Costs of subcutaneous and intravenous administration of trastuzumab for patients with HER2-positive breast cancer
Abstract
Aim: Trastuzumab is available in an intravenous (iv.) and a subcutaneous (sc.) formulation. The objective of this study was to estimate the costs of administration of iv. and sc. trastuzumab treatment. Materials & methods: Via interviews, we identified all the activities associated with iv. and sc. administration. The outcome was time estimates. To estimate the administration costs, the time estimates were valued by average gross wages. Results: The iv. administration takes longer time as infusion time is longer (25 or 85 min). The iv. administration is associated with higher cost for 17 cycles; €971 (€1858 vs €887). Conclusion: sc. administration is associated with lower administration costs. Switching patients from iv. to sc. would make it possible to treat more patients without increasing the personnel resources.
Research into cancer treatment continues with the aim of improving outcomes. New, innovative medicines (e.g., biologics) have bettered the prognosis as improved overall survival and improved progression free survival are experienced for many cancer patients [1].
Most oncology medicines are administered intravenously (iv.). However, some therapies can also be administered subcutaneously (sc.) which is more convenient and faster. Healthcare resources, as well as other resources associated with the patients, are limited, among others, implying a continuous focus on efficient treatment modes and monitoring. If possible, intuitively sc. administration should be preferred to iv. administration as sc. administration is faster and requires fewer resources.
Trastuzumab (Herceptin®) is available in an iv. formulation and an sc. formulation. Trastuzumab, as monotherapy or in combination with paclitaxel, docetaxel or carboplatin, is indicated for treatment of patients with HER2-positive breast cancer [2].
Trastuzumab is given every 3 weeks as neoadjuvant (prior to surgery) and adjuvant (after surgery) to patients with early breast cancer and as palliative treatment for patients with metastatic breast cancer. One year of trastuzumab treatment is the standard of care in the adjuvant setting, and the adjuvant setting is the focus of the comparison in manuscript.
Clinical trials have proven that the treatment effect and safety of trastuzumab is the same for iv. and sc. administration [3,4]. For the iv. formulation, infusion time is 90 min the first time and 30 min in the subsequent cycles. Injection time for the sc. formulation is 2–5 min [2]. In addition, the sc. formulation does not require drug preparation (fixed dose of 600 mg) apart from syringe preparation.
In Denmark, breast cancer is the most frequent cancer for women, and approximately 4800 are diagnosed every year [1]. Approximately 13% of all cases are HER2-positive [5]. Both administration forms, iv. and sc., are used in Denmark, but the trastuzumab administration practice and organization vary between oncology departments.
On average, the drug costs of the iv. (dose depending on body weight) and sc. (fixed dose) formulation are the same implying that knowledge about nondrug cost levels (i.e., administration costs) may be important in ensuring an efficient treatment mode.
It was the objective of this study to estimate the costs of the administration of iv. and sc. trastuzumab treatment, respectively, for patients with HER2-positive breast cancer from a healthcare and patient perspective.
Methods
Data on resource use
In Denmark, 12 oncology departments are treating HER2-positive breast cancer patients. Seven departments are located at regional hospitals and five at university hospitals. Data input on resource use were based on interviews in oncology departments with medical specialists and nurses and at hospital pharmacies with pharmacists and laboratory technicians.
Initially, we listed all the patient-related activities and tasks associated with the iv. and sc. administration of trastuzumab, respectively. Based on this list, we drafted an interview guide including questions covering all activities, tasks and time consumption associated with these activities and tasks. The interview guide also included questions regarding the usage of utensils related to iv. and sc. administration, respectively.
We pilot tested this interview guide at the department of oncology at Rigshospitalet in Copenhagen where we interviewed a nurse with comprehensive experience with trastuzumab treatment.
Based on this pilot interview, we adjusted the interview guide and subsequently additional interviews were performed in other oncology departments and at hospital pharmacies. The interviews at the pharmacies had a different focus as these interviews concentrated on the resources used at the pharmacies related to the preparation of trastuzumab (iv. and sc., respectively).
