Cost–effectiveness analysis of empagliflozin compared with glimepiride in patients with Type 2 diabetes in China
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: The study assesses the cost–effectiveness of empagliflozin versus glimepiride in patients with Type 2 diabetes and uncontrolled by metformin alone in China, based on the EMPA-REG H2H-SU trial. Materials & methods: A calibrated version of the IQVIA Core Diabetes Model was used. Cost of complications and utility were taken from literature. The Chinese healthcare system perspective and 5% discounting rates were applied. Results: Empagliflozin+metformin provides additional quality-adjusted life-years (0.317) driven by a reduction in the number of cardiovascular and renal events, for an additional cost of $1382 (CNY9703) compared with glimepiride+metformin. Conclusion: Empagliflozin is cost-effective treatment versus glimepiride applying a threshold of $30,290 (CNY212,676).
Type 2 diabetes (T2D) is a chronic medical condition characterized by inadequate insulin production and its impaired function leading to hyperglycemia [1]. Burden of diabetes is amplified by both microvascular and macrovascular complications [1]. T2D is often associated with co-morbidities that increase the risk of cardiovascular events and mortality [2]. SGLT-2 inhibitors recently have been studied in several large cardiovascular outcome trials (CVOT) of patients with T2D and established cardiovascular disease (CVD) [3]. A meta-analysis of all CVOTs available to date, in Type 2 diabetic patients, showed that SGLT-2 inhibitors reduced the risk of major cardiovascular events by 11% (hazard ratio: 0.89; 95% CI: 0.83–0.96) [3]. These CVOTs assessed SGLT-2 inhibitors in patients with a long disease history of T2D and established CVD and so patients were at high risk of experiencing further cardiovascular events. In contrast, the EMPA-REG H2H-SU trial (NCT01167881) compared empagliflozin versus glimepiride in patients with T2D uncontrolled on metformin monotherapy and no history of established CVD, thus reflecting a population that is relatively less prone to cardiovascular complications [4]. The results of this trial showed that after 4 years, patients receiving empagliflozin experienced less cardiovascular complications versus glimepiride, initiated on top of metformin as background therapy.
According to the International Diabetes Federation (IDF) Diabetes Atlas (2019), People’s Republic of China has more than 116 million people living with diabetes, setting China at the top position for diabetes prevalence worldwide [5]. SGLT-2 inhibitors are the newest class of diabetes treatments and assessing its cost–effectiveness will support decision makers to measure the value of this therapy class compared with other antidiabetes treatments available in the Chinese market [6]. With this purpose in mind, the aim of the present work was to estimate, the lifetime cost–effectiveness of empagliflozin versus glimepiride in patients with T2D uncontrolled with metformin alone and without history of CVD in China, based on the CVOT results of the EMPA-REG H2H-SU.
Methods
Model structure
The IQVIA Core Diabetes Model (CDM) version 9.0 was used to quantify survival, cardiovascular and renal outcomes treated either with empagliflozin or glimepiride when glycemic control is not achieved with metformin alone in Chinese patients with T2D.
The CDM is a web-based computer microsimulation model that estimates the long-term health outcomes and economic consequences of interventions in patients with Type 1 diabetes and T2D. To project diabetes progression, it uses a set of 17 inter-dependent Markov submodels, and risk factor progression models, together with standard risk equations (REs) and landmark clinical data that estimate the risk of diabetes complications and adverse events [7].
To capture the cardiovascular effects observed in the trial, the CDM was calibrated in a step-wise approach (Table 1). First, the observed annual progression of risk factors (HbA1c, systolic blood pressure [SBP] and BMI) per treatment arm were programmed in the CDM for the follow-up period of the EMPA-REG H2H-SU trial (4 years). These inputs were incorporated into REs to predict the risk of diabetes complications and to define the trajectory within each Markov submodel. Several well-established REs are available in the CDM: the United Kingdom Prospective Diabetes Study (UKPDS) 68 [8], UKPDS 82 [9], Advance [10], Swedish national Diabetes Register [11,12], ARIC study [13], Fremantle [14] and PROCAM [15]. These different REs were tested and the UKPDS 82 equations were found to be the closest fit to predict the 4-year clinical outcomes of the EMPA-REG H2H-SU trial [4,8]. The second step of the calibration was an iterative adjustment process to identify the best set of relative risk (RR) adjustments needed to fine-tune the UKPDS 82 RE predictions, so that predictions would match the observed 4-year clinical outcomes of EMPA-REG H2H-SU. The outcomes used to calibrate the predictions were: primary and subsequent myocardial infarction, primary and subsequent stroke, hospitalization for angina, hospitalization for heart failure, cardiovascular death and noncardiovascular death.
| Clinical outcomes | Trial observed outcome† | CDM projected outcome after calibration† | Difference | |||
|---|---|---|---|---|---|---|
| Empagliflozin | Glimepiride | Empagliflozin | Glimepiride | Empagliflozin | Glimepiride | |
| Myocardial Infarction | 0.52 | 1.70 | 0.54 | 1.70 | -0.02 | 0 |
| Stroke | 1.05 | 0.78 | 1.07 | 0.78 | -0.02 | 0 |
| Hospitalization for unstable angina | 0.13 | 0.39 | 0.13 | 0.37 | 0 | 0.02 |
| Hospitalization for heart failure | 0.13 | 0.26 | 0.13 | 0.27 | 0 | -0.01 |
| Death from cardiovascular cause | 0.26 | 0.52 | 0.27 | 0.52 | -0.01 | 0 |
| Death from noncardiovascular cause | 1.02 | 0.80 | 1.00 | 0.80 | 0.02 | 0 |
†
Outcomes are cumulative incidence of events.
CDM: Core Diabetes Model; CV: Cardiovascular.
The outcomes of the CDM are life years (LY), quality-adjusted life years (QALY), event rate per 100 patient-years for diabetes-related complications and associated costs as well as incremental costs, incremental LY and QALY, and the incremental cost–effectiveness ratio (ICER). To assess different levels of uncertainty, scenario and sensitivity analyses, as well as a probabilistic sensitivity analysis (PSA) are also to be conducted.
