CYD-TDV dengue vaccine: systematic review and meta-analysis of efficacy, immunogenicity and safety
Abstract
Introduction: Dengue virus (DENV) is a serious global health problem. CYD-TDC (Dengvaxia®) was the first vaccine to gain regulatory approval to try and address this problem. Aim: Summarize all available evidence on the immunogenicity, efficacy and safety of the CYD-TDV dengue vaccine. Method: Meta-analysis and systematic review. Results: The best and worst immunogenicity results were for DENV4 and DENV1, respectively. Vaccine efficacy of 60% was derived from studies with participants aged 2–16 years old, with DENV4 and DENV2 presenting the best and worst results, respectively. Erythema and swelling were more frequent with CYD-TDV. No differences were detected for systemic adverse events. Conclusion: CYD-TDV showed moderate efficacy in children and adolescents. From the immunogenicity results in adults, we can expect satisfactory efficacy from vaccination in this population.






First draft submitted: 1 July 2016; Accepted for publication: 11 November 2016; Published online: 13 January 2017
Dengue is a mosquito-borne virus disease considered a serious global health problem with an estimated 390 million dengue infections per year [1]. Most dengue virus infections are asymptomatic, and clinical manifestations range from mild fever to severe life-threatening disease [2–6]. Dengue virus (DENV) belongs to the genus Flavivirus of the Flaviviridae family [3,4], and has four DENV serotypes (DENV1–4) with distinct phylogenetic and antigenic characteristics [3,4,7,8,9].
Dengue is rapidly expanding and has a global footprint, representing a public health challenge with an appreciable economic burden. Trade globalization and rapid urbanization in Asia and Latin America, and the abundance of vector breeding sites within crowded urban communities, have contributed to the endemicity observed in these regions [3,4,10]. It is estimated that in 2013 there were a total of 58.40 million symptomatic DENV infections, including more than 13,500 fatal cases [11]. For 2015, it was estimated that over 3.9 billion people lived at risk for infection worldwide [2]. The annual costs of dengue have ranged from US$ 13.5 million in Nicaragua to US$56 million in Malaysia (in 2010 values) up to 2013 [12]. Considering 141 countries and territories with active dengue transmission, the total annual global cost of dengue illness was estimated at US$8.9 billion in 2013 [11].
The development of an effective vaccine against the four DENV serotypes represents an important strategy for the control of the disease [13,14]. The vaccines for monotype Flavivirus, such as yellow fever, Japanese encephalitis, have a 95% efficacy and were used as an inspiration for the development of a dengue vaccine [15,16]. Since the 1970s, several techniques have been applied to provide a vaccine capable of inducing immunity to the four virus serotypes [11]. Several vaccine candidates have been developed using live attenuated viruses, inactivated viruses and DNA vaccines [13,14,17–33]. The tetravalent dengue vaccine (CYD-TDV) of Sanofi Pasteur, Dengvaxia®, contains four recombinant viruses engineered with DENV1–4 and capsid proteins of the attenuated Yellow Fever (YF-17D) vaccine virus [29]. CYD-TDV was the first vaccine to be licensed to dengue prevention [34]. By October 2016, 11 countries had granted regulatory approval for Dengvaxia®, for example, Mexico, Philippines, Brazil, El Salvador, Costa Rica, Paraguay, Guatemala, Peru, Indonesia, Thailand and Singapore [34–38]. Vaccination is indicated for individuals living in endemic regions aged between 9 and 45 years old, with the exception of Paraguay which extended the upper limit to people of 60 years old [39].
The capacity of a vaccine to generate an immune response may be influenced by many factors including age, presence of underlying disease, immune status and previous exposure to the same or similar substances (seropositivity). It is likely that in endemic settings, presensitization may cause an immune response before vaccination [40], which may have been the case with CYD-TDV. In Phase III trials, vaccination showed lower efficacy in seronegative individuals, suggesting that the vaccine broadens pre-existing immunity rather than efficiently raises new protective immunity [41,42].
The lower age limit of 9 years old for CYD-TDV vaccination is explained by the results from the age stratified analysis of the two available multicentric double-blind randomized controlled trials conducted with subjects between 2 and 16 years old [30,31]. More importantly, long-term safety analysis revealed a higher risk of hospitalization due to dengue in patients vaccinated between 2 and 5 years old [43]. Up to now, there has been no published Phase III trial with adults, and the indication for adult vaccination is probably derived from immunogenicity results.
In this context, it was demonstrated that with a routine CYD-TDV vaccination program in endemic countries at 9 years of age, a reduction of 10–30% in symptomatic and hospitalized dengue illness is expected over the next 30 years [41,44]. In addition, Ferguson et al. developed a model that considering routine vaccination at 80% coverage of individuals between 2 and 18 years old, there was an expected reduction of 20–30% in both symptomatic disease and hospitalization in high-transmission settings [45]. Both models predicted that as transmission intensity increased, the optimal age for routine vaccination decreased [44,45].
The purposes of this systematic review with meta-analysis were to access efficacy and safety of CYD-TDV and for the first time explore its immunogenicity results, as to better understand the indication of the vaccine to this age group. As a result, help governments with their ongoing deliberations regarding the utilization and funding of such vaccines.
Methods
We conducted a systematic review with meta-analysis following principles described in the Cochrane Handbook [46]. The manuscript was prepared using the Preferred Reporting Items for Systematic Reviews and Meta-Analysis [47].
Eligibility criteria
We considered for inclusion all Phase II and III randomized clinical trials of Sanofi Pasteur's tetravalent dengue vaccine (CYD-TDV) as well as a control group including placebo or other vaccines, for example, pneumococcal polysaccharide or meningococcal polysaccharide, or a combination of these. We considered studies assessing safety, immunogenicity and efficacy of the vaccine in children, adolescents and adults. We excluded Phase I trials and studies that had not reported outcomes of interest. Our population of interest involved individuals in dengue endemic regions independents of age (i.e., children, adolescent and adult). We also excluded Phase IIb in this analysis due to the differences between the populations involved in the Phase IIb and III trials making the analysis difficult.
Study search
Article searches were performed in the Cochrane Controlled Trials Register, PubMed and LILACS (March/2016). Various combinations of terms were used to search these electronic databases, including terms referring to the disease, interventions and types of studies. The complete search strategies are provided as Supplementary Material (Search Strategy).
We also searched for trials at ClinicalTrials.gov. Ongoing trials were assessed for eligibility, and studies described as completed were manually searched (when not captured by the initial search strategy). A gray literature search was also performed at ProQuest Dissertation and Theses Database. In addition, considering the importance of dengue in Brazil, we used the following theses and dissertations databases in Brazil: Brazilian Digital Library of Theses and Dissertations, the Digital Library of Theses and Dissertations of USP (University of São Paulo) and of UFMG (Universidade Federal de Minas Gerais).
Study selection & data collection processes
Two independent reviewers (Isabella Piassi Godói, Braúlio Cesar Bonoto) performed the selection of potential papers in three phases, in other words, the analyses of titles, abstracts and whole texts. A third reviewer (Livia Lovato Pires Lemos) analyzed any dissimilar results to resolve any differences. Three independent researchers collected the data (Isabella Piassi Godói, Braúlio Cesar Bonoto, Livia Lovato Pires Lemos). When reports mentioned the existence of supplementary material or appendix, they were consulted for data collection.
