Comparative risk of hip fractures in elderly nursing home patients with depression using paroxetine and other selective serotonin reuptake inhibitors
Abstract
Aim: To evaluate comparative safety of paroxetine and other selective serotonin reuptake inhibitors (SSRIs) for the risk of hip fractures. Patients & methods: A propensity score-matched retrospective cohort study was conducted using 2007–2010 Minimum Data Set linked Medicare data. Robust Cox proportional hazards model was used to evaluate the risk of hip fractures in depressed elderly nursing home residents. Results: Cox analysis did not find any significant difference in the risk of hip fractures for the paroxetine users (hazard ratio: 1.09; 95% CI: 0.91–1.32) when compared with other SSRIs. Results from the sensitivity analysis supported the main findings. Conclusion: There was no differential risk of hip fractures between paroxetine and other SSRIs. Future studies are needed to evaluate other anticholinergic effects of paroxetine.
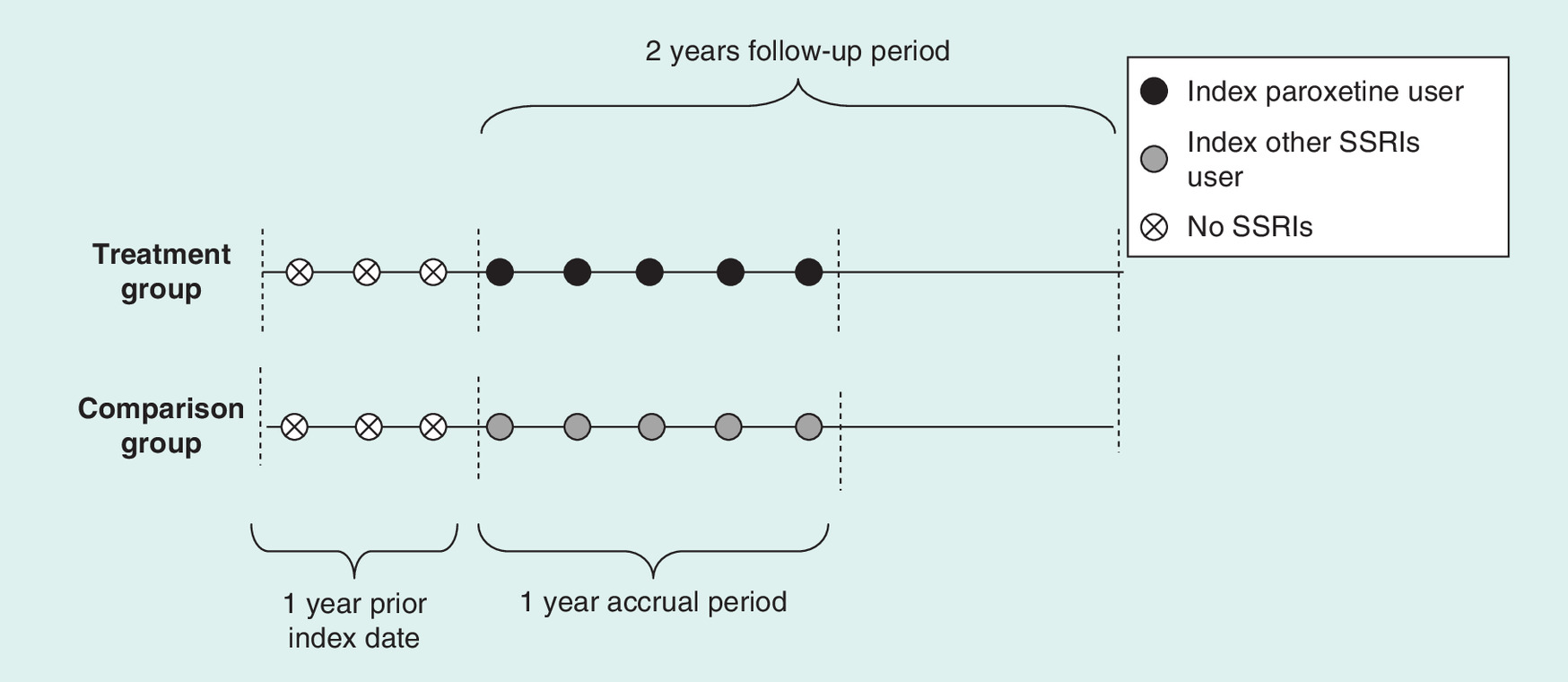
Figure 1. Cohort construction.
SSRI: Selective serotonin reuptake inhibitor.
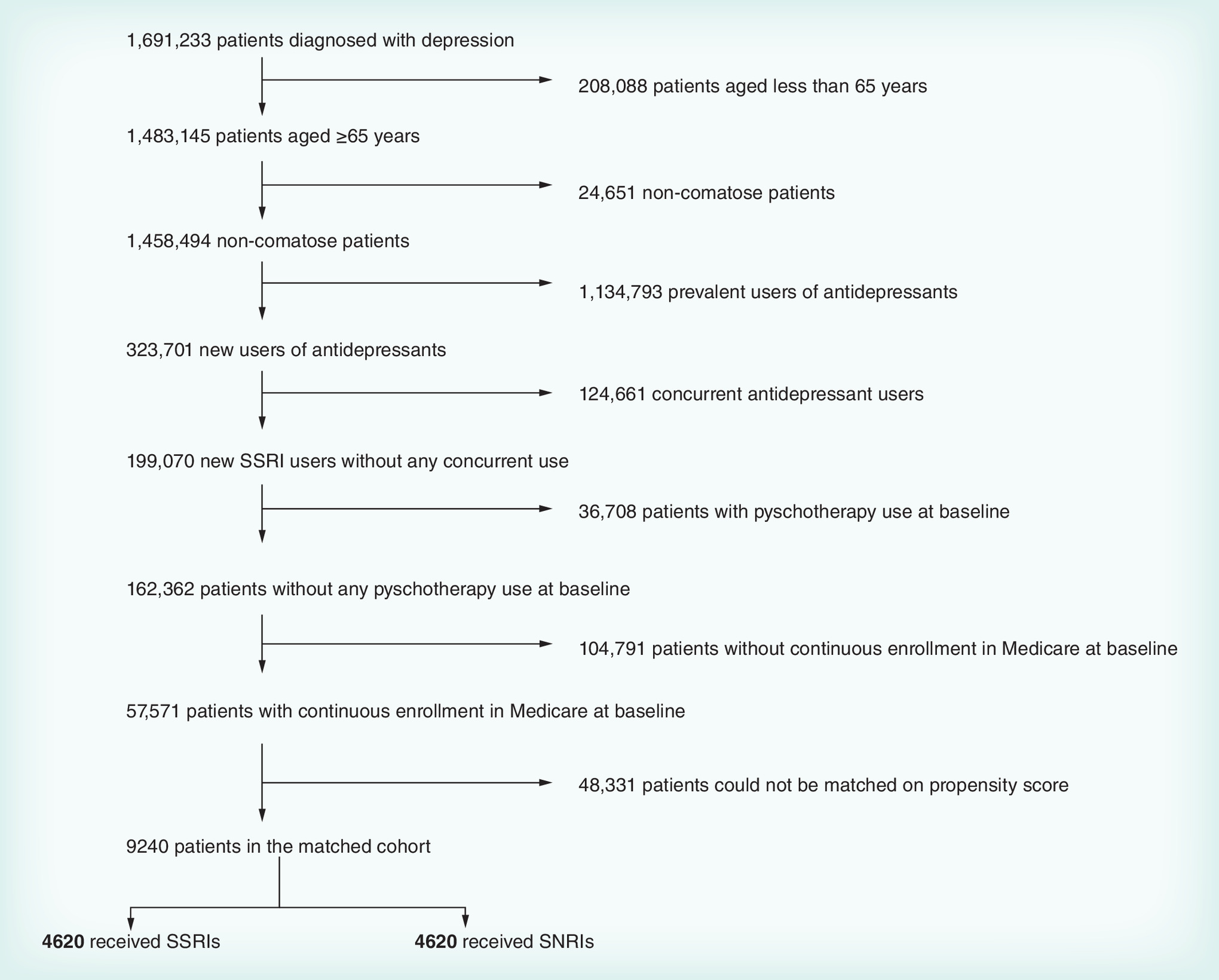
Figure 2. Identification of elderly patients with depression using paroxetine and other selective serotonin reuptake inhibitors.