Patient cohort
Baseline characteristics of the EMPA-REG H2H-SU trial were programmed in the CDM. The data represented patients with T2D and no established CVD whose glycemia was inadequately controlled with metformin alone. Thirty-three percent of the patients in the EMPA-REG H2H-SU trial were Asian [4]. Patients had a starting age of 56 years, average diabetes duration of 6 years and baseline HbA1c level of 7.92% (Supplementary Table 1). Patients were defined as Asian in the CDM.
Intervention & comparator
This economic evaluation compared empagliflozin with glimepiride as an add on to metformin. When the patients’ HbA1c level exceeded the defined threshold of 8.5%, patients moved to a rescue therapy. This next-line therapy was defined equally in both arms, as a combination of insulin glargine and glimepiride. The efficacy of this treatment combination was informed by a published meta-analysis [16]. In both lines, HbA1c progression evolved over time following the UKPDS 68 progression model. The average daily dose of insulin was not reported per kg and hence was used as such (40.6 IU/day). For glimepiride, the dose was not reported in the meta-analysis and so we assumed 2 mg daily following the defined daily dose recommended by the WHO [17].
Clinical data
The efficacy data of both empagliflozin and glimepiride were extracted from the trial (Table 2) [18]. These effects show the impact of treatments on the evolution of patients’ physiological parameters, which will influence the progression of the disease and the projections on the occurrence of events (i.e., clinical outcomes). After the 4-year time-point, treatment effect on CV and mortality outcomes were maintained until treatment escalation occurred at HbA1c level of 8.5%. After treatment switch, the occurrence of diabetes complications was predicted by the standard UKPDS 82 REs (i.e., without calibration). Hypoglycemia, urinary tract infection (UTI) and genital infection (GI) were considered as adverse events (Table 2). Table 2 also describes the treatment effects of the second-line therapy, insulin glargine and glimepiride [16]. Mortality data were predicted using the UKPDS82 combined mortality approach.
| Empagliflozin | Glimepiride | Glargine + Glimepiride (second-line treatment) | |||
|---|---|---|---|---|---|
| Mean | SE | Mean | SE | Mean | |
| Treatment effects | |||||
| – Change from baseline HbA1c (%-points) | -0.74 | 0.029 | -0.66 | 0.032 | -1.70 |
| – Change from baseline in SBP (mmHg) | -4.39 | 0.540 | 1.44 | 0.960 | – |
| – Change from baseline in BMI (kg/m2) | -1.14 | 0.003 | 0.56 | 0.001 | 0.80 |
| Adverse events | |||||
| – NSHE rate (per 100 patient-years) | 0.42 | – | 3.33 | – | 486 |
| – SHE1 rate (per 100 patient-years) | 0.16 | – | 2.69 | – | 1.76 |
| – SHE2 rate (per 100 patient-years) | 0 | – | 0.16 | – | 0.24 |
| – GI/UTI (annual probability; 0–1) | 0.08 | – | 0.05 | – | – |
Source: Clinical study report (first-line treatment), Fonseca et al. [16] (second-line treatment).
GI: Genital infection; NSHE: Nonsevere hypoglycemia rate; SBP: Systolic blood pressure; SE: Standard error; SHE1: Severe hypoglycemia rate (not requiring medical assistance); SHE2: Severe hypoglycemia rate (requiring medical assistance); UTI: Urinary tract infection.
Utility data
Baseline quality of life utility of Chinese patients with T2D without complications was 0.876 [19] and BMI-related disutility applied per BMI point increase was 0.0061 [20]. For acute events, a disutility was subtracted from the base utility, leading to a final utility score recorded for the patient experiencing the event. In case, a patient suffered different multiple events (e.g., a myocardial infarction [MI] and a stroke), the model followed the minimum approach, recording the utility value of the health state with the lowest individual score, while still applying a disutility related to adverse events. The full list of utilities and disutilities can be retrieved from Supplementary Table 2.
Perspective & cost data
A healthcare system perspective was taken, therefore only direct medical costs were considered. These included medicine acquisition costs, cost of managing complications, adverse events costs and costs related to long-term clinical management of the disease. Treatment acquisition costs were derived from a Chinese big-data service platform for the health industry (Table 3) [21] and from the tendering prices [22], in line with National Development and Reform Commission’s price-difference policy [23]. The daily cost of empagliflozin 25 mg in China was calculated according to the Chinese rules of price difference and based on the tendering price of empagliflozin 10 mg. The information on costs were derived from a recent publication that assessed the burden of T2D in China using the CDM, which provided detailed cost data in the Chinese setting (Supplementary Table 3) [24]. All costs were inflated and reported as 2020 Chinese Yuan (CNY). Additionally, results were also reported in US dollars to allow convenient interpretation by the international health community.
| Medicine | Strength | Daily dose | Daily cost (CNY) | Annual drug costs (CNY) |
|---|---|---|---|---|
| Empagliflozin | 25 mg | 1 | 8.55† | 3123 |
| Glimepiride | 4 mg | 1 | 0.104‡ | 38 |
| Metformin | 500 mg | 3 | 2.400§ | 877 |
| Glargine¶ | – | 40.6 UI/day | 8.400‡ | 6764 |
| Glimepiride# | 2 mg | 1 | 0.052 | 19 |
| NPH¶ | – | 15 UI/day | 2.43 | 4656 |
| Empagliflozin + metformin | – | – | – | 3999 |
| Glimepiride + metformin | – | – | – | 915 |
| Glimepiride + glargine | – | – | – | 6783 |
†
‡
The lowest price of the drugs winning the VBP tendering in China in 2020 [22].
§
Volume-weighted average cost including generics calculated by using IQVIA CHPA data [25].
¶
Annual cost includes cost of blood glucose monitoring strips, lancets and disposable syringe.
#
Glimepiride in second-line treatment as a combination with insulin glargine.
CNY: Chinese Yuan; NPH: Neutral protamine Hagedorn; VBP: Volume-based procurement.
Time horizon & discounting
The base case was defined as lifelong analysis. With a baseline age of 56 years, a time horizon of 50 years was considered long enough to have all patients in the death state. An annual discount rate of 5% was applied to both future costs and effects in line with Chinese economic guidelines [26]. To assess the impact of discounting rates on the results, scenarios were run with different discount rates (0, 3 and 8%).