Costs
The main outcome of the interviews was estimates of the time consumptions associated with the specific patient-related activities and tasks in the oncology departments and at hospital pharmacies, respectively. The interviewees’ information about estimates of time consumption (including minimum and maximum estimates) was organized in input tables categorized by activity and profession (medical specialist, nurse, secretary, pharmacist and laboratory technician).
| Personnel | Mean time consumption (min) | Minimum time consumption (min) | Maximum time consumption (min) |
|---|---|---|---|
| sc. | |||
| Secretary | 1 | 1 | 3 |
| Nurse | 16 | 13 | 21 |
| Medical specialist | 2 | 1 | 3 |
| Pharmacist | 3 | 2 | 4 |
| Laboratory technician | 9 | 8 | 10 |
| Hospital porter | 5 | 2 | 8 |
| Patient: | |||
| Direct contact with nurse | 13 | 10 | 19 |
| Waiting time | 0 | 0 | 0 |
| Observation time: | |||
| – First cycle | 360 | 360 | 360 |
| – Second cycle | 93 | 93 | 94 |
| – Third cycle | 66 | 66 | 66 |
| – Subsequent cycles | 0 | 0 | 0 |
| iv. | |||
| Secretary | 1 | 1 | 3 |
| Nurse: | |||
| – First cycle | 66 | 62 | 72 |
| – Second cycle | 36 | 32 | 42 |
| – Third cycle | 36 | 32 | 42 |
| – Subsequent cycles | 26 | 22 | 30 |
| Medical specialist | 1 | 1 | 1 |
| Pharmacist | 3 | 2 | 4 |
| Laboratory technician | 22 | 21 | 23.5 |
| Hospital porter | 5 | 2 | 8 |
| Patient | |||
| Direct contact with nurse: | |||
| – First cycle | 111 | 106 | 117 |
| – Second cycle | 51 | 46 | 57 |
| – Third cycle | 51 | 46 | 57 |
| – Subsequent cycles | 31 | 27 | 36 |
| Waiting time | 4 | 3 | 4 |
| Observation time: | |||
| – First cycle | 360 | 360 | 360 |
| – Second cycle | 61 | 61 | 61 |
| – Third cycle | 56 | 56 | 57 |
| – Subsequent cycles | 1 | 1 | 1 |
iv.: Intravenous; sc.: Subcutaneous.
To estimate the administration costs, the time estimates for the specific activities, categorized by profession, were assessed in hours, and these time estimates were valued by national, average, hourly gross wages including payroll tax for each profession (Table 2).
| Profession | Hourly gross wages (incl. overhead), € | Source | ||
|---|---|---|---|---|
| Secretary | 70 | Estimated based on yearly wages [6] | ||
| Nurse | 82 | Estimated based on yearly wages [6] | ||
| Medical specialist | 191 | Estimated based on yearly wages [6] | ||
| Pharmacist | 74 | Estimated based on yearly wages [6] | ||
| Laboratory technician | 103 | Estimated based on yearly wages [6] | ||
| Hospital porter | 67 | Estimated based on yearly wages [6] | ||
| Cost per hour, € | Source | |||
| Patient's time | 15 | [7] | ||
| Utilization of department rooms | Cost per hour, € | Min, € | Max, € | Source |
| Treatment room, iv. | 3.3 | 2.8 | 3.5 | [8] |
| Treatment room, sc. | 2.1 | 1.9 | 2.4 | [8] |
| Observation/waiting room | 1.3 | 0.9 | 1.7 | [8] |
2017 price level.
Incl.: Including; iv.: Intravenous; Max: Maximum; Min: Minimum; sc.: Subcutaneous.
As different departments participated in the study, the time estimates were assessed as a weighted average (weighted based on the number of patients in treatment).
Similar to other studies and Danish guidelines, an overhead percentage on 100% for all wages was applied [8,9]. The overhead costs are included to take costs that are not directly related to labor or patient related activities (e.g., administrative costs or training/education costs) into account.
Patients’ time was valued by applying national weighted unit costs for working and leisure time (Table 2) [7] assuming that some patients work whereas others are outside the workforce. Patients’ time included the time spent at the hospital department (i.e., from arrival till leaving) whereas transportation time and possible time for accompanying relative is not included.
iv. administration's extra use of utensils was estimated on the basis of information from the hospital pharmacies and a previous Danish study [8].
Instead of a peripheral vein catheter (venflon), some iv. patients have a permanent port (port-a-cath). National tariffs for implanting the permanent port were applied to a unit cost estimate for this procedure [10].
Both iv. and sc. patients occupy the department's waiting/observation rooms and treatment rooms when they are treated and subsequently observed. In estimating the cost of utilization of the department rooms, we applied a standard cost per square meter per hour estimated in a previously published Danish study (Table 2) [8].
Results were estimated from a healthcare (hospital) perspective. In addition, the costs of the patients’ time were included, that is, the administration costs are presented with and without the inclusion of the costs of the patients’ time.
Univariate sensitivity analyses were performed by presenting the range in the administration costs by applying the minimum and maximum estimates for time consumption related to the specific activities and by lowering the applied overhead percentage.