SNRI: Serotonin–norepinephrine reuptake inhibitor; SSRI: Selective serotonin reuptake inhibitor.
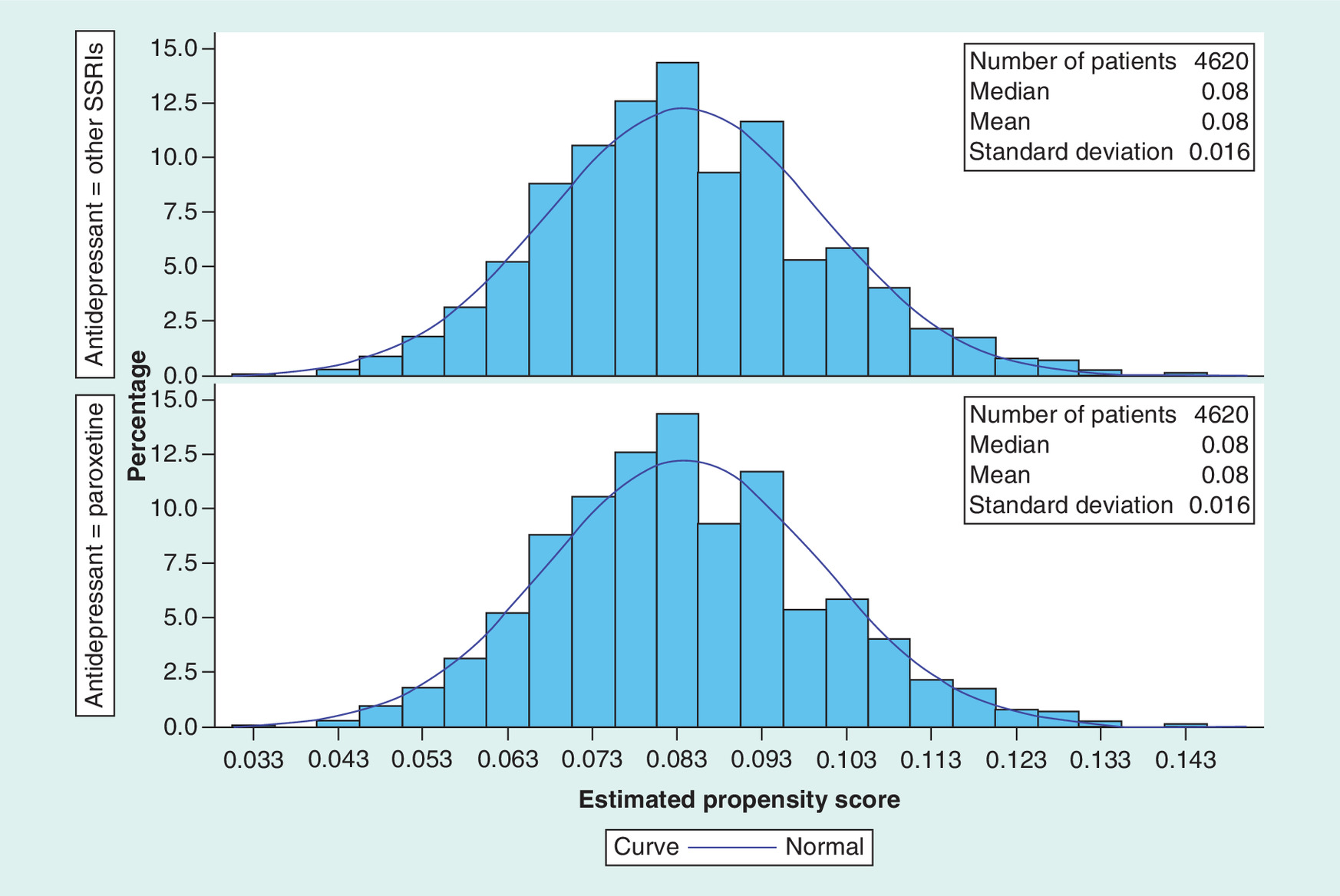
Figure 3. Distribution of propensity scores among the users of paroxetine and other selective serotonin reuptake inhibitors.
SSRI: Selective serotonin reuptake inhibitor.
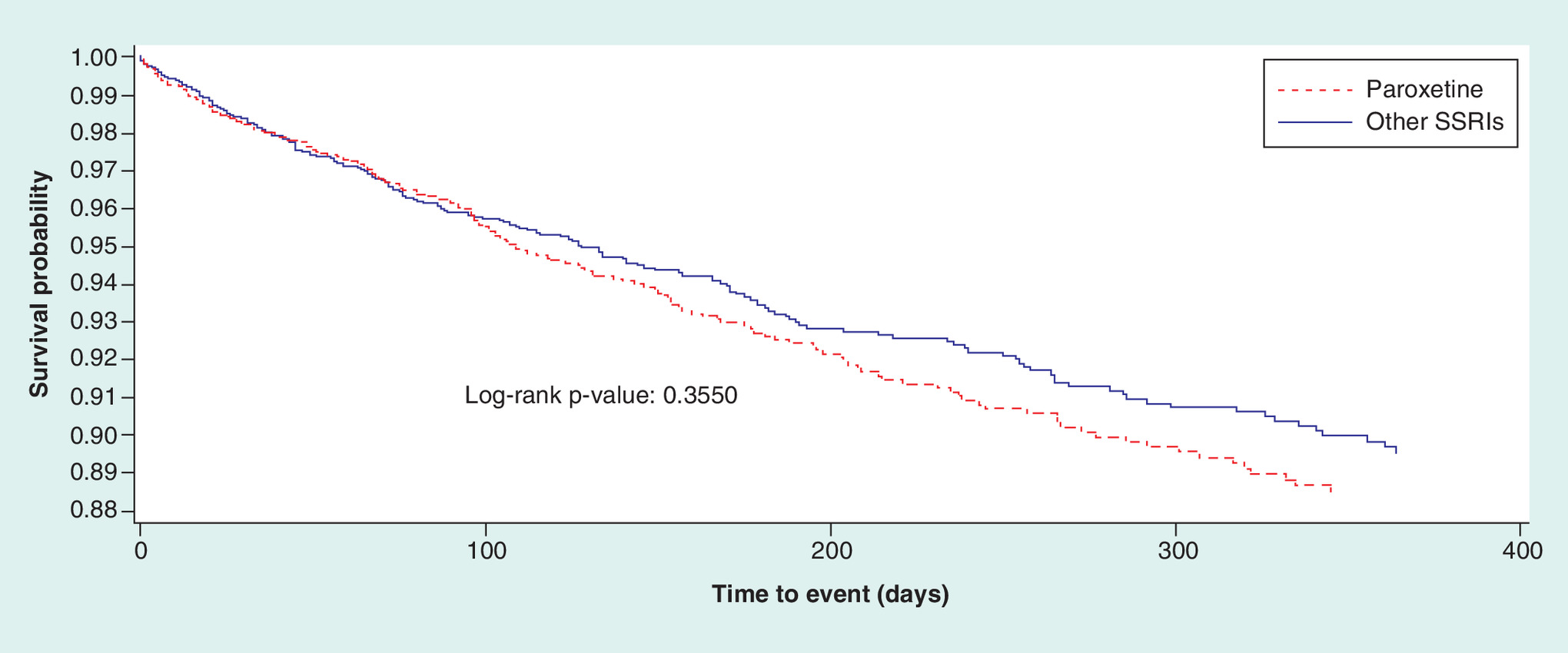
Figure 4. Kaplan–Meier curve for the risk of hip fracture for users of paroxetine and other selective serotonin reuptake inhibitors.
