Donor insemination: Israel as a representative case of a competitive market examining the possibility of policy reform
Abstract
Aim: To measure the private and social benefits of donor insemination (DI). Methods: An empirical model investigates the general public and DI clients’ willingness to pay (WTP) for DI, and the willingness of potential donors to become altruistic or paid sperm donors. Results: The general public and DI clients value DI and have a positive WTP for it, whereas willingness to donate, altruistically or for payment, is either low or very low. Conclusion: The general public’s and DI clients’ WTP for DI is in average above actual cost, so the government should consider funding or subsidizing DI. The government should encourage altruistic gamete donation through information and education of all parties involved directly and indirectly in the process of donation whose ultimate goal is the birth of a child.
First draft submitted: 21 September 2016; Accepted for publication: 31 October 2016; Published online: 17 November 2016
In Israel as well as in most developed countries (i.e., the USA), human gametes are sellable like any other commercially offered product in the modern market for reproductive services and products [1,2]. In some other countries (i.e., the UK, France, Canada and New Zealand), the reproductive market is controlled by government policies that support altruistic gamete donation. Regardless of governmental intervention, however, the modern reproductive market is dominated by principles of economic theory: utility, efficiency and rationality. These economic realities raise significant questions relating to our understanding of the motivations, interests and relative power dynamics of parties in the reproductive market [2]. The proposed research investigates the opportunities and expectations of the sperm industry by positing an empirical economic model to describe and explain some economic phenomena underlying sperm commerce. Using empirical models, the private and social benefits of donor insemination (DI) are investigated. The general public and DI clients’ (single women, and heterosexual or lesbian couples) willingness to pay (WTP) for DI (WTP is the maximum amount that a respondent - user or non-user, states he is wilingness to pay for a good or a service), as well as the willingness of potential donors (single males aged 18–40 years) to become altruistic or paid sperm donors is evaluated. Toward this aim, three surveys were conducted: one survey was used to evaluate public attitudes toward the DI process (in terms of the public’s WTP for DI); the second survey was targeted at DI clients’ WTP for DI; and the third survey focused on the willingness of potential donors to become either altruistic or paid sperm donors. The proposed research yields some important practical implications for balancing between costs and utilities in relation to limited resources. In considering the appropriate allocation of limited public resources, the question of the desirability of public intervention through encouraging altruistic sperm donation and/or through subsidizing the provision of DI is examined. These options might prove to be beneficial if the net benefits for both patients and society are high.
Scientific background
DI is a procedure facilitating people’s ability to achieve fertility. Fertility levels are determined by biological, social, religious and cultural factors on the one hand, and on the other by financial considerations that influence the demand for children as well as the supply. The economic approach to fertility that provides an analytical framework to explain observed fertility behavior, with emphasis on economic considerations, combines two approaches. One dates back to Becker’s [3,4] ‘household production function’ formulation, emphasizing the demand for children as the key to understanding fertility behavior, and the other is that of Easterlin [5,6], and Easterlin & Crimmins [7], who noted the possibility of shifts in the supply of children independent of demand conditions [8].
Fertility theory
The theory of the demand and the supply of children has undergone substantial modification as a result of the dramatic technological improvements in limiting or enhancing fertility. The supply of children dependent on the natural potential fertility (which reflects the number of surviving children a household may have if fertility was not deliberately limited or expanded) combined with the medical technology to enhance or limit fertility, alongside the demand for children, determine the motivation for fertility regulation. If the potential output exceeds demand – an ‘excess supply’ situation – parents are faced with the prospect of having unwanted children and are motivated to regulate their fertility. On the other hand, if the potential output falls short of the demand, no desire to limit fertility emerges; on the contrary, an ‘excess demand’ situation of this type would result in a demand for a way to enhance fertility [8].
The current study focuses on the desire for children among individuals whose potential output of children falls short of the demand due to infertility, sexual orientation for a same sex partner or lack of a partner (single individuals wishing to conceive). Their desire for children drives the reproductive market: “for a market in babies (or baby-making) to exist, babies must be something people affirmatively want and are willing to trade for” ([9] page 72). Assisted reproductive technology (ART) provides the possibility of childbearing via technologically controlled conception, for individuals falling into these categories.
Assisted reproductive technology
ART is a general term referring to methods and scientific means used to achieve pregnancy by artificial or partially artificial means, rather than sexual intercourse. ART includes in vitro fertilization (IVF – a process whereby an ovum is fertilized by sperm outside the body), ovum and embryo donation, surrogacy, and DI (a procedure that involves introducing a sperm into a woman’s uterus). The use of ART is expected to rise in upcoming years, due to factors such as the increase in single and same-sex parenthood, and the increasingly common choice by many couples to delay having children until later in life, resulting in many couples trying to conceive at a later age and under less fertile hormonal conditions [10].
The present research is concerned with a crucial element of ART – sperm donation. We seek to assess the opportunities and expectations of the sperm donation market, including issues such as the advantages of competitive or altruistic markets, public and private welfare issues, social and private utility and public intervention.
Donor insemination
The DI process has become a key option for specific groups seeking to conceive: single women, same-sex female couples and couples with an infertile male. For some heterosexual couples and for most single and lesbian women seeking to conceive, sperm from a fertile, healthy and carefully screened third-party male is the original, simplest and most-used fertility technique on hand [11–15] Nonetheless, recipients must be informed that this form of reproduction carries certain risks. At present sperm banks perform a limited number of genetic tests to screen for and exclude donors bearing recessive disease mutations, but there is a need for the banks to update their screening methods and make them more comprehensive and affordable. This should include new techniques based on DNA screening, which are able to detect many more potentially heritable diseases and thus protect unborn children from these risks [16,17].
Daniels and Lewis [18] point to two known models of semen provision: the commercial and the donor-based one. The predominant commercial model involves buyers and sellers of semen. DI practitioners (sperm banks) buy semen from providers and sell it to clients for a profit, with a price markup to allow for the costs of the recruitment, semen screening testing, semen storage and payment to semen providers. In this model, sperm banks buy semen from providers and sell it to fertility clinics for a profit, while the clinics act as brokers who meet purchasers’ shortage with providers’ supplies. In a simpler hypothetical model of commercial semen provision, infertile couples would purchase semen directly from providers in a free market. However, this type of exchange is forbidden due to medical and legal constraints, and is virtually unknown in practice.
In a noncommercial model of semen provision, health professionals are the intermediaries who obtain semen from volunteers who receive no payment (except for reimbursement of expenses) and make this sperm available to their clients. Of course, this service often comes at a cost to the recipients, who must still pay for the recruitment and screening of providers, and for semen testing and storage. A model of semen provision whereby providers give semen directly to recipients is not common; however, the use of semen directly from donors is known in the case of single women or lesbian couples seeking help outside the realm of medicalized DI services.
Indeed, since sperm banking began in the 1970s, the industry has mostly been self-regulated and has had a great deal of flexibility to shape its institutions according to the legal and social atmosphere [19,20]. Sperm banks have streamlined the process of recruiting sperm donors and the subsequent sale of their genetic material. They ensure that the genetic material is disease-free and with a high sperm count, and allow potential recipients of donated genetic material to select gametes according to donor profiles [19]. In most countries (i.e., the USA and Israel), the commercial model of semen provision dominates, and the sperm donation industry is governed by laissez-faire economics. This “where the ‘customer’ (i.e., the donor/recipient) seeks the jurisdictions where it is easiest to acquire the services desired and sperm banks have created a business model governed by supply, demand, value, prices and the benefit of both donors and recipients” ([19] page 132). This laissez-faire approach to the sperm donation industry, which views parents’ ability to conceive a child as a private choice free of any government intervention and allows the market for donated genetic material to develop at will, raises several complex issues regarding government intervention, healthcare, insurance, religion, science and ethics [19]. Scholars frequently cite the problem that only few legislative actions have been taken to regulate the free market of the sperm donation industry. The scarcity of formal regulations results in this industry’s ‘wild west’ nature – sperm banks operate in a free market regulated by profit-driven and cost–benefit considerations [19,21–22].
In some countries (i.e., the UK, France, Canada and New Zealand), in contrast, the noncommercial model of sperm provision is the dominant official model (despite the reservations presented below). In the UK, the Human Fertilization and Embryology Authority stated that one of its goals was to gradually phase out payments for semen, in favor of donation. The legislation administered by the Human Fertilization and Embryology Authority states that “no money or other benefit shall be given or received in respect of any supply of gametes or embryos unless authorized by directions (donors may be paid no more than £15, plus reimbursement of expenses)” as quoted in Daniels & Lewis ([18] page 1526). In France, since July 1994, a law called ‘bioethical’ has governed medically assisted procreation. This law adopted the rules of the ‘Centre d’Etude et de la Conservation du Sperme Humain’ concerning the donation of gametes. The central tenets of the law establish that sperm donation must be unpaid and anonymous. Semen donation in Canada is mandated as altruistic and anonymous under the Assisted Human Reproduction Act. However, reimbursement of expenditures is permitted, and a donor can choose to be identifiable [11]. The New Zealand Parliament “has passed the Human Assisted Reproductive Technology Act in 2004, which uses criminal sanctions to prohibit a commercial supply of human embryos and human gametes” ([23] page 4).
