Outcomes research examining treatments, quality of life and costs in HER2-negative and triple-negative metastatic breast cancer: a systematic literature review
Abstract
Aim: With the aggregation of real-world data in healthcare, opportunities for outcomes research are growing. In this study, we summarize published literature examining comparative effectiveness research (CER), treatment patterns, quality of life (QoL) and costs in HER2-negative and triple-negative (TN) metastatic breast cancer (mBC). Methods: PubMed (2010–January 2016) and four conferences (2013–January 2016) were searched using MeSH/keywords, including mBC, QoL, morbidity and therapeutics. Studies relating to CER, treatment patterns, QoL, costs or treatment appropriateness in US patients with HER2-negative/TN mBC were included in the review. Results: Of 1782 identified records, 33 studies met full inclusion criteria: seven related to CER, 18 to treatment patterns, one to treatment appropriateness/navigation, two to QoL and five to costs. Studies varied in objectives, designs and outcomes. Study designs included retrospective chart reviews (52%), retrospective secondary database analyses (27%), economic models (12%), physician surveys (6%) and patient surveys (3%). 25 studies reported results on HER2-negative mBC, six on TN mBC and two on both subtypes. The most common end points examined were treatment patterns, overall survival and progression-free survival. Conclusion: Outcomes research in HER2-negative mBC in the USA was limited, specifically among TN patients, indicating an opportunity for further research in this high unmet need population. Endpoints and treatment options varied, thus, it is difficult to draw summary conclusions about these studies. Outcomes research examining real-world data in mBC has increased in recent years, and may continue to grow with the implementation of new policy programs.
Breast cancer is the most common cancer type among women in the USA. 29% of incident cancer cases are attributable to breast cancer alone [1]. About 66% of women with breast cancer have HER2-negative and 10–17% have HER2-negative, estrogen receptor-negative (ER-negative) and progesterone receptor-negative (PR-negative) cancer, referred to as triple-negative breast cancer (TNBC) [2,3]. In 2016, an estimated 246,660 women were newly diagnosed with breast cancer, of which approximately 6% had metastatic or stage IV disease at the time of diagnosis [1,4,5]. About 30% of women initially diagnosed with early-stage breast cancer develop recurrent advanced or metastatic disease [6,7]. The 5-year survival rate with stage IV breast cancer is only 26.3% [4,5].
Tumor markers in breast cancer impact prognosis, treatment and survival [8]. Prognosis has improved significantly for patients with metastatic HER2-positive breast cancer with emergence of trastuzumab and other anti-HER2 agents but has lagged for patients with advanced HER2-negative breast cancer since the emergence of effective new targeted therapies such as everolimus is only beginning [9]. Moreover, an important minority of these patients, those with triple-negative (TN) disease, has a relatively poor prognosis given the lack of targeted therapies, leaving cytotoxic chemotherapy as the primary treatment [2,8–10].
According to a recent estimate, breast cancer accounts for about US$16.5 billion in expenditures in the USA, which is the leading cost for any single cancer type [11,12]. Quality of life (QoL) research also indicates that QoL of breast cancer patients is poor [13–15]. While there is a large body of literature on topics related to the burden of disease in breast cancer, the literature in metastatic breast cancer (mBC) is limited and variable in methodologic quality, particularly in patients with HER2-negative and TN subtypes (e.g., Foster et al. [16]). Considering the substantial economic and humanistic burden of breast cancer, research into both patient-centered and economic outcomes is important in informing clinicians, patients and payers [5,12,17].
With the passage of the 21st Century Cures Act in 2016 and the abundance of healthcare data collected via electronic health records and insurance claims, the potential of outcomes research using real-world data (RWD) is being widely acknowledged in the USA. The US FDA defines real-world evidence as “data regarding the usage, or the potential benefits or risks, of a drug derived from sources other than randomized control trials” [55]. Within the 21st Century Cures Act, there are plans to establish a framework describing sources for RWD, and developing standards and methodologies for collection and analysis of RWD. Additionally, American Society of Clinical Oncology (ASCO) recently published their position on the use of observational research in informing clinical decision-making and highlighting the potential of this research to help advance the evidence base for cancer care, serving as a complement for data that have already been generated in randomized control trials and answering questions that were not answered in randomized control trials. [56].
In this literature review, we examined several different types of observational research, and broadened our search to include economic studies and those related to QoL, thus describing the included studies as ‘outcomes research’. Conducting outcomes research in oncology, specifically to compare effectiveness end points, can be challenging as disease biology differs by cancer type, line of therapy definitions can be arbitrary and many RWD sources do not capture clinical response, progression or even survival. To better understand the extent and study characteristics of current outcomes research related to HER2-negative and TN mBC, we conducted a systematic literature review to summarize the recent publications on comparative effectiveness research (CER), treatment patterns and appropriateness, QoL and costs in these patients.
Methods
Data sources & search strategy
We searched PubMed and four online conference databases: ASCO Annual Meeting, ASCO Breast Cancer Symposium, ASCO Quality Care Symposium and San Antonio Breast Cancer (SABC) Symposium. To supplement this search, we also reviewed the references of articles included for data abstraction.
PubMed was searched to identify studies in HER2-negative and TN mBC patients, accounting for a variety of ways the terms of interest may be referenced in the literature using keywords and Medical Subject Headings terms: ‘metastatic breast cancer’, ‘breast neoplasms’, ‘triple negative’, ‘estrogen receptor negative’, ‘progesterone receptor negative’, ‘human epidermal growth factor receptor 2 negative’, ‘costs and cost analysis’, ‘economics’, ‘cost of illness’, ‘quality of life’, ‘health services’, ‘morbidity’, ‘survival’, ‘mortality’, ‘epidemiologic studies’, ‘therapeutics’, ‘comparative’, ‘effectiveness’, ‘guidelines as topic’, ‘pain’, ‘self report’, ‘evaluation studies as a topic’ and ‘disease management’ (Tables 1 & 2).
| Search terms | PubMed search string |
|---|---|
| Metastatic breast cancer | (‘secondary’ [Subheading] OR ‘secondary’ [All Fields] OR ‘metastatic’ [All Fields]) AND (‘breast neoplasms’ [MeSH Terms]) OR (‘breast’ [All Fields] AND ‘neoplasms’ [All Fields]) OR ‘breast neoplasms’ [All Fields] OR (‘breast’ [All Fields] AND ‘cancer’ [All Fields]) OR ‘breast cancer’ [All Fields] |
| Triple negative | triple [All Fields] AND negative [All Fields] |
| ER negative | ‘er’ [All Fields] AND negative [All Fields] |
| ER negative | (‘receptors, estrogen’ [MeSH Terms] OR ‘receptors’ [All Fields] AND ‘estrogen’ [All Fields]) OR ‘estrogen receptors’ [All Fields] OR (‘estrogen’ [All Fields] AND ‘receptor’ [All Fields]) OR ‘estrogen receptor’ [All Fields] AND negative [All Fields] |
| PR negative | ‘pr’ [All Fields] AND negative [All Fields] |
| PR negative | (‘receptors, progesterone’ [MeSH Terms] OR (‘receptors’ [All Fields] AND ‘progesterone’ [All Fields]) OR ‘progesterone receptors’ [All Fields] OR (‘progesterone’ [All Fields] AND ‘receptor’ [All Fields]) OR ‘progesterone receptor’ [All Fields] AND negative [All Fields] |
| HER2-negative | HER2-negative [All Fields] |
| HER2-negative | (‘ERBB2 protein, human’ [Supplementary Concept] OR ‘ERBB2 protein, human’ [All Fields] OR ‘human epidermal growth factor receptor 2’ [All Fields]) AND negative [All Fields] |
ER: Estrogen receptor; PR: Progesterone receptor.
