Young adult and parent stakeholder perspectives on participation in patient-centered comparative effectiveness research
Abstract
Aim: Explore perspectives of adolescent and young adult (AYA) and parent stakeholders regarding their engagement in comparative effectiveness research (CER) evaluating cholesterol screening and treatment strategies for 17–21 year olds. Methods: All nine AYAs and parent stakeholders participating in a 20-member panel of AYAs, parents and professionals (i.e., clinicians, researchers, policy makers, payers), completed a quantitative survey and a semistructured interview at the completion of the core CER study. Results & Conclusion: AYAs and parents stakeholders emphasized the role of power differentials regarding shared knowledge, relationships and trust, and logistics. To mitigate power differentials, stakeholders recommended more materials, clearer definition of roles and in-person meetings. Perceived positive outcomes included diversity of perspectives provided, better understanding their own health and decision-making and improving CER.
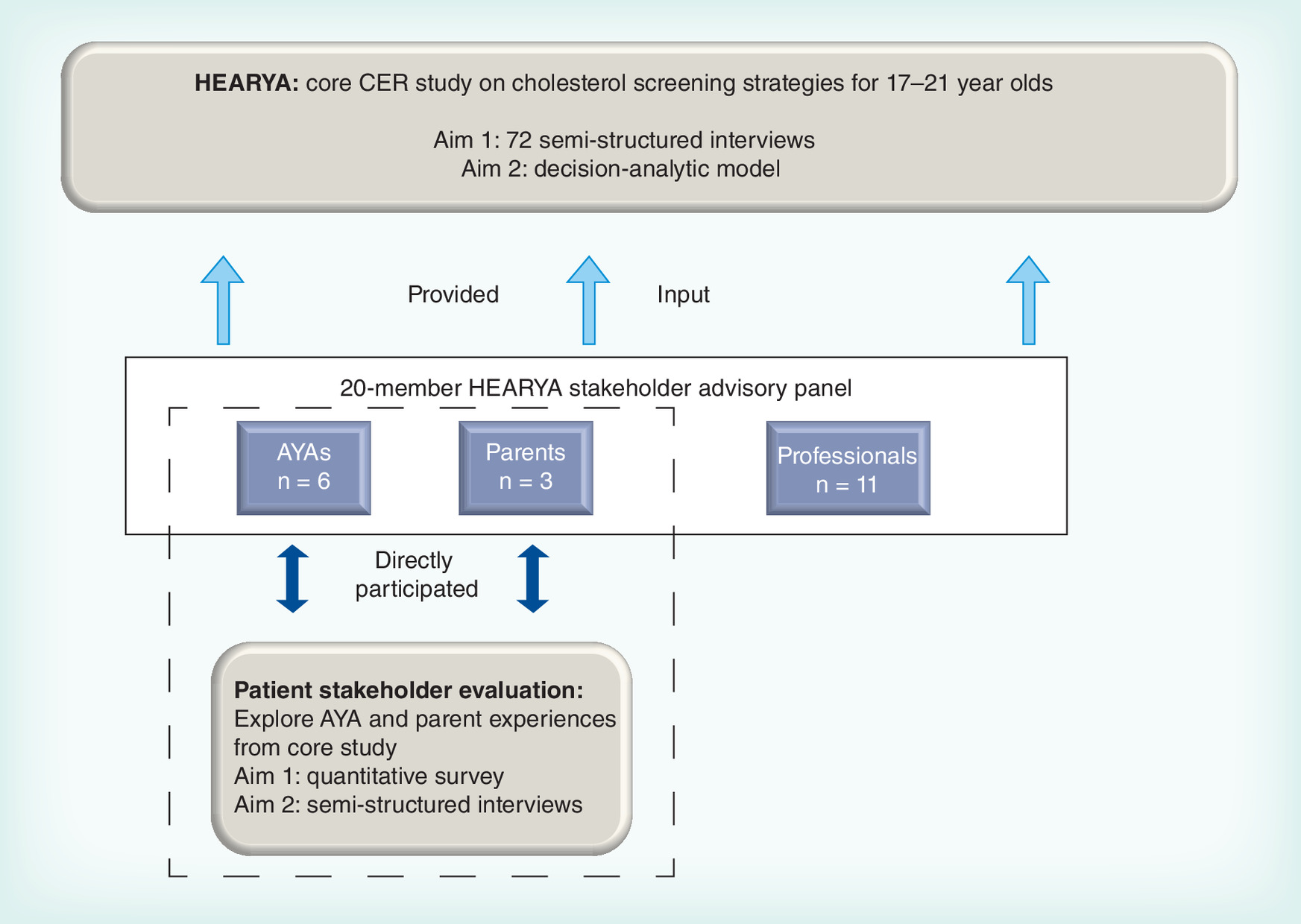
Figure 1. Adolescent and young adult and parent stakeholders directly participated in the Patient Stakeholder Evaluation while all 20 members of the Stakeholder Panel provided input to the core HEARYA study.
AYA: Adolescent and young adult; CER: Comparative effectiveness research.