The concept of altruism in gamete donation has aroused many debates, given the complexity and the dynamics involved in altruistic semen donation [23]. Although some semen donors choose to donate for altruistic reasons, such as their desire to help infertile couples or others who are unable to conceive children on their own [10], semen supply is in decline and is failing to meet demand. This is in the wake of the intensification of donor regulations and the prohibition in some countries on the commercial supply of human gametes [11,23].
Since financial incentives play a key role in decision-making for almost all individuals [23], many health professionals see the commercialized model of semen provision as the easiest route to resolve the shortage in semen supply by offering financial incentives to men willing to provide semen. And so despite the declared policy of a number of countries (i.e., Canada, New Zealand and the UK), which opposes the commercialization of sperm donation and favors altruistic donation, many factors, such as resource constraints, legal and religious proscriptions, quality and health issues, and sociocultural hurdles continue to drive the commercialized model of payment for imported sperm. This is obtained from sperm banks in countries such as the USA and Denmark, and in addition, infertile couples are crossing national borders to seek sperm donations in countries where it is permitted [24–28]. As Pietrzak ([19] page 131) notes, “even if the buying and selling of sperm were wholly prohibited, the market would not be affected because gamete transfer could still occur by an ‘inconvenience allowance’ or by gift. Sperm banks and recipients could still compensate donors monetarily for their time and discomfort in transferring gametes.”
The variation in models of sperm donation is likely to reflect the norms and regulations in a community, the attitudes and policies of sperm banks and clinics, and the types of men recruited and their motivations. Whether the reproductive market is ruled by restrictive government policies that fully ban certain ART procedures or by laissez-faire economics, as Spar [22] argues, the reproductive market is correctly identified as a ‘market’, given the involved elements of demand and supply, prices that link supply and demand, and businesses that sell their products. As economist John McMillan [29] expressed it simply, “a market exists if there are people who want to buy and others who want to sell” (quoted in Sanger, 2007; [9] page 70). The basic necessities for market formation are buyers who want the product, sellers willing to provide the goods or services, and background conditions that make a particular trade both desirable and possible [9]. Indeed, the development of a reproductive market is not spontaneous, but rather driven by new technologies, medical professionalization and medical regulatory regimes [20].
In this article, with the aim of shedding more light on the field of DI in general, I investigate the sperm industry from the unique sociocultural perspective of the Israeli fertility ethos. I bring the Israeli case as an example, since the commercial model with paid donation is well established there, and discussions revolving around altruistic gamete donation are frequently held in the public domain. Significance might be found in the attempt by policy makers to institute the altruistic model even if not in full. Perhaps even a partly altruistic market could contribute more to the social and private welfare than the commercial market. My study tries to find out whether altruistic donation brings benefit and should therefore be considered. Based on this study conducted in Israel, we can infer in general about the needs of DI clients, the preferences of potential donors and the question of whether the government should participate in the funding of the DI process and/or encourage altruistic sperm donation through the use of the state medical budget with limited resources.
DI in Israel
Israel is characterized by its pronatalist ideology, expressed in the formulation of state policy on reproductive medical care [30–32]. The need to establish a family is deeply rooted, engrained in Jewish religious, cultural, social norms and philosophy, and features prominently in Jewish sources as well as literature [33], which sanctifies the desire to have children as a fundamental human need and the right to have children as one of the fundamental human rights. The historical persecution of diaspora Jews, the annihilation of the Jewish people during the Holocaust and the loss of life in multiple wars heighten the crucial importance of Israel maintaining a positive birth rate. Israel’s pronatalist approach is supported by proactive means such as funding-assisted reproductive treatments and legislation regulating IVF, gamete donation and allocation, and surrogacy contracts [30,34–37].
The Israeli Ministry of Health monitors reproductive technologies through regulations; the first DI regulations were published in 1979, when sperm banks began to operate and the most recent version of these rules was updated in 1992 when the state imposed its control over DI by outlawing private DI services and restricting DI to hospital-based sperm banks headed by gynecologists. The Israeli Health Ministry regulations explicitly prohibit a sperm bank from disclosing any identifying information about the donor. In recent years there have been voices in Israeli public discourse calling for a change in regulations on sperm donations: the demand is for the establishment of a central records repository to coordinate the data on sperm donors, which might even make it possible for donor-conceived offspring to identify them in the future. This led to protests by many single women who urged state authorities to eschew a measure that might cause a shortage of sperm donations and as a result, deprive them of their right to a child. Countering this protest were child rights organizations who spoke up as advocates of the child’s right to know his identity and family connections. A conflict of interests was thus created between ‘the right to parenthood’ and the ‘welfare of the child to-be-conceived’ [38]. Sperm bank regulations require donors to undergo blood tests (hepatitis B and C, and Tay–Sachs) and syphilis tests every 6 months. The sperm is examined and tested for HIV antibodies on the day of the donation, and this test is repeated 6 months later.
The number of donations accepted from any donor is supposed to be limited, according to Israeli Ministry of Health regulations, but this is enforced in a very general way and is difficult to monitor, since there is no centralized method of monitoring donors so that a donor may choose to donate at several sperm banks.
Today there are 17 sperm banks operating in Israel, which are approved by the Israeli Health Ministry [39].
The donors are single men only, not married, divorced or widowed who are responsible for and cognizant of their actions. The preferred age range for donors is between 18 and 30 years. Financial compensation is made directly to the donor by the sperm bank. Donors receive US$80–US$150 per sample per donation [31]. In total, 42% of sperm donors in Israel are students, 37% are soldiers and 20% older men with a profession [40].
Sperm donations are intended mostly for women who, for medical reasons, need sperm from a source other than their partner, or for women who do not have a partner. Today, sperm banks primarily serve single and lesbian women. There is no precise data on the number of women who conceive from sperm donations since sperm banks in Israel do little follow-up on the sperm recipients [40]. The cost of the sperm donations is not included in the current health basket, nor do the Health Maintenance Organizations pay the cost of the donations that are borne by the buyers and varies between the banks. Recent years have seen a decrease in the number of local sperm donors. The private import of sperm donations is driven by this shortage [41], and the globalization of markets has made purchasing sperm abroad convenient and feasible. The price for sperm, both local and ‘foreign’, is steadily rising: in 2011, the price of domestic donor sperm had doubled from US$100 to US$210 per vial [31]. The cost of imported sperm ranges from US$650 to US$1000 [42].
For more information regarding DI in Israel (the donors, recipients and donor-conceived offspring: i.e., legal aspects of sperm donation in Israel, information regarding the donors and the target audience seeking a sperm donation from a donor), please see Supplementary Material 1.
Cost-benefit analysis, contingent valuation, willingness to accept & WTP
The proposed research deals with the implications of the DI market and its resulting effect on private and social welfare by employing a cost–benefit analysis (CBA). CBA has been the major practical result of welfare economic theory over the past decades [43,44]. Within CBA, the benefits of an intervention are evaluated in units commensurate with the cost – typically monetary units. Two main methods can be applied to elicit these values. The first, using market information is called the ‘hedonic’ or ‘revealed preference’ technique. The second involves an experimental survey, or ‘contingent valuation’ (CV) technique. For our research, the most appropriate method is the CV method since it is a simple, flexible nonmarket valuation method that has become the dominant technique used in the monetary valuation of benefits in healthcare in absence of conventional markets or for services/products whose market prices fail to reflect their value to society [45–48].
However, the CV method is subject to criticism related chiefly to two aspects: the validity and reliability of the results, and the effects of various biases and errors. In order to overcome the controversy over the ability of the CV method to predict the value of DI, I followed the recommendations and instructions put forth by the US National Oceanographic and Atmospheric Administration panel [49]. The National Oceanographic and Atmospheric Administration panel assessed the use of the CV method in estimating the nonuse values and concluded that the CV could be used to derive important information about the nonuse values, provided that the panel’s guidelines are followed while conducting CV study.
The CV is based on either willingness to accept (WTA) or on WTP. The WTA is the willingness to accept compensation, that is, minimum monetary amount required for a person to forgo or sell some good or service, and the WTP is the maximum monetary amount that a person willing to pay to acquire a service/product. The current research will conduct two WTP surveys and one WTA survey.
There are various elicitation methods for CV: bidding technique, payment cards technique (PC), open-ended questions and dichotomous choice-closed-ended questions. This research will apply the PC technique, whereby the respondents will be presented with various amounts of money and will be requested to choose their own WTP from them. The payment cards method has unique advantages: it matches the purchasing behavior of ‘shopping’ (i.e., potential buyers check out a number of stores that sell the same goods and services at different prices) [50,51] and allows for degrees of uncertainty regarding values. Given the nature of healthcare, and the fact that most individuals often do not have experience with the healthcare intervention being evaluated, the increased use of such payment ladders is required. Indeed, in recent years, health economists have retained an interest in payment card approaches. Attention must be paid to the existence of the so-called ‘range bias’ in the payment cards method [52,53]. This means that the WTP responses are affected by the range of the presented amounts. In order to avoid this risk, the range of the presented amounts was determined on the basis of findings from a pilot round of questionnaires.
Research objectives
In the proposed research, we seek to explore the Israeli DI market and its participants in order to contribute to the discourse regarding the opportunities and challenges of this market. An empirical model is applied to evaluate the general public and the DI clients’ utility derived from DI by applying the WTP technique, which as described above is implemented in healthcare services and allows for an individual preference evaluation to be derived from respondents’ answers.
