Efficacy and metabolic effects of lurasidone versus brexpiprazole in schizophrenia: a network meta-analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To assess the relative efficacy and metabolic effects of lurasidone and brexpiprazole in the acute treatment of schizophrenia. Methods: Five lurasidone and three brexpiprazole trials were identified. In the absence of head-to-head trials, a Bayesian network meta-analysis comparing lurasidone and brexpiprazole was performed. Results: Nonstatistically significant differences in efficacy measures were observed between lurasidone and brexpiprazole. Significant differences favoring lurasidone for weight change (-0.69 kg; 95% CrI: -1.22 to -0.15), total cholesterol (-7.60 mg/dl; 95% CrI: -13.94 to -1.22), and low-density lipoprotein (-6.58 mg/dl; 95% CrI: -12.11 to -1.04) were observed, with a trend indicating half the risk of experiencing ≥7% weight gain. Conclusion: This network meta-analysis suggested that lurasidone had similar efficacy and fewer metabolic effects than brexpiprazole in patients with acute schizophrenia.
The lifetime prevalence of schizophrenia, one of the most debilitating and expensive chronic psychiatric disorders, is 0.5–1.0% [1,2]. Patients with schizophrenia experience incapacitating symptoms such as hallucinations, delusions and disorganized thinking that can compromise normal daily activities [3]. Antipsychotic medications are the first-line treatment of schizophrenia during acute episodes, when the primary goal is to reduce the severity of psychosis and associated symptoms, as well as during the stable phase, when the goals are to maximize functioning and prevent relapses [4,5].
Adherence often remains sub-optimal in schizophrenia due in part to the difficulty of finding a treatment that is both efficacious and tolerable for a given patient [6–8]. Identifying an antipsychotic that balances efficacy and tolerability could improve treatment adherence, thereby lowering the risk of relapse and hospitalization [9]. A large network meta-analysis that incorporated 212 schizophrenia clinical trials and examined 15 different antipsychotics demonstrated that there are small but consistent differences in efficacy, with clozapine appearing to be the most efficacious [10]. However, treatments clearly differed on tolerability attributes, with extrapyramidal symptoms and weight gain being two primary areas of concern [10].
Atypical antipsychotics are generally preferred over typical antipsychotics because of their lower risk for extrapyramidal symptoms [11]. However, some atypicals are associated with negative metabolic changes such as weight gain and adverse changes in cholesterol and triglyceride levels [12]. Weight gain, as well as other metabolic effects, may increase treatment discontinuations. In a large 3-year observational study of 7728 patients with schizophrenia, only 39.7% stayed on their prescribed antipsychotic for the entire study period, and among patients who discontinued their antipsychotic medications, 38.7% discontinued due to lack of efficacy, and 14.2% discontinued due to tolerability issues [13]. In a clinical effectiveness trial, among 1432 patients who received their randomized antipsychotic, only 25.9% stayed on treatment for the full 18-months, with 23.7% discontinuing due to lack of efficacy and 14.9% due to lack of tolerability [6].
Both efficacy and tolerability appear to play an important role in the discontinuation rates for antipsychotics. Patients with schizophrenia are at greater risk of developing diabetes and cardiovascular disease and some atypical antipsychotics appear to increase these risks [14,15]. When examining patient concerns about antipsychotics in a patient preference study, treatment-induced weight gain was the third greatest concern for patients with schizophrenia, after improvement in symptoms and elimination of hyperglycemia [16]. Reducing weight gain and the associated cardiometabolic changes may improve treatment adherence [8] and patient outcomes. Even relatively small differences in treatment adherence have been linked to a lower risk of hospitalization [9].
The National Association of State Mental Health Program Directors recognized that antipsychotics are not interchangeable and recommend including at least one weight-neutral treatment on formulary for those patients with potential metabolic issues [17]. Successful treatment for the majority of patients with schizophrenia involves balancing the benefits and risks of antipsychotics, with clozapine being the last resort treatment for refractory patients [17]. Due to the complexity of successfully managing schizophrenia, an individualized treatment for schizophrenia which is based on the patient’s needs and preference should be considered [17–19].
Two atypical antipsychotics that had a low incidence of weight gain in a large meta-analysis were lurasidone and aripiprazole [10]. Preclinical studies indicate that lurasidone has a high affinity for dopamine receptor D2 and the serotonin receptor 5-HT2A, and little to no affinity for histaminergic receptors [20]. In contrast, preclinical studies indicate that aripiprazole is a partial D2 agonist, with high affinity for 5-HT2A and modest H1 binding [21]. In the meta-analysis, both lurasidone and aripiprazole had a low risk for weight gain, and similar levels of improvement in symptoms, rates of all-cause discontinuation and rates of sedation [10].
Brexpiprazole, approved by the US FDA in 2015, has a similar binding profile to aripiprazole as a partial D2 agonist with moderate histamine binding, but with a higher affinity for serotonin receptor 5-HT2A [22]. In a clinical trial that directly compared aripiprazole and brexpiprazole, both had similar efficacy, similar rates of weight gain reported as an adverse event (aripiprazole 9.4% and brexpiprazole 9.1%), but aripiprazole-treated patients were more likely to have extrapyramidal symptoms (21.2 vs 9.4%) [23]. As aripiprazole and lurasidone have comparable efficacy and weight gain rates, examining if brexpiprazole has similar results when compared with lurasidone would be of interest for patients that are particularly vulnerable to metabolic changes.
Currently, there are no head-to-head clinical trials comparing the efficacy and metabolic parameters of lurasidone and brexpiprazole. Given that both of these antipsychotics appear to be relatively weight neutral atypical antipsychotics, evidence is needed to assist physicians and formulary decision makers in understanding potential differences between them. This study, using a network meta-analysis, summarized the relative efficacy and metabolic effects of lurasidone and brexpiprazole based on acute randomized clinical trials in adults with schizophrenia.
Methods
Literature search & selection
A systematic literature review was conducted using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement, aligned with the Centre for Reviews and Dissemination guide for conducting systematic reviews [24,25], and informed by the Population, Intervention, Comparison, Outcome and Study (PICOS) type framework [26]. Randomized controlled trials that included lurasidone and brexpiprazole (Phase II, III and IV trials) for adult populations (≥18 years old) with schizophrenia were identified. Searches were conducted in MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials and PubMed in November 2015. In addition, proceedings from Schizophrenia International Research Society Conference and the proceedings from the American Psychiatric Association conference were searched from 2013 through the third quarter of 2015. Only articles in English were included. Randomized clinical trials were restricted to those using at least one arm with the FDA-approved doses of lurasidone (40–160 mg/day) or brexpiprazole (2–4 mg/day). The review was restricted to clinical trials assessing the efficacy of the medications in reducing symptoms during acute episodes of schizophrenia. See Supplementary Information for further details on the literature search.