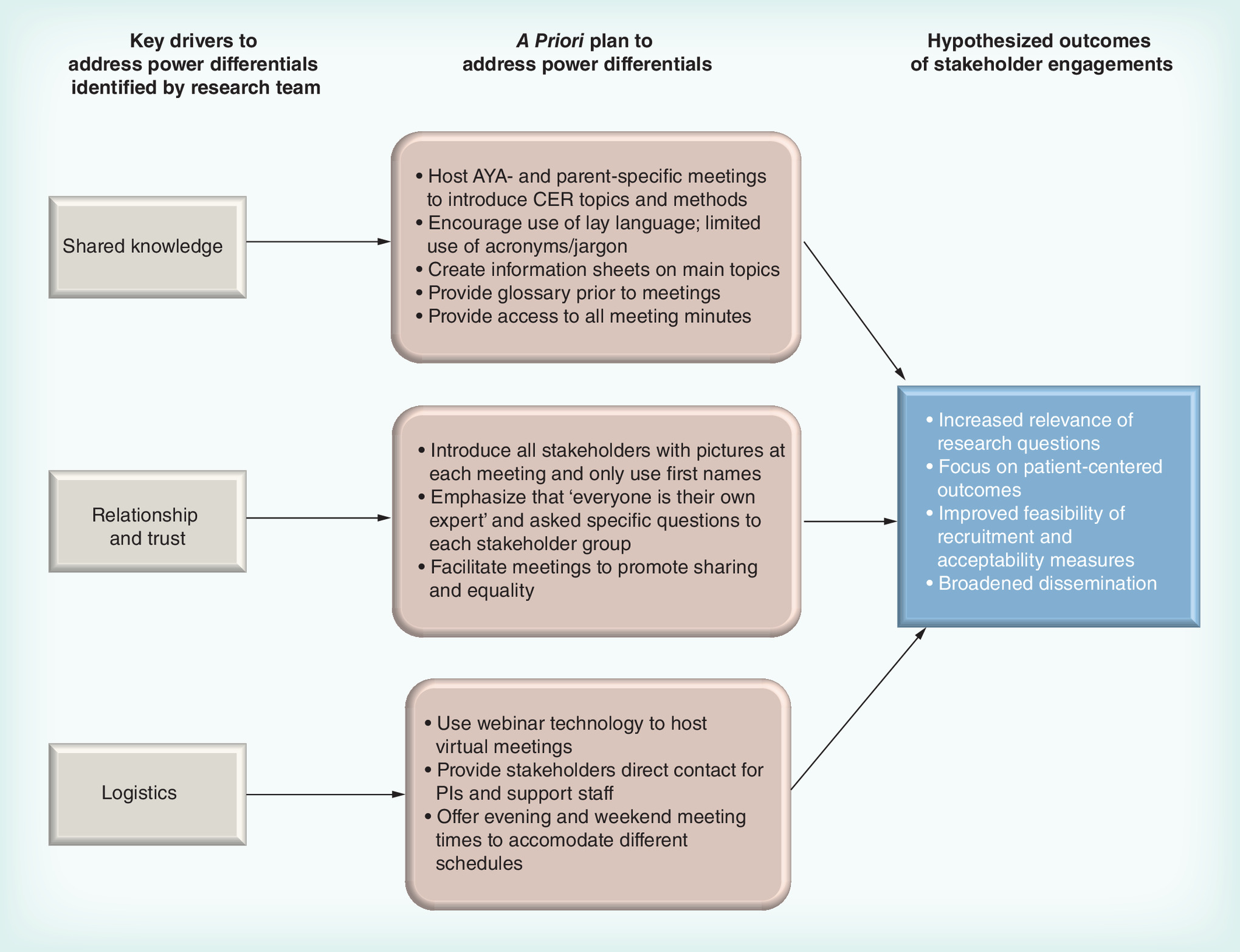
Figure 2. Framework to address power differentials among stakeholders.
AYA: Adolescent and young adult; CER: Comparative effectiveness research; PI: Principal Investigator.
First draft submitted: 18 April 2016; Accepted for publication: 3 June 2016; Published online: 18 July 2016
Stakeholder engagement (SE) in patient-centered comparative effectiveness research (CER) is endorsed by the Agency for Healthcare Research and Quality (AHRQ), the Patient-Centered Outcomes Research Institute (PCORI), and the Institute of Medicine [1–3]. Recent perspectives on SE in CER call for the inclusion of a variety of stakeholder groups, ranging from patients to clinicians, employers, insurers, manufacturers and policymakers, who serve in an advisory or investigator capacity in CER [4–6]. Compelling arguments have been made for the specific inclusion of patient voices to improve the relevance of research questions, identify patient-centered outcomes, enhance the feasibility of recruitment and completion of study protocols, and facilitate the dissemination and adoption of findings [7,8].
While the inclusion of patients in CER holds strong conceptual appeal, there is a limited literature on the firsthand experiences of patients as stakeholders and examples of how to facilitate meaningful patient engagement, particularly when patients are one of a number of stakeholder groups participating in CER. Attention to power differentials is particularly critical when patients serve as stakeholder participants in conjunction with individuals who may be viewed to hold higher authoritative positions in society due to their professional roles (e.g., clinicians, administrators, researchers, policymakers) and who bring a different knowledge base to an identified clinical area in a CER study compared with patients’ experiential knowledge.
These power differentials are even more charged for adolescents and young adults (AYAs) who face the added challenge of navigating AYA–adult relationships with representatives from other stakeholder groups, within the context of serving as a patient voice in the research process. Adolescence and young adulthood is characterized by multiple developmental transitions to independence. Life-stage transitions often include high school to college or workforce, dependent to independent living and frequent relocation [9]. The primary decision-maker for many life choices shifts from other authority figures (e.g., teachers, coaches) to more autonomous decision-making. Clinically, the ages of 17–21 years are a time of transitioning from pediatric- to adult-based care and from parent-driven visits to autonomous healthcare patterns. Parents may or may not continue to exert a substantial role in an AYA's healthcare, particularly with the extension of health insurance coverage to dependents through the age of 26 years [10].
