Web-based decision aids to support breast cancer screening decisions: systematic review and meta-analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Breast cancer is a leading cause of cancer among women. Because guidelines on screening for breast cancer for certain ages are controversial, many experts advocate the use of shared decision making (SDM) using validated decision aids (DAs). Recent studies have concluded that DAs are beneficial; however, the results have great heterogeneity. Therefore, further studies are needed to improve understanding of these tools. Objective: This systematic review and meta-analysis aimed to investigate the impact of using web-based DAs in women aged 50 years and below facing the decision to be screened for breast cancer in comparison with usual care. Methods: PubMed, Web of Science, Embase and the Cochrane CENTRAL databases were searched up to February 2020 for studies assessing web-based DAs for women making a breast cancer screening decision and reported quality of decision-making outcomes. Using a random-effects model or a fixed-effects model, meta-analyses were conducted pooling results using mean differences (MD), standardized mean differences (SMD) and relative risks (RR). Results: Of 1097 unique citations, three randomized controlled trials and two before–after studies met the study eligibility criteria. Compared with usual care, web-based DAs increased knowledge (SMD = 0.69; 95% CI: 0.57–0.80; p < 0.00001), reduced decision conflict and increased the proportion of women who made an informed choice (RR = 1.86; 95% CI: 1.38 to 2.50; p < 0.0001), but did not change the intention of women deciding to be screened or affect decision regret. Conclusion: This analysis showed the positive effect of web-based DAs on patient-centered outcomes in breast cancer screening. In the future, more internet devices and free or larger discount WI-FI should be established to ensure more women can benefit from this effective tool.
Mammography screening for breast cancer is an effective breast examination measure and is recommended as a primary screening procedure for asymptomatic women to detect breast cancer at its earliest stage [1]. The ultimate goal of mammography screening is to reduce the mortality of breast cancer [2]. Some trials have demonstrated that mammography reduces breast cancer mortality by about 20% for women of different ages at general risk [3], but these data and increasing evidence about the harms of mammography screening have generated controversy. Initiating biennial screening at age 40 years (vs 50 years) reduced mortality by an additional 3% (range, 1–6%) [4], the net benefit is less, consume more resources and produce more false-positive results (false positives are abnormalities detected that are found to not be disease after additional [5], and with annual screening, which will increase false positive and would also be expected to increase overdiagnosis (overdiagnosis is a diagnosis of breast cancer that would not have caused harm) [6] and overtreatment (overtreatment is defined as treatment of cancer that would not have negatively affected a woman's health in her lifetime) [7]. Screening every 2 years after the age of 69 can further reduce mortality in all models, but due to older age, more comorbidities as well as shortening life expectancy, the overdiagnosis of the elderly population is the most obvious [4,8,9].
The concerns about overdiagnosis have emphasized the importance of providing information on the benefits and harms of screening with mammography, so that women can actively participate in decision-making and make an informed choice based on their values and preferences. However, current information on mammography screening for women usually overestimate the benefits and underestimate the harms of screening [10]. As a result, women generally tend to have biased expectations of the benefits and harms of health interventions [11]. Allen et al. demonstrated that since the release of the revised US Preventive Services Task Force (USPSTF) screening mammogram guidelines, women have experienced confusion, anxiety and lack of confidence in the current screening guidelines and even when based on the same evidence, cancer screening guidelines can differ among different organizations and can create confusion among the public, healthcare providers and policy makers [12]. There is a high net benefit for the average risk of mammography for women of 50–74 years of age with an average risk for breast cancer. But only a few organizations recommend 40–50 for breast cancer screening [13,14]. After reviewing the available evidence, the USPSTF issued a recommendation in 2016 that the decision to start mammography for women before 50 years of age should be a separate decision [13], and women who value potential benefits more than potential harm can choose to be screened every 2 years from 40 to 49 years old (Recommendation C), and patients should make decision about whether to accept screening based on their values and preferences with their doctors. Similarly, American College of Physicians (ACP) recommends that in average-risk women aged 40–49 years, clinicians should discuss whether they should be screened for breast cancer by mammography before the age of 50. The discussion should include potential benefits and harms as well as women's preferences [14]. In fact, American College of Obstetricians and Gynecologists (ACOG), Canadian Task Force on Preventive HealthCare (CTFPHC) and American Cancer Society (ACS) support joint shared decision making (SDM) process for breast cancer screening that consider patient preferences [15–17]. How to communicate balanced information about the pros and cons of mammography screening to women facing screening, and encourage them to participant in SDM process with healthcare professionals has become the focus of global attention. According to the International Patient Decision Aids Standards (IPDAS) Collaboration, decision aids (DAs) are defined as evidence-based tools designed to help people participate in decision making about healthcare options. They provide information on the options and help patients clarify and communicate the personal value they associate with different features of the options [18]. DAs may facilitate SDM by providing a common understanding of the risks and benefits associated with screening choices, tailored, when possible, to each patient's value. The Cochrance systematic review and meta-analysis assessing the impact of DAs for screening decisions concluded that DAs, which clearly state the decisions that need to be considered, provide evidence-based information about health status, options, related benefits, hazards, probability and scientific uncertainty and help patients recognize the sensitivity of decision-making to value and clarify their value to benefits and harms implicitly or explicitly, can increase patient knowledge, make people feel clearer about their values, reduce decision conflict and promote an active patient role in decision making [19]. But the authors stated that more studies are needed to deepen understanding of formats such as web-based DAs. In addition, if new studies can be included in the analysis, it may be possible to sort out the reasons for heterogeneity of different results (e.g., the formats of the DAs).