The empirical model will estimate, among samples from the general public, DI clients and potential donors:
monetary evaluation of DI – what is the maximum amount a respondent is WTP for DI.
willingness (of potential donors) to become altruistic or paid sperm donors.
Working hypothesis
The proposed research deals with three populations: the general public, DI clients and potential donors. It yields some important practical implications in balancing costs and utilities in relation to limited resources. In considering the appropriate allocation of limited public resources, public intervention through encouraging altruistic sperm donation and/or subsidizing the provision of DI should be considered in the following scenarios:
the desire of the general public to pay for DI (the social desire to pay for DI) may differ from the desire of the DI clients to pay for DI (the private desire to pay for DI).
The general public population includes individuals who with a high degree of certainty will not be clients of DI. Their WTP will be determined by external advantages and an evaluation regarding future potential use of this treatment – either for their own use (with a low degree of likelihood) or use by their friends and relatives. The general public’s WTP depends also on the altruistic motivation that people who are not DI clients have toward DI clients. The DI client population, on the other hand, includes individuals who will need DI treatments with absolute certainty. Their WTP for DI, which is derived from their utility function, depends on their socioeconomic status and their condition as DI clients.
If a significant statistical difference between the average WTP for DI among DI’s DI clients and the general public emerges, the gap between the social and the private WTP could mandate government intervention. Since the medical care market has imperfect information as well as an inability to bear suitable risk, there is a need for adjustments and institutional interference by the health authorities, through budget decisions regarding medical infrastructure and technologies including the use of subsidies and other devices to close the gap between WTP of different interest groups [54].
The general public’s average WTP for the DI process will exceed the actual average cost of it. In this scenario, public provision should be encouraged up until the point that current marginal government expenditure is equal to marginal WTP [55]. The government should participate in the funding of DI medical process at least up to the point that is optimal from society’s perspective. Other intervention policies that can be considered would include establishing insurance specifically for DI treatments. The insurance fee would reflect the insurance element and would constitute the implementation of the general public altruism that might emerge from the study;
The potential donor population, comprised of single males, does not demonstrate potential to become altruistic sperm donors. Public intervention through encouraging altruistic sperm donation might be considered.
Experimental design & methods
Data gathering
Data were gathered via WTP surveys that were carried out among the general public, DI clients and potential sperm donors, preceded by in-depth interviews.
The surveys were constructed and carried out within three data-gathering stages:
Primary stage: The primary stage involves identification of items to be included in the research questionnaires. For this purpose, in-depth interviews with four fertility experts and five DI patients were conducted. The initial construction of questionnaires was based on content analysis of interview results;
Pilot study: Once constructing the first version of the questionnaires (based on the primary-stage findings) was finished, a pilot study was conducted, comprised of 52 participants (30 questionnaires for the general public, ten questionnaires for DI clients and 12 questionnaires for potential donors). The goal of the pilot study was to evaluate the questionnaire’s difficulty and clarity, and the respondents’ willingness to respond to various items within it. The pilot study presented detailed information about DI treatments and included face-to-face interviews conducted by the researcher. This provided important information concerning the research questions. The credibility and quality of the values received from WTP/WTA surveys usually depend on the research questions. Interviews enable the presentation of relevant information in a supervised manner while gathering responses to many complex factors;
Main survey: Based on pilot study findings, the research questionnaires were modified and adjusted. Final versions created for each of the three population groups.
1067 valid questionnaires were filled out (out of 1500 questionnaires distributed – 71%) by the general public population (613 women and 454 men). One hundred and forty-four valid questionnaires were filled out (out of 200 distributed – 72%) by the potential donors’ population, and 202 valid questionnaires were filled out (out of 300 distributed – 67%) by the DI client (166 women and 36 men).
The general public population sample consisted of Jewish Israeli men and women. Interviews were conducted in selected areas: four large cities in four major population regions in Israel (Tel Aviv, Jerusalem, Haifa and Beer Sheba) by trained student interviewers from the university’s Department of Economics and Business Administration.
The DI client population sample was composed of Jewish Israeli single women, lesbian couples and heterosexual couples with male infertility who need sperm donation with absolute certainty. The DI clients were recruited via snowball sampling and also following an ad on forums targeting single mothers, heterosexual couples with male infertility and lesbian couples. The sole criterion for inclusion was whether they had applied for DI and purchased sperm over the past 2 years.
The potential donor population sample was aimed at Jewish Israeli single men aged 18–40 years. Interviews were conducted in selected areas (four large cities in four major population regions in Israel: Tel Aviv, Jerusalem, Haifa and Beer Sheba) by trained student interviewers from the university’s Department of Economics and Business Administration.
The main surveys applied the CV PCs technique and included questions regarding factors deemed to affect WTP and WTA, such as age, gender, educational level, income, ethnic origin, residence, religiosity and number of siblings. All questions in the questionnaire form were in multiple-choice format.
Ethical approval
Anonymous, self-administered questionnaires were filled out without experimental interventions. From the cover letter of the questionnaire, the subjects were informed that data collection and analysis will be fully anonymous so that their personal information would be fully protected, all the answers would be kept confidential, processed statistically and used for scientific research only; they were free to decide to participate or refuse to participate. Written informed consent for participation in the study was obtained from each participant.
Statistical analysis
Each one of the three surveys was analyzed. Mean WTP and median WTP were calculated. The relationship between the respondents’ WTP/WTA and their income was studied. Furthermore, in order to adjust various factors at the same time, regression analysis was conducted assuming that WTP/WTA is a dependent variable and that age, gender, education level, income, ethnic origin, residence and religiosity are independent variables. Pseudo R-squares were calculated for the regression models, and p-values of <0.05 were to be considered statistically significant. All analyses were performed using SPSS (version 19.0 for Windows, SPSS, Inc., IL, USA) and SAS (version 9.4 for Windows, SAS Institute, Inc., NC, USA).
Results
The sample of DI clients includes 202 participants. The DI clients’ age is between 21 and 60 years, with the average of 35.67 years and standard deviation (SD) of 7.42. Background variable frequencies are presented in Table 1.
The sample of the general public includes 1067 participants. The participants’ age is between 18 and 73, with the average 29.79 years and SD of 8.22. Background variable frequencies are presented in Table 2.
Comparison results between the mean ages, gender frequencies, familial status frequencies, previous parenting (children), education levels, occupational status and ethnic origin of the two groups are presented in the Supplementary Information – Supplementary Material 2.1
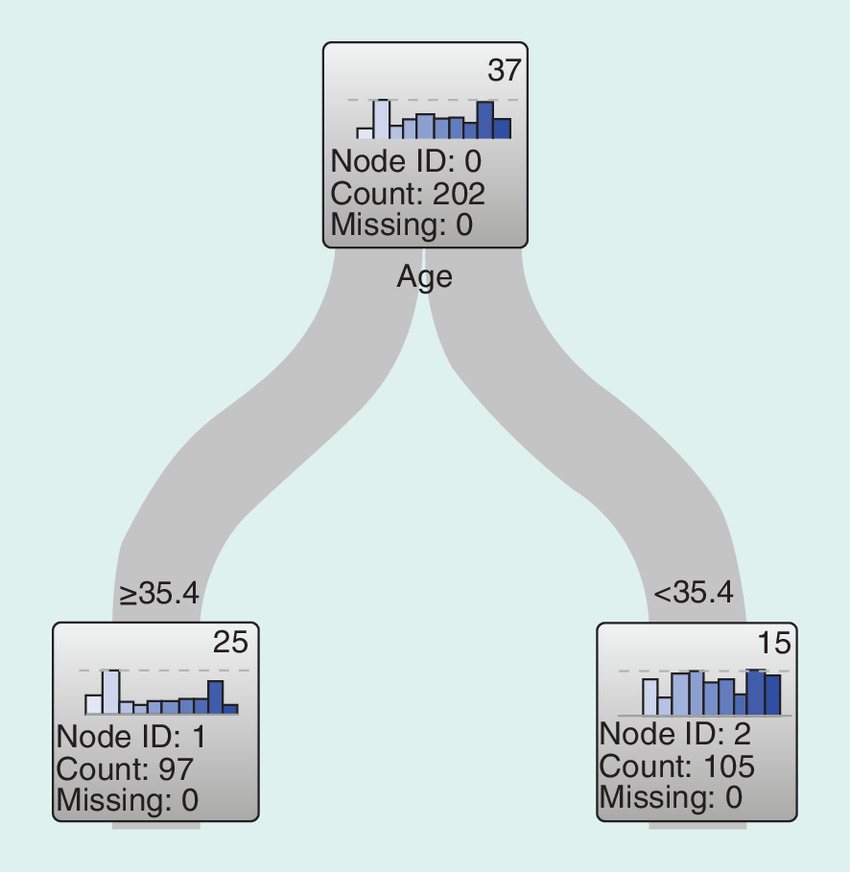
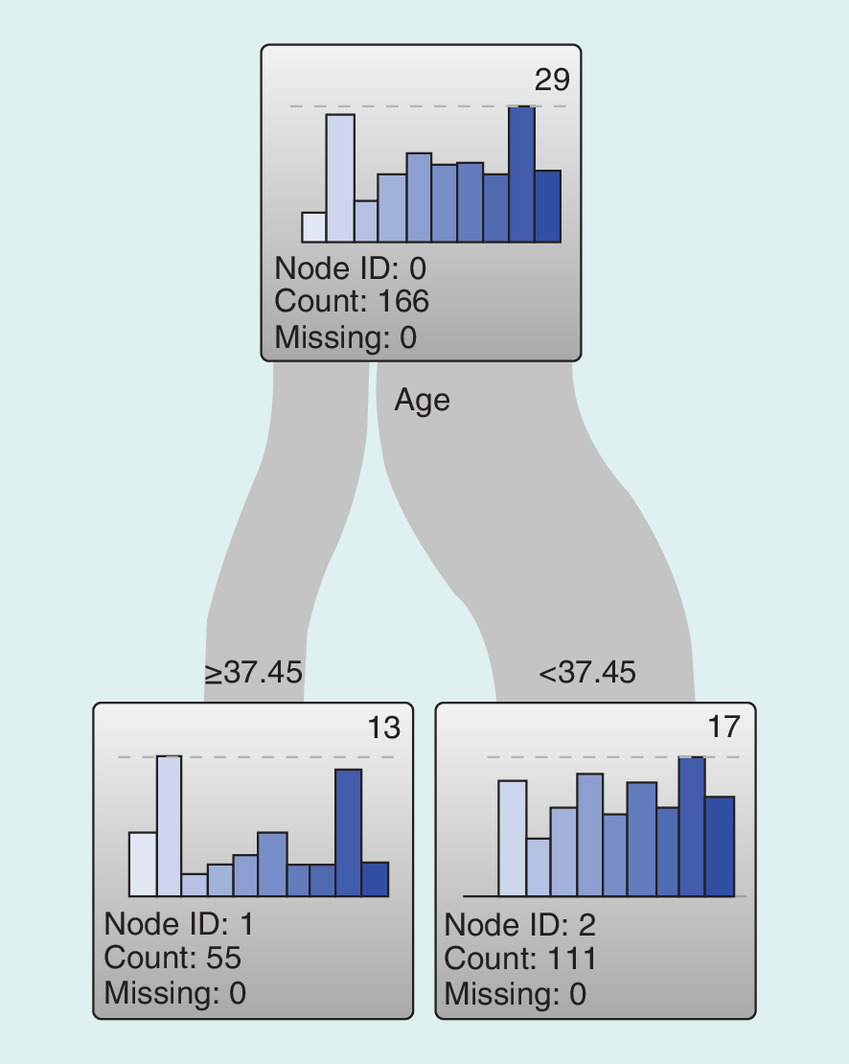