In this paper, we report the results of an evaluation exploring AYA and parent perspectives on the patient engagement processes over the course of a 2 years, PCORI-funded core study examining the comparative effectiveness of cholesterol screening and treatment strategies for 17–21 year olds. The core study, titled HEARYA, employed two inter-related research aims: semistructured interviews with 72 AYAs and parents of AYAs to characterize decision-making regarding cholesterol screening and treatment at the individual patient level, and creation of a decision-analytic model to quantify the trade-offs of different cholesterol screening and treatment strategies at the population level. To inform these research activities, a stakeholder panel including AYAs, parents of AYAs and professionals (i.e., clinicians, researchers, policy makers and payers) was convened to enhance feasibility and relevance by advising on select methodological questions, outcomes and decision-analytic model inputs and improve the dissemination of findings.
The purpose of our stakeholder evaluation was to explore the experiences of AYAs and parent panel members regarding their roles as patient stakeholders in the core study, challenges they encountered and recommendations for patient engagement, with the goal of illuminating best practices in engaging AYAs and parents as patient stakeholders for future CER (see Figure 1). To address power differentials and engage AYA and parent stakeholders in our core study, we drew on community-based participatory research (CBPR) frameworks for addressing issues of knowledge and power differentials in conducting research that engages community members [11,12].
Methods
Description of the HEARYA stakeholder advisory panel
Stakeholder recruitment
To recruit stakeholders for the core HEARYA study, we employed AHRQ's definition of stakeholders: “persons or groups that have a vested interest in the clinical decision and the evidence that supports that decision” [13]. A 20-person stakeholder panel was convened to inform the research methods, inputs, analysis and dissemination for the overall study.
The panel comprised six AYAs, three parents and eleven clinician, researcher, policymaker, payer (hereafter ‘professional’) stakeholders. Stakeholders were recruited through affiliation with two academic medical centers in Boston, MA and the professional and personal networks of research team members. The AYAs and parents were purposely selected to represent one of three clinical groups of interest in the HEARYA study: patients diagnosed with familial hypercholesterolemia (FH), patients with cardiovascular risk due to another chronic illness (e.g., obesity) and patients with no known cardiovascular risks (e.g., general population). We deliberately sought out socioeconomic and racial/ethnic diversity where possible across the patient members of the panel.
Stakeholder approach
Prior to engaging the stakeholder panels members, we articulated an approach based on the CBPR literature to inform our SE activities and address possible power differentials; specifically, we identified three mechanisms in the CBPR literature: build shared knowledge through research training, recognize and address power differentials by prioritizing relationships and trust and address logistics of stakeholder engagement through careful consideration of stakeholder meetings, communication and access [14,15]. A priori we identified these challenges and developed a framework with specific strategies to mitigate power differentials prior to the core study's inception (see Figure 2).
Stakeholder meetings
The geographical spread of stakeholders across the country and finite resources available through PCORI funds led us to host only virtual meetings, drawing on published resources on best practices in virtual teams [16,17]. We hosted three separate, 90 min capacity building sessions at the study outset for the AYAs and parents, and one 90-min session for the professional group that addressed both the content of the study and mechanisms for addressing power differentials. Subsequent meetings included all panel members based on recommendations arising from early PCORI studies [7]. Each of the 18 regularly scheduled stakeholder meetings were held as webinars consisting of a conference call; shared materials (e.g., information sheets, articles, slides) were provided prior to the meeting. Meetings were predominantly facilitated by core-study Principal Investigators (SD de Ferranti, LK Leslie).
Patient stakeholder evaluation
Sample
All AYA (n = 6) and parent (n = 3) stakeholders were invited to complete a brief quantitative survey and follow-up semistructured phone interviews in months 22–23 of the core study; 100% (n = 9) participated.
Instruments
For this evaluation, we employed both a quantitative survey and semistructured interviews sequentially. The survey aimed to facilitate quantification of core goals for the SE process while the qualitative interviews facilitated an in-depth understanding of their experiences, preferences and values. The survey assessed stakeholder comfort level with the SE process, perceived contribution and impact to the core study using five-point Likert scales (strongly agree to strongly disagree). Semistructured interviews with stakeholders were subsequently conducted over the phone by a member of the research team, audio recorded, professionally transcribed and routinely assessed for quality assurance. The research team member who conducted all nine interviews (T Saunders) had interaction with the stakeholders primarily around scheduling meetings over the course of the core study. As part of the consent process, stakeholders were reminded that their responses would be de-identified and aggregated at the stakeholder group level (i.e., AYA, parent). The interview was designed to reflect PCORI engagement principles as articulated in the published rubric [18], but also to elicit emergent themes regarding SE in CER [19]. Domains of the interview guide included: overall experience, process of engagement, research topics and methods, logistics of engagement and impact and outcomes.
Analysis
The frequency of responses was calculated from the quantitative survey results. A codebook for all qualitative data were iteratively developed through rigorous group discussion and included both a priori themes based on PCORI principles and emergent themes from the interviews. Transcripts were analyzed using a ‘coding consensus, co-occurrence and comparison’ approach, in which codebook domains are derived from the data and then illustrated by characteristic examples [20]. Two research team members who had not actively participated in the stakeholder meetings (T Saunders, S Shah) independently coded each interview and resolved any discrepancies by consensus as our goal was agreement rather than measures of inter-rater reliability [21]. Oversight was provided by a trained qualitative researcher (T Mackie). To reflect the heterogeneity of patient experiences, themes were included based on responses provided by any patient. To capture the breadth of experience and preferences among the panel, we report on all coded data without setting criteria for the number of times a particular theme was mentioned [22]. Once coded in hard copy and reconciled, researchers coded and subsequently collated and compared thematic areas in DeDoose©, a mixed methods software program. All AYA and parent stakeholders were provided the opportunity to review this manuscript. The patient stakeholder perspectives study was approved by the Tufts Health Sciences Institutional Review Board.