Finally, for iv. and sc., respectively, results are presented as the total cost of administration for 17 cycles (corresponding to 1-year treatment) and as the costs for the first, secondand third cycle and subsequent cycles.
Results
Interviews were performed in five oncology departments, three departments located at a university hospital and two departments located at a regional hospital. This corresponds to 42% of all oncology departments involved in treatment of HER2-positive breast cancer. The participating departments can be considered geographically representative as four out of five hospital regions are represented in the interviews. At three departments, oncologists and nurses participated in the interview and at two departments only nurses participated. In total, three oncologists and five nurses were interviewed.
In addition, we performed interviews with pharmacists and laboratory technicians at two hospital pharmacies, one at a pharmacy located at a university hospital and one at a regional hospital.
Figure 1 provides an overview of the activities and tasks for iv. and sc. administration, respectively, that were identified via the interviews. The iv. administration takes longer time as infusion time is 90 min at the first cycle and 30 min at subsequent cycles whereas the injection time is 2–5 min at all sc. cycles. In addition, there may be extra waiting time for iv. patients as some departments do not order trastuzumab until the iv. patient has arrived at the department.
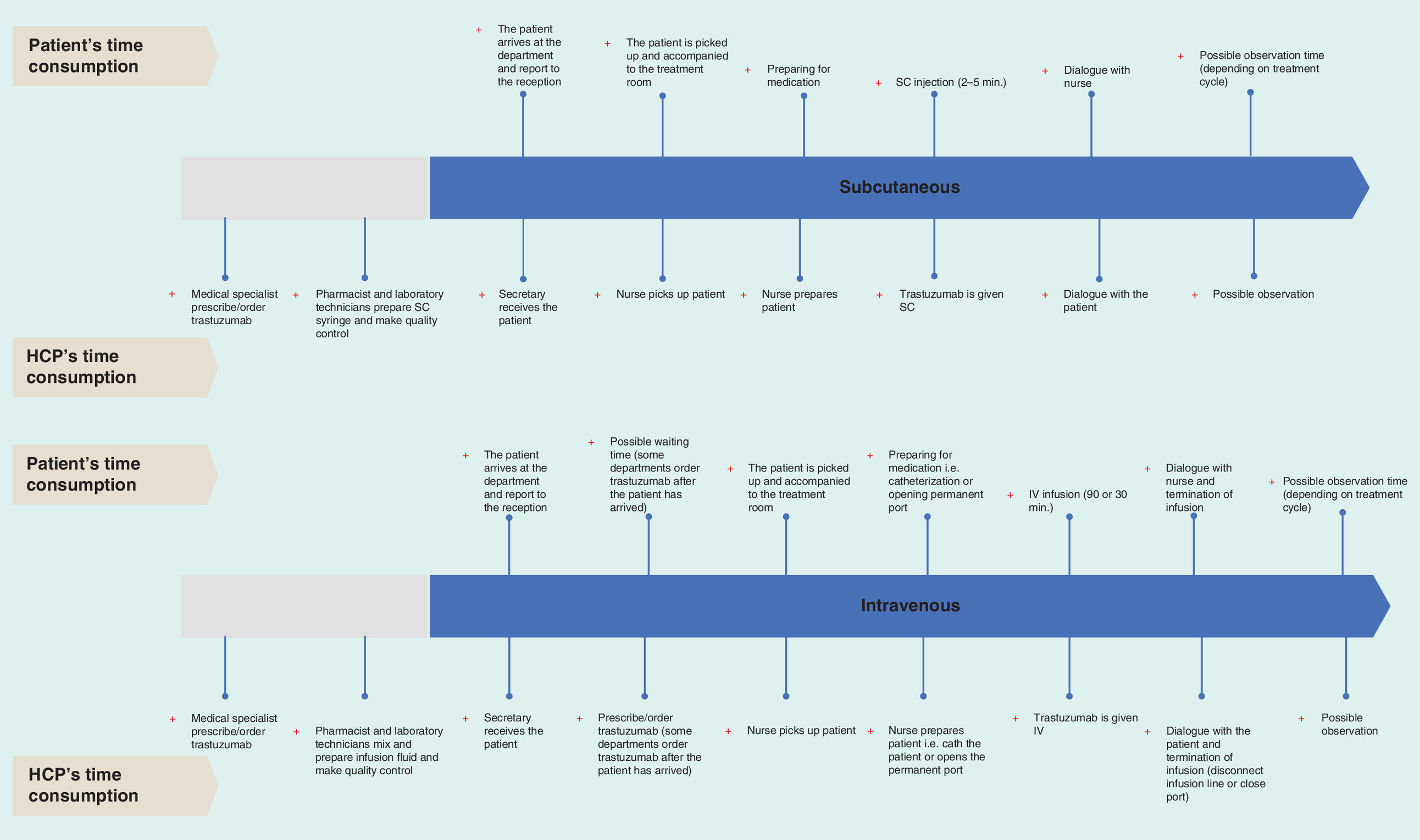
Figure 1. Activities.