| Search terms | PubMed search string |
|---|---|
| Comparative effectiveness, unmet need, patient-reported outcomes, self-report or self-reported, pain | (comparative [All Fields] AND effectiveness [All Fields]) OR (unmet [All Fields] AND need [All Fields]) OR (‘patients’ [MeSH Terms] OR ‘patients’ [All Fields] OR ‘patient’ [All Fields]) AND (‘research report’ [MeSH Terms] OR (‘research’ [All Fields] AND ‘report’ [All Fields]) OR ‘research report’ [All Fields] OR ‘reported’ [All Fields]) AND outcomes [All Fields]) OR ((‘self report’ [MeSH Terms] OR (‘self’ [All Fields] AND ‘report’ [All Fields]) OR ‘self report’ [All Fields]) OR self-reported [All Fields]) OR (‘pain’ [MeSH Terms] OR ‘pain’ [All Fields]) |
| Burden of illness, outcomes, healthcare utilization, healthcare service use, morbidity, co-morbidity or co-morbidities, survival or mortality | (‘cost of illness’ [MeSH Terms] OR (‘cost’ [All Fields] AND ‘illness’ [All Fields]) OR ‘cost of illness’ [All Fields] OR (‘burden’ [All Fields] AND ‘illness’ [All Fields]) OR ‘burden of illness’ [All Fields]) OR (‘health services administration’ [MeSH Terms] OR ‘epidemiologic studies’ [MeSH Terms] OR ‘epidemiology’ [Subheading]) OR((‘delivery of health care’ [MeSH Terms] OR (‘delivery’ [All Fields] AND ‘health’ [All Fields] AND ‘care’ [All Fields]) OR ‘delivery of health care’ [All Fields] OR ‘healthcare’ [All Fields]) AND (‘utilization’ [Subheading] OR ‘utilization’ [All Fields]) OR (‘patient acceptance of health care’ [MeSH Terms] OR (‘patient’ [All Fields] AND ‘acceptance’ [All Fields] AND ‘health’ [All Fields] AND ‘care’ [All Fields]) OR ‘patient acceptance of health care’ [All Fields] OR (‘health’ [All Fields] AND ‘care’ [All Fields] AND ‘utilization’ [All Fields]) OR ‘health care utilization’ [All Fields])) OR ((‘delivery of health care’ [MeSH Terms] OR (‘delivery’ [All Fields] AND ‘health’ [All Fields] AND ‘care’ [All Fields]) OR ‘delivery of health care’ [All Fields] OR ‘healthcare’ [All Fields]) AND service [All Fields]) OR ((‘health services’ [MeSH Terms] OR (‘health’ [All Fields] AND ‘services’ [All Fields]) OR ‘health services’ [All Fields] OR (‘health’ [All Fields] AND ‘care’ [All Fields] AND ‘service’ [All Fields]) OR ‘health care service’ [All Fields])) OR ((‘epidemiology’ [Subheading] OR ‘epidemiology’ [All Fields] OR ‘morbidity’ [All Fields] OR ‘morbidity’ [MeSH Terms])) OR ((‘comorbidity’ [MeSH Terms] OR ‘comorbidity’ [All Fields]) OR (‘comorbidity’ [MeSH Terms] OR ‘comorbidity’ [All Fields] OR ‘comorbidities’ [All Fields])) OR ((‘mortality’ [Subheading] OR ‘mortality’ [All Fields] OR ‘survival’ [All Fields] OR ‘survival’ [MeSH Terms]) OR (‘mortality’ [Subheading] OR ‘mortality’ [All Fields] OR ‘mortality’ [MeSH Terms])) |
| Appropriateness and treatment, adherence and treatment, appropriateness and guideline, adherence and guideline, inappropriate and treatment, inappropriate and guideline | (appropriateness [All Fields] AND (‘therapy’ [Subheading] OR ‘therapy’ [All Fields] OR ‘treatment’ [All Fields] OR ‘therapeutics’ [MeSH Terms] OR ‘therapeutics’ [All Fields])) OR (adherence [All Fields] AND (‘therapy’ [Subheading] OR ‘therapy’ [All Fields] OR ‘treatment’ [All Fields] OR ‘therapeutics’ [MeSH Terms] OR ‘therapeutics’ [All Fields])) OR (adherence [All Fields] AND (‘therapy’ [Subheading] OR ‘therapy’ [All Fields] OR ‘treatment’ [All Fields] OR ‘therapeutics’ [MeSH Terms] OR ‘therapeutics’ [All Fields])) OR (Appropriateness [All Fields] AND (‘guideline’ [Publication Type] OR ‘guidelines as topic’ [MeSH Terms] OR ‘guideline’ [All Fields])) OR (adherence [All Fields] AND (‘guideline’ [Publication Type] OR ‘guidelines as topic’ [MeSH Terms] OR ‘guideline’ [All Fields])) OR (inappropriate [All Fields] AND (‘therapy’ [Subheading] OR ‘therapy’ [All Fields] OR ‘treatment’ [All Fields] OR ‘therapeutics’ [MeSH Terms] OR ‘therapeutics’ [All Fields])) OR (inappropriate [All Fields] AND (‘guideline’ [Publication Type] OR ‘guidelines as topic’ [MeSH Terms] OR ‘guideline’ [All Fields])) |
| Quality of care, monitoring and guidelines, evaluation and guidelines, management and guidelines, follow-up and guidelines | (quality [All Fields] AND care [All Fields]) OR (monitoring [All Fields] AND (‘guideline’ [Publication Type] OR ‘guidelines as topic’ [MeSH Terms] OR ‘guideline’ [All Fields])) OR ((‘evaluation studies’ [Publication Type] OR ‘evaluation studies as topic’ [MeSH Terms] OR ‘evaluation’ [All Fields]) AND (‘guideline’ [Publication Type] OR ‘guidelines as topic’ [MeSH Terms] OR ‘guideline’ [All Fields])) OR ((‘organization and administration’ [MeSH Terms] OR (‘organization’ [All Fields] AND ‘administration’ [All Fields]) OR ‘organization and administration’ [All Fields] OR ‘management’ [All Fields] OR ‘disease management’ [MeSH Terms] OR (‘disease’ [All Fields] AND ‘management’ [All Fields]) OR ‘disease management’ [All Fields]) AND (‘guideline’ [Publication Type] OR ‘guidelines as topic’ [MeSH Terms] OR ‘guideline’ [All Fields])) OR (follow [All Fields] AND up [All Fields] AND (‘guideline’ [Publication Type] OR ‘guidelines as topic’ [MeSH Terms] OR ‘guidelines’ [All Fields])) |
| Quality of life (QoL) | QoL [All Fields] OR ‘quality of life’ [MeSH Terms] OR (‘quality’ [All Fields] AND ‘life’ [All Fields]) OR ‘quality of life’ [All Fields] |
| Costs, economics, cost of treatment, cost of illness | (cost [tiab] OR costs [tiab] OR ‘costs and cost analysis’ [MeSH Terms] OR ‘economics’ [Subheading]) OR (costs [tiab] OR cost effective [tiab] OR economic [tiab]) OR (‘economics’ [Subheading] OR ‘economics’ [All Fields] OR (‘cost’ [All Fields] OR ‘costs and cost analysis’ [MeSH Terms] OR (‘costs’ [All Fields] AND ‘cost’ [All Fields] AND ‘analysis’ [All Fields]) OR ‘costs and cost analysis’ [All Fields]) OR (‘economics’ [Subheading] OR ‘economics’ [All Fields] OR ‘economics’ [MeSH Terms])) OR ((‘economics’ [Subheading] OR ‘economics’ [All Fields] OR ‘cost’ [All Fields] OR ‘costs and cost analysis’ [MeSH Terms] OR (‘costs’ [All Fields] AND ‘cost’ [All Fields] AND ‘analysis’ [All Fields]) OR ‘costs and cost analysis’ [All Fields]) AND (‘therapy’ [Subheading] OR ‘therapy’ [All Fields] OR ‘treatment’ [All Fields] OR ‘therapeutics’ [MeSH Terms] OR ‘therapeutics’ [All Fields])) OR (‘cost of illness’ [MeSH Terms] OR (‘cost’ [All Fields] AND ‘illness’ [All Fields]) OR ‘cost of illness’ [All Fields]) |
The search strings, shown in Tables 1 & 2, were developed based on review of keywords in relevant published literature and the US National Library of Medicine Health Services Research PubMed Queries [19]. The PubMed search (conducted in January 2016) was limited to literature published within the past 5 years and written in the English language. The 5-year search limit was imposed to capture the most current literature, while also considering the recent availability of everolimus for women with advanced hormone receptor (HR)-positive/HER2-negative mBC [20]. The four conferences (ASCO Annual Meeting, ASCO Breast Cancer Symposium, ASCO Quality Care Symposium and SABC Symposium) were searched online for abstracts presented in 2013 through 2015, using generic keywords – breast, metastatic and negative.
Screening & selection criteria
Identified articles were screened in three phases. In the first phase, the article titles and abstracts were screened to ensure the reported results were in human subjects, in patients with HER2-negative or TN mBC and in the US market. In the second Phase, the titles and abstracts of the articles that passed the first Phase were screened for acceptable study types: for example, not systematic reviews/meta-analyses reporting on one or fewer treatments, Phase I, II or III clinical trials and clinical studies on biomarkers in vivo/vitro. In the final screening phase, the full-texts of the remaining articles were screened to ensure the studies were in treated US human subjects with HER2-negative or TN mBC, reporting real-world research of interest. Finally, the references of the accepted articles were mined for key articles. This was done by flagging any reference for a study published in 2010 or later that mentioned ‘human epidermal growth factor receptor 2’, ‘HER2’ or ‘negative’ in the title. All flagged articles were then screened using the approach described above. Conference abstracts were screened in one phase, and all studies (full-text articles and conference abstracts) that passed the screenings were abstracted. The entire screening and abstraction process of this review was conducted using specialized software [21].
Results
Search & screening overview
The search of PubMed, online ASCO and SABC conference databases, conducted on 12 January 2016, yielded 1070 studies identified in PubMed and 712 identified in conference searchers (Figure 1). After screening the literature, 22 full text articles and 11 conference abstracts (seven from ASCO; four from SABC) were accepted for abstraction; among these, four studies were included after mining references of accepted articles. Of the 34 accepted records, seven were on CER (six full-length articles; one abstract), 18 were on treatment patterns (ten full-length articles; eight abstracts), one was on treatment navigation and categorized as a treatment appropriateness study in this review (one full-length article; zero abstracts), two were on QoL (two full-length articles; zero abstracts) and five were on costs (three full-length articles; two abstracts).
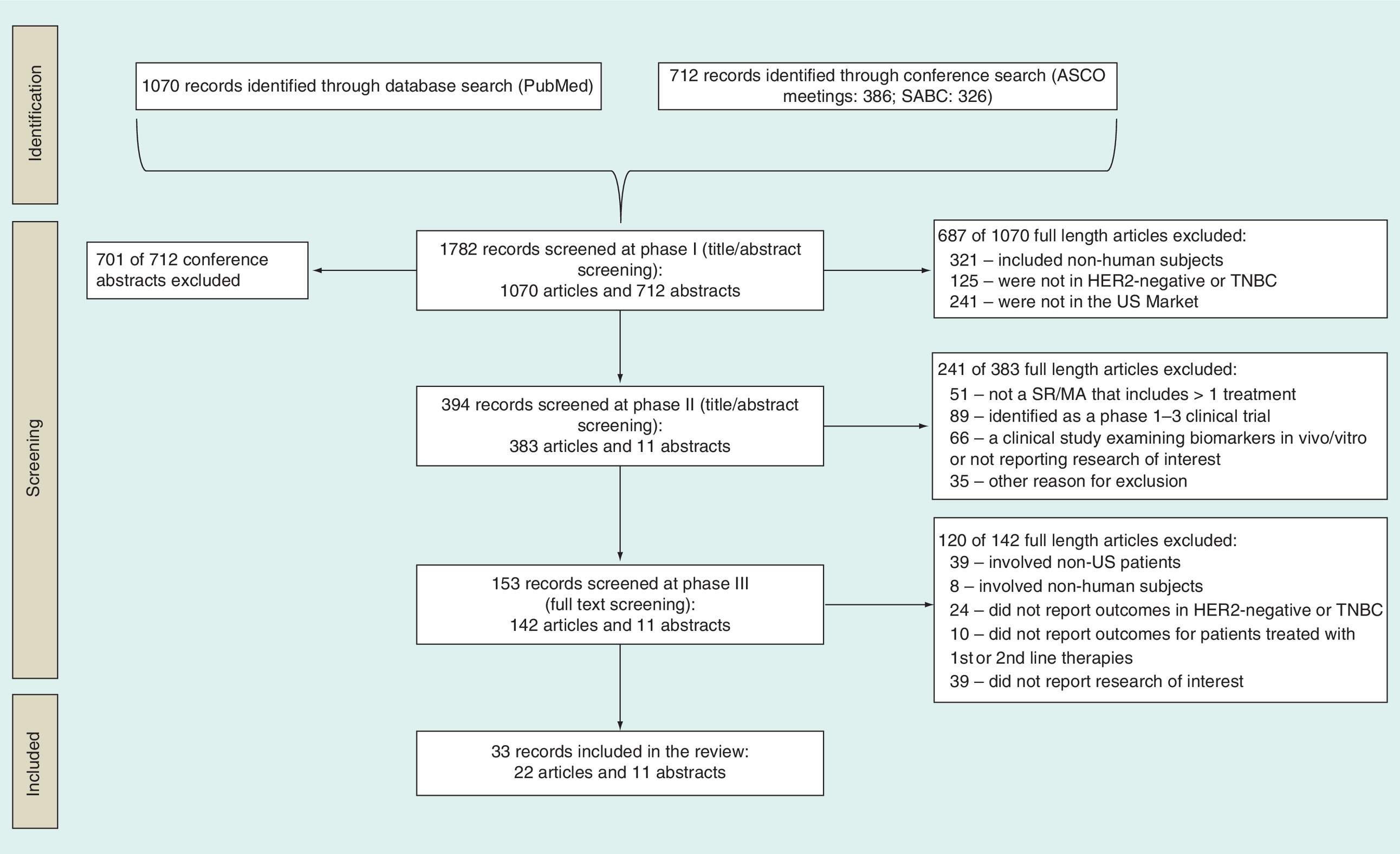
Figure 1. Flow diagram of search and screening progress.
