Adherence and economic impact of paliperidone palmitate versus oral atypical antipsychotics in a Medicare population
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To compare adherence, healthcare utilization and costs among real world, Medicare-eligible patients with schizophrenia using long-acting injectable paliperidone palmitate (PP) versus oral atypical antipsychotics. Patients & methods: Historical cohort study used Medicare Advantage claims data. Inverse probability of treatment weighting was applied to adjust for baseline differences. 12-month adherence, healthcare utilization and costs were compared. Results: Patients using PP were more adherent (proportion of days covered ≥0.8; 48.1 vs 32.6%; p < 0.001), had lower odds of hospitalization (odds ratio [OR]: 0.81; 95% CI: 0.68–0.96) and lower medical costs ($11,095; 95% CI: $10,374–11,867 vs $15,551; 95% CI: $14,584–16,583), but higher pharmacy costs ($14,787; 95% CI: $14,117–15,488 vs $5781; 95% CI: $5530–6043). Conclusion: Compared with patients using oral atypical antipsychotics, PP had lower hospitalizations and medical costs with greater medication adherence accompanied by higher pharmacy costs.
Schizophrenia is a serious psychiatric disorder associated with personal and economic burden, but consistent use of antipsychotic medications may effectively manage schizophrenia symptoms. Although the benefits of antipsychotic medications are well documented [1], poor adherence and high rates of discontinuation continue to be issues leading to more hospitalizations and greater medical costs [2–4]. In 2013 schizophrenia-related direct healthcare costs in the USA exceeded $37.7 billion [5]. For management of schizophrenia symptoms, atypical antipsychotics administered as short-acting oral formulations and long-acting injectable (LAI) formulations are preferred for clinical effectiveness in patients with schizophrenia [6–8]. Oral atypical antipsychotics (OAAs) are considered the first-line treatment for the management of schizophrenia. LAI may be warranted in refractory patients or patients demonstrating nonadherence with OAAs [9,10]. Paliperidone palmitate (PP) is a once-monthly LAI US FDA approved for the treatment of schizophrenia and schizoaffective disorder in adults [11].
The effectiveness of PP compared with OAAs in patients with schizophrenia has been evaluated in certain real-world populations, including Medicaid, Medicare and Veteran’s Health Administration (VHA) enrollees. Medicare is a US federal program that primarily serves people 65 years and older, younger patients with disabilities and dialysis patients; the Medicaid program serves low-income people regardless of age; the VHA program provides healthcare for US military veterans [12,13]. Prior observational studies using VHA claims or Medicaid claims to compare real-world use of PP versus OAA have found greater adherence with PP, lower healthcare resource utilization (HCRU) and lower medical costs with PP use [14–19]. Findings related to total costs have been mixed. One study by Pesa et al. using Medicaid claims data found significantly higher total costs for patients treated with PP [14], while two other studies using Medicaid claims data (Xiao et al. [2015] and Xiao et al. [2016]) and VHA claims data (Baser et al.) did not find differences on total costs between PP users and OAA users [16–18], and one additional study by Young-Xu et al. using VHA electronic health records data found significantly lower total costs for patients treated with PP compared with those treated with OAA [19].
The existing paucity in evidence remains within patients with Medicare coverage being treated with PP versus OAA. Patients receiving treatment for schizophrenia who are Medicare eligible or dually eligible for Medicare and Medicaid may be characteristically different from patients in a Medicaid-eligible population or those covered under the VHA system. Patients who are deemed eligible for Medicare meet one or more of the following requirements: 65 years of age or older; physically or mentally disabled; and/or diagnosed with end-stage renal disease. Compared with traditional Medicaid and VHA populations, Medicare-eligible patients who are eligible for Medicare because of disability may have conditions at a more advanced disease stage. Able-bodied patients in a Medicare-eligible population may have lived longer with schizophrenia than those in traditional Medicaid or VHA populations given that the onset of schizophrenia generally occurs well before age 65.
The primary goals of this study were to describe and compare treatment patterns (including medication adherence, persistence and discontinuation), HCRU and healthcare costs in patients with schizophrenia treated with PP as compared with those being treated with OAA among the Humana Medicare population.
Methods & patients
Data sources
The study sample was selected from the Humana Research Database (KY, USA). Humana, Inc. is a health and wellbeing company serving millions of people across the USA through Medicare Advantage with Prescription Drug plan (MAPD), stand-alone Prescription Drug Plan (PDP) and commercial plan offerings. The database has national coverage with a high proportion of individuals from Texas, Florida and Ohio, and is one of the largest MAPD claims databases. For this study, medical claims and pharmacy claims for the MAPD population were examined. Medical claims data included information regarding physician visits, outpatient visits, emergency department (ED) visits and hospitalizations. Pharmacy claims data included detailed information on each individual’s prescription fill. The full study period was from 1 January 2009 to 30 September 2015. The study protocol was reviewed and approved by Schulman and Associates IRB, Inc. (OH, USA).
Design
This retrospective, longitudinal cohort study identified patients based on paid pharmacy claims for OAA or PP during 1 July 2009 through 30 September 2014. 6 months of baseline data and 12 months of follow-up data within a full study period of 1 January 2009 through 30 September 2015 were required.
Patient selection
Patients were included in the study if they had at least two paid claims for PP or an OAA (aripiprazole, asenapine, iloperidone, lurasidone, olanzapine, paliperidone, quetiapine or ziprasidone) within 90 days of each other during the identification period and enrolled in an MAPD plan at the time of the claim. The date of the first claim was the index date. Patients who met the criteria for the PP cohort as well as the OAA cohort were attributed to the PP cohort and the date of the first PP prescription served as the index date. Patients were only included in the study if they were 18–89 (19–89 if residing in Alabama or Nebraska) years of age and had 18 months of continuous plan enrollment (6 months prior to and 12 months after the index date). PP cohort patients with any PP claims in the preindex period were excluded. OAA cohort patients with an OAA claim for the indexed OAA in the preindex period or with a claim for PP in either the preindex or the 12-month postindex period were excluded. Patients with multiple OAA medications at index were also excluded from the OAA cohort. Patients in PP or OAA cohorts who had a claim for clozapine anywhere in the study period were excluded. Last, patients were also required to have two separate medical claims with a diagnosis code for schizophrenia (ICD-9-CM 295.xx) with at least one occurring in the 6-month preindex period.
Variable definitions
The baseline demographic measures for the study included age, sex, race/ethnicity and geographic region. Age was calculated as of the index date based on date of birth. Sex was categorized as male or female. Race/ethnicity was coded as white, black or other/unknown. Region was recorded as northeast, midwest, south or west based on United States Census region assignments and were determined using the subject’s resident state as of the index date. Low-income subsidy status and dual-eligibility for Medicare and Medicaid were also identified.
The baseline clinical characteristics measured over the 6-month preindex period in this study included the Quan Charlson Comorbidity Index (QCCI), specific physical comorbidities, specific mental health comorbidities and preindex mental health medication use. The QCCI is a medical claims-based risk index that uses 17 disease categories with a score ranging 0–24 based on disease weights [20]. Physical comorbidities included diabetes with chronic complications (ICD-9-CM 250.4–250.9), diabetes without chronic complications (250.0–250.3), obesity (278.00, 278.01, 278.03, 649.1x, V85.3x-V85.4x, V85.54 and 793.91) and hepatitis C (070.41, 070.44, 070.51, 070.54, 070.7x and V02.62) were measured along with mental health comorbidities that included depressive disorders (293.83, 296.2x-296.3x, 300.4 and 311), anxiety disorders (293.84, 300.0x, 300.10, 300.2x, 300.3, 300.5, 300.89, 300.9, 308.x, 309.81, 313.0, 313.1, 313.21, 313.22, 313.3, 313.82 and 313.83), bipolar disorder (296.0x, 296.1x and 296.4x-296.6x) and substance-related and addictive disorders (292.0–292.9, 304.xx, 305.2x-305.9x, 648.3x, 655.5x, 760.72, 760.73, 760.75, 779.5, 965.0x and V65.42). Preindex mental health medication use included antipsychotics (typical and atypical, short-acting and long-acting), antidepressants, anxiolytics and mood stabilizers or anticonvulsants.