Outcome measures
For immunogenicity, we considered the geometric mean titers of neutralizing antibodies against each dengue serotype 28 days after the last dose of vaccination. In this test, the sera were tested by plaque reduction neutralization test (PRNT), a geometric interpretation of the titers of selected human sera against DENV (1–4) [48]. As a result, the participants with PRNT50 >10 against one or more serotypes were considered seropositive. For efficacy measures, we considered the number of virologically confirmed dengue cases and the number of person-years of follow-up in each group. For this evaluation, blood samples were taken from all participants at month 13 (28 days after the third dose), per protocol analysis. The intention to treat efficacy population included volunteers who receive ≥1 dose, and the efficacy against each serotype was determined by episodes occurring from month 13–25 in the modified per-protocol population, in other words, participants who had received all three doses [30,31]. For adverse, events and safety measures, we considered the following: Injection site reactions (0–7 days after first dose) (pain, erythema and swelling); systemic safety parameters in any grade (fever, headache, malaise, myalgia, arthralgia); serious adverse events (SAEs) were collected until 21 or 28 days after each vaccination scheme. A risk ratio lower than 1.0 demonstrated better results for CYD-TDV.
Statistical analysis
We used the Review Manager® 5.3 software to pool data using a random effects meta-analysis model. Analyses with an I2> 40% and p-value for the X2 test < 0.10 [49] were considered to have substantial heterogeneity. We presented the risk ratio (dichotomous) and the mean difference (continuous) with a 95% CI as association measures and the results of I2 and p-value of the heterogeneity test. Subgroup analysis was performed to evaluate the immunogenicity and safety results according to geographic region (Supplementary Table 2).
Quality of evidence & risk of bias
We assessed the risk of bias of the clinical trials using the Cochrane Collaboration methodology. We judged the possible bias in three levels – high risk, low risk and unclear (when the provided information was not sufficient to make a clear judgment). We considered the following possible bias: random sequence generation and allocation concealment (selection bias); blinding of participants and personnel (performance bias); blinding of outcome assessment (detection bias); and selective reporting (reporting bias) [50]. For studies with laboratory measures or efficacy as an outcome, blinding of participants and personnel was considered of minor importance. In these cases, the trials were judged as presenting a low risk of bias for performance bias. Since safety assessments typically include subjective outcomes such as pain and myalgia, blinding of participants and personnel was considered of high importance. If the same study reported laboratory/efficacy and safety outcomes and the participants were not blinded, the judgment was a high risk for performance bias.
Results
Study inclusion
Of the 895 titles screened, the abstracts of 321 records were assessed, and among these, 89 full-text studies were assessed for eligibility. Six Phase II [23–28] and three Phase III randomized clinical trials [29–31] were included. Figure 1 provides details of how the final nine studies were derived. From the search at ClinicalTrials.gov, we included one ongoing trial in Phase II trials for CYD-TDV (Figure 1).
Characteristics of the studies
Three Phase III trials evaluated CYD-TDV [29–31]. All included studies were conducted in endemic areas of Latin America [21,23,25,28] or Southeast Asia [24,26,27,29,30] (Table 1). A total of 34,631 volunteers participated in CYD-TDV Phase II-III trials (CYD-TDV, n = 23,193; control, n = 11,438). The trials applied a 2:1 [23–25,27,28,30,31], 3:1 [26] and a 4:1 [29] randomization ratio. Vaccine schedule was of three doses with 6 months interval. The control groups of the Phase II trials were composed of a combination of placebo (one or two doses) and another vaccine (e.g., pneumococcal polysaccharide, meningococcal polysaccharide) (one or two doses).
All Phase III studies were placebo controlled. As a group, the Phase II trials evaluated children adolescents and adults (2–45 years old), whereas Phase III trials were conducted only with children and adolescents (2–17 years old) (Table 1). 6% of participants did not complete the CYD-TDV vaccination schedule in the Phase II trials [23–28]. Two Phase III trial reported losses to follow-up (0.8% in the CYD-TDV) [29,30]. The main reason for the losses to follow-up was voluntary withdrawal not due to an adverse event (Supplementary Table 1). This vaccine was approved for individuals between 9–45 and 9–60 years old [39].
There is one study ongoing Phase II randomized control trial (NCT01943305) that evaluates CYD and is being conducted in Singapore with 90 volunteers (18–45 ages), expected to be completed by the end of 2016. This study is being funded by Sanofi Pasteur and the Medical School of Singapore, with the Singapore General Hospital collaborating.
Methodological quality & risk of bias
All trials presented low risk of bias for important aspects, such as random sequence generation, allocation concealment and selective reporting. The losses to follow-up of the included trials were few and balanced between vaccine and control arms, resulting in low risk of attrition bias in most studies. In one trial, the reasons participants did not complete as per the protocol vaccination schedule was not completely reported, resulting in unclear risk for attrition bias (Figure 2) [26].
Immunogenicity
All meta-analysis results favored CYD for both children and adolescents (2–16 years old) [21,23,25,26,28,29] and adults [26,27]. The best results for serotype-specific immune response 28 days after the last dose of CYD or control in both groups were for DENV4 (children and adolescents, MD = 0.84; 95% CI: 0.73, 0.95; I2 = 0%; p = 0.71; adults, MD = 0.77; 95% CI: 0.60, 0.93; I2 = 0%; p = 0.97) and DENV3 (children and adolescents, MD = 0.67; 95% CI: 0.55, 0.79; I2 = 9%; p = 0.36; and adults, MD = 0.72; 95% CI: 0.56, 0.89; I2 = 0%; p = 0.96). DENV1 was the worst result for children and adolescents (MD = 0.41; 95% CI: 0.23, 0.58; I2 = 58%; p = 0.03) and adults (MD = 0.46; 95% CI: 0.30, 0.63; I2 = 0%; p = 0.79). The immunogenicity was presented in Figure 3A (children and adolescent) and Figure 3B (adults).
Efficacy
The pooled analysis of 27,355 person-years [30,31] showed a global risk ratio of 0.41 (95% CI: 0.35, 0.48; I2 = 0%; p = 0.52). The global efficacy of 59% was found after 28 days after the third dose (13 months) (per protocol analysis) (Figure 4).