SSRI: Selective serotonin reuptake inhibitor.
First draft submitted: 5 February 2016; Accepted for publication: 13 May 2016; Published online: 18 July 2016
Falls and fractures among elderly people constitute a major public health concern with an estimated cost of US$19 billion [1]. Falls are the leading cause of accidental death and the seventh leading cause of death in persons more than 65 years of age [2]. More than 90% of hip fractures in elderly are caused by falls which can cause severe health problems including reduced quality of life and premature death [3]. Prevalence of hip fractures is estimated to be around 36–44% in nursing home residents [4,5]. Incidence of hip fractures is much higher in elderly nursing home residents than in community-dwelling elderly. Nursing home residents are at two-times higher risk of hip fractures than community-dwelling elderly patients [6–8]. Hip fractures are the major cause of hospitalization [9], morbidity, mortality and lack of ability to walk in nursing home patients [10,11,12].
Depression is a significant risk factor for hip fractures [13,14]. Selective serotonin reuptake inhibitors (SSRIs) are the first-line agent for the treatment of depression in older patients. These include paroxetine, escitalopram, fluoxetine and sertraline as the drugs of choice [15]. Various studies indicate that the use of SSRIs is associated with lower bone mineral density [16,17] and increased risk of hip and other fractures [18–20]. Various meta-analyses have examined association between the use of SSRIs and risk of fractures. Results from these meta-analyses indicate that patients getting SSRIs have 1.64–2.76 times higher risk of hip fractures than the others [18,20].
Previous studies have consistently found that anticholinergic medications are significantly associated with risk of hip fractures [21,22]. As per the past literature, paroxetine has higher affinity for muscarinic cholinergic receptors than other SSRIs [23,24]. Owen et al. found that the muscarinic binding properties of paroxetine were similar to desipramine but much lower than amitriptyline and substantially higher than sertraline [23]. Thus, the propensity of anticholinergic side effects is expected to be higher in paroxetine than other SSRIs. Goodnick et al. reported that all SSRIs, except paroxetine are devoid of anticholinergic properties [25]. A recent review concluded that paroxetine is a muscarinic antagonist and has less favorable tolerability profile than escitalopram [24]. The 2015 American Geriatrics Society Updated Beers Criteria classifies paroxetine as a strong anticholinergic antidepressant and potentially inappropriate for use in elderly patients [26]. The Anticholinergic Drug Scale (ADS) also classifies paroxetine as a level 2 anticholinergic agent when compared with other SSRIs [27]. The strong anticholinergic nature of paroxetine could lead to higher risk of hip fractures than the other SSRIs.
Paroxetine, although considered potentially inappropriate, is commonly used in depressed elderly patients [28–30]. However, limited comparitive data exist regarding the risk of hip fractures in elderly nursing home patients with depression who are prescribed paroxetine versus other SSRIs. In 1998, Lapane and colleagues evaluated risk of femur fractures with the use of SSRIs and tricyclic antidepressants. Their results show an increased risk of femur fractures with the use of paroxetine [31]. Recently, Vestergaard et al. conducted a case–control study in Danish population to examine risk of fractures among users of various antidepressants. They did not find any association between paroxetine use and risk of fractures [32]. However, more research is needed to evaluate the risk of hip fractures in elderly residents with cognitive issues such as depression, especially among those who reside in nursing homes, a setting with highly vulnerable population. This research is designed to evaluate the comparative risk of paroxetine and other SSRIs for hip fractures due to differential anticholinergic effects of antidepressants in elderly patients. The study findings can help to optimize antidepressant use by increasing the use of low-level anticholinergic antidepressants in depressed elderly nursing home residents. This research will test the hypothesis that elderly with depression receiving paroxetine are at a greater risk for hip fractures due to the anticholinergic effect than users of other SSRIs.
Patients & methods
Data source
The current study used 2007–2010 Minimum Data Set linked Medicare data files from all the states in the US to examine the comparative safety of paroxetine versus other SSRIs for the risk of hip fractures in a cohort of depressed elderly nursing home patients. The Medicare data including Medicare Provider Analysis and Review (MEDPAR) file (part A), carrier file (part B), prescription claims file (part D), Minimum Data Set (MDS) and master beneficiary summary file (MBSF) chronic condition segments were used in this research. The chronic condition (CC) segments of the MBSF contain information regarding the presence of 27 common or chronic conditions using inpatient and outpatient claims-based algorithms [33,34]. The cohort included Medicare beneficiaries with depression based on the MBSF CC segments and those with MDS assessments for 2007–2010. This study was approved by the University of Houston Committee for the Protection of Human Subjects under the exempt category.
Study design & sample
The present study used retrospective cohort design matched on propensity score to examine the risk of hip fractures associated with the use of paroxetine versus other SSRIs in elderly nursing home patients with depression. Development of study cohort is outlined in Figure 1. Index antidepressant use was defined as the first prescription of antidepressant after at least 1 year without any prescription fill date for any of the antidepressant medications. Patients were included in the study cohort if they: had nursing home stay anytime during the study period, were 65 years and older; received a depression diagnosis during the 1-year baseline period, initiated SSRIs between 1 January 2008 and 31 December 2009 and had continuous coverage for Medicare part A, B and D; and no health maintenance organization (HMO) during the 1-year baseline period. Patients with HMO coverage during the study period were excluded because predefined chronic condition indicators were only obtained from the claims files of fee-for-service beneficiaries and not from managed care organizations [35,36].
