk of major bleeding between two cohorts of NVAF patients newly initiating a VKA or apixaban in a real-world setting in Italy.
This study shows that NVAF patients who initiated VKA did not differ in some characteristics as compared with those who received apixaban (i.e., history of stroke risk factors) but for others, for example, age and previous major bleeding events they did.
The Italian NHS reimburses NOACs only if at least one of the following points is achieved: both CHA2DS2-VASc ≥ 1 and HAS-BLED > 3; or Time in Therapeutic Range < 70%; or documented poor INR control with VKA, and objective impossibility to perform blood tests for INR measurement. It is, therefore, clear how such prescription schemes may strongly impede the dissemination of a highly effective class of drugs to the wider groups of patients recommended for therapy based on major international clinical guidelines (i.e., those with ≥2 stroke risk factors irrespective of bleeding risk). Despite the presence of the TP, surprisingly in our cohort of study the patient bleeding (HAS-BLED score) and stroke (CHA2DS2-VASc score) risks and the prevalence of comorbidities (CCI score), between the VKA and apixaban groups were only slightly different.
After controlling for key significant differences in patient characteristics we found that, compared with warfarin, apixaban was associated with a lower risk of major bleeding. Our findings regarding apixaban are consistent with the findings of other recent studies in the real-world setting and the findings from the ARISTOLE trial [15,19,25–28]. Our estimate of the magnitude of relative risk reduction in major bleeding with apixaban of 0.44 [0.20, 0.97] (as compared with VKA) was also consistent with the estimate reported in the recent systematic review and meta-analysis including 16 studies. However, based on the small number of bleeding episodes in NOAC users, this limited the statistical power to confirm the reduction in bleeding risk in further adjusted analyses. Future studies with more patients on NOACs and with a greater control for potential confounders will allow comparisons between these drugs for multiple clinical outcomes.
A key strength of this study is that our cohort of patients reflected real clinical practice, however, the results must be interpreted, taking into account of limitations related to the observational nature of the study and limitations related to data collected through administrative and laboratory databases. As a consequence, we cannot exclude the possibility that some data may have been missed due to inaccurate or lost medical records. Since information concerning comorbidities and the information related to disease severity is not routinely captured in administrative databases, a proxy for identifying comorbidities was used based on the use of specific drugs and hospitalizations. Despite this method being widely used, we cannot exclude that this can lead to a bias relative to the actual prevalence of comorbidities (possible underestimation). Bleeding events were identified through codes used in the datasets, and not prospectively using criteria defined by international societies.
Conclusion
In recent years, the development of NOACs provides a promise of less complicated management of anticoagulation compared with VKA. However, many patients are not treated because of concerns of major bleeding and limited experience with NOACs outside the research setting. After controlling for differences in patient characteristics, in our study apixaban was associated with a lower major bleeding risk as compared to VKA. Our findings provide evidence of the safety of NOAC use in the real-world setting and may facilitate clinical decision-making, especially in Italy where data on the real-world use of NOACs have been lacking. Nevertheless, the final choice between NOACs and VKA will ultimately depend on individual patient risk and preferences. Future additional studies with larger sample sizes and longer follow-up may be needed to further confirm the results of this early evaluation of the effect of apixaban versus VKA on risk of major bleeding.
Patients with atrial fibrillation (AF) have up to a fivefold increased risk of stroke.
Anticoagulation therapy is offered to patients for stroke prevention, however, these treatments can lead to an increased risk of bleeding.
Warfarin has up until recently been the main anticoagulation agent available. Recent advances in AF treatment have led to the availability of novel or direct oral anticoagulants, such as apixaban.
Given the availability of newer treatments, it is unclear how patients are currently treated in the ‘real-world’ in Italy.
In this investigation, we sought to describe AF patients receiving either warfarin or apixaban and to compare the risk of major bleeding in these groups of patients.
We found that patients being initiated on apixaban differed to those being initiated on warfarin.
After controlling for these differences in patient characteristics, the risk of major bleeding was significantly less in patients taking apixaban as compared with patients taking warfarin.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Acknowledgments
LHU group consists of the following members: M Andretta (Local Pharmaceutical Service, Verona Local Health Authority, Verona, Italy); C Montinari (Pharmaceutical Department ASL Lecce, Local Health Unit Lecce, Lecce, Italy); E Nava (Department of Pharmacy, Local Health Unit Naples 3 South, Naples, Italy); A Pisterna (Local Pharmaceutical Service, Local Health Unit Vercelli, Vercelli, Italy); L Poggi (Pharmacy Complex Operation Unit, Local Health Unit VCO, Omegna, Italy); G Riccioni (Local Pharmaceutical Service, Roma 1, Italy); S Sonzogni (Local Pharmaceutical Service, Bergamo, Italy); N Storti (Health Directorate, ASUR Marche, Ancona, Italy); A Vercellone (Department of Pharmacy, Local Health Unit Naples 3 South, Napoli, Italy), E Vighi (Pharmacy Complex Operation Unit, Local Health Unit VCO, Omegna, Italy) and M Pisani M and F Lena (USL Toscana Sud Est Local Health Unit, Grosseto, Italy). S Ramagopalan et al. are the copyright holder.