All-cause HCRU and total healthcare costs were measured during the baseline period as well. The measurements of HCRU and cost are described in the outcomes measures section.
Outcomes measures
Medication adherence during the follow-up period was evaluated using proportion of days covered (PDC). PDC was calculated for the index drug and was separately calculated based on a composite of all antipsychotics, where PDC equaled the number of days with drug therapy on hand divided by the number of days in the measurement period (365 days).
Image (equation1.eps) is missing or otherwise invalid.
The number of days with drug therapy on hand was calculated using a set of rules to avoid double-counting covered days when prescription fills overlap, as opposed to summing the days of supply for all prescription fills. For PP claims identified through medical services, 37 days of supply (30 days of planned supply + 7 days of additional therapeutic coverage) was used for adherence computation [11]. For PP claims identified through pharmacy claims, 7 days of supply were added to every month of supply so that 28 (or 30) days reported on a claim was estimated as 35 (or 37) days of supply and 84 (or 90) days as 105 (or 111) days, respectively [11]. Medication use during inpatient hospital stays was not captured for the calculation of PDC in this study. The number of days in the measurement period was 365 days for all patients (12 months after the index date). Adherence was defined as PDC ≥0.8.
Further, discontinuation of PP or OAA was defined as exceeding a gap of 60 days without index treatment supply during the 12-month postindex period. Sensitivity analyses for discontinuation were conducted using gaps of 30 and 90 days.
HCRU was represented by outpatient visits, ED visits and hospitalizations, and was measured during the 12-month follow-up period. Multiple hospitalization episodes where the discharge and the admit dates appeared within 1 day (reflecting a possible transfer) were collapsed into a single hospitalization episode. ED encounters that resulted in a hospitalization were considered part of the hospitalization. For HCRU visits lasting more than 1 day, if the first day of service fell in the preindex period, all days for the visit were attributed as preindex HCRU. All-cause HCRU included all visits while mental health-related HCRU was limited to visits with a mental health diagnosis (Supplementary Table 1) in the primary diagnosis position.
Costs were calculated as medical (hospitalization, ED, physician office visits and other outpatient encounters), pharmacy (outpatient pharmacy services) and total costs (medical + pharmacy) and were adjusted to 2015 dollars using the Medical Component of Consumer Price Index.
Statistical methods
The inverse probability of treatment weights (IPTW) method was used to adjust for baseline differences between PP and OAA patients [21]. Propensity score estimates (p) were calculated using a logistic regression model and were used to create a weight for each patient. Propensity scores were generated using the following demographic, clinical and HCRU characteristics: age, gender, race, geographic region, dual Medicare and Medicaid eligibility, low-income subsidy status, physical health comorbidities (proportion with specific conditions), mental health comorbidities (proportion with specific conditions), QCCI, Rx Risk-V score, preindex all-cause costs, preindex all-cause medical visits (ED, hospitalization and outpatient), preindex mental health-related visits (ED, hospitalization and outpatient) and preindex use of antipsychotics, antidepressants, mood stabilizers/anticonvulsants and/or anxiolytics. Weighted cohorts were then compared on 12-month adherence, healthcare utilization and costs [21]. IPTW weighting is inclusive of all patients in a study, unlike other methods such as propensity score matching where unmatched patients would be excluded. The IPTW weight was calculated based on a propensity score model, which modeled the odds of initiating on PP versus OAA medication. For patients in the PP cohort, the weight was calculated as 1/p, where p was the propensity score, and the weight was calculated as 1/(1-p) for patients in the OAA cohort. Normalized weights were truncated at 30 after reviewing for extreme values. Standardized differences were used to evaluate balance on baseline patient characteristics in the IPTW weighted study cohorts.
Frequencies and proportions were used for describing categorical variables and means and standard deviations were used for describing continuous variables. Weighted two-sample t-tests for continuous variables and weighted χ2 tests for categorical variables were used to compare treatment patterns in the two study cohorts. IPTW-weighted logistic regression and Poisson models, without additional covariates, were used to evaluate HCRU in PP versus OAA cohorts. IPTW-weighted generalized linear models with log link and γ distributions, without additional covariates, were used to evaluate costs. Model-specified standard errors were used for IPTW-weighted models.
Data management and analyses were conducted using SAS Enterprise Guide version 7.1 (NC, USA). The a priori α level for all inferential analyses was set at 0.05, and all statistical tests were two-tailed.
Results
Study sample
There were 2591 patients identified for this study, 295 in the PP cohort and 2296 in the OAA cohort (Figure 1). Baseline characteristics of the study population are reported for unweighted and the IPTW-weighted cohorts in Table 1. IPTW weighting resulted in reduced baseline differences between the PP and OAA cohorts as evidenced by lower standardized differences after weighting. As presented in Table 1, a majority of baseline demographic and clinical variables were balanced between the two cohorts after IPTW weighting. Before weighting, the largest standardized differences were 119.3 for unique number of preindex antipsychotic medications, 98.5 for PDC for preindex antipsychotic medications, 81.6 for low-income subsidy status and 71.9 for dual Medicare and Medicaid eligibility; 10 other variables had a standard difference >20.0. After weighting, the largest standardized differences were 25.0 for diabetes with chronic complications and 22.4 for preindex use of antidepressants, with all others <20.0.
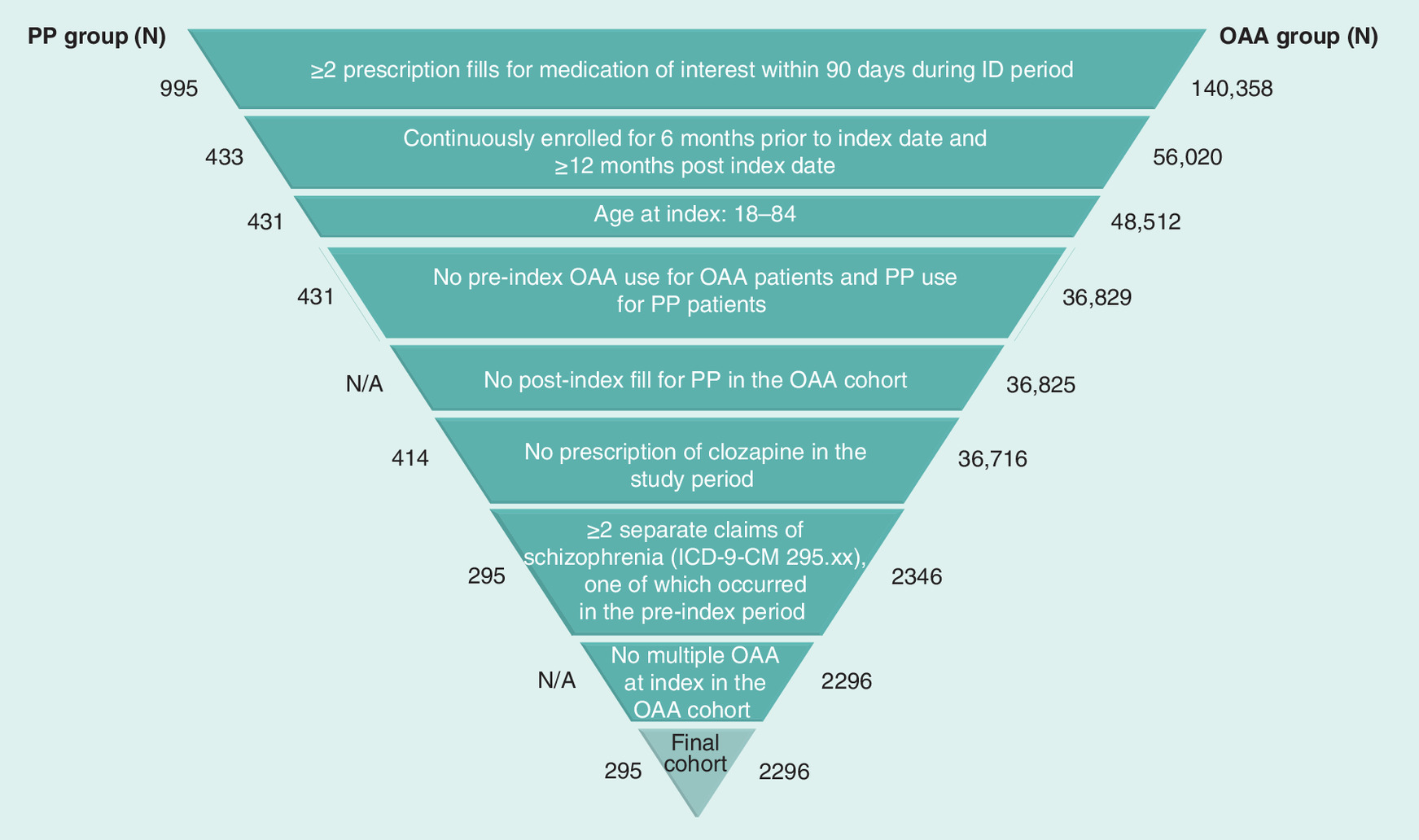
Figure 1. Study sample attrition diagram.