American Society of Clinical Oncology (ASCO) meetings: ASCO Breast Cancer Symposium, ASCO Quality Care Symposium and ASCO Annual Meeting.
mBC: Metastatic breast cancer; SABC: San Antonio Breast Cancer Symposium; SR/MA: Systematic review/meta-analysis; TNBC: Triple-negative breast cancer.
Overview of CER
There were six full-length CER studies identified: Dawood et al., Dranitsaris et al., Li et al., Li et al., Lin et al., Xie et al. (Table 3) [22,23,24,25,26,27]. One CER study was reported in a conference abstract: Dranitsaris et al. [28].
| Study (year) | Study design | Data source | Primary outcomes | Patients | Treatments |
|---|---|---|---|---|---|
| Dawood et al. (2010) | Retrospective chart review | MD Anderson Cancer Center (1782 pts) | 1-year, 2-year, 5-year OS | HER2/neu-negative mBC | Breast conserving surgery, mastectomy |
| Dranitsaris et al. (2013) | Retrospective chart review | Eight community oncology practices (90 pts) | TTF; toxicity; treatment intensity and duration | mTNBC | Eribulin; prior anthracycline |
| Dranitsaris et al. (2015) | Retrospective chart review | 19 community oncology practices, part of the Cancer Clinics of Excellence network (225 pts) | TTF, HCRU, treatment-related toxicities, factors related to treatment choice, treatment duration, treatment discontinuation, morbidity, death | mTNBC | Eribulin, capecitabine, gemcitabine or vinorelbine and targeted agents |
| Li et al. (2016) | Retrospective secondary data analysis | MarketScan, PharMetrics commercial health insurance databases (2002Q1–2014Q2; 3298 pts) | TOT | HR+/HER2-mBC | Everolimus-based therapy, chemotherapy, capecitabine monotherapy |
| Li et al. (2015) | Retrospective chart review | Community oncology practice (371 pts) | OS; PFS; TOT | Postmenopausal women with HR+/HER2-stage IV mBC | Everolimus-based therapy, chemotherapy |
| Lin et al. (2015) | Retrospective chart review | 98 physicians from community-based practices, recruited from a nationwide online panel, contributed data (202 pts) | TOT; PFS | Stage IV HR+/HER2-mBC with liver metastasis | Everolimus-based therapy, endocrine monotherapy or chemotherapy |
| Xie et al. (2015) | Retrospective chart review | Sample collected from a panel of community-based oncologists and hematologists registered with the American Medical Association (513 pts) | TOT; PFS; TTC | Postmenopausal, stage IV, HR+/HER2-mBC women | Everolimus-based therapy, endocrine monotherapy |
HCRU: Healthcare resource utilization; HR+: Hormone receptor-positive; mBC: Metastatic breast cancer; mTNBC: Metastatic triple-negative breast cancer; OS: Overall survival; PFS: Progression-free survival; pts: Patients; TOT: Time on treatment; TTC: Time to chemotherapy; TTF: Time to treatment failure.
Dawood et al. [22] conducted a retrospective chart review, using data from the Breast Medical Oncology Department of the University of Texas MD Anderson Cancer Center, to compare the prognosis of women with metastatic HER2-positive breast cancer with (n = 191) and without (n = 118) the addition of trastuzumab with the prognosis of women with HER2-negative disease (n = 1782). The main outcomes examined were 1-year survival rates among patients with HER2-negative disease, HER2-positive disease and trastuzumab treatment and HER2/neu-positive disease and no trastuzumab treatment, which were 75.1, 86.6 and 70.2%, respectively. After adjustment, women with HER2-positive disease who received trastuzumab had a 44% reduction in the risk of death compared with women with HER2-negative disease. Dranitsaris et al. [28] carried out a retrospective chart review to examine the time to treatment failure, safety and efficacy of eribulin in 90 patients with mBC, treated at eight US community oncology clinics. About 17 of 90 patients (18.9%) had TN mBC and 57 of 90 (63.3%) had prior anthracycline treatment. The differences in time to failure by TN status (p = 0.49) and prior exposure to anthracyclines (hazard ratio: 0.78; p = 0.15) were not significant. The authors concluded that time to treatment failure with eribulin was comparable regardless of TN status and prior exposure to anthracyclines. Dranitsaris et al. [23] conducted a retrospective comparative effectiveness analysis of four different monotherapies with cytotoxic agents (eribulin, capecitabine, gemcitabine or vinorelbine) in 225 TN mBC treated at 19 community oncology clinics across the USA. The four treatment groups were comparable with respect to age, performance status, duration of disease-free survival, presence of co-morbidities and hemoglobin level before the start of chemotherapy. The median durations of treatment were roughly 2 months with eribulin, capecitabine and gemcitabine compared with 1.6 months with vinorelbine. Overall, eribulin was used as a later line of therapy relative to capecitabine, gemcitabine and vinorelbine, although eribulin was reported to have had at least comparable drug activity and tolerability, even when used in more heavily pretreated patients. Li et al. [24] conducted a retrospective chart review study to compare the real-world effectiveness of everolimus-based therapy and chemotherapy in a national sample of 371 postmenopausal women with HR-positive/HER2-negative mBC. Data came from patient charts at community oncology/hematology practices and outcomes assessed included overall survival (OS), progression-free survival (PFS) and time on treatment (TOT). Results were compared between patients that received everolimus-based therapy or chemotherapy, after failure of a nonsteroidal aromatase inhibitor (NSAI). The authors concluded patients treated with everolimus-based therapy tended to have less aggressive mBC than patients treated with chemotherapy. After controlling for the observed baseline characteristics, everolimus-based therapy was associated with significantly longer OS, PFS and TOT than chemotherapy. Li et al. [25] conducted a secondary data analysis of commercial health insurance claims to compare the TOT among 3298 patients treated with everolimus and chemotherapy among postmenopausal women with HR-positive/HER2-negative mBC. Data were from MarketScan and PharMetrics databases (2002Q1–2014Q2). HR-positive/HER2-negative mBC patients receiving everolimus experienced significantly longer TOT than those on chemotherapy overall and those on capecitabine monotherapy. Lin et al. [26] conducted a retrospective chart review at community oncology clinics to examine the comparative effectiveness of everolimus-based therapy versus endocrine monotherapy and chemotherapy in the treatment of 202 patients with HR-positive/HER2-negative breast cancer with liver metastasis in the USA. Patients treated with everolimus-based therapy had significantly longer treatment duration than those treated with endocrine monotherapy or chemotherapy, and longer PFS than those treated with endocrine monotherapy. These findings were similar in the first- and second-line settings. Xie et al. [27] conducted a retrospective chart review study in several community oncology practices across the USA to examine the comparative effectiveness of everolimus-based therapy versus endocrine monotherapy among 513 postmenopausal women with HR-positive/HER2-negative mBC. The review included postmenopausal HR-positive/HER2-negative mBC patients who received everolimus-based therapy or endocrine monotherapy as any line of therapy for mBC after NSAI failure. The study evaluated TOT, PFS and time to chemotherapy. In this nationwide sample of postmenopausal HR-positive/HER2-negative mBC patients treated in community oncology settings, treatment with everolimus-based therapy was associated with significantly longer TOT and PFS compared with endocrine monotherapy.
Overall, CER studies most commonly reported treatment duration (e.g., TOT) and various survival outcomes (e.g., OS, PFS, mortality); each reported in at least 71% of these studies. The most common study design was a retrospective chart review, with data acquired most commonly from community-oncology centers.