Results
Stakeholder demographics
Occupations of AYA and parent stakeholders at study inception included high school, college or graduate student or working full time. Three AYAs had prior research experience, including two who had served on a research advisory panel for the Division of Adolescent Medicine at Boston Children's Hospital [23]. All parents had prior research experience, one as a research subject, one through professional activities and one had been a member of an established stakeholder panel (see Table 1). Each AYA and parent stakeholder self-identified with one of the three clinical groups of interest.
Stakeholder roles
Both AYAs and parents endorsed their role as providing a voice for the larger population they represented, engaging as part of a team, and working among a diverse group of stakeholders as unique roles. Illustrative of the value placed on being part of a team that engages a diverse set of stakeholder perspectives, one AYA stated: “I think being a stakeholder is part of being a team…the position's there to provide perspective and to be able to give ideas or opinions on a specific topic. And I think that like it's a big important part of a study to have like a variety of different ages, or people, or personalities”.
One parent articulated an additional theme of giving back as part of stakeholder engagement: “So from my (child's) medical experience, I really do like the opportunity to feel like I'm giving back a little bit to the medical community”.
All stakeholders emphasized that involving a diverse set of stakeholders with varied backgrounds, experiences and perspectives was positive for the research team and the quality of the research conducted. They also described a mutual respect for the expertise of the different stakeholder panel members.
AYA & parental expertise
All AYAs recognized their lived experience as the source of greatest expertise that they brought to the core research study. The three AYAs with FH or other cardiovascular risk factors cited the specific experiences of living with their respective health conditions, including previous experiences interacting with parents and clinicians making medical decisions. One AYA commented that his expertise included: “Just knowing like what personal decisions I would make in my medical treatments and how to involve my parents and that kind of thing because I'm at that age”.
The AYAs freely acknowledged having limited to no medical expertise, deferring to the professional stakeholder panel members. One AYA felt that her lack of clinical knowledge actually helped her better represent all AYAs: “I don't have high cholesterol in my family. I've never been asked that my doctors test my cholesterol. So it was never like even a thought that crossed my mind. So just the lack of information, and I feel like that might be similar to a lot of young adults as well”.
Parents similarly rejected possessing medical expertise, noting their expertise came from their experiences in personal and familial decision-making. All parents referenced experiences in making decisions pertinent to a specific health condition for their child; for example, the parent of a child with FH described educating and advocating for her son for over 20 years. Parents also voiced drawing on their experiences in helping their children make decisions within the context of their transition from pediatric- to adult-based care and gaining autonomy in their decision-making. As one mother stated: “…especially with the transition from adolescence to young adults, it's the parents who have done the initial legwork with making the medical decisions, and so their emotional experience I think, has a lot of weight”.
Power differentials: challenges & recommendations
All AYAs and two parents endorsed the power differentials of the stakeholder meetings as a challenge to participation on the surveys. Power differentials existed due to imbalances in expertise/profession and societal stature. First, both AYAs and parents reported feeling initially ‘intimidated’ by the ‘really high level of expertise’ of the professional stakeholders. Imbalances in expertise were not identified in meetings only involving the patient stakeholders, suggesting the presence of the professional stakeholders accentuated this dynamic. Second, several AYAs described some insecurity when disagreeing with a parent's perspective given the parent's inherent ‘authority.’ AYAs experienced this dynamic even though none of the AYAs and parents were related. Stakeholders recognized the value of activities the research team implemented to mitigate power differentials but identified persistent challenges. We discuss these challenges and the corresponding stakeholder-identified recommendations by the three identified drivers to address power differentials: building shared knowledge, building relationships and acquiring trust and logistics (see Table 2).
Building shared knowledge
Despite efforts made to build shared knowledge by the research team, two challenges were identified. From the survey results, at least half of the AYAs found vocabulary and acronyms around cholesterol, the clinical focus of the core study and CER methods challenging and some of the research topics, especially regarding decision modeling, were too complex. From the interviews, AYAs expressed the challenge of processing material shared prior to the meetings, then having to form and articulate perspective on new information to the other stakeholders.
Recommendations were commensurate with the identified challenges. To promote capacity around research and clinical understanding, AYAs suggested continued reminders to professionals to decrease use of complex terminology as well as more preparatory materials prior to meetings, including an updated glossary and ‘refresher’ materials sent out the week before for the meeting to give stakeholders the opportunity to review decisions from the previous meeting. Building off of the initial stakeholder-specific meetings, both AYAs and parents endorsed the idea of meeting in their respective ‘small groups’ prior to the larger panel calls to prepare for and present ideas to the ‘big group’ during meetings. These meetings would establish a more unified voice for their stakeholder group.
Building relationships & acquiring trust
Two challenges were raised from the interviews: clarity regarding the role of the patient stakeholder and discomfort with disclosure of personal and family medical history without more trust between stakeholders. For both AYAs and parents, challenges arose when meetings involved the professional stakeholders as the pace of the conversation often accelerated and patient stakeholders were less clear on their role. Both AYAs and parents also struggled with not having more of a relationship with other stakeholders that would facilitate their personal disclosures of their own healthcare experiences and decisions. AYAs and parents also expressed discomfort with professional stakeholders disclosing their own personal health decisions without the opportunity to get to know them better.
To build relationships and establish trust, both stakeholder groups suggested in-person meetings at least once at the study outset but potentially as frequently as monthly over the study duration. Proposed benefits of an initial face-to-face meeting included more efficient and enhanced collaboration and increased comfort levels for disclosure.
