Improved clinical, functional and work outcomes in spondyloarthritides during real-life adalimumab treatment in central–eastern Europe
Abstract
Aim: Adalimumab effectiveness on clinical, functional and work-related outcomes was evaluated in patients with active ankylosing spondylitis or psoriatic arthritis treated in routine clinical practice in central–eastern Europe. Methods: Patients (n = 555) were followed for 12 months. Primary end point was percentage of patients with a treatment response (≥50% decrease from baseline in Bath Ankylosing Spondylitis Disease Activity Index or ≥1.2 point decrease from baseline in Disease Activity Index-28 joint for axial or peripheral symptoms, respectively). Functional status was evaluated by the Bath Ankylosing Spondylitis Functional Index and Health Assessment Questionnaire Disability Index. Working ability was evaluated by the Work Productivity and Activity Impairment Questionnaire − Specific Health Problem. Results: 76.1% of patients with axial symptoms and 83.5% with peripheral symptoms achieved a treatment response. Frequency of extra-articular manifestations decreased. Improvements were observed in functional status and workability. No new safety signals were observed. Conclusion: Adalimumab was effective and well tolerated during real-world use in central–eastern Europe.
First draft submitted: 21 March 2016; Accepted for publication: 16 June 2016; Published online: 14 July 2016

Figure 1. Patient disposition.
AE: Adverse event; AS: Ankylosing spondylitis; FAS: Full analysis set; PsA: Psoriatic arthritis.

Figure 2. Evolution of disease activity in the axial analysis set and peripheral analysis set.
AAS: Axial analysis set; ASDAS: Ankylosing Spondylitis Disease Activity Score; BASDAI: Bath Ankylosing Spondylitis Disease Activity Index; CRP: C-reactive protein; DAS28: Disease Activity Score – 28 joints; ESR: Erythrocyte sedimentation rate; LOCF: Last observation carried forward; PAS: Peripheral analysis set.

Figure 3. Evolution of extra-articular manifestations in patients with ankylosing spondylitis or psoriatic arthritis.
AS: Ankylosing spondylitis; IBD: Inflammatory bowel disease; LOCF: Last observation carried forward; PsA: Psoriatic arthritis.
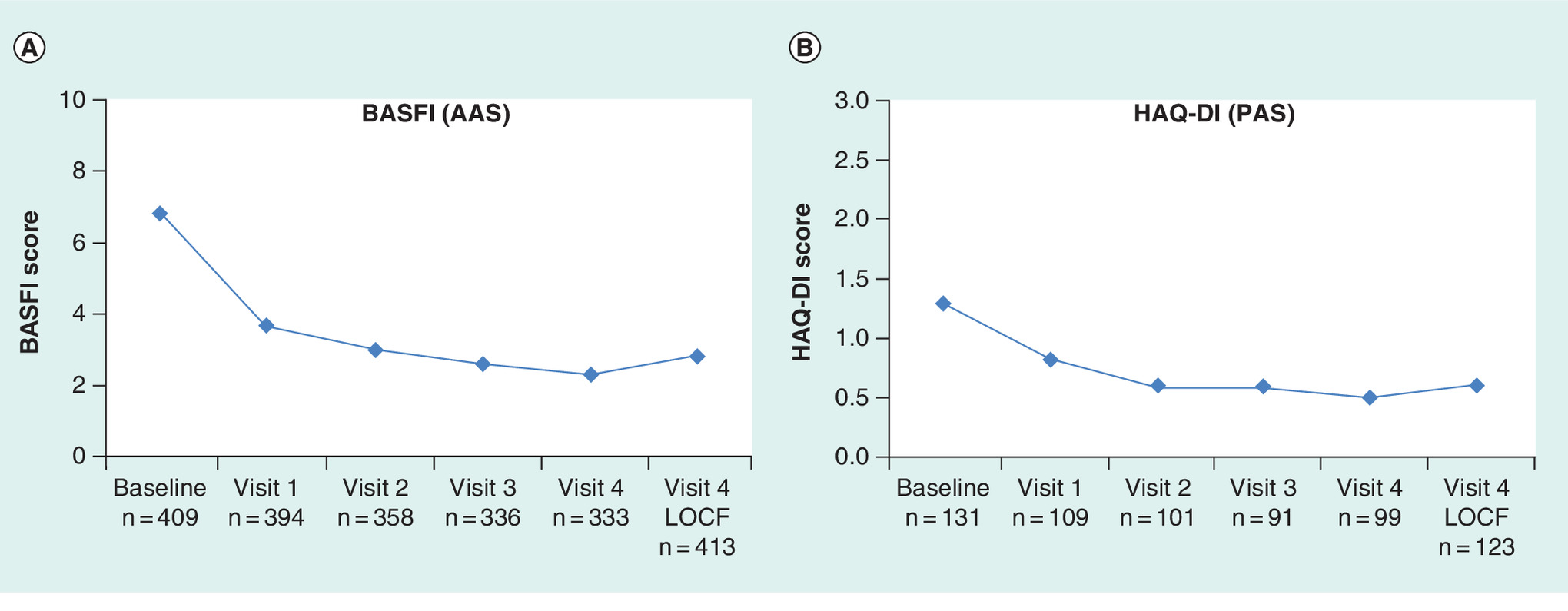
Figure 4. Evolution of functional activity in (A) the axial analysis set and (B) the peripheral analysis set.
AAS: Axial analysis set; BASFI: Bath Ankylosing Spondylitis Functional Index; HAQ-DI: Health Assessment Questionnaire – Disability Index; LOCF: Last observation carried forward; PAS: Peripheral analysis set.