Overview of treatment patterns studies
Of all the topics we searched, we found the greatest number of studies on treatment patterns in HER2-negative and TN mBC: ten articles [29–38] and eight conference abstracts (Table 4) [39,40,41,42,43,44,45,46]. Ten of these were retrospective chart reviews [29,30,32–34,37,38,41,44,45], two were physician surveys [31,46] and six were analyses of secondary databases (e.g., Surveillance, Epidemiology and End Results [SEER]-Medicare database, commercial claims) [35,36,39,40,42,43]. These studies examined a variety of therapeutic options, including endocrine therapy, chemotherapy and surgery. Most of the studies examined HR-positive/HER2-negative metastatic (or ‘advanced’) breast cancer patients, except for five studies that examined patients with TNBC [29,33,39,41,45].
| Study (year) | Study design | Data source | Primary outcomes | Patients | Treatments |
|---|---|---|---|---|---|
| Clarke et al. (2014) | Retrospective secondary data analysis | California Cancer Registry (6268 pts) | OS | De novo metastatic breast cancer by HER2 (included TNBC) | Breast surgery; full or partial mastectomy; lumpectomy; bilateral mastectomy; chemotherapy; radiation |
| Engel-Nitz et al. (2013) | Retrospective secondary data analysis | Linked medical and pharmacy claims from a large national US health plan with a proprietary clinical cancer database containing physician-reported data (317 pts) | Mortality; length of survival; treatment patterns | HR+/HER2- advanced breast cancer | Endocrine therapy; chemotherapy |
| Faria et al. (2014) | Retrospective chart review | 21 US community oncology practices (173 pts) | TTP; TTF | mTNBC; HER2- mBC | Eribulin mesylate |
| Hao et al. (2013) | Retrospective secondary data analysis | Physician reports linked to medical and pharmacy claims database from a large national US health plan (317 pts) | Treatment sequencing, patterns and duration; mortality | HR+/HER2- advanced breast cancer | Endocrine therapy; chemotherapy |
| Karve et al. (2013) | Retrospective secondary data analysis | SEER-Medicare database (13,170 pts) | Treatment patterns; survival | HR+/HER2- mBC women ≥65-year-old | Surgery; radiation; hormone therapy (megestrol; anastrazole; fulvestrant); chemotherapy (cyclophosphamide; doxorubicin; paclitaxel) |
| Koshy et al. (2010) | Retrospective chart review | Louisiana State University Health Sciences Center (17 pts) | PFS; OS | mBC (including TNBC) | Cisplatin–gemcitabine chemotherapy |
| Krook et al. (2013) | Retrospective chart review | Community oncologists in southeast USA (205 pts) | Treatment patterns | HR+/HER2- stage IV mBC | Anthracyclines |
| Li et al. (2015) | Retrospective chart review | Data from community-based oncologists and hematologists (699 pts) | Everolimus treatment patterns; reasons for prescribing everolimus | Postmenopausal HR+/HER2- mBC; failed nonsteroidal aromatase inhibitor | Everolimus; endocrine therapy; chemotherapy |
| Lin et al. (2015) | Physician survey | 213 community-based oncologists/hematologists from a nationwide online panel (1323 pts) | Treatment patterns; survival | Postmenopausal, stage IV, HR+/HER2- mBC women | Endocrine therapy or chemotherapy |
| Macalad et al. (2015) | Retrospective chart review | Network of community-based oncology practices (144 pts) | Treatment patterns and durations by lines of treatment | HR+/HER2- mBC | Endocrine therapy or chemotherapy |
| Morris et al. (2012) | Retrospective chart review | Memorial Sloan-Kettering Cancer Center (298 pts) | OS; treatment patterns; incidence of brain metastases | mTNBC | Radiotherapy, surgery, systemic chemotherapy |
| Pahuja et al. (2014) | Retrospective chart review | Magee Women's Breast Cancer Program at University of Pittsburgh (86 pts) | TTR; TTP | TNBC pts that did not receive pCR after NAC | Anthracycline and taxane-based NAC |
| Patt et al. (2014) | Physician survey | US oncology network physicians (104 physicians) | nab-Paclitaxel utilization, toxicity, frequency, management, duration | HER2- mBC | Nab-Paclitaxel |
| Seah et al. (2014) | Retrospective chart review | Dana-Farber Cancer Institute (318 pts) | Treatment patterns; duration of chemotherapy; OS | HR+/HER2- mBC | Adjuvant/NAC, endocrine therapy or anti-HER2 therapy |
| Swallow et al. (2014) | Retrospective secondary data analysis | Truven Health MarketScan Commercial and Medicare Supplemental health insurance claims databases (19,120 pts) | Treatment patterns and durations by lines of treatment | HR+/HER2- mBC | Endocrine therapy or chemotherapy |
| Vaz-Luis et al. (2015) | Retrospective secondary data analysis of Medicare data | SEER-Medicare data (4364 pts) | OS; treatment utilization; time to treatment initiation | ≥66-year-old women with mBC with first invasive breast cancer diagnosed 1998–2009, by HER2 (included HER2-) | Received versus did not receive trastuzumab |
| Xie et al. (2015) | Retrospective chart review | 188 physicians from community-based oncology practices contributed data (699 pts) | PFS; TOT; OS | Postmenopausal women, HR+/HER2- mBC | Endocrine therapy or chemotherapy |
| Zeichner et al. (2015) | Retrospective chart review | Medical records from a large breast cancer oncology private practice and a second dataset from the UM/SCCC tumor database (153 pts) | OS | mBC by HER2 status (included HER2-) | Chemotherapy, hormone therapy reported as observed |
HR+: Hormone receptor-positive; mBC: Metastatic breast cancer; mTNBC: Metastatic triple-negative breast cancer; NAC: Neoadjuvant chemotherapy; OS: Overall survival; pCR: Pathological complete response rate; PFS: Progression-free survival; pts: Patients; TNBC: Triple-negative breast cancer; TOT: Time on treatment; TTF: Time to treatment failure; TTP: Time to progression; TTR: Time to local or distant recurrence; UM/SCCC: University of Miami/Sylvester Comprehensive Cancer Center.
Seah et al. [34] examined the use and duration of chemotherapy in 318 patients with mBC according to line of therapy and tumor subtype (HR-positive, TN or HER2-negative amplified breast cancer). Data were from medical records of patients with mBC at Dana-Farber Cancer Institute. Median OS was 32 months: 54 months for HER2-positive disease, 36 months for HR-positive and 17 months for TNBC. Overall, tumor subtypes influenced the number of lines, duration of chemotherapy and survival. Morris et al. [33] retrospectively assessed OS, patterns of recurrence, treatment and incidence of brain metastases in 1323 patients with TNBC, using data from patient medical records at a single institution. A total of 298 (23%) patients developed metastases. Of these patients, 240 had died, which resulted in a crude death rate of 81%. The median OS from the time of metastatic disease diagnosis for the 298 patients with metastatic disease was 14 months (95% CI: 13–16 months). Of 1323 patients, 99 (7.5%) patients developed brain metastases. Following brain metastasis, observed treatments were radiotherapy (88%), resection (26%) and systemic chemotherapy (71%). The median survival from diagnosis of brain metastasis in mTNBC was 5 months. Li et al. [30] conducted a retrospective chart review of 699 postmenopausal HR-positive/HER2-negative mBC women who received everolimus, endocrine therapy or chemotherapy after a NSAI failure, with data from community-based oncology practices across the USA. The study aim was to examine the factors associated with everolimus use in these patients in the real-world setting. The top reason for prescribing everolimus was efficacy (69–85%). About 15 and 29% of everolimus users in second-line and third-line or above received prior chemotherapy. Exemestane was the most common concomitant therapy with everolimus (56–87%). The majority of patients used everolimus according to the labeled combination and dose. This study indicated that in HR-positive/HER2-negative mBC, everolimus is used in more severe (e.g., metastasis, tumor volume and performance status) patients than endocrine therapy but in less severe patients than chemotherapy. Lin et al. [31] assessed physicians’ preferences and self-reported prescribing patterns for endocrine therapy and chemotherapy in the treatment of HR-positive/HER2-negative mBC at community practices. Data were from a survey of 213 physicians from small/intermediate practices; of which, 58% referred to the National Comprehensive Cancer Network (NCCN) guidelines when treating mBC. Survey results suggested that after first-line endocrine therapy, mono- or combination-endocrine therapy was commonly used for second- and third-line treatments and chemotherapy monotherapy for third- or later-line treatments. Chemotherapies were used in early lines for patients with visceral symptoms. Efficacy was the most important factor for treatment choice. Karve et al. [43] reported the treatment patterns and survival of 13,170 women aged ≥65 years diagnosed with HR-positive/HER-negative mBC based on the SEER-Medicare linked database (2000–2009). 54% of patients had surgery, followed by radiation (50%), hormone therapy (49%) and chemotherapy (40%). Of patients treated with hormonal therapy, 20% received megestrol, 16% received anastrazole and 11% had fulvestrant. Most commonly used chemotherapy agents were cyclophosphamide (21%), doxorubicin (17%) and paclitaxel (14%). Patients in this study had a median OS of 50 months; the 5-year survival rate was 45%. The authors found that survival remains lower in older and ER-/PR+ mBC despite advances in treatment. Krook et al. [44] described the patterns of use of anthracyclines in a community setting among 247 patients with HER2+ and HER2-negative stage IV mBC. Of 420 unique chemotherapy requests in these patients, 54 were anthracycline requests (50 patients); 357 of these requests were for treatment of 205 HER2-negative mBC patients. Approximately 83% of anthracycline requests were for conventional doxorubicin, while the rest were for liposomal doxorubicin. This analysis shows that anthracyclines are primarily used in HER2-negative mBC in the southeast USA, with use occurring in about one out of four patients. Patt et al. [46] analyzed data from a US oncology survey of 104 network physicians to examine the treatment experience of nab-paclitaxel (nab-P) in HER2-negative mBC patients. The 100 mg/m2 every week was the most common first line (51%) and second line (58%) dosage, followed by 125 mg/m2 every week (22 and 14%), 150 mg/m2 every week (4 and 2%) and 260 mg/m2 every three weeks (14 and 7%). Common factors affecting choice of nab-P monotherapy for more and less experienced users included co-morbidities/performance status, quality of prior taxane response, steroid intolerance/contraindications/hypersensitivity, predominant visceral metastases and age. Overall, the study showed that 100 mg/m2 every week nab-P is the most commonly used starting dosage for HER2-negative mBC patients, and peripheral neuropathy and neutropenia were common dose-limiting toxicities. Hao et al. [42] reported patterns of chemotherapy and endocrine therapy use in patients with HR-positive/HER2-negative advanced breast cancer (stage IV or metastases) based on a retrospective analysis of physician-reported clinical data linked to medical and pharmacy claims (2008–2012) from a large national US health plan. Of 317 metastatic patients, 50% started chemotherapy without prior endocrine treatment (CH), 30% received only endocrine therapy (OT), 17% had endocrine therapy prior to chemotherapy and 3% had neither endocrine therapy nor chemotherapy. Of CH patients, 55% of patients later initiated treatment with aromatase inhibitors, compared with 64% of OT patients (p = 0.104). Overall, this study showed that a large proportion of patients with HR-positive/HER2-negative advanced breast cancer initiated chemotherapy without prior endocrine therapy. Engel-Nitz et al. [40] described the mortality outcomes of patients with HR-positive/HER2-negative advanced and mBC based on a retrospective analysis of clinical data linked to medical and pharmacy claims (2008–2012) from a large national US health plan. There were 263 stage III, 71 stage IV and 317 patients with metastases. Of these, 3.4% of stage III, 22.5% of stage IV and 10.7% of metastatic patients died during follow-up (p ≤ 0.010). 