Network meta-analysis
A network meta-analysis of lurasidone and brexpiprazole randomized clinical trials for acute treatment of schizophrenia was conducted using a Bayesian framework in WinBUGS1.4. The framework used guidelines from the National Institute for Health and Care Excellence Decision Support Unit Technical Support Guidance [27]. Using placebo as the common comparator, the analysis compared the efficacy and the tolerability of lurasidone and brexpiprazole. For trials with multiple fixed dose arms, the arms with FDA-approved doses were pooled.
The primary efficacy outcome measure was response rate, defined as ≥20% improvement in Positive and Negative Syndrome Scale (PANSS). Secondary efficacy outcome measures included change from baseline in PANSS and change from baseline in Clinical Global Impressions-Severity Scale (CGI-S) scores. Metabolic outcomes included the proportion with clinically significant weight gain (i.e., ≥7% increase in weight) and changes from baseline in the following parameters: weight, total cholesterol, low-density lipoprotein (LDL), high-density lipoprotein (HDL), and triglycerides.
For continuous outcomes, median difference in change from baseline over 6 weeks was estimated along with the 95% credible interval (CrI). CrIs are the Bayesian equivalent of confidence intervals. For dichotomous outcomes, a logit model estimated the odds ratio (OR) and 95% CrI. Results were considered significant if the 95% CrI did not include zero for continuous outcome variables or one for dichotomous outcome variables.
Following the recommendation of the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) task force [28], a vague prior distribution was used where any parameter value was equally likely. Simulation convergence was evaluated from history, trace plots, and Brooks–Gelman–Rubin convergence statistics model diagnostics from 40,000 iterations with additional iterations used when diagnostics suggested sufficient convergence was not achieved [29,30].
The goodness-of-fit for each model was evaluated using the Deviance Information Criterion (DIC) score, with a lower DIC score indicating a better fitting model. The DIC provides an estimate of model fit that is penalized for increased model complexity [31]. All outcome variables were assessed using both fixed and random effects models. The fixed effects models generally had a better fit and were reported here. Results of the random effect models are available upon request.
Results
Study selection
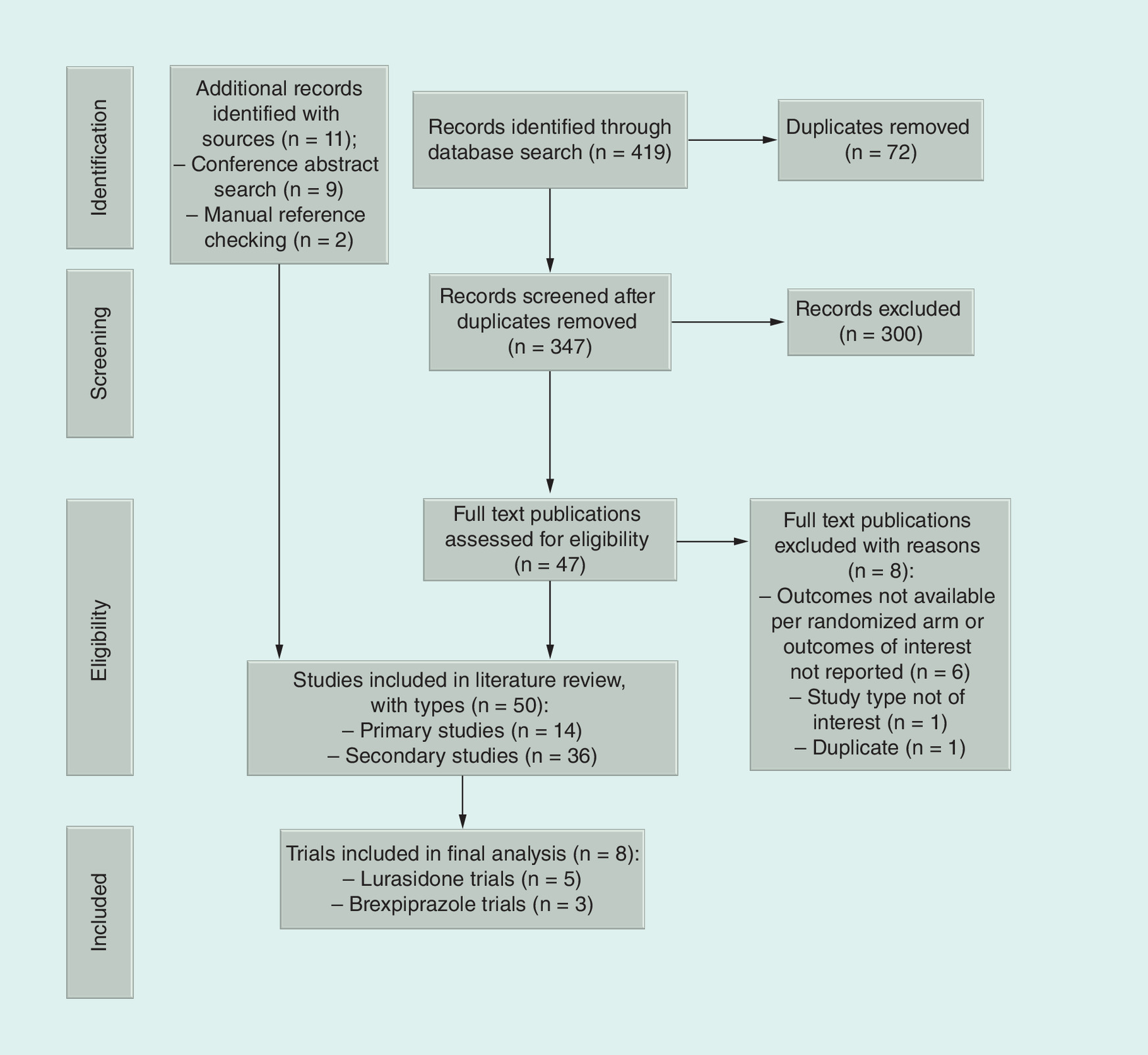
The systematic literature review identified a total of 419 citations. After removing duplicates and abstract screening, 50 publications (full text and conference abstracts) were included. Of these, 14 were primary publications (10 lurasidone and four brexpiprazole). Figure 1 summarizes the selection and review process.