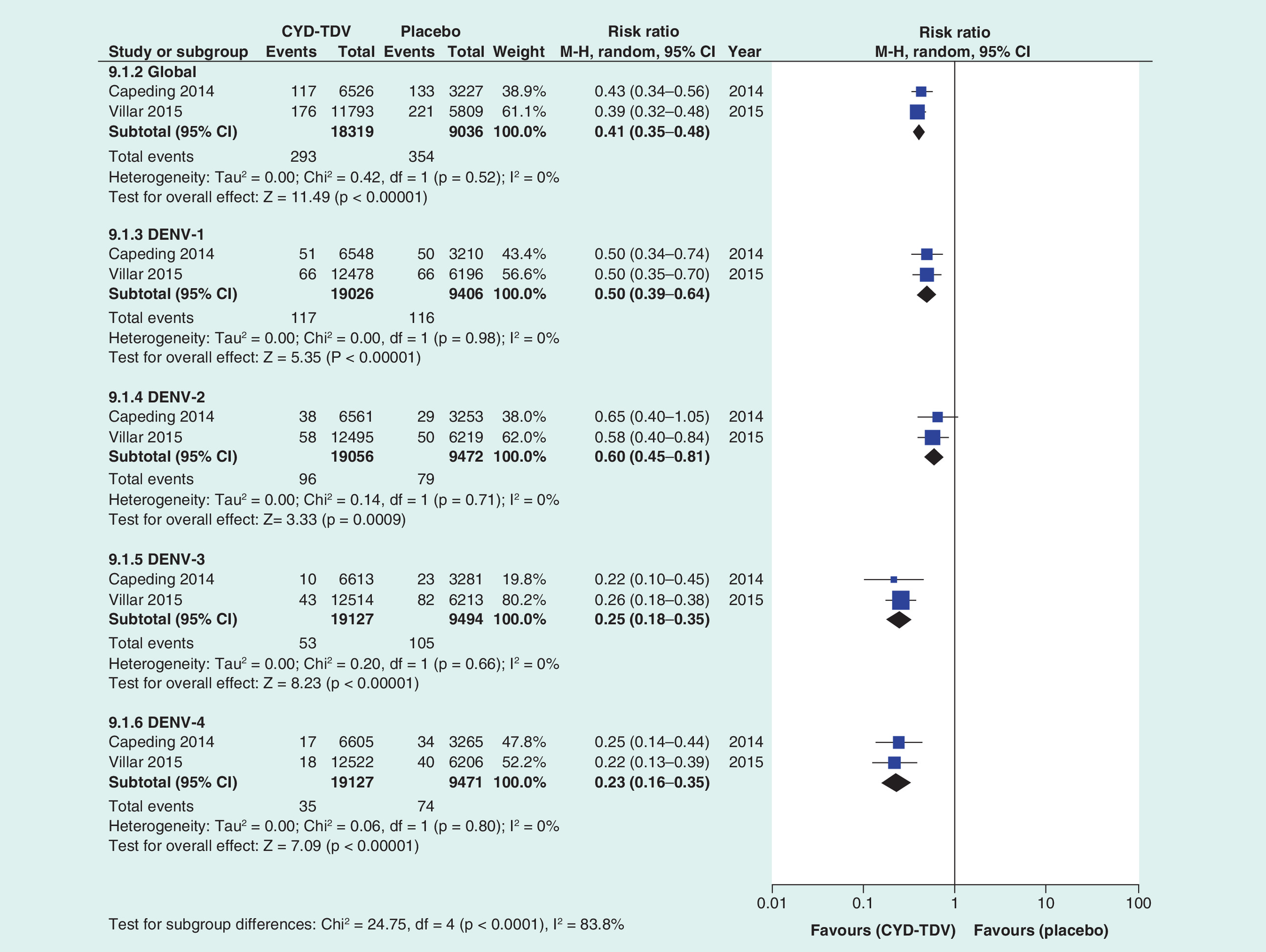
Intention to treat analysis revealed a global efficacy of 60% (RR = 0.40; 95% CI: 0.31, 0.51; I2 = 79%; p = 0.003) and serotype stratified analysis showed that DENV4 and DENV2 presented the best and worst results, respectively 77% (RR = 0.23; 95% CI: 0.16, 0.34; I2 = 39%; p = 0.20) and 43% (RR = 0.57; 95% CI: 0.44, 0.74; I2 = 36%; p = 0.21) (Figure 5).
Vaccine efficacy in the cohort of DENV seropositive patients at baseline was 78% (RR = 0.22; 95% CI: 0.14, 0.35; I2 = 0%; p = 0.36). The meta-analysis result for seronegative patients at baseline was not statistically significant (RR = 0.62; 95% CI: 0.37, 1.03; I2 = 0%; p = 0.82) (Figure 6).
Safety
Injection site reactions seen with CYD-TDV were erythema (RR = 0.55; 95% CI: 0.34, 0.89; I2 = 70%; p = 0.005) and swelling (RR = 0.33; 95% CI: 0.17, 0.64; I2 = 67%; p = 0.009). No differences were detected between CYD-TDV and the control arm for the following outcomes: pain (RR = 0.71; 95% CI: 0.45, 1.12; I2 = 91%; p < 0.0001); fever (RR = 1.20; 95% CI: 0.78, 1.83; I2 = 65%; p = 0.02); malaise (RR = 1.19; 95% CI: 0.98, 1.45; I2 = 44%; p = 0.11); headache (RR = 1.12; 95% CI: 0.88, 1.42; I2 = 72%; p = 0.003); myalgia (RR = 0.85; 95% CI: 0.63, 1.16; I2 = 73%; p = 0.05); and asthenia (RR = 1.03; 95% CI: 0.72, 1.47; I2 = 57%; p = 0.07). SAEs occurred more frequently in the control group when compared with CYD-TDV (RR = 0.76; 95% CI: 0.59, 0.98; I2 = 28%; p = 0.20). With exception of SAE, all other meta-analysis presented high heterogeneity (Table 2).
Subgroup & heterogeneity analysis
For global efficacy (intention to treat), the stratification based on age in the Phase III studies [30,31] led to decrease in I2. The involvement of children under 9 years old, for example, in the study of Capeding et al. demonstrated lower efficacy of CYD-TDV in this group. This can be explained by the heterogeneity between the studies [30,31]. When we substratified global efficacy results by age such as 2–5 years old: 34% (RR = 0.66; 95% CI: 0.51, 0.87), 6–11 years old: 61% (RR = 0.39; 95% CI: 0.34, 0.46; I2 = 0%; p = 0.72) and ≥12 years old: 69% (RR = 0.31; 95% CI: 0.25, 0.38; I2 = 0%; p = 0.34), the heterogeneity was lower and the results continued to favor CYD-TDV for each age evaluated (Supplementary Table 2).
Age is not the only factor that can influence the heterogeneity of the efficacy findings in the various trials, seropositivity is another important aspect that needs to be considered [40,42]. As seen in Figure 6, it was possible to evaluate that the higher number of seropositivity participants contributed to better efficacy results.
Discussion
In accordance with the pooled analysis presented by Hadinegoro et al. [43], meta-analysis results with 27,355 volunteers aged 2–16 years old from two Phase III trials [28,29] showed a moderate overall vaccine efficacy of 60% (intention to treat analysis). CYD-TDV ability to stimulate an immune response was measured by comparing the geometric mean titers of neutralizing antibodies against each dengue serotype of vaccines and controls. In 1600 children and adolescents, the immunogenicity response revealed distinct profiles according to the DENV serotype, with DENV3 and DENV4 presenting best results [23–28]. The lower immunogenicity result for DENV1 was a prelude to the efficacy of 55% of CYD-TDV for this serotype. The efficacy against DENV2 was even lower (43%) [30,31]. These results coincided with the observation of the long-term safety analysis in which the majority of hospitalizations cases were due to DENV1 or DENV2 infections [43].