Scenarios
Additional scenarios were run to test the impact of various assumptions on the results. In the first scenario, an HbA1c threshold of 9% was tested in contrast to the 8.5% considered in the base case. Second, the impact of BMI on utility was removed to evaluate the effect of this assumption on the base-case results due to differences in BMI reductions of both arms. Third, the short-term outcomes were assessed by shortening the time horizon to 4 years to align with the duration of the actual clinical trial (EMPA-REG H2H-SU). Fourth, as neutral protamine Hagedorn (NPH) insulin is the most used insulin in China, the costs of glargine in next-line therapy were replaced by NPH insulin costs (daily dosage: 15 IU/day and cost per unit: 0.16 CNY). As NPH insulin is applicable to both arms when first line of treatment fails in maintaining glycemic control, the additional risk of hypoglycemia given by this treatment was ignored to be conservative. Fifth, given that Asians have on average a lower BMI compared with Caucasians, a starting BMI of 24 was considered at baseline instead of 29 in the base case.
Probabilistic sensitivity analysis
A PSA was also conducted to capture parameter uncertainty. This is achieved through Monte Carlo simulations together with nonparametric bootstrapping (using 1000 patients and 1000 iterations), so that the robustness of the cost–effectiveness results could be assessed. The parameters included in the PSA are patient characteristics, treatment efficacy, utility and cost of complications. Log normal distributions and 20% variation were applied to sample the costs of complications. Treatment effects were sampled based on the estimated standard error detailed in Table 2. The utility data were varied according to the variability reported in standard deviations values displayed in Supplementary Table 2. All were sampled following the beta distribution. For sampling patient’ baseline characteristics, truncated Normal distributions were used following the mean and standard error (SE) reported in Supplementary Table 1.
Results
Base case
In the long-term, when compared with glimepiride, patients on empagliflozin gained an incremental 0.232 LYs and 0.317 QALYs (Table 5). Furthermore, treatment with empagliflozin costed $1368 (CNY9703) more per patient compared with glimepiride, resulting in an ICER of $4364 (CNY30,648) per QALY gained. The WHO defines the WTP threshold as three-times the national gross domestic product (GDP) per capita [27]. For China, this approximates $30,290 (CNY212,676) [28]. As such, at this threshold empagliflozin is a cost-effective treatment option in patients with T2D, without established CVD and not controlled with metformin alone in China.
Patients receiving empagliflozin stayed on first-line therapy for 9 years, whereas for patients on glimepiride this was 7 years. After that, in both arms, patients received insulin glargine plus glimepiride, however in the glimepiride arm, patients initiated insulin glargine 2 years earlier, which lead to higher hypoglycemia and CVD costs.
Patients receiving empagliflozin showed better survival (24.785 years) than those receiving glimepiride (24.167 years; Table 4). This is driven by the improved cardiovascular and renal event rates of empagliflozin over lifetime compared with glimepiride where the RR were below 1 (0.829–0.961; Table 4). Only the estimated number of stroke events was more favorable for glimepiride compared with empagliflozin (RR = 1.025).
| Empagliflozin | Glimepiride | Incremental | |
|---|---|---|---|
| Undiscounted life expectancy (years) | 24.785 | 24.167 | 0.618 |
| Outcome | Event rates per 1000 patient years | Relative risk | |
|---|---|---|---|
| Empagliflozin | Glimepiride | ||
| Myocardial infarction | 7.718 | 9.302 | 0.830 (0.825–0.835) |
| Hospitalization for angina | 5.031 | 5.628 | 0.894 (0.887–0.902) |
| Hospitalization for heart failure | 3.256 | 3.927 | 0.829 (0.820–0.839) |
| Stroke | 4.438 | 4.328 | 1.025 (1.015–1.036) |
| End-stage renal disease | 2.401 | 2.499 | 0.961 (0.947–0.973) |
| Empagliflozin (mean [SD]) | Glimepiride (mean [SD]) | Incremental (mean) | |
|---|---|---|---|
| Base case | |||
| – Life expectancy (years) | 13.347 (0.105) | 13.114 (0.104) | 0.232 |
| – Quality-adjusted life expectancy (years) | 10.492 (0.085) | 10.175 (0.084) | 0.317 |
| – Direct costs | 160,219 (2655) | 150,516 (2826) | 9703 |
| – ICER | 30,648 | 30,648 | |
| HbA1c threshold = 9% | |||
| – Life expectancy (years) | 13.49 (0.094) | 13.327 (0.098) | 0.163 |
| – Quality-adjusted life expectancy (years) | 10.628 (0.079) | 10.371 (0.078) | 0.258 |
| – Direct costs | 158,149 (2597) | 143,113 (2736) | 15,036 |
| – ICER | – | – | 58,346 |
| Discount rate = 0% (costs and effects) | |||
| – Life expectancy (years) | 24.785 (0.312) | 24.167 (0.302) | 0.618 |
| – Quality-adjusted life expectancy (years) | 19.19 (0.24) | 18.483 (0.231) | 0.707 |
| – Direct costs | 357,450 (7436) | 34,590 (7712) | 11,546 |
| – ICER | – | – | 16,326 |
| Discount rate = 3% (costs and effects) | |||
| – Life expectancy (years) | 16.657 (0.156) | 16.322 (0.154) | 0.335 |
| – Quality-adjusted life expectancy (years) | 13.023 (0.123) | 12.598 (0.12) | 0.425 |
| – Direct costs | 214,432 (3806) | 204,289 (4004) | 10,143 |
| – ICER | – | – | 23,871 |
| Discount rate = 8% | |||
| – Life expectancy (years) | 10.075 (0.063) | 9.934 (0.063) | 0.141 |
| – Quality-adjusted life expectancy (years) | 7.972 (0.053) | 7.757 (0.053) | 0.215 |
| – Direct costs | 110,113 (1733) | 100,836 (1874) | 9277 |
| – ICER | – | – | 43,149 |
| BMI disutility option OFF† | |||
| – Life expectancy (years) | 13.347 (0.105) | 13.114 (0.104) | 0.232 |
| – Quality-adjusted life expectancy (years) | 10.708 (0.087) | 10.47 (0.086) | 0.237 |
| – Direct costs | 160,219 (2655) | 150,516 (2826) | 9703 |
| – ICER | – | – | 40,890 |
| Time horizon = 4 years | |||
| – Life expectancy (years) | 3.52 (0.008) | 3.52 (0.009) | 0.001 |
| – Quality-adjusted life expectancy (years) | 2.86 (0.014) | 2.832 (0.014) | 0.028 |
| – Direct costs | 23,665 (513) | 13,826 (542) | 9840 |
| BMI at baseline = 24 | |||
| – Life expectancy (years) | 13.27 (0.085) | 13.156 (0.104) | 0.115 |
| – Quality-adjusted life expectancy (years) | 10.66 (0.083) | 10.503 (0.085) | 0.157 |
| – Direct costs | 157,250 (2514) | 150,866 (2860) | 6384 |
| – ICER | – | – | 40,767 |
| Cost of insulin glargine replaced by NPH costs | |||
| – Direct costs | 146,218 (2556) | 134,268 (2721) | 11,950 |
| – ICER | – | – | 37,745 |
†
The effect of BMI on utility is switched off.