‘Delivering DAs on the Web’ is defined as the process of using the Internet to provide some or all components of DAs to help individuals (e.g., patients, caregivers, etc.) involved in the process of choosing between two or more medically appropriate healthcare options (e.g., preference-sensitive care) [20]. The purpose of this definition is to distinguish web-based DAs that support SDM from online health education websites, clinical practice guidelines, clinicians' decision support or expert systems [21]. This broad conceptual definition covers a range of operating methods, from providing downloadable copies of paper-based DAs to online streaming of DAs to providing interactive decision support websites that can be tailored to each individual's needs and preferences. Web-based DAs is a kind of subcategories of Web delivery, it can be described as DAs that were specifically designed and tested for use on the web. Examples include websites designed to help patients with specific healthcare decisions by interactively tailoring information and support to their needs, or by providing opportunities for family members to participate in the discussion. Web-based DAs often have the following characteristics, such as, interactivity (individuals can navigate the content and/or respond to interactive questions), dynamic (the content it provides can be different according to user input and interaction, or change according to user, time, data correction, etc.), tailored (It can be used to construct evidence based on patient demographics or clinical conditions, so that only feasible treatment options can be proposed and the associated risks and benefits can be estimated more accurately), etc. [20,22]. The IPDAS Collaboration has identified 12 dimensions to assess the quality of DAs, one of which is the delivery of web-based DAs [18]. In fact, the updated theoretical rationale and emerging evidence suggest potential benefits to delivering Wed-based DAs on quality of decision making by engaging patients in decision making beyond traditional static approaches, such as, it can spread information widely for a long time, and this information can be customized according to the needs and preferences of patients [20]. Therefore, IPDAS emphasizes the need for a comprehensive and systematic review of the web-based DAs [20]. In summary, the purpose of this systematic review and meta-analysis is to evaluate the effectiveness of web-based delivery of DAs in order to improve women's decision-making ability to the mammography screening. To our knowledge, ours is the first systematic review and meta-analysis to explore the web-based DAs intervention effect in breast cancer screening. We sought to investigate their impact on decision quality for women making a screening decision regarding breast cancer.
Materials & methods
This systematic review and meta-analysis was designed and conducted according to the principles of the PRISMA statement for reporting of systematic reviews and meta-analyses [23].
Search strategy
We performed a literature search to identify articles published before February 2020 using the following databases: Cochrane CENTRAL databases, Embase, Web of Science and Pubmed. We selected these databases since they focus on health, nursing and psychology publications. By using extensive search terms and including published papers and conference abstracts, the search strategy (Supplementary Material 1) is designed to be most inclusive. DAs was defined as: a tool or technology, web-based or application (app) and containing information about two or more options and the associated relevant decision-related outcomes. The IPDAS checklist enabled broad assessments in 12 dimensions, however, the checklist is not intended to provide an accurate, quantitative, assessments, so the quality of DAs can be judged on the project, dimension or global level. In addition, since not all checklist items are applicable to the comparability of each DAs, even at the checklist level, was not possible [24]. So, the IPDAs has established quality criteria for development and assessment of DAs: providing information in sufficient detail, presenting probabilities in an unbiased manner, including methods to clarify values and preferences, providing structured guidance for deliberation and communication, presenting information in a balanced manner, using a systematic development process, using up-to-date evidence, disclosing conflicts of interest, using plain language and ensuring that the decision is informed and values-based [18]. The reference lists of included studies and relevant articles were hand-searched to identify additional eligible publications. Letters, case series, case reports, comments, review articles and conference abstracts were excluded because of their limited datasets.