Data from two cluster studies conducted in Thailand suggested that higher levels of neutralizing antibodies are needed for protection against DENV2 in comparison to the other serotypes [51]. The explanation may lay in the fact that DENV2 strain can change in structure at body temperature (37°C), suggesting that antibody binding may be affected, which may be associated with lower efficacy of CYD-TDV against DENV2 [52,53]. It is known that secondary heterologous infections may increase the risk of severe disease [54]. Since CYD-TDV did not provide an adequate response, especially against DENV2, it is possible that after mass vaccination, a future DENV-2 epidemic may result in an increase of severe cases. This is the reason the WHO recommended long-term safety assessments of dengue vaccine candidates [55].
Meta-analysis of immunogenicity in adults was derived from two Phase II trials with a total of 757 volunteers. The values of the mean difference showed that the vaccine showed best response against DENV4 and DENV 3, followed by DENV2 and DENV1, but unlike the situation in children and adolescents, the 95% CI of the best response (against DENV4) and the worst response (DENV1) overlapped. In addition, Costa et al. [6] also demonstrated the best immunogenicity results for DENV3 and DENV4, however in an analysis where children, adolescent and adult result were grouped. Accordingly, the moderate efficacy obtained in children and adolescents previously predicted from immunogenicity results may also be attained in adults.
According to the Office of Vaccines Research and Review in the US FDA, immunogenicity assessment, as an auxiliary parameter for predicting efficacy, may be used for licensing purposes when a clinical efficacy study is not possible, such as when the burden of the disease is low, or when targeting a new population (age group) for which there is no comparator [56]. For the EMA, pre-authorization efficacy trials may be waived when it is justifiable to ‘to gauge the likely efficacy of a vaccine by comparison of immunological responses with those seen in past studies of protective efficacy with similar vaccines’, even when there is no correlate of protection [57]. Sanofi has filed for approval of the vaccine in 20 other countries where the DENV is most widespread and will file for approval in Europe in 2016, and in the USA in 2017 [58].
In both Phase III trials seropositivity was evaluated at the time of study enrollment, and participants with PRNT50 >10 against one or more serotypes were considered seropositive baseline [30,31], which was interpreted as evidence of previous exposure to at least one of the four DENVs [42]. When we stratified the efficacy results according to dengue seropositivity at baseline, we verified that CYD-TDV was effective in preventing dengue cases for seropositive volunteers (RR = 0.22, 95% CI: 0.14–0.35) but not for those seronegative at baseline, at least not in a conservative analysis (RR = 0.62, 95% CI: 0.37–1.03) [54].
This fact can be viewed in two opposite perspectives. On the positive side, antidengue vaccination will be adopted in dengue endemic areas with presumed high seropositivity status [55]. On the negative side, the fact that the vaccination was not effective for protection against dengue in seronegative volunteers indicates that the efficacy of CYD-TDV may be very different from country to country [30,31]. This highlights the need for seroprevalence studies capable of indicating the expected vaccine efficacy in each endemic country before any CYD-TDV pricing and funding considerations among health authorities within countries. The need for serosurveys was also stressed out by the WHO, as they are considered the best method for selecting populations suitable for vaccination [41,42].
The low efficacy in seronegative volunteers, along with the long vaccination scheme (0, 6 and 12 months), may diminish the usefulness of this vaccine for travelers. According to GeoSentinel surveillance network, dengue is considered the leading cause of febrile illness among those with a specific diagnosis returning from every geographic region except sub-Saharan Africa and Central America. It is estimated that annually more than 53 million travelers from nonendemic areas arrived in the 21 most popular dengue endemic destinations between 2006 and 2007 [59]. In Japan, there have been 1007 reports of imported dengue cases between 2006 and 2014 from Indonesia (n = 202), the Philippines (n = 230), Thailand (n = 160) and India (n = 152) [60].
In our meta-analysis, we did not find any statistical difference between CYD-TDV and control for occurrence of adverse events. SAEs were more frequently seen in the control group (RR = 0.76; 95% CI: 0.59–0.98). A safety overview of Phase I to III trials of CYD-TDV with volunteers between 2–60 years old showed that 0.3% of participants discontinued vaccination for safety reasons in the control and intervention groups, and the most common unsolicited adverse events were injection-site reactions, gastrointestinal disorders and infections [61]. According to the WHO, an increased risk of hospitalized dengue was identified in the age group of 2–5 years old in the third year of follow-up post-dose 1. This fact, along with the lower efficacy observed in under 9 years olds, led to a decision to exclude individuals aged 2–5 (and also those aged 6–8 years as a precautionary measure) from vaccination [42]. In addition, Hadinegoro et al. (2015) demonstrated that hospitalization was more frequent in participants under the age of 9 years (RR = 1.58; 95% CI: 0.83, 3.02) than for participants 9 or more years of age (RR = 0.50; 95% CI: 0.29, 0.86). Hospitalization for severe dengue occurred in 18 of 22,177 in the vaccine group and six of the 11,089 in the control group [43].
The global vaccines market was estimated at around US$32.05 billion in 2012. The market witnessed growth rates of above 8% and is expected to reach US$84.44 billion by 2022 [62,63]. Specifically for dengue vaccine, it was estimated there would be 250 million dengue vaccines doses for Brazil and Colombia for the period 2015–2019, 38 million for routine doses, 148 million for catch-up vaccination of under 15 year olds and 62 million doses for vaccination of adults. In addition, the public sector cost would be US$2.4 million over 5 years [64]. In Brazil, one state, Parana, decided to include CTD-TDV in the state immunization program. From the target population of 400,000 inhabitants (80% coverage), only 190,000 took the first dose [65,66].
The consortium created by WHO in 2015 estimated that CYD-TDV can be cost-effective in settings with intensity of transmission between 30 and 90%, if the vaccine can be purchased and delivered cheaply enough. Vaccination will only be cost effective using the public payer perspective if the total cost of fully vaccinating one person is below US$40 [41]. Dengvaxia® was granted regulatory approval first in Mexico (December 2015), followed by the Philippines and in Brazil [34–36]. Until October 2016, eight more endemic countries (El Salvador, Costa Rica, Paraguay, Guatemala, Peru, Indonesia, Thailand and Singapore) gave Dengvaxia® regulatory approval [38]. Currently, the actual acquisition price in these countries is unknown. In Brazil, CYD-TDV has not been evaluated for incorporation into the national immunization program, however the National Health Surveillance Agency (ANVISA CMED) established a reference maximum price for government purchase, yielding a total of U$96.79 [67] for the three dose scheme (World Bank for Purchase Power Parity, 2015: US$1 = 3.330 BRL).
In addition to CYD-TDV, another candidate vaccine, developed by the Butantan Institute (Brazil) in partnership with the US National Institutes of Health, is going to be evaluated in a Phase III clinical trial that has recently been registered at ClinicalTrials.gov [68].
A potential limitation of the present study is associated with the fact that the included studies were funded through pharmaceutical companies. It is known that studies of this financing type showed favorable results in response to the technologies [69,70]. However, the quality of evidence and risk of bias demonstrated that the clinical trials included were high-quality studies to address such concerns.