HCP: Healthcare professional; IV: Intravenous; SC: Subcutaneous.
The average time estimates for the activities categorized by personnel appear in Table 1. Compared with sc. administration, it is seen that the time consumption for nurses and laboratory technicians and the patients’ time consumption is markedly higher for iv. administration. This results from the fact that the infusion time for iv. patients is markedly longer than the injection time for sc. patients and that preparation of the infusion fluid at the hospital pharmacy also takes a longer time than preparation of the sc. syringe. However, for iv. administration the nurse is on average treating two patients simultaneously. As more iv. patients are treated in the same room the nurse can initiate two to four treatments within an hour.
According to guidelines, patients treated with trastuzumab should be observed by a healthcare professional after the infusion or injection. All patients regardless of administration form are observed 6 h (360 min) after the first cycle. For the second, third and fourth cycle, observation times are shorter and there is variation in practice. After the fourth cycle, the patients are no longer observed.
Applying the results from Table 1 and the unit cost estimates (Table 2), the total administration costs for 17 cycles (corresponding to approximately 1 year) for sc. and iv., respectively, are shown in Figure 2, and the administration costs per cycle (i.e., first, second, third and subsequent cycles) for sc. and iv., respectively, appear in Table 3.
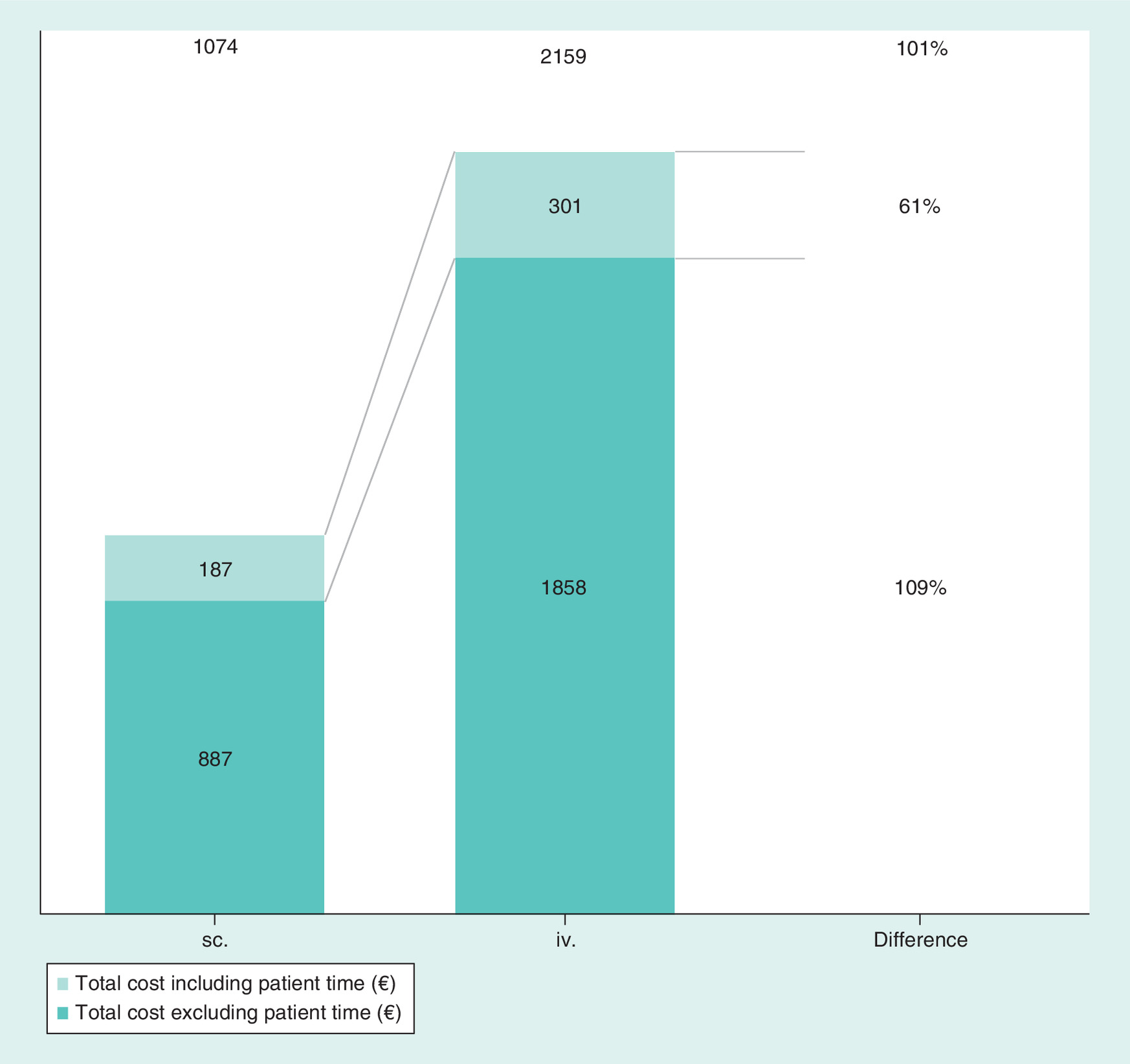
Figure 2. Total administration costs for 17 cycles sc. and iv., respectively (€, 2017 price level).