ICD-9-CM: International Classification of Diseases, Clinical modification, Ninth Revision, Clinical Modification; ID: Identification; N/A: Not applicable; OAA: Oral atypical antipsychotics; PP: Paliperidone palmitate.
| Demographic | Before IPTW weighting | After IPTW weighting | ||||
|---|---|---|---|---|---|---|
| PP | OAA | Std d. | PP weighted | OAA weighted | Std d. | |
| All patients (n) | 295 | 2296 | 295 | 2296 | ||
| Weighted n | 1087 | 1190 | ||||
| Age in years, mean ± SD (median) | 48.7 ± 12.9 (49.0) | 55.9 ± 12.6 (56.0) | -55.9 | 56.0 ± 28.5 (56.0) | 55.1 ± 9.2 (56.0) | 4.4 |
| Age category, n (%) | ||||||
| below 35 | 44 (14.9%) | 137 (6.0%) | 29.4 | 113 (10.4%) | 87 (7.3%) | 10.9 |
| 35–44 | 72 (24.4%) | 287 (12.5%) | 31.0 | 163 (15.0%) | 157 (13.2%) | 5.2 |
| 45–54 | 82 (27.8%) | 616 (26.8%) | 2.2 | 225 (20.7%) | 313 (26.3%) | -13.2 |
| 55–64 | 63 (21.4%) | 657 (28.6%) | -16.7 | 254 (23.4%) | 346 (29.1%) | -13.0 |
| 65–74 | <30 | 425 (18.5%) | – | 214 (19.6%) | 204 (17.2%) | 6.2 |
| 75–84 | <10 | 174 (7.6%) | – | 118 (10.9%) | 83 (6.9%) | 14.1 |
| Gender (% female) | 145 (49.2%) | 1251 (54.5%) | -10.6 | 661 (60.8%) | 655 (55.0%) | 11.8 |
| Race/ethnicity, n (%) | ||||||
| White | 194 (65.8%) | 1660 (72.3%) | -14.1 | 854 (78.6%) | 862 (72.4%) | 14.5 |
| Black | 79 (26.8%) | 488 (21.3%) | 12.9 | 205 (18.9%) | 253 (21.3%) | -6.0 |
| Other/unknown | 22 (7.5%) | 148 (6.4%) | 4.3 | 28 (2.6%) | 74 (6.3%) | -18.0 |
| Geographic region, n (%) | ||||||
| Northeast | <10 | 58 (2.5%) | – | 39 (3.6%) | 29 (2.4%) | 7.0 |
| Midwest | 78 (26.4%) | 489 (21.3%) | 12.0 | 325 (29.9%) | 287 (24.1%) | 13.1 |
| South | 190 (64.4%) | 1566 (68.2%) | -8.0 | 639 (58.8%) | 783 (65.8%) | -14.5 |
| West | <30 | 183 (8.0%) | – | 84 (7.7%) | 91 (7.7%) | 0.0 |
| LIS, n (%) | 262 (88.8%) | 1258 (54.8%) | 81.6 | 618 (56.8%) | 702 (58.9%) | -4.3 |
| Dual-eligibility, n (%) | 227 (76.9%) | 1005 (43.8%) | 71.9 | 464 (42.7%) | 572 (48.0%) | -10.7 |
| QCCI, mean ± SD (median) | 0.7 ± 1.2 (0.0) | 1.0 ± 1.6 (0.0) | -23.0 | 0.7 ± 2.3 (0.0) | 1.0 ± 1.1 (0.0) | -14.6 |
| Preindex mental health medication use, n (%) | ||||||
| Antipsychotics | 544 (50.1%) | 575 (48.3%) | 3.6 | |||
| Typical LAI | 35 (11.9%) | 74 (3.2%) | 33.4 | 40 (3.7%) | 78 (6.6%) | -13.1 |
| Atypical LAI | 52 (17.6%) | 32 (1.4%) | 57.5 | 50 (4.6%) | 52 (4.3%) | 1.5 |
| Mean PDC of preindex antipsychotics, mean ± SD (median) | 0.7 ± 0.3 (0.8) | 0.3 ± 0.4 (0.0) | 98.5 | 0.4 ± 0.8 (0.2) | 0.4 ± 0.3 (0.0) | 1.7 |
| Unique number of antipsychotics, mean ± SD (median) | 1.7 ± 1.1 (2.0) | 0.5 ± 0.7 (0.0) | 119.3 | 0.7 ± 1.7 (1.0) | 0.8 ± 1.0 (0.0) | -4.8 |
| Antidepressants | 175 (59.3%) | 1364 (59.4%) | -0.2 | 516 (47.5%) | 697 (58.6%) | -22.4 |
| Antianxiety (anxiolytics) | 83 (28.1%) | 902 (39.3%) | -23.9 | 341 (31.4%) | 448 (37.7%) | -13.3 |
| Mood stabilizers/anticonvulsants | 143 (48.5%) | 823 (35.8%) | 25.9 | 358 (33.0%) | 438 (36.8%) | -8.0 |
| Preindex physical health comorbidities, n (%) | – | |||||
| DM without chronic complications | 65 (22.0%) | 665 (29.0%) | -16.1 | 229 (21.0%) | 350 (29.4%) | -19.4 |
| Obesity | 65 (22.0%) | 399 (17.4%) | 11.6 | 160 (14.7%) | 210 (17.7%) | -8.1 |
| DM with chronic complications | 17 (5.8%) | 274 (11.9%) | -21.6 | 50 (4.6%) | 134 (11.3%) | -25.0 |
| Hepatitis C | <10 | 67 (2.9%) | – | 30 (2.8%) | 34 (2.8%) | 0.0 |
| Number of cardiovascular conditions, mean ± SD (median) | 0.2 ± 0.6 (0.0) | 0.5 ± 1.0 (0.0) | -31.1 | 0.4 ± 1.4 (0.0) | 0.5 ± 0.7 (0.0) | -8.6 |
| Preindex mental health comorbidities, n (%) | ||||||
| Depressive disorders | 113 (38.3%) | 1057 (46.0%) | -15.6 | 441 (40.6%) | 535 (45.0%) | -8.9 |
| Anxiety disorders | 103 (34.9%) | 889 (38.7%) | -7.9 | 348 (32.1%) | 452 (38.0%) | -12.4 |
| Bipolar and related disorders | 114 (38.6%) | 845 (36.8%) | 3.7 | 498 (45.8%) | 439 (36.9%) | 18.1 |
| Schizophrenia | 118 (40.0%) | 690 (30.1%) | 20.9 | 332 (30.6%) | 382 (32.1%) | -3.2 |
| Substance-related and addictive disorders | 59 (20.0%) | 385 (16.8%) | 8.3 | 165 (15.1%) | 205 (17.2%) | -5.7 |
| Number of preindex hospitalizations, mean ± SD (median) | 1.01 ± 1.2 (1.0) | 0.76 ± 1.1 (0.0) | 22.61 | 0.80 ± 2.1 (0.0) | 0.80 ± 0.8 (0.0) | -0.31 |
| Number of preindex mental health-related hospitalizations, mean ± SD (median) | 0.29 ± 0.7 (0.0) | 0.25 ± 0.6 (0.0) | 6.54 | 0.27 ± 1.5 (0.0) | 0.25 ± 0.4 (0.0) | 1.65 |
| Total costs | $14,936 ± 14,188 ($10,270) | $13,091 ± 21,717 ($5946) | 10.06 | $10,896 ± 24,220 ($5983) | $13,708 ± 15,810 ($6727) | -13.75 |
The table above lists the clinical characteristics used in the model to generate propensity scores which were then used in the calculation of IPTW weights. The weighted N represents the number of observations in each IPTW weighted pseudo-cohort. Cell counts of <30 patients and corresponding Std d. are masked for confidentiality purposes. Patients <65 years of age may be eligible for Medicare due to disability or diagnosis of end-stage renal disease.