Although video conferencing technologies were suggested as a way to enhance the webinar experience, the consensus was that in-person meetings had no substitute. While most stakeholder acknowledged the fiscal and time constraints of hosting in-person meetings, all agreed the benefits would outweigh these costs.
Last, during the interviews, patient stakeholders also suggested ongoing clarification and refinement of their respective roles. While roles had been discussed in the initial meetings, AYAs and parents suggested revisiting those roles over the course of the study. They also suggested assigning topics or questions on which each group could focus, raising their level of expertise in that area and balancing the power dynamic with professionals. For example, a parent recommended that the research team routinely pose specific questions to their group, which would become their ‘area of expertise’ for that meeting.
Logistics
All stakeholders took very seriously their responsibility to participate and went to significant efforts to stay engaged. However, in both the survey and interviews, AYAs and parents acknowledged scheduling meeting times convenient to their schedule was a significant challenge. The AYA and parent stakeholders routinely requested evening and weekend times outside of the school or work day as they were less in control over their schedules. Medical issues also impacted participation; one AYA shared he was either in the emergency room or hospitalized multiple times when stakeholder meetings were scheduled. Neither group had issues accessing the needed technology, although parents described a learning curve with using Doodle for scheduling and webinars for sharing information as a ‘generational thing.’
In addition, AYA stakeholders experienced several significant transitions over the course of the study. Two stakeholders graduated high school and college, starting college and a full-time job, respectively. Another AYA spent a college semester abroad and another relocated across the country. These transitions presented competing demands that impacted their engagement in the research despite a willingness to continue participation.
Recommendations primarily consisted of ongoing attention to logistical issues.
Impact of patient engagement
The perception of patient impact emerged into two categories: personal, related to the stakeholder's own beliefs, practices and decision-making, and research, with regard to the research study and patient population.
Personal impact
Both AYAs and parents reported enhanced understanding of medical knowledge (i.e., the impact of cholesterol on health), healthcare decision-making, and the research process in general. On the surveys, five AYAs and all three parents agreed that being a stakeholder changed how they think about their own health. In the interviews, AYAs described better understanding the effects of hyperlipidemia and the importance of maintaining a healthy lipid level, as one AYA shared: “Yeah. But I'm more aware of the dangers of high cholesterol and what it takes for someone to do a screening for cholesterol. And I know I've had high cholesterol for, throughout all my life. And I think I'm more aware and more conscious of what I still need to do to keep my cholesterol on the safe level”.
AYAs also commented that exposure to research methodologies and results influenced their own medical decision-making and consideration of their and their parents’ role in decision-making. All parents agreed that being a stakeholder impacted how they thought about health and made medical decisions as well as the importance of their children implementing a healthy lifestyle and understanding the long-term effects of hyperlipidemia. Two parents described feeling ‘empowered’ by the stakeholder engagement process; one stated: “as a parent of a kid with FH, I felt pretty powerless over his disease, and it's just been a way for me to feel like I can have some effect on the future of how other, you know, what might come about for other kids in the future”.
Research impact
Most AYA and parent stakeholders endorsed that their contributions as a stakeholder impacted how the research was conducted. In particular, the inclusion of AYAs was heavily endorsed; as one AYA summarized, their inclusion was critical for “representing a part of the population that doesn't necessarily always get talked to”. Two AYAs thought they could have had a better impact with a more thorough grounding in the topic and research methods. All parents perceived their participation as improving the science and care of AYAs with hyperlipidemia.
Discussion
This is one of the first studies to examine the engagement of AYA and parent stakeholders in a CER study. Our findings are consistent with existing work articulating the roles for stakeholders in research, including informing research questions, identifying patient-centered outcomes, improving research processes and facilitating dissemination of findings [24]. We expand upon this work by capturing the unique perspectives of AYA and parents following participation in a core CER study, highlighting challenges and stakeholder-suggested solutions unique to engaging patients, including AYAs, as members of a multistakeholder panel in CER.
Employing three methodologies for patient engagement that addressed shared knowledge, trust and relationships, and logistics, we were able to mitigate against some issues with respect to power differentials. Patient stakeholders identified additional strategies for reducing power differentials, including advance resource sharing, hosting in-person and stakeholder-specific meetings, explicitly defining and continuously revisiting roles, and calling out the contributions of AYA and parent team members.
Unique to the AYA population were the logistical challenges of participation. Partially because of power differentials in the school or work setting, AYAs had less ability to change their schedules. In addition, transitions occurring during this life stage affected participation in the research process. Extra efforts will likely be needed to meet AYAs where they are at, both literally if they change educational, occupational or geographic locations during the study and metaphorically, as they acquire emotional and cognitive complexity with their advancing age.
Stakeholders also shared the personal benefits of participation in CER. Both AYAs and parents described intrinsic benefits from this level of participation in the research process, including better attention to their own health or that of their AYA child and empowerment to speak up in the medical decision-making process.
Further engagement of AYAs in CER holds great promise. One of the tenants of Positive Youth Development, a strength-based theoretical framework that focuses on developmental assets, is the engagement of youth in meaningful roles with caring adult mentors [25]. Engagement of AYAs in the planning, execution and interpretation of results for research designed to improve AYA health is critical for moving adolescent health forward. The Society for Adolescent Health and Medicine Committee on Research endorses this approach [26] and there is a long history of consulting AYAs on research design via teen advisory boards or as part of CBPR [23,27]. With new funding mechanisms tied to the inclusion of patient stakeholders in research, engagement of AYAs in the research process will hopefully expand further.
