Effects of calcimimetics on long-term outcomes in dialysis patients: literature review and Bayesian meta-analysis
Abstract
Aim: Randomized controlled trials (RCTs) with clinical outcomes are considered the gold standard for regulatory approval. However, by design they are only able to answer a small number of clinical questions. Other high-quality studies are required for clinical decision-making. The EVOLVE was the largest RCT, evaluating the effects of cinacalcet on clinical outcomes among adult patients receiving maintenance dialysis suffering from secondary hyperparathyroidism. While the EVOLVE trial did not reach its primary end point, imbalance in subjects’ age at randomization and discontinuation rates are two of the reasons that the lack of mortality benefit is in question. We undertook a systematic literature review and Bayesian meta-analysis combining randomized and observational studies on the estimated effects of the oral calcimimetic cinacalcet on clinical outcomes including all-cause mortality, cardiovascular-related mortality, hospitalization for cardiovascular events, fracture and parathyroidectomy among patients on maintenance dialysis. Methods: Data sources included MEDLINE, EMBASE and Cochrane Central Register of Controlled Trials databases. RCTs and observational studies were included. Data extraction was completed by two authors independently and in duplicate determined the methodological quality of the studies and extracted data. Results: Of 564 unique citations identified, 16 studies were included: six observational studies and ten RCTs. Four high-quality studies (two observational and two RCTs) were deemed suitable for meta-analysis. Results indicated a statistically significant reduction in the risk of death associated with cinacalcet (hazard ratio: 0.83; 95% credible interval: 0.78–0.89).Conclusion: The results of this meta-analysis indicate that treatment of secondary hyperparathyroidism with calcimimetic therapy may in fact reduce mortality among patients receiving maintenance dialysis. This finding provides justification for a well-designed and adequately powered randomized trial to definitively address the question.
Cinacalcet (Sensipar®/Mimpara®, Amgen Inc., CA, USA) is an oral calcimimetic agent available since 2004 for the reduction of parathyroid hormone (PTH) in patients with secondary hyperparathyroidism (sHPT) on maintenance dialysis [1,2]. Randomized controlled trials (RCTs) have established that cinacalcet lowers serum concentrations of PTH, calcium and phosphate relative to placebo [3–8]. Four randomized trials found that cinacalcet significantly reduced the likelihood of parathyroidectomy, fracture and cardiovascular (CV) hospitalization, improved self-reported physical function and diminished pain [9]. To examine the effect on long-term outcomes, the EVOLVE trial tested cinacalcet versus placebo in 3883 patients with moderate-to-severe sHPT on a composite end point including mortality, myocardial infarction, hospitalization for unstable angina, heart failure or peripheral vascular event [10]. The EVOLVE trial's prespecified primary analysis, an unadjusted intention-to-treat (ITT) comparison, showed the relative hazard of the composite end point in the cinacalcet group versus the placebo group of 0.93 (95% CI: 0.85–1.02; p = 0.11). The EVOLVE investigators concluded that “cinacalcet did not significantly reduce the risk of death or major CV events in patients with moderate-to-severe sHPT who were undergoing dialysis”.
However, there are reasons to suspect that the finding is not conclusive. First, after adjustment for baseline characteristics, the relative hazard for the primary composite end point was 0.88 (95% CI: 0.79–0.97; p = 0.008), in other words, statistically significant. Second, there was a high degree of crossover: more than one in five patients randomized to placebo was treated with cinacalcet. Third, approximately one in seven patients underwent parathyroidectomy, reducing intergroup differences in PTH control and biasing the estimate of treatment effect toward the null [10]. As a result, analyses adjusted for baseline characteristics showed a nominally significant benefit of cinacalcet on the primary composite end point and on mortality. Fourth, in a prespecified subgroup analysis based on an age threshold of 65 years, adjusted analyses indicated that among older patients, the adjusted relative hazard for mortality was 0.68 (95% CI: 0.51–0.81) and for the composite CV end point was 0.70 (95% CI: 0.60–0.81) [11].
To examine the totality of the evidence regarding the estimated effect of cinacalcet plus standard of care compared with standard of care, we conducted a systematic literature review and meta-analysis of published RCTs and observational studies that included relevant clinical outcomes (all-cause mortality, CV-related mortality, hospitalization for CV events, fracture and parathyroidectomy) among patients receiving maintenance dialysis with sHPT.
Methods
Data source
We performed electronic database searches in MEDLINE, EMBASE and the Cochrane Central Register of Controlled Trials (CENTRAL) to identify English language articles published from database inception until 3rd April 2014 (search date in MEDLINE and EMBASE) and until 10th April 2014 (search date in CENTRAL) to identify relevant articles. Abstracts from the 2012 and 2013 American Society of Nephrology and the European Renal Association and European Dialysis and Transplant Association conferences were also included. The search strategy is provided in the Supplementary Material.
Inclusion & exclusion criteria & study selection
Included studies were RCTs or observational studies that reported on relevant clinical outcomes in adult patients receiving maintenance dialysis (including hemodialysis and peritoneal dialysis). Therapies of interest included cinacalcet (with or without other concomitant therapies), vitamin D sterols, phosphate binders or both. Studies were excluded if the comparator was placebo alone.
Two authors independently screened the abstracts and full texts of all potentially eligible articles; disagreements between reviewers were resolved by a third reviewer. Both the Preferred Reporting Items for Systematic Reviews and Meta-analyses and Meta-analysis Of Observational Studies in Epidemiology checklists for the conduct of systematic literature review and meta-analysis were followed [12,13].
Data extraction & quality assessment
Two authors independently extracted data for study descriptors, baseline patient characteristics, dialysis type and vintage, characteristics of treatment, treatment discontinuation and clinical outcomes. A third author resolved any discrepancies. The authors of the original manuscripts were contacted for additional information as needed. Risk of bias in RCTs was assessed using the Cochrane Collaboration's tool [14]; and the quality of observational studies was assessed using the Scottish Intercollegiate Guidelines Network [15]. We performed the bias assessment of each outcome using the Grading of Recommendations Assessment, Development and Evaluation guidelines (details provided in the Supplementary Material) [16].
Outcomes & effect measures
Data synthesis & analysis
To determine the adequacy of a meta-analysis, we assessed the heterogeneity across studies for patient characteristics and outcomes for studies that reported hazard ratios for all-cause and CV-related mortality. The hazard ratio is the preferred effect measure for synthesis for the meta-analysis because the proportional hazard assumption accommodates variable study durations. Hazard ratios had to either be reported by study authors or sufficient data reported to allow their calculation [18]. Kaplan–Meier curves were visually inspected to verify that the proportional hazard assumption was not violated.
We reviewed published models for pooling evidence from both RCT and observational studies [19–21], and employed Sutton et al.'s approach [19] to allow evidence from observational studies to inform the prior belief on the relative treatment effect when pooling estimates from RCTs with Bayesian meta-analysis techniques.
The meta-analysis conducted here used an ‘equivalent prior’ on the relative treatment effect where both observational and RCT evidences were given equal weighting to inform the prior belief with respect to the relative treatment effect. The prior distribution of treatment effect was normally distributed, centered about the mean derived from meta-analyzed observational evidence, with variance informed from the meta-analyzed RCT evidence. The analysis was conducted using both a fixed and random effects framework. The fixed effect model was selected over the random effects model if any of the following conditions were met: it offered better model fit, based on the Deviance Information Criterion [22], and the posterior distribution of the between-studies variance was not updated from the prior distribution.