Ankylosing spondylitis (AS) and psoriatic arthritis (PsA) are chronic inflammatory diseases belonging to a group of rheumatic diseases known as spondyloarthritides (SpA). AS primarily affects the axial skeleton, with characteristic involvement of the spine and sacroiliac joints, which can lead to spine deformity and disability. Certain peripheral joints and tendons can be affected, and extra-articular manifestations (EAMs) may be present [1]. PsA is an inflammatory arthritis that occurs in up to a third of patients with psoriasis. Although peripheral joint synovitis is a major articular feature of PsA, other manifestations include axial disease, enthesitis, dactylitis, and skin and nail disease (psoriasis) [2]. If not managed effectively, PsA may lead to joint destruction and disability [2].
Over the past decade, the treatment of AS and PsA has been revolutionized by the incorporation of tumor necrosis factor (TNF) inhibitors into the management algorithm. The greater efficacy of TNF inhibitors compared with conventional disease-modifying antirheumatic drugs has been largely responsible for the shift in emphasis toward achieving a low disease activity status or even remission and preventing loss of function [1,2].
The clinical efficacy and safety of the recombinant, fully human, IgG1 monoclonal antibody adalimumab in the treatment of patients with AS and PsA have been demonstrated in randomized, double-blind, placebo-controlled clinical trials [3–6]. Subsequent extension studies with open-label adalimumab reported sustained benefit through 5 years in patients with AS [7] and 2 years in patients with PsA [8]. While randomized controlled trials are the foundation of evidence-based medicine, it is necessary also to determine the effectiveness and tolerability of a medicinal product outside the strict environment of experimental studies; this is the domain of noninterventional observational studies.
There is a dearth of published literature on clinical effectiveness and patient-reported outcomes in patients with AS and PsA treated with adalimumab in central and eastern Europe. The purpose of the current study was to evaluate the long-term clinical outcomes of adalimumab therapy in routine clinical practice in central–eastern Europe; in particular, its effectiveness on disease activity and EAMs, and its impact on functional capacity, work productivity impairment and the need for co-medication with NSAIDs. Additional objectives were to evaluate current diagnostic and treatment practices, including use of the new, and potentially more appropriate, Ankylosing Spondylitis Disease Activity Score (ASDAS) to determine the effect of adalimumab treatment on axial symptoms, and to collect additional safety-related data in everyday practice.
Methods
Study design & population
This multicenter, prospective, single-arm, noninterventional, observational study was conducted in six countries in central and eastern Europe: the Czech Republic, Estonia, Hungary, Romania, Slovakia and Ukraine. All participating sites were medical centers experienced in the biological treatment of patients with AS and PsA. Investigators were selected for participation if they had the available patient population (representative of the target patient population) in their respective country, and the ability to appropriately conduct the observational study in accordance with applicable legal and regulatory requirements. The study was approved by local Ethics Committees of participating countries according to local law and regulations.
Eligible patients were adults greater than 18 years of age with a diagnosis of AS (primarily by modified New York criteria [9]) or PsA (primarily by Moll-Wright criteria [10] or ClASsification for Psoriatic ARthritis [CASPAR] criteria [11]) who were eligible for adalimumab treatment and were prescribed adalimumab within a maximum of 1 month prior to study enrolment (and independent of study inclusion). Patients had to either have a negative test result for tuberculosis (TB) or receive TB prophylaxis as per local guidelines. Patients had to be willing to authorize use and disclosure of personal and health data, and to provide written informed consent to participate in the study. Patients with contraindications for adalimumab treatment [12] were excluded from the study.
Patients were treated with adalimumab according to the local product label and prescription/reimbursement guidelines and were observed for up to 12 months. Patients received adalimumab 40 mg subcutaneously every other week throughout the 12-month observation period. Evaluations were to be conducted at enrollment (baseline), and then at 3 months (visit 1), 6 months (visit 2), 9 months (visit 3) and 12 months (visit 4), although the actual number and timing of follow-up visits were at the investigator’s discretion. In the case of premature discontinuation of adalimumab treatment before study end, the patient’s next routine follow-up visit was the termination visit from the study.
Assessments
At each clinic visit, data were collected by physicians or designated site personnel using an electronic clinical report form. Baseline documentation included socio-demographic characteristics, medical and diagnostic history, pharmacological treatment of spondyloarthritis (past and present), EAMs, laboratory parameters (erythrocyte sedimentation rate [ESR] and/or C-reactive protein [CRP]), and scores on the following indices: ASDAS, either as ASDASCRP or ASDASESR [13,14]; Bath Ankylosing Spondylitis Disease Activity Index (BASDAI; measured from 0 to 10) [15]; Disease Activity Score–28 joints (DAS28) [16]; Bath Ankylosing Spondylitis Functional Index (BASFI; measured from 0 to 10) for axial symptoms (defined as BASFI >4) [17]; Health Assessment Questionnaire-Disability Index (HAQ-DI; measured from 0 to 3) for peripheral symptoms (defined as DAS28 >5.1) [18]; Work Productivity and Activity Impairment Questionnaire − Specific Health Problem (WPAI-SHP; four outcomes, each expressed as a percentage from 1 to 100) [19]. Composite score values on these instruments and laboratory parameters (CRP and ESR) were assessed at each follow-up visit (if part of the normal routine). Additional documentation recorded throughout the observation period included concomitant medication, EAMs, occupation and working status, and serious adverse events (SAEs). SAEs were reported based on MedDRA (version 17.0, English) system organ class (SOC) and preferred term (PT). A SAE was classified as a serious adverse drug reaction (SADR) if the investigator rated causality with adalimumab as probably or possibly related.
Study end points
The primary end point was the percentage of patients with a response to adalimumab at 12 months, where response was defined as a ≥50% decrease from baseline on the BASDAI for patients with axial symptoms and a ≥1.2-point decrease from baseline on the DAS28 for patients with peripheral symptoms. A co-primary end point was the percentage of patients in remission at 12 months. Remission was defined as an ASDAS score <1.3 for patients with axial symptoms and a DAS28 score ≤2.6 for patients with peripheral symptoms. In the absence of agreed remission criteria for SpA, these criteria were selected by protocol authors.