Eligibility & exclusion criteria
Eligibility criteria included reported data from primary studies; included data about women aged 50 and below who had not been diagnosed with breast cancer; contained an intervention that were web-based DAs. The intervention evaluated in the study had to be DAs, defined as information provided about the pros and cons of at least two screening options (including no screening) that allows the user to consider trade-offs between options. Trials that compared DAs to one or more comparators (e.g., control condition, general breast cancer screening information, other DAs) had to have at least a post-evaluation. For interventions to be considered web-based, they had to correspond to any program accessed over a network connection using HTTP or through a Web-based APP, according to this definition, materials such as CD or DVDs, although computer-based, were not considered web-based [25].The studies were randomized controlled trials (RCTs), non-randomized studies, cohort studies, case–control studies or before–after studies. Nonrandomized studies or those studies that compared outcomes with a within-subjects design had to report a pre–post evaluation, that is, a comparison of outcomes measured before and after the patient viewed the DAs. Thus, studies with such interventions were excluded and publications were excluded if they did not meet the eligibility criteria or if they addressed the question of promoting adherence of breast cancer screening. We included studies in which at least one quality of decision-making outcomes (e.g., informed choice, knowledge, decision conflict, intention to screening and decision regret) was reported. There were no language restrictions. There were no restrictions regarding the year of publication or the publication status.
Paper coding
After removing the duplicate results, titles and abstracts were screened according to the eligibility criteria independently by two reviewers (Yu, Yang). They were rejected if the reviewers determined from the title or abstract that the study did not meet the eligibility criteria. After this screening process, full texts were retrieved and further assessed for eligibility independently by two reviewers. Any disagreement was solved by discussion among the reviewers.
Data extraction
One reviewer (Yu) extracted the study characteristics and outcome data from the included studies. The two reviewers (Yu, Yang) extracted and assessed the following data for accuracy and completeness: author; year of publication; country; type of study; patient demographic and clinical information; the time of follow-up; measures of intervention and control and patient-reported outcomes. For RCTs, data were obtained for control and intervention groups. For before–after studies, data were abstracted for pre/post-intervention. Two reviewers (Guo, Zhang) compared the findings independently. We contacted authors to obtain missing data. We evaluated the effects of the DAs based on the outcomes used in the studies.
Assessment of risk of bias in included studies
The quality of RCTs was evaluated using the Cochrane Collaborations' risk of bias tool [26]. This tool uses seven criterias to measure quality. For studies that did not randomize patients, The quality of the before–after studies was evaluated with the risk of bias. In Nonrandomised Studies-of Interventions (ROBINS-I) assessment tool, which is recommended for quality assessment of nonrandomised studies of interventions [27]. This tool uses six bias domains to measure quality. Each domain was judged to have a low, moderate, serious or critical risk of bias. Only if all the criterias would be rated as having a low risk of bias, the study receives an overall rating of ‘low’. If one criterion of a study was considered as ‘high risk’, the study was classified as having a high risk of bias over all. The evaluation of study quality was performed independently by two reviewers (Yu, Yang). A third reviewer (Guo) was consulted in case of disagreement of item ratings. No study was excluded based on quality assessment.
Statistical analysis
Statistical analysis was performed using Review Manager (RevMan version 5.3). We used mean differences (MD) for continuous variables that were measured with the same instrument, standardized mean differences (SMD) when a similar outcome was assessed with different instruments and relative risks (RR) for dichotomous variables, if at least two same designed studies assessed the similar outcome. We used the Cochrane Q statistic and assessed I2 value to estimate statistical heterogeneity. The Cochrane Q statistic was based on a p-value. If the p-value was less than 0.05, there was heterogeneity between included studies. Among the outcome measures, the percentage of the heterogeneity was quantified by the I2 value, which were perceived as moderate (more than 25%) and high heterogeneity (more than 50%), separately. When high heterogeneity was showed (p < 0.05 or I2 >50%), we implemented the random-effects model, otherwise, we applied the fixed-effects model. Neither funnel plots nor the Egger test was used to examine the effect of publication bias, since only five studies were ultimately included in the analysis [28].