The meta-analysis was executed using Markov chain Monte Carlo techniques, using the interactive Windows version of Bayesian Inference using Gibbs Sampling Statistical Package [23]. We used unadjusted hazard ratios for our base-case analysis because those estimates were the most conservative with respect to the magnitude of the effect of cinacalcet on all-cause mortality. Two sensitivity analyses were conducted using hazard ratios from adjusted ITT and lag-censoring (i.e., discontinuation-adjusted) analyses, respectively, where available.
Results
Selection of studies
We identified 19 studies that met the eligibility criteria [3–5,10,24–38]; one article [9] reported post hoc-pooled analysis of one Phase II [24] and three Phase III RCTs [3–5], to simplify reporting, we refer to this as a single study (Figure 1). All included studies investigated cinacalcet as add-on to standard therapy (i.e., vitamin D sterols, phosphate binders or both) compared with standard therapy alone.

Figure 1. Flow diagram for study selection.
Note: Searches conducted from database inception until 3 April 2014 for EMBASE and MEDLINE, and 10 April 2014 for CENTRAL.
RCT: Randomized-controlled trial.
Characteristics of studies included
Detailed study characteristics and study durations are described in Table 1 and Figure 2, respectively.

| Study (year) | Study location (year) | Study design/data source | Dialysis | Total follow-up time (years) | n | Ref. |
|---|---|---|---|---|---|---|
| RCTs | ||||||
| Chertow et al. (2012) | International (2006–2008) | Double-blind | HD | 5.3 | 3883 | [10] |
| Cunningham et al. (2005)† | International | Double-blind | HD and PD | 1.1 | 1184 | [9] |
| Messa et al. (2008) | Europe | Open-label | HD and PD | 0.4 | 552 | [25] |
| Malluche et al. (2008) | USA and Europe (2001–2003) | Double-blind | HD | 1.0 | 48 | [26] |
| Raggi et al. (2011) | International | Open-label | HD | 1.0 | 360 | [27] |
| El-Shafey et al. (2011) | Middle East (2009–2010) | Open-label | HD | 0.7 | 82 | [28] |
| Fishbane et al. (2008) | – | Open-label | HD | 0.5 | 173 | [29] |
| Urena-Torres et al. (2013) | International (2009–2011) | Open-label | iHD | 1.1 | 309 | [30] |
| Kim et al. (2013) | Korea (2010–2012) | Open-label | PD | 0.3 | 66 | [31] |
| Ketteler et al. (2012) | USA and Russia | Open-label | HD | 0.5 | 272 | [32] |
| Observational | ||||||
| Block et al. (2010) | USA (2004–2006) | Prospective‡/DaVita database | pHD | 2.2 | 19,186 | [33] |
| Schumock et al. (2011) | USA (2001–2007) | Retrospective/MCCE | HD | 1.4 | 2704 | [34] |
| Abouchacra et al. (2014) | UAE (2012–2013) | Retrospective/hospital | HD | 2.0 | 71 | [35] |
| Friedl et al. (2013) | Austria (2004–2009) | Retrospective§/ADTR | pHD and pPD | 7.0 | 8225 | [36] |
| Gillespie et al. (2015) | Europe (2007–2009) | Prospective¶/ARO | iHD | 5.8 | 2322 | [37] |
| Akizawa et al. (2012) | Japan | Prospective#/MBD-5D | HD | 3.0 | 8229 | [38] |
†Pooled analysis of four RCTs: published by Quarles et al. (2003) [24], Lindberg et al. (2003) [4], Block et al. (2004) [3] and Lindberg et al. (2005) [5]. Those four studies did not make study selection as none of them reported the outcomes of interest.
‡Data from DaVita database.
§Data from the Austrian Dialysis and Transplant Registry.
¶Data from the Analyzing data, Recognizing excellence and Optimizing outcomes-CKD Research Initiative.
#Study is a planned analysis of the Mineral and Bone Disorders Outcomes Study for Japanese CKD stage-5D.
ADTR: Austrian dialysis and transplant registry; ARO: Analyzing data, Recognizing excellence, and Optimizing outcomes; CKD: Chronic kidney disease; HD: Hemodialysis; iHD: Incident HD; MBD-5D: Mineral and Bone Disorders Outcomes Study for Japanese CKD stage-5D; MCCE: MarketScan commercial claims and encounter; PD: Peritoneal dialysis; pHD: Prevalent HD; pPD: Prevalent PD; RCT: Randomized-controlled trial.
Mean age at study entry ranged from 48 to 67 years and mean dialysis vintage ranged from 7 to 79 months. The severity of sHPT as indicated by serum PTH (median: 231–695 pg/ml) and calcium concentrations (median: 8.9–9.8 mg/dl) varied across studies, as did the proportion and type of CV comorbidities. Baseline characteristics for the subset of studies included in the meta-analysis are provided in Table 2.
| Variable | Chertow | Cunningham | Block | Gillespie | ||||
|---|---|---|---|---|---|---|---|---|
| Cinacalcet | Placebo | Cinacalcet | Placebo | Cinacalcet | Noncinacalcet | Cinacalcet | Noncinacalcet | |
| n | 1948 | 1935 | 697 | 487 | 5976 | 13,210 | 532 | 1790 |
| Age (year): | ||||||||
| – Median | 55.0 | 54.0 | – | – | – | – | 67 | 67 |
| – IQR (min, max) | 35.0–74.0 | 35.0–73.0 | – | – | – | – | – | – |
| – Mean | 54.4 | 54.4 | 53.0 | 54.7 | 59.2 | 65.0 | – | – |
| – SD | 14.4 | 14.4 | 14.2 | 14.6 | – | – | – | – |
| – Proportion of male (%) | 58.5 | 60.3 | 61 | 63 | 51.8 | 54.6 | 59.0 | 58.9 |
| Dialysis vintage (months): | ||||||||
| – Median | 45.4 | 45.1 | – | – | – | – | – | – |
| – IQR (min, max) | 8.5–142.0 | 9.9–149.0 | – | – | – | – | – | – |
| – Mean | – | – | 65.8 | 70.1 | 52.8 | 42.0 | 16.3 | 14.6 |
| – SD | – | – | 59.9 | 67.1 | – | – | 11.7 | 11.3 |
| CV comorbidities: | ||||||||
| – Hypertension | 92.5 | 91.7 | – | – | – | – | – | – |
| – Heart failure/CHF | 23.1 | 23.6 | – | – | 40.6 | 48.9 | – | – |
| – PVD | 16.1 | 16.6 | – | – | 29.8 | 38.4 | – | – |
| – MI | 12.3 | 12.6 | – | – | – | – | – | – |
| – CVA/stroke/TIA | 8.3 | 10.0 | – | – | 13.3 | 18.8 | – | – |
| – History of CVD | 95.4 | 94.6 | – | – | – | – | 35.7 | 34.5 |
| PTH (pg/ml): | ||||||||
| – Median | 695 | 690 | – | – | 323 | 231 | 481 | 404 |
| – IQR (min, max) | 362–1707 | 363–1683 | 317-NR | 187-NR | – | – | ||
| – Mean | – | – | 731 | 682 | – | – | – | – |
| – SD | – | – | 531 | 399 | – | – | – | – |
| Ca (mg/dl): | ||||||||
| – Median | 9.8 | 9.8 | – | – | – | – | 9.0 | 8.9 |
| – IQR (min, max) | 9.0–10.7 | 9.0–10.7 | – | – | – | – | – | – |
| – Mean | 9.8 | 9.8 | 9.9 | 9.9 | 9.8 | 9.5 | – | – |
| – SD | 0.7 | 0.7 | 0.8 | 0.8 | 0.7 | 0.7 | – | – |
Ca: Calcium; CHF: Congestive heart failure; CV: Cardiovascular; CVA: Cerebrovascular attack; CVD: Cardiovascular disease; IQR: Interquartile range; MI: Myocardial infarction; NR: Not reported; PTH: Parathyroid hormone; PVD: Peripheral vascular disease; TIA: Transient ischemic attack; SD: Standard deviation.