1-year mortality also varied by disease stage: 1.1% (stage III), 12.7% (stage IV) and 5.1% (metastatic patients; p < 0.001). Metastatic patients had significantly shorter mean survival if they did not have endocrine treatment prior to chemotherapy versus other metastatic patients: 35.7 versus 76.1 months; a similar pattern was observed for stage IV patients: 10.0 versus 14.8 months. This study showed that mortality rates varied by stage of HR-positive/HER2-negative disease, while length of survival varied by pretreatment with endocrine therapy prior to chemotherapy. Koshy et al. [29] conducted a single institution retrospective chart review study of 36 patients at the Louisiana State University Health Sciences Center to determine if TNBC (n = 17) is preferentially sensitive to platinum therapy as compared with non-TNBC by reviewing the outcomes of patients treated with cisplatin–gemcitabine chemotherapy. The median PFS for TNBC was 5.3 months compared with 1.7 months in non-TNBC. The risk of progression was reduced by 47% for metastatic TNBC (mTNBC) compared with non-TNBC patients treated with the cisplatin–gemcitabine. The median OS after the start of cisplatin–gemcitabine was 10.8 months in TNBC patients compared with 4.3 months in non-TNBC patients. OS from date of breast cancer diagnosis for the TNBC group was 47.8 months compared with 66.8 months in non-TNBC. The authors concluded that cisplatin–gemcitabine combination chemotherapy is an effective regimen for patients with mTNBC. Xie et al. [37] conducted a retrospective chart review study to compare clinical outcomes, PFS, TOT and OS between 699 HR-positive/HER2-negative mBC patients with multiple metastases versus those with a single metastasis. The authors concluded that patients with multiple metastases had significantly shorter PFS, TOT and OS than single metastasis patients, with similar outcomes in each line of therapy, highlighting the substantial clinical burden and unmet need for more efficacious treatments for the former group of patients. Zeichner et al. [38] examined the survival of patients with de novo mBC by retrospectively analyzing breast cancer data from patient records from a large breast cancer oncology private practice (n = 62) and from the University of Miami/Sylvester Comprehensive Cancer Center tumor database (n = 91). The authors also conducted a review of literature. The goal was to assess how advances in treatment have impacted OS. The authors concluded that the median survival for patients with de novo metastatic disease is in excess of 3 years compared with studies reported from prior to 1996. In the HER2-negative subset, the OS was 39 months among the patients in the private practice group and 36 months in the University of Miami/Sylvester Comprehensive Cancer Center group. They were unable to confirm whether survival for de novo metastatic disease is better than for patients with recurrent disease, however, a subset of these patients can have a prolonged survival with good QoL in excess of 10 years. Macalalad et al. [32] collected data from patient charts across a network of community-based oncology practices to describe the treatment patterns and treatment duration by lines of therapy for endocrine therapy and chemotherapy in 144 postmenopausal women with HR-positive/HER2-negative mBC. Considering that clinical guidelines recommend endocrine therapy as initial treatment for postmenopausal HR-positive/HER2-negative mBC women, with chemotherapy reserved for patients that develop symptomatic visceral disease or have no clinical benefit from three lines of endocrine therapy, the authors examined whether real-world clinical practice reflects these recommendations. Of 144 patients in this study, less than 10% had three or more lines of endocrine therapy before chemotherapy was initiated; a median of two lines of endocrine therapy was observed in these patients. The authors observed that few patients received three lines of endocrine therapy as suggested by NCCN guidelines, and concluded that single-agent endocrine therapy may not be as effective beyond first line, given most patients received less than three lines of endocrine therapy before receiving chemotherapy and the median duration of endocrine therapy decreased from first to second line. Swallow et al. [35] evaluated the real-world patterns of endocrine therapy for HR-positive/HER2-negative mBC in 19,120 postmenopausal mBC patients in the USA from 2002 to 2012. The authors examined mean numbers of lines of therapy and median duration of each line using the MarketScan commercial health insurance claims database (2002Q3–2012Q2). Although endocrine therapy is the preferred first-line treatment option in HER-positive/HER2-negative mBC according to guidelines, only 11,545 (60%) patients initiated endocrine therapy as the first treatment following metastatic diagnosis in this study. Most of these patients received only one line of endocrine therapy (n = 8524; 74%) before discontinuation or transition to chemotherapy, and only 821 (7%) patients were treated with three or more lines of endocrine therapy as recommended by the NCCN treatment guidelines. Overall, patients were treated with a mean of 1.36 lines of endocrine therapy during the study period. In patients that were treated with more than one line of endocrine therapy, the duration of this therapy decreased with each subsequent line. Vaz-Luis et al. [36] conducted a secondary database analysis of Medicare data to examine the impact of race on survival of 4364 women ≥66-year old with de novo mBC by disease subtype. The investigators used trastuzumab as a proxy for HER2-positive status. Patients with HER2-positive disease experienced longer median OS compared with HER2-negative/unknown/HR-positive and HER2-negative/unknown/HR-negative disease. Racial differences in OS were only observed among patients with HER2-positive tumors. Results for breast cancer-specific survival were similar. Overall, racial differences in survival were only apparent for those with inferred HER2-positive tumors. In a chart review of 173 patients, Faria et al. [41] compared time to treatment progression and time to treatment failure in mBC patients with TN disease versus those with ER-positive/HER2-negative mBC receiving eribulin therapy. The authors concluded that in these heavily pretreated HER2-negative mBC patients, treated in a community oncology setting, patients with TNBC achieved similar treatment benefit from eribulin therapy compared with the ER-positive/HER2-negative cohort. Clarke et al. [39] examined 6268 de novo mBC patients by HER2 subtypes in California. The authors found that a high proportion of patients with mBC are not treated surgically and that survival remains poor, with worse survival strongly associated with tumor biology (TN and HR-negative/HER2-positive molecular subtypes). Pahuja et al. [45] retrospectively examined medical charts of 117 TNBC patients to assess responses to subsequent therapies after failure to achieve pathologic complete response after neoadjuvant chemotherapy in patients with TNBC. The authors determined that response to subsequent chemotherapeutic regimens in mTNBC patients who do not achieve pathologic complete response to anthracycline and taxane-based neoadjuvant chemotherapy is limited.
Overall, treatment patterns studies varied both by methodology and objectives. The most common end points examined were treatment patterns and survival. Most common data sources used included physician reports and medical records from cancer centers and university hospitals. We found that most, but not all, patients with HR-positive/HER2-negative disease are treated with at least one line of endocrine therapy. Beyond first line, multiple regimens may be used. Studies often reported that most important factor for treatment choice was efficacy. Unlike for HR-positive/HER2-negative mBC, real-world treatment patterns data in TN mBC are limited.
Overview of treatment appropriateness & navigation research
Treatment appropriateness was addressed by one study, in terms of patient treatment navigation (Table 5) [47]. Ko et al. [47] examined whether patient navigation improved receipt of recommended breast cancer care. In this study, women with breast cancer who participated in the national Patient Navigation Research Program were examined to determine whether the care they received included: initiation of antiestrogen therapy in patients with HR-positive breast cancer; initiation of postlumpectomy radiation therapy; and initiation of chemotherapy in women less than 70-year-old with TN tumors greater than 1 cm. Due to small sample size and limited variation in the receipt of recommended chemotherapy treatment, the authors were unable to assess the relationship between patient navigation and chemotherapy, and concluded that the value of the addition of a navigator is inconclusive from the available data. Overall, studies on treatment appropriateness were limited for TNBC, considering the single study identified was inconclusive for TNBC patients due to a small sample size [47].
| Study (year) | Study design | Data source | Primary outcomes | Patients | Treatments |
|---|---|---|---|---|---|
| Ko et al. (2014) | Secondary database analysis | Data from National Cancer Institute- and American Cancer Society-sponsored Patient Navigation Research Program, at eight research centers (158 patients) | Quality of care: i.e., receipt of recommended standard breast cancer care. | TNBC, tumors >1 cm, age <70 years | Chemotherapy |
TNBC: Triple-negative breast cancer.
Overview of QoL research
Only two full-length articles were identified that reported QoL in mBC patients (Table 6) [48,49]. Both studies examined HER2-negative mBC but QoL measures reported varied widely, including overall QoL (using Patient Care Monitor [PMC]), symptom burden, treatment satisfaction and the use of the Functional Assessment of Cancer Therapy-Breast.
| Study (year) | Study design | Data source | Primary outcomes | Patients | Treatments |
|---|---|---|---|---|---|
| Gupta et al. (2014) | Patient survey | Patient survey (200 USA pts) | Health-related quality of life (FACT-B), treatment satisfaction and daily productivity loss | Postmenopausal ≥50-year-old HR+/HER2- mBC women | Chemotherapy or hormonal therapy |
| Walker et al. (2011) | Retrospective chart review | Seven community-based oncology practices (102 pts) | Symptom burden; health-related quality of life (PMC version 2.0) | ≥18-year-old, stage IV, HER2- mBC women | Surgery, radiation, neoadjuvant/adjuvant therapy, hormonal therapy, chemotherapy |
FACT-B: Functional assessment of cancer therapy-breast; HR: Hormone receptor; mBC: Metastatic breast cancer; PMC: Patient care monitor; pts: Patients.
Walker et al. [48] conducted a retrospective chart review study to evaluate the impact of disease progression and of specific sites of metastasis on patient reported outcomes in 102 women with HER2-negative mBC from seven community oncology practices. The study used PMC assessments, a self-report measure of symptom burden and QoL, which was administered as part of routine care. PMC assessments of fatigue, physical pain and trouble sleeping were sensitive to effects of disease progression. Progression was also associated with worsening of physical symptoms, treatment side effects, acute distress and impaired performance scores. Gupta et al. [49] examined the association of chemotherapy versus hormonal therapy on health outcomes among patients with HR-positive, HER2-negative mBC. Data came from a cross-sectional survey of postmenopausal women (200 from the USA; 160 from EU) aged ≥50 years with HR-positive, HER2-negative mBC, undergoing treatment with hormonal therapy or chemotherapy for ≤1 year. Measures included cancer therapy satisfaction questionnaire, Functional Assessment of Cancer Therapy-Breast and work and productivity loss impairment items. Hormonal therapy was associated with better patient-reported outcomes, including better health-related QoL, greater satisfaction with treatment, better feelings about side effects, less bother with treatment side effects and activity impairment and lower family burden, than chemotherapy in first line mBC.