Within the ten lurasidone trials, six trials assessed outcomes for acute schizophrenia [32–37]. Four other lurasidone trials [38–41] were excluded from the review because they included only stable patients. One acute trial for lurasidone, OPTIMIZE [36], was subsequently excluded from the analysis due to its unique study design which involved a nested randomization of patients not having an early response to a higher dose of lurasidone.
Within the brexpiprazole trials, three trials assessing acute episodes of schizophrenia [23,42,43] were included and one trial [44] was excluded from the review as it was in stable patients. Among the 14 primary lurasidone and brexpiprazole publications, eight trials met all the selection criteria: five for lurasidone [32–35,37] and three for brexpiprazole [23,42,43].
Trial heterogeneity
Trial heterogeneity for every treatment arm using an FDA-approved dose was assessed by examining distribution of the trial baseline characteristics. These characteristics were plotted by drug to assess whether suitably comparable patients were included across the trials available for pooling.
Table 1 presents the baseline characteristics across trials, with weighted averages for the fixed-dose trials that had multiple treatment arms. All eight studies had reasonably comparable baseline characteristics and appeared appropriate to include in the network meta-analysis: mean age ranged from 37.0 to 42.2 years, percent of females ranged from 16.0 to 38.7%, mean age of symptom onset ranged from 23.3 to 27.4, mean BMI ranged from 25.7 to 31.2, mean PANSS ranged from 91.2 to 97.2, and mean CGI-S ranged from 4.8 to 5.0. Table 2 gives the outcome measures from each trial at the end of 6 weeks. Not all trials measured all variables. The relative homogeneity of patients and outcomes across the trials, along with the DIC values, appeared consistent with fixed effects model assumptions.
| Baseline variables | Lurasidone schizophrenia trials | Brexpiprazole schizophrenia trials | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Nakamura | Meltzer | Loebel | Ogasa | Nasrallah | Correll | Kane | Citrome | ||||||||
| LUR | PBO | LUR | PBO | LUR | PBO | LUR | PBO | LUR | PBO | BRE | PBO | BRE | PBO | BRE | |
| Age (years) | 39.7 | 41.9 | 37.8 | 37.0 | 37.0 | 37.4 | 40.4 | 38.1 | - | - | 40.2 | 39.7 | 37.7 | 39.3 | 42.2 |
| Female gender | 24.4 | 22.2 | 21.5 | 23.0 | 27.4 | 36.0 | 27.3 | 16.0 | 31.5 | 27.4 | 38.7 | 35.9 | 36.5 | 39.7 | 28.1 |
| BMI (kg/m2) | 30.7 | 31.2 | 25.9 | 25.8 | 25.7 | 26.1 | 29.5 | 29.4 | 26.6 | 26.9 | 27.2 | 26.5 | 26.7 | 26.6 | - |
| Age at onset (years) | -† | - | 23.3 | 23.9 | 25.1 | 25.5 | - | - | 24.6 | 24.2 | 27.3 | 27.4 | 25.3 | 25.6 | 25.6 |
| PANSS | 94.4 | 96.0 | 97.2 | 95.8 | 97.6 | 96.6 | 91.2 | 93.3 | 96.2 | 96.8 | 95.4 | 95.9 | 95.7 | 94.8 | 94.1 |
| CGI-S | 4.8 | 4.8 | 5.0 | 4.9 | 5.0 | 4.9 | 4.8 | 4.6 | 4.9 | 4.9 | 4.9 | 4.8 | 5.0 | 4.9 | 5.0 |
Numbers represent means across trial arms. The Citrome et al. trial had patients randomized to either brexpiprazole or aripiprazole. Trials are identified in the table based on the primary authors name. The associated references are as follows: Nakamura [33], Meltzer [35], Loebel [37], Ogasa [32], Nasrallah [34], Correll [42], Kane [43], and Citrome [23].
†- indicates no data available.
BRE: Brexpiprazole; CGI-S: Clinical Global Impressions – Severity; LUR: Lurasidone; PANSS: Positive and Negative Syndrome Scale; PBO: Placebo.
| Outcome variables | Lurasidone schizophrenia trials | Brexpiprazole schizophrenia trials | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Nakamura | Meltzer | Loebel | Ogasa | Nasrallah | Correll | Kane | Citrome | ||||||||
| LUR | PBO | LUR | PBO | LUR | PBO | LUR | PBO | LUR | PBO | BRE | PBO | BRE | PBO | BRE | |
| Response rate | 44.4 | 26.7 | -† | 49.0 | - | - | 48.0 | 18.3 | 63.2 | 54.0 | 53.0 | 34.8 | 49.2 | 40.0 | 39.0 |
| PANSS | -14.1 | -5.5 | -24.7 | -16.0 | -24.3 | -10.3 | -15.5 | -6.2 | -21.0 | -17.0 | -20.2 | -12.0 | -18.3 | -13.5 | -22.9 |
| CGI-S | -0.6 | -0.2 | -1.5 | -1.1 | -1.6 | -0.9 | -0.8 | -0.1 | -1.2 | -1.0 | -1.2 | -0.8 | -1.1 | -0.8 | - |
| Weight change (kg) | 0.9 | 0.5 | 1.0 | 0.6 | 0.6 | 0.1 | 0.3 | 0.0 | 0.9 | 0.3 | 1.4 | 0.4 | 1.7 | 0.4 | 4.3 |
| Clinically significant weight gain (≥7%) | 6.7 | 7.8 | 5.9 | 7.0 | 4.3 | 2.6 | - | - | 8.2 | 3.2 | 8.9 | 4.4 | 11.8 | 3.9 | - |
| Total cholesterol (mg/dl) | -10.1 | -7.1 | -8.0 | -6.8 | - | - | - | - | - | - | 2.4 | -3.1 | 2.8 | -3.4 | -3.0 |
| LDL (mg/dl) | -5.2 | -0.7 | -4.8 | -1.8 | - | - | - | - | - | - | 0.9 | -2.1 | 1.8 | -1.5 | 0.8 |
| HDL (mg/dl) | -1.2 | -3.0 | -0.7 | -1.2 | - | - | - | - | - | - | 0.9 | -1.2 | 1.1 | -2.4 | -4.6 |
| Triglycerides (mg/dl) | -24.4 | -31.7 | -6.7 | 0.1 | - | - | - | - | - | - | 3.3 | -0.8 | -3.1 | 1.5 | 3.9 |
Numbers represent averages across trial arms. The Citrome et al. trial had patients randomized to either brexpiprazole or aripiprazole. Response was defined as a ≥20% improvement in PANSS. Trials are identified in the table based on the primary authors name. The associated references are as follows: Nakamura [33], Meltzer [35], Loebel [37], Ogasa [32], Nasrallah [34], Correll [42], Kane [43], and Citrome [23].