DM: Diabetes mellitus; IPTW: Inverse probability of treatment weight; LAI: Long-acting injectable therapy; LIS: Low-income subsidy; MAPD: Medicare Advantage Prescription Drug; OAA: Oral atypical antipsychotic; PDC: Proportion of days covered; PP: Paliperidone palmitate; QCCI: Quan Charlson’s Comorbidity Index; SD: Standard deviation; Std d.: Standardized difference.
Antipsychotic utilization & adherence
A significantly lower proportion of patients initiating PP discontinued treatment (defined as a gap of 60 days) as compared with those initiating OAA (50.3 vs 59.2%; p < 0.001) (Table 2). This result was robust to a sensitivity analysis using alternative gaps of 30 days (60.6 vs 73.2%; p < 0.001) and 90 days (44.5 vs 51.6%; p < 0.001) (Table 2). Also, patients in the PP cohort had better adherence to their index medication compared with patients in the OAA cohort based on either the mean PDC (0.66 vs 0.57; p < 0.001) or the proportion of patients who had PDC at 0.8 or above (48.1 vs 32.6%; p < 0.001) (Table 2). Similar results were seen when the unit of analysis was the overall antipsychotic class rather than just the index medication where PDC for any antipsychotic was greater for patients in the PP cohort (0.77 vs 0.70; p < 0.001) and more patients had PDC at 0.8 or above (65.9 vs 49.3%; p < 0.001) (Table 2).
| Measure | PP | OAA | p-value |
|---|---|---|---|
| All patients | 295 | 2296 | |
| Weighted n | 1087 | 1190 | |
| PDC for antipsychotics, mean ± SD (median) | 0.77 ± 0.54 (0.92) | 0.70 ± 0.19 (0.79) | <0.001 |
| PDC ≥0.8, n (%) | 716 (65.9%) | 586 (49.3%) | <0.001 |
| Discontinuation of index medication | |||
| 30-day gap, n (%) | 659 (60.6%) | 871 (73.2%) | <0.001 |
| 60-day gap, n (%) | 547 (50.3%) | 704 (59.2%) | <0.001 |
| 90-day gap, n (%) | 483 (44.5%) | 614 (51.6%) | <0.001 |
| PDC for index drug, mean ± SD (median) | 0.66 ± 0.62 (0.75) | 0.57 ± 0.21 (0.57) | <0.001 |
| PDC ≥0.8, n (%) | 523 (48.1%) | 388 (32.6%) | <0.001 |
The weighted n represents the number of observations in each IPTW weighted pseudo-cohort.
IPTW: Inverse probability of treatment weight; LAI: Long-acting injectable therapy; MAPD: Medicare Advantage Prescription Drug; OAA: Oral atypical antipsychotic; PDC: Proportion of day covered; PP: Paliperidone palmitate; SD: Standard deviation.
Healthcare utilization & costs
Comparisons of all-cause HCRU during the follow-up period demonstrated lower healthcare use in the PP relative to OAA cohort (Table 3 & Figure 2). Almost all patients had an outpatient visit, but a lower proportion of patients in the PP cohort had an all-cause outpatient visit and the difference, although marginal, was statistically significant (93.8 vs 94.4%; p < 0.001) (Table 3). A significantly lower proportion of the PP cohort had an all-cause hospitalization compared with the OAA cohort (34.1 vs 39.1%; p = 0.013) (Table 3). The average number of hospitalizations were also significantly lower for patients in the PP cohort compared with the OAA cohort (0.62 vs 0.85; p = 0.002). For patients with a hospitalization, the average inpatient days were significantly lower for patients in the PP cohort compared with the OAA cohort (4.73 vs 7.28; p = 0.0014) (Table 3). Results from the logistic and Poisson regression model provided additional evidence of the above findings. PP patients had significantly lower odds (odds ratio [OR]; CI) of having an all-cause hospitalization compared with OAA patients (OR: 0.81; 95% CI: 0.68–0.96) (Figure 2); incidence rate of all-cause hospitalizations was also lower in the PP cohort compared with the OAA cohort (incidence rate ratio: 0.73; 95% CI: 0.64–0.83) (Figure 2). Proportions of patients with an all-cause ED visit were not statistically different between the PP and OAA cohorts (58.7 vs 55.9%; p = 0.176) (Table 3). Logistic regression and Poisson regression models corroborated the lack of statistically significant differences between the PP cohort and OAA cohort in terms of all-cause ED visits (Figure 2).
| PP | OAA | p-value | |
|---|---|---|---|
| Unique number of patients (n) | 295 | 2296 | |
| Weighted n | 1087 | 1190 | |
| All-cause | |||
| Outpatient visits | |||
| Had ≥1 outpatient visit, n (%) | 1,019 (93.8%) | 1171 (98.4%) | <0.001 |
| Number of visits, mean ± SD (median) | 18.03 ± 30.8 (15.0) | 19.24 ± 12.2 (15.0) | 0.2289 |
| ED visits | |||
| Had ≥1 ED visit, n (%) | 638 (58.7%) | 666 (55.9%) | 0.1756 |
| Number of visits, mean ± SD (median) | 2.29 ± 9.7 (1.0) | 2.54 ± 4.0 (1.0) | 0.4326 |
| Hospitalizations | |||
| Had ≥1 hospitalization, n (%) | 371 (34.1%) | 466 (39.1%) | 0.0134 |
| Number of hospitalizations, mean ± SD (median) | 0.62 ± 2.1 (0.0) | 0.85 ± 1.3 (0.0) | 0.002 |
| Average inpatient days per patient, mean ± SD (median) | 4.73 ± 23.4 (0.0) | 7.28 ± 12.2 (0.0) | 0.0014 |
| Mental health-related resource utilization | |||
| Outpatient visits | |||
| Had ≥1 outpatient visit, n (%) | 346 (31.8%) | 563 (47.3%) | <0.001 |
| Number of visits, mean ± SD (median) | 3.03 ± 13.9 (0.0) | 3.37 ± 6.2 (0.0) | 0.4694 |
| ED visits | |||
| Had ≥1 ED visit, n (%) | 179 (16.5%) | 216 (18.1%) | 0.305 |
| Number of visits, mean ± SD (median) | 0.41 ± 2.6 (0.0) | 0.42 ± 1.0 (0.0) | 0.9866 |
| Hospitalizations | |||
| Had ≥1 hospitalization, n (%) | 111 (10.2%) | 143 (12.0%) | 0.1624 |
| Number of hospitalizations, mean ± SD (median) | 0.15 ± 0.9 (0.0) | 0.21 ± 0.5 (0.0) | 0.0629 |
| Average inpatient days per patient, mean ± SD (median) | 1.03 ± 7.8 (0.0) | 1.86 ± 6.4 (0.0) | 0.006 |
The weighted n represents the number of observations in each IPTW weighted pseudo-cohort. p-values were computed using the weighted two-sample t-test for continuous variables and the weighted χ2 test for categorical variables (all tests are two-sided).