Overall, studies that reported QoL research were based on validated questionnaires and instruments, and included assessments of patient reported outcomes to be able to understand QoL from the patient's perspective. The two QOL studies not only varied in study designs (one was a patient survey and the other a retrospective chart review) but in patient populations, where one study examined ≥50-year-old patients and the other ≥18-year-old patients with HER2-negative mBC.
Overview of cost studies
Findings on costs were reported by three articles [50–52] and two conference abstracts (Table 7) [53,54]. These studies varied in aims, designs, data sources and therapies: for example, three were cost–effectiveness analyses [50,51,54], one study was a budget impact model [52] and one study was a retrospective secondary database analysis [53]. All patients examined were women with HER-negative mBC.
| Reference | Study design | Data source | Primary outcomes | Patients | Treatments |
|---|---|---|---|---|---|
| Diaby et al. (2014) | CEA | BOLERO-2 trial; cost from the Center for Medicare Services drug payment table and physician fee schedule (in 2013 US$); costs/use associated with AEs were from published literature | Incremental cost–effectiveness ratio | Postmenopausal HR+/HER2- mBC | Everolimus plus exemestane versus exemestane alone |
| Pawaskar et al. (2013) | Retrospective secondary data analysis | SEER-Medicare database (13,170 patients) | All-cause and mBC-related annual healthcare utilization and cost | HR+/HER2- mBC women aged ≥65 years old | Not specified |
| Refaat et al. (2014) | CEA | E2100 trial; cost from the Center for Medicare Services drug payment table and physician fee schedule | Incremental cost–effectiveness ratio | HER2- mBC, chemotherapy-naive, women | Bevacizumab plus paclitaxel versus paclitaxel alone as first line chemotherapy |
| Xie et al. (2013) | Budget impact model | Model input sources included US Census 2010, SEER, literature, WAC | Budget impact for the first year of everolimus entry | HR+/HER2- advance breast cancer | Everolimus |
| Zeichner et al. (2013) | CEA | Data form BOLERO-2 Phase III trial; costs from Center for Medicare Services drug payment table and physician fee schedule | Incremental cost–effectiveness ratio | Postmenopausal HR+/HER2- mBC | Everolimus plus exemestane versus exemestane alone |
AE: Adverse event; CEA: Cost–effectiveness analysis; HR: Hormone receptor; mBC: Metastatic breast cancer; SEER: Surveillance, Epidemiology and End Results; WAC: Whole sale acquisition cost.
Pawaskar et al. [53] assessed the cost and healthcare utilization burden in HER2-negative, HR-positive, ≥65-year-old women with mBC using the SEER-Medicare Database (2000–2009). The study focused on patients who were not part of a health maintenance organization but who had continuous Medicare (Parts A and B) enrollment for ≥12 months before the date of mBC diagnosis or progression or 2009. The main end points examined were incremental cost–effectiveness ratio, all-cause and mBC-related annual healthcare utilization and costs, and budget impacts. Among 13,170 study patients, the mean number of hospitalizations was 2.5 and emergency department visits were three. Mean (standard deviation) annual all-cause costs per patient were US$34,264 (US$33,429), of which US$16,397 (US$18,284) were attributable to mBC. The authors found hospitalizations, hospital outpatient visits and physician office visits accounted for over three-quarters of total all-cause costs and 75% of mBC-related costs. Of mBC-related costs, mean (standard deviation) annual costs were US$1442 (US$4095) for chemotherapy, US$1872 (US$4086) for radiation and US$579 (US$1197) for hormone therapy. Xie et al. [52] conducted an analysis to estimate the budget impact of everolimus as the first and second treatment option after letrozole or anastrozole failure for postmenopausal women with HR-positive/HER2-negative advanced breast cancer. The study found that introduction of everolimus in combination with exemestane is projected to increase the pharmacy budget while reducing medical service expenditures, yielding a modest net increase of US$522,336 in total budget for the first year from a US payer perspective. Diaby et al. [50] conducted a cost–effectiveness analysis (CEA) of everolimus plus exemestane versus exemestane alone for treatment of HR-positive/HER2-negative mBC. Using the BOLERO-2 data and costs obtained from the Center for Medicare Services drug payment table and physician fee schedule, the benefits were expressed as quality-adjusted PFS weeks and quality-adjusted progression-free years, with utilities/disutilities derived from the literature. Considering an estimated incremental cost–effectiveness ratio (ICER) of US$265,498.5/quality-adjusted progression-free years, the authors concluded that everolimus plus exemestane is not cost-effective compared with exemestane alone. Zeichner et al. [54] conducted a CEA of everolimus in combination with exemestane versus exemestane alone in postmenopausal women with HR-positive/HER2-negative mBC, using the BOLERO-2 trial data, utilities derived from literature and costs obtained from the Center for Medicare Services drug payment table and physician fee schedule (US$2012). The main end points and corresponding results were overall cost of US$62,751.54 per year of PFS gained and an ICER of US$79,376/quality-adjusted life year, and by local assessment an overall cost of US$83,222 per year of PFS gained with an ICER of US$108,131/quality-adjusted life year. The authors concluded that everolimus plus exemestane versus exemestane alone is cost-effective in the treatment of mBC. Refaat et al. [51] conducted a CEA of bevacizumab plus paclitaxel versus paclitaxel alone as first-line chemotherapy in HER2-negative mBC using efficacy and toxicity data from the E2100 study. This study demonstrated that, despite a significant PFS advantage, the addition of bevacizumab to paclitaxel is not cost-effective (marginal cost–effectiveness was US$232,721) in comparison to paclitaxel given alone for the cohort of patients with HER2-negative mBC.
Overall, the cost studies reported a variety of results in HER2-negative mBC patients. Most cost studies were economic models, specifically cost–effectiveness models and the most common end points were ICERs. Data were derived from a variety of sources including the published literature, clinical trials and Center for Medicare Services.
Discussion
We found that the most abundant literature was on treatment patterns, followed by CER studies, and studies of costs, QoL and treatment appropriateness. The majority of studies examined patients with HER2-negative mBC, although specific subject inclusion criteria varied: for example, postmenopausal women, chemotherapy-naive patients, advance breast cancer patients, ≥50-year-old and ≥18-year-old patients. Only a few studies examined patients with TN mBC. Overall, this analysis found that outcomes research in mBC has increased over time, with two studies published in 2010, one in 2011, one in 2012, eight in 2013, ten in 2014, ten in 2015 and one as of January 2016. With the passage of the 21st Century Cures Act, and the FDA developing a program to evaluate the potential use of RWD in regulatory decisions, we anticipate publications using RWD for outcomes research in healthcare will continue to grow [55].
The majority of the included CER and treatment patterns studies were retrospective chart reviews (six CER and ten treatment patterns studies), others were retrospective secondary database analyses (one CER and six treatment patterns studies) and physician surveys (two treatment patterns studies). RWD sources included commercial insurance claims, SEER-Medicare and the California Cancer Registry data. 18 studies reported results in patients with HER2-negative mBC, and seven reported in TNBC patients. Primary end points included OS, PFS and treatment duration. In the CER studies, the most commonly reported outcomes were related to treatment duration and various survival measures (e.g., OS, PFS), reported in 71–86% of the studies. Treatment patterns studies also most commonly examined survival outcomes (61% of studies), in addition to a variety of treatment patterns or duration-related outcomes. Treatment patterns studies reported that most, but not all, patients with HR-positive/HER2-negative disease are treated with at least one line of endocrine therapy. Studies on QoL included specific instruments to measure patient-reported outcomes, which is an important consideration in treatment selection. The cost studies identified in this review varied widely in research objectives and methods, but consisted mostly of economic models. Finally, real-world clinical treatment patterns of endocrine therapy use indicate that there is room to improve concordance with targets recommended by guidelines for patients with HR-positive/HER2-negative mBC.
This study is not without limitations. Considering the increasing publication trend of RWD research in mBC over the past years, an update to the current review may be necessary in the near future. Although this was a rigorous systematic literature review on multiple broad research topics using RWD in mBC, a search of different literature databases and implementation of different search terms, search strings and timeframes may have yielded somewhat different results. Finally, as this study only focused on US data, future literature reviews should consider summarizing global findings on the topic.
Conclusion
Outcomes research in patients with HER2-negative mBC in the USA varies with respect to study design and objectives. Of all study designs, there was a dearth of literature on QoL, costs and treatment appropriateness in these patient populations; yet, this review suggests that as the availability of RWD has increased, the number of published CER and treatment patterns studies has also increased, and may continue to grow with the implementation of new policy programs. Given the paucity of studies on each of the topics examined in this review, it is difficult to draw summary conclusions. Research analyzing outcomes in TN mBC patients was particularly limited, indicating opportunities to generate real-world evidence in this high unmet need population.
Future perspective
There is limited availability of published evidence based on RWD examining CER, treatment patterns, QoL and costs in mBC, focusing on HER2-negative and TN subtypes. Future research perspective in this area should encompass further real-world research in these patients.
With the passage of the 21st Century Cures Act in 2016 and the abundance of healthcare data collected via electronic health records and insurance claims, the potential of outcomes research in oncology using real-world data is being widely acknowledged in the USA. To better understand the extent and study characteristics of current outcomes research related to HER2-negative and triple-negative (TN) metastatic breast cancer (mBC), we conducted a systematic literature review to summarize the recent publications on comparative effectiveness research, treatment patterns and appropriateness, quality of life and costs in these patients.
Methods
We searched PubMed and four online conference databases using MeSH/keywords to identify relevant literature.
Comparative effectiveness research
Six full length articles and one conference abstract were included; studies most commonly reported treatment duration and various survival outcomes.
Treatment patterns studies
The greatest number of studies were found on treatment patterns (ten articles and eight conference abstracts); studies varied in both methodology and objectives.