†- indicates no data available.
BRE: Brexpiprazole; CGI-S: Clinical Global Impressions – Severity; HDL: High-density lipoprotein; LDL: Low-density lipoprotein; LUR: Lurasidone; PANSS: Positive and Negative Syndrome Scale; PBO: Placebo.
Network meta-analysis results
Forest plots of results for efficacy and metabolic measures are presented in Figures 2 & 3, respectively. For the efficacy variables, there were no significant differences based on the 95% CrIs. Although not statistically significant, lurasidone was associated with a higher likelihood of treatment response (OR: 1.28; 95% CrI: 0.88–1.87) and greater improvements (median changes) for both PANSS (-2.48; CrI: -6.39–1.46) and CGI-S (-0.14; 95% CrI: -0.35–0.07) than brexpiprazole (Figure 2).
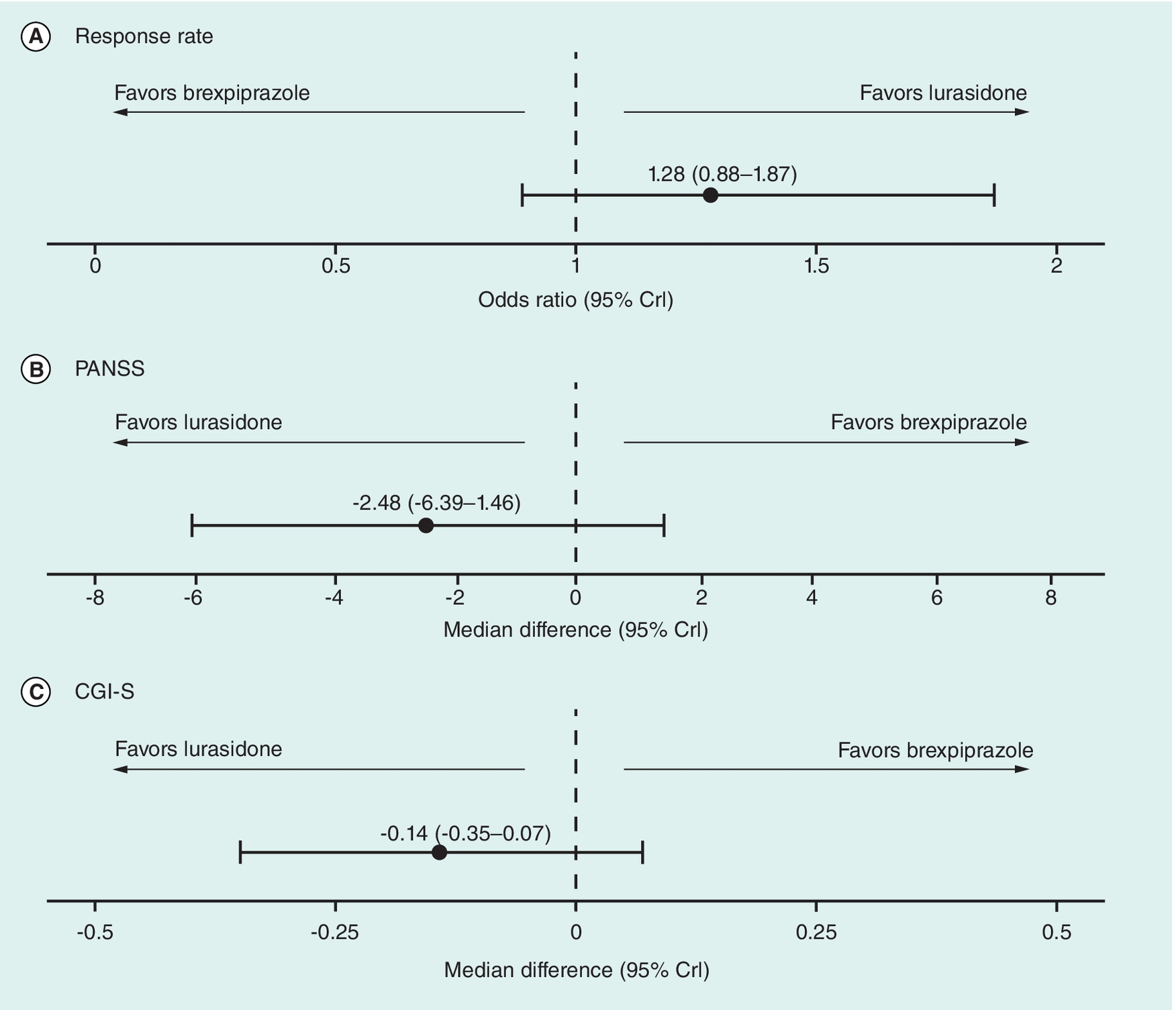
Figure 2. Forest plots comparing lurasidone with brexpiprazole on efficacy measures: results of the network meta-analysis.
Data were from the fixed effect models. Error bars represent the 95% CrI. Response was defined as a ≥20% improvement in PANSS.
CrI: Credible interval; CGI-S: Clinical Global Impressions – Severity; PANSS: Positive and Negative Syndrome Scale.
The fixed effects models showed significant differences in metabolic outcomes favoring lurasidone for less weight gain (-0.69 kg; 95% CrI -1.22 to -0.15), total cholesterol (-7.60 mg/dl; 95% CrI: -13.94 to -1.22) and LDL (-6.58 mg/dl; 95% CrI: -12.11 to -1.04). There was also a nonsignificant trend showing lurasidone patients were half as likely to experience clinically significant (≥7%) weight gain (OR: 0.50; 95% CrI: 0.22–1.07) (Figure 3). Both fixed and random effects models produced directionally similar estimates for all efficacy and metabolic outcomes, with random effects model yielding wider CrIs for the estimates that were not statistically significant.