Exposures & outcome definitions
Exposure to paroxetine and other SSRIs was the primary exposure variable in this study. Use of paroxetine and other SSRIs was measured using Medicare part D claims data. Other SSRI users included elderly who were prescribed sertraline, citalopram, fluoxetine, fluvoxamine or citalopram. The National Drug Codes in the part D file were used to identify exposure to paroxetine and other SSRIs [37]. Time to hip fractures was the primary outcome variable of this study. It was measured using the CC indicator for hip fractures in the MBSF CC segments. The maximum follow-up period was 1 year. Study subjects were censored if they reached the end of the follow-up period; switched to a different antidepressant class or switched from paroxetine to other SSRIs or vice versa, had a gap of more than 15 days in the use of index antidepressant [38–40] or died, whichever occurred earlier.
Cohort matching
Observational studies provide treatment estimates in real-world settings. However, selection bias is a common problem in these studies due to nonrandomization of patients to different treatment groups [41]. Lack of randomization leads to pretreatment differences rather than actual treatment effects in observational studies [42]. Propensity scoring is a common technique to control for selection bias in observational studies [43,44]. This technique was proposed by Rosenbaum and Rubin in 1983 [45], and is the conditional probability of assignment to a particular treatment given a vector of observed covariates [46]. Propensity score matching is commonly used to achieve balance between the two groups such that the matched groups differ only on treatment assignment and thereby suitable for the estimation of treatment effect. A large number of covariates were used for the calculation of propensity scores based on previously published literature, expert opinions of experienced clinicians and variable selection on the basis of their association with treatment and outcome [47–50]. These covariates included sociodemographic characteristics such as age, gender and race and clinical characteristics such as co-medications and illness history during the 1-year baseline period. Hip fracture at baseline was used as one of the covariates for the calculation of propensity scores. All the covariates used in this study for the calculation of propensity scores are listed in Table 1.
Propensity scores were calculated for each individual as a function of baseline covariates using logistic regression model. Nursing home patients taking paroxetine were matched with nursing home patients taking other SSRIs using GREEDY 5→1 matching technique. This technique matches cases to controls on the first 5 digits of the propensity score. Those who remain unmatched are then matched on 4 digits of the propensity score. This process is repeated until the subjects in both the treatment groups are matched on the 1 digit of the propensity score. A control is selected at random if more than one matched control is found for a case. The GREEDY 5→1 matching technique reduces matched-pair bias caused by incomplete and inexact matching [51].
Statistical analysis
The differences between the two groups were examined using ϰ2 test for categorical variables and t-test for continuous variables, before and after matching. Survival analysis was conducted using matched cohort of paroxetine and other SSRI users to evaluate the risk of hip fractures. The Cox proportional-hazard model was utilized to evaluate the risk of hip fractures associated with paroxetine using other SSRIs as the reference category. An ID option of PROC PHREG in SAS 9.1 was used to run Robust Cox regression model [52]. Conventional Cox models assume independence of observations whereas the robust Cox regression model uses robust sandwich estimator to account for the clustering within matched pairs [53]. This model has been found to yield hazard ratios with minimal bias when compared with other propensity score-matched Cox models [54,55].
The Cox proportional-hazard model is based on proportional hazards (PH) assumption. This assumption was checked using the interaction term between SSRIs treatment and log of time to hip fractures. Additionally, Schoenfeld test was conducted to confirm the PH assumption. The PH assumption was met based on the diagnostic tests performed, thus robust Cox regression was performed to estimate the risk of hip fractures across the two treatment groups. An a priori level of 0.05 was used to check the statistical significance in this study.
Sensitivity analysis
Sensitivity analysis was conducted to confirm the robustness of the study findings. In the sensitivity analysis, patients were excluded if they did not have at least one MDS assessment at baseline. Both MDS assessment and chronic condition indicator was used to ascertain diagnosis of hip fractures during the 1-year follow-up.
Results
Patient selection & matching
The process used for the identification of the elderly patients with depression who initiated treatment with paroxetine or other SSRIs is presented in Figure 2. Analysis of 2007–2010 MDS linked Medicare data yielded 57,571 new users of SSRIs between January 2008 and December 2009 after applying inclusion and exclusion criteria. Out of these, 4620 (8.02%) received paroxetine and 52,951 received other SSRIs (91.98%). Results from the propensity score matching revealed 4620 patients in each of the two treatment groups. Table 1 reports differences in baseline characteristics between paroxetine and other SSRIs before and after matching. After matching, both the treatment groups were similar in terms of distribution of the baseline characteristics and fairly comparable. Figure 3 presents distribution of propensity scores after matching. This figure indicates a fair balance in the majority of the pretreatment characteristics between the two treatment groups.
Risk of hip fractures
A total of 430 cases of hip fractures were observed in the matched cohort during the follow-up period. Out of these, 213 (4.6%) cases were in paroxetine group and 217 (4.7%) were in other SSRIs group. Figure 4 presents risk of hip fracture among elderly patients with depression who used paroxetine or other SSRI antidepressants. The graph demonstrates that there was no difference in the risk of hip fracture between the two treatment groups. The results from the Schoenfeld test indicated that the proportional hazards assumption was met (p = 0.81). Table 2 presents results from the robust Cox proportional hazard model for the risk of hip fractures between users of paroxetine and other SSRIs. The robust Cox proportional hazard model did not find any significant difference in risk of hip fractures between paroxetine users (hazard ratio [HR]: 1.09; 95% CI: 0.91–1.32) when compared with the other SSRI users.
Sensitivity analysis
Results of the sensitivity analysis were consistent with the findings of the main study (Table 2). The sensitivity analysis showed no difference in the risk of hip fractures based on MDS criterion between patients who initiated treatment with paroxetine (HR: 1.19; 95% CI: 0.91–1.56) and those who initiated treatment with other SSRIs.
Discussion
Past literature indicates strong association between the use of SSRIs and risk of fractures due to antidepressant's affinity for serotonin [18,20]. Paroxetine has higher serotonergic potential than other SSRIs which can lead to higher risk of hip fractures [19]. Additionally, paroxetine is a strong anticholinergic and thus, might carry a higher risk of hip fractures than other SSRIs. However, no previous study has directly compared the safety of paroxetine with other SSRIs for the risk of hip fractures in depressed elderly nursing home residents. The current propensity score–matched retrospective cohort study indicates that paroxetine does not differ significantly from other SSRIs regarding the risk of hip fractures. Vestergaard et al. also did not find any significant relationship between paroxetine use and risk of fractures based on a case–control design [32].
The pharmacological differences in paroxetine and other SSRIs at the receptor level could lead to a differential risk of hip fractures. However, results from the present study suggest that pharmacological differences between paroxetine and other SSRIs do not translate into clinically significant difference for the risk of hip fractures in elderly nursing home residents with depression. The study findings do not indicate absence of risk of hip fractures with the use of SSRIs. In fact, these findings suggests that paroxetine and other SSRIs carry similar risk for hip fractures. Future studies are needed to better understand the similarity in the safety profile of paroxetine when compared with other SSRIs, in spite of paroxetine having strong anticholinergic properties and strong affinity for serotonin receptors.