Studies show that most, but not all patients, with hormone receptor (HR)-positive/HER2-negative disease are treated with at least one line of endocrine therapy. Beyond first line, multiple regimens may be used.
Treatment appropriateness & navigation research
Only one study was found on treatment appropriateness; the authors of the study were unable to assess the relationship between patient navigation and chemotherapy due to small sample size.
Quality of life research
Only two studies were identified; studies indicated that progressive disease is associated with worsening of symptoms, that symptom severity may partly depend on the organ systems affected by metastatic disease and that hormone therapy compared with chemotherapy results in better patient-reported outcomes.
Cost studies
Five studies (three articles and two abstracts) were included and reported different results. One concluded that HR-positive/HER2-negative elderly women with mBC have a substantial economic burden on the Medicare system. The budget impact analyses showed that for postmenopausal patients with HR-positive/HER2-negative advance breast cancer and history of failed letrozole or anastrozole therapy, treatment with everolimus in combination with exemestane may result in a modest net increase in total budget from a US payer perspective. The three cost–effectiveness studies included in this review examined different end points and varied in methods.
Discussion/conclusion
Outcomes research in HER2-negative mBC in the USA was limited, specifically among TN patients, indicating an opportunity for further research in this high unmet need population.
Financial & competing interests disclosure
M Parisi and C Pelletier are employees of the Celgene Corporation. D Cherepanov and M Broder are employees of Partnership for Health Analytic Research, LLC a health services research company paid by the Celgene Corporation to conduct this research. Funding for this study was provided by Celgene Corporation. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest
1.
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J. Clin. 66(1), 7–30 (2016).
2.
Clark O, Botrel TE, Paladini L, Ferreira MB. Targeted therapy in triple-negative metastatic breast cancer: a systematic review and meta-analysis. Core Evid. 9, 1–11 (2014).
3.
Lin NU, Vanderplas A, Hughes ME et al. Clinicopathologic features, patterns of recurrence, and survival among women with triple-negative breast cancer in the National Comprehensive Cancer Network. Cancer 118(22), 5463–5472 (2012).
4.
National Cancer Institute. SEER Cancer Statistics Review, 1975–2013 (2016). http://seer.cancer.gov/csr/1975_2013/.
5.
National Cancer Institute. Surveillance, Epidemiology, and End Results Program (SEER) cancer statistics factsheets: female breast cancer (2016). http://seer.cancer.gov/statfacts/html/breast.html.
6.
Redig AJ, McAllister SS. Breast cancer as a systemic disease: a view of metastasis. J. Intern. Med. 274(2), 113–126 (2013).
7.
O'Shaughnessy J. Extending survival with chemotherapy in metastatic breast cancer. Oncologist 10(Suppl. 3), 20–29 (2005).
8.
Bauer KR, Brown M, Cress RD, Parise CA, Caggiano V. Descriptive analysis of estrogen receptor (ER)-negative, progesterone receptor (PR)-negative, and HER2-negative invasive breast cancer, the so-called triple-negative phenotype: a population-based study from the California cancer Registry. Cancer 109(9), 1721–1728 (2007).
9.
Partridge AH, Rumble RB, Carey LA et al. Chemotherapy and targeted therapy for women with human epidermal growth factor receptor 2-negative (or unknown) advanced breast cancer: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 32(29), 3307–3329 (2014).
10.
Rakha EA, El-Sayed ME, Green AR, Lee AHS, Robertson JF, Ellis IO. Prognostic markers in triple-negative breast cancer. Cancer 109, 25–32 (2007).
11.
Yabroff KR, Lund J, Kepka D, Mariotto A. Economic burden of cancer in the United States: estimates, projections, and future research. Cancer Epidemiol. Biomarkers Prev. 20(10), 2006–2014 (2011).
12.
Mariotto AB, Yabroff KR, Shao Y, Feuer EJ, Brown ML. Projections of the cost of cancer care in the United States: 2010–2020. J. Natl Cancer Inst. 103(2), 117–128 (2011).
13.
Reed E, Simmonds P, Haviland J, Corner J. Quality of life and experience of care in women with metastatic breast cancer: a cross-sectional survey. J. Pain Symptom Manage. 43(4), 747–758 (2012).
14.
Smith AW, Reeve BB, Bellizzi KM et al. Cancer, comorbidities, and health-related quality of life of older adults. Health Care Financ. Rev. 29(4), 41–56 (2008).
15.
Kent EE, Malinoff R, Rozjabek HM et al. Revisiting the Surveillance Epidemiology and End Results Cancer Registry and Medicare Health Outcomes Survey (SEER-MHOS) linked data resource for patient-reported outcomes research in older adults with cancer. J. Am. Geriatr. Soc. 64(1), 186–192 (2016).
16.
Foster TS, Miller JD, Boye ME, Blieden MB, Gidwani R, Russell MW. The economic burden of metastatic breast cancer: a systematic review of literature from developed countries. Cancer Treat. Rev. 37(6), 405–415 (2011).
17.
Skrepnek GH. Health economic and outcomes research in cancer. In: Supportive Cancer Care. Alberts D, Lluria-Prevatt M, Kha S et al. (Eds). Springer International Publishing, Cham, Switzerland, 291–316 (2016).
18.
Centers for Medicare & Medicaid Services (CMMS). Oncology care model (2017). https://innovation.cms.gov/initiatives/Oncology-Care/.
19.
U.S. National Library of Medicine at the National Institutes of Health. Health Services Research (HSR) PubMed queries (2016). www.nlm.nih.gov/nichsr/hedges/search.html.
20.
National Cancer Institute. FDA approval for everolimus (2013). www.cancer.gov/about-cancer/treatment/drugs/fda-everolimus.
21.
Evidence Partners Incorporated. DistillerSR (Version 2.0) (2015). http://systematic-review.ca.
22.
Dawood S, Broglio K, Buzdar AU, Hortobagyi GN, Giordano SH. Prognosis of women with metastatic breast cancer by HER2 status and trastuzumab treatment: an institutional-based review. J. Clin. Oncol. 28(1), 92–98 (2010).
23.
Dranitsaris G, Gluck S, Faria C, Cox D, Rugo H. Comparative effectiveness analysis of monotherapy with cytotoxic agents in triple-negative metastatic breast cancer in a community setting. Clin. Ther. 37, 134–144 (2015).
• Eribulin was used as a later line of therapy and was reported to have had comparable drug activity and tolerability versus other cytotoxic agents in patients with metastatic triple-negative breast cancer in a community oncology setting.
24.
Li N, Hao Y, Xie J et al. Everolimus-based therapy versus chemotherapy among patients with HR+/HER2- metastatic breast cancer: comparative effectiveness from a chart review study. Int. J. Breast Cancer 2015, 240750 (2015).
25.
Li N, Hao Y, Kageleiry A et al. Time on treatment of everolimus and chemotherapy among postmenopausal women with HR+/HER2- metastatic breast cancer: a retrospective claims study in the US. Curr. Med. Res. Opin. 32(2), 385–394 (2016).
• Analyses of large US insurance claim databases revealed that hormone receptor (HR)-positive/HER2-negative metastatic breast cancer (mBC) patients receiving everolimus had significantly longer time on treatment than those on chemotherapy.
26.
Lin PL, Hao Y, Xie J et al. Real-world effectiveness of everolimus-based therapy versus endocrine monotherapy and chemotherapy in patients of HR+/HER2- breast cancer with liver metastasis in the USA. Expert Opin. Pharmacother. 16, 2101–2111 (2015).
27.
Xie J, Hao Y, Li N et al. Comparative effectiveness of everolimus-based therapy versus endocrine monotherapy among postmenopausal women with HR+/HER2- metastatic breast cancer: a retrospective chart review in community oncology practices in the US. Curr. Med. Res. Opin. 31, 1095–1103 (2015).
28.
Dranitsaris G, Tripathy D, Beegle NL, Kalberer TL, Cox JD, Faria C. Real-world analysis of eribulin in metastatic breast cancer (MBC): an assessment of time to treatment failure (TTF) in a community oncology setting. Presented at: ASCO 2013 Breast Cancer Symposium. San Francisco, CA, USA, 7–9 September 2013.
29.
Koshy N, Quispe D, Shi R, Mansour R, Burton GV. Cisplatin–gemcitabine therapy in metastatic breast cancer: improved outcome in triple negative breast cancer patients compared with non-triple negative patients. Breast 19(3), 246–248 (2010).
30.
Li N, Hao Y, Xie J et al. Everolimus use and associated factors among post-menopausal women with hormonal receptor positive/human epidermal growth factor receptor 2 negative metastatic breast cancer. Curr. Med. Res. Opin. 31(8), 1573–1582 (2015).
• This retrospective chart review study of community-based oncology practices indicates that in HR-positive/HER2-negative mBC, everolimus is used in more severe patients than endocrine therapy but in less severe patients than chemotherapy.
31.
Lin PL, Hao Y, Xie J et al. Physician experiences and preferences in the treatment of HR+/HER2- metastatic breast cancer in the United States: a physician survey. Cancer Med. 5(2), 209–220 (2015).
• A survey of physicians suggested that after first-line endocrine therapy, mono- or combination-endocrine therapy was commonly used for second- and third-line treatments and chemotherapy monotherapy for third or later line treatments for HR-positive/HER2-negative metastatic breast cancer; efficacy was the most important factor for treatment choice.
32.
Macalalad AR, Hao Y, Lin PL et al. Treatment patterns and duration in post-menopausal women with HR+/HER2- metastatic breast cancer in the US: a retrospective chart review in community oncology practices (2004–2010). Curr. Med. Res. Opin. 31, 263–273 (2015).
33.
Morris PG, Murphy CG, Mallam D et al. Limited overall survival in patients with brain metastases from triple negative breast cancer. Breast J. 18, 345–350 (2012).
34.
Seah DS, Luis IV, Macrae E et al. Use and duration of chemotherapy in patients with metastatic breast cancer according to tumor subtype and line of therapy. J. Natl Compr. Canc. Netw. 12(1), 71–80 (2014).
35.
Swallow E, Zhang J, Thomason D, Tan RD, Kageleiry A, Signorovitch J. Real-world patterns of endocrine therapy for metastatic hormone-receptor-positive (HR+)/human epidermal growth factor receptor-2-negative (HER2-) breast cancer patients in the United States: 2002–2012. Curr. Med. Res. Opin. 30, 1537–1545 (2014).