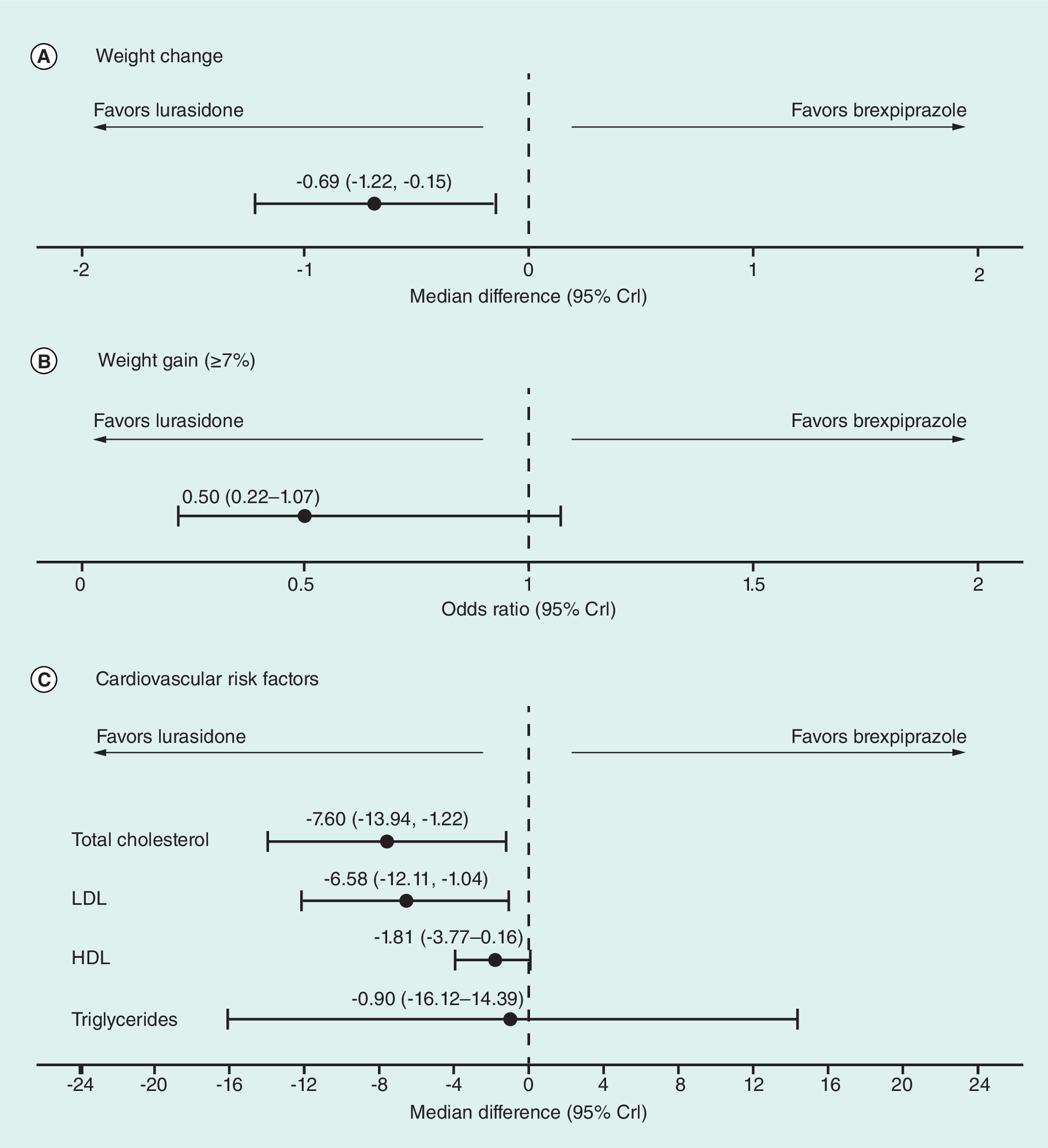
Figure 3. Forest plots comparing lurasidone and brexpiprazole on metabolic measures: results of the network meta-analysis.
Error bars represent the 95% CrI. Cholesterol and triglycerides were measured in mg/dl. Lower OR on clinically significant weight gain (≥7%) indicate a lower risk for lurasidone than brexpiprazole. Negative median differences on weight change and cardiovascular risk factors indicate greater reductions for lurasidone than brexpiprazole.
CrI: Credible interval; HDL: High-density lipoprotein; LDL: Low-density lipoprotein; OR: Odd ratio.
Discussion
The results from this network meta-analysis indicate that lurasidone was associated with similar improvements in efficacy compared with brexpiprazole. However, the results also demonstrated that lurasidone was associated with significantly lower weight gain compared with brexpiprazole, with an average difference of -0.69 kg, after 6 weeks. Longer-term head-to-head trials are needed to estimate potential differences in long-term weight change and clinical implications and relevance of this finding.
Brexpiprazole is a partial D2 agonist with a similar molecular structure [22] and clinical profile to aripiprazole [23]. When lurasidone and aripiprazole were compared in an earlier network meta-analysis, efficacy was similar, but lurasidone was associated with a nonsignificant greater reduction in weight gain [10]. Although variability in efficacy across atypical antipsychotics is generally low with the possible exception of clozapine, there are significant differences in tolerability [10]. Comparisons between lurasidone and brexpiprazole in the current network meta-analysis were largely consistent with these earlier findings comparing lurasidone and aripiprazole: similar efficacy, but with lurasidone associated with significantly less weight gain than brexpiprazole.
As most atypical antipsychotics are associated with weight gain [45], the National Association of State Mental Health Program Directors recommended that patients have access to at least one weight-neutral prescribing option [17]. Studies with lurasidone have consistently indicated a potentially more favorable weight gain profile compared with other antipsychotics. In a pooled analysis of six lurasidone clinical trials in schizophrenia that were at least 12-months in length, lurasidone-treated patients had lower rates of clinically significant weight gain compared with patients treated with risperidone or quetiapine [46]. Similarly, in usual clinical care, a study of electronic medical records found that the patients who gained weight on their previous antipsychotic subsequently lost weight after switching to lurasidone [47].
Reducing weight gain may help prevent cardiovascular disease [14] and reduce negative cardiometabolic changes such as increased cholesterol levels and glucose levels [48]. Some atypical antipsychotics appear to increase the risk of developing diabetes and cardiovascular disease in patients with schizophrenia [14,15]. This analysis found that lurasidone was associated with significantly greater reductions in total cholesterol and LDL levels compared with patients treated with brexpiprazole. Prior research suggests that a relatively modest weight loss (i.e., 5%) may lead to improvement in cardiometabolic parameters [49]. Treatment adherence may be improved by minimizing weight gain and potentially improving cardiometabolic measures [8] and patient outcomes. The findings of reduced weight gain and improvements in cardiometabolic parameters with the use of lurasidone instead of brexpiprazole corroborate this previous research about the potential relationship between weight gain and cardiometabolic disease. A prescribing option with reasonable efficacy that does not significantly increase the risk of developing or exacerbating common metabolic disorders in the patients with schizophrenia could be particularly helpful for this patient population.