ED: Emergency department; IPTW: Inverse probability of treatment weight; MAPD: Medicare Advantage Prescription Drug; OAA: Oral atypical antipsychotic; PP: Paliperidone palmitate; SD: Standard deviation.
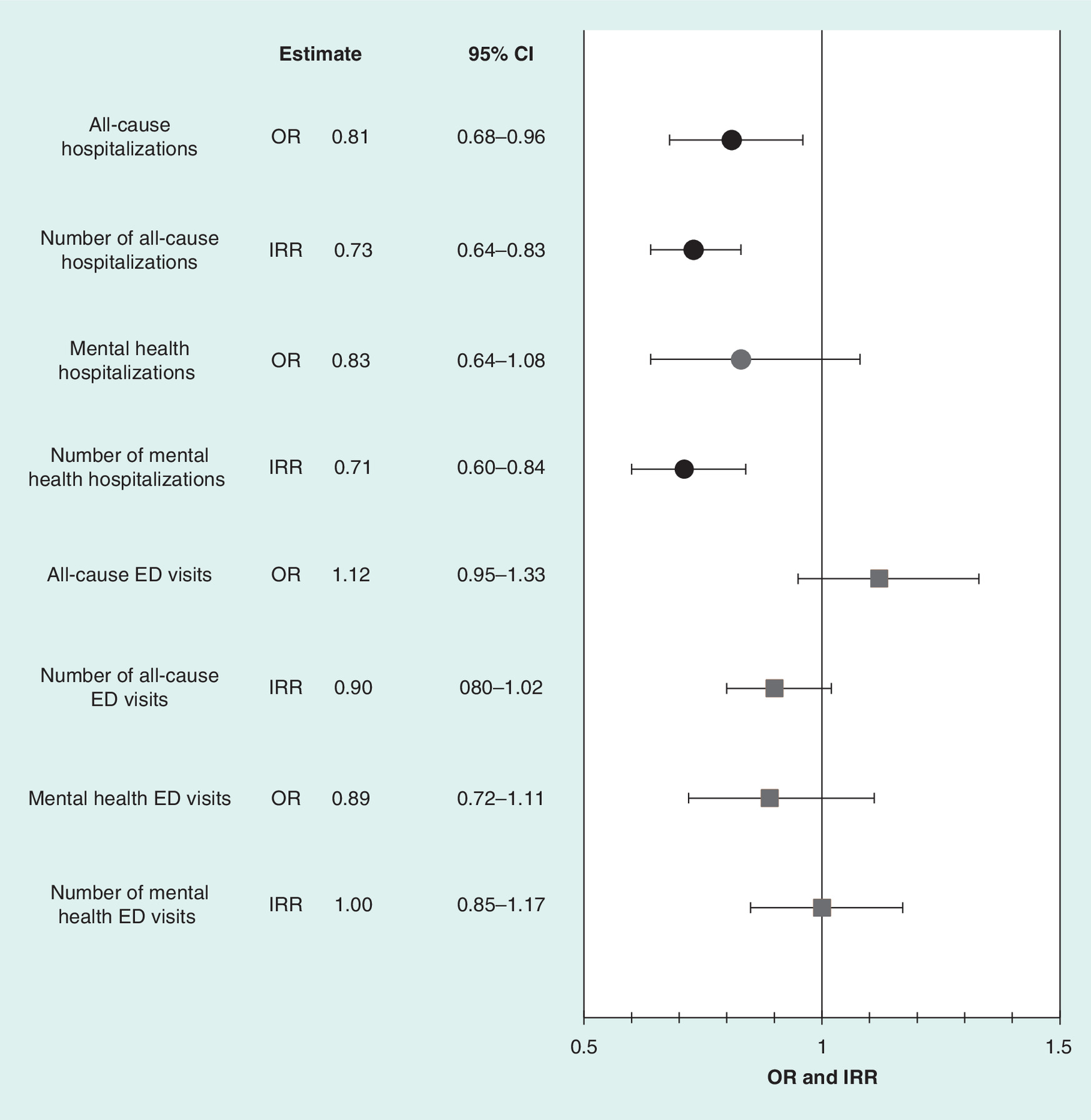
Figure 2. Healthcare resource utilization based on weighted logistic regression and Poisson model (oral atypical antipsychotic as reference).
CI: Confidence interval; ED: Emergency department; IRR: Incidence rate ratio; OAA: Oral atypical antipsychotic; OR: Odd ratio.
Comparison of mental health-related outpatient visits followed the same patterns as all-cause outpatient visits with a significantly lower proportion of the PP cohort having a mental health-related outpatient visit than the OAA cohort (31.8 vs 47.3%; p < 0.001) (Table 3). There was no statistically significant difference between the PP and OAA cohorts for the average number of mental health-related hospitalizations or the proportion of patients with a mental health-related hospitalization (Table 3), but for those patients with a mental health-related hospitalization, the average inpatient days were lower for PP patients than for OAA patients (1.03 vs 1.86; p = 0.006) (Table 3). Based on results of the logistic regression model, the number of mental health-related hospitalizations was significantly lower in the PP cohort compared with the OAA cohort based on Poisson regression (incidence rate ratio: 0.71; 95% CI: 0.60–0.84) (Figure 2). Consistent with the finding of a lower count of mental health-related hospitalizations, the average mental health-related inpatient days was lower for the PP cohort based on weighted t-test (1.03 vs 1.86; p = 0.006). Proportions of patients with a mental health-related ED visit were not statistically different for the PP and OAA cohorts (Table 3). Logistic regression and Poisson regression models corroborated the lack of statistically significant differences between the PP cohort and OAA cohort in terms of mental health-related ED visits (Figure 2).
Pharmacy costs were significantly higher for the PP cohort compared with the OAA cohort ($14,787 vs 5781; p < 0.001) (Table 4). However, the significantly lower medical costs for the PP group ($11,095 vs 15,551; p < 0.001) offset some of the increased pharmacy costs, but total costs were significantly higher for the PP cohort compared with the OAA cohort ($25,882 vs 21,332; p < 0.001) (Table 4).
| Type of cost | PP | OAA | Mean difference | p-value† | ||
|---|---|---|---|---|---|---|
| Mean ± SD (median) | 95% CI of mean cost† | Mean ± SD (median) | 95% CI of mean cost† | |||
| Total costs | $25,882 ± 36,747 ($20,459) | $24,662–27,163 | $21,332 ± 19,699 ($11,616) | $20,370–22,340 | $4550 | < .001 |
| Rx costs | $14,787 ± 20,381 ($12,489) | $14,117–15,488 | $5781 ± 4623 ($3943) | $5530–6043 | $9006 | <0.001 |
| Medical costs | $11,095 ± 31,618 ($4433) | $10,374–11,867 | $15,551 ± 17,802 ($5443) | $14,584–16,583 | -$4456 | <0.001 |
| Hospital costs | $4885 ± 21,831 ($0) | $4227–5645 | $8333 ± 13,662 ($0) | $7258–9568 | -$3448 | <0.001 |
| ED costs | $984 ± 4211 ($218) | $879–1101 | $1281 ± 2146 ($182) | $1150–1427 | -$297 | <0.001 |
| Outpatient costs | $2501 ± 6270 ($1406) | $2346–2666 | $3206 ± 3656 ($1,728) | $3016–3408 | -$705 | <0.001 |
| Other medical costs | $2725 ± 14,886 ($377) | $2474–3003 | $2731 ± 5306 ($558) | $2489–2996 | -$6 | 0.977 |
†
95% CI and p-value were based on generalized linear model.