IV: Intravenous; SC: Subcutaneous.
| 1st cycle, € | 2nd cycle, € | 3rd cycle, € | Subsequent cycles, € | |
|---|---|---|---|---|
| sc. | ||||
| Personnel | ||||
| Secretary | 1.4 | 1.4 | 1.4 | 1.4 |
| Nurse | 22.4 | 22.4 | 22.4 | 22.4 |
| Medical specialist | 5.5 | 5.5 | 5.5 | 5.5 |
| Pharmacist | 5.1 | 5.1 | 5.1 | 5.1 |
| Laboratory technician | 11.1 | 11.1 | 11.1 | 11.1 |
| Hospital porter | 5.6 | 5.6 | 5.6 | 5.6 |
| Other costs | ||||
| Treatment room | 0.5 | 0.5 | 0.5 | 0.5 |
| Observation/waiting room | 8.0 | 2.1 | 1.5 | 0.0 |
| Patient's time | ||||
| Direct contact with HCP | 3.3 | 3.3 | 3.3 | 3.3 |
| Waiting time | 0.0 | 0.0 | 0.0 | 0.0 |
| Observation time | 90.4 | 23.4 | 16.5 | 0.0 |
| Total cost, excl. patient's time | 60 | 54 | 53 | 52 |
| Total cost, incl. patient's time | 153 | 80 | 73 | 55 |
| iv. | ||||
| Personnel | ||||
| Secretary | 1.7 | 1.7 | 1.7 | 1.7 |
| Nurse | 90.2 | 49.3 | 49.3 | 35.5 |
| Medical specialist | 4.0 | 4.0 | 4.0 | 4.0 |
| Pharmacist | 5.1 | 5.1 | 5.1 | 5.1 |
| Laboratory technician | 27.3 | 27.3 | 27.3 | 27.3 |
| Hospital porter | 5.6 | 5.6 | 5.6 | 5.6 |
| Other costs | ||||
| Treatment room | 6.1 | 2.8 | 2.8 | 1.7 |
| Observation/waiting room | 8.1 | 1.4 | 1.3 | 0.1 |
| Utensils | 8.4 | 8.4 | 8.4 | 8.4 |
| Port-a-cath | 14.0 | 14.0 | 14.0 | 14.0 |
| Patient's time | ||||
| Direct contact with HCP | 27.8 | 12.7 | 12.7 | 7.7 |
| Waiting time | 0.9 | 0.9 | 0.9 | 0.9 |
| Observation time | 90.4 | 15.3 | 14.1 | 0.3 |
| Total cost, excl. patient's time | 171 | 120 | 120 | 103 |
| Total cost, incl. patient's time | 290 | 149 | 147 | 112 |
2017 price level.
excl.: Excluding; HCP: Healthcare professional; incl.: Including; iv.: Intravenous; sc.: Subcutaneous.
Excluding the patient's time consumption, iv. administration is associated with higher cost for 17 cycles; €971 (i.e., €1858 vs €887 cf.; Figure 2). Inclusion of the patient's time consumption increases the extra costs associated with iv. administration from €971 to €1085 (i.e., €2159 vs €1074).
From Table 3, it is seen that all sc. cycles are associated with higher costs and especially the administration costs for the first cycle are high (€171 vs €60, excluding patient's time). Excluding patient's time consumption, the extra administration costs are €111 for the first cycle, €66 for the second cycle, €67 for the third cycle and €51 for subsequent sc. cycles. Including patient's time consumption, the extra administration costs are €137 for the first, €69 for the second, €74 for the third and €57 for subsequent sc. cycles.