Secondary end points measured from baseline to 12 months were: change in BASDAI and ASDAS scores (for axial symptoms) or DAS28 score (for peripheral symptoms); change in the frequency of EAMs; change in BASFI score (for axial symptoms) or HAQ-DI score (for peripheral symptoms); change in scores for individual outcomes of the WPAI-SHP (presenteeism – percentage of impairment while working due to AS or PsA; absenteeism – percentage of work time missed due to AS or PsA; total work productivity impairment – percentage of overall work impairment due to AS or PsA; total activity impairment – percentage of general [nonwork] activity impairment due to AS or PsA); and percentage of patients who discontinued concomitant treatment with NSAIDs.
Statistical analysis
All statistical analyses were conducted using SAS® version 9.2 (SAS Institute, Cary, NC, USA). Due to the observational nature of the study, no hypothesis testing or statistical tests were performed. Descriptive statistics and last observation carried forward (LOCF) method were used. Continuous parameters are described as number of subjects and mean ± standard deviation (SD). Qualitative data (e.g., gender) are described by absolute and relative (%) frequency distributions. For assessments over time, analyses by visit (visits 1–4) are complemented by an analysis using LOCF based on patients with a baseline value and at least one follow-up assessment, and are designated as visit 4 LOCF.
Analyses were performed separately for the two main datasets: the axial analysis set (AAS), which included all patients of the full analysis set (FAS) who had axial symptoms at baseline (i.e., BASDAI >4) and the peripheral analysis set (PAS), which included all patients of the FAS who had peripheral symptoms at baseline (i.e., DAS28 >5.1). Patients with both axial and peripheral symptoms were assigned to each of these analysis sets. Additional analyses were performed after further stratifying the analysis sets according to underlying diagnosis (AS or PsA).
Results
Patient disposition & distribution
The study was conducted between November 2011 and May 2014. Out of 566 enrolled patients, 280 patients (49.5%) participated in Hungary, 180 patients (31.8%) in Romania, 40 patients (7.1%) in Slovakia, 30 patients (5.3%) in the Czech Republic, 22 patients (3.9%) in Estonia and 14 patients (2.5%) in the Ukraine.
Patient disposition is shown in Figure 1. Eleven patients were lost to follow-up after baseline, with no further record of adalimumab treatment. These patients were excluded from the FAS. Altogether, 89 patients (16.0%) discontinued treatment with adalimumab during the observation period, mainly because of investigator’s decision/patient’s request (n = 59), or because of adverse events (n = 16), SAEs (n = 5) or loss to follow-up (n = 9).
A total of 431 patients (AS: 87.2%; PsA: 12.5%) with active axial symptoms comprised the AAS and 148 patients (AS: 25.7%; PsA: 74.3%) with active peripheral symptoms comprised the PAS; 61 patients with both axial and peripheral symptoms were included in both analysis sets. Enrolled patients (n = 37) who did not fulfill the criteria for either analysis set (due to baseline BASDAI ≤4 or DAS28 ≤5.1) were included only in analyses concerning the FAS (results not presented herein).
In study completers, mean treatment duration was 11.8 months in patients with AS and 11.6 months in patients with PsA.
Baseline demographics & clinical characteristics
The demographic and clinical characteristics of patients at baseline are summarized in Table 1. The majority of patients had AS (n = 403; 72.6%). The slight preponderance of males in the FAS (64.9%) reflected the expected gender distribution in AS. The mean age of the patient population was 45.6 ± 12.9 years (range: 18–80 years), although slightly higher in the PsA patient subset (49.7 ± 12.1 years). Mean disease duration (defined as time from symptom onset to study enrollment) was longer in patients with AS than in those with PsA (12.9 ± 10.3 vs 10.4 ± 9.2 years). The mean diagnostic delay (time frame between first symptoms and diagnosis) was 4.6 and 2.0 years, respectively. Investigator reports confirmed that all 79 patients (14.3%) with a baseline positive TB screening test received TB prophylaxis according to local professional guidelines. At study inclusion, approximately half of patients (n = 279; 50.3%) were in full-time paid employment, a minority worked part-time (n = 28; 5.0%) and a considerable proportion were work-disabled (n = 101; 18.2%).
A third of the population (n = 185) had previously been treated for spondyloarthritis. Most frequently used prior medications were sulfasalazine (13.6%) for AS and methotrexate (22.5%) for PsA; 17.7% of patients had previously been exposed to biological therapy. At the time of study inclusion, 426 patients (76.8%) were receiving concomitant medication, mainly diclofenac (19.4%) or sulfasalazine (19.1%) for AS and methotrexate (53.6%) or leflunomide (22.5%) for PsA. Concomitant use of NSAIDs (including COX-2 inhibitors) was recorded in 65.8% of patients (n = 265) with AS and 25.8% of patients (n = 39) with PsA.
Baseline scores on the BASDAI (6.4 ± 2.3) and DAS28 (5.9 ± 0.9) indicated a high level of disease activity. More than half the population (n = 299; 53.9%) had at least one EAM at study inclusion, most frequently enthesitis (23.1%) and uveitis (12.7%) in patients with AS, and psoriasis (90.1%) and enthesitis (17.2%) in patients with PsA. (N.B. while psoriasis is an inherent feature of PsA, it is also considered an EAM [20], and was classified as such in the study protocol).