Outcomes of studies included in systematic literature review
The count or proportion of deaths from any cause, or the hazard ratio between study arms, was reported in 13 studies (Table 3). The underlying absolute event rate varied substantially across studies, which was associated with duration of follow-up (i.e., fewer deaths reported in shorter duration studies); however, in comparing the risk of death between study arms, the direction of association was consistently toward a protective effect of cinacalcet (one study reported a null effect with a point estimate of 1.00). In three studies – one RCT and two observational studies – investigators reported a significant effect size; however, in several cases this effect size was from a sensitivity analysis rather than a primary outcome.
| Study (year) | Reference arm | Percentage† | Relative risk‡ | Hazard ratio | |||
|---|---|---|---|---|---|---|---|
| Cinacalcet | Reference | (95% CI) | Type | Value | (95% CI) | ||
| All-cause mortality – RCTs | |||||||
| Chertow et al. (2012) | Placebo | 36.1 | 37.1 | 0.97 (0.90–1.06) | Unadjusted | 0.94 | (0.85–1.04) |
| Adjusted | 0.86 | (0.78–0.96) | |||||
| Lag censored | 0.83 | (0.73–0.96) | |||||
| Cunningham et al. (2005) | Placebo | N/R | N/R | – | Unadjusted | 0.81 | (0.45–1.45) |
| Messa et al. (2008) | Placebo | 3 | 3 | 0.92 (0.34–2.44) | N/R | ||
| Malluche et al. (2008) | Placebo | 9 | 13 | 0.75 (0.14–4.05) | N/R | ||
| Raggi et al. (2011) | Placebo | 6.7 | 6.7 | 1.00 (0.46–2.17) | N/R | ||
| El-Shafey et al. (2011) | Noncinacalcet§ | 2 | 3.7 | 0.49 (0.03–7.55) | N/R | ||
| Fishbane et al. (2008) | Vitamin D sterol | 2 | 2 | 0.99 (0.14–6.86) | N/R | ||
| Kim et al. (2013) | Noncinacalcet | 0 | 0 | – | N/R | ||
| Ketteler et al. (2012) | Paricalcitol | 0¶ | 1.6 | – | N/R | ||
| Cinacalcet oral | 0 | ||||||
| Paricalcitol oral | 4.2 | ||||||
| All-cause mortality – observational | |||||||
| Block et al. (2010) | Noncinacalcet | 19.2 | 30.7 | 0.43 (0.41–0.45) | Unadjusted | 0.73 | (0.68–0.78) |
| Adjusted | 0.74 | (0.67–0.83) | |||||
| Abouchacra et al. (2014) | Noncinacalcet | 9.5 | 10 | 0.95 (0.29–3.17) | N/R | ||
| Gillespie et al. (2015) | Noncinacalcet | 15.8 | 16.6 | 0.95 (0.76–1.19) | Unadjusted | 1.03 | (0.78–1.35) |
| Lag censored | 0.84 | (0.60–1.18) | |||||
| Akiwaza et al. (2012) | Noncinacalcet | N/R | N/R | – | Adjusted | 0.65 | (0.52–0.81) |
| CV-related mortality – RCTs | |||||||
| Chertow et al. (2012) | Placebo | 19.4 | 20.2 | 0.96 (0.84–1.09) | Unadjusted | 0.92 | (0.80–1.07) |
| Messa et al. (2008) | Placebo | 0.8 | 1.1 | 0.75 (0.13–4.45) | N/R | ||
| Ketteler et al. (2012) | Paricalcitol | 0¶ | 1.6 | – | N/R | ||
| Cinacalcet oral | 0 | ||||||
| Paricalcitol oral | 1.4 | ||||||
| CV-related mortality – observational | |||||||
| Block et al. (2010) | Noncinacalcet | 8.8 | 13.4 | 0.66 (0.60–0.72) | Unadjusted | 0.78 | (0.71–0.86) |
| Adjusted | 0.76 | (0.66–0.86) | |||||
| Abouchacra et al. (2014) | Noncinacalcet# | 4.8 | 5 | 0.95 (0.17–5.45) | N/R | ||
| Friedl et al. (2013) | Noncinacalcet | N/R | N/R | – | Unadjusted | 0.76†† | – |
| Akizawa et al. (2012) | Noncinacalcet | N/R | N/R | – | Adjusted | 0.68 | (0.48–0.98) |
Note: Unadjusted rates were reported by Cunningham et al. to be 5.2 per 100 patient year in the cinacalcet arm versus 7.4 per 100 patient year in the placebo arm. Block et al. reported rates of 17.6 (95% CI: 16.6–18.6) per 100 patient year in the cinacalcet arm versus 23.0 (22.4–23.6) per 100 patient year in the placebo arm. Chertow et al. adjusted for age, sex, race, BMI, vintage, blood pressure, medical history, vitamin D, phosphate binders, CV medication and laboratory information (including calcium, phosphorus, and PTH among many others). Block et al. adjusted for age, sex, race, dialysis duration, BMI, primary cause of renal failure, co-morbidities, hospital days, vascular access and laboratory information (including calcium, phosphorus and PTH among many others). Akizawa et al. adjusted for calcium, phosphorus, PTH, VDRA, phosphate binder, albumin, BMI, age, sex, vintage, primary renal disease, CV morbidity and number of non-CV co-morbidities).
†Either reported or estimated from count of events.
‡Crude relative risks were calculated from data reported.
§Conventional therapy.
¶Cinacalcet intravenous.
#On vitamin D or analogs.
††Calculated relative risk at end of study using Kaplan–Meier curves was estimated to be approximately 0.76 from a figure.
CV: Cardiovascular; n: Number of patients who had the event; N: Number of patients in analysis; N/R: Not reported; PTH: Parathyroid hormone; RCT: Randomized controlled trial; VDRA: Vitamin D receptor activator.
Similar results were observed in the seven studies reporting on CV-related mortality (Table 3): the directions of effect estimates consistently indicated a protective effect of cinacalcet, although the findings were statistically significant in only two of the six studies reporting this outcome.
Two studies reported evidence for the composite outcome of all-cause mortality or CV event. In both studies, the effect estimate indicated a significant beneficial effect of cinacalcet relative to standard of care: the hazard ratio was 0.67 (95% CI: 0.52–0.85) in one (observational) study, [38] and 0.88 (95% CI: 0.79–0.97) in the adjusted analysis of the EVOLVE RCT (of note: in the unadjusted analysis of the EVOLVE study, the hazard ratio was not significantly different from 1.0) [10].