Results
Study selection
The search initially yielded 1097 articles, additional records identified through manual search of the reference lists was 1 article, 112 articles after duplicates removed, of which 955 were excluded upon systematic review of titles and abstracts against selection criteria (Figure 1). Among the 31 remaining articles, 26 were excluded after systematic full text review of the articles against selection criteria.

Figure 1. Study flow diagram.
MA: Meta-analysis; SR: Systematic review.
Characteristics of eligible studies
Data were extracted from all five selected studies (Table 1). Of these, three were RCTs [29–33] while the other two were uncontrolled before–after studies [32,33]. All five studies measured women who are facing the choice of screening mammography. These data were available for all trials, which randomized 1731 patients. Data for 126 women from before–after studies were included; the meta-analysis included a total of 1857 women from five studies. Five DAs for breast cancer screening used a web-based format. The studies were published between 2010 and 2019, three studies were conducted in United States [31–33], one in Australia [29] and one in Germany [30]. Participants' characteristics are shown in Table 1. Means of age were located in the 38–50 years interval. There are differences between studies in the prevalence of previous mammograms and in education level. Women in all studies have higher education levels, and most women had a statutory health insurance [21,33] or were offered biennial mammography screening free of charge for all women over the age of 40 [29]. Except Reder et al. did not report at what level women are at risk [30], the majority of women included in the studies were assessed as being at average risk [29,32,33].
| Citation | Design | Country | Patients | Clarifying values | Intervention | Control | Timing of assessment first follow-up | Primary and secondary outcome | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Number of interventions, age in years, range | Number of control, average age | No. at baseline (in before–after) | Assessed breast cancer risk | ||||||||
| Mathieu et al. (2010) | RCT | Australia | 117, 38–45 | 209, 38–45 | N/A | Yes† | Yes | DAs to identify women's knowledge of the benefits and harms of screening for breast cancer. The web-based DAs were based on a previously developed and evaluated paper-based DAs, modified to provide age-appropriate data. Both DAs were developed according to standard guidelines and underwent extensive consumer pilot testing | Patients did not have access to the DAs until they were offered to answer outcome questions | After intervention | Knowledge Intention, value, informed choice, anxiety, acceptablity |
| Reder et al. (2017) | RCT | Germany | 602, 50 | 604, 50 | N/A | No | Yes | DAs to increase informed choice about mammography screening program participation, The DAs were conceptualized as an interactive online tool consisting of a static information part and an interactive part. In line with IPDAS criteria. DAs propose a choice of options in the context of decision-making. The advantages and disadvantages of MSP and their probabilities are described. These include the possibility of absolute numbers supported by the graphical representation of positive and negative screening results, and explain overdiagnosis, overtreatment and procedures after positive results | A brochure contained written and numerical information about the MSP | After intervention three months | Informed choice knowledge, attitude, intention and uptake, decision conflict, decision regret, decision stage |
| Schapira et al. (2019) | RCT | USA | 102, 40–49 | 102, 40–49 | N/A | Yes | Yes | DAs to strengthen the relationship between individual risk and the decision to initiate BCS, knowledge and decision conflict. The web-based DAs were developed using a framework of SDM, incorporating exemplification theory and in line with IPDAS criteria. Content included: Breast Cancer Risk Assessment Tool; an introduction to the decision problem; a table outlining USPSTF and ACS guidelines; comparison of mortality reduction attributed to mammography between women 40–49 and 50–59 years of age; pictographs depicting outcomes of mammography; pictographs comparing 10-year and lifetime risk for the individual woman to an average-risk woman the same age; exemplars that demonstrated women considering the impact of breast cancer risk on their decisions about when to initiate mammography; and a value clarification exercise | Participants randomized to the control group were asked to fill out a breast cancer risk assessment after randomization and then proceeded with usual care | After intervention twelve months | Association between NCI-BCRAT-determined lifetime breast cancer risk and initiation of mammography screening, knowledge, decision conflict breast cancer worry, anticipated regret and the accuracy of risk perceptions, intentions regarding age of initiation of mammography |
| Scariati et al. (2015) | Before–after study | USA | 51, 38–48 | N/A | 51 | Yes | Yes | DAs to promote a shared decision making process with women's provider to make an individualized choice about screening mammography. Recommendations included replacing terms like ‘false negatives’ with plain language such as, ‘results that say you don't have cancer when you actually do.’, and a decision tree diagrams with flash animations or explanatory text, providing the user with hyperlinks to definitions of more complex words or potentially confusing concepts. Women can access the risk assessment on a personal computer through the internet with a username and password | N/A | After intervention | Decision conflict, intention, value |
| Eden et al. (2015) | Before–after study | USA | 75, 40–49 | N/A | 75 | Yes | No | ‘Mammography DAs as a web-based application’. They use IPDAs as a web-based application for mammography DAs. This module is based on several decision-making theories derived from descriptive analyses about how people use information to make difficult decisions. The Mammopad DAs include a breast cancer risk assessment component with the same questions from the B-RST instrument that were used to determine eligibility for the study. The Mammopad DAs also contains separate modules providing information about breast cancer and mammography and a priority setting activity | N/A | After intervention | Decision conflict, decision self-efficacy. The preparation for decision making |
†
Women were eligible for the study if they were not previously diagnosed with breast cancer.