Effectiveness
Disease activity
Disease activity outcomes are summarized in Tables 2 & 3. Clinical response at study end (visit 4 LOCF) was achieved in 76.1% of patients with axial symptoms (76.5% with AS; 73.1% with PsA) and in 83.5% of patients with peripheral symptoms (83.3% with AS; 83.6% with PsA). Clinical remission at study end (visit 4 LOCF) was achieved in 33.6% of patients with axial symptoms (34.3% with AS; 28.8% with PsA) and in 13.9% of patients with peripheral symptoms (11.1% with AS; 14.8% with PsA).
Disease activity index scores indicated rapid improvement within the first 3 months of adalimumab treatment, followed by a more gradual but continuous improvement up to the final visit for axial (BASDAI, ASDASCRP, ASDASESR) and peripheral symptoms (DAS28) (Figure 2). In parallel, the prevalence of EAMs decreased between baseline and study end (visit V4 LOCF). Evolution in individual types of EAMs over the 12-month observation period is illustrated in Figure 3. With regard to the most prevalent manifestations by specific disease, the frequency of enthesitis decreased from 23.1 to 3.2% and uveitis from 12.7 to 1.7% in patients with AS, and the frequency of psoriasis decreased from 90.1 to 43.0% and enthesitis from 17.2 to 4.0% in patients with PsA.
The decrease in disease activity associated with adalimumab treatment was further reflected in discontinuation rates for concomitant NSAID treatment. Among the 265 patients with AS (65.8%) and 39 patients with PsA (25.8%) who were receiving NSAIDs at the time of study inclusion, 96.6 and 94.9%, respectively, discontinued NSAID treatment during the 12-month observation period.
Functional status
The sustained effectiveness of adalimumab was reflected by improvements in functional status throughout the observation period (Figure 4). In patients with axial symptoms, the mean BASFI score decreased continuously from 6.8 ± 2.0 at baseline to 2.8 ± 2.3 at study end (visit 4 LOCF), with no relevant difference in the magnitude of change between the AS and PsA patient subgroups (-4.1 vs -3.8). In patients with peripheral symptoms, the HAQ-DI score decreased continuously from 1.3 ± 0.6 at baseline to 0.6 ± 0.5 at visit 4 LOCF, with no relevant difference in the magnitude of change between the AS and PsA patient subgroups (-0.9 vs -0.7).
Work productivity
Improvement in work ability and general (nonwork) activity during the observation period was demonstrated by mean percentage decreases from baseline to study end (visit V4 LOCF) in WPAI-SHP outcomes. Among patients who were in paid employment at study inclusion (n = 313; 56.4%), 255 had baseline WPAI-SHP data (n = 250 at visit V4 LOCF). In these patients, presenteeism (percentage of impairment while working) decreased from 56.7 to 20.1%, absenteeism (percentage of work time missed) decreased from 15.6 to 6.4%, and total work productivity impairment decreased from 59.9 to 22.1%. In the overall population with available data (n = 487), general (nonwork) activity impairment decreased from 64.3 to 28.0%. In general, baseline values tended to be slightly higher and mean decreases somewhat more pronounced for patients with AS compared with those with PsA.
Safety
A total of 52 SAEs were reported in 26 patients (4.7% of the population) during the course of the study. The most common events were skin and subcutaneous tissue disorders (seven patients; 1.3%) and surgical and medical procedures (six patients; 1.1%). Out of these SAEs, 31 events in 20 patients (3.6%) were considered to be SADRs based on investigator-assessed causality (probably or possibly related to treatment) (Table 4). SADRs were mainly skin and subcutaneous tissue disorders (six events; 1.1% of patients), general disorders and administration site conditions (four events; 0.7%) and nervous system disorders (three events; 0.5%). ‘Skin ulcer’ was the only SADR reported by more than one patient (n = 2).
Discussion
This prospective, single-arm, multicenter, observational study was undertaken to evaluate the effectiveness of adalimumab during routine use in patients with AS and PsA in six central and eastern European countries. End points of interest were the impact of adalimumab on disease activity, EAMs, functional capacity, work ability and concomitant use of NSAIDs.
In a previous observational study of AS patients from western Europe, Canada and Australia, evaluable patients (n = 1207) had a mean disease duration since symptom onset of 16 years and a mean BASDAI score of 4.6 at the initiation of anti-TNF therapy [21]. Although baseline disease duration was somewhat shorter in our patient population (mean 12 years), the level of disease activity was considerably higher as indicated by mean scores of 6.4 ± 2.3 on the BASDAI and 5.9 ± 0.9 on the DAS28. Irrespective, adalimumab had a sustained positive impact on measures of disease activity over the 12-month observation period. The majority of patients with axial (76.1%) or peripheral (83.5%) symptoms were treatment responders, and 33.6% and 13.9% of patients in these respective subsets achieved clinical remission. Adalimumab effectively attenuated patients’ EAMs, most notably halving the frequency of dermal psoriasis in patients with PsA from 90.1% at baseline to 43.0% at visit V4 LOCF. The sustained effectiveness of adalimumab was further evidenced by an NSAID discontinuation rate of >95% in both analysis sets during the course of the study.
The burden of AS and PsA on work status and productivity has been well documented. A cross-sectional study from The Netherlands involving 685 patients with AS aged 16–60 years found that labor force participation was 11% lower and AS-related work disability was 15% higher than that in the general population [22]. An observational study from Europe which followed 209 patients with AS for 2 years reported adjusted work disability rates of 41, 23 and 9% in The Netherlands, France and Belgium, respectively, higher in all countries than would be expected in the general population [23]. Among patients who had a paid job, the mean number of sick leave days per patient per year due to AS was 19, 6 and 9, respectively [23]. In patients with PsA, work disability rates of 25–39% at the start of treatment with disease-modifying agents or biological therapy have been reported [24,25].