The relative risk of CV events was reported in three studies, and one other study looked at the risk of hospitalization for CV events. In the pooled analysis of RCTs by Cunningham et al., the risk of hospitalization for CV events was significantly lower in the cinacalcet arm compared with the standard of care arm (unadjusted hazard ratio: 0.61; 95% CI: 0.43–0.86) [9]. Similarly, there were significantly fewer CV events in the cinacalcet arm than in the control cohort in the retrospective observational study by Abouchacra et al. (33.3 vs 67.5%, p = 0.001) [35]. In the EVOLVE RCT, cinacalcet resulted in a nominally significant beneficial effect over standard of care for heart failure [10]. For myocardial infarction, unstable angina and peripheral vascular events (other nonfatal components of the primary composite end point), results suggested a protective effect of cinacalcet (hazard ratios ranging from 0.82 to 0.97); however, none reached statistical significance [10]. The RCT by Keteller et al. reported higher rates of serious CV events in the noncinacalcet arms (3.1% in the cinacalcet/IV vitamin D and 1.4% in the cinacalcet/oral vitamin D stratums vs 9.7% in the paricalcitol/IV vitamin D and 8.3% in the paricalcitol/oral vitamin D stratums) [32].
In the three studies reporting on fracture, the risk was generally lower in RCT arms involving cinacalcet. In the pooled trials reported by Cunningham et al., this finding was statistically significant with a hazard ratio of 0.46 (95% CI: 0.22–0.95) [9]. In EVOLVE, an analysis adjusted for baseline characteristics showed a significant reduction among cinacalcet users; the hazard ratio was 0.83 (95% CI: 0.72–0.98) [39]. El-Shafey et al. reported a lower rate of lower extremity fractures in patients randomized to cinacalcet compared with standard of care (3.8 vs 19.2%, respectively) [28].
The direction of association for the outcome of parathyroidectomy tended toward a lower risk in the cinacalcet arm in five of the six studies reporting this outcome; the finding was statistically significant in the two studies that reported a p-value. In contrast, in the analysis of administrative claims data, Schumock et al. reported an increased risk of parathyroidectomy associated with cinacalcet compared with paricalcitol (adjusted hazard ratio = 0.21 for paricalcitol vs cinacalcet; p < 0.001), perhaps related to the severity of sHPT [34].
The results of the quality assessment of RCTs, observational studies and meta-analyses are provided (Tables 4–6, respectively).
| Study (year) | Selection bias | Performance bias | Detection bias | Attrition bias | Analysis by ITT | Reporting bias | Other potential threats to validity | ||
|---|---|---|---|---|---|---|---|---|---|
| Random sequence generation | Allocation concealment | Blinding of participants and personnel | Blinding of outcome assessment | Incomplete outcome data addressed | Selective outcome reporting | Imbalance in baseline characteristics | Intervention (misclassification of exposure, other) | ||
| Chertow et al. (2012) | Low | Low | Low | Low | Low | Low | Low | High | High |
| Cunningham et al. (2005) | – | – | – | – | – | – | – | – | – |
| Block et al. (2004)† | Low | Low | Low | Low | Unclear | Low | Low | Low | Low |
| Lindberg et al. (2003)† | Low | Low | Low | Low | Low | High | High | Low | Low |
| Lindberg et al. (2005)† | Low | Low | Low | Low | Low | High | High | Low | Low |
| Quarles et al. (2003)† | Low | Low | Low | Low | Low | High | High | Low | Unclear |
| Messa et al. (2008) | Unclear | Unclear | High | Low | Low | Unclear | Low | Low | High |
| Malluche et al. (2008) | Low | Low | Low | Low | High | High | Low | Low | Low |
| Raggi et al. (2011) | Unclear | Unclear | High | Low | Low | High | High | Unclear | Low |
| El-Shafey et al. (2011) | Unclear | Unclear | High | Low | High | High | Low | Low | Unclear |
| Fishbane et al. (2008) | Unclear | Unclear | High | Low | Low | Low | Low | Low | Unclear |
| Urena-Torres et al. (2013) | Low | Low | High | Low | Low | Low | Low | Low | Unclear |
| Kim et al. (2013) | Unclear | Unclear | High | Low | High | High | Unclear | Low | High |
| Ketteler et al. (2012) | Unclear | Unclear | High | Low | High | Low | Low | High | Low |
| Total low risk | 6 | 6 | 5 | 12 | 7 | 5 | 8 | 9 | 5 |
| Total unclear risk | 6 | 6 | 0 | 0 | 1 | 1 | 1 | 1 | 4 |
| Total high risk | 0 | 0 | 7 | 0 | 4 | 6 | 3 | 2 | 3 |
An unclear risk was occasionally given due to a lack of reporting rather than due to a poorly conducted trial.
†RCTs by Block et al., Lindberg et al. (2003), Lindberg et al. (2005) and Quarles et al. were included in the pooled analysis reported by Cunningham et al. Although the authors of the individual RCT studies did not report sequence generation and allocation concealment, Cunningham et al. stated that a computer-generated randomization system was used.
ITT: Intent-to-treat; RCT: Randomized-controlled trial.
| Study (year) | Internal validity | Overall assessment of study | |||
|---|---|---|---|---|---|
| Selection of subjects | Assessment of outcomes | Confounding | Statistical analysis | ||
| Block et al. (2004) | Low | Low | Low | Low | High quality |
| Schumock et al. (2011) | High | Low | High | Low | Acceptable |
| Abouchacra et al. (2014) | High | Unclear | High | Low | Acceptable |
| Friedl et al. (2013) | Low | Unclear | Low | Low | High quality |
| Gillespie et al. (2015) | High | Low | Low | Low | High quality |
| Akizawa et al. (2012) | Unclear | Unclear | Unclear | Unclear | Unknown |
An unclear risk was occasionally given due to a lack of reporting rather than due to a poorly conducted trial.
| Number of studies/study type | Quality assessment | Summary of findings | ||||||
|---|---|---|---|---|---|---|---|---|
| Limitations | Indirectness | Inconsistency | Imprecision | No. of patients | Relative effect | Quality of body of evidence (GRADE) | ||
| Cinacalcet | Noncinacalcet | Unadjusted HR (95% CI) | ||||||
| All-cause mortality – unadjusted hazard ratios | ||||||||
| Two RCTs | Some | None | None | Some | 2645 | 2422 | 0.87 (0.71, 1.06) | Moderate |
| Two OBS | None | None | Some | Some | 5976 | 13,120 | – | – |
| Quality | +1 | 0 | -1 | -1 | NA | NA | NA | – |
| CV-related mortality – unadjusted hazard ratios | ||||||||
| One RCT | Some | None | None | Some | 1948 | 1935 | 0.84 (0.71, 0.99) | Moderate |
| One OBS | None | None | None | Some | 5976 | 13,120 | – | – |
| Quality | -1 | 0 | 0 | -1 | NA | NA | NA | – |
CV: Cardiovascular; GRADE: Grading of Recommendations Assessment, Development and Evaluation; HR: Hazard ratio; NA: Not applicable; OBS: Observational study; RCT: Randomized-controlled trial.