Financial & competing interests disclosure
This study was funded by Bristol-Myers Squibb and Pfizer. S Ramagopalan, V Allan, G Stynes, C Toma and F DeSolda are employees of Bristol-Myers Squibb. S Ramagopalan, G Stynes and F DeSolda are shareholders in Bristol-Myers Squibb. S Saragoni, LD Esposti, D Alessandrini, V Perrone and S Buda are employees of Clicon. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_file.docx)
- Download
- 24.52 KB
References
1.
Kirchhof P, Benussi S, Kotecha D et al. 2016 ESC guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. Heart J. 37, 2893–2962 (2016).
2.
Heidbuchel H, Verhamme P, Alings M et al. Updated European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist anticoagulants in patients with non-valvular atrial fibrillation. Europace 17, 1467–1507 (2015).
3.
Lip G, Freedman B, De Caterina R, Potpara TS. Stroke prevention in atrial fibrillation: past, present and future. Comparing the guidelines and practical decision-making. Thromb. Haemost. 117, 1230–1239 (2017).
4.
Agenzia Italiana del Farmaco (AIFA). AIFA Concept paper. I nuovi anticoagulanti orali nella prevenzione di ictus e tromboembolismo sistemico in pazienti con fibrillazione atriale non valvolare. www.agenziafarmaco.gov.it/sites/default/files/version_2012_09_24_cp_noacs_1.pdf
5.
Filippi A. Nuovi Anticoagulanti orali per la prevenzione di ictus ed embolia sistemica nella fibrillazione atriale non valvolare. S.I.M.G. Società Italiana di Medicina Generale Area Cardiovascolare. www.dbcf.unisi.it/sites/st13/files/allegati/02-02-2015/nao.pdf
6.
Nardi F, Gulizia MM, Colivicchi F et al. ANMCO position paper: direct oral anticoagulants for stroke prevention in atrial fibrillation: clinical scenarios and future perspectives. Eur. Heart J. Suppl. 19, D70–D88 (2017).
7.
Perrone V, Sangiorgi D, Buda S, Degli Esposti L. Farmacoutilizzazione e consumo di risorse sanitarie nei pazienti in terapia con anticoagulanti orali: il progetto Nemawashi. SPS n. 2, 2017 Supplemento a Politiche sanitarie, 18, 2 (2017).
8.
Agenzia Italiana del Farmaco (AIFA). Guideline for the classification and conduction of the observational studies on medicines. (2010). www.agenziafarmaco.gov.it/ricclin/sites/default/files/files_wysiwyg/files/CIRCULARS/Circular%2031st%20May%202010.pdf
9.
Gonnella JS, Louis DZ, Gozum MV, Callahan CA, Barnes CA. Disease Staging Clinical and Coded Criteria (Version 5.26). Thomson Medstat, Ann Arbor, MI, USA (2010).
10.
Pisters R, Lane DA, Nieuwlaat R, de Vos CB, Crijns HJ, Lip GY. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey. Chest 138, 1093–100 (2010).
11.
Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the Euro Heart Survey on atrial fibrillation. Chest 137, 263–272 (2010).
12.
Camm AJ, Kirchhof P, Lip GY et al. Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Europace 12, 1360–1420 (2010).
13.
Posner MA, Ash AS (Eds). Comparing weighting methods in propensity score analysis. www.stat.columbia.edu/∼gelman/stuff_for_blog/posner.pdf
14.
Opinion 05/2014 on Privacy and Data Protection. http://ec.europa.eu/justice/data-protection/article-29/documentation/opinion-recommendation/files/2014/wp216_it.pdf
15.
Adeboyeje G, Sylwestrzak G, Barron JJ et al. Major bleeding risk during anticoagulation with warfarin, dabigatran, apixaban, or rivaroxaban in patients with nonvalvular atrial fibrillation. J. Manag. Care Spec. Pharm. 23, 968–978 (2017).
16.
Weitz JI, Semchuk W, Turpie AG et al. Trends in prescribing oral anticoagulants in Canada, 2008–2014. Clin. Ther. 37, 2506–2514.e4 (2015).
17.
Gadsbøll K, Staerk L, Fosbøl EL et al. Increased use of oral anticoagulants in patients with atrial fibrillation: temporal trends from 2005 to 2015 in Denmark. Eur. Heart J. 38(12), 899–906 (2017).
18.
Loo SY, Dell'Aniello S, Huiart L, Renoux C. Trends in the prescription of novel oral anticoagulants in UK primary care: novel oral anticoagulant prescription trends. Br. J. Clin. Pharmacol. 83, 2096–2106 (2017).
19.
Deitelzweig S, Bruno A, Trocio J et al. An early evaluation of bleeding-related hospital readmissions among hospitalized patients with nonvalvular atrial fibrillation treated with direct oral anticoagulants. Curr. Med. Res. Opin. 32, 573–582 (2016).