Although paroxetine and other SSRIs are similar for the risk of hip fractures, these newer antidepressant agents are not same. Therefore, the prescribers need to weigh the risk–benefit ratio along with patient characteristics such as age, gender, physical conditions, illness and medication history when prescribing these antidepressants to the more vulnerable population such as elderly patients residing in nursing homes. Previous research indicates frequent use of paroxetine in nursing homes for the treatment of depression in elderly patients [28–30]. In the present study of the new SSRI users, around 8% of the patients initiated treatment with paroxetine. With an aging population and concerns of inappropriate medication use, there is a pressing need to optimize medication use and pharmaceutical care of elderly patients residing in nursing homes.
The present study had several strengths. Use of MDS-linked Medicare claims data provided actual practice data involving large sample size and long follow-up period. Prescription claims such as Medicare part D claims are valid and reliable sources for gathering medication-related information [56,57]. Using new-user cohorts for paroxetine and other SSRIs helped to minimize prevalence bias. Class-specific analyses using propensity score matching technique helped to control for the indication and selection bias. However, this study has some limitations. The diseases and outcome measurements were based on diagnostic data in medical claims. Exposure to SSRIs was ascertained using pharmacy claims. The claims capture only dispensing data and not the actual use by patients. Central anticholinergic effects may be dose-dependent and may involve selective muscarinic receptor antagonism in the central nervous system. However, doses of paroxetine, other SSRIs and co-medications were not accounted in the present study as dose information is not captured well in claims databases. Also, drug-related anticholinergic burden was not accounted. However, other anticholinergic drugs used at baseline were included as covariates in the calculation of propensity scores. The present study used Medicare claims, which is secondary data and thus has limitations due to miscoding and undercoding [58]. Propensity score–matched cohort was used to compare the risk of hip fractures between the two treatment groups. Propensity scores control for observed confounding due to measured confounders. There is a chance for unobserved confounding due to unmeasured confounders in the present study. However, sensitivity analysis was conducted and it supported the study findings. Lastly, this study might have limited generalizability as the study population was limited to elderly nursing home residents. Future studies need to replicate the study findings in other settings.
Conclusion
This retrospective cohort study evaluated comparative safety of paroxetine and other SSRIs in elderly nursing home residents with depression; the study did not find any statistically significant difference in the risk of hip fractures between the two treatment groups. The findings were consistent in the sensitivity analysis using a different cohort definition. Future studies are needed to evaluate other anticholinergic effects of paroxetine to optimize pharmaceutical care of elderly patients residing in nursing homes.
Future perspective
Evidence-based medicine emphasizes on scientific evidence along with clinician expertise and patient preferences. The comparative evaluation of safety and effectiveness of new and existing treatments is essential to establish strong empirical evidence base for an informed decision-making. The results of the present study revealed that use of paroxetine is not associated with increased risk of hip fractures when compared with the use of other SSRIs in depressed elderly nursing home patients. However, future studies are needed to evaluate other anticholinergic effects of paroxetine. The stewardship for such safety research lies with academia as pharmaceutical industry traditionally focuses on comparitive effectiveness once the drug is approved by regulatory agencies. With widespread use of approved agents in different populations and indications, there is a constant need to evaluate the safety of medications. The pharmacoepidemiological studies provide real world data to evaluate comparative safety and effectiveness. The concerns of bias are limited for safety studies when compared to effectiveness studies. Therefore, comparative safety research provides the needed balance to optimize medication use in vulnerable populations.
| Characteristics | Unmatched cohort (n = 57,571) | Matched cohort (n = 9240) | ||||
|---|---|---|---|---|---|---|
| Paroxetine users (n = 4620; %) | Other SSRI users (n = 52,951; %) | p-value | Paroxetine users (n = 4620; %) | Other SSRI users (n = 4620; %) | p-value | |
| Gender: | 0.35 | 0.21 | ||||
| – Female | 67.8 | 67.1 | 67.8 | 66.6 | ||
| – Male | 32.2 | 32.9 | 32.2 | 33.4 | ||
| Age in years: | 0.95 | 0.33 | ||||
| – 65–84 | 56.1 | 56.1 | 56.1 | 57.1 | ||
| – 85 and above | 43.9 | 43.9 | 43.9 | 42.9 | ||
| Race: | 0.08 | 0.11 | ||||
| – White | 79.0 | 77.9 | 79.0 | 77.6 | ||
| – Non-White | 21.0 | 22.1 | 21.0 | 22.4 | ||
| Medical history in past 12 months: | ||||||
| – CHF | 51.9 | 54.3 | 0.002* | 51.9 | 55.4 | 0.001* |
| – Endocarditis | 5.6 | 6.1 | 0.24 | 5.6 | 6.5 | 0.09 |
| – Ischemic heart disease | 67.2 | 68.2 | 0.14 | 67.2 | 67.9 | 0.49 |
| – Acute myocardial infarction | 9.0 | 9.9 | 0.04* | 9.0 | 9.8 | 0.18 |
| – Stroke/transient ischemic attack | 31.2 | 34.7 | <0.0001* | 31.2 | 29.1 | 0.03* |
| – Cardiac arrhythmia | 32.2 | 33.5 | 0.07 | 32.2 | 33.0 | 0.41 |
| – Circulatory disorder | 36.2 | 38.2 | 0.01* | 36.2 | 37.7 | 0.13 |
| – Thromboembolic disorder | 7.9 | 8.4 | 0.19 | 7.9 | 8.5 | 0.30 |
| – Peripheral arterial disorder | 13.7 | 14.5 | 0.13 | 13.7 | 14.4 | 0.29 |
| – Hypertension | 91.6 | 93.3 | <0.0001* | 91.6 | 92.0 | 0.54 |
| – Diabetes mellitus | 39.3 | 41.5 | 0.004* | 39.3 | 42.4 | 0.002* |