Limitations
We highlight several limitations. First, even though all AYA and parent stakeholders who were stakeholders on the core CER study participated, the sample size is small. This study is exploratory in nature so the inability to achieve thematic saturation does not make the finding invalid but does suggest the phenomenon requires further exploration [22]. Second, professional stakeholders’ evaluation data was excluded from this analysis to focus on patient stakeholders. Last, the research team member who conducted the individual interviews had administrative interactions with stakeholders throughout the study; this familiarity could have biased stakeholders’ responses.
Conclusion
Our study underscores the unique opportunities and challenges that arise when AYAs and parents serve as formal patient stakeholders on multidisciplinary stakeholder panels. AYAs and parents felt their participation as stakeholders benefitted both the core HEARYA study and their own healthcare decision-making. However, both experienced power differentials when engaged in CER. Despite efforts by the research team to lessen such differences, unequal power dynamics existed among AYA, parent and professional stakeholders. Recommendations provided by AYAs and parents can inform future efforts with engaging patients as stakeholders.
Future perspective
Engaging stakeholders in CER has been theorized to improve the relevance, feasibility and dissemination and adoption of research. Patient stakeholders are crucial to include but only limited information is available at this time. PCORI has already begun to target best practices for engaging relevant and diverse stakeholders, and we expect both the quantity of studies engaging stakeholders and the quality with respect to patient participation to improve.
| Characteristics | AYAs (n = 6) | Parents (n = 3) |
|---|---|---|
| Female | 4 | 3 |
| Age range (years) | 17–25 | 50–55 |
| Race/ethnicity: | ||
| – Hispanic/white | 1 | 0 |
| – Hispanic/black | 2 | 0 |
| – Non-Hispanic/black | 1 | 0 |
| – Non-Hispanic/white | 1 | 2 |
| – Non-Hispanic/white/Asian | 1 | 0 |
| – Non-Hispanic/Asian | 0 | 1 |
| Identification with clinical group of interest: | ||
| – Familial hypercholesterolemia | 1 | 1 |
| – Other cardiovascular risk factor | 2 | 1 |
| – No known cardiovascular risks | 3 | 1 |
AYA: Adolescent and young adult.
| A priori domains identified by research team. Key drivers to address power differentials | SH-identified challenges | SH-identified recommendations | ||
|---|---|---|---|---|
| Specific challenges | Illustrative SH perspective | Specific recommendations | Illustrative SH recommendation | |
| Shared knowledge | Complexity of clinical and research terminology Ability of young adult and parent stakeholders to keep up with clinician and researcher stakeholders | I feel like it was a lot more clinical, so sometimes I feel like well I do not know if I should say anything because I'm not obviously experienced around cholesterol, like clinically (AYA) I think the biggest challenge for me was learning everything as we went, and sharing an opinion on it. Especially as it related to the more technical questions, more specifically about FH, or more specifically about a certain modeling process. Because you can read about materials all day but if you're in an environment where you see a lot, or do it a lot, you're going to know the ins and outs of it better than someone who is just reading materials on it (AYA) | Reminders about jargon More preparatory materials SH-specific meetings | I guess it might be helpful for the facilitator to again emphasize and to remind those who have the clinical background to speak in plain laymen terms. Like to explain things in a way that people who are not from this country or who is language is not English, to better understand, to have a better grasp of what they're talking about (PT) If we had a little more time to read through and digest the material prior to the call, I think I would have had a little bit more to offer in terms of comments or questions (AYA) Whether it is all young adults or all parents…it could definitely bring about more of the same opinions, and maybe different opinions, and give people an opportunity to speak among people who they can relate to (AYA) |
| Relationships and trust | Interaction with clinician and researcher stakeholders Disclosure of personal and family history | And then I wanted, sometimes I did want to say something but I did not really know what to say because I did not really understand what was being said and then I didn't know how to change the topic either, because (the clinicians) looked like they were really into their conversation (AYA) At first I did not know that one of the other parents had a child with FH, and so I was a little concerned… talking about long-term effects, and…making decisions. So some of the early questions about whether or not I personally would…put my child on the statins at a young age, and there's another parent that really has to face that. That was a little uncomfortable (PT) | Host at least one in-person SH meeting Use video conferencing technologies Clear definition of roles on SH panel Assigning SH specific topics or questions | I think maybe if there were more specific questions to the parents of what was needed from them, from maybe specific questions, and you know, as being a parent, that might be helpful, maybe just filling out, you know, some surveys. And then the other thing that I was thinking about is, some of them not being a researcher, if it was as specifically said, “This is the areas that you are helping out in (PT) I actually think that if there was a way to do meetings in person that could be really helpful. Because I think even if it's just the first meeting is in person, and then after that you have webinars, I think it is beneficial for everyone to kind of meet everybody, do a little bit of intro. You gain comfort a lot faster. You're able to share things that you think are helpful versus nonhelpful (AYA) |
| Logistics | Difficult to plan meeting times around different schedules Including young adult SHs through major transitions | I'm not sure there is a way, because as a working parent, typically the daytime hours are shot, but then you come home, and who wants to give up their evening hours if that's the only time that you might have with your kids? So I think it's just one of those things that you have to figure out how to work around (PT) I just think that the stakeholder meetings are just a bit too far apart and it is hard for me to really remember what was done the last time (AYA) | Ongoing attention to logistics | I just think if we had more periodic meetings, and I know this is very difficult because everyone has a crazy schedule, it would be better for me to keep the flow as in this is what was done during my last meeting, and this is what I am supposed to focus on for the next meeting, maybe like 2 weeks after (AYA) |
AYA: Adolescent and young adult; FH: Familial hypercholesterolemia; PT: Parent; SH: Stakeholder.
Power differentials exist between patient and professional researchers.