Differences in the WTP for DI between age groups (younger women/older women and younger men/older men) were found to be significant among the DI client group and among women in the DI client group. DI clients under the age of 35 are willing to pay more for DI compared with women above the age of 35. Women under 37 years old in the DI client group are willing to pay more for DI compared with women over 37 years old.
The results of the decision tree I used in order to split the data in each of the groups mentioned above into two age sub-groups are presented in Figures 1 & 2.
The Mann–Whitney U tests showing the significant differences in the WTP for DI among each of the above groups are presented in Tables 3, 4, 5, 6, 7 & 8.
Ordinal regression analysis of the relationship between the DI clients’ WTP for DI and their income, controlling for age, gender, education level, ethnic origin, familial status and religiosity is presented in Table 9.
The regression analysis results show that there is a significant correlation between the respondents’ WTP for DI and their income: respondents who earn US$2632–$3421 per month are willing to pay more than respondents in other income levels, even after controlling for background variables. Additionally, there is significant correlation between the WTP and age (older participants are willing to pay less than younger), and between the WTP and education levels (participants with partial academic education are willing to pay more than the other groups).
Ordinal regression analysis of the relationship between the general public respondents’ WTP for DI and their income, controlling for age, gender, education level, ethnic origin familial status and religiosity is presented in Table 10.
The regression analysis results show that there is a significant correlation between the respondents’ WTP for DI and their income: respondents who earn less than US$2632 per month are willing to pay less than respondents with other income levels, even after controlling for background variables. Additionally, there is a significant correlation between the WTP and education level – participants with professional education are willing to pay more than the other groups. Between the WTP and the participant’s ethnic origin – Asians and Africans are willing to pay less than the other groups and between the WTP and the familial status – married participants are willing to pay less than the other groups.
The ordinal regression analysis of the relationship between the respondents’ WTP for DI and their income, controlling for age, gender, education level, ethnic origin, familial status, religiosity and group (DI clients vs general public), is presented in the Supplementary Material 2.2.
The sample of the potential donors includes 144 participants. The participants’ age is between 18 and 40 years, with the average 29.74 years and SD of 5.19. Background variable frequencies are presented in the Table 11.
In Table 12 below the frequencies table of willingness to donate altruistically and willingness to donate for payment are presented.
The willingness to donate, either altruistically or for payment, is low or very low among >40% of the respondents.
Table 13 shows that the most popular reasons to donate are “Giving makes me feel fulfilled,” “I was raised with values of giving” and “I understand the longing for a child.” The least popular reason is “Through donation I can spread my genes.”
Table 14 presents the WTA frequencies.
Ordinal regression analysis of the relationship between the respondents’ WTA and their income, controlling for education level, familial status and religiosity is presented in Table 15.
The table shows that there is no significant correlation between WTA and the personal income among potential donors. Instead, there is a correlation between the WTA and the level of donor’s education: potential donors with a partial academic education are willing to accept less than donors with other levels of education.
Conclusion & implications
In today’s world of technology, ART is a growth industry. According to an estimate by the European Society of Human Reproduction, some 3.5 million children have been born worldwide with the help of this technology. It would therefore be no exaggeration to state that donor conception is relevant to the lives of millions of people, from the donors, recipients and donor-conceived people themselves, to the siblings of donor-conceived people (biological and nonbiological) and their extended families.
In this study, I evaluated the private and social benefit of DI in Israel as microcosm with the aim of understanding the economic forces operating in a competitive reproductive market, and to test the market’s willingness to act as an altruistic market. The results and conclusions of this study are relevant to competitive reproductive markets as well as to altruistic reproductive markets around the world. They reflect religious, moral and social views as well as ethical and legal arguments. This indicates that the DI markets should be examined, interpreted and explained in light of these factors. The Israeli sociocultural environment, for instance, gives rise to the supreme value placed on fertility, that is, Israelis of all ethnic and class origins and level of educational attainment are highly familistic. This social climate, which is a product of Jewish religious beliefs (the biblical commandment to ‘be fruitful and multiply’), the Israeli culture (Israelis marry, and typically do so at a younger age), encourages people to have more children (about one child more than in most west European countries), give birth less frequently out of wedlock and also divorce less frequently than in most western countries [32]). These, together with a consciousness of national history (in the twentieth century, the trauma of the Holocaust and the establishment of the Jewish state highlight the importance of replenishing the decimated Jewish population and rebuilding the nation in its own land) have made childbearing an act of both self-realization and contribution to the nation, and was rewarded by economic incentives [33–34,36,56].
The study findings demonstrate that both the general public and the DI clients value DI and have a positive WTP for it. The average WTP for DI, among the general public, is US$855 whereas for the DI clients, it is US$724. There is a significant statistical difference between the average WTP among the general public and the DI clients (p < 0.0001). The seemingly bizarre findings whereby the WTP of the general public exceeds the WTP of the DI clients (i.e., the general public who do not need the procedure for certain, value DI more than the DI clients who need the procedure) can be explained in several ways. First, the DI clients, unlike the general public, have full, comprehensive and updated information regarding the purchase cost of sperm donation so their WTP is based upon their knowledge and experience. The general public can only speculate the costs. Moreover, the DI clients live in a different set of circumstances than the general public, so that different variables, which are specific to DI clients (i.e., expenses that relate indirectly to purchasing DI, such as time spent searching for a donor, loss of working days due to testing and inseminations, among others) affect the WTP for DI. Due to limited resources, DI clients take into account all the direct and indirect expenses, and WTP for DI accordingly.
Another novel explanation can be found in the attitude of patients in relation to DI. DI clients (single women and couples in which the male partner suffers from infertility) tend to shroud the treatment in secrecy [32,57]. This may be due to religious reasons or traditional mores and notions regarding parenthood and family. Another explanation may be owing to the strong stigma that often – mistakenly – conflates infertility with impotence, whatever the reason for it, male infertility has been found to be highly stigmatic across a broad range of cultures and settings [36,57]. The pain and shame that infertility entails are especially pronounced. DI is therefore a highly sensitive field. DI clients are extremely sensitive and might feel ashamed of their situation, trying to repress or deny it and hence underestimate and undervalue DI.
The general public, and the DI clients are willing to pay for DI on average more than its true costs for buyers, on average US$605. This suggests that DI delivers benefits and appears to have contributed to improved well-being. According to the economic literature, funding of DI is supposed to extend to the point where the costs of DI equal the social benefit from DI. Based on the findings of this study, the Israeli government could consider funding DI up to the point where the costs of DI equal US$855.