Medical costs include hospitalization, ED, outpatient and other medical costs. The costs above represent the amount paid by the plan. Actual amount charged for the service may be higher than the costs displayed.
ED: Emergency department; OAA: Oral atypical antipsychotic; PP: Paliperidone palmitate; SD: Standard deviation.
Discussion
This study compared treatment persistence and adherence, HCRU and healthcare costs in patients with schizophrenia treated with PP versus OAAs among the Humana Medicare population.
The results of this study indicate that treatment with PP was associated with greater adherence, lower discontinuation of treatment, fewer hospitalizations, lower medical costs and greater pharmacy costs than treatment with OAA. The price for a monthly PP injection is certainly higher than a month’s supply of OAA, and the higher price for PP or other LAIs relative to OAAs may discourage widespread use of LAIs. It is important to note that greater 12-month adherence for PP or another LAI relative to OAA would inevitably result in higher pharmacy costs even if the price of a monthly injection were the same as a month’s supply of OAA. Beyond drug prices, it is important to assess the value of medications based on the associated real-world outcomes that demonstrate the all-encompassing perspective on healthcare costs. This study found a lower mean medical cost over 12 months that offset about 50% of the higher mean pharmacy costs over the same 12-month period. Additionally, the amount of medical cost offset observed for this study should be considered as conservative since pharmacy costs did not account for branded drug discounts or rebates, which are unknown but may have overestimated PP costs in this study. Medical cost offsets for PP treated patients as compared with OAA treated patients have been observed in all other real-world studies and in some cases the medical offsets for PP treated patients are sufficient to overcome the higher pharmacy costs of PP ultimately resulting in similar or lower total costs relative to OAA treated patients [15–19]. This applies to all branded antipsychotic medications.
This study contributes to the existing body of published literature by demonstrating lower rates of hospitalization, lower medical costs, higher pharmacy costs, lower rates of medication discontinuation and greater medication adherence in patients with schizophrenia who received PP versus OAAs in a large national fully-insured MAPD health plan. Prior real-world studies have made similar observations of lower rates of hospitalization and lower medical costs in Medicaid and VHA populations [14–19]. Although treatment with PP was associated with significantly lower odds of hospitalization, the lower odds of the more specific mental health-related hospitalization was not statistically significant. The study might have had insufficient power to detect the difference between PP and OAA on the more specific measure of mental health-related hospitalization. Although the finding of lower medical costs observed in this study is consistent with the findings from other studies, some studies of Medicaid patients and VHA patients found a greater medical cost offset relative to pharmacy costs for patients using PP than was observed for this study [14–19]. The adherence to PP observed for the MAPD patients in the current study might partially explain the higher pharmacy costs and lower medical cost offset for this study as compared with studies of Medicaid or VHA populations. Another study also found higher antipsychotic adherence levels for MAPD patients compared with Medicaid patients [22]. While some prior studies of PP versus OAA did not report medication adherence [14–18], several studies have reported proportions of patients adherent to PP that were lower than those reported in the current study [19,23]. Our study observed adherence for 65.9% of PP patients, which is greater than the 51.0% of PP patients adherent in a Medicaid population [23] and considerably greater than the 35.8% of PP patients adherent in a VHA population [19]. The study of VHA patients measured PDC over 12 months like our study, but the study of Medicaid patients measured PDC over 6 months [23]. Given that pharmacy cost and adherence are necessarily related, the pharmacy costs incurred over 12 months in this current study of MAPD patients may have been too great to be offset by medical costs that can be avoided within the same 12 months. Future studies should observe outcomes, including cost, over a longer follow-up period.
This study is the first to focus on MAPD patients who are typically older than the general population. Patients under the age of 65 may be eligible for MAPD plans due to disability, which is another potentially unique characteristic of this study’s populations. The patients in this study may be substantially different than patients in Medicaid or VHA populations, yet the overall findings of greater adherence and fewer hospitalizations for patients using PP within this Medicare population are similar to those of previous studies of Medicaid and VHA populations [14–19]. Additionally, MAPD plans may provide different benefits or have different benefit structures as compared with Medicaid plans and most certainly have different benefits and structure than that of the VHA. Future studies could explore the possible differences among various populations in terms of comorbid conditions, underlying risk for antipsychotic nonadherence, risk of hospitalizations, among others, and evaluate the impact of those differences on antipsychotic medication adherence and avoidable hospitalizations. Alternatively, a pooled analysis of patients from multiple populations could be executed to remove population differences from effecting the comparison of LAIs, like PP and OAAs, so long as methodological issues can be overcome using a common data model or other method.
This study focused on PP versus OAAs, and the findings could be applied to all LAIs rather than just PP given that several studies have failed to find clinically meaningful differences between PP and other LAIs [24–26]. However, other observational studies suggest that PP and other LAIs are not interchangeable [27,28], so more evidence may be needed to determine whether the findings of this study would hold if all LAIs were grouped and compared with OAAs.
Our study has several limitations. Comparing PP or other LAI use to OAA use in a real-world population is challenging because patients typically start atypical antipsychotic treatment with an OAA before they start an LAI such as PP. Managed care plans may even require trial of an OAA before reimbursement for an LAI will be permitted. Patients using an OAA followed by an LAI may have been nonadherent to the OAA, but were using an OAA due to the treatment norms and systematic access limitations for LAIs. Because patients using LAIs including PP are fundamentally different from the general population of OAA users, propensity score methods like IPTW are necessary to reduce bias for real-world observational studies. In the study populations, there were substantial differences among the PP cohort and OAA cohort before weighting. Patients using PP were younger, had lower comorbidity as defined by the Quan–Charlson Index, were much more likely to be dually eligible for Medicare and Medicaid, much more likely to receive a low-income subsidy, and more likely to have used antipsychotic drugs previously. After weighting, the analytical cohorts were more balanced in terms of these characteristics.
The measurements of treatment discontinuation and treatment adherence in this study were potentially influenced by adjustment of the days of supply for PP to add seven days of expected benefit beyond the documented days of supply. While the adjustment could be seen as introducing bias to the study, it was warranted based on clinical reasoning for the actual expected days of benefit and dosing instructions for PP [11]. In this case, the expected days of treatment benefit for an injection of PP simply does not align with typical, standard estimates for days of supply of 28 or 30 days that is historically based on daily dosing of oral medications such as OAAs.
Common limitations associated with use of administrative claims data apply to this study. Utilization of PP or OAA was identified using pharmacy and medical claims data which only implies receipt and payment for the respective medication, but actual medication consumption is presumed. As is the case with studies using administrative pharmacy claims data, the measurement of pharmacy cost did not account for branded drug rebates, so pharmacy cost as reported could be higher than the actual net costs of drugs from the payer’s perspective. The potential impact to the magnitude of effect on pharmacy costs if the actual net costs of drugs were known cannot be determined for this study. Diagnosis of schizophrenia among MAPD patients was determined based on diagnosis codes intended for processing claims payments rather than for clinical diagnostics. We presume the diagnosis code reflects the patient’s actual condition, but misclassification was possible. The requirement of at least two claims with a schizophrenia diagnosis code should have limited misclassification due to miscoding of administrative claims.