In the current study, the positive impact of adalimumab on disease activity was paralleled by improvements in patients’ functional status and working ability. The BASFI and patient-reported HAQ-DI scales indicated sustained and continuous improvements in axial and peripheral symptoms throughout the observation period. Moreover, the substantial improvement observed in WPAI-SHP outcomes was particularly relevant considering that SpA typically affects young to middle-aged adults. Our findings are consistent with a post hoc analysis of the pivotal Adalimumab Trial Evaluating Long-Term Efficacy and Safety in AS [3], which reported sustained improvements in work outcomes (also measured on the WPAI-SHP) throughout 3 years of adalimumab exposure [26].
Tools to measure disease activity in patients with AS and PsA are considered to be an essential aspect of patient management. Current opinion is that composite measures inclusive of all clinical domains are more likely to provide complete and reliable information regarding disease activity and treatment response [27]. Recognized weaknesses in single-item variables (e.g., pain, CRP) and indices (e.g., BASDAI) used to measure AS disease severity led to development of the ASDAS [13], which has been shown to perform well methodologically and has high construct and discriminatory validity [13,14]. Inclusion of the acute phase reactants, CRP or ESR, enhances its clinical relevance [28]. In a post hoc analysis of the observational RHAPSDODY trial [29], the ASDAS and BASDAI were similarly sensitive to changes over time as calculated by standardized response means. Both instruments discriminated well between responders and nonresponders according to Assessment of SpondyloArthritis International Society 40% improvement criteria and ASAS partial remission criteria [30]. In this same analysis, the ASDAS proved to be applicable for analysis of treatment effects in AS subpopulations, covering both the patient’s and physician’s perspective without an obvious predominance of any construct, which is a recognized weakness of the fully patient-oriented BASDAI [28]. In the current observational study, the ASDAS was used widely by participating physicians suggesting that further investigation in clinical studies of anti-TNF therapy in patients with AS and PsA and more widespread use in routine clinical practice may be warranted.
Adalimumab was well tolerated in this study. All adverse events were within the scope of expected adverse drug reactions for this biological agent [12]. Consistent with another observational study which reported on the safety and effectiveness of adalimumab over 5 years of treatment in routine clinical practice [31], no new safety concerns were identified.
In terms of limitations, it is generally acknowledged that data collected in an observational study are of a lower evidence quality than those derived from a randomized clinical trial. Nevertheless, real-world data have advantages in terms of more readily allowing generalizations and deductions to the standard of care situation in other patients with AS and PsA. That said, values reported for disease activity in the current study must be interpreted with a degree of caution. Some instruments used to measure disease activity lack construct validity (e.g., BASDAI), while others were originally designed for other diseases (e.g., DAS28) or have yet to be widely adopted into daily practice (e.g., ASDAS). Notwithstanding these limitations, the long-term effectiveness of adalimumab observed in the current study aligns with results reported in other observational or open-label studies of adalimumab in routine clinical practice [7,8,31,32].
Conclusion
Adalimumab was shown to be an effective and well-tolerated treatment in patients with AS and PsA in central–eastern Europe. Axial and peripheral joint symptoms, as well as EAMs, were managed effectively. Along with disease activity, patients’ physical function and working ability improved. No new clinical concerns were identified with regard to type or incidence of SADRs, and no new safety signals were observed.
| Characteristics | FAS (n = 555)† | AS (n = 403) | PsA (n = 151) |
|---|---|---|---|
| Male, n (%) | 360 (64.9) | 294 (73.0) | 65 (43.0) |
| Age (years), mean ± SD | 45.6 ± 12.9 | 44.0 ± 12.8 | 49.7 ± 12.1 |
| Disease duration (years)‡, mean ± SD | 12.2 ± 10.0 | 12.9 ± 10.3 | 10.4 ± 9.2 |
| Positive TB screening at baseline, n (%) | 79 (14.3) | 58 (14.4) | 21 (13.9) |
| Working full-time (paid), n (%) | 279 (50.3) | 202 (50.1) | 76 (50.3) |
| Concomitant NSAID use§, n (%) | 304 (54.8) | 265 (65.8) | 39 (25.8) |
| BASDAI (0–10), mean ± SD | 6.4 ± 2.3 | 6.9 ± 1.7 | 4.5 ± 3.5 |
| DAS28, mean ± SD | 5.9 ± 0.9 | 5.5 ± 1.0 | 6.0 ± 0.9 |
| Patients with EAMs, n (%) | 299 (53.9) | 163 (40.4) | 136 (90.1) |
| Type of EAMs, n (%) | |||
| – Enthesitis | 119 (21.4) | 93 (23.1) | 26 (17.2) |
| – Uveitis | 56 (10.1) | 51 (12.7) | 5 (3.3) |
| – Psoriasis | 151 (27.2) | 15 (3.7) | 136 (90.1) |
| – Inflammatory bowel disease | 38 (6.8) | 36 (8.9) | 2 (1.3) |
†Includes one patient with a missing diagnosis.
‡From symptom onset to study enrolment.
§NSAIDs include COX-2 inhibitors.
AS: Ankylosing spondylitis; BASDAI: Bath Ankylosing Spondylitis Disease Activity Index; DAS28: Disease Activity Index – 28 joints; EAM: Extra-articular manifestation; FAS: Full analysis set; PsA: Psoriatic arthritis; SD: Standard deviation; TB: Tuberculosis.
| AAS (≥50% decrease on BASDAI) | PAS (≥1.2 decrease on DAS28) | ||||||
|---|---|---|---|---|---|---|---|
| Visit | n | Responder rate (%) | 95% CI (%) | Visit | n | Responder rate (%) | 95% CI (%) |
| V4 | 341 | 83.9 | − | V4 | 29 | 93.1 | − |
| V4 LOCF | 419 | 76.1 | 71.8–80.1 | V4 LOCF | 79 | 83.5 | 73.5–90.9 |
AAS: Axial analysis set; BASDAI: Bath Ankylosing Spondylitis Disease Activity Index; DAS28: Disease Activity Index – 28 joints;
PAS: Peripheral analysis set; V4: Visit 4; V4 LOCF: Visit 4 last observation carried forward.