For adolescent/young adult patients, engagement efforts also must address inherent authority differences between adolescents/young adults and older adults.
Addressing shared knowledge, relationships and trust, and logistics can help mitigate these power differentials.
Patient perspectives on stakeholder engagement, particularly from adolescents and young adults, deserve additional study.
Acknowledgements
The authors thank the young adult and parent members of the stakeholder panel for the Hyperlipidemia Evaluation and Treatment in Young Adults (HEARYA) study. A special thanks to the young adult and parent stakeholders for their invaluable contributions and dedication to this research.
Disclaimer
The views expressed in this paper are those of the authors and do not necessarily reflect the official views of the Patient-Centered Outcomes Research Institute (PCORI).
Financial & competing interest disclosure
The study was funded by the Patient Centered Outcomes Research Institute (PCORI). The funder was in no way involved with the design and conduct of the study; collection, management, analysis and interpretation of the data; or preparation, review or approval of the article. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all humans or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained for the participants involved.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Selby JV, Beal AC, Frank L. The Patient-Centered Outcomes Research Institute (PCORI) national priorities for research and initial research agenda. JAMA 307(15), 1583–1584 (2012).
2.
Clinical and Translational Science Award Program. Community Engagement Key Function Committee. Principles of Community Engagement Second Edition. NIH Publication No. 1-53 (2011).
3.
Balshem H, Curtis P, Joplin L, Justman RA, Rosenberg AB. Stakeholder involvement in improving comparative effectiveness reviews: AHRQ and the Effective Health Care Program (Prepared by the AHRQ Effective Health Care Program Product Development Work Group under Contract No. HHSA 290–2007–10057-I), (11-EHC079-EF) (2011). www.effectivehealthcare.ahrq.gov.
4.
Concannon TW, Meissner P, Grunbaum JA et al. A new taxonomy for stakeholder engagement in patient-centered outcomes research. J. Gen. Intern. Med. 27(8), 985–991 (2012).
5.
Gliklich RE, Leavy MB, Velentgas P et al. Incorporating stakeholder perspectives in developing a translation table framework for comparative effectiveness research. J. Comp. Eff. Res. 1(3), 281–292 (2012).
• Describes the assembly of a diverse committee of stakeholders to create a framework for selecting a comparative effectiveness research (CER) study design. Exemplifies how to engage multidisciplinary stakeholders around a shared task.
6.
Deverka PA, Lavallee DC, Desai PJ et al. Stakeholder participation in comparative effectiveness research: defining a framework for effective engagement. J. Comp. Eff. Res. 1(2), 181–194 (2012).
7.
Forsythe LP, Ellis LE, Edmundson L et al. Patient and stakeholder engagement in the PCORI pilot projects: description and lessons learned. J. Gen. Intern. Med. (2015) (Epub ahead of print).
8.
Concannon TW, Fuster M, Saunders T et al. A systematic review of stakeholder engagement in comparative effectiveness and patient-centered outcomes research. J. Gen. Intern. Med. 29(12), 1692–1701 (2014).
• Summarizes the relatively limited and highly varied literature around stakeholder engagement in CER. Offers guidance on how to report stakeholder engagement activities as to benefit ongoing and future studies.
9.
Arnett JJ. Emerging adulthood. A theory of development from the late teens through the twenties. Am. Pyschologist 55(5), 469–480 (2000).
10.
Bleyer A, Ulrich C, Martin S. Young adults, cancer, health insurance, socioeconomic status, and the Patient Protection and Affordable Care Act. Cancer 118(24), 6018–6021 (2012).
11.
Bogart LM, Uyeda K. Community-based participatory research: partnering with communities for effective and sustainable behavioral heath interventions. Heath Psychol. 28(4), 391–393 (2009).
12.
Kauffman KS, Dosreis S, Ross M, Barnet B, Onukwugha E, Mullins CD. Engaging hard-to-reach patients in patient-centered outcomes research. J. Comp. Eff. Res. 2(3), 313–324 (2013).
•• Identifies methods to engage often vulnerable, hard-to-reach patient populations in the CER process. Focuses on building and maintaining trust with both patients and the communities in which they live.
13.
O'Haire C, McPheeters M, Nakamoto EK et al. Methods for engaging stakeholders to identify and prioritize future research needs. methods future research needs report No. 4. (prepared by the Oregon Evidence-based Practice Center and the Vanderbilt Evidence-based Practice Center under Contract No. 290–2007–10057-I.). AHRQ Publication No. 11-EHC044-EF (2011). www.effectivehealthcare.ahrq.gov.
•• Served as a guide on how to define, recruit and engage the patient stakeholders in our core study. We directly used many of the methods presented in this report because we began engaging stakeholders prior to the release of the PCORI engagement rubric.
14.
Meredith Minkler VR. Ten case studies of community-based participatory research and their policy efforts and outcomes. University of California Berkeley. Policy Link 16–38 (2008).
15.
Israel BA. Methods in Community-Based Participatory Research for Health. Jossey-Bass Inc., San Francisco, CA, USA (2005).
16.
Rothschild SK, Lapidos S. Virtual integrated practice: integrating teams and technology to manage chronic disease in primary care. J. Med. Syst. 27(1), 85–93 (2003).
17.
Kirschner PA, Van Bruggen J. Learning and understanding in virtual teams. Cyberpsychol. Behav. 7(2), 135–139 (2004).
18.
Frank L, Forsythe L, Ellis L et al. Conceptual and practical foundations of patient engagement in research at the Patient-Centered Outcomes Research Institute. Qual. Life Res. 24(5), 1033–1041 (2015).