| – Hyperlipidemia | 73.4 | 74.5 | 0.09 | 73.4 | 71.6 | 0.06 |
| – Renal failure | 19.2 | 22.1 | <0.0001* | 19.2 | 27.4 | <0.0001* |
| – Other renal disease | 46.1 | 49.3 | <0.0001* | 46.1 | 48.1 | 0.06 |
| – Fall and fracture | 16.9 | 18.6 | 0.004* | 16.9 | 16.9 | 0.98 |
| – Osteoporosis | 36.3 | 36.2 | 0.71 | 36.3 | 32.3 | <0.0001* |
| – Rheumatoid arthritis and osteoarthritis | 68.4 | 71.2 | <0.0001* | 68.4 | 60.2 | <0.0001* |
| – Gout and other crystal arthropathies | 4.1 | 4.2 | 0.75 | 4.1 | 3.8 | 0.49 |
| – Back pain | 24.0 | 23.1 | 0.19 | 24.0 | 20.6 | 0.0001* |
| – Parkinson | 3.5 | 3.8 | 0.38 | 3.5 | 3.5 | 0.96 |
| – Extrapyramidal syndrome | 2.4 | 2.5 | 0.88 | 2.4 | 2.1 | 0.26 |
| – Fibromyalgia | 1.8 | 1.9 | 0.44 | 1.8 | 1.8 | 0.75 |
| Psychotic disorder: | ||||||
| – Anxiety | 12.6 | 10.8 | 0.0002* | 12.6 | 11.3 | 0.07 |
| – Mood disorder | 21.7 | 24.3 | <0.0001* | 21.7 | 21.9 | 0.80 |
| – Migraine | 0.5 | 0.5 | 0.95 | 0.5 | 0.5 | 0.88 |
| – Schizophrenia | 5.3 | 6.2 | 0.02* | 5.3 | 6.1 | 0.11 |
| – Bipolar disorder | 1.0 | 1.0 | 0.78 | 1.0 | 1.0 | 0.92 |
| – Insomnia | 2.7 | 2.6 | 0.79 | 2.7 | 2.6 | 0.75 |
| – Dementia | 37.3 | 42.5 | <0.0001* | 37.3 | 14.1 | 0.59 |
| – Other psychiatric disorders | 13.8 | 12.7 | 0.02* | 13.8 | 36.8 | 0.76 |
| – Liver disorder | 8.7 | 8.4 | 0.38 | 8.7 | 8.6 | 0.77 |
| – Gastric disorder | 50.7 | 50.8 | 0.92 | 50.7 | 41.7 | <0.0001* |
| – Ulcers | 10.5 | 11.4 | 0.08 | 10.5 | 11.1 | 0.38 |
| – Cancer | 20.6 | 20.9 | 0.58 | 20.6 | 21.2 | 0.46 |
| – Dysphagia | 8.8 | 10.8 | <0.0001* | 8.8 | 8.7 | 0.85 |
| – Anemia | 72.1 | 75.4 | <0.0001* | 72.1 | 72.0 | 0.84 |
| – Asthma | 16.2 | 15.0 | 0.03* | 16.2 | 16.8 | 0.43 |
| – Chronic obstructive pulmonary disease | 42.7 | 41.2 | 0.05 | 42.7 | 51.4 | <0.0001* |
| – Pneumonia | 15.0 | 15.7 | 0.20 | 15.0 | 17.4 | 0.002* |
| – Benign prostatic hyperplasia | 16.1 | 16.8 | 0.27 | 16.1 | 18.9 | 0.001* |
| – Hypothyroidism | 27.3 | 28.8 | 0.03* | 27.3 | 26.8 | 0.54 |
| – Cataract | 77.4 | 78.8 | 0.02* | 77.4 | 76.5 | 0.30 |
| – Glaucoma | 24.1 | 25.6 | 0.02* | 24.1 | 24.2 | 0.92 |
| – Obesity | 4.7 | 5.1 | 0.26 | 4.7 | 5.4 | 0.13 |
| – Alcohol | 3.2 | 3.3 | 0.58 | 3.2 | 3.6 | 0.25 |
| Other drugs used in past 12 months: | ||||||
| – Anti-infective agents | 71.0 | 71.5 | 0.39 | 71.0 | 70.6 | 0.68 |
| – Endocrine and metabolic drugs | 61.2 | 61.7 | 0.46 | 61.2 | 61.6 | 0.64 |
| – Cardiovascular agents | 83.4 | 85.5 | 0.0001* | 83.4 | 82.9 | 0.54 |
| – Anti-hyperlipidemic drugs | 39.6 | 42.1 | 0.0008* | 39.6 | 39.5 | 0.95 |
| – Respiratory agents | 32.2 | 31.7 | 0.46 | 32.2 | 35.1 | 0.003* |
| – Antihistamines and other cold remedies | 20.5 | 19.7 | 0.18 | 20.5 | 18.9 | 0.05 |
| – Gastrointestinal agents | 22.9 | 22.7 | 0.68 | 22.9 | 20.3 | 0.002* |
| – Genitourinary products | 12.1 | 12.3 | 0.67 | 12.1 | 11.9 | 0.70 |
| – Antianxiety agents | 4.9 | 4.2 | 0.03* | 4.9 | 4.4 | 0.30 |
| – Antipsychotics | 12.8 | 13.4 | 0.26 | 12.8 | 12.5 | 0.66 |
| – Hypnotics | 10.8 | 10.7 | 0.87 | 10.8 | 11.5 | 0.29 |
| – Stimulants/anti-obesity/anorexiants | 3.3 | 3.1 | 0.36 | 3.3 | 3.0 | 0.31 |
| – Other psychotherapeutic agents | 7.3 | 9.4 | <0.0001* | 7.3 | 7.5 | 0.84 |
| – Anticonvulsants | 13.4 | 14.2 | 0.12 | 13.4 | 14.1 | 0.32 |
| – Antiparkinsonian | 5.4 | 6.0 | 0.06 | 5.4 | 6.1 | 0.11 |
| – Analgesics and anti-inflammatories | 54.7 | 54.9 | 0.84 | 54.7 | 52.8 | 0.07 |
| – Musculoskeletal agents | 22.4 | 23.3 | 0.19 | 22.4 | 22.7 | 0.78 |
| – Nutritional products | 26.5 | 28.1 | 0.02* | 26.5 | 27.8 | 0.17 |
| – Hematological agents | 32.7 | 33.9 | 0.10 | 32.7 | 33.1 | 0.66 |
| – Topical products | 45.7 | 46.5 | 0.27 | 45.7 | 45.5 | 0.85 |
| – Central acetylcholinesterase inhibitors | 12.3 | 14.9 | <0.0001* | 12.3 | 13.4 | 0.11 |
| – Alcohol- and drug-dependence agents | 0.4 | 0.6 | 0.11 | 0.4 | 0.6 | 0.15 |
| – Antineoplastic agents | 5.5 | 5.5 | 0.97 | 5.5 | 4.8 | 0.13 |
†All medication use and diagnostic data are based on 1 year prior to the initiation of the SSRI medication.
*p-value significant at 0.05.
CHF: Congestive heart failure; SSRI: Selective serotonin reuptake inhibitor.
| Variables | Hazard ratio | 95% CI | p-value |
|---|---|---|---|
| PS matched Cox proportional hazard model | |||
| Paroxetine (n = 4620) | 1.09 | 0.91–1.32 | 0.35 |
| Other SSRIs (n = 4620) | 1.00 | Reference | |
| Sensitivity analysis | |||
| Paroxetine (n = 2084) | 1.19 | 0.91–1.56 | 0.20 |
| Other SSRIs (n = 2084) | 1.00 | Reference | |
SSRI: Selective serotonin reuptake inhibitor.
Paroxetine is a strong anticholinergic antidepressant with high serotonergic potential than other selective serotonin reuptake inhibitors (SSRIs). Thus, paroxetine can increase the risk of hip fractures compared to other SSRIs in elderly patients.
The present study used propensity score-matched retrospective cohort study design and 2007–2010 Minimum Data Set linked Medicare data to compare the risk of hip fractures in new users of paroxetine and other SSRIs.
The findings from this study reveal no differential risk of hip fractures between the two treatment groups. Results from the sensitivity analysis corroborated the main findings.
Future studies need to replicate the study findings in other clinical settings and also evaluate other anticholinergic effects of paroxetine.
Financial & competing interests disclosure
This study was supported by grants from the Agency for Healthcare Research and Quality (AHRQ) (Grant R01HS021264. Principal Investigator: RR Aparasu). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors obtained approval from the University of Houston Committee for the Protection of Human Subjects under the exempt category. This study involved use of existing de-identified databases and thus informed consent was not required.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Stevens JA, Corso PS, Finkelstein EA, Miller TR. The costs of fatal and non-fatal falls among older adults. Inj. Prev. 12(5), 290–295 (2006).
2.
Akyol AD. Falls in the elderly: what can be done? Int. Nurs. Rev. 54(2), 191–196 (2007).