| AAS (ASDAS <1.3) | PAS (DAS28 <2.6) | ||||||
|---|---|---|---|---|---|---|---|
| Visit | n | Responder rate (%) | 95% CI (%) | Visit | n | Responder rate (%) | 95% CI (%) |
| V4 | 322 | 41.0 | − | V4 | 29 | 27.6 | − |
| V4 LOCF | 414 | 33.6 | 29.0–38.3 | V4 LOCF | 79 | 13.9 | 7.2–23.5 |
AAS: Axial analysis set; ASDAS: Ankylosing Spondylitis Disease Activity Score; DAS28: Disease Activity Index – 28 joints; PAS: Peripheral analysis set; V4: Visit 4; V4 LOCF: Visit 4 last observation carried forward.
| System organ class | SADR | Patients | |
|---|---|---|---|
| Preferred term | n | n | % |
| Any SADR | 31 | 20 | 3.6 |
| Ear and labyrinth disorders: | 2 | 1 | 0.2 |
| – Hypoacusis | 1 | 1 | 0.2 |
| – Tinnitus | 1 | 1 | 0.2 |
| Gastrointestinal disorders: | 3 | 2 | 0.4 |
| – Abdominal pain | 1 | 1 | 0.2 |
| – Oral mucosal blistering | 1 | 1 | 0.2 |
| – Vomiting | 1 | 1 | 0.2 |
| General disorders and administration site conditions: | 4 | 4 | 0.7 |
| – Feeling abnormal | 1 | 1 | 0.2 |
| – Injection site erythema | 1 | 1 | 0.2 |
| – Injection site rash | 1 | 1 | 0.2 |
| – Pyrexia | 1 | 1 | 0.2 |
| Immune system disorders: | 1 | 1 | 0.2 |
| – Hypersensitivity | 1 | 1 | 0.2 |
| Infections and infestations: | 3 | 2 | 0.4 |
| – Erysipelas | 1 | 1 | 0.2 |
| – Lymphadenitis bacterial | 2 | 1 | 0.2 |
| Investigations: | 4 | 2 | 0.4 |
| – Alanine aminotransferase increased | 1 | 1 | 0.2 |
| – Aspartate aminotransferase increased | 1 | 1 | 0.2 |
| – Gamma-glutamyltransferase increased | 1 | 1 | 0.2 |
| – White blood cell count decreased | 1 | 1 | 0.2 |
| Musculoskeletal and connective tissue disorders: | 2 | 2 | 0.4 |
| – Morphea | 1 | 1 | 0.2 |
| – Pain in extremity | 1 | 1 | 0.2 |
| Neoplasms benign, malignant and unspecified (including cysts and polyps): | 1 | 1 | 0.2 |
| – Chronic lymphocytic leukemia | 1 | 1 | 0.2 |
| Nervous system disorders: | 3 | 3 | 0.5 |
| – Dysgeusia | 1 | 1 | 0.2 |
| – Guillain–Barré syndrome | 1 | 1 | 0.2 |
| – Headache | 1 | 1 | 0.2 |
| Skin and subcutaneous tissue disorders: | 6 | 6 | 1.1 |
| – Dermatitis | 1 | 1 | 0.2 |
| – Dermatitis allergic | 1 | 1 | 0.2 |
| – Dermatitis atopic | 1 | 1 | 0.2 |
| – Skin ulcer | 2 | 2 | 0.4 |
| – Toxic skin eruption | 1 | 1 | 0.2 |
| Surgical and medical procedures: | 1 | 1 | 0.2 |
| – Lymphadenectomy | 1 | 1 | 0.2 |
| Vascular disorders | 1 | 1 | 0.2 |
| – Hypertension | 1 | 1 | 0.2 |
SADR: Serious adverse drug reaction.
There is no published literature on clinical effectiveness and patient-reported outcomes in patients with ankylosing spondylitis and psoriatic arthritis treated with adalimumab in central and eastern Europe.
This multicenter, prospective, single-arm, observational study evaluated long-term clinical outcomes of adalimumab therapy in routine clinical practice at sites in Hungary, Romania, Slovakia, Czech Republic, Estonia and Ukraine.
Out of 555 evaluable patients, 403 had ankylosing spondylitis and 151 had psoriatic arthritis. Patients received adalimumab 40 mg subcutaneously every 2 weeks and were followed for 12 months.
At study end, 319 patients (76.1%) with axial symptoms and 66 patients (83.5%) with peripheral symptoms achieved a clinical response, and 33.6% of patients with axial symptoms and 13.9% of patients with peripheral symptoms achieved clinical remission, according to predefined criteria.
Adalimumab had sustained effectiveness on extra-articular manifestations and improved patients’ physical function and working ability.
No new clinical concerns were identified with regard to type and incidence of adverse drug reactions.
The long-term effectiveness of adalimumab observed in the current study is consistent with other reports of adalimumab in routine clinical practice.
Acknowledgements
The authors would like to thank all patients, study nurses and investigators for their contribution to the study. We would also like to thank Maja Hojnik (AbbVie, GMA) for her support in protocol development.