In Israel, familism fosters and is, in turn, shaped by reproductive policy, which plays a major role in the national ethos. Israel is unique in the world in funding fertility treatments for all interested persons regardless of their marital status and/or sexual orientation. The state is also willing to fund fertility treatment for individuals who have children from previous relationships, until they have produced two children with their present mate (the age limit for women is 51 years). Consequently, the scope of treatment is also the highest worldwide [34–36]. The public healthcare system also provides DI but it is not fully funded, and the user participates in part of the payment. The higher state funding provided for procreative medicine as compared with subsidies provided for DI demonstrates the ascendant importance attributed to biogenetic parenthood (biological parenthood, having biogenetic offspring). The findings of the present study suggest that DI should receive the same full funding as other fertility treatments, representing a departure from the current public policy to prefer biogenetic procreation (regardless of the economic, social and health costs).
The significant differences that were found in the WTP for DI between age groups are of most interest since they may indicate the level of knowledge possessed by the infertile persons (the recipients). This result complies with the scientific, medical knowledge regarding fertility. As women approach their later reproductive years, ovarian function gradually declines until menopause, so that increased age is correlated with lowered fertility. Natural fertility begins to decline when a woman reaches her mid-30s [58], and this process accelerates around the age of 38 years [59]. There is an age-related decline in pregnancy rates corroborated in research conducted on DI, which shows there is a noticeable decrease in pregnancy rates in women above the age of 35 years [60–63]. More cycles of DI treatment are often needed for women over the age of 35 [61,63]. Knowledge of these facts could be the reason for the decline in the WTP for DI among DI clients over the age of 35 and DI clients – women aged above 37 years. Namely, because of the decline in fertility and the increased conception time that occurs after the age of 35 years, women above the age of 35 years prefer to consider different ART treatments such as IVF rather than another DI cycle.
Unlike the findings regarding the WTP of both the general public and the DI clients, which were found to be positive and significant in relation to income, no significant correlation between WTA and the personal income among potential donors was found. Instead, there is a correlation between the WTA and the level of donor’s education: potential donors with partial academic education are willing to accept less than donors with other levels of education. Partial academic education means students who did not yet finish their academic studies, and who are in the process of studying. Since the majority of young university students have no or limited income from employment, it is somehow surprising that students are willing to accept a lower payment for sperm donation, and do not take into account their personal income when considering the WTA payment for sperm donation. This is also in contrast to other studies that found that the majority of university students are motivated primarily by payment [64–66].
Moreover, in Israel, the monetary payment for donors is a norm and compensation is expected. These men had prior knowledge of payment and therefore had the expectation of being paid [23]. So not to pay donors for their semen may indirectly imply exploitation [66,67]. Despite this, the empirical results of the present study show that the average amount of the WTA payment for donation among approximately 50% of the potential donors is lower than the sum that is actually paid for a donation on average, US$138. It means that although in Israel, the commercial model of semen provision currently dominates in the sperm market; altruistic gamete donation might be the preferable option.
The findings of the present study can be explained due to the growing legitimacy of different family forms and the nontraditional parenthood by single and lesbian women [40,57], and the expansion of neoliberalism [31]. Students who are at the forefront of knowledge are the first to absorb new approaches and state of minds. This is expressed in the motives for sperm donation revealed in the present study. The most popular reasons to donate are “Giving makes me feel fulfilled,” “I was raised with values of giving” and “I understand the longing for a child.” The least popular reason is “Through donation I can spread my genes.”
The notion of paid DI or altruistic DI has aroused many debates; in the present study, the findings show that the willingness to donate, either altruistically or for payment, is low or very low among >40% of the respondents. This brings to mind the regression results regarding the significant correlation between the WTA and the level of donor’s education, and the understanding of the importance of education in the encouragement of DI and altruistic DI. If the government wants to encourage gamete donation, it must intervene in the gamete market and support gamete donation through information and education. Gamete donation must be understood within the sociostructural framework that provides incentives and opportunities for the donors and recipients to act [68] while addressing the rights of the child born from sperm donation – the most important concern and the one that must be addressed even before encouraging gamete donation. Today, there is an acceptance and understanding that the impact of DI upon the donor-conceived offspring should be discussed and handled in light of psychosocial, ethical and legal aspects, that is, the legal aspects of being conceived through donor insemination; the question of the right of children born through sperm donation to investigate their biological origins on reaching maturity (access to identifying and nonidentifying information about donors granted to donor-conceived people so that they are able to learn about their genetic heritage [57]; the medical interests of donor-conceived individuals. Some donor-conceived people wish to find out more information about their familial medical history – the importance of knowing whether or not there is a familial history of, diabetes, cancer, heart disease, mental Illness and other inherited diseases [69,70]); revealing information about the donor’s identity – the desire to know more about themselves and the desire to know more about their donor [71,72]; the fear of unknowingly forming relationships with siblings or half-siblings and the serious consequences of such a relationship; the psychological implications of being born through DI, among others.
The recognition of the need for education and public awareness regarding balancing the interests of all involved in DI is essential for all concerned and important in promoting the view that sperm donation is an altruistic act [73].
Well-coordinated national and regional public awareness programs including community education activities such as public seminars for the general public, parents, donor-conceived people and donors, coupled with educational campaigns in the mass media to raise the awareness of, and the need for, altruistic gamete donation are needed in order to change attitudes toward gamete donation and especially toward altruistic gamete donation. Hopefully education will lead to reduction of the social stigma commonly associated with infertility and promote the recognition of the immense difficulty caused by infertility and involuntary childlessness. This, in turn, may lead to legislation that reflects the needs and rights of the donor-conceived people in relation to parents, donors and the general public, and generate a positive image of the altruistic sperm donor aimed at enhancing the donor’s self-perceived social approval of his act.
Significance
This study’s findings bear critical implications for a range of institutions and individuals involved in the field of DI in general.
The findings shed light on the utility for the general public and the DI clients from DI and of potential donors’ benefit from becoming altruistic or paid sperm donors.
Findings will also contribute solid data to the debate regarding whether the government should participate in the funding/subsidizing of the DI process and/or encourage altruistic sperm donation through the use of the general public medical insurance. This, in light of the limited public resources, since the social desirability of the general public to pay for DI may differ from the private desire of the DI clients. The theoretical economic idea behind the public funding is to encourage intervention up to the point where the marginal social cost to the government will equal the marginal social utility from the DI procedure. Health economists who develop economic instruments for utility estimation of medical intervention in general may also benefit from this kind of analysis and research. The CV methodology is applied. Since some health economics studies use CV but contradictory opinions exist concerning the validity and reliability of this methodology, our research could help to establish and validate this method.
Israel is a productive arena for this kind of research (due to local sociocultural characteristics of fertility patterns). Paid donation is well established in Israel, and the consideration of an altruistic gamete donation is both necessary and important. Statistical analysis indicate that the Israeli government should consider supporting altruistic sperm donation and/or subsidizing DI, so as to increase public welfare.
| Variable | Value | Frequency | % |
|---|---|---|---|
| Sex | Men | 36 | 17.8 |
| Women | 166 | 82.2 | |
| Country of birth | Israel | 170 | 84.2 |
| Other | 32 | 15.8 | |
| Ethnic origin | Europe/Americas | 31 | 15.3 |
| Asia/Africa | 63 | 31.2 | |
| Israel | 108 | 53.5 | |
| Familial status | Married | 73 | 36.1 |
| Single | 72 | 35.6 | |
| In a relationship (not married) | 57 | 28.2 | |
| Children | No children | 106 | 52.5 |
| Adopted children | 15 | 7.4 | |
| Biological children | 81 | 40.0 | |
| Education | Elementary | 12 | 5.9 |
| High school (partial) | 3 | 1.5 | |
| High school (complete) | 25 | 12.4 | |
| Professional | 29 | 14.4 | |
| Academic (partial) | 32 | 15.8 | |
| Academic (complete) | 101 | 50.0 | |
| Occupational status | Full time | 159 | 78.7 |
| Part time | 36 | 17.8 | |
| Unemployed | 7 | 3.5 | |
| Personal income | <4000 NIS | 24 | 11.9 |
| 4000–7000 NIS | 74 | 36.6 | |
| 7000–10,000 NIS | 65 | 32.2 | |
| 10,000–13,000 NIS | 24 | 11.9 | |
| >13,000 NIS | 15 | 7.4 | |
| Household income | <7000 NIS | 41 | 20.3 |
| 7000–10,000 NIS | 49 | 24.3 | |
| 10,000–15,000 NIS | 73 | 36.1 | |
| 15,000–20,000 NIS | 25 | 12.4 | |
| >20,000 NIS | 14 | 6.9 | |
| Sexual orientation | Heterosexual | 123 | 60.9 |
| Homosexual | 45 | 22.3 | |
| Other | 34 | 16.8 |
NIH: New Israeli Shekel.
| Variable | Value | Frequency | % |
|---|---|---|---|
| Sex | Men | 454 | 42.5 |
| Women | 613 | 57.5 | |
| Country of birth | Europe/Americas | 190 | 17.8 |
| Asia/Africa | 150 | 14.0 | |
| Israel | 506 | 47.4 | |
| Other | 221 | 20.7 | |
| Ethnic origin | Europe/Americas | 260 | 24.4 |
| Asia/Africa | 241 | 22.6 | |
| Israel | 566 | 53.0 | |
| Familial status | Married | 420 | 39.4 |
| Single | 331 | 31.0 | |
| In a relationship (not married) | 316 | 29.6 | |
| Children | No children | 699 | 65.5 |
| Adopted children | 34 | 3.2 | |
| Biological children | 334 | 31.3 | |
| Education | Elementary | 36 | 3.4 |
| High school (partial) | 25 | 2.3 | |
| High school (complete) | 149 | 14.0 | |
| Professional | 123 | 11.5 | |
| Academic (partial) | 327 | 30.6 | |
| Academic (complete) | 407 | 38.1 | |
| Occupational status | Full time | 677 | 63.4 |
| Part time | 283 | 26.5 | |
| Unemployed | 107 | 10.0 | |
| Personal income | <4000 NIS | 278 | 26.1 |
| 4000–7000 NIS | 398 | 37.3 | |
| 7000–10,000 NIS | 233 | 21.8 | |
| 10,000–13,000 NIS | 82 | 7.7 | |
| >13,000 NIS | 76 | 7.1 | |
| Household income | <7000 NIS | 358 | 33.5 |
| 7000–10,000 NIS | 233 | 21.8 | |
| 10,000–15,000 NIS | 247 | 23.1 | |
| 15,000–20,000 NIS | 145 | 13.6 | |
| >20,000 NIS | 84 | 7.9 |
The exchange rate is NIS 3.8 per US$1.