•• Explains PCORI's Engagement Rubric, a unique model for how to effectively engage multidisciplinary stakeholders. The rubric informed the questions asked in the interview guide used to interview young adult and parent stakeholders as part of the Patient Stakeholder Perspectives study.
19.
Frank L, Basch C, Selby JV. The PCORI perspective on patient-centered outcomes research. JAMA 312(15), 1513–1514 (2014).
20.
Willms DG, Best JA, Taylor DW et al. A systematic approach for using qualitative methods in primary prevention research. Med. Anthro. Q. 4(4), 391–409 (1990).
21.
Harry B, Sturges K, Klingner J. Qualitative data analysis: mapping the process. Educ. Res. 34(2), 3–13 (2005).
22.
O'Reilly M, Parker N. ‘Unsatisfactory Saturation’: a critical exploration of the notion of saturated sample sizes in qualitative research. Qual. Res. 13(2), 190–197 (2013).
23.
Rich C, Goncalves A, Guardiani M, O'Donnell E, Strzelecki J. Teen Advisory Committee: lessons learned by adolescents, facilitators, and hospital staff. Pediatr. Nurs. 40(6), 289–296 (2014).
24.
Brett J, Staniszewska S, Mockford C et al. Mapping the impact of patient and public involvement on health and social care research: a systematic review. Health Expect. 17(5), 637–650 (2014).
25.
Lerner RM, Brentano C, Dowling EM, Anderson PM. Positive youth development: thriving as the basis of personhood and civil society. New Dir. Youth Dev. (95), 11–33 (2002).
•• Provides guidance around engaging adolescents and young adults in meaningful roles in the context of adult mentors. Used principles to facilitate young adult stakeholder engagement in the core study.
26.
Santelli JS, Rosenfeld WD, Durant RH et al. Guidelines for adolescent health research: a position paper of the society for adolescent medicine. J. Adolesc. Health 17(5), 270–276 (1995).
27.
Vaughn LM, Wagner E, Jacquez F. A review of community-based participatory research in child health. MCN Am. J. Matern. Child Nurse 38(1), 48–53 (2013).
Information & Authors
Information
Published In
Copyright
© Future Medicine Ltd.
History
Published online: 18 July 2016
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Young adult and parent stakeholder perspectives on participation in patient-centered comparative effectiveness research. (2016) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0025
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Kayla R. Mehl, Stephanie R. Morain, Jeremy Sugarman, Empirical research related to the ethics of pragmatic clinical trials: A scoping review, Learning Health Systems, 10.1002/lrh2.70041, 10, 1, (2025).
- Vence L. Bonham, Kiana Amini, Ashley J. Buscetta, Diba Seddighi, Hasmin C. Ramirez, Rachele Willard, Kimberly A. Kaphingst, Democratizing Education for Sickle Cell Disease Gene Therapy: A Community-Based Model for Creating Patient Education Materials, Public Health Genomics, 10.1159/000548133, 28, 1, (292-300), (2025).
- Christine A March, Elissa Naame, Ingrid Libman, Chelsea N Proulx, Linda Siminerio, Elizabeth Miller, Aaron R Lyon, School-Partnered Collaborative Care (SPACE) for Pediatric Type 1 Diabetes: Development and Usability Study of a Virtual Intervention With Multisystem Community Partners, JMIR Diabetes, 10.2196/64096, 10, (e64096), (2025).
- Amy G. Nevin, Christine A. March, Lauren Jones, Kenneth Nash, Radhika Muzumdar, Justin Schreiber, Ingrid M. Libman, Measuring Outcomes for Community Partner Engagement: The Case of the High-Fidelity Wraparound Program for Pediatric Type 1 Diabetes, Diabetes Spectrum, 10.2337/ds24-0036, 38, 2, (161-170), (2024).
- Daniella Watson, Mimi Mhlaba, Gontse Molelekeng, Thulani Andrew Chauke, Sara Correia Simao, Sarah Jenner, Lisa J. Ware, Mary Barker, How do we best engage young people in decision-making about their health? A scoping review of deliberative priority setting methods, International Journal for Equity in Health, 10.1186/s12939-022-01794-2, 22, 1, (2023).
- Jonathan Lauzon-Schnittka, Sophie Audette-Chapdelaine, Denis Boutin, Catherine Wilhelmy, Anne-Marie Auger, Magaly Brodeur, The experience of patient partners in research: a qualitative systematic review and thematic synthesis, Research Involvement and Engagement, 10.1186/s40900-022-00388-0, 8, 1, (2022).
- Rachel Hemphill, Laura P. Forsythe, Andrea L. Heckert, Andrew Amolegbe, Maureen Maurer, Kristin L. Carman, Rikki Mangrum, Lisa Stewart, Ninma Fearon, Laura Esmail, What motivates patients and caregivers to engage in health research and how engagement affects their lives: Qualitative survey findings, Health Expectations, 10.1111/hex.12979, 23, 2, (328-336), (2019).
- Jenny Martinez, Carin Wong, Catherine Verrier Piersol, Dawn Clayton Bieber, Bonita L Perry, Natalie E Leland, Stakeholder engagement in research: a scoping review of current evaluation methods, Journal of Comparative Effectiveness Research, 10.2217/cer-2019-0047, 8, 15, (1327-1341), (2019).
- Rachel Flynn, Sarah Walton, Shannon D. Scott, Engaging children and families in pediatric Health Research: a scoping review, Research Involvement and Engagement, 10.1186/s40900-019-0168-9, 5, 1, (2019).
- Kristin N Ray, Elizabeth Miller, Strengthening stakeholder-engaged research and research on stakeholder engagement, Journal of Comparative Effectiveness Research, 10.2217/cer-2016-0096, 6, 4, (375-389), (2017).