ICER: Incremental cost–effectiveness ratio; NPH: Neutral protamine Hagedorn; SD: Standard deviation.
Scenario analysis
The results of the scenario analyses further anchored the cost–effectiveness profile of empagliflozin observed in the base case ($4364/QALY). Empagliflozin remained cost-effective across all scenarios, with the exception of the shorter-time horizon scenario (Table 5). Applying a higher HbA1c threshold 9% for treatment switch increased the ICER to $8309 (CNY58,346) per QALY gained. When assessing the results without the effect of BMI change on utility, as per Bagust et al., absolute QALYs increased in both arms and the incremental gain declined, leading to an ICER of $5824 (CNY40,890) per QALY gained. Running the analysis over a time horizon of 4 years highlighted the benefit of empagliflozin versus glimepiride as add on to metformin, by reducing the progression of renal disease and the risk of CV events. This scenario showed that, compared with glimepiride plus metformin, patients on empagliflozin plus metformin have lower incidence of congestive heart failure, peripheral vascular disease, angina and MI, as well as of microalbuminuria, gross proteinuria and end-stage renal disease. In this scenario, the ICER was $49,871 (CNY350,161) per QALY gained (Figure 1). By replacing the cost of insulin glargine by NPH insulin, absolute total and treatment costs decreased, nevertheless both incremental cost and ICER slightly increased to $1702 (CNY11,950) and $5376 (CNY37,745), respectively. By replacing the baseline BMI by 24, the average BMI of adult Asians with diabetes, absolute QALYs increased and total costs decreased in both arms. Incremental QALYs and costs decrease, leading to a small rise of the ICER to $5806 (CNY40,767).
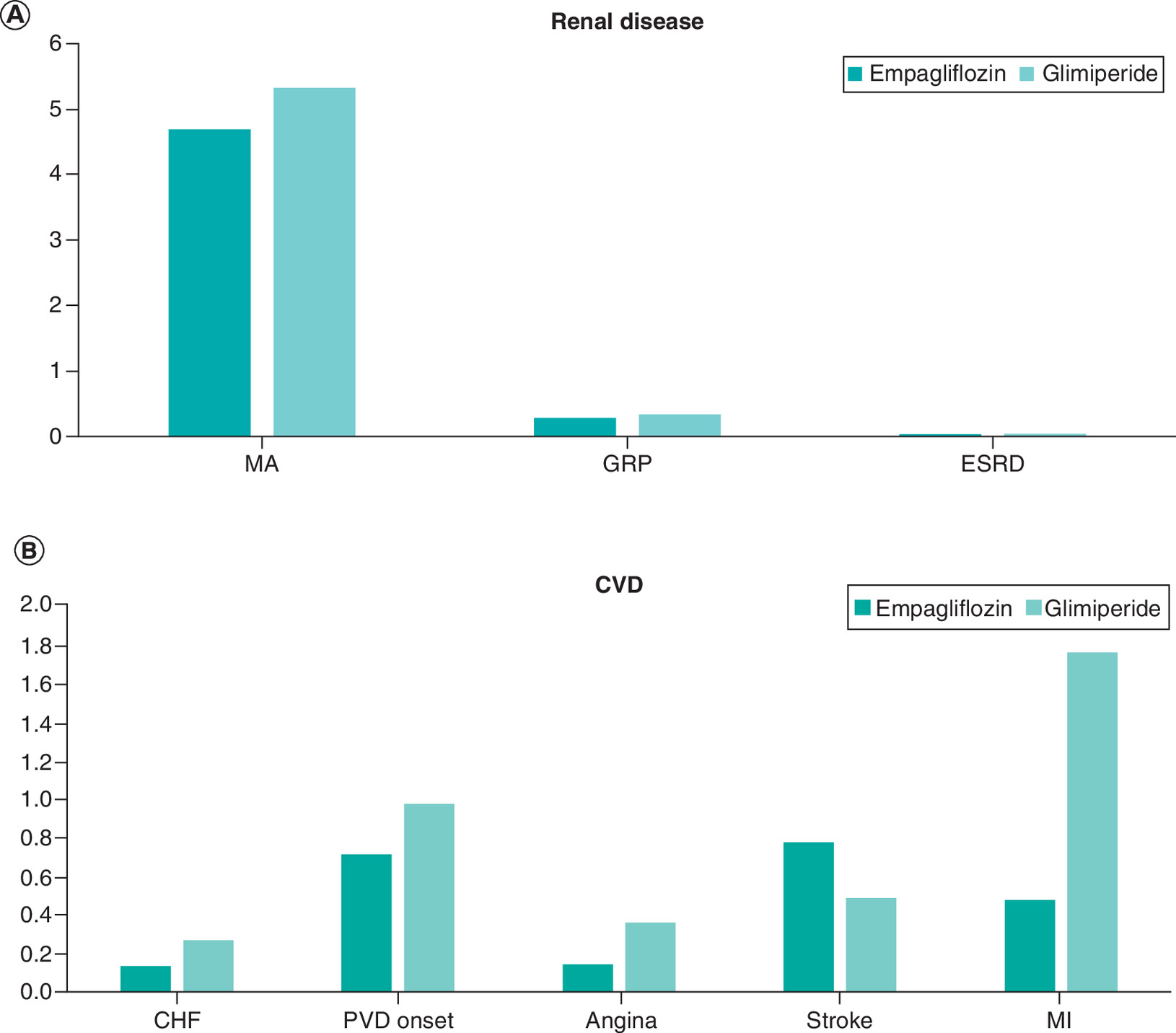
Figure 1. Short-term cumulative incidence of renal and cardiovascular disease complications (empagliflozin vs glimepiride).