NIH: New Israeli Shekel.
| Below age | n | Sum of scores | Expected under H0 | SD under H0 | Mean score |
|---|---|---|---|---|---|
| The NPAR1WAY procedure | |||||
| 0 | 97 | 8813.0 | 9845.50 | 411.852301 | 90.855670 |
| 1 | 105 | 11,690.0 | 10,657.50 | 411.852301 | 111.333333 |
Average scores were used for ties.
Donor insemination clients split by age = 35 years.
H0: Expected sum of the scores under the null hypothesis of no difference among classes; SD: Standard deviation under the null hypothesis.
| The NPAR1WAY procedure | Value |
|---|---|
| Statistic | 8813.0000 |
| Normal approximation | |
| Z | -2.5058 |
| One-sided Pr <Z | 0.0061 |
| Two-sided Pr >|Z| | 0.0122 |
| t approximation | |
| One-sided Pr <Z | 0.0065 |
| Two-sided Pr >|Z| | 0.0130 |
Donor insemination clients split by age = 35 years.
Z includes a continuity correction of 0.5.
| The NPAR1WAY procedure | Value |
|---|---|
| Chi-square | 6.2849 |
| DF | 1 |
| Pr >Chi-square | 0.0122 |
Donor insemination clients split by age = 35 years.
DF: Degrees of freedom.
| Below age | n | Sum of scores | Expected under H0 | SD under H0 | Mean score |
|---|---|---|---|---|---|
| The NPAR1WAY procedure | |||||
| 0 | 55 | 4038.0 | 4592.50 | 289.255619 | 73.418182 |
| 1 | 111 | 9823.0 | 9268.50 | 289.255619 | 88.495495 |
Average scores were used for ties.
Donor insemination clients women split by age = 37 years.
SD: Standard deviation.
| The NPAR1WAY procedure | Value |
|---|---|
| Statistic | 4038.0000 |
| Normal approximation | |
| Z | -1.9153 |
| One-sided Pr <Z | 0.0277 |
| Two-sided Pr >|Z| | 0.0555 |
| t approximation | |
| One-sided Pr <Z | 0.0286 |
| Two-sided Pr >|Z| | 0.0572 |
Z includes a continuity correction of 0.5.
Donor insemination clients women split by age = 37 years.
| The NPAR1WAY procedure | Value |
|---|---|
| Chi-square | 3.6748 |
| DF | 1 |
| Pr >Chi-square | 0.0552 |
Donor insemination clients women split by age = 37 years.
| Variable | Value | Estimate | Wald |
|---|---|---|---|
| Age | -0.045 | 5.081* | |
| Sex | Man | -0.647 | 2.749 |
| Woman | (Redundant) | – | |
| Education | Elementary | -0.414 | 0.414 |
| High school (partial) | -1.748 | 2.398 | |
| High school (complete) | 0.174 | 0.189 | |
| Professional | -0.152 | 0.147 | |
| Academic (partial) | 1.263 | 10.015** | |
| Academic (complete) | (Redundant) | – | |
| Ethnic origin | Europe/Americas | 0.521 | 1.801 |
| Asia/Africa | -0.364 | 1.385 | |
| Israel | (Redundant) | – | |
| Familial status | Married | 0.292 | 0.691 |
| Single | -0.314 | 0.839 | |
| In a relationship (not married) | (Redundant) | – | |
| Religiosity | Secular | 0.114 | 0.012 |
| Traditional | -0.249 | 0.054 | |
| Religious | -0.307 | 0.083 | |
| Orthodox | (Redundant) | – | |
| Personal income | <4000 NIS | 0.269 | 0.178 |
| 4000–7000 NIS | 0.594 | 1.346 | |
| 7000–10,000 NIS | 0.446 | 0.735 | |
| 10,000–13,000 NIS | 2.290 | 13.904** | |
| >13,000 NIS | (Redundant) | – |
-2 Log likelihood = 848.709; χ2 = 50.102; p < 0.01; n = 202.
The exchange rate is NIS 3.8 per US$1.
*p < 0.05.
**p < 0.01.
NIH: New Israeli Shekel.
| Variable | Value | Estimate | Wald |
|---|---|---|---|
| Age | 0.007 | 0.761 | |
| Sex | Man | -0.103 | 0.844 |
| Woman | (Redundant) | – | |
| Education | Elementary | 0.473 | 2.270 |
| High school (partial) | -0.572 | 2.425 | |
| High school (complete) | 0.140 | 0.674 | |
| Professional | 0.370 | 4.030* | |
| Academic (partial) | 0.230 | 2.676 | |
| Academic (complete) | (Redundant) | – | |
| Ethnic origin | Europe/Americas | -0.252 | 3.445 |
| Asia/Africa | -0.431 | 9.219** | |
| Israel | (Redundant) | – | |
| Familial status | Married | -0.282 | 3.920* |
| Single | -0.046 | 0.107 | |
| In a relationship (not married) | (Redundant) | – | |
| Religiosity | Secular | 1.336 | 3.300 |
| Traditional | 1.182 | 2.565 | |
| Religious | 1.224 | 2.736 | |
| Orthodox | (Redundant) | – | |
| Personal income | <4000 NIS | -0.934 | 12.642** |
| 4000–7000 NIS | -0.652 | 7.219** | |
| 7000–10,000 NIS | -0.481 | 4.028* | |
| 10,000–13,000 NIS | -0.432 | 2.309 | |
| >13,000 NIS | (Redundant) | – |
-2 Log likelihood = 4477.562; χ2 = 45.444; p < 0.01; n = 1067.
The exchange rate is NIS 3.8 per US$1.
*p < 0.05.
**p < 0.01.
NIH: New Israeli Shekel.
| Variable | Value | Frequency | % |
|---|---|---|---|
| Single | 102 | 70.8 | |
| In a relationship (not married) | 42 | 29.2 | |
| Education | High school (partial) | 13 | 9.0 |
| High school (complete) | 35 | 24.3 | |
| Professional | 18 | 12.5 | |
| Academic (partial) | 31 | 21.5 | |
| Academic (complete) | 47 | 32.6 | |
| Occupational status | Full time | 115 | 79.9 |
| Part time | 4 | 2.8 | |
| Unemployed | 5 | 3.5 | |
| Personal income | <4000 NIS | 24 | 16.7 |
| 4000–7000 NIS | 42 | 29.2 | |
| 7000–10,000 NIS | 42 | 29.2 | |
| 10,000–13,000 NIS | 19 | 13.2 | |
| >13,000 NIS | 7 | 11.8 | |
| Household income | <7000 NIS | 44 | 30.6 |
| 7000–10,000 NIS | 31 | 21.5 | |
| 10,000–15,000 NIS | 25 | 17.4 | |
| 15,000–20,000 NIS | 30 | 20.8 | |
| >20,000 NIS | 14 | 9.7 |
The exchange rate is NIS 3.8 per US$1.
NIH: New Israeli Shekel.
| Willingness to donate | Very low | Low | Medium | High | Very high |
|---|---|---|---|---|---|
| Willingness to donate altruistically | 13.7% | 27.5% | 26.5% | 14.7% | 17.6% |
| Willingness to donate for payment | 29.7% | 10.9% | 24.8% | 21.8% | 12.9% |
| Reason | Mean | SD |
|---|---|---|
| I feel committed to my nation | 2.715 | 1.513 |
| I think that helping each other is important | 2.571 | 1.440 |
| I was raised with values of giving | 3.035 | 1.411 |
| Giving makes me feel fulfilled | 3.174 | 1.401 |
| I understand the longing for a child | 2.924 | 1.385 |
| I know personally people who need a donation | 2.500 | 1.389 |
| Helping other people helps me feel better with myself | 2.799 | 1.427 |
| Donation is an opportunity to do something meaningful | 2.387 | 1.373 |
| Through donation I can spread my genes | 2.085 | 1.301 |
| I agree to donate only to a woman I know personally | 2.570 | 1.441 |
SD: Standard deviation.
| Sum (NIS) | Frequency | % |
|---|---|---|
| 10–100 | 10 | 6.9 |
| 101–200 | 2 | 1.4 |
| 201–300 | 1 | 0.7 |
| 301–400 | 2 | 1.4 |
| 401–500 | 23 | 16.0 |
| 501–600 | 33 | 22.9 |
| 601–700 | 21 | 14.6 |
| 701–800 | 12 | 8.3 |
| 801–900 | 17 | 11.8 |
| 901–1000 | 23 | 16.0 |
| Total | 144 | 100.00 |
The exchange rate is NIS 3.8 per US$1.