DA: Decision aid.
Breast cancer screening DAs intervention characteristics
All DAs were computerized and presented screening information as text and diagrams [29–33]. Only one of these five used APP to provide information to women [32]. The authors of all studies reported using IPDAS when creating DAs [29–33], however, the level of IPDAS implementation differed among the DAs. Two DAs were developed using a decision support framework at the same time [31,32]. The DAs in Schapira et al. were developed using the SDM framework in conjunction with incorporating exemplification theory [34,35]. The theory shows that experienced and directly or indirectly witnessed events will affect subjective risk perception, support risk information processing and promote behavior change [36,37]. The DAs in Eden et al. greatly borrowed from the theory of decision conflicts, which recognizes the competitive gains and losses of each choice. To address this potential conflict, women set priorities between the benefits and harms of breast cancer screening [38]. All web-based DAs included: information about the pros and cons of breast cancer screening, introduction to decision-making issues, charts and pictographs to express some confusion concepts, such as: overdiagnosis, false positives, etc. and the risk of breast cancer in different young segments. Three DAs contained an algorithm that assessed the risk of breast cancer in users and gave women described risk factors that could lead to breast cancer [31–33]. Four DAs contained a valuable clarification technique involving rating the importance of selected factors, which can help women to clarify their values and preferences in the context of breast cancer screening [29–31,33].
Outcome
Knowledge
Knowledge refers to the test results on the improvement of women's knowledge on specific topics targeted by DAs design. Three RCTs of the included studies reported the scores of knowledge [29–31]. The questions in Mathieu et al. were comprised of four numerical and five concept questions [29]. Reder et al. used a seven multiple choice items, six questions assessed conceptual knowledge and only one question assessed numerical knowledge with four value ranges as response options [30]. Schapira et al. assessed knowledge with five multiple-choice questions [31]. Overall, compared with the control groups, women who use the DAs have higher scores in knowledge, the SMD for pooled data from three RCTs was 0.69 (95% CI: 0.57–0.80, p < 0.00001). The heterogeneity is 37%, p = 0.21. The great variability of topics and questionnaires used to assess the knowledge of each included study may help us to explain the heterogeneity for this specific variable (Figure 2).