Generalizing the study findings to the overall USA population should be approached with caution since this study only focused on patients enrolled in Medicare plans in which eligibility is determined by age ≥65 or by disability, suggesting that this study population is older than the general population of patients with schizophrenia. Caution should also be exercised in generalizing the findings to the overall Medicare-eligible population because the focus was on an MAPD population. Most patients with schizophrenia, particularly those receiving the LIS, enroll in PDPs. Additionally, the share of patients aged 65 and older was higher in this MAPD population with schizophrenia than in the PDP population with schizophrenia. The data presented in this study should be evaluated in combination with data from other populations to better understand the impact of using PP versus OAA on the overall population of patients with schizophrenia. Although study subjects were selected from the membership of a national health plan (Humana, Inc.), the geographic distribution was unbalanced, with the largest number of individuals residing in the southern region, fewer in the midwest region, and much smaller number of individuals in the west and northeast.
Conclusion
The study found that Medicare patients with schizophrenia being treated with PP had greater adherence, fewer hospitalizations, lower medical costs and higher pharmacy costs than those treated with OAA. This study’s findings are consistent with those of previous studies using similar methods for real-world observations among Medicaid and VHA patients treated with PP versus OAA.
•
Comparing a long-acting injectable (LAI) antipsychotic, like paliperidone palmitate (PP), to oral atypical antipsychotics (OAAs) in a real-world population is challenging because patients typically start atypical antipsychotic treatment with an OAA before starting an LAI.
•
LAIs administered each month have adherence advantages over daily OAAs and may be utilized by patients who struggle with OAA adherence.
•
Since patients indexing to PP were fundamentally different than patients indexing to an OAA, our study utilized propensity scores and inverse probability of treatment weighting to reduce bias associated with differences across PP and OAA cohorts.
•
The results of this study indicate that treatment with PP was associated with greater adherence and lower discontinuation of treatment as compared with OAAs.
•
The results of this study also indicate that PP patients experience fewer hospitalizations and lower overall medical costs, than patients treated with OAA.
•
Prior real-world studies have made similar observations of lower rates of hospitalization and lower medical costs with PP relative to OAAs in Medicaid and Veteran’s Health Administration populations.
•
Pharmacy costs were higher for PP treated patients as compared with OAA treated patients, likely due to higher product costs of PP and greater adherence to PP.
•
Approximately 50% of the higher pharmacy costs were offset by lower medical costs. Other real-world studies have observed medical offsets for PP treated patients that are sufficient to overcome the higher pharmacy costs of PP ultimately resulting in similar or lower total costs relative to OAA treated patients.
•
This study contributes to the existing body of published literature by demonstrating benefits and costs of PP relative to OAAs in a Medicare-eligible population, who are generally much older than the national population. The Medicare-eligible population has not been studied previously.
Financial & competing interests disclosure
This study was funded by Janssen Scientific Affairs, LLC. Janssen Pharmaceuticals, Inc. owns a branded paliperidone palmitate product (Invega Sustenna®). K Joshi and E Muser are employees of Janssen Scientific Affairs, LLC, and are Johnson & Johnson stockholders. Y Xu, P Schwab and B Suehs are employees of Comprehensive Health Insights, Inc., a wholly owned subsidiary of, Humana, Inc. that received funding from Janssen Scientific Affairs, LLC for data and research consulting services to conduct this study. M Datar was an employee of Comprehensive Health Insights, Inc. at the time of the study. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
The authors acknowledge N Davis, PharmD, an employee of Comprehensive Health Insights, Inc., for assistance with writing the manuscript.
Ethical conduct of research
The study protocol, waiver of written informed consent, and waiver of authorization to use and disclose protected health information were approved by Schulman IRB (OH, USA), an independent Institutional Review Board (IRB) fully accredited by the Association for the Accreditation of Human Research Protection Programs (registration number is 00000971). This study followed the principles outlined in the Declaration of Helsinki.
Supplementary Material
File (supplementary_table_1.docx)
- Download
- 31.66 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Tandon R. Safety and tolerability: how do newer generation “atypical” antipsychotics compare? Psychiatr. Q. 73(4), 297–311 (2002).
2.
Haddad PM, Brain C, Scott J. Nonadherence with antipsychotic medication in schizophrenia: challenges and management strategies. Patient Relat. Outcome Meas. 5, 43–62 (2014).
• Provides a good overall review of the problem of adherence with antipsychotic medications, its assessment and interventions to improve adherence.
3.
Lang K, Meyers JL, Korn JR et al. Medication adherence and hospitalization among patients with schizophrenia treated with antipsychotics. Psychiatr. Serv. 61(12), 1239–1247 (2010).
4.
Gilmer TP, Dolder CR, Lacro JP et al. Adherence to treatment with antipsychotic medication and health care costs among Medicaid beneficiaries with schizophrenia. Am. J. Psychiatry 161(4), 692–699 (2004).
5.
Cloutier M, Aigbogun MS, Guerin A et al. The economic burden of schizophrenia in the United States in 2013. J. Clin. Psychiatry 77(6), 764–771 (2016).
•• Estimates direct and nondirect healthcare costs, as well as nonhealthcare costs attributable to schizophrenia. Excess costs for schizophrenia were attributable to unemployment, productivity loss due to caregiving, and direct healthcare costs.
6.
Lehman AF, Lieberman JA, Dixon LB et al. Practice guideline for the treatment of patients with schizophrenia, second edition. Am. J. Psychiatry 161(2 Suppl.), 1–56 (2004).
7.
Kreyenbuhl J, Buchanan RW, Dickerson FB, Dixon LB, Schizophrenia Patient Outcomes Research Team (PORT). The schizophrenia patient outcomes research team (PORT): updated treatment recommendations 2009. Schizophr. Bull. 36(1), 94–103 (2009).
8.
Barnes T; Schizophrenia Consensus Group of British Association for Psychopharmacology. Evidence-based guidelines for the pharmacological treatment of schizophrenia: recommendations from the British Association for Psychopharmacology. J. Psychopharmacol. 25(5), 567–620 (2011).
9.
Patel MX, Taylor M, David AS. Antipsychotic long-acting injections: mind the gap. Br. J. Psychiatry Suppl. 52, S1–S4 (2009).
10.
Kaplan G, Casoy J, Zummo J. Impact of long-acting injectable antipsychotics on medication adherence and clinical, functional, and economic outcomes of schizophrenia. Patient Prefer. Adherence 7, 1171–1180 (2013).
11.
Invega Sustenna (paliperidone palmitate) extended-release injectable suspension, for intramuscular use [package insert]. Titusville, NJ, USA: Janssen Pharmaceuticals, Inc. (June 2017). www.janssenlabels.com/package-insert/product-monograph/prescribing-information/INVEGA+SUSTENNA-pi.pdf
12.
US Department of Health and Human Services. What is the difference between Medicare and Medicaid? www.hhs.gov/answers/medicare-and-medicaid/what-is-the-difference-between-medicare-medicaid/index.html
13.
US Department of Veterans Affairs. About VHA. www.va.gov/health/aboutVHA.asp
14.
Pesa JA, Muser E, Montejano LB, Smith DM, Meyers OI. Costs and resource utilization among Medicaid patients with schizophrenia treated with paliperidone palmitate or oral atypical antipsychotics. Drugs Real World Outcomes 2(4), 377–385 (2015).
• As in this study, paliperidone palmitate (PP) was associated with greater adherence, lower medical costs, but higher pharmacy costs relative to treatment with oral atypical antipsychotics.
15.
Lafeuille MH, Grittner AM, Fortier J et al. Comparison of rehospitalization rates and associated costs among patients with schizophrenia receiving paliperidone palmitate or oral antipsychotics. Am. J. Health Syst. Pharm. 72(5), 378–389 (2015).
•• The authors found lower rehospitalization rates and lower medical costs for patients taking PP versus patients taking oral atypical antipsychotics.
16.
Baser O, Xie L, Pesa J, Durkin M. Healthcare utilization and costs of Veterans Health Administration patients with schizophrenia treated with paliperidone palmitate long-acting injection or oral atypical antipsychotics. J. Med. Econ. 18(5), 357–365 (2015).