CHF: Congestive heart failure; CVD: Cardiovascular disease; ESRD: End stage renal disease; GRP: Gross proteinuria; MA: Microalbuminuria: MI: Myocardial infarction; PVD: Peripheral vascular disease.
Probabilistic sensitivity analysis
Most iterations lie on the first quadrant (North–East) of the scatterplot, showing incremental positive benefits and slightly higher costs (Figure 2). The cost–effectiveness acceptability curve revealed that empagliflozin has a probability of being dominant in 10% of cases in China with a 95% probability of being cost-effective at the defined local WTP threshold of $30,290 (CNY212,676; Figure 3).

Figure 2. Probabilistic sensitivity analysis scatterplot (empagliflozin vs glimepiride).
CNY: Chinese yuan; QALY: quality adjusted life-years.
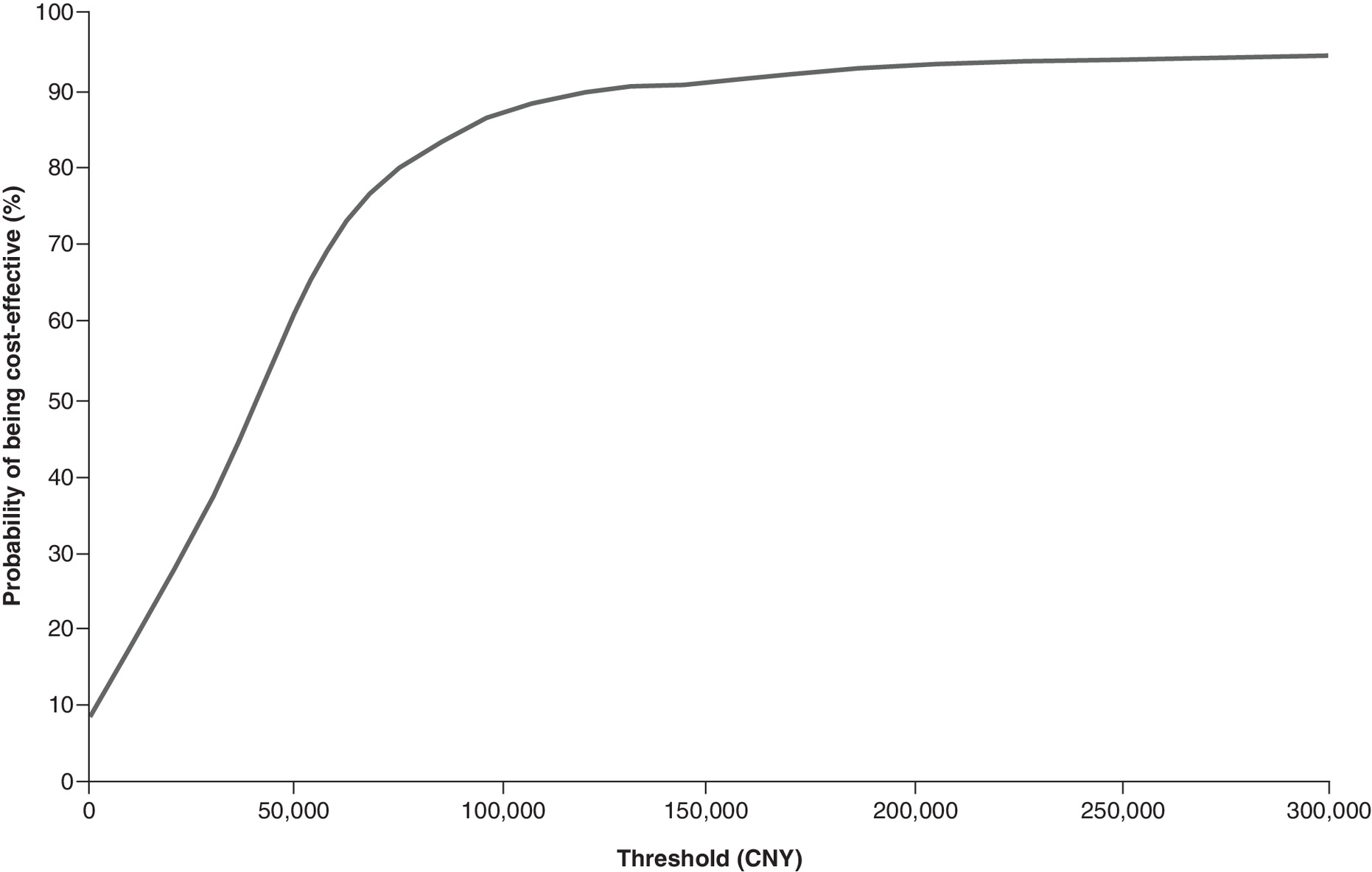
Figure 3. Cost–effectiveness analysis acceptability curve (empagliflozin vs glimepiride).
CNY: Chinese yuan.
Discussion
This analysis assessed the lifetime cost–effectiveness of empagliflozin versus glimepiride in patients with T2D without established CVD in China, uncontrolled on metformin alone. The underlying treatment effects applied were based on results from the EMPA-REG H2H-SU trial in which patients with T2D did not have a history of cardiovascular complications and 33% of patients were of Asian descent. The trial duration was 4 years. The CDM was calibrated to predict, in both arms, the observed 4-year outcome of the trial and treatment effects were maintained until treatment escalation (at a HbA1c threshold of 8.5%).
Patients receiving empagliflozin survived on average 0.62 years (undiscounted) longer than individuals receiving glimepiride, in addition to experiencing 11% less cardiovascular events and 4% less renal events. Over lifetime, empagliflozin accrued positive incremental discounted life years (0.232) and QALY (0.317) per patient, compared with glimepiride, with an incremental cost of $1368 (CNY9703).
Compared with glimepiride, the study showed that empagliflozin reduces the number of complications and modestly increases life expectancy with 0.272 life years, which makes it a good value for money compared with glimepiride when given in second-line therapy after metformin alone as failed in the Chinese healthcare setting.
The PSA and the scenario analyses highlighted the robustness of the base-case results, which allowed to evaluate and confirm the cost–effectiveness profile of empagliflozin compared with glimepiride. Short-term findings confirmed the value of empagliflozin in reducing the progression of renal disease and the risk of CVD (as proven by the trial).