Bayesian meta-analysis of all-cause mortality
Four studies (two based on RCTs [9,10] and two observational [33,37]) reported hazard ratios as the measure of effect and thus were suitable for inclusion in the meta-analysis. Tests of heterogeneity indicated that studies could validly be combined in meta-analysis. In the remaining studies, outcomes were reported as counts, proportions or rates, and did not provide the requisite data for the calculation of hazard ratios.
Unadjusted and adjusted estimates from the contributing RCTs and observational studies are presented in Figure 3 as well as an estimate based on a lag-censoring analysis reported by Chertow et al. [10]. All estimates were either statistically significant in favor of a reduced hazard associated with cinacalcet, or not significantly different versus standard of care.
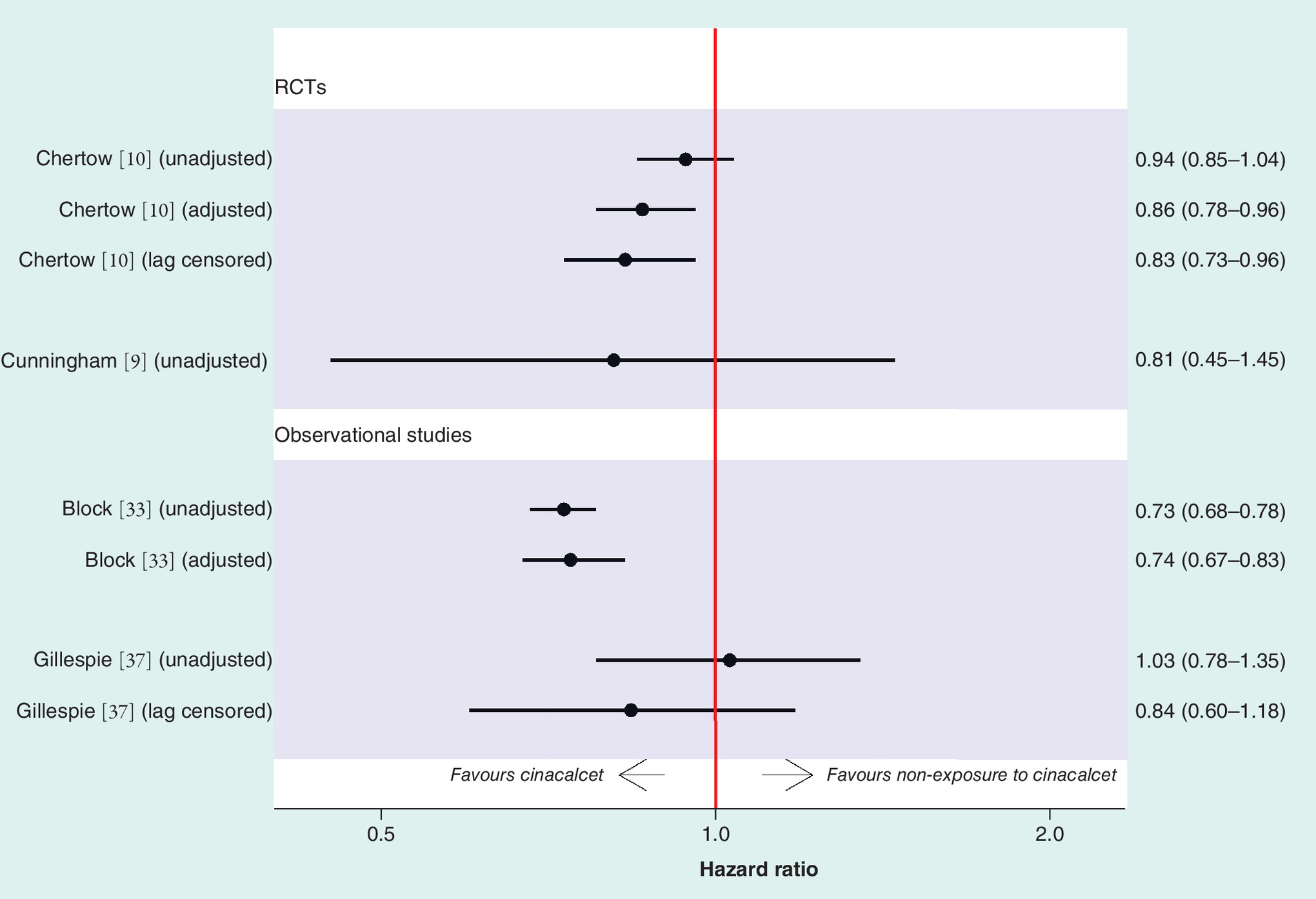
Figure 3. Evidence base for all-cause mortality.
RCT: Randomized-controlled trial.
The estimated hazard ratio from the base-case meta-analysis was 0.83 (0.78, 0.89), indicative of a statistically significant reduction in the risk of death associated with cinacalcet compared with standard therapy. The contributing evidence is fully described in Figure 4, including the pooled estimates generated from RCTs alone and from the observational studies alone, as well as the evidence that was borrowed from each to inform the prior belief of treatment effect. The estimate from the base-case model was consistent with those obtained through sensitivity analyses (Table 7) including: the random effects models (a fixed effect model was selected in the base case, as there were not sufficient data to estimate the between-study variance under the random effects model); scenarios where adjusted and hazard ratios based on lag-censoring analyses were used when available (Table 7, analyses 4 and 7).

Figure 4. Bayesian meta-analysis of all-cause mortality evidence and evidence synthesis.
Note: Prior belief of relative treatment effect was informed from point estimate obtained from the meta-analysis of observational studies, and variance obtained from the meta-analysis of randomized-controlled trials (black markers).
RCT: Randomized-controlled trial.
| Analysis | Evidence | Random effects model | Fixed effect model | |||||
|---|---|---|---|---|---|---|---|---|
| HR | (95% CI) | Between-study SD prior: uniform (0, 5) | DIC | HR | (95% CI) | DIC | ||
| Base – case analysis; using unadjusted HRs | ||||||||
| 1 | RCTs, informed prior of treatment effect | 0.89 | (0.23–3.36) | 0.96 (0.02, 4.08) | -1.225 | 0.83 | (0.78–0.89) | 1.728 |
| 2 | RCTs only | 0.89 | (0.05–16.43) | 1.28 (0.02, 4.56) | 0.94 | (0.85–1.03) | ||
| 3 | Observational studies only | 0.86 | (0.04–20.45) | 1.47 (0.09, 4.62) | 0.74 | (0.70–0.80) | ||
| SA; using adjusted HRs where available | ||||||||
| 4 | RCTs, informed prior of treatment effect | 0.81 | (0.21–3.02) | 0.93 (0.02, 4.04) | -0.709 | 0.78 | (0.71–0.86) | -2.256 |
| 5 | RCTs only | 0.82 | (0.04–15.36) | 1.26 (0.02, 4.55) | 0.83 | (0.73–0.95) | ||
| 6 | Observational studies only | 0.77 | (0.05–13.18) | 1.18 (0.02, 4.51) | 0.73 | (0.69–0.78) | ||
| SA; using lag-censoring HRs where available | ||||||||
| 7 | RCTs, informed prior of treatment effect | 0.85 | (0.22–3.20) | 0.93 (0.02, 4.06) | -1.234 | 0.81 | (0.76–0.88) | -2.591 |
| 8 | RCTs only | 0.84 | (0.05–15.69) | 1.26 (0.02, 4.55) | 0.86 | (0.77–0.95) | ||
| 9 | Observational studies only | 0.86 | (0.04–19.79) | 1.44 (0.07, 4.61) | 0.77 | (0.70–0.85) | ||
DIC: Deviance information criterion; HR: Hazard ratio; RCT: Randomized clinical trial; SA: Sensitivity analysis; SD: Standard deviation.