17.
Xiao Y, Muser E, Lafeuille MH et al. Impact of paliperidone palmitate versus oral atypical antipsychotics on healthcare outcomes in schizophrenia patients. J. Comp. Effectiveness Res. 4(6), 579–592 (2015).
18.
Xiao Y, Muser E, Fu DJ et al. Comparison of Medicaid spending in schizoaffective patients treated with once monthly paliperidone palmitate or oral atypical antipsychotics. Curr. Med. Res. Opin. 32(4), 759–769 (2016).
19.
Young-Xu Y, Duh MS, Muser E et al. Impact of paliperidone palmitate versus oral atypical antipsychotics on health care resource use and costs in veterans with schizophrenia. J. Clin. Psychiatry 77(10), e1332–e1341 (2016).
•• Treatment with PP was associated with significantly reduced inpatient hospitalization and higher mental health intensive case management. Higher pharmacy and outpatient costs with PP treatment were offset by lower inpatient stay costs, resulting in total overall cost savings with PP relative to oral agents.
20.
Quan H, Sundararajan V, Halfon P et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 43(11), 1130–1139 (2005).
21.
Austin PC, Stuart EA. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 34(28), 3661–3679 (2015).
22.
Roberto P, Brandt N, Onukwugha E et al. Adherence to antipsychotic therapy: association with hospitalization and Medicare spending among part D enrollees with schizophrenia. Psychiatr. Serv. 68(11), 1185–1188 (2017).
23.
Marcus SC, Zummo J, Pettit AR, Stoddard J, Doshi JA. Antipsychotic adherence and rehospitalization in schizophrenia patients receiving oral versus long-acting injectable antipsychotics following hospital discharge. J. Manag. Care Spec. Pharm. 21(9), 754–768 (2015).
• This claims-based analysis of posthospitalization and rehospitalization outcomes in Medicaid patients shows lower rates of nonadherence, continuous 60-day gap in medication coverage, and rehospitalization in patients using long-acting injectables (LAIs) compared with oral medication; second-generation LAIs conferred the greatest benefits. PP was the only LAI associated with a statistically significant lower risk of rehospitalization compared with oral medication.
24.
Fleischhacker WW, Gopal S, Lane R et al. A randomized trial of paliperidone palmitate and risperidone long-acting injectable in schizophrenia. Int. J. Neuropsychopharmacol. 15(1), 107–118 (2012).
25.
McEvoy JP, Byerly M, Hamer RM et al. Effectiveness of paliperidone palmitate vs haloperidol decanoate for maintenance treatment of schizophrenia: a randomized clinical trial. JAMA 311(19), 1978–1987 (2014).
26.
Rosenheck RA, Leslie DL, Sint KJ et al. Cost-effectiveness of long-acting injectable paliperidone palmitate versus haloperidol decanoate in maintenance treatment of schizophrenia. Psychiatr. Serv. 67(10), 1124–1130 (2016).
27.
NAMI Utah. Preferred drug list. http://namiut.org/images/PDL_-_Research_Summary__NAMI_Utah__Visuals_2016.pdf
• Data from the National Alliance on Mental Illness, Utah, outlining the consequences of access restrictions to mental health medications.
28.
Basu A, Jena AB, Goldman DP, Philipson TJ, Dubois R. Heterogeneity in action: the role of passive personalization in comparative effectiveness research. Health Econ. 23(3), 359–373 (2014).
•• A study of antipsychotic drug use in Medicaid patients with schizophrenia found that patients receiving generic medications had significantly higher numbers of overall and schizophrenia-related hospitalizations within 1 year.
Information & Authors
Information
Published In
Pages: 723 - 735
PubMed: 29722547
Copyright
© 2018 Future Medicine Ltd.
History
Received: 5 January 2018
Accepted: 11 April 2018
Published online: 3 May 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Adherence and economic impact of paliperidone palmitate versus oral atypical antipsychotics in a Medicare population. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0003
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Laura Morrison, Dominic Pilon, Arthur Voegel, Lilian Diaz, Kana Yokoji, Carmela Benson, Antipsychotic Treatment Pathways, Real-World Adherence, Healthcare Resource Utilization, and Healthcare Costs Among Patients With Schizophrenia Treated With Once-Monthly, Once-Every-Three-Months, and Once-Every-Six-Months Paliperidone Palmitate in the United States, Clinical Therapeutics, 10.1016/j.clinthera.2026.02.006, 48, 4, (317-325), (2026).
- G. HEYLENS, A. AELBRECHT, Therapietrouw bij psychotische stoornissen: orale versus langwerkende injecteerbare antipsychotica, Tijdschrift voor Geneeskunde en Gezondheidszorg, 10.47671/TVG.82.25.080, (2026).
- Michael Grabner, Yueh-Yi Chiang, Chia-Chen Teng, Susan dosReis, Katherine Harris, Characteristics and Utilization Patterns of Medicare Beneficiaries Initiating Long-Acting Injectable Antipsychotic Medications, ClinicoEconomics and Outcomes Research, 10.2147/CEOR.S567370, Volume 18, (1-13), (2026).
- Aleksandr M. Reznik, Olga A. Karpenko, Elena A. Shumakova, Aleksandr V. Mudrak, Andrey V. м, Svetlana V. Nazimova, Alina M. Saifulina, Anton M. Eliseenko, Tatjana K. Matvievskaya, Angelina N. Khannanova, Vladimir I. Revenko, Dmitriy V. Scherbakov, Yuriy L. Martynyuk, Aleksandr L. Arbuzov, Oleg A. Yacenko, Polina N. Alekseeva, Aleksandr B. Berdalin, Larisa A. Burygina, Dynamics of Clinical Manifestations and Social Functioning in Schizophrenia: A Non-interventional Observational Study of Paliperidone Palmitat Dosage Forms, Consortium Psychiatricum, 10.17816/CP15567, 5, 4, (16-38), (2024).
- Yixiang Zhou, Binbin Chen, Yinghua Huang, Healthcare utilization and economics evaluation of paliperidone palmitate once-monthly in schizophrenia: a one-year, real-world, and retrospective mirror image study in China, Frontiers in Psychiatry, 10.3389/fpsyt.2024.1415275, 15, (2024).
- Rui Luo, He Lu, Hengfen Li, Cost-utility analysis of using paliperidone palmitate in schizophrenia in China, Frontiers in Pharmacology, 10.3389/fphar.2023.1238028, 14, (2023).
- Stefano Bramante, Gabriele Di Salvo, Giuseppe Maina, Gianluca Rosso, Paliperidone Palmitate: A Breakthrough Treatment for Schizophrenia? A Review on Patient Adherence Levels, Healthcare Resource Utilization and Costs, Neuropsychiatric Disease and Treatment, 10.2147/NDT.S374696, Volume 19, (519-530), (2023).
- Péter Takács, Péter Kunovszki, Valeria Timtschenko, László Fehér, Tamás Balázs, Ramóna Hegyi, Pál Czobor, István Bitter, Comparative Effectiveness of Second Generation Long-acting Injectable Antipsychotics Based on Nationwide Database Research in Hungary: An Update, Schizophrenia Bulletin Open, 10.1093/schizbullopen/sgac013, 3, 1, (2022).
- Chizimuzo T.C. Okoli, Amani Kappi, Tianyi Wang, Andrew Makowski, Andrew T. Cooley, The effect of long‐acting injectable antipsychotic medications compared with oral antipsychotic medications among people with schizophrenia: A systematic review and meta‐analysis, International Journal of Mental Health Nursing, 10.1111/inm.12964, 31, 3, (469-535), (2021).
- Sun Lee, Shaina Schwartz, Adherence and persistence to long-acting injectable dopamine receptor blocking agent therapy in the United States: A systematic review and meta-analysis of cohort studies, Psychiatry Research, 10.1016/j.psychres.2021.114277, 306, (114277), (2021).