Conclusion
This systematic review summarized the results of high-quality studies and showed the safety of CYD-TDV. Denvaxia® showed global efficacy of 60% in volunteers under 16 years old and from the immunogenicity results in adults, we can expect satisfactory efficacy in this population after comercialization. However, there is a need to continue to evaluate the efficacy and safety of this vaccine. The numerous infections and occurrence of severe manifestations of the DENV in endemic regions reinforces the need for an effective and cost-effective vaccine to prevent this fever.
Our systematic review also emphasizes the need for pharmaceutical companies and researchers to comply with the technical rigor of the protocols for each Phase of the clinical trials to support health authorities in decisions concerning the incorporation of such technologies into their healthcare systems and, above all, to enable the provision of a safe, effective and affordable vaccine to all to prevent dengue fever in the future.
Future perspective
Dengue will continue to pose an important challenge to health systems in endemic areas since despite efforts to control the disease through vector control, the number of cases have continued to increase in recent years. This has not been helped by accelerated urbanization and low adhesion among the population to control measures, which is likely to continue. In addition, climate change (global warming) may continue to facilitate mosquitos’ reproduction. Consequently, the availability of effective dengue vaccines, building on Dengvaxia® from Sanofi Pasteur, will continue to be welcomed. In addition, vaccines made available through partnerships with research institutes such as Butantan Institute (Brazil) and the US National Institutes of Health. In the next 5 years, it is hoped that more studies and assessments of Dengvaxia®'s effectiveness, risks and benefits will be performed across all pertinent age groups. In addition, continued assessments of the effectiveness and safety of new vaccines will also be performed to aid decision making. The lack of a specific treatments and the difficulties for effectively controlling the vectors associated with dengue reinforce the need for vaccines with adequate safety and efficacy profiles as recommended by the WHO across key age groups.
| Study (year) | Design | Age range (years) | Country | Duration (months) | Groups | n | Age (SD); years | Male, n (%) |
|---|---|---|---|---|---|---|---|---|
| Daylan et al. (2013) [23]† | II | 9–16 | Brazil | 13 | CYD-TDV | 100 | 12.7 (2.1) | 40 (40) |
| Placebo | 50 | 12.7 (2.1) | 28 (55) | |||||
| Sabchareon et al. (2012) [24]§ | II B | 4–11 | Thailand | 12 | CYD-TDV | 2452 | 8.26 (2.0) | 1187 (48) |
| Placebo + rabies vaccine | 1221 | 8.23 (2.1) | 583 (48) | |||||
| Villar et al. (2013) [25]† | II | 9–16 | Colombia, Honduras, Mexico, Puerto Rico | 13 | CYD-TDV | 401 | 12.6 (NR) | 197 (49) |
| Placebo + (tetanus + diphtheria + acelular pertusis) | 199 | 12.5 (NR) | 91 (46) | |||||
| Leo et al. (2012) [26]‡ | II | 2–45 | Singapore | 18 | CYD-TDV | 438 | 17.8 (10.9) | 193 (44) |
| Placebo + hepatite A | 147 | 18.2 (11.2) | 80 (54) | |||||
| Tran et al. (2012) [27]† | II | 2–45 | Vietnam | 18 | CYD-TDV | 120 | – | 58 (48) |
| Menomune A + placebo + typhim virus | 60 | – | 35 (58) | |||||
| Lanata et al. (2012) [28]† | II | 2–11 | Peru | 12 | CYD-TDV (2–5 years) | 100 | 3.9 (1.1) | 55 (55) |
| Placebo + pneumococcal polysaccharide (2–5 years) | 50 | 3.9 (1.2) | 25 (50) | |||||
| CYD-TDV (6–11 years) | 99 | 8.8 (1.9) | 46 (46) | |||||
| Placebo + Pneumococcal polysaccharide (6–11 years) | 49 | 8.8 (1.8) | 21 (43) | |||||
| Amar-Singh et al. (2013) [29]¶ | III | 2–11 | Malaysia | 18 | CYD-TDV | 199 | 6.4 (2.8) | 96 (48) |
| Placebo | 51 | 6.5 (3.0) | 32 (63) | |||||
| Capeding et al. (2014) [31]§ | III | 2–14 | Indonesia, Malaysia, Philippines, Thailand, Vietnam | 25 | CYD-TDV | 6710 | 8.8 (3.4) | 3253 (48) |
| Placebo | 3350 | 8.8 (3.4) | 1623 (48) | |||||
| Villar et al. (2015) [31]§ | III | 9–16 | Brazil, Colombia, Mexico, Honduras, Puerto Rico | 25 | CYD-TDV | 12,574 | 12.4 (2.1) | 6254 (50) |
| Placebo | 6261 | 12.4 (2.1) | 3105 (50) |
†Population described: Participants that vaccinated with at least the first dose.
‡Population described: Immunogenicity analysis set.
§Population described: Per-protocol analysis for efficacy.
¶Population described: Safety analysis set.
| Outcome/group | Vaccine (cases/total participants), n | Control (cases/total participants), n | Risk ratio (CI 95%) | Heterogeneity (I2; p-value) | Ref.† |
|---|---|---|---|---|---|
| Pain | |||||
| CYD-TDV | 390/1880 | 248/739 | 0.71 (0.45–1.12) | 91%; <0.00001 | [23,25–29] |
| Erythema | |||||
| CYD-TDV | 189/1880 | 107/739 | 0.55 (0.34–0.89) | 70%; 0.005 | [23,25–29] |
| Swelling | |||||
| CYD-TDV | 67/1880 | 73/739 | 0.33 (0.17–0.64) | 67%; 0.009 | [23,25–29] |
| Fever | |||||
| CYD-TDV | 225/1679 | 78/688 | 1.20 (0.78–1.83) | 65%; 0.02 | [23,25–28] |
| Malaise | |||||
| CYD-TDV | 700/1906 | 216/739 | 1.19 (0.98–1.45) | 44%; 0.11 | [23,25–29] |
| Headache | |||||
| CYD-TDV | 764/1880 | 261/739 | 1.12 (0.88–1.42) | 72%; 0.003 | [23,25–29] |
| Myalgia | |||||
| CYD-TDV | 561/1681 | 238/688 | 0.85 (0.63–1.16) | 73%; 0.005 | [23,25–28] |
| Asthenia | |||||
| CYD-TDV | 300/1561 | 103/628 | 1.03 (0.72–1.47) | 57%; 0.07 | [23,25–28] |
| Serious adverse event | |||||
| CYD-TDV | 595/25,309 | 325/11,114 | 0.76 (0.59–0.98) | 28%; 0.20 | [23–31] |
†See Table 1 for study names.
Dengue virus is a serious global health problem with an estimated 3.97 billion people at risk for infection worldwide. Sanofi Pasteur's dengue vaccine (CYD-TDV) has already been granted regulatory approval in a number of countries for the prevention of dengue fever, and the numbers will grow.
This systematic review summarized the results of high-quality studies in terms of the efficacy and safety of CYD-TDV.
The Global Efficacy of CYD-TDV (Dengvaxia®) – 60% intention to treat (RR = 0.40; 95% CI: 0.31–0.51; I2 = 79%; p = 0.03) and 59% per protocol (RR = 0.41; 95% CI: 0.35– 0.48; I2 = 0%; p = 0.52).