Bayesian meta-analysis of CV-related mortality
There was only one RCT and one observational study available for inclusion in the CV-related mortality meta-analysis. The meta-analysis was run using these two studies: the estimate from the single RCT by Chertow et al. [10] was updated through a prior distribution of the treatment effect informed by evidence from the observational study by Block et al. [33]. The resulting hazard ratio from the fixed effect model was 0.91 with CI (0.79–1.05), indicating a nonsignificant protective effect of cinacalcet on CV-related mortality.
Bayesian meta-analysis of other outcomes
There was insufficient evidence to conduct meta-analyses on the composite outcome of all-cause mortality and CV events, or on the outcomes of hospitalization for CV events, fracture or parathyroidectomy.
Discussion
This is the first systematic literature review and quantitative synthesis that includes evidence from both RCTs and observational studies on the effects of cinacalcet on all-cause and CV-related mortality, hospitalization for CV events, fracture and parathyroidectomy, among patients with sHPT-receiving maintenance dialysis. The findings of our study provide additional evidence that cinacalcet may be associated with a lower risk of mortality among patients receiving maintenance dialysis.
By design, each of the RCTs of cinacalcet was insufficient to detect differences in clinical outcomes; however, by pooling results from several study types, the power to estimate the hazard ratio within the initial time window was increased. To reduce the risk of bias, investigators of the observational studies employed strategies for adjusting for known confounders and the observational studies that were included into the meta-analysis were assessed as having low risk of confounding bias, and overall high quality [33,37]. Thus, coupling these high-quality observational studies with the pooled power from the individual RCTs provided the strongest possible evidence base upon which to assess the effects of cinacalcet on clinical outcomes.
The benefits and risks of cinacalcet therapy in adults with end-stage renal disease (ESRD) have been previously meta-analyzed [40,41]. However, only randomized studies have been included. For all-cause mortality, Palmer et al. [40] reported a relative risk of 0.97 (0.89, 1.05); Zhang et al. [41] reported an odds ratio of 0.86 (0.46, 1.60), each of which is consistent with the findings of our study. Many of the studies included in the meta-analyses by Palmer et al. and Zang et al. could not be included in our meta-analysis, because they did not report hazard ratios, which were our selected outcomes.
This study has several strengths. First, we adopted a state-of-the-art and rigorous approach to assess the quality of the evidence and the feasibility of combining observational and RCT evidence in a meta-analysis. The systematic literature review identified all published evidence for the outcomes of interest in a well-defined adult patient population (i.e., patients with ESRD receiving maintenance dialysis). Second, the meta-analysis was conducted using appropriate statistical techniques that allowed for the incorporation of all available evidence to inform an estimate of the effect of cinacalcet, compared with standard of care, in reducing all-cause and CV-related mortality for individuals with ESRD who are on maintenance dialysis. We selected unadjusted hazard ratios for the base-case analysis to adopt a conservative approach to the estimate of effect as adjusted estimates from included studies tended to show a stronger treatment effect. We reported the impact of this choice in sensitivity analyses. Additionally, to reduce variability arising from different study durations, we included the hazard ratio as the preferred measure of effect. While there are methodologies that allow for combining count and hazard ratio statistics [42], we chose not to combine the two types of evidence here. Hazard ratios are ideally suited to describe the prolongation in time-to-event [18], which is the relevant effect for cinacalcet; while a binary measure would imply assessing the effect of cinacalcet with regard to prevention of death. However, few studies reported the outcomes as hazard ratios, which in turn, limited our ability to: conduct a more robust statistical analysis directly incorporating evidence from observational studies in the meta-analysis [19] rather than via a prior distribution; estimate the between-study variance, under a random effects model; and explore sources of heterogeneity through covariate adjustment [21].
The main limitation lies in the evidence base itself. Randomized trials of this question have provided lessons about future trials of patients on dialysis on end points, analytic strategies including the need to account for effect modification, power and sample size after accounting for crossover, nonadherence and cointerventions, and interpretation of the findings [43].
We synthesized all available evidence on the effect of cinacalcet on all-cause and CV-related mortality; however, due to the limited reporting of outcomes on the hazard ratio scale, we were only able to incorporate 4 out of the 16 studies into a quantitative estimate of the estimated effect of cinacalcet and overall mortality, and only two studies into an estimate for CV-related mortality. While the identified evidence suggests that cinacalcet does provide a protective effect, more studies (or more data from the existing studies) are needed to reach a statistically significant result from a quantitative synthesis, under a random effect model, which we considered, a priori, a more appropriate model.
Conclusion
The results of this meta-analysis indicate that treatment of sHPT with calcimimetic therapy may in fact reduce mortality among patients receiving maintenance dialysis. This finding provides justification for a well-designed and adequately powered randomized trial to definitively address the question.
Traditional meta-analyses of clinical evidence include only randomized controlled trials (RCTs) for the summary measures.
Key limitations of RCTs include a threat to external validity and, often, lack of power to demonstrate effects on hard outcomes such as hospitalizations and mortality; well-designed observational studies can help address these limitations.
Including evidence from well-designed observational studies can help overcome the limitations of traditional meta-analyses to provide more robust estimates of effect in real-world populations.
This study aimed to quantitatively summarize studies of the real-world effects of a calcimimetic therapy on clinical outcomes among patients on dialysis including RCTs and observational studies using the Bayesian approach.
The combined estimate of effect suggests potential survival improvement associated with calcimimetic therapy.
When limited data are available from RCTs, a thoughtful evidence synthesis from trials and well-designed observational studies can aid in medical decision-making.
Author's contributions
All the authors contributed to manuscript writing, critical revision and final review of the manuscript. ME Bensink, GA Block, GM Chertow, ML Trotman, K Cooper and V Belozeroff contributed to the conception and design of the study. G Lozano-Ortega, S Goring, H Bennett and AR Levy contributed to the conception and design of the study, development of the search strategy and data extraction forms, and study selection process. N Waser contributed to the development of the search strategy and data extraction forms, and study selection process.
Financial & competing interests disclosure
This research was funded by Amgen, Inc. GA Block and GM Chertow have received research support from Amgen, Inc. for advisory and consulting services. The authors ME Bensink, ML Trotman, K Cooper and V Belozeroff are employees and stockholders of Amgen, Inc. Other authors (G Lozano-Ortega, S Goring, H Bennett, N Waser and AR Levy) declare no financial conflict. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Supplementary Material
File (supplementary_materials.docx)
- Download
- 28.10 KB
References
Papers of special note have been highlighted as: •• of considerable interest
1.
Emergensy Medicines Agency. Mimpara EPAR Product Information (2009). www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000570/WC500028900.pdf.
2.
US FDA. FDA approved label: Sensipar (cinacalcet) (2011). https://www.accessdata.fda.gov/drugsatfda_docs/label/2011/021688s017lbl.pdf.