Financial & competing interests disclosure
The design, study conduct and financial support for the clinical trial were provided by AbbVie. AbbVie participated in the interpretation of data, drafting, review and approval of the manuscript. S Szántó has served as a consultant for Abbott Laboratories, AbbVie, EGIS, MSD, Pfizer, Roche and UCB; has received research funding from AbbVie, MSD, Pfizer, and UCB; and has received speaker fees from Abbott Laboratories, AbbVie, Berlin Chemie, EGIS, MSD, Pfizer, Roche, UCB and Valeant Pharma. G Poór has served as a consultant for Abbott Laboratories, AbbVie, Amgen, MSD, Pfizer, Roche and UCB; has received research funding from Abbott Laboratories, AbbVie; and has received speaker fees from Abbott Laboratories, AbbVie, Amgen, MSD, Pfizer, Roche and UCB. D Opriş has served as a consultant for AbbVie, MSD, Teva, UCB; and has received speaker fees from BMS, Eli Lilly, MSD, Pfizer, Roche, Sanofi, Teva and UCB. O Iaremenko has served as a consultant to AbbVie, DILEO, MSD, Roche and Pfizer; and has received speaker fees from AbbVie, DILEO, MSD and Roche. L Procházková has served as a consultant for Abbott Laboratories, AbbVie and Pfizer; and has received speaker fees from Abbott Laboratories, AbbVie, MSD, Pfizer, Roche and UCB. R Kuuse has received speaker fees from AbbVie, MSD, Roche and Pfizer. O Nagy and V Chernyshov are employees of AbbVie and may own AbbVie stock or stock options. P Géher has served as a consultant for Abbott Laboratories, AbbVie, EGIS, MSD, Roche, UCB and Wyeth; has received research funding from Abbott Laboratories, MSD, UCB and Wyeth; and has received speaker fees from Abbott Laboratories, AbbVie, Berlin Chemie, EGIS, MSD, Roche, UCB and Wyeth. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Kerry Dechant of Content Ed Net (Madrid, Spain) provided medical writing and editing services in the development of this manuscript, which was funded by AbbVie.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
References
Papers of special note have been highlighted as: •• of considerable interest
1.
Daikh DI, Chen PP. Advances in managing ankylosing spondylitis. F1000Prime Rep. 6, 78 (2014).
2.
Sritheran D, Leung YY. Making the next steps in psoriatic arthritis management: current status and future directions. Ther. Adv. Musculoskelet. Dis. 7(5), 173–186 (2015).
3.
van der Heijde D, Kivitz A, Schiff MH et al. Efficacy and safety of adalimumab in patients with ankylosing spondylitis: results of a multicenter, randomized, double-blind, placebo-controlled trial. Arthritis Rheum. 54(7), 2136–2146 (2006).
4.
Mease PJ, Gladman DD, Ritchlin CT et al. Adalimumab for the treatment of patients with moderately to severely active psoriatic arthritis: results of a double-blind, randomized, placebo-controlled trial. Arthritis Rheum. 52(10), 3279–3289 (2005).
5.
Rudwaleit M, Van den Bosch F, Kron M, Kary S, Kupper H. Effectiveness and safety of adalimumab in patients with ankylosing spondylitis or psoriatic arthritis and history of anti-tumor necrosis factor therapy. Arthritis Res. Ther. 12(3), R117 (2010).
6.
Wang H, Zuo D, Sun M, Hua Y, Cai Z. Randomized, placebo controlled and double-blind trials of efficacy and safety of adalimumab for treating ankylosing spondylitis: a meta-analysis. Int. J. Rheum. Dis. 17(2), 142–148 (2014).
7.
van der Heijde D, Breban M, Halter D et al. Maintenance of improvement in spinal mobility, physical function and quality of life in patients with ankylosing spondylitis after 5 years in a clinical trial of adalimumab. Rheumatology (Oxford) 54(7), 1210–1219 (2015).
•• Sustained clinical and functional benefit with adalimumab in patients with ankylosing spondylitis.
8.
Mease PJ, Ory P, Sharp JT et al. Adalimumab for long-term treatment of psoriatic arthritis: 2-year data from the Adalimumab Effectiveness in Psoriatic Arthritis Trial (ADEPT). Ann. Rheum. Dis. 68(5), 702–709 (2009).
•• Sustained clinical and functional benefit with adalimumab in patients with psoriatic arthritis.
9.
van der Linden S, Valkenburg HA, Cats A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum. 27(4), 361–368 (1984).
10.
Moll JM, Wright V. Psoriatic arthritis. Semin. Arthritis Rheum. 3, 55–78 (1973).
11.
Taylor W, Gladman D, Helliwell P et al. Classification Criteria for Psoriatic Arthritis. Development of new criteria from a large international study. Arthritis Rheum. 54, 2665–2673 (2006).
12.
Humira. Summary of Product Characteristics. www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000481/WC500050870.pdf
13.
Lukas C, Landewé R, Sieper J et al. Development of an ASAS-endorsed disease activity score (ASDAS) in patients with ankylosing spondylitis. Ann. Rheum. Dis. 68(1), 18–24 (2009).
14.
van der Heijde D, Lie E, Kvien TK et al. ASDAS, a highly discriminatory ASAS-endorsed disease activity score in patients with ankylosing spondylitis. Ann. Rheum. Dis. 68(12), 1811–1818 (2009).
15.
Garrett S, Jenkinson T, Kennedy LG, Whitelock H, Gaisford P, Calin A. A new approach to defining disease status in ankylosing spondylitis: the Bath Ankylosing Spondylitis Disease Activity. Index J. Rheumatol. 21, 2286–2291 (1994).
16.
Prevoo ML, van ‘t Hof MA, Kuper HH, van Leeuwen MA, van de Putte LBA, van Riel PL. Modified disease activity scores that include twenty-eight-joint counts: development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum. 38, 44–48 (1995).
17.
Calin A, Garrett S, Whitelock H et al. A new approach to defining functional ability in ankylosing spondylitis: the development of the Bath Ankylosing Spondylitis Functional Index. J. Rheumatol. 21, 2281–2285 (1994).
18.
Fries JF, Spitz P, Kraines G, Holman H. Measurement of patient outcome in arthritis. Arthritis Rheum. 23, 137–145 (1980).