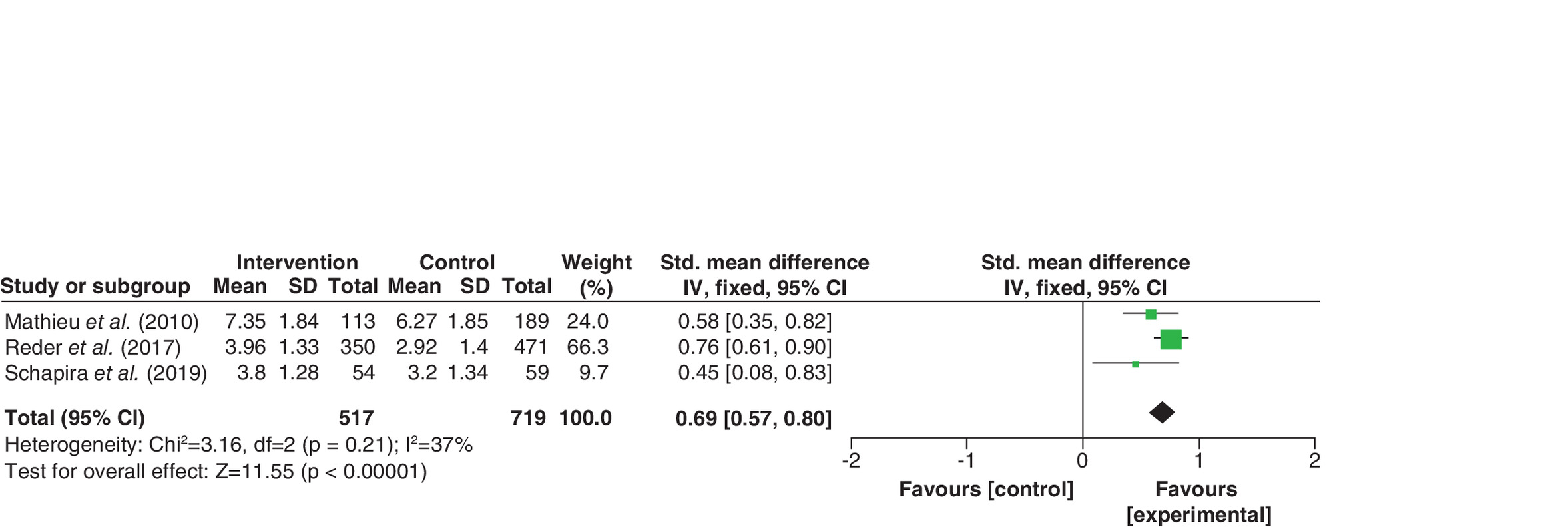
Figure 2. Forest plots of standardized mean differences for knowledge.
IV: Inverse variance; SD: Standard deviation.
Intention to screening
In established models of healthy behavior change, intention is a recognized indicator of future behavior [39]. Four studies of the included studies demonstrated the proportion of women who intended to screening [29,30,32,33]. The meta-analysis of the RCTs [29,30] and before–after studies [32,33] showed there was no significant difference in the intention to screening respectively, 95% CI (0.85–1.06, p = 0.33), 95% CI (0.82–1.13, p = 0.28). For RCTs, we found that the heterogeneity was small (I2 = 17%, p = 0.23). For before–after studies, we found that there was no significant heterogeneity. (I2 = 0%, p = 0.73; Figure 3).
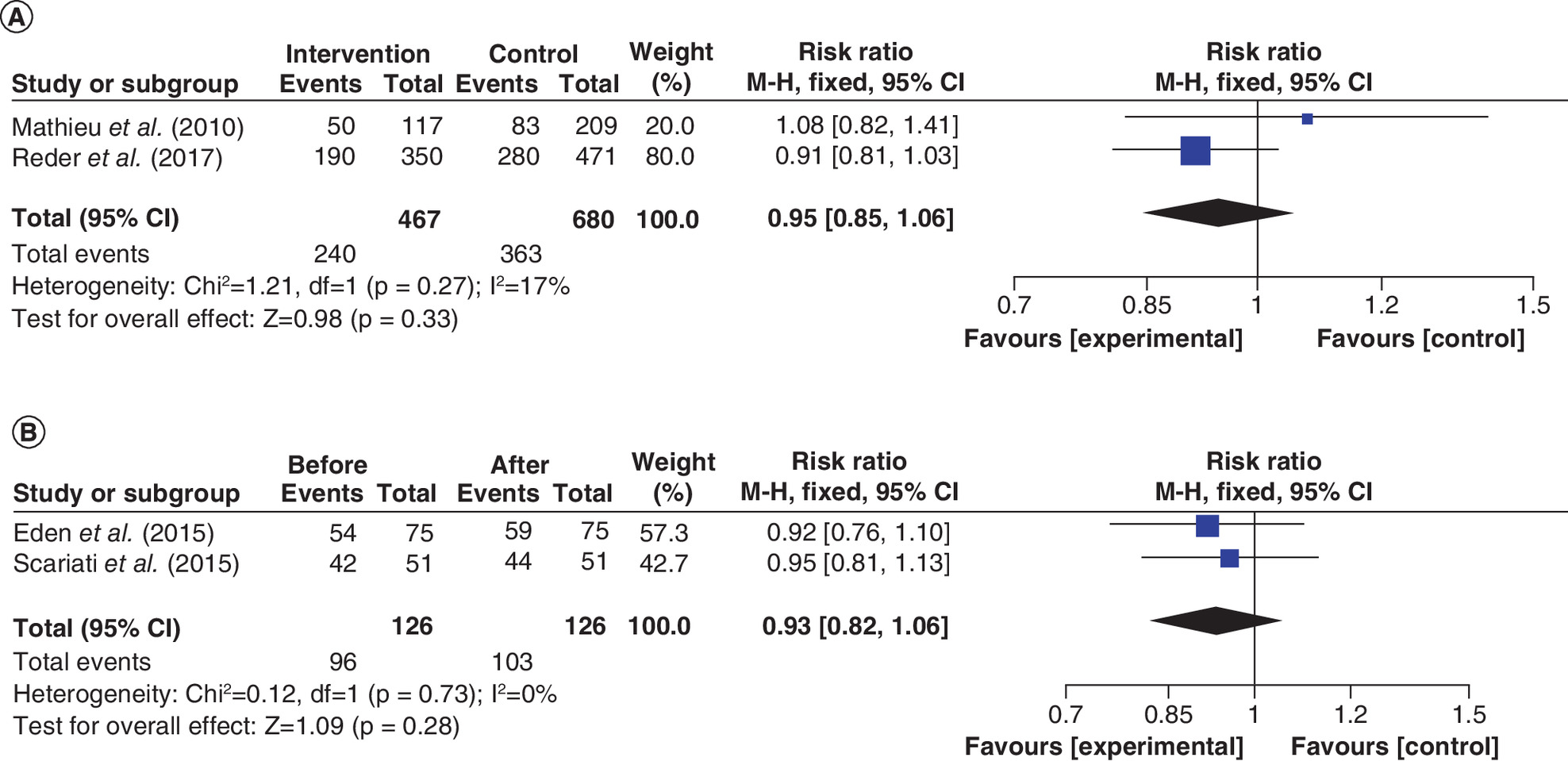
Figure 3. Forest plots of risk ratio for intention to screening.
(A) Randomized controlled trials, (B) before–after study.
Informed choice
If a woman had adequate knowledge and her attitudes and intentions were consistent (positive attitudes and intentions, or negative attitudes and intentions), then she was judged to have made an informed choice [40]. There were two RCTs [29,30] and two before–after studies [32,33] assessing the condition of women who felt informed. The DAs increased the proportion of women who making an informed decision, 58.0 versus 36.5% according to Mathieu et al. [29] and 40.6 versus 18.9% according to Reder et al. [30]. Analysis of the overall effect of two RCTs indicated that, compared with usual care interventions, DAs resulted in a statistically significant increase in the proportion of women making informed choice. The meta-analysis of two RCTs comparing the informed choice that the woman making for having a mammography screening was 1.86 (95% CI: 1.38–2.50, p < 0.0001). Two before–after studies [32,33] did not report the percentage of woman who making informed choice directly, they used scores of the subscales of the low-literacy version of the O'Connor's Decisional Conflict Scale (DCS) [41] to show whether they felt informed when they facing screening mammography. Their result reported that women, after using DAs, felt significantly more informed when making a decision about when they should begin screening mammography. The MD for pooled data from two before–after studies was 38.38 (95% CI: 32.61–44.15, p < 0.00001). The heterogeneity in each study was great (I2 = 69%, p = 0.07), so we used the random-effects model to analyze the data collected (Figure 4).