Efficacy by serotype (intention to treat) – DENV1 (RR = 0.45; 95% CI: 0.38–0.55; I2 = 0%; p = 0.97), DENV2 (RR = 0.57; 95% CI: 0.44–0.74; I2 = 36%; p = 0.21), DENV3 (RR = 0.29; 95% CI: 0.22–0.38; I2 = 6%; p = 0.30) and DENV4 (RR = 0.23; 95% CI: 0.16–0.33; I2 = 39%; p = 0.20).
Global efficacy/seropositivity: seronegative: 38% (RR = 0.62; 95% CI: 0.37–1.03; I2 = 0%; p = 0.82) and seropositivity: 78% (RR = 0.22; 95% CI: 0.14–0.35; I2 = 0%; p = 0.36).
Safety – local events: erythema (RR = 0.55; 95% CI: 0.34–0.89; I2 = 70%; p = 0.005) and swelling (RR = 0.33; 95% CI: 0.17–0.64; I2 = 67%; p = 0.009); systemic events – no statistical difference between the control and the intervention groups.
The efficacy and safety of dengue vaccines need to continue to be evaluated after commercialization.
The numerous infections and occurrence of severe manifestations of the dengue virus in endemic regions reinforce the need for effective, safe and cost-effective vaccines across age groups to prevent this fever.
Financial & competing interests disclosure
IP Godói received financial support from CAPES (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
The write-up was in part supported by a Newton Advanced Fellowship awarded to Professor Augusto Afonso Guerra Junior by the Academy of Medical Sciences, through the UK Government's Newton Fund programme.
Supplementary Material
File (suppl_materials.doc)
- Download
- 86.00 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Bhatt S, Gething PW, Brady OJ et al. The global distribution and burden of dengue. Nature 25, 504–507 (2013).
2.
Brady OJ, Gething PW, Bhatt S et al. Refining the global spatial limits of dengue virus transmission by evidence-based consensus. PLoS Negl. Trop. Dis. 6, e1760 (2012).
3.
Thoisy B, Lacoste V, Germain A et al. Dengue infection in neotropical forest mammals. Vector Borne Zoonotic Dis. 9, 157–169 (2009).
4.
Simmons CP, Farrar JJ, Chau NV, Wills B. Current concepts dengue. N. Engl. J. Med. 366, 1423–1432 (2012).
5.
Godoi IP, Taranto MFR, Lima WG et al. NS2B-NS3pro as a molecular target drugs development against dengue. Biochem. Biotech. Rep. 2, 16–30 (2004).
6.
Costa VG, Marques-Silva AG, Floriano VG, Moreli ML. Safety, immunogenicity and efficacy of a recombinant tetravalent dengue vaccine: a meta-analysis of randomized trials. Vaccine 32, 4885–4892 (2014).
7.
Tomlinson SM, Malmstrom RD, Watowich SJ. New approaches to structure-based discovery of dengue protease inhibitors. Infect. Disord. Drug Targets 9, 1–17 (2009).
8.
Forshey BM, Stoddard ST, Halsey ES. Direct feeding on dengue patients yields new insights into human to mosquito dengue virus transmission. Future Virol. 8, 1145–1149 (2013).
9.
Yacoub S, Mongkolsapaya J, Screaton G. Recent advances in understanding dengue. F1000Research 78, 1–10 (2016).
10.
Reiter P. Aedes albopictus and the world trade in used tires, 1988–1995: the shape of things to come? J. Am. Mosq. Control Assoc. 14, 83–94 (1998).
11.
Shepard DS, Undurraga EA, Halasa YA, Stanaway JD. The global economic burden of dengue: a systematic analysis. Lancet Infect. Dis. 16, 935–941 (2016).
12.
Constenia D, Garcia C, Lefcourt N. Assessing the economics of dengue: results from a systematic review of the literature and expert survey. Pharmacoeconomics 33, 1107–1135 (2015).
13.
Webster DP, Farrar J, Rowland-Jones S. Progress towards a dengue vaccine. Lancet Infect. Dis. 9, 678–687 (2009).
14.
Durbin AP, Whitehead SS. Next-generation dengue vaccines: novel strategies currently under development. Viruses 3, 800–814 (2011).
15.
Coulange BH, Benabdelmoumen G, Gergely A et al. Long term persistence of yellow fever neutralising antibodies in elderly persons. Bull. Soc. Pathol. Exot. 104, 260–265 (2011).
16.
Kumar R, Tripathi P, Rizvi A. Effectiveness of one dose of SA 14–14-2 vaccine against Japanese encephalitis. N. Engl. J. Med. 360, 1465–1466 (2009).
17.
Del Angel RM, Reyes-del VJ. Dengue vaccines: strongly sought but not a reality just yet. PLoS Pathog. 9, e1003551 (2013).
18.
Torresi J, Tapia-Conyer R, Margolis H. Preparing for dengue vaccine introduction: recommendations from the 1st dengue v2V international meeting. PLoS Negl. Trop. Dis. 7, e2261 (2013).
19.
Züst R, Dong H, Li XF et al. Rational design of a live attenuated dengue vaccine: 2-o-methyltransferase mutants are highly attenuated and immunogenic in mice and macaques. PLoS Pathog. 9, e1003521 (2013).
20.
Huang CY, Kinney RM, Livengood JA et al. Genetic and phenotypic characterization of manufacturing seeds for a tetravalent dengue vaccine (DENVax). PLoS Negl. Trop. Dis. 7, e2243 (2013).
21.
Zhao H, Jiang T, Zhou XZ et al. Induction of neutralizing antibodies against four serotypes of dengue virusesby MixBiEDIII, a tetravalent dengue vaccine. PLoS ONE 9, e86573 (2014).
22.
Dayan GH, Thakur M, Boaz M, Johnson C. Safety and immunogenicity of three tetravalent dengue vaccine formulations in healthy adults in the USA. Vaccine 31, 5047–5054 (2013).
23.
Dayan GH, Garbes P, Noriega F et al. Immunogenicity and safety of a recombinant tetravalent dengue vaccinein children and adolescents ages 9–16 years in Brazil. Am. J. Trop. Med. Hyg. 89, 1058–1065 (2013).
24.
Sabchareon A, Wallace D, Sirivichayakul C et al. Protective efficacy of the recombinant, live-attenuated, CYD tetravalent dengue vaccine in Thai schoolchildren: a randomized, con-trolled Phase IIb trial. Lancet 380, 1559–1567 (2012).
25.
Villar LA, Rivera-Medina DM, Arredondo-García JL et al. Safety and immunogenicity of a recombinant tetravalentdengue vaccine in 9–16 year olds. A randomized, controlled, Phase II trial in Latin America. Pediatr. Infect. Dis. J. 32, 1102–1109 (2013).
26.
Leo YS, Wilder-Smith A, Archuleta S et al. Immunogenicity and safety of recombinant tetravalent dengue vaccine (CYD-TDV) in individuals aged 2–45 years-Phase II randomized controlled trial in Singapore. Hum. Vaccines Immunother. 8, 1259–1271 (2012).
27.
Tran NH, Luong CQ, Vu TQH et al. Safety and immuno-genicity of recombinant, live attenuated tetravalent dengue vaccine (CYD-TDV) in healthy Vietnamese adults and children. J. Vaccines Vaccin. 3, 1–7 (2012).
28.