3.
Hayes WC, Myers ER, Morris JN, Gerhart TN, Yett HS, Lipsitz LA. Impact near the hip dominates fracture risk in elderly nursing home residents who fall. Calcif. Tissue Int. 52(3), 192–198 (1993).
4.
Andersson G. The Burden of Musculoskeletal Diseases in the United States: Prevalence, Societal and Economic Cost. Amer Academy of Orthopaedic, IL, USA (2008).
5.
Rodondi A, Chevalley T, Rizzoli R. Prevalence of vertebral fracture in oldest old nursing home residents. Osteoporos. Int. 23(11), 2601–2606 (2012).
6.
Brennan Nee Saunders J, Johansen A, Butler J et al. Place of residence and risk of fracture in older people: a population-based study of over 65-year-olds in Cardiff. Osteoporos. Int. 14(6), 515–519 (2003).
7.
Butler M, Norton R, Lee-Joe T, Cheng A, Campbell AJ. The risks of hip fracture in older people from private homes and institutions. Age Ageing 25(5), 381–385 (1996).
8.
Norton R, Campbell AJ, Reid IR et al. Residential status and risk of hip fracture. Age Ageing 28(2), 135–139 (1999).
9.
Ronald LA, McGregor MJ, McGrail KM, Tate RB, Broemling AM. Hospitalization rates of nursing home residents and community-dwelling seniors in British Columbia. Can. J. Aging 27(1), 109–115 (2008).
10.
Bentler SE, Liu L, Obrizan M, Cook EA, Wright KB et al. The aftermath of hip fracture: discharge placement, functional status change, and mortality. Am. J. Epidemiol. 170(10), 1290–1299 (2009).
11.
Neuman MD, Silber JH, Magaziner JS, Passarella MA, Mehta S, Werner RM. Survival and functional outcomes after hip fracture among nursing home residents. JAMA Int. Med. 174(8), 1273–1280 (2014).
12.
Clayer MT, Bauze RJ. Morbidity and mortality following fractures of the femoral neck and trochanteric region: analysis of risk factors. J. Trauma 29(12), 1673–1678 (1989).
13.
Oude Voshaar RC, Banerjee S, Horan M et al. Fear of falling more important than pain and depression for functional recovery after surgery for hip fracture in older people. Psychol. Med. 36(11), 1635–1645 (2006).
14.
Guideline for the prevention of falls in older persons. American Geriatrics Society, British Geriatrics Society, and American Academy of Orthopaedic Surgeons Panel on Falls Prevention. J. Am. Geriatr. Soc. 49(5), 664–672 (2001).
15.
American Medical Directors Association. Depression in the Long-Term Care Setting (2011). www.guideline.gov/content.aspx?id=32668.
16.
Haney EM, Chan BK, Diem SJ et al. Association of low bone mineral density with selective serotonin reuptake inhibitor use by older men. Arch Intern. Med. 167(12), 1246–1251 (2007).
17.
Diem SJ, Blackwell TL, Stone KL et al. Use of antidepressants and rates of hip bone loss in older women: the study of osteoporotic fractures. Arch Intern. Med. 167(12), 1240–1245 (2007).
18.
Eom CS, Lee HK, Ye S, Park SM, Cho KH. Use of selective serotonin reuptake inhibitors and risk of fracture: a systematic review and meta-analysis. J. Bone Mineral Res. 27(5), 1186–1195 (2012).
19.
Sansone RA, Sansone LA. SSRIs: bad to the bone? Innov. Clin. Neurosci. 9(7–8), 42–47 (2012).
20.
Rabenda V, Nicolet D, Beaudart C, Bruyere O, Reginster JY. Relationship between use of antidepressants and risk of fractures: a meta-analysis. Osteoporos. Int. 24(1), 121–137 (2013).
•• Results from this large meta-analysis showed that both selective serotonin reuptake inhibitors (SSRIs) and tricyclic antidepressants are associated with a moderate and clinically significant increase in the risk of fractures of all types. Studies examining SSRIs use showed systematically higher increase in the risk of fractures of all types, nonvertebral and hip fractures than studies evaluating tricyclic antidepressant use.
21.
Wilson NM, Hilmer SN, March LM et al. Associations between drug burden index and falls in older people in residential aged care. J. Am. Geriatr. Soc. 59(5), 875–880 (2011).
22.
Aizenberg D, Sigler M, Weizman A, Barak Y. Anticholinergic burden and the risk of falls among elderly psychiatric inpatients: a 4-year case–control study. Int. Psychogeriatr. 14(3), 307–310 (2002).
23.
Owens MJ, Morgan WN, Plott SJ, Nemeroff CB. Neurotransmitter receptor and transporter binding profile of antidepressants and their metabolites. J. Pharmacol. Exp. Ther. 283(3), 1305–1322 (1997).
24.
Sanchez C, Reines EH, Montgomery SA. A comparative review of escitalopram, paroxetine, and sertraline: are they all alike? Int. Clin. Psychopharmacol. 29(4), 185–196 (2014).
•• For readers interested in the comparative effectiveness of SSRIs, this study concluded that, although escitalopram, paroxetine and sertraline belong to the SSRI antidepressant class, differences exist with respect to efficacy and tolerability. Paroxetine may have an impact on its tolerability due to its cholinergic muscarinic antagonism and potent inhibition of CYP2D6. Escitalopram has better efficacy and tolerability profiles than paroxetine and sertraline.
25.
Goodnick PJ, Goldstein BJ. Selective serotonin reuptake inhibitors in affective disorders – I. Basic pharmacology. J. Psychopharmacol. 12(3 Suppl. B), S5–S20 (1998).
26.
Fick DM, Semla TP, Beizer J et al. American Geriatrics Society 2015 updated beers criteria for potentially inappropriate medication use in older adults. J. Am. Geriatr. Soc. 63(11), 2227–2246 (2015).
• This criteria provides lists of potentially inappropriate medications to be avoided in older patients. Among antidepressants, it lists paroxetine as a drug with strong anticholinergic properties that is potentially inappropriate for use in older adults.
27.
Kersten H, Molden E, Willumsen T, Engedal K, Bruun Wyller T. Higher anticholinergic drug scale (ADS) scores are associated with peripheral but not cognitive markers of cholinergic blockade. Cross sectional data from 21 Norwegian nursing homes. Br. J. Clin. Pharmacol. 75(3), 842–849 (2013).
28.
Karkare SU, Bhattacharjee S, Kamble P, Aparasu RR. Prevalence and predictors of antidepressant prescribing in nursing home residents in the United States. Am. J. Geriatr. Pharmacother. 9(2), 109–119 (2011).
29.
Chatterjee S, Aparasu RR, Carnahan RM, Johnson ML, Chen H. Prevalence of anticholinergic medication use among elderly nursing home residents with depression. Value Health 17(3), A211 (2014).
30.
Bali V, Aparasu RR, Johnson ML, Chen H, Carnahan RM. Risk of dementia associated with the use of paroxetine among the elderly nursing home patients with depression. Value Health 17(3), A209 (2014).
31.
Lapane KL, Gambassi G, Hume A, Sgadari A, Mor V. Which antidepressants increase the risk of femur fracture in long term care. Presented at: American Geriatric Society and American Federation for Aging Research, Annual Meeting, 142 (1998).