20.
Graham DJ, Reichman ME, Wernecke M et al. Stroke, bleeding, and mortality risks in elderly medicare beneficiaries treated with dabigatran or rivaroxaban for nonvalvular atrial fibrillation. JAMA Intern. Med. 176, 1662–1671 (2016).
21.
Noseworthy PA, Yao X, Abraham NS, Sangaralingham LR, McBane RD, Shah ND. Direct comparison of dabigatran, rivaroxaban, and apixaban for effectiveness and safety in nonvalvular atrial fibrillation. Chest 150, 1302–1312 (2016).
22.
Yao X, Abraham NS, Sangaralingham LR et al. Effectiveness and safety of dabigatran, rivaroxaban, and apixaban versus warfarin in nonvalvular atrial fibrillation. J. Am. Heart Assoc. 5, e003725 (2016).
23.
Chang HY, Zhou M, Tang W, Alexander GC, Singh S. Risk of gastrointestinal bleeding associated with oral anticoagulants: population based retrospective cohort study. BMJ 350, h1585 (2015).
24.
Proietti M, Romanazzi I, Romiti GF, Farcomeni A, Lip GYH. Real-world use of apixaban for stroke prevention in atrial fibrillation: a systematic review and meta-analysis. Stroke 49, 98–106 (2018).
25.
Yao X, Abraham NS, Sangaralingham LR et al. Effectiveness and safety of dabigatran, rivaroxaban, and apixaban versus warfarin in nonvalvular atrial fibrillation. J. Am. Heart Assoc. 5(6), (2016) (Epub ahead of print).
26.
López-López JA, Sterne JAC, Thom HHZ et al. Oral anticoagulants for prevention of stroke in atrial fibrillation: systematic review, network meta-analysis, and cost effectiveness analysis. BMJ 359, j5058 (2017).
27.
Amin A, Keshishian A, Vo L et al. Real-world comparison of all-cause hospitalizations, hospitalizations due to stroke and major bleeding, and costs for non-valvular atrial fibrillation patients prescribed oral anticoagulants in a US health plan. J. Med. Econ. 21(3), 244–253 (2018).
28.
Granger CB, Alexander JH, McMurray JJ et al. Apixaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 365, 981–992 (2011).
Information & Authors
Information
Published In
Copyright
© 2018 Sreeram Ramagopalan et al.
History
Received: 14 June 2018
Accepted: 27 July 2018
Published online: 13 August 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Patient characteristics and bleeding events in nonvalvular atrial fibrillation patients treated with apixaban or vitamin K antagonists: real-world evidence from Italian administrative databases. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0054
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Allie Cichewicz, Shantanu Jawla, Priccila Zuchinali, Morodoluwa Akin-Fajiye, Daniela Massierer, Italo Porto, Xavier Garcia-Moll, Real-world evidence comparing oral anticoagulants for NVAF in Europe: a systematic review and network meta-analysis, Future Cardiology, 10.1080/14796678.2025.2484119, 21, 6, (371-390), (2025).
- Benjamin J. R. Buckley, Deirdre A. Lane, Peter Calvert, Juqian Zhang, David Gent, C. Daniel Mullins, Paul Dorian, Shun Kohsaka, Stefan H. Hohnloser, Gregory Y. H. Lip, Effectiveness and Safety of Apixaban in over 3.9 Million People with Atrial Fibrillation: A Systematic Review and Meta-Analysis, Journal of Clinical Medicine, 10.3390/jcm11133788, 11, 13, (3788), (2022).
- Valentina Lorenzoni, Salvatore Pirri, Giuseppe Turchetti, Cost-Effectiveness of Direct Non-Vitamin K Oral Anticoagulants Versus Vitamin K Antagonists for the Management of Patients with Non-Valvular Atrial Fibrillation Based on Available “Real-World” Evidence: The Italian National Health System Perspective, Clinical Drug Investigation, 10.1007/s40261-021-01002-z, 41, 3, (255-267), (2021).
- Katrin Krueger, Kathrin Jobski, Annemarie Voss, Ulrike Haug, Different Risk Profiles of European Patients Using Direct Oral Anticoagulants or Vitamin K Antagonists: a Rapid Review, Current Epidemiology Reports, 10.1007/s40471-020-00257-y, 7, 4, (290-299), (2020).
- Sreeram V Ramagopalan, Antoni Sicras-Mainar, Carlos Polanco-Sanchez, Robert Carroll, Jaime F de Bobadilla, Patient characteristics and stroke and bleeding events in nonvalvular atrial fibrillation patients treated with apixaban and vitamin K antagonists: a Spanish real-world study, Journal of Comparative Effectiveness Research, 10.2217/cer-2019-0079, 8, 14, (1201-1212), (2019).
- Ameenathul M. Fawzy, Wang-Yang Yang, Gregory YH. Lip, Safety of direct oral anticoagulants in real–world clinical practice: translating the trials to everyday clinical management, Expert Opinion on Drug Safety, 10.1080/14740338.2019.1578344, 18, 3, (187-209), (2019).