Limitations
Given that brexpiprazole is a recently approved atypical antipsychotic, a systematic literature search identified only three brexpiprazole randomized clinical trials that were suitable for inclusion in the network meta-analysis. The majority (12/13) of randomized clinical trials were designed and statistically powered to compare the treatment to the placebo, not for head-to-head comparisons in a network meta-analysis. The analysis only included randomized clinical trials, which have rigorous patient selection and study oversight, further observational research is needed to verify the findings generalize to real-world settings. The lack of statistical significance in some of the analyses does not indicate that meaningful differences do not exist, only that there was insufficient statistical power to identify the differences. The clinical relevance of weight difference and changes in cholesterol over a longer-time period remain unclear and need further study. Although glucose was not analyzed in this study, if differences exist they most likely would not have manifested in the 6-week-time period.
This network meta-analysis did not include a 6-week, double-blind, placebo- and haloperidol-controlled Phase II study of lurasidone that failed to demonstrate statistically significant improvement in the primary and secondary efficacy measures, Brief Psychiatric Rating Scale (BPRS) and PANSS, respectively for either lurasidone or haloperidol [50]. Thus, it is not clear if inclusion of the study in this analysis may have affected the study results.
As more data are gathered over time, especially head-to-head randomized trials directly comparing lurasidone and brexpiprazole, other important differences may emerge. Although the populations of included trials were comparable with respect to reported patient characteristics, potential differences in other unreported baseline characteristics could have influenced the results reported in this analysis.
Conclusion
This network meta-analysis suggests that lurasidone has comparable efficacy to brexpiprazole along with less weight gain and greater reductions in total cholesterol and LDL compared with brexpiprazole. These metabolic differences may be important with respect to overall health outcomes. Head-to-head effectiveness studies comparing the relative efficacy and tolerability of lurasidone and brexpiprazole in patients with acute episodes of schizophrenia are warranted.
Background
•
Schizophrenia is challenging to treat and the exact etiology remains unknown. Atypical antipsychotics are the treatment of choice. Although the efficacy of different atypical antipsychotics appears similar, they differ in tolerability most likely due to different neurological binding profiles.
•
Two of the newer treatment choices for schizophrenia were compared: lurasidone and brexpiprazole.
•
This is the first time these treatments have been compared, by using a network meta-analysis.
Methods
•
An extensive literature search was preformed using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) approach.
•
Five lurasidone trials and three brexpiprazole trials met the inclusion criteria. A network meta-analysis compared the two treatments on efficacy and metabolic outcomes. For efficacy, response rate, Positive and Negative Syndrome Scale, and Clinical Global Impressions – Severity score were examined. Metabolic measures were weight change, total cholesterol, low-density lipoprotein, high-density lipoprotein and triglycerides.
Results
•
The network meta-analysis found that lurasidone and brexpiprazole had similar efficacy, with the nonsignificant improvements in efficacy consistently favoring lurasidone.
•
Significant benefits for lurasidone on weight gain, total cholesterol and low-density lipoprotein were observed.
Conclusion
•
Lurasidone appears to have a better metabolic profile when compared with brexpiprazole.
•
These metabolic differences may be important with respect to overall health outcomes.
•
The ability to identify significant differences may have been limited by the small number of trials available for inclusion in the network meta-analysis.
Financial & competing interests disclosure
D Ng-Mak, K Rajagopalan and A Loebel are employees of Sunovion Pharmaceuticals, Inc. V Tongbram and K Ndirangu are employees of ICON Health Economics, who served as paid consultants to Sunovion Pharmaceuticals, Inc. for the development and publication of this study. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Technical writing support was provided by MD Stensland, and GF Elphick, Agile Outcomes Research, Inc. and was funded by Sunovion Pharmaceuticals, Inc.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementaryinformation.docx)
- Download
- 26.28 KB
References
Papers of special note have been highlighted as: • of interest
1.
Saha S, Chant D, Welham J, McGrath J. A systematic review of the prevalence of schizophrenia. PLoS Med. 2(5), e141 (2005).
2.
van Os J, Kapur S. Schizophrenia. Lancet 374(9690), 635–645 (2009).
3.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (5th Edition). American Psychiatric Publishing, Washington, DC, USA (2013).
4.
Hasan A, Falkai P, Wobrock T et al. World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines for Biological Treatment of Schizophrenia, part 1: update 2012 on the acute treatment of schizophrenia and the management of treatment resistance. World J. Biol. Psychiatry 13(5), 318–378 (2012).
5.
Hasan A, Falkai P, Wobrock T et al. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for biological treatment of schizophrenia, part 2: update 2012 on the long-term treatment of schizophrenia and management of antipsychotic-induced side effects. World J. Biol. Psychiatry 14(1), 2–44 (2013).
6.
Lieberman JA, Stroup TS, McEvoy JP et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N. Engl. J. Med. 353(12), 1209–1223 (2005).
7.
Markowitz M, Karve S, Panish J, Candrilli SD, Alphs L. Antipsychotic adherence patterns and health care utilization and costs among patients discharged after a schizophrenia-related hospitalization. BMC Psychiatry 13, 246 (2013).
8.
Velligan DI, Weiden PJ, Sajatovic M et al. The expert consensus guideline series: adherence problems in patients with serious and persistent mental illness. J. Clin. Psychiatry 70(Suppl. 4), 1–46 (2009).
9.
Weiden PJ, Kozma C, Grogg A, Locklear J. Partial compliance and risk of rehospitalization among California medicaid patients with schizophrenia. Psychiatr. Serv. 55(8), 886–891 (2004).
10.
Leucht S, Cipriani A, Spineli L et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis. Lancet 382(9896), 951–962 (2013).
11.
Rummel-Kluge C, Komossa K, Schwarz S et al. Second-generation antipsychotic drugs and extrapyramidal side effects: a systematic review and meta-analysis of head-to-head comparisons. Schizophr. Bull. 38(1), 167–177 (2012).
12.
Nasrallah HA. Atypical antipsychotic-induced metabolic side effects: insights from receptor-binding profiles. Mol. Psychiatry 13(1), 27–35 (2007).
13.