The clinical and economic value of empagliflozin in patients with history of CVD and a long history of diabetes has been shown before in the EMPA-REG OUTCOME study and several cost–effectiveness analyses [29–32]. The novelty of the current cost–effectiveness analysis is that it considers patients without established CVD and with a much shorter duration of diabetes, and thus describes patients with a lower risk of developing complications.
The clinical trial reported a baseline BMI of 30.11 kg/m2 that might be considered high for a Chinese patients with T2D. As such, this assumption was tested in the scenario analysis by applying an initial BMI of 24 at the baseline of both cohorts of the two arms. The resulting ICER increased slightly from $4364 to $5376, confirming the cost–effectiveness profile of empagliflozin in a population with lower BMI values. Consequently, our findings are not driven by assumptions around BMI.
The use of UKPDS risk engines could be considered a limitation (based on UK data) to predict diabetes complications in Chinese patients with T2D. However, this approach has been followed before by many other authors [32–36].
One of these studies, Shao et al. conducted a cost–effectiveness analysis comparing dapagliflozin versus glimepiride as monotherapy in China, showing cost-savings in favor of SGLT-2 inhibitors [32]. This was a lifelong analysis with baseline demographics based solely on Chinese subjects. The results showed cost-savings in favor of dapagliflozin, driven mainly by assumptions related to BMI. In the latter, for every BMI increase of 1 kg/m2, there was an associated decrease in utility of 0.0472 and for every decrease of 1 kg/m2, there was an associated increase in utility of 0.0171. Both are higher increments compared with Bagust et al.’s value (0.0061 per 1 kg/m2 change) used in the current analyses. Furthermore, a separate cost per BMI level is applied, which could be considered as double counting costs of events like MI and stroke (these events are more frequent in more obese patients) [37]. In our analysis, however, we did not include a specific cost associated directly with a BMI level. The impact of BMI change in our evaluation was measured through differences in progression of the disease and in incidences of complications between the two arms that influence patients’ survival and quality of life. The latter was tested in a scenario analysis.
Furthermore, the clinical data used in this analysis applied efficacy data reported for the full trial population, of which only 33% were Asians. Although we recognize this as a limitation of the study, many other health economic (HE) studies published Chinese findings using clinical data of trial populations not involving Asians or Chinese patients [36,38]. Therefore, considering this geographic region to recruit patients for the trial can be considered as an improvement when compared with other trials.
The choice of second-line therapy in China after a combination of SLGT-2 with metformin could be questioned. We opted for a combination of insulin and glimepiride, whereas NPH insulin is the most common insulin used in China.
The treatment effects of insulin glargine and glimepiride were based on a pooled analysis of 11 retrospective trials [16] and although the baseline patient characteristics were not exactly the same, they were considered comparable to the modeled cohort after 7–9 years of history of dual therapy, before escalation to insulin glargine and sulfonylurea (SU). Using NPH insulin cost had no impact on the conclusions.
The generated evidence of this study emphasizes the strong tendency of empagliflozin being cost-effective compared with glimepiride over lifetime in patients with T2D and no history of CVD in China.
Conclusion
The present economic evaluation is believed to be the first analysis comparing empagliflozin versus glimepiride in China and in patients with T2D and without established CVD not well controlled with metformin alone. It was shown that empagliflozin is cost-effective compared with glimepiride. Scenarios and sensitivity analyses confirmed the robustness of our findings. The results of the present work aim to support decision-making efforts in China toward efficient resource use with regard to the management of patients with T2 diabetes.
Future perspective
Typical diabetes disease models use well-established REs to predict diabetes complications. Several CVOTs reporting 3–5 years of diabetes outcomes in patients with established CVD have shown that the classic REs did not predict CVO outcomes well, therefore calibration of diabetes models is necessary. In patients with diabetes and without history of CVD, fewer long-term studies have been conducted. Driven by the CVOT results on SGLT-2 inhibitors, but also on GLP-1 agonists, more and more of these drugs are recommended as first choice after metformin alone. Evidence on CVO outcomes in patients without a history of CVD is recent, justifying the need for this study. This manuscript is the first of its kind to study the cost–effectiveness in patients with T2D without history of CVD and using data from EMPA-REG H2H-SU trial (NCT01167881). The current analysis has shown that also here calibration of the REs is needed to obtain the study predictions. More studies are needed to refine the current REs and define risk factors to be added to the equations.
•
EMPA-REG H2H-SU trial (NCT01167881) provided relevant information about the safety profile of empagliflozin and glimepiride as add-on to metfomin, in patients without established cardiovascular disease. Cardiovascular (CV) complications are the main outcomes of the cardiovascular outcome trials (CVOT).
•
Using the treatment effects reported in this trial, the Core Diabetes Model was calibrated to predict well the observed outcomes of both treatments with less than 5% variation.
•
In the calibration process, the UKPDS 82 risk equations were found to be the best option to predict diabetes complications.
•
The analysis assumed that CVOT benefits would apply while patients were on treatment. Several scenarios were added to assess the impact of this assumption.
•
In the short-term, empagliflozin+metformin reduced the risk of primary and subsequent myocardial infarction, primary and subsequent stroke, hospitalization for angina, hospitalization for heart failure, CV death and non-CV death.
•
In the long run, treatment with empagliflozin resulted in additional life years (+0.232) and quality-adjusted life years (+0.317), for an incremental cost of USD (+9703) compared with glimiperide+metformin.
•
The present analysis has demonstrated that empagliflozin+metformin is a cost-effective therapy compared with glimiperide+metformin from the Chinese healthcare payer perspective.
Financial & competing interests disclosure
This study was funded by Boehringer Ingelheim International GmbH. M Ramos and M Lamotte are full-time employees of IQVIA. A Salem was a full-time employee of IQVIA at the time the study was conducted. IQVIA received consulting fees from Boehringer Ingelheim to conduct this work. A Ustyugova is a full-time employee of Boehringer Ingelheim, the manufacturer of empagliflozin. YJ Zhang was full-time employee of Boehringer Ingelheim, at the time the study was conducted. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The current study is a cost–effectiveness analysis conducted on 1000 hypothetical patients and as such, no ethical committee approval was required.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_file.docx)
- Download
- 40.82 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
The UK Prospective Diabetes Study Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 352(9131), 837–853 (1998).