Finally, in Table 4, as a univariate sensitivity analysis, the range in the cost estimates is shown. Lowering the overhead percentage from 100 to 50% or applying the minimum time estimates, iv. administration is still associated with higher costs. Including patient's time, the extra cost for iv. administration compared with sc. administration ranges from €945 to €1122, when minimum estimates for sc. and iv. and maximum estimates for sc. and iv. are compared. However, when minimum time estimates for iv. and maximum time estimates for sc. are compared, the extra cost of iv. treatment is estimated to €484. Similarly, when maximum time estimates for iv. and minimum time estimates for sc. are compared, the extra cost of iv. treatment is estimated to €1654.
| Administration costs | Average, € | Average: 50% OH, € | Min, € | Max, € |
|---|---|---|---|---|
| Total adm. cost, incl. patient's time, sc. | 1074 | 857 | 790 | 1428 |
| Total adm. cost, incl. patient's time, iv. | 2159 | 1802 | 1912 | 2444 |
2017 price level.
adm.: Administration; incl.: Including; iv.: Intravenous; Max: Maximum; Min: Minimum; OH: Overhead; sc.: Subcutaneous.
As stated, the drug costs of the iv. and sc. formulation are on average the same and the hospital pharmacies report that there is no drug waste associated with iv. administration. That is, drug wastage is limited as several trastuzumab patients (iv.) are treated the same day. However, in real life it can be difficult to dose precisely according to patients’ weight and there can be wastage if veils do not equal the exact amounts of patients regarding iv. treatment.
Discussion
This study estimated the administration costs for iv. and sc. treatment, respectively, of HER2-positive breast cancer patients. The results show that sc. compared with iv. trastuzumab treatment primarily saves nurse, laboratory technician and patient time and results in cost savings for the first and subsequent treatment cycles. Depending on the assumptions and applied time estimates, the extra cost of administration associated with iv. is approximately €1000 for 17 cycles corresponding to 1-year treatment.
Costs of patient's time must be considered as a conservative estimate as transportation time is not included.
The cost of implanting of a permanent port in some patients was included. As this port may be used for other iv. treatments as well, a 100% inclusion of these costs may constitute an overestimate.
Our results are similar to another Danish study reporting the costs of iv. and sc. administration in biologic treatment of patients with inflammatory bowel disease [11] as well as the results are confirmed by other studies analyzing sc. and iv. administration of trastuzumab [12–14].
Our analysis is based on interviews and not an observational; time and motion study assuming the latter would generate more precise time consumption estimates. However, the reported time estimates from the interviewed participants for the specific activities are quite consistent, indicating that the estimates are consistent and that observations probably would not change the time estimates notably.
In addition to being cost saving, it should also be noted that sc. administration, compared with iv., is preferred by most patients if given the option. This is documented in a Swedish study and in the PrefHER study [13,15]. Furthermore, the safety profile of sc. trastuzumab is consistent with the known safety profile of iv. treatment in early breast cancer.
This study focuses on the administration cost. However, in addition to increased administration cost, iv. treatment may also lead to drug wastage (due to dose depending on body weight). However, laboratory technicians and pharmacists report that drug wastage is minimized as infusion fluid for more patients are prepared the same day, implying that surplus from one patient is used for another patient. Other studies do report that the drug wastage may be considerable [16].
Conclusion
As sc. administration is associated with lower administration costs, this implies that switching patients from iv. to sc. would make it possible to treat more patients without increasing the personnel resources.
Interviews were performed in five oncology departments, three departments located at a university hospital and two departments located at a regional hospital corresponding to 42% of all oncology departments involved in treatment of HER2-positive breast cancer.
Subcutaneous (sc.) compared with intravenous (iv.) trastuzumab treatment primarily saves nurse, laboratory technician and patient time and results in cost savings for the first and subsequent treatment cycles.
The safety profile of sc. trastuzumab is consistent with the safety profile of iv. treatment.
sc. administration, compared with iv., is preferred by most patients if given the option.
sc. administration is associated with lower administration costs, implying that switching patients from iv. to sc. would make it possible to treat more patients without increasing the personnel resources.
Financial & competing interests disclosure
This study was supported by an unrestricted grant from Roche. KF Jensen is an employee at Roche. Incentive was a paid vendor by Roche. J Olsen and DS Olesen are employees of Incentive. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Sundhedsdatastyrelsen. Cancer incidence in Denmark, The Cancer Register 2015 [Nye Kræfttilfælde i Danmark, Cancerregisteret 2015]. www.sundhedsdatastyrelsen.dk.