Haro JM, Suarez D, Novick D, Brown J, Usall J, Naber D. Three-year antipsychotic effectiveness in the outpatient care of schizophrenia: observational versus randomized studies results. Eur. Neuropsychopharmacol. 17(4), 235–244 (2007).
14.
Graham KA, Cho H, Brownley KA, Harp JB. Early treatment-related changed in diabetes and cardiovascular disease risk markers in first episode psychosis subjects. Schizophr. Res. 101(1–3), 287–294 (2008).
15.
American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists, North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. J. Clin. Psychiatry 65(2), 267–272 (2004).
16.
Levitan B, Markowitz M, Mohamed AF et al. Patients' preferences related to benefits, risks, and formulations of schizophrenia treatment. Psychiatr. Serv. 66(7), 719–726 (2015).
17.
Parks J, Radke A, Parker G et al. Principles of antipsychotic prescribing for policy makers, circa 2008. Translating knowledge to promote individualized treatment. Schizophr. Bull. 35(5), 931–936 (2008).
18.
Godman B, De Bruyn K, Miranda J, Raschi E, Bennie M, Barbui C, Simoens S. Generic atypical antipsychotic drugs in Belgium: their influence and implications. J. Comp. Eff. Res. 2(6), 551–561 (2013).
19.
Godman B, Petzold M, Bennett K et al. Can authorities appreciably enhance the prescribing of oral generic risperidone to conserve resources? Findings from across Europe and their implications. BMC Med. 12, 98 (2014).
20.
Ishibashi T, Horisawa T, Tokuda K et al. Pharmacological profile of lurasidone, a novel antipsychotic agent with potent 5-hydroxytryptamine 7 (5-HT7) and 5-HT1A receptor activity. J. Pharmacol. Exp. Ther. 334(1), 171–181 (2010).
21.
Shapiro DA, Renock S, Arrington E et al. Aripiprazole, a novel atypical antipsychotic drug with a unique and robust pharmacology. Neuropsychopharmacology 28(8), 1400–1411 (2003).
22.
Das S, Barnwal P, Winston AB, Mondal S, Saha I. Brexpiprazole: so far so good. Ther. Adv. Psychopharmacol. 6(1), 39–54 (2016).
23.
Citrome L, Ota A, Nagamizu K, Perry P, Weiller E, Baker RA. The effect of brexpiprazole (OPC-34712) and aripiprazole in adult patients with acute schizophrenia: results from a randomized, exploratory study. Int. Clin. Psychopharmacol. 31(4), 192–201 (2016).
• This is a brexpiprazole clinical trial used for this network meta-analysis.
24.
Centre for Reviews Dissemination. Systematic reviews: CRD's guidance for undertaking reviews in health care. (2009). www.york.ac.uk/media/crd/Systematic_Reviews.pdf
25.
Moher D, Liberati A, Tetzlaff J, Altman D, The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int. J. Surg. 8(5), 336–341 (2010).
26.
Schardt C, Adams MB, Owens T, Keitz S, Fontelo P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 7, 16 (2007).
27.
Dias S, Welton NJ, Sutton AJ, Ades AE. NICE DSU technical support document 2: a generalised linear modelling framework for pairwise and network meta-analysis of randomised controlled trials. National Institute for Health and Clinical Excellence (2011). www.ncbi.nlm.nih.gov/pubmedhealth/PMH0088912/pdf/PubMedHealth_PMH0088912.pdf
28.
Hoaglin DC, Hawkins N, Janse JP et al. Conducting indirect-treatment-comparison and network-meta-analysis studies; report of the ISPOR task force on indirect treatment comparisons good research practices: part 2. Value Health 14, 429–437 (2011).
29.
Welton NJ, Sutton AJ, Cooper NJ, Abrams KR, Ades AE. Evidence Synthesis for Decision Making in Healthcare. John Wiley and Sons, Ltd, Hoboken, NJ, USA (2012).
30.
Lunn DJ, Thomas A, Best N, Spiegelhalter D. Winbugs – a Baysesian modelling framework: concepts, structure, and extensibility. Stat. Comput. 10, 325–337 (2000).
31.
Spiegelhalter DJ, Best NG, Carlin BP, Van Der Linde A. Bayesian measures of model complexity and fit. J. R. Stat. Soc. Ser. B Stat. Methodol. 64(4), 583–639 (2002).
32.
Ogasa M, Kimura T, Nakamura M, Guarino J. Lurasidone in the treatment of schizophrenia: a 6-week, placebo-controlled study. Psychopharmacology (Berl.). 225(3), 519–530 (2013).
• This is a lurasidone clinical trial used for this network meta-analysis.
33.
Nakamura M, Ogasa M, Guarino J et al. Lurasidone in the treatment of acute schizophrenia: a double-blind, placebo-controlled trial. J. Clin. Psychiatry 70(6), 829–836 (2009).
• This is a lurasidone clinical trial used for this network meta-analysis.
34.
Nasrallah HA, Silva R, Phillips D et al. Lurasidone for the treatment of acutely psychotic patients with schizophrenia: a 6-week, randomized, placebo-controlled study. J. Psychiatr. Res. 47(5), 670–677 (2013).
• This is a lurasidone clinical trial used for this network meta-analysis.
35.
Meltzer HY, Cucchiaro J, Silva R et al. Lurasidone in the treatment of schizophrenia: a randomized, double-blind, placebo- and olanzapine-controlled study. Am. J. Psychiatry 168(9), 957–967 (2011).
• This is a lurasidone clinical trial used for this network meta-analysis.
36.
Loebel A, Citrome L, Correll CU, Xu J, Cucchiaro J, Kane JM. Treatment of early non-response in patients with schizophrenia: assessing the efficacy of antipsychotic dose escalation. BMC Psychiatry 15, 271 (2015).
37.
Loebel A, Cucchiaro J, Sarma K et al. Efficacy and safety of lurasidone 80 mg/day and 160 mg/day in the treatment of schizophrenia: a randomized, double-blind, placebo- and active-controlled trial. Schizophr. Res. 145(1–3), 101–109 (2013).
• This is a lurasidone clinical trial used for this network meta-analysis.
38.
Citrome L, Cucchiaro J, Sarma K et al. Long-term safety and tolerability of lurasidone in schizophrenia: a 12-month, double-blind, active-controlled study. Int. Clin. Psychopharmacol. 27(3), 165–176 (2012).
39.
Harvey PD, Ogasa M, Cucchiaro J, Loebel A, Keefe RSE. Performance and interview-based assessments of cognitive change in a randomized, double-blind comparison of lurasidone vs. ziprasidone. Schizophr. Res. 127(1–3), 188–194 (2011).