2.
Gourzoulidis G, Tzanetakos C, Ioannidis I et al. Cost–effectiveness of empagliflozin for the treatment of patients with Type 2 diabetes mellitus at increased cardiovascular risk in Greece. Clin. Drug Investig. 38(5), 417–426 (2018).
3.
Zelniker TA, Wiviott SD, Raz I et al. SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet 393(10166), 31–39 (2019).
4.
Ridderstrale M, Rosenstock J, Andersen KR, Woerle HJ, Salsali A, EMPA-REG H2H-SU trial investigators. Empagliflozin compared with glimepiride in metformin-treated patients with type 2 diabetes: 208-week data from a masked randomized controlled trial. Diabetes Obes. Metab. 20(12), 2768–2777 (2018).
5.
International Diabetes Federation (IDF). Dibetes Atlas. Ninth edition (2019). https://diabetesatlas.org/upload/resources/material/20200302_133351_IDFATLAS9e-final-web.pdf
6.
Rahman W, Solinsky PJ, Munir KM, Lamos EM. Pharmacoeconomic evaluation of sodium-glucose transporter-2 (SGLT2) inhibitors for the treatment of type 2 diabetes. Expert Opin. Pharmacother. 20(2), 151–161 (2019).
7.
McEwan P, Foos V, Palmer JL, Lamotte M, Lloyd A, Grant D. Validation of the IMS CORE Diabetes Model. Value Health 17(6), 714–724 (2014).
• A description of the IQVIA Core Diabetes Model structure is provided.
8.
Das SR, Everett BM, Birtcher KK et al. 2018 ACC Expert Consensus Decision Pathway on novel therapies for cardiovascular risk reduction in patients with type 2 diabetes and atherosclerotic cardiovascular disease: a report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways. J. Am. Coll. Cardiol. 72(24), 3200–3223 (2018).
9.
Hayes AJ, Leal J, Gray AM, Holman RR, Clarke PM. UKPDS outcomes model 2: a new version of a model to simulate lifetime health outcomes of patients with type 2 diabetes mellitus using data from the 30 year United Kingdom Prospective Diabetes Study: UKPDS 82. Diabetologia 56(9), 1925–1933 (2013).
• A description of the risk equation used to predict diabetes complication is detailed.
10.
Kengne AP. The ADVANCE cardiovascular risk model and current strategies for cardiovascular disease risk evaluation in people with diabetes. Cardiovasc. J. Afr. 24(9-10), 376–381 (2013).
11.
Ahmad Kiadaliri A, Clarke PM, Gerdtham UG et al. Predicting changes in cardiovascular risk factors in Type 2 diabetes in the post-UKPDS era: longitudinal analysis of the Swedish National Diabetes Register. J. Diabetes Res. 24134 (2013).
12.
Cederholm J, Eeg-Olofsson K, Eliasson B et al. Risk prediction of cardiovascular disease in type 2 diabetes: a risk equation from the Swedish National Diabetes Register. Diabetes Care 31(10), 2038–2043 (2008).
13.
Folsom AR, Chambless LE, Duncan BB, Gilbert AC, Pankow JS. Prediction of coronary heart disease in middle-aged adults with diabetes. Diabetes Care 26(10), 2777–2784 (2003).
14.
Davis WA, Knuiman MW, Davis TM. An Australian cardiovascular risk equation for type 2 diabetes: the Fremantle Diabetes Study. Intern. Med. J. 40(4), 286–292 (2010).
15.
Assmann G, Cullen P, Schulte H. Simple scoring scheme for calculating the risk of acute coronary events based on the 10-year follow-up of the prospective cardiovascular Munster (PROCAM) study. Circulation 105(3), 310–315 (2002).
16.
Fonseca V, Gill J, Zhou R, Leahy J. An analysis of early insulin glargine added to metformin with or without sulfonylurea: impact on glycaemic control and hypoglycaemia. Diabetes Obes. Metab. 13(9), 814–822 (2011).
17.
World Health Organization (WHO). Defined Daily Dose (DDD) (2020). www.whocc.no/ddd/definition_and_general_considera/
18.
Clinicaltrials.gov. Efficacy and safety of empagliflozin (BI 10773) with metformin in patients with type 2 diabetes (2016). https://clinicaltrials.gov/ct2/show/NCT01167881
• This reference provides a link to the trial design and features and on the clinical data produced and considered in the analyses produced in this manuscript.
19.
Li T, Wan X, Ma J, Wu B. Cost–effectiveness of primary prevention with statin treatment for chinese patients with Type 2 diabetes. Adv. Ther. 35(12), 2214–2223 (2018).
20.
Bagust A, Beale S. Modelling EuroQol health-related utility values for diabetic complications from CODE-2 data. Health Econ. 14(3), 217–230 (2005).
21.
Yaozh.com. (2020). www.yaozh.com/
23.
National Development and Reform Commission (NDRC). Rules of Drug Price Difference (2011). www.ndrc.gov.cn/xxgk/zcfb/tz/201112/t20111201_964344.html, https://www.ndrc.gov.cn/xxgk/zcfb/tz/201112/W020190905511109587604.pdf
24.
Foos V, Wang K, McEwan P et al. Assessing the burden of Type 2 diabetes in China considering the current status-quo management and implications of improved management using a modeling approach. Value Health Reg. Issues 18, 36–46 (2018).
25.
IQVIA China Hospital Pharmaceutical Audit database (2019).
26.
Liu GE, Wu JH et al. China PharmaceuEconomics: Evaluations and Guidance, 2015 Edition. (2015).
27.
Marseille E, Larson B, Kazi DS, Kahn JG, Rosen S. Thresholds for the cost–effectiveness of interventions: alternative approaches. Bull. World Health Organ. 93(2), 118–124 (2015).
28.
China NBoSo. GDP per capita (2020). www.stats.gov.cn/tjsj/zxfb/202002/t20200228_1728913.html
29.
Zinman B, Wanner C, Lachin JM et al. Empagliflozin, Cardiovascular outcomes, and mortality in Type 2 diabetes. N. Engl. J. Med. 373(22), 2117–2128 (2015).
30.
Ramos M, Foos V, Ustyugova A, Hau N, Gandhi P, Lamotte M. Cost–effectiveness analysis of empagliflozin in comparison to sitagliptin and saxagliptin based on cardiovascular outcome trials in patients with Type 2 diabetes and established cardiovascular disease. Diabetes Ther. 10(6), 2153–2167 (2019).