2.
European Medicines Agency. Annex 1. Summary of product characteristics (Herceptin). Report No.: 15/09/2016. www.ema.europa.eu/ema/.
3.
Ismael G, Hegg R, Muehlbauer S et al. Subcutaneous versus intravenous administration of (neo)adjuvant trastuzumab in patients with HER2-positive, clinical stage I–III breast cancer (HannaH study): a Phase 3, open-label, multicentre, randomised trial. Lancet Oncol. 13(9), 869–878 (2012).
•• Provides information about the effect and safety of intravenous (iv.) versus subcutaneous (sc.) administration.
4.
Jackisch C, Kim S-B, Semiglazov V et al. Subcutaneous versus intravenous formulation of trastuzumab for HER2-positive early breast cancer: updated results from the Phase III HannaH study. Ann. Oncol. 26(2), 320–325 (2015).
•• Provides updated information about the effect and safety of iv. versus sc. administration.
5.
Danish Breast Cancer Cooperative Group (DBCG). Kvalitetsindikatorrapport for Brystkræft 2015. Landsdækkende Klinisk Kvalitetsdatabase for Brystkræft. Databasernes Fællessekretariat. www.dbcg.dk.
6.
Danish Regions and Municipalities Office for Wage Statistics [Kommunernes og Regionerens Løndatakontor]. www.fldnet.dk/statistik/lpx7/.
7.
Transportøkonomiske Enhedspriser. www.modelcenter.transport.dtu.dk/Noegletal/Transportoekonomiske-Enhedspriser.
8.
Sørensen J. Analysis of differences in resource use and costs for intravenous and subcutaneous administration of Herceptin treatment of HER2-positive breast cancer [Analyse af forskelle i ressourceforbrug og omkostninger ved intravenøs og subkutan administration af Herceptin til behandling af HER2 positiv brystkræft]. University of Southern Denmark, Denmark (2014).
9.
Amgros. Værdisætning af enhedsomkostninger (2017). www.amgros.dk.
10.
Sundhedsdatastyrelsen. Tariffs. 2017 [Takstsystem. Vejledning. 2017] (2017). www.drg.dk.
11.
Jakobsen M, Rasmussen SR, Kjelberg J. Differences in costs of administration of biologics – a case study within gastroenterology [Forskelle i omkostninger ved administrering af biologiske lægemidler – Et casestudie inden for gastroenterologien]. KORA (2015). www.kora.dk/media/3887491/10724_administrering_biologiske_laegemidler.pdf.
12.
Ponzetti C, Canciani M, Farina M, Era S, Walzer S. Potential resource and cost saving analysis of subcutaneous versus intravenous administration for rituximab in non-Hodgkin's lymphoma and for trastuzumab in breast cancer in 17 Italian hospitals based on a systematic survey. Clin. Outcomes Res. 8, 227–233 (2016).
• Information and results from a similar study in an Italian setting.
13.
Olofsson S, Norrlid H, Karlsson E, Wilking U, Ragnarson Tennvall G. Societal cost of subcutaneous and intravenous trastuzumab for HER2-positive breast cancer – an observational study prospectively recording resource utilization in a Swedish healthcare setting. Breast Edinb. Scotl. 29, 140–146 (2016).
• Information and results from a similar study in a Swedish setting.
14.
Rule S, Collins GP, Samanta K. Subcutaneous vs intravenous rituximab in patients with non-Hodgkin lymphoma: a time and motion study in the United Kingdom. J. Med. Econ. 17(7), 459–468 (2014).
15.
Pivot X, Gligorov J, Müller V et al. Preference for subcutaneous or intravenous administration of trastuzumab in patients with HER2-positive early breast cancer (PrefHer): an open-label randomised study. Lancet Oncol. 14(10), 962–970 (2013).
•• Provides information about patients’ preferences for sc. and iv. administration.
16.
Pearson S-A, Ringland CL, Ward RL. Trastuzumab and metastatic breast cancer: trastuzumab use in Australia – monitoring the effect of an expensive medicine access program. J. Clin. Oncol. 25(24), 3688–3693 (2007).
Information & Authors
Information
Published In
Copyright
© 2017 Future Medicine Ltd.
History
Received: 26 June 2017
Accepted: 27 October 2017
Published online: 4 December 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Costs of subcutaneous and intravenous administration of trastuzumab for patients with HER2-positive breast cancer. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0048
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Saby George, Maria T. Bourlon, Michael J. Overman, Matt Dixon, Karishma Shelley, Kristen J. Markus, Rachel M. Kewley, Sophie I. Pope, Laurence Albigès, Systematic literature review of intravenous versus subcutaneous administration of oncology therapies: A clinical, economic and patient perspective, Cancer Treatment Reviews, 10.1016/j.ctrv.2025.102974, 139, (102974), (2025).