•• Found that both tricyclic antidepressants and SSRIs were associated with a similarly increased (30–40%) risk of femur fracture. They found significant differences among the SSRIs for the risk of femur fracture. Paroxetine was associated with almost two-times risk of femur fracture whereas fluoxetine was not associated with a significant increased risk of femur fracture.
32.
Vestergaard P, Rejnmark L, Mosekilde L. Selective serotonin reuptake inhibitors and other antidepressants and risk of fracture. Calcif. Tissue Int. 82(2), 92–101 (2008).
•• The age- and gender-matched case–control study found that among SSRIs, citalopram, fluoxetine and sertraline were associated with an increase in fracture risk. Paroxetine was not associated with an increase in fracture risk. Among tricyclic antidepressants, amitriptyline and clomipramine were associated with increased fracture risk, while imipramine and nortriptyline were not. Other tricyclic antidepressants were not. The other groups of other antidepressants were not associated with fracture risk.
33.
Hanlon JT, Donohue J. Medicare part D data: a valuable tool for pharmacoepidemiology and pharmacoeconomic research. Am. J. Geriatr. Pharmacother. 8(6), 483–484 (2010).
34.
Centers for Medicare & Medicaid Services. Medicare Standard Analytical Files: Identifiable Data Files. www.cms.gov/Research-Statistics-Data.
35.
Thorpe CT, Thorpe JM, Kind AJ, Bartels CM, Everett CM, Smith MA. Receipt of monitoring of diabetes mellitus in older adults with comorbid dementia. J. Am. Geriatr. Soc. 60(4), 644–651 (2012).
36.
Schneider KM, O'Donnell BE, Dean D. Prevalence of multiple chronic conditions in the United States’ Medicare population. Health Qual. Life Outcomes 7, 82 (2009).
37.
Fung V, Brand RJ, Newhouse JP, Hsu J. Using Medicare data for comparative effectiveness research: opportunities and challenges. Am. J. Manag. Care 17(7), 489–496 (2011).
• Provides guidance regarding Medicare data for conducting comparative effectiveness research in geriatric population. It also discusses about other data sources that could be used to enhance the value of Medicare data for conducting comparative effectiveness research in geriatric patients.
38.
Cantrell CR, Eaddy MT, Shah MB, Regan TS, Sokol MC. Methods for evaluating patient adherence to antidepressant therapy: a real-world comparison of adherence and economic outcomes. Med. Care 44(4), 300–303 (2006).
39.
Cramer JA, Roy A, Burrell A et al. Medication compliance and persistence: terminology and definitions. Value Health 11(1), 44–47 (2008).
40.
Liu X, Chen Y, Faries DE. Adherence and persistence with branded antidepressants and generic SSRIs among managed care patients with major depressive disorder. Clinicoecon. Outcomes Res. 3, 63–72 (2011).
41.
Winship C, Mare RD. Models for sample selection bias. Ann. Rev. Soc. 18, 327–350 (1992).
42.
Rosenbaum PR. Discussing hidden bias in observational studies. Ann. Intern. Med. 115(11), 901–905 (1991).
43.
Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav. Res. 46(3), 399–424 (2011).
44.
Stukel TA, Fisher ES, Wennberg DE, Alter DA, Gottlieb DJ, Vermeulen MJ. Analysis of observational studies in the presence of treatment selection bias: effects of invasive cardiac management on AMI survival using propensity score and instrumental variable methods. JAMA 297(3), 278–285 (2007).
• Provides comparison of multivariable model risk adjustment, propensity score risk adjustment, propensity score matching and instrumental variable analysis for removing the effects of selection bias in observational studies.
45.
Rosenbaum PR, Rubin DB. The central role of the propensity score in observational studies for causal effects. Biometrika 70(1), 41–55 (1983).
46.
Brookhart MA, Schneeweiss S, Rothman KJ, Glynn RJ, Avorn J, Sturmer T. Variable selection for propensity score models. Am. J. Epidemiol. 163(12), 1149–1156 (2006).
47.
Aparasu RR, Chatterjee S, Mehta S, Chen H. Risk of death in dual-eligible nursing home residents using typical or atypical antipsychotic agents. Med. Care 50(11), 961–969 (2012).
48.
Chatterjee S, Chen H, Johnson ML, Aparasu RR. Risk of falls and fractures in older adults using atypical antipsychotic agents: a propensity score-adjusted, retrospective cohort study. Am. J. Geriatr. Pharmacother. 10(2), 83–94 (2012).
49.
Chatterjee S, Chen H, Johnson ML, Aparasu RR. Comparative risk of cerebrovascular adverse events in community-dwelling older adults using risperidone, olanzapine and quetiapine: a multiple propensity score-adjusted retrospective cohort study. Drugs Aging 29(10), 807–817 (2012).
50.
Aparasu RR, Chatterjee S, Chen H. Risk of hospitalization and use of first- versus second-generation antipsychotics among nursing home residents. Psychiatr. Serv. 65(6), 781–788 (2014).
51.
Parsons LS. Reducing bias in a propensity score matched-pair sample using greedy matching techniques. Presented at: Proceedings of the Twenty-sixth Annual SAS Users group international conference. April 2001. www2.sas.com/proceedings/sugi26/p214-26.pdf.
52.
SAS Institute Inc. SAS®. 9.3 Guide to Software Updates. Cary, NC: SAS Institute Inc (2011).
53.
Lin DY, Wei L-J. The robust inference for the Cox proportional hazards model. J. Am. Stat. Assoc. 84(408), 1074–1078 (1989).
54.
Austin PC. The performance of different propensity score methods for estimating marginal hazard ratios. Stat. Med. 32(16), 2837–2849 (2013).
• Compared the performance of propensity score matching, propensity score stratification, inverse probability of treatment weighting using the propensity score and covariate adjustment using the propensity score to estimate marginal hazard ratios. Researchers found that both propensity score matching and inverse probability of treatment weighting using the propensity score allow for the estimation of marginal hazard ratios with minimal bias.
55.
Gayat E, Resche-Rigon M, Mary JY, Porcher R. Propensity score applied to survival data analysis through proportional hazards models: a Monte Carlo study. Pharm. Stat. 11(3), 222–229 (2012).
56.
Tamblyn R, Lavoie G, Petrella L, Monette J. The use of prescription claims databases in pharmacoepidemiological research: the accuracy and comprehensiveness of the prescription claims database in Quebec. J. Clin. Epidemiol. 48(8), 999–1009 (1995).
57.
Kirking D, Ammann M, Harrington C. Comparison of medical records and prescription claims files in documenting prescription medication therapy. J. Pharmacoepidemiology 5, 3–16 (1996).
58.
Crocco EA, Castro K, Loewenstein DA. How late-life depression affects cognition: neural mechanisms. Curr. Psychiatry Rep. 12(1), 34–38 (2010).
Information & Authors
Information
Published In
Copyright
© Future Medicine Ltd.
History
Published online: 18 July 2016
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparative risk of hip fractures in elderly nursing home patients with depression using paroxetine and other selective serotonin reuptake inhibitors. (2016) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0009
Export citation
Select the citation format you wish to export for this article or chapter.