• A similar study has been published recently using similar methodology in which analyses were run on patients with Diabetes and established cardiovascular disease.
31.
Ramos M, Ustyugova A, Hau N, Lamotte M. Cost–effectiveness of empagliflozin compared with liraglutide based on cardiovascular outcome trials in Type II diabetes. J. Comp. Eff. Res. 9(11), 781–794 (2020).
•• A similar study has been published recently using similar methodology in which analyses were run on patients with Diabetes and established cardiovascular disease.
32.
Peng M, Tianbi L, Suodi Z. Empagliflozin in type 2 diabetes mellitus patients with high cardiovascular risk: a model-based cost-utility analysis in China. Diabetes Metab. Syndr. Obes. 13, 2823–2831 (2020).
33.
Gao L, Zhao FL, Li SC. Cost-utility analysis of liraglutide versus glimepiride as add-on to metformin in type 2 diabetes patients in China. Int. J. Technol. Assess. Health Care 28(4), 436–444 (2017).
34.
Hu S, Deng X, Ma Y, Li Z, Wang Y, Wang Y. Cost-Utility analysis of dapagliflozin versus saxagliptin treatment as monotherapy or combination therapy as add-on to metformin for treating Type 2 diabetes mellitus. Appl. Health Econ. Health Policy 19(1), 69–79 (2021).
35.
Xie X, Vondeling H. Cost-utility analysis of intensive blood glucose control with metformin versus usual care in overweight type 2 diabetes mellitus patients in Beijing, P.R. China. Value Health 11(Suppl. 1), S23–S32 (2008).
36.
McEwan P, Bennett H, Khunti K et al. Assessing the cost–effectiveness of sodium-glucose cotransporter-2 inhibitors in type 2 diabetes mellitus: a comprehensive economic evaluation using clinical trial and real-world evidence. Diabetes Obes Metab. 22(12), 2364–2374 (2020).
•• Provides additional evidence on the cost–effectiveness profile of sodium-glucose cotransporter-2 in China and other locations.
37.
Shao H, Zhai S, Zou D et al. Cost–effectiveness analysis of dapagliflozin versus glimepiride as monotherapy in a Chinese population with type 2 diabetes mellitus. Curr. Med. Res. Opin. 33(2), 359–369 (2017).
38.
Palmer J, Gibbs M, Scheijbeler H et al. Cost–effectiveness of switching to biphasic insulin aspart in poorly-controlled type 2 diabetes patients in China. Adv. Ther. 25(8), 752–774 (2008).
Information & Authors
Information
Published In
Pages: 469 - 480
PubMed: 33576249
Copyright
© 2021 Mafalda Ramos. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 16 December 2020
Accepted: 14 January 2021
Published online: 12 February 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost–effectiveness analysis of empagliflozin compared with glimepiride in patients with Type 2 diabetes in China. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0284
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Ian W. Campbell, Kerstin M. G. Brand, Ulrike Gottwald-Hostalek, Julian Dettenbach, Evaluating Cost-Effectiveness in Relation to the Supporting Clinical Evidence Across the Type 2 Diabetes Continuum: A Review of Metformin and SGLT2is, Advances in Therapy, 10.1007/s12325-026-03592-6, (2026).
- Huiyuan Zhang, Jiaojiao Chen, Quan Zhao, Bei Zhang, Cost-utility analysis of empagliflozin compared with dapagliflozin in patients with type 2 diabetes in China, Frontiers in Public Health, 10.3389/fpubh.2025.1566101, 13, (2025).
- Mari Pesonen, Virpi Jylhä, Eila Kankaanpää, Adverse drug events in cost-effectiveness models of pharmacological interventions for diabetes, diabetic retinopathy, and diabetic macular edema: a scoping review, JBI Evidence Synthesis, 10.11124/JBIES-23-00511, 22, 11, (2194-2266), (2024).
- İsmail Keleş, Aynur Koyuncu, Ayla Yava, Nermin Olgun, Examination of Type 2 Diabetes Risk, Behavioural and Family Risk Factors, and Type 2 Diabetes Awareness in Healthcare Professionals Vocational School Students: The case of the Eastern Anatolian region of Turkey, Bingöl Üniversitesi Sağlık Dergisi, 10.58605/bingolsaglik.1419824, 5, 1, (19-28), (2024).
- Mohammed AlHarbi, Abdullah Othman, Ahmed Ali Nahari, Ahmed Hamdan Al-Jedai, Daniel Cuadras, Faisal Almalky, Fayez AlAzmi, Hajer Yousef Almudaiheem, Hamad AlShubrumi, Hameed AlSwat, Homaid AlSahafi, Kamelia Sindi, Khadija Basaikh, Majed AlQahtani, Mark Lamotte, Moataz Yahia, Mohamed El-Khedr Hassan, Mohammed AlMutlaq, Mohammed AlRoaly, Somaya AlZelaye, Zein AlGhamdi, Burden of Illness of Type 2 Diabetes Mellitus in the Kingdom of Saudi Arabia: A Five-Year Longitudinal Study, Advances in Therapy, 10.1007/s12325-023-02772-y, 41, 3, (1120-1150), (2024).
- Zixuan He, Xianqin Huang, Dingyi Chen, Guoan Wang, Yuezhen Zhu, Huangqianyu Li, Sheng Han, Luwen Shi, Xiaodong Guan, Sponsorship bias in published pharmacoeconomic evaluations of national reimbursement negotiation drugs in China: a systematic review, BMJ Global Health, 10.1136/bmjgh-2023-012780, 8, 11, (e012780), (2023).
- Wayne H‐H Sheu, Yutaka Seino, Elise Chia‐Hui Tan, Daisuke Yabe, Kyoung Hwa Ha, Masaomi Nangaku, Wook‐Jin Chung, Koichi Node, Atsutaka Yasui, Wei‐Yu Lei, Sunwoo Lee, Anastasia Ustyugova, Riho Klement, Anouk Deruaz‐Luyet, Moe H Kyaw, Dae Jung Kim, Healthcare resource utilization in patients treated with empagliflozin in East Asia, Journal of Diabetes Investigation, 10.1111/jdi.13728, 13, 5, (810-821), (2022).