NIS: New Israel Shekel.
| Variable | Value | Estimate | Wald |
|---|---|---|---|
| Education level | High school (partial) | 0.214 | 0.109 |
| High school (complete) | -0.814 | 2.663 | |
| Professional | -0.558 | 1.072 | |
| Academic (partial) | -1.151 | 4.691* | |
| Academic (complete) | (Redundant) | – | |
| Religiosity | Secular | 0.491 | 1.390 |
| Traditional | 0.580 | 1.651 | |
| Religious | (Redundant) | – | |
| Personal income | <4000 NIS | -0.029 | 0.002 |
| 4000–7000 NIS | 0.238 | 0.154 | |
| 7000–10,000 NIS | -0.153 | 0.081 | |
| 10,000–13,000 NIS | -0.232 | 0.149 | |
| >13,000 NIS | (Redundant) | – |
-2 Log likelihood = 455.420; χ2 = 13.872; n = 144.
The exchange rate is NIS 3.8 per US$1.
*p < 0.05.
**p < 0.01.
NIH: New Israeli Shekel.
Background
The modern reproductive market is dominated by principles of economic theory.
These economic realities raise significant questions relating to our understanding of the motivations, interests, relative power dynamics, and welfare of the parties in the reproductive market.
The questions we asked
What are the private and social benefits of donor insemination (DI) in Israel?
Summary answer
DI delivers benefits and appears to have contributed to improved wellbeing.
Study design, size & duration
Surveys were carried out among the general public (Jewish Israeli men and women – 1067 valid questionnaires), DI clients (single women, and heterosexual or lesbian couples – 202 valid questionnaires), and potential sperm donors, (single males aged 18–40 years – 144 valid questionnaires).
The study was conducted over one year in 2014.
Participants/materials, setting – methods
The proposed research deals with the implications of the DI market and its resulting effect on private and social welfare by employing a cost-benefit analysis (CBA).
An empirical model investigates the general public and DI clients' willingness to pay (WTP) for DI, as well as the willingness of potential donors to become altruistic or paid sperm donors.
Main results
The findings demonstrate that the general public and DI clients value DI and have a positive WTP for DI.
The average WTP for DI, amongst the general public, is US$855 whereas for the DI clients' it is US$724.
The general public, and the DI clients' are willing to pay for DI on average more than it costs for buyers, on average US$ 605.
The willingness to donate, altruistically or for payment, is either low or very low among more than 40% of the respondents.
The average monetary amount among approximately 50% of the potential donors who show willingness to accept payment for donation is lower than the amount that is actually paid for a donation, on average US$138.
Limitations, reasons for caution
Within CBA, the benefits of an intervention are assessed using the contingent valuation (CV) technique, which is subject to certain criticism.
The criticism revolves mainly around two aspects; namely, the validity and the reliability of the results, and the effects of various biases and errors.
In order to overcome the controversy over the ability of the CV method to predict the value of DI, I followed the recommendations and instructions put forth by the US National Oceanographic and Atmospheric Administration (NOAA, 1993) panel.
Wider implications of the findings
This present study combines and tests both the DI clients and the general public's WTP for DI. It is also considers the option of altruistic sperm donations.
Israel is a productive arena for this kind of study due to local socio-cultural characteristics of fertility patterns. Paid donation is well established in Israel, and the consideration of an altruistic gamete donation is both necessary and important.
The findings demonstrate that the general public and the DI clients value DI and have a positive WTP for DI. This suggests that DI delivers benefits and appear to have contributed to improved wellbeing.
The study contributes solid data to the debate regarding whether the government should participate in the funding of the DI process and/or encourage altruistic sperm donation through the use of the general public medical insurance, given the limited public resources.
The theoretical economic idea behind public funding is to encourage intervention up to the point where the marginal social cost to the government will equal the marginal social utility derived from the DI procedure. Since in the present paper, it was found that the general public and the DI l clients are willing to pay for DI on average more than the buyer is actually asked to pay, this suggests that the government should consider funding or subsidizing DI.
Statistical analysis indicates that the Israeli government should intervene in the gamete market and support altruistic sperm donation through information and education, so as to improve public welfare.
This study's findings bear critical implications for a range of institutions and individuals involved in the field of DI in general.
Health economists who develop economic instruments for utility estimation of medical intervention in general may also benefit from this kind of analysis and research.
Financial & competing interests disclosure
The author has no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The author states that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Supplementary Material
File (suppl_material.docx)
- Download
- 40.13 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Almeling R. Gender and the value of bodily goods: commodification in egg and sperm donation. Law Contemp. Probl. 72(3), 37–58 (2009).
2.
Bridgewater PD. Reconstructing rationality: towards a critical economic theory of reproduction. Emory Law J. 56, 1215–1234 (2007).
•• Presents economic realities that raise significant questions relating to the understanding of the motivations, interests and relative power dynamics of parties in the reproductive market.
3.
Becker G. An economic analysis of fertility. In: Demographic & Economic Change in Developed Countries. Universities-National Bureau Conference Series. Columbia University Press, NJ, USA, 209–240 (1960).
4.
Becker G. A theory of the allocation of time. Economic J. 75, 493–517 (1965).
5.
Easterlin R. An economic framework for fertility analysis. Stud. Fam. Plan. 6, 54–63 (1975).
6.
Easterlin R. The economics and sociology of fertility: a synthesis. In: Historical Studies of Changing Fertility. Princeton University Press, NJ, USA, 57–133, (1978).
7.
Easterlin R, Crimmins E. The Fertility Revolution: A Supply-Demand Analysis. University of Chicago Press, IL, USA, 209 (1985).
8.
Spiegel U, Gonen LD, Templeman J. Economic implications of in vitro fertilization using willingness to pay. J. Public Health 21(6), 535–557 (2013).
9.
Sanger C. Developing markets in baby making: in the matter of baby M. Harvard J. Law Gender 30, 67–97 (2007).
10.
Pi VL. Regulating sperm donation: why requiring exposed donation is not the answer. Duke J. Gender Law Policy 16(2), 379–401 (2009).
11.
Bowen JM, Hughes E, O’Reilly DJ, Perampaladas K, Xie F. Presentation to Assisted Human Reproduction Canada (AHRC) (2010). http://publications.gc.ca/collections/collection_2011/pac-ahrc/H176-2-2011-eng.pdf
12.
Blyth E, Crawshaw M, Haase J, Speirs J. The implications of adoption for donor offspring following donor-assisted conception. Child & Family Social Work. 6, 295–304 (2001).
13.
Golombok S, Murray C, Brinsden P, Abdalla H. Social versus biological parenting: family functioning and the socioemotional development of children conceived by egg or sperm donation. In: Annual Progress In Child Psychiatry And Child Development. Hertzig ME, Farber EA (Eds). Brunner-Routledge, NY, USA, 155–175 (2003).
14.
Murray C, Golombok S. Solo mothers and their donor insemination infants: follow-up at age 2 years. Hum. Reprod. 20, 1655–1660 (2005).
15.
Zeifman DM, MA JE. Experimental examination of women’s selection criteria for sperm donors versus life partners. Pers. Relationships 20, 311–327 (2013).
16.
Silver AJ, Larson JL, Silver MJ et al. Carrier screening is a deficient strategy for determining sperm donor eligibility and reducing risk of disease in recipient children. Genet. Test. Mol. Biomarkers 20(6), 276–284 (2016).
17.
Sims CA, Callum P, Ray M, Iger J, Falk RE. Genetic testing of sperm donors: survey of current practices. Fertil. Steril. 94(1), 126–129 (2010).
18.
Daniels KR, Lewis GM. Donor insemination: the gifting and selling of semen. Soc. Sci. Med. 42(11), 1521–1536 (1996).
• Points to two models of semen provision upon which my paper is based: commercial and donor-based.
19.
Pietrzak A. The price of sperm: an economic analysis of the current regulations supporting the gamete donation industry. J. Law Fam. Stud. 14, 121–135 (2012).
•• Discusses the Laissez-Faire approach to the sperm donation industry and raises several complex questions regarding government intervention, healthcare, insurance, religion, science and ethics.
20.
Swanson KW. Body Banks: A History Of Milk Banks, Blood Banks, And Sperm Banks In The United States. Oxford University Press on behalf of the Business History Conference, Oxford, UK (2011).
21.
Hasan O, Johnson A, Lipton S, Turow R. Infertility treatment: an overview; new ways of making babies: the biology, ethics and policy of infertility. (2013). www.stanford.edu/class/siw198q/websites/reprotech/New%20Ways%
22.
Spar DL. The Baby Business: How Money, Science, And Politics Drive The Commerce Of Conception. Harvard Business School Press. Boston, MA, USA (2006).
• The reproductive market is identified as a ‘market’, given the involved elements of demand and supply, prices that link supply and demand, and businesses that sell their products.
23.
Yee S. ‘Gift without a price tag’: altruism in anonymous semen donation. Hum. Reprod. 24(1), 3–13 (2009).
•• Deals with the concept of altruism in gamete donation, given the complexity and the dynamics involved.