3.
Block GA, Martin KJ, De Francisco AL et al. Cinacalcet for secondary hyperparathyroidism in patients receiving hemodialysis. N. Engl. J. Med. 350(15), 1516–1525 (2004).
4.
Lindberg JS, Moe SM, Goodman WG et al. The calcimimetic AMG 073 reduces parathyroid hormone and calcium x phosphorus in secondary hyperparathyroidism. Kidney Int. 63(1), 248–254 (2003).
5.
Lindberg JS, Culleton B, Wong G et al. Cinacalcet HCl, an oral calcimimetic agent for the treatment of secondary hyperparathyroidism in hemodialysis and peritoneal dialysis: a randomized, double-blind, multicenter study. J. Am. Soc. Nephrol. 16(3), 800–807 (2005).
6.
Nakayama K, Nakao K, Takatori Y et al. Long-term effect of cinacalcet hydrochloride on abdominal aortic calcification in patients on hemodialysis with secondary hyperparathyroidism. Int. J. Nephrol. Renovasc. Dis. 7, 25–33 (2013).
7.
Vervloet M, Bencova V, Malberti F et al. ‘Real-world’ use of cinacalcet for managing SHPT in different European countries: analysis of data from the ECHO observational study. Clin. Nephrol. 74(3), 198–208 (2010).
8.
St Peter WL, Yusuf AA, Do T et al. Parathyroid hormone change after cinacalcet initiation and one-year clinical outcome risk: a retrospective cohort study. BMC Nephrol. 16, 41 (2015).
9.
Cunningham J, Danese M, Olson K et al. Effects of the calcimimetic cinacalcet HCl on cardiovascular disease, fracture, and health-related quality of life in secondary hyperparathyroidism. Kidney Int. 68(4), 1793–1800 (2005).
10.
Chertow GM, Block GA, Correa-Rotter R et al. Effect of cinacalcet on cardiovascular disease in patients undergoing dialysis. N. Engl. J. Med. 367(26), 2482–2494 (2012).
•• This was a large randomized controlled trial in dialysis patients – while the primary end point was not achieved at the expected level of statistical significance, the prespecified analyses adjusting for baseline covariates and therapy discontinuation showed trends for better long-term outcomes in patients treated with a calcimimetic.
11.
Parfrey PS, Drueke TB, Block GA et al. The effects of cinacalcet in older and younger patients on hemodialysis: the evaluation of cinacalcet HCl therapy to lower cardiovascular events (EVOLVE) trial. Clin. J. Am. Soc. Nephrol. 10(5), 791–799 (2015).
12.
Liberati A, Altman DG, Tetzlaff J et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ann. Intern. Med. 151(4), W65–W94 (2009).
13.
Stroup DF, Berlin JA, Morton SC et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 283(15), 2008–2012 (2000).
14.
Higgins JP, Altman DG, Gotzsche PC et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 343, d5928 (2011).
15.
Scottish Intercollegiate Guidelines Network, Healthcare Improvement. Methodology checklist 3: cohort studies (2014). www.bioenv.gu.se/digitalAssets/1440/1440747_checklist3.pdf.
16.
Guyatt GH, Oxman AD, Vist GE et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 336(7650), 924–926 (2008).
17.
Tripepi G, Heinze G, Jager KJ et al. Lag-censoring analysis: lights and shades. Nephrol. Dial. Transplant. 30(5), 700–705 (2015).
18.
Parmar MK, Torri V, Stewart L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat. Med. 17(24), 2815–2834 (1998).
19.
Sutton AJ, Abrams KR. Bayesian methods in meta-analysis and evidence synthesis. Stat. Meth. Med. Res. 10(4), 277–303 (2001).
20.
Dias S, Sutton AJ, Welton NJ et al. Evidence synthesis for decision making 3: heterogeneity – subgroups, meta-regression, bias, and bias-adjustment. Med. Decis. Making 33(5), 618–640 (2013).
21.
McCarron CE, Pullenayegum EM, Thabane L et al. Bayesian hierarchical models combining different study types and adjusting for covariate imbalances: a simulation study to assess model performance. PLoS ONE 6(10), e25635 (2011).
22.
Dias S, Welton N, Sutton A, Ades AE. National Institut for Health and Clinical Excellence (NICE) Decsion Support Unit (DSU) technical support document 2: a generalised linea modelling framework for pairwise and network meta-analysis of randomised controlled trials (2016). www.ncbi.nlm.nih.gov/pubmedhealth/PMH0088912/pdf/PubMedHealth_PMH0088912.pdf.
23.
Lunn DJ, Thomas A, Best N et al. WinBUGS – a Bayesian modelling framework: concepts, structure, and extensibility. Stat. Comput. 10(4), 325–337 (2000).
24.
Quarles LD, Sherrard DJ, Adler S et al. The calcimimetic AMG 073 as a potential treatment for secondary hyperparathyroidism of end-stage renal disease. J. Am. Soc. Nephrol. 14(3), 575–583 (2003).
25.
Messa P, Macario F, Yaqoob M et al. The OPTIMA study: assessing a new cinacalcet (Sensipar®/Mimpara®) treatment algorithm for secondary hyperparathyroidism. Clin. J. Am. Soc. Nephrol. 3(1), 36–45 (2008).
26.
Malluche HH, Monier-Faugere MC, Wang G et al. An assessment of cinacalcet HCl effects on bone histology in dialysis patients with secondary hyperparathyroidism. Clin. Nephrol. 69(4), 269–278 (2008).
27.
Raggi P, Chertow GM, Torres PU et al. The ADVANCE study: a randomized study to evaluate the effects of cinacalcet plus low-dose vitamin D on vascular calcification in patients on hemodialysis. Nephrol. Dial. Transplant. 26(4), 1327–1339 (2011).
28.
El-Shafey EM, Alsahow AE, Alsaran K et al. Cinacalcet hydrochloride therapy for secondary hyperparathyroidism in hemodialysis patients. Ther. Apher. Dial. 15(6), 547–555 (2011).
29.
Fishbane S, Shapiro WB, Corry DB et al. Cinacalcet HCl and concurrent low-dose vitamin D improves treatment of secondary hyperparathyroidism in dialysis patients compared with vitamin D alone: the ACHIEVE study results. Clin. J. Am. Soc. Nephrol. 3(6), 1718–1725 (2008).
30.
Urena-Torres P, Bridges I, Christiano C et al. Efficacy of cinacalcet with low-dose vitamin D in incident haemodialysis subjects with secondary hyperparathyroidism. Nephrol. Dial. Transplant. 28(5), 1241–1254 (2013).
31.
Kim HJ, Kim H, Shin N et al. Cinacalcet lowering of serum fibroblast growth factor-23 concentration may be independent from serum Ca, P, PTH and dose of active vitamin D in peritoneal dialysis patients: a randomized controlled study. BMC Nephrol. 14, 112 (2013).
32.
Ketteler M, Martin KJ, Wolf M et al. Paricalcitol versus cinacalcet plus low-dose vitamin D therapy for the treatment of secondary hyperparathyroidism in patients receiving haemodialysis: results of the IMPACT SHPT study. Nephrol. Dial. Transplant. 27(8), 3270–3278 (2012).
33.