40.
Tandon R, Cucchiaro J, Phillips D et al. A double-blind, placebo-controlled, randomized withdrawal study of lurasidone for the maintenance of efficacy in patients with schizophrenia. J. Psychopharmacol. 30(1), 69–77 (2016).
41.
McEvoy JP, Citrome L, Hernandez D et al. Effectiveness of lurasidone in patients with schizophrenia or schizoaffective disorder switched from other antipsychotics: a randomized, 6-week, open-label study. J. Clin. Psychiatry 74(2), 170–179 (2013).
42.
Correll CU, Skuban A, Ouyang J et al. Efficacy and safety of brexpiprazole for the treatment of acute schizophrenia: a 6-week randomized, double-blind, placebo-controlled trial. Am. J. Psychiatry 172(9), 870–880 (2015).
• This is a brexpiprazole clinical trial used for this network meta-analysis.
43.
Kane JM, Skuban A, Ouyang J et al. A multicenter, randomized, double-blind, controlled Phase III trial of fixed-dose brexpiprazole for the treatment of adults with acute schizophrenia. Schizophr. Res. 164(1–3), 127–135 (2015).
• This is a brexpiprazole clinical trial used for this network meta-analysis.
44.
Fleischhacker WW, Hobart M, Ouyang J et al. Efficacy and safety of brexpiprazole (OPC-34712) as maintenance treatment in adults with schizophrenia: a randomized, double-blind, placebo-controlled study. Int. J. Neuropsychopharmacol. 20(1), 11–21 (2017).
45.
Newcomer JW. Metabolic considerations in the use of antipsychotic medications: a review of recent evidence. J. Clin. Psychiatry 68(Suppl. 1), 20–27 (2007).
46.
Meyer JM, Mao Y, Pikalov A, Cucchiaro J, Loebel A. Weight change during long-term treatment with lurasidone: pooled analysis of studies in patients with schizophrenia. Int. Clin. Psychopharmacol. 30(6), 342–350 (2015).
47.
Meyer JM, Ng-Mak DS, Chuang C-C, Rajagopalan K, Loebel A. Weight changes before and after lurasidone treatment: a real-world analysis using electronic health records. Ann. Gen. Psychiatry 16, 36 (2017).
48.
De Hert M, Yu W, Detraux J, Sweers K, van Winkel R, Correll CU. Body weight and metabolic adverse effects of asenapine, iloperidone, lurasidone and paliperidone in the treatment of schizophrenia and bipolar disorder. CNS Drugs 26(9), 733–759 (2012).
49.
Blackburn G. Effect of degree of weight loss on health benefits. Obes. Res. 3(Suppl. 2), S211–S216 (1995).
50.
Potkin SG, Kimura T, Guarino J. A 6-week, double-blind, placebo- and haloperidol-controlled, Phase II study of lurasidone in patients with acute schizophrenia. Ther. Adv. Psychopharmacol. 5(6), 322–331 (2015).
Information & Authors
Information
Published In
Pages: 737 - 748
PubMed: 29697278
Copyright
© 2018 Sunovion Pharmaceuticals Inc.
History
Received: 15 February 2018
Accepted: 12 April 2018
Published online: 26 April 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Efficacy and metabolic effects of lurasidone versus brexpiprazole in schizophrenia: a network meta-analysis. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0016
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Srinivas Kamath, Alexander Hunter, Kate Collins, Anthony Wignall, Paul Joyce, The atypical antipsychotics lurasidone and olanzapine exert contrasting effects on the gut microbiome and metabolic function of rats, British Journal of Pharmacology, 10.1111/bph.16507, 181, 22, (4531-4545), (2024).
- Valerio Ricci, Domenico De Berardis, Giuseppe Maina, Third-Generation Antipsychotics and Lurasidone in the Treatment of Substance-Induced Psychoses: A Narrative Review, Healthcare, 10.3390/healthcare12030339, 12, 3, (339), (2024).
- Mehak Pahwa, Ahmad Sleem, Omar H. Elsayed, Megan Elizabeth Good, Rif S. El-Mallakh, New Antipsychotic Medications in the Last Decade, Current Psychiatry Reports, 10.1007/s11920-021-01298-w, 23, 12, (2021).
- Shih-Ku Lin, Chin-Bin Yeh, Katsuhiko Hagi, Lurasidone Switching in Patients with Schizophrenia Who Showed Suboptimal Effect and/or Intolerability to Current Antipsychotics, Taiwanese Journal of Psychiatry, 10.4103/TPSY.TPSY_26_21, 35, 3, (132-139), (2021).
- Benjamin Kearns, Katy Cooper, Anna Cantrell, Chloe Thomas, Schizophrenia Treatment with Second-Generation Antipsychotics: A Multi-Country Comparison of the Costs of Cardiovascular and Metabolic Adverse Events and Weight Gain, Neuropsychiatric Disease and Treatment, 10.2147/NDT.S282856, Volume 17, (125-137), (2021).
- Lauren Stummer, Marija Markovic, Megan Maroney, Brexpiprazole in the Treatment of Schizophrenia and Agitation in Alzheimer’s Disease, Neurodegenerative Disease Management, 10.2217/nmt-2020-0013, 10, 4, (205-217), (2020).
- Yuan Feng, Jianguo Shi, Lili Wang, Xia Zhang, Yunlong Tan, Jingyuan Zhao, Yuping Ning, Shiping Xie, Xuejun Liu, Qi Liu, Keqing Li, Xiaoliang Wang, Lehua Li, Xiufeng Xu, Wei Deng, Xiaoyan Luo, Gang Wang, Randomized, double‐blind, 6‐week non‐inferiority study of lurasidone and risperidone for the treatment of schizophrenia, Psychiatry and Clinical Neurosciences, 10.1111/pcn.12965, 74, 6, (336-343), (2020).
- Filippo Corponi, Chiara Fabbri, Istvan Bitter, Stuart Montgomery, Eduard Vieta, Siegfried Kasper, Stefano Pallanti, Alessandro Serretti, Novel antipsychotics specificity profile: A clinically oriented review of lurasidone, brexpiprazole, cariprazine and lumateperone, European Neuropsychopharmacology, 10.1016/j.euroneuro.2019.06.008, 29, 9, (971-985), (2019).
- James E. Frampton, Brexpiprazole: A Review in Schizophrenia, Drugs, 10.1007/s40265-019-1052-5, 79, 2, (189-200), (2019).