Lanata CF, Andrade T, Gil AI et al. Immunogenicity and safety of tetravalent dengue vaccine in 2–11 year-oldspreviously vaccinated against yellow fever: randomized, controlled, Phase II study in Piura, Peru. Vaccine 30, 5935–5941 (2012).
29.
Amar-Singh HSS, Koh MT, Tan KK et al. Safety and immunogenicity of a tetravalent dengue vaccine in healthy children aged 2–11 years in Malaysia: a randomized, placebo-controlled Phase III study. Vaccine 31, 5814–5821 (2013).
30.
Capeding MR, Tran NH, Hadinegoro SRS et al. Clinical efficacy and safety of a novel tetravalent dengue in healthy children in Asia: a Phase 3, randomized, observer-masked, placebo-controlled trial. Lancet 384, 1358–1365 (2014).
•• Phase III trials (efficacy) of a dengue vaccine candidate which is included in our meta-analysis.
31.
Villar L, Dayan GH, Arredondo-García JL et al. Efficacy of a tetravalent dengue vaccine in children in Latin America. N. Engl. J. Med. 372, 113–123 (2015).
•• Phase III trials (efficacy) of a dengue vaccine candidate which is included in our meta-analysis.
32.
Guy B, Saville M, Lang J et al. Development of Sanofi Pasteur tetravalent dengue vaccine. Rev. Pan-Amaz. Saude. 2, 51–64 (2011).
33.
Coller GBA, Clements DE. Dengue vaccines: progress and challenges. Curr. Opin. Immunol. 23, 391–398 (2011).
34.
Sanofi Pasteur. Dengvaxia®, world's first dengue vaccine, approved in Mexico (2015). www.sanofipasteur.com/en/articles/dengvaxia-world-s-first-dengue-vaccine-approved-in-mexico.aspx.
35.
Sanofi Pasteur. Sanofi Pasteur's dengue vaccine approved in the Philippines (2015). www.sanofipasteur.com/en/articles/sanofi-pasteur-dengue-vaccine-approved-in-the-philippines.aspx.
36.
Sanofi Pasteur. Dengvaxia® first dengue vaccine approved in Brazil (2015). www.sanofipasteur.com/en/articles/Dengvaxia-First-Dengue-Vaccine-Approved-in-Brazil.aspx.
37.
Sanofi Pasteur. Sanofi Pasteur dengue vaccine approved in Costa Rica (2016). www.sanofipasteur.ca/node/49001.
38.
Sanofi Pasteur. First dengue vaccine approved in more than 10 countries (2016). www.sanofipasteur.com/en/Documents/PDF/PR/20161004_First_Dengue_Vaccine_Approved_in_More_than_10_Countries_EN.pdf.
39.
Dengue Vaccine Initiative. Dengue vaccine initiative statement on SAGE dengue vaccine recommendations (2016). www.denguevaccines.org/sites/default/files/DVI%20Statement%20-%20SAGE%20Recommendations%20Dengue%20Vaccines%20April%202016_0.pdf.
40.
European Medicines Agency. Committee for Human Medicinal Products – Guideline on immunogenicity assessment of biotechnology-derived Therapeutic proteins (2007). www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2009/09/WC500003946.pdf.
41.
WHO. Background paper on dengue vaccines (2016). www.who.int/immunization/sage/meetings/2016/april/1_Background_Paper_Dengue_Vaccines_2016_03_17.pdf.
•• WHO publication that is important to dengue vaccine context.
42.
WHO. Dengue Vaccine: WHO position paper – July 2016. Wkly Epidemiol. Rec., 30, 91, 349–364 (2016). www.who.int/wer/2016/wer9130.pdf?ua=1.
•• WHO publication that is important to dengue vaccine context.
43.
Hadinegoro SR, Arredondo-Garcia JL, Capeding MR et al. Efficacy and long-term safety of dengue vaccine in regions of endemic disease. N. Engl. J. Med. 13, 1195–1206 (2015).
•• Important to complement our knowledge of the disease and of CYD-TDV.
44.
Flashe S, Jit M, Rodrigues-Barraquer et al. Comparative modelling of dengue vaccine public health impact (CMDVI) (2016). www.who.int/immunization/sage/meetings/2016/april/2_CMDVI_Report_FINAL.pdf.
45.
Ferguson NM, Rodríguez-Barraquer I, Dorigatti I. Benefits and risks of the Sanofi-Pasteur dengue vaccine: modeling optimal deployment. Science 353(6303), 1033–1036 (2016).
46.
Higgins JPT, Green S (Eds). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration (2011). www.cochrane-handbook.org.
• Important reference source for conducting meta-analyses.
47.
Liberati A, Altman DG, Tetzlaff J et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 7, 1–97 (2009).
• Important reference source for conducting meta-analyses.
48.
Mansfield KL, Horton DL, Johnson N et al. Flavivirus-induced antibody cross-reactivity. J. Gen. Virol. 92, 2821–2829 (2011).
49.
Deeks JJ, Higgins J, Altman DG. Chapter 9: Analysing data and undertaking meta-analyses. In: Higgins JPT, Green S (Eds). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration (2011). www.cochrane-handbook.org.
50.
Higgins JPT, Altman AD, Sterne JAC. Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S (Eds). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration (2011). www.cochrane-handbook.org.
51.
Buddhari D, Aldstadt J, Endy TP et al. Dengue virus neutralizing antibody levels associated with protection from infection in Thai cluster studies Darunee Buddhari. PLoS Negl. Trop. Dis. 8, e3230 (2014).
52.
Guntur F, Thiam-Seng Ng, Victor AK et al. Structural changes in dengue virus when exposed to a temperature of 37°C. J. Virol. 13, 7585–7592 (2013).
53.
Guntur F, Kristie DI, Thiam-Seng Ng et al. Cryo-EM structure of an antibody that neutralizes dengue virus type 2 by locking E protein dimers. Science 6243, 88–90 (2015).
54.
Guy B, Jackson N. Dengue vaccine: hypotheses to understand CYD-TDV induced protection. J. Vector Borne Dis. 14, 45–54 (2016).
55.
WHO. Guidelines for the clinical evaluation of dengue vaccines in endemic areas – immunization, vaccines and biologicals (2008). http://whqlibdoc.who.int/hq/2008/WHO_IVB_08.12_eng.pdf.
•• WHO publications that are important to dengue vaccine context.
56.
US FDA. Office of Vaccines Research and Review Center for Biologics Evaluation and Research. Use of Immunogenicity Data to Assess Vaccine Effectiveness (2013). www.google.com.br/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&cad=rja&uact=8&ved=0ahUKEwjJ8eemiZTQAhXFDpAKHeO_AjsQFggiMAA&url=http%3A%2F%2Fwww.fda.gov%2Fdownloads%2FBiologicsBloodVaccines%2FNewsEvents%2FWorkshopsMeetingsConferences%2FUCM338945.ppt&usg=AFQjCNH191BGAMd4lpfWf9lwo3TS7Vn2qw.
57.
European Medicines Agency. Committee for Human Medicinal Products - Note for Guidance on the Clinical Evaluation of Vaccines (2005). www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2009/09/WC500003875.pdf.
58.