Block GA, Zaun D, Smits G et al. Cinacalcet hydrochloride treatment significantly improves all-cause and cardiovascular survival in a large cohort of hemodialysis patients. Kidney Int. 78(6), 578–589 (2010).
•• This was the largest retrospective cohort study to assess comparative effectiveness of a calcimimetic in a nonrandomized setting. The analysis addressed confounding by stratification and adjustment and reported potential improvement in long-term outcomes in a real-world patients treated with calcimimetic therapy.
34.
Schumock GT, Walton SM, Lee TA et al. Comparative effectiveness of paricalcitol versus cinacalcet for secondary hyperparathyroidism in patients receiving hemodialysis. Nephron. Clin. Prac. 117(2), c151–c159 (2011).
35.
Abouchacra S, Chaaban A, Budruddin M et al. Before the jury is out on cinacalcet's cardiovascular effects in hemodialysis patients: is troponin a missing link? Open J. Nephrol. 4, 47–53 (2014).
36.
Friedl C, Reibnegger G, Kramar R et al. Cinacalcet improves survival in dialysis patients – a European cohort study. J. Am. Soc. Nephrol. 24 (Abstract SA-PO546), 752A (2013).
37.
Gillespie IA, Floege J, Gioni I et al. Propensity score matching and persistence correction to reduce bias in comparative effectiveness: the effect of cinacalcet use on all-cause mortality. Pharmacoepidemiol. Drug Saf. 24(7), 738–747 (2015).
38.
Akizawa T, Kurita N, Mizobuchi M. Consistent use of cinacalcet improves clinical outcomes in Japanese heamodialysis patients with secondary hyperparathyroidism: marginal structural analyses from the mineral and bone disorder outcomes study for Japanese CKD stage 5D patients (MBD-5D). European Renal Association and European Dialysis and Transplant Association (ERA-EDTA) Conference. Paris, France, 24–27 May (2012).
39.
Moe SM, Abdalla S, Chertow GM et al. Effects of cinacalcet on fracture events in patients receiving hemodialysis: the EVOLVE trial. J. Am. Soc. Nephrol. 26(6), 1466–1475 (2015).
40.
Palmer SC, Nistor I, Craig JC et al. Cinacalcet in patients with chronic kidney disease: a cumulative meta-analysis of randomized controlled trials. PLoS Med. 10(4), e1001436 (2013).
41.
Zhang Q, Li M, You L et al. Effects and safety of calcimimetics in end stage renal disease patients with secondary hyperparathyroidism: a meta-analysis. PLoS ONE 7(10), e48070 (2012).
42.
Woods BS, Hawkins N, Scott DA. Network meta-analysis on the log-hazard scale, combining count and hazard ratio statistics accounting for multi-arm trials: a tutorial. BMC Med. Res. Methodol. 10, 54 (2010).
43.
Parfrey PS, Block GA, Correa-Rotter R et al. Lessons learned from EVOLVE for planning of future randomized trials in patients on dialysis. Clin. J. Am. Soc. Nephrol. 11(3), 539–546 (2016).
Information & Authors
Information
Published In
Copyright
© 2018 Future Medicine Ltd.
History
Received: 15 February 2018
Accepted: 12 April 2018
Published online: 15 May 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Effects of calcimimetics on long-term outcomes in dialysis patients: literature review and Bayesian meta-analysis. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0015
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Tomohiro Saito, Masahide Mizobuchi, Kiryu Yoshida, Tadashi Kato, Kazuki Abe, Toshiaki Takezaki, Noriyuki Kato, Eisuke Inoue, Hiroaki Ogata, Fumihiko Koiwa, Hirokazu Honda, Association of serum magnesium levels and calcimimetic use: fractures and cardiovascular events in Japanese haemodialysis patients, Journal of Bone and Mineral Metabolism, 10.1007/s00774-025-01682-z, 44, 3, (312-324), (2026).
- Dominik Lewandowski, Miłosz Miedziaszczyk, Katarzyna Lacka, Ilona Idasiak-Piechocka, Cinacalcet Efficacy in Hyperparathyroidism—Chronic Kidney Disease—Non-Dialysis, Hemodialysis, Peritoneal Dialysis, Kidney Transplantation: Critical Review, Biomedicines, 10.3390/biomedicines14010016, 14, 1, (16), (2025).
- Riad Mohammed Abdelrahman, Azmi Mohamed Ali Abdallah, Ayaz Ahmed Ahmed, Taha Hussien Musa, Ismail Adam Arbab, Eltieb Omer Abuelgasim, Mohammed Jalal, Kannan O. Ahmed, Yousif Amin Hassan, Zainab Altrefe, Huda Babikir Ahmed, Real-world evaluation of cinacalcet on hard outcomes in hemodialysis patients in Saudi Arabia, BMC Nephrology, 10.1186/s12882-025-04455-y, 26, 1, (2025).
- L.P. Martynyuk, T.L. Malska, Effect of calcimimetic therapy on bone mineral disorders in patients with stage 5D chronic kidney disease, PAIN, JOINTS, SPINE, 10.22141/pjs.15.3.2025.475, 15, 3, (99-107), (2025).
- Riad Abdelrahman, Taha H. Musa, Chiamaka Linda Mgbechidinma, Eltieb Omer Ahmed, Exploring global calcimimetics research trends: a systematic and thematic review of Web of Science and Scopus databases from 1997 to 2024, Frontiers in Nephrology, 10.3389/fneph.2025.1617466, 5, (2025).
- Kuo-Cheng Lu, Joshua Wang, Cai-Mei Zheng, Kuo-Wang Tsai, Yi-Chou Hou, Chien-Lin Lu, Vitamin D Deficiency and the Clinical Outcomes of Calcimimetic Therapy in Dialysis Patients: A Population-Based Study, Nutrients, 10.3390/nu17091536, 17, 9, (1536), (2025).
- King-Chuen Wu, Iat-Lon Leong, Yuk-Man Leung, Ca2+-sensing receptor-TRP channel-mediated Ca2+ signaling: Functional diversity and pharmacological complexity, European Journal of Pharmacology, 10.1016/j.ejphar.2024.176717, 977, (176717), (2024).
- Xing Liu, Yichen Liu, Peimin Zheng, Xun Xie, Zhouzhou Li, Rui Yang, Lie Jin, Ziwei Mei, Peipei Chen, Limei Zhou, Effects of active vitamin D analogs and calcimimetic agents on PTH and bone mineral biomarkers in hemodialysis patients with SHPT: a network meta-analysis, European Journal of Clinical Pharmacology, 10.1007/s00228-024-03730-5, 80, 10, (1555-1569), (2024).
- Jeremy Rott, Eva Teresa Töpfer, Maria Bartosova, Ivan Damgov, Ana Kolevica, Alexander Heuser, Rukshana Shroff, Sotirios G. Zarogiannis, Anton Eisenhauer, Claus Peter Schmitt, Calcimimetic AMG-416 induced short-term changes in calcium concentrations and calcium isotope ratios in rats, Biochemical and Biophysical Research Communications, 10.1016/j.bbrc.2023.07.060, 677, (88-92), (2023).
- Sevcan A. Bakkaloğlu, Bone Disease in Children with Chronic Kidney Disease, Evidence‐Based Nephrology, 10.1002/9781119105954.ch63, (356-378), (2022).