19.
Reilly MC, Zbrozek AS, Dukes E. The validity and reproducibility of a work productivity and activity impairment measure. Pharmacoeconomics 4(5), 353–365 (1993).
20.
Peluso R, Iervolino S, Vitiello M, Bruner V, Lupoli G, Di Minno MN. Extra-articular manifestations in psoriatic arthritis patients. Clin. Rheumatol. 34(4), 745–753 (2015).
21.
Pham T, Landewé R, van der Linden S et al. An international study on starting tumour necrosis factor-blocking agents in ankylosing spondylitis. Ann. Rheum. Dis. 65(12), 1620–1625 (2006).
22.
Boonen A, Chorus A, Miedema H et al. Employment, work disability, and work days lost in patients with ankylosing spondylitis: a cross sectional study of Dutch patients. Ann. Rheum. Dis. 60(4), 353–358 (2001).
23.
Boonen A, van der Heijde D, Landewé R et al. Work status and productivity costs due to ankylosing spondylitis: comparison of three European countries. Ann. Rheum. Dis. 61(5), 429–437 (2002).
24.
Wallenius M, Skomsvoll JF, Koldingsnes W et al. Work disability and health-related quality of life in males and females with psoriatic arthritis. Ann. Rheum. Dis. 68(5), 685–689 (2009).
25.
Verstappen SM, Watson KD, Lunt M et al. Working status in patients with rheumatoid arthritis, ankylosing spondylitis and psoriatic arthritis: results from the British Society for Rheumatology Biologics Register. Rheumatology (Oxford) 49(8), 1570–1577 (2010).
26.
Maksymowych WP, Gooch KL, Wong RL, Kupper H, van der Heijde D. Impact of age, sex, physical function, health-related quality of life, and treatment with adalimumab on work status and work productivity of patients with ankylosing spondylitis. J. Rheumatol. 37(2), 385–392 (2010).
•• Sustained improvement on work outcomes with adalimumab in patients with ankylosing spondylitis.
27.
Machado PM, Raychaudhuri SP. Disease activity measurements and monitoring in psoriatic arthritis and axial spondyloarthritis. Best Pract. Res. Clin. Rheumatol. 28(5), 711–728 (2014).
28.
Machado P, van der Heijde D. How to measure disease activity in axial spondyloarthritis? Curr. Opin. Rheumatol. 23(4), 339–345 (2011).
29.
van der Heijde D, Landewe R, Rudwaleit M et al. [OP-0166] Performance of the ankylosing spondylitis disease activity score in 1,250 ankylosing spondylitis patients treated with adalimumab. Ann. Rheum. Dis. 68(Suppl. 3), 126 (2009).
30.
Sieper J, Rudwaleit M, Baraliakos X et al. The Assessment of SpondyloArthritis international Society (ASAS) handbook: a guide to assess spondyloarthritis. Ann. Rheum. Dis. 68(Suppl. 2), ii1–ii44 (2009).
31.
Burmester GR, Matucci-Cerinic M, Mariette X et al. Safety and effectiveness of adalimumab in patients with rheumatoid arthritis over 5 years of therapy in a Phase 3b and subsequent postmarketing observational study. Arthritis Res. Ther. 16(1), R24 (2014).
•• Large observational study (∼3400 patients) demonstrates long-term effectiveness and tolerability of adalimumab in routine clinical practice.
32.
Menter A, Thaçi D, Papp KA et al. Five-year analysis from the ESPRIT 10-year postmarketing surveillance registry of adalimumab treatment for moderate to severe psoriasis. J. Am. Acad. Dermatol. 73(3), 410.e6–419.e6 (2015).
•• Large observational study (∼6000 patients) demonstrates long-term effectiveness and tolerability of adalimumab in routine clinical practice.
Information & Authors
Information
Published In
Copyright
© Future Medicine Ltd.
History
Published online: 15 July 2016
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Improved clinical, functional and work outcomes in spondyloarthritides during real-life adalimumab treatment in central–eastern Europe. (2016) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0020
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Anna M. Sukhanova, Mariam A. Gilavian, Elizaveta V. Melnik, Evgenia V. Shikh, Alexey E. Petukhov, Vladimir I. Gegechkori, Sergey P. Dementev, Alexander M. Vlasov, Galina V. Ramenskaya, An Overview of Adalimumab Therapy for Ankylosing Spondylitis, Current Rheumatology Reviews, 10.2174/0115733971289295240223095751, 20, 5, (501-513), (2024).
- Mary Lucy Marques, Alessia Alunno, Annelies Boonen, Marieke M ter Wee, Louise Falzon, Sofia Ramiro, Polina Putrik, Methodological aspects of design, analysis and reporting of studies with work participation as an outcome domain in patients with inflammatory arthritis: results of two systematic literature reviews informing EULAR points to consider, RMD Open, 10.1136/rmdopen-2020-001522, 7, 1, (e001522), (2021).
- Liudan Tu, Ya Xie, Zetao Liao, Yutong Jiang, Qing Lv, Shuangyan Cao, Qiujing Wei, Jieruo Gu, Cost of Illness, Quality of Life, and Work Outcomes in Active Ankylosing Spondylitis Patients Treated With Adalimumab in China, Frontiers in Public Health, 10.3389/fpubh.2020.602334, 8, (2020).
- Hidemi Nakagawa, Yoshiya Tanaka, Shigetoshi Sano, Hideto Kameda, Atsuo Taniguchi, Tomoko Kashiwagi, Takeshi Kawaberi, Junko Kimura, Akimichi Morita, Real-World Postmarketing Study of the Impact of Adalimumab Treatment on Work Productivity and Activity Impairment in Patients with Psoriatic Arthritis, Advances in Therapy, 10.1007/s12325-018-0866-y, 36, 3, (691-707), (2019).