24.
Pennings G. The rough guide to insemination: cross-border travelling for donor semen due to different regulations. Facts Views Vis. OBGYN Mongraph, 55–60 (2010).
25.
Blyth E. Fertility patients’ experiences of cross-border reproductive care. Fertil. Steril. 94, e11–e15 (2010).
26.
Hudson N, Culley L, Blyth E, Norton W, Rapport F, Pacey A. Cross-border reproductive care: a review of the literature. Repro. BioMed. Online 22, 673–685 (2011).
27.
Inhorn MC, Gürtin ZB. Cross-border reproductive care: a future research agenda. Reprod. Biomed. Online 23, 665–676 (2011).
28.
Inhorn MC, Patrizio P. Infertility around the globe: new thinking on gender, reproductive technologies and global movements in the 21st century. Hum. Reprod. Update 21(4), 411–426 (2015).
29.
McMillan J. The Bazaar: A Natural History of Markets. W. W. Norton, NY, USA (2002).
30.
Gonen LD. Social and private benefits of assisted reproductive technology: a national survey-based evaluation in Israel. J. Comp. Eff. Res. 5(1), 49–63 (2016).
31.
Birenbaum-Carmeli D. Thirty-five years of assisted reproductive technologies in Israel. Repro. BioMed. Soc. Online 2, 16–23 (2016).
• Presents the assisted reproductive technology market in Israel and the donor insemination market included within it.
32.
Birenbaum-Carmeli D, Carmeli YS, Yavetz H. Secrecy among Israeli recipients of donor insemination. Polit. Life Sei. 19, 69–76 (2000).
33.
Safir M. Religion, tradition and public policy give family first priority. In: Calling the Equality Bluff. Swirski B, Safir MP (Eds). Pergamon, NY, USA, 57–65 (1991).
34.
Birenbaum-Carmeli D. “Cheaper than a newcomer”: on the social production of IVF policy in Israel. Social Health Bin. 26, 897–924 (2004).
35.
Birenbaum-Carmeli D, Carmeli YS. Reproductive policy in context: implications on the rights of Jewish women in Israel, 1945–2000. Policy Stud. 24(2), 101–114 (2003).
36.
Birenbaum-Carmeli D, Carmeli YS. Reproduction and reproductive technologies in Israel: an introduction. In: Kin, Gene, Community: Reproductive Technology Among Jewish Israelis. Birenbaum-Carmeli D, Carmeli YS (Eds). Berghahn Books, Oxford and New York (2008).
37.
Ministry of Health, State of Israel, Sperm Bank Regulations. Director General’s circular: management of sperm banks and artificial insemination – regulations regarding the management of a sperm bank and instructions for carrying out artificial insemination. 13 November 1992.
38.
Ravitsky V. The right to parenthood in an age of technological insemination. In Dilemmas in Medical Ethics. Cohen-Almagor R (Ed.). HaKibbutz HaMeuchad and the Van Leer Institute, (2002).
39.
Israeli Ministry of Health. www.health.gov.il/Subjects/Med_Inst/Sperm_Bank/Documents/sperm_banks_Israel.pdf
40.
Donath O. Regretting motherhood: a sociopolitical analysis. J. Women Culture Soc. 40(2), 343–367 (2015).
41.
Israeli Ministry of Health. www.health.gov.il/Subjects/Med_Inst/Sperm_Bank/Documents/sperm_banks_abroad.pdf
42.
Doron A. What is the most highly demanded product? Donor sperm. NRG. (2011). www.nrg.co.il/online/1/ART2/244/578.html
43.
Olsen AR, Smith EP. Introduction to special issue on surveys over time. J. Agric. Biol. Environ. Stat. 4(4), 328–330 (1999).
44.
Olsen D, Smith R. Theory versus practice: a review of ‘willingness to pay’ in health and health care. Health Econ. 10, 39–52 (2001).
•• The willingness to pay methodology that I use in the empirical model in my paper is presented.
45.
Cummings RG, Brookshire DS, Schulze WD. Valuing Environmental Goods: An Assesssment of the Contingent Valuation Method. Rowman & Allanheld, NJ, USA (1986).
46.
Mitchell RC, Carson RT. Using Surveys to Value Public Goods: The Contingent Valuation Method. Resources for the Future, WA, USA (1989).
47.
Carson R, Wright J, Alberini A, Carson N, Flores N. A Bibliography Of Contingent Valuation Studies And Papers. Natural Resource Damage Assessment, CA, USA (1994).
48.
Diener A, O’Brien B, Gafni A. Health care contingent valuation studies: a review and classification of the literature. Health Econ. 7(4), 313–326 (1998).
• The cost–benefit analysis on which I based my empirical model is presented.
49.
NOAA. National Oceanic and Atmospheric Administration. Report of the NOAA panel on contingent valuation. Federal Register. 58, 4602–4614 (1993).
50.
Thomas R, Donaldson C, Torgerson D. Who answers ‘willingness to pay’ questions? J. Health Serv. Res. Policy 5, 7–11 (2000).
51.
Donaldson C, Shackley P, Abdalla M, Miedzybrodzka Z. Willingness to pay for antenatal carrier screening for cystic fibrosis. Health Econ. 4, 439–452 (1995).
52.
Johannesson M, Jonsson B. Economic evaluation in health care: is there a role for cost-benefit analysis? Health Policy 17, 1–23 (1991).
53.
Klose T. The contingent evaluation method in health care. Health Policy 47, 97–123 (1991).
54.
Arrow K. Uncertainty and the welfare economics of medical care. Am. Econ. Rev. 53(5), 941–973 (1963).
55.
Ryan M. Should government fund assisted reproductive techniques? A study using willingness to pay. Appl. Econ. 29(7), 841–849 (1997).
56.
Carmeli YS, Birenbaum-Carmeli D. Ritualizing the ‘natural family’: secrecy in Israeli donor insemination. Sci. Culture 9(3), 301–325 (2000).
57.
Allan S. Donor conception, secrecy and the search for information. J. Law Med. 19(4), 631–650 (2012).
58.
Menken J, Trussell J, Larsen U. Age and infertility. Science 233(4771), 1389–1394 (1986).
59.
Faddy MJ, Gosden RG, Gougeon A, Richardson SJ, Nelson JF. Accelerated disappearance of ovarian follicles in mid-life: implications for forecasting menopause. Hum. Reprod. 7, 1342–1346 (1992).
60.
Schwartz D, Mayaux MJ. Female fecundity as a function of age: results of artificial insemination in 2193 nulliparous women with azoospermic husbands. Federation CECOS. N. Engl. J. Med. 306, 404–406 (1982).
61.
Shenfield F, Doyle P, Valentine A, Steele SJ, Tan SL. Effects of age, gravidity and male infertility status on cumulative conception rates following artificial insemination with cryopreserved donor semen: analysis of 2998 cycles of treatment in one centre over 10 years. Hum. Reprod. 8, 60–64 (1993).
62.
Van Noord-Zaadstra BM, Looman CW, Alsbach H, Habbema JD, te Velde ER, Karbaat J. Delaying childbearing: effect of age on fecundity and outcome of pregnancy. BMJ 302(6789), 1361–1365 (1991).
63.
Virro MR, Shewchuk AB. Pregnancy outcome in 242 conceptions after artificial insemination with donor sperm and effects of maternal age on the prognosis for successful pregnancy. Am. J. Obstet. Gynecol. 148, 518–524 (1984).
64.
Cook R, Golombok S. A survey of semen donation: Phase II – the view of the donors. Hum. Reprod. 10, 951–959 (1995).
65.
Lui SC, Weaver SM, Robinson J et al. A survey of semen donor attitudes. Hum Reprod. 10, 234–238 (1995).
66.
Lyall H, Gould GW, Cameron IT. Should semen donors be paid? A survey of the attitudes of the general public. Hum. Reprod. 13, 771–775 (1998).
67.
Lui SC, Weaver SM. Attitudes and motives of semen donors and non-donors. Hum. Reprod. 11, 2061–2066 (1996).
68.
Healy K. Embedded altruism: blood collection regimes and the European Union’s donor population. Am. J. Sociol. 105, 1633–1657 (2000).
69.
Centers for Disease Control and Prevention (CDC). Awareness of family health history as a risk factor for disease. Morb. Mortal. Wkly Rep. 53(44), 1044 (2004).
70.
Ravitsky V. Conceived and deceived: the medical interests of donor-conceived individuals. Hastings Center Report 42, 17–22 (2012).
71.
Turner A, Coyle A. What does it mean to be donor offspring? the identity experience of adults conceived by donor insemination and the implications for counselling and therapy. Hum. Reprod. 15(9), 2041 (2000).
72.
Jadva V, Freeman T, Kramer W, Golombok S. Experiences of offspring searching for and contacting their donor siblings and donor. Reprod. Biomed. Online 20(4), 523–532 (2010).
73.
Daniels K. Donor gametes: anonymous or identified? Best Pract. Res. Clin. Obstet. Gynaecol. 21, 113–128 (2007).
Information & Authors
Information
Published In
Copyright
© Future Medicine Ltd.
History
Published online: 17 November 2016
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Donor insemination: Israel as a representative case of a competitive market examining the possibility of policy reform. (2016) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0066
Export citation
Select the citation format you wish to export for this article or chapter.