Roland D, Bisserbe N. Mexico approves Sanofi's dengue vaccine but pricing questions remain. The Wall Street Journal. (2015). www.wsj.com/articles/mexico-approves-sanofis-dengue-vaccine-but-pricing-questions-remain-1449676613.
59.
Leder K, Torresi J, Libman MD. GeoSentinel surveillance of illness in returned travelers, 2007– 2011. Ann. Intern. Med. 19, 456–468 (2013).
60.
Fukusumi M, Arashiro T, Arima Y et al. Dengue Sentinel traveler surveillance: monthly and yearly notification trends among Japanese travelers, 2006–2014. PLoS Negl. Trop. Dis. 10, 1–14 (2016).
61.
Gailhardou S, Skipetrova A, Dayan GH. Safety overview of a recombinant live-attenuated tetravalent dengue vaccine: pooled analysis of data from 18 clinical trials. PLoS Negl. Trop. Dis. 10, 1–25 (2015).
62.
Vaccine market by technology & types, various classes & indications – global forecasts to 2022. Research and Markets (2013). www.researchandmarkets.com/research/x5nr7d/vaccine_market_by.
63.
Jadhav S, Gautam M, Gairola S. Role of vaccine manufacturers in developing countries towards global healthcare by providing quality vaccines at affordable prices. Clin. Microbiol. Infect. 20, 37–44 (2014).
64.
Dengue Vaccine Initiative. Planning for the introduction of dengue vaccines (2011). www.denguevaccines.org/sites/default/files/ADPB-Brazil_11-Short.pdf.
65.
Secretaria de Saúde do Paraná. Manual de Normas e Procedimentos para vacinação – Dengue (2016). www.saude.pr.gov.br/arquivos/File/VacinaDENGUE_protocolo.pdf.
66.
O DIARIO. Maringa vacinou 190 mil contra Dengue. http://maringa.odiario.com/parana/2016/09/parana-vacinou-190-mil-contra-a-dengue/2247982/.
67.
Brasil. Câmara de Regulação de Preços (CMED) (2016). http://portal.anvisa.gov.br/documents/374947/2829072/LISTA_CONFORMIDADE_GOV_2016–10–20.pdf/20b61fe1-f8a9–41ae-a55d-cb8613953dd8.
68.
BRASIL. Anvisa autoriza Instituto Butantan a iniciar Ensaio Clínico fase 3 da vacina contra dengue (2015). http://portal.anvisa.gov.br/wps/content/anvisa+portal/anvisa/sala+de+imprensa/menu+-+noticias+anos/2015/anvisa+autoriza+instituto+butantan+a+iniciar+ensaio+clinico+fase+3+da+vacina+contra+dengue.
•• Indicates that the vaccine developed by the Butantan Institute (Brazil) gained approval for a Phase III trial, which will probably lead to licensing of the vaccine in Brazil in the coming years.
69.
Bero L, Oostvogel F, Bachetti P, Lee K. Factors associated with findings of published trials of drug–drugs comparisons: why some stations appear more efficacious than others. PLoS Med. 4(6), e184 (2007).
70.
Lexchini J, Bero LA, Djulbegovic B, Clark O. Pharmaceutical industry sponsorship and research outcome and quality: systematic review. BMJ 1167(326), 1167–1170 (2003).
Information & Authors
Information
Published In
Copyright
© Future Medicine Ltd.
History
Published online: 13 January 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
CYD-TDV dengue vaccine: systematic review and meta-analysis of efficacy, immunogenicity and safety. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0045
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Viviana Maria Gianguzzo, Michelangelo Rottura, Federica Maria Sacco, Matthew Gavino Donadu, Giuseppina Sanna, Natasha Irrera, Egidio Imbalzano, Vincenzo Arcoraci, Giuseppinella Melita, Ylenia Marino, Sara Manti, Giovanni Pallio, Post-marketing safety profile of dengue vaccines CYD-TDV and TAK-003: analysis of adverse event reports from a European database, Frontiers in Pharmacology, 10.3389/fphar.2026.1789762, 17, (2026).
- Guowei Sun, Ali Mai, Yunfeng Liu, Mosquito control models based on Wolbachia or sterile insect techniques, Discrete and Continuous Dynamical Systems - B, 10.3934/dcdsb.2025160, 33, 0, (464-489), (2026).
- Qian Ding, Jianshe Yu, Zhiming Guo, Yuming Chen, Yunfeng Liu, Periodic dynamics of a general switching dynamical system, European Journal of Applied Mathematics, 10.1017/S0956792525100065, 37, 4, (882-896), (2025).
- Antonio Ferreira Mendes-Sousa, Veruska Cavalcanti Barros, Andressa Barros Ibiapina, Maria Clara Moura Silva, Vagner José Mendonça, Bruno Guedes Alcoforado Aguiar, Elisabeth Biruel, Carmen Verônica Mendes Abdala, Lilian Silva Catenacci, Evidence map of strategies for preventing and controlling Aedes aegypti infestation and related viral infections, Revista Panamericana de Salud Pública, 10.26633/RPSP.2025.63, 49, (1), (2025).
- Jarvis Z. H. Goh, Lachlan De Hayr, Alexander A. Khromykh, Andrii Slonchak, The Flavivirus Non-Structural Protein 5 (NS5): Structure, Functions, and Targeting for Development of Vaccines and Therapeutics, Vaccines, 10.3390/vaccines12080865, 12, 8, (865), (2024).
- Anastasia Latanova, Vadim Karpov, Elizaveta Starodubova, Extracellular Vesicles in Flaviviridae Pathogenesis: Their Roles in Viral Transmission, Immune Evasion, and Inflammation, International Journal of Molecular Sciences, 10.3390/ijms25042144, 25, 4, (2144), (2024).
- Daniel Msellemu, Marcel Tanner, Rajpal Yadav, Sarah J. Moore, Occupational exposure to malaria, leishmaniasis and arbovirus vectors in endemic regions: A systematic review, Current Research in Parasitology & Vector-Borne Diseases, 10.1016/j.crpvbd.2024.100185, 6, (100185), (2024).
- Eveline Bezerra De Souza, Priscila Da Silva Castro, Isabella Piassi Dias-Godói, Maíra Catherine Pereira Turiel Silva, Leticia Dias Lima Jedlicka, TRANSDISCIPLINARIDADE COMO ESTRATÉGIA DE ENSINO E EXTENSÃO EM EDUCAÇÃO EM SAÚDE, Revista Chão da Escola, 10.55823/rce.v19i19.142, 19, (69-81), (2022).
- Camila Lorenz, Francisco Chiaravalloti-Neto, Control methods for Aedes aegypti: Have we lost the battle?, Travel Medicine and Infectious Disease, 10.1016/j.tmaid.2022.102428, 49, (102428), (2022).
- Dawid Pieper, Irma Hellbrecht, Linlu Zhao, Clemens Baur, Georgia Pick, Sarah Schneider, Thomas Harder, Kelsey Young, Andrea C. Tricco, Ella Westhaver, Matthew Tunis, Impact of industry sponsorship on the quality of systematic reviews of vaccines: a cross-sectional analysis of studies published from 2016 to 2019, Systematic Reviews, 10.1186/s13643-022-02051-x, 11, 1, (2022).