36.
Vaz-Luis I, Lin NU, Keating NL et al. Racial differences in outcomes for patients with metastatic breast cancer by disease subtype. Breast Cancer Res. Treat. 151, 697–707 (2015).
• An analysis of Medicare data of ≥66-year-old women with de novo mBC indicated that patients with HER2-positive disease experienced longer median overall survival compared with HER2-negative disease; racial differences in overall survival were observed in patients with HER2-positive tumors.
37.
Xie J, Hao Y, Li N et al. Clinical outcomes among HR+/HER2- metastatic breast cancer patients with multiple metastatic sites: a chart review study in the US. Exp. Hematol. Oncol. 4, 31 (2015).
38.
Zeichner SB, Herna S, Mani A et al. Survival of patients with de-novo metastatic breast cancer: analysis of data from a large breast cancer-specific private practice, a university-based cancer center and review of the literature. Breast Cancer Res. Treat. 153, 617–624 (2015).
39.
Clarke CA, Chu L, Tao L et al. Characteristics of de novo metastatic breast cancer in California, 2005–2011. Presented at: Thirty-Seventh Annual CTRC-AACR San Antonio Breast Cancer Symposium. San Antonio, TX, USA, 9–13 December 2014.
40.
Engel-Nitz NM, Hao Y, Gomez Rey G, Sullivan J, Willemann Rogerio J. Survival among patients with hormone receptor positive (HR+)/human epidermal growth factor receptor 2 negative (HER2-) advanced breast cancer: a real-world observational study. Presented at: Thirty-Sixth Annual CTRC-AACR San Antonio Breast Cancer Symposium. San Antonio, TX, USA, 10–14 December 2013.
41.
Faria C, Jackson J, Lunacsek O, Hennenfent KL. Time to progression and time to treatment failure in patients with triple-negative metastatic breast cancer receiving eribulin mesylate in a community oncology setting. Presented at: 2014 ASCO Annual Meeting. Chicago, IL, USA, 30 May–3 June 2014.
42.
Hao Y, Engel-Nitz NM, Sullivan J, Henk HJ, Willemann Rogerio J, Newcomer L. Chemotherapy and endocrine therapy treatment patterns among patients with hormone receptor positive (HR+)/HER2 negative advanced breast cancer. Presented at: Thirty-Sixth Annual CTRC-AACR San Antonio Breast Cancer Symposium. San Antonio, TX, USA, 10–14 December 2013.
43.
Karve S, Pawaskar M, Davis KL, Dalvi T, Deeter R. Treatment patterns and survival in elderly women with HER2-negative, hormone receptor positive metastatic breast cancer: analysis of the SEER-Medicare database. Presented at: 2013 ASCO Annual Meeting. Chicago, IL, USA, 31 May–4 June 2013.
44.
Krook JE, Kumar A, Fishman ML et al. Community use of anthracyclines in metastatic breast cancer (MBC). Presented at: 2013 ASCO Annual Meeting. Chicago, IL, USA, 31 May–4 June 2013.
45.
Pahuja S, McGuire K, Davidson N et al. [P3–11–10] Response to subsequent therapies after failure to achieve pathologic complete response (pCR) after neo-adjuvant chemotherapy (NAC) in patients (pts) with triple negative breast cancer (TNBC). Presented at: Thirty-Seventh Annual CTRC-AACR San Antonio Breast Cancer Symposium. San Antonio, TX, USA, 9–13 December 2014.
46.
Patt DA, Richardson P, Rembert D, Corzo D, Chen C. Treatment of patients (pts) with HER2- metastatic breast cancer (MBC) with nab-paclitaxel (nab-P) in the clinical practice setting – results of a US oncology survey. Presented at: 2014 ASCO Annual Meeting. Chicago, IL, USA, 30 May–3 June 2014.
47.
Ko NY, Darnell JS, Calhoun E et al. Can patient navigation improve receipt of recommended breast cancer care? Evidence from the National Patient Navigation Research Program. J. Clin. Oncol. 32, 2758–2764 (2014).
• Due to small sample size and limited variation in the receipt of recommended chemotherapy treatment, the authors were unable to assess the relationship between patient navigation and chemotherapy, concluding that the value of the addition of a navigator is inconclusive from available data.
48.
Walker MS, Hasan M, Yim YM, Yu E, Stepanski EJ, Schwartzberg LS. Retrospective study of the effect of disease progression on patient reported outcomes in HER-2 negative metastatic breast cancer patients. Health Qual. Life Outcomes 9, 46 (2011).
49.
Gupta S, Zhang J, Jerusalem G. The association of chemotherapy versus hormonal therapy and health outcomes among patients with hormone receptor-positive, HER2-negative metastatic breast cancer: experience from the patient perspective. Expert Rev. Pharmacoecon. Outcomes Res. 14(6), 929–940 (2014).
• A cross-sectional survey of postmenopausal women with hormone receptor-positive, HER2-negative mBC revealed that hormonal therapy was associated with better patient-reported outcomes than chemotherapy.
50.
Diaby V, Adunlin G, Zeichner SB et al. Cost-effectiveness analysis of everolimus plus exemestane versus exemestane alone for treatment of hormone receptor positive metastatic breast cancer. Breast Cancer Res. Treat. 147(2), 433–441 (2014).
• Concluded that everolimus plus exemestane is not cost-effective compared with exemestane alone for treatment of HR-positive/HER2-negative mBC, with an estimated incremental cost–effectiveness ratio of US$265,498.5/quality-adjusted progression-free years.
51.
Refaat T, Choi M, Gaber G et al. Markov model and cost–effectiveness analysis of bevacizumab in HER2-negative metastatic breast cancer. Am. J. Clin. Oncol. 37(5), 480–485 (2014).
52.
Xie J, Diener M, De G, Yang H, Wu EQ, Namjoshi M. Budget impact analysis of everolimus for the treatment of hormone receptor positive, human epidermal growth factor receptor-2 negative (HER2-) advanced breast cancer in the United States. J. Med. Econ. 16(2), 278–288 (2013).
53.
Pawaskar M, Karve S, Dalvi T, Davis KL, Deeter R. Health care utilization and costs among HER2-negative, HR-positive, elderly women with metastatic breast cancer in the United States. Presented at: 2013 ASCO Annual Meeting. Chicago, IL, USA, 31 May–4 June 2013.
54.
Zeichner SB, Avancha KKVR, Lopes G, Gluck S, Montero AJ. Cost–effectiveness of everolimus plus exemestane in post-menopausal hormone receptor positive metastatic breast cancer. Presented at: 2013 ASCO Annual Meeting. Chicago, IL, USA, 31 May–4 June 2013.
55.
Rules Committee Print 114-67 Text of House Amendment to the Senate Amendment to H.R. 34, Tsunami Warning, Education, and Research Act of 2015. http://docs.house.gov/billsthisweek/20161128/CPRT-114-HPRT-RU00-SAHR34.pdf.
56.
Visvanathan K, Levit LA, Raghavan D et al. Untapped potential of observational research to inform clinical decision making: American Society of Clinical Oncology Research Statement. J. Clin. Oncol. 35(16), 1845–1854 (2017).
Information & Authors
Information
Published In
Copyright
© 2018 Dasha Cherepanov.
History
Received: 12 April 2017
Accepted: 1 September 2017
Published online: 5 January 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Outcomes research examining treatments, quality of life and costs in HER2-negative and triple-negative metastatic breast cancer: a systematic literature review. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0027
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Chengying Cui, Haojie Zhang, Congcong Yang, Mingwei Yin, Xinkun Teng, Miaomiao Yang, Dejie Kong, Jinzhi Zhang, Weidong Peng, Zhimin Chu, Jingjing Wang, Yating Sun, Liping Kang, Bin Lyu, Qian Gao, Mingqing Wu, Yongqiang Wang, Yang Li, Inhibition of JNK Signaling Overcomes Cancer-Associated Fibroblast-Mediated Immunosuppression and Enhances the Efficacy of Immunotherapy in Bladder Cancer, Cancer Research, 10.1158/0008-5472.CAN-24-0940, 84, 24, (4199-4213), (2024).
- Sadeq Rezaei, Majid Babaei, A systematic literature review on direct and indirect costs of triple-negative breast cancer, Cost Effectiveness and Resource Allocation, 10.1186/s12962-023-00503-2, 21, 1, (2023).
- Kim Borsky, Fiona Tsang-Wright, Quality of Life and Patient Reported Outcomes in Breast Cancer, Patient Reported Outcomes and Quality of Life in Surgery, 10.1007/978-3-031-27597-5_11, (169-179), (2023).
- Min Huang, Amin Haiderali, Grace E. Fox, Andrew Frederickson, Javier Cortes, Peter A. Fasching, Joyce O’Shaughnessy, Economic and Humanistic Burden of Triple-Negative Breast Cancer: A Systematic Literature Review, PharmacoEconomics, 10.1007/s40273-021-01121-7, 40, 5, (519-558), (2022).
- Ami Vyas, Meghan Gabriel, Sobha Kurian, Disparities in Guideline-Concordant Initial Systemic Treatment in Women with HER2-Negative Metastatic Breast Cancer: A SEER-Medicare Analysis, Breast Cancer: Targets and Therapy, 10.2147/BCTT.S295526, Volume 13, (259-269), (2021).
- Carlo Piccinni, Letizia Dondi, Giulia Ronconi, Silvia Calabria, Antonella Pedrini, Immacolata Esposito, Nello Martini, Maurizio Marangolo, HR+/HER2− Metastatic Breast Cancer: Epidemiology, Prescription Patterns, Healthcare Resource Utilisation and Costs from a Large Italian Real-World Database, Clinical Drug Investigation, 10.1007/s40261-019-00822-4, 39, 10, (945-951), (2019).
- Laura Dormer, Introducing Volume 8 of the Journal of Comparative Effectiveness Research , Journal of Comparative Effectiveness Research, 10.2217/cer-2018-0119, 8, 1, (1-5), (2018).
- Laura Dormer, Introducing Volume 7 of the Journal of Comparative Effectiveness Research , Journal of Comparative Effectiveness Research, 10.2217/cer-2017-0087, 7, 1, (1-4), (2018).