- Amir Abbas Tahami Monfared, Stephanie Barrows, Lindsey Fox, Brittney Herbel, William L. Herring, Alisha Krumbach, Quanwu Zhang, Societal Costs and Efficiency of Subcutaneous versus Intravenous Lecanemab in Early Alzheimer’s Disease: A U.S. Cost Comparison Model, Neurology and Therapy, 10.1007/s40120-025-00790-2, 14, 5, (1863-1888), (2025).
- undefined Tran Thi My Duyen, undefined Nguyen Vu Lan Chi, undefined Pham Tri Dung, undefined Nguyen Thi Thu Thuy, Economic value of subcutaneous versus intravenous trastuzumab administration in the treatment of HER2-positive breast cancer: A systematic review, Tạp Chí Khoa học Trường Đại học Quốc tế Hồng Bàng, 10.59294/HIUJS.VOL.7.2024.686, (61-72), (2024).
- Raquel Aguiar-Ibáñez, Iain Fotheringham, Lalith Mittal, Arthur Sillah, Smit Pathak, Differences Between Intravenous and Subcutaneous Modes of Administration in Oncology from the Patient, Healthcare Provider, and Healthcare System Perspectives: A Systematic Review, Advances in Therapy, 10.1007/s12325-024-02985-9, 41, 12, (4396-4417), (2024).
- Luciana Castro Garcia Landeiro, Tamie de Camargo Martins, Ruth Bartelli Grigolon, Isabel Monteiro, Joana Bisol Balardin, Eduardo Padilha, Gilberto Amorim, Stephen Stefani, The burden of systemic therapy administration route in treating HER2-positive breast cancer (for patients, healthcare professionals, and healthcare system): a systematic literature review, Frontiers in Pharmacology, 10.3389/fphar.2024.1338546, 15, (2024).
- Elisabetta Munzone, Alessandra Fabi, Giuseppe Buono, Roberta Caputo, Emilia Montagna, Mara Negri, Francesco Nuzzo, Antonella Palazzo, Ida Paris, Luca Conti, Anna Baggi, Jean Marie Franzini, Michelino De Laurentiis, The PHASTER Study: Economic and Organizational Impact of Subcutaneous (SC) Pertuzumab and Trastuzumab Fixed-Dose Combination (PH FDC SC) for Treatment of HER2+ Breast Cancer Patients, Drugs & Therapy Perspectives, 10.1007/s40267-023-01038-5, 39, 12, (432-446), (2023).
- Eric C. Barat, Marianne L.E. Arrii, Annaelle Soubieux-Bourbon, Mikaël Daouphars, Rémi Varin, Patrick R. Tilleul, Cost effectiveness of using trastuzumab biosimilars compared to trastuzumab original drugs to treat breast cancer in a hospital setting, The Breast, 10.1016/j.breast.2023.103588, 72, (103588), (2023).
- Ana Parra, Claudia Hernández, Laura Prieto-Pinto, Evaluation of the economic benefits, administration times, and patient preferences associated with the use of biotechnological drugs administered subcutaneously and intravenously in patients with cancer: a systematic review, Expert Review of Pharmacoeconomics & Outcomes Research, 10.1080/14737167.2023.2249232, 23, 9, (1017-1026), (2023).
- A. M. Alonso Torres, A. G. Arévalo Bernabé, N. Becerril Ríos, M. F. Hellín Gil, J. M. Martínez Sesmero, V. Meca Lallana, Ll. Ramió-Torrentà, A. Rodríguez-Antigüedad, L. Gómez Maldonado, I. Triana Junco, M. Gómez-Barrera, N. Espinoza Cámac, I. Oyagüez, Cost-Analysis of Subcutaneous vs Intravenous Administration of Natalizumab Based on Patient Care Pathway in Multiple Sclerosis in Spain, PharmacoEconomics - Open, 10.1007/s41669-023-00394-2, 7, 3, (431-441), (2023).
- Conor McCloskey, María Toboso Ortega, Sunita Nair, Maria João Garcia, Federico Manevy, A Systematic Review of Time and Resource Use Costs of Subcutaneous Versus Intravenous Administration of Oncology Biologics in a Hospital Setting, PharmacoEconomics - Open, 10.1007/s41669-022-00361-3, 7, 1, (3-36), (2022).