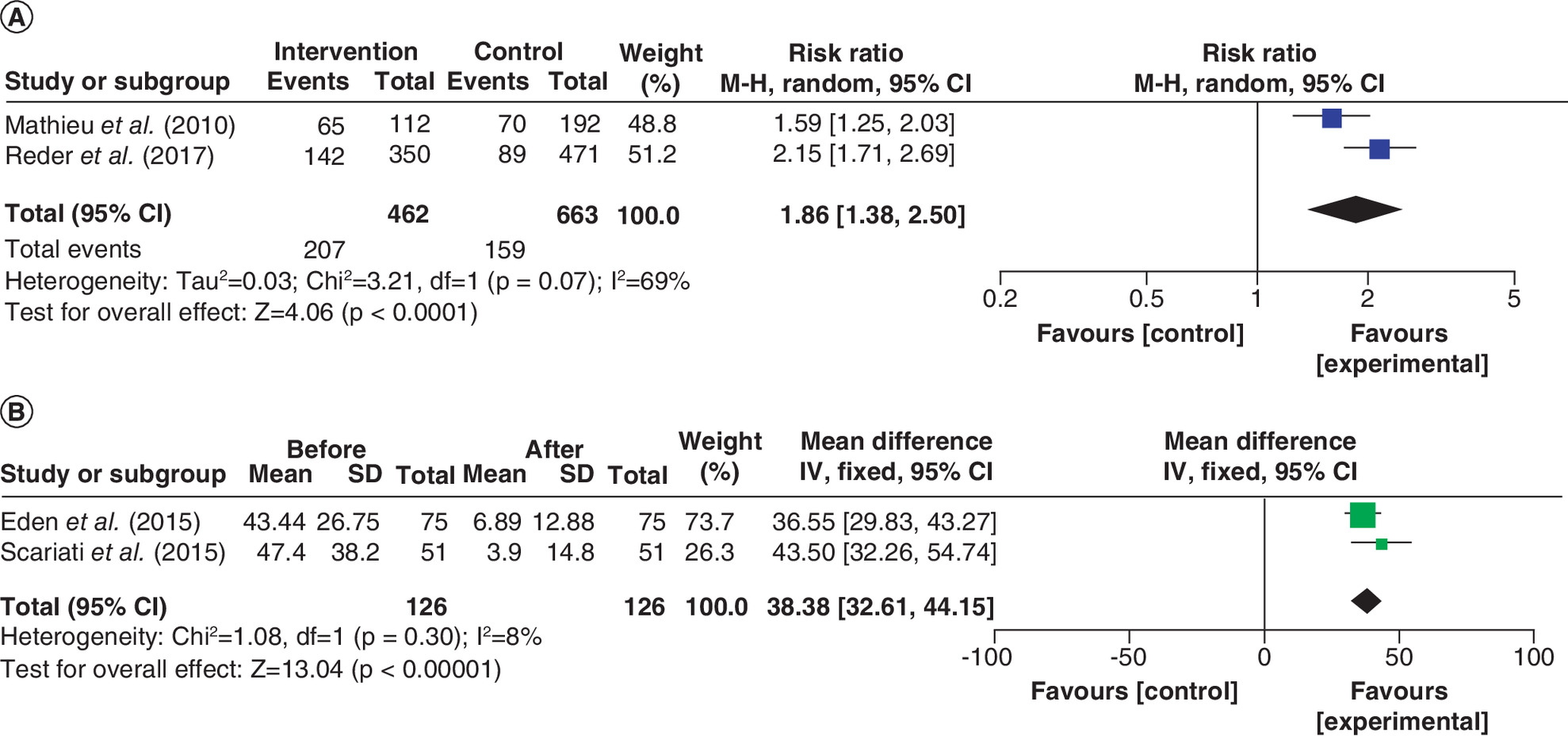
Figure 4. Forest plots of standardized mean differences for making informed choice and forest plots of risk ratio for making informed choice.
(A) Randomized controlled trials, (B) Before–after study.
M-H: Mantel-Haenszel.
Decision conflict
Decision conflict is a state of uncertainty about the preferred course of action, which often occurs when choices involve risks or uncertainties of outcomes, high risks of potential gains and losses and anticipated regret about the positive aspects of rejected options [42]. The effect of interventions on decision conflict was assessed by four studies [29–33]. Two before–after studies [32,33] used the low-literacy version of DCS to calculate the scores of decision conflict [41], one RCT [29] used the DCS [36], while another RCT [30] used a 4-item SURE (Sure of myself; Understand information; Risk–benefit ratio; Encouragement) [43]. The MD for pooled data from two before–after studies was 0.68 (95% CI: -1.46 to 2.83, p < 0.00001). It demonstrated that women who used the DAs had less decision conflict. The SMD for pooled data from two RCTs was -0.40 (95% CI: -0.54 to -0.27, p < 0.00001), The result showed there was a great statically significant difference in overall decision conflict scores. For both RCTs and before–after studies, we found that there was no significant heterogeneity (I2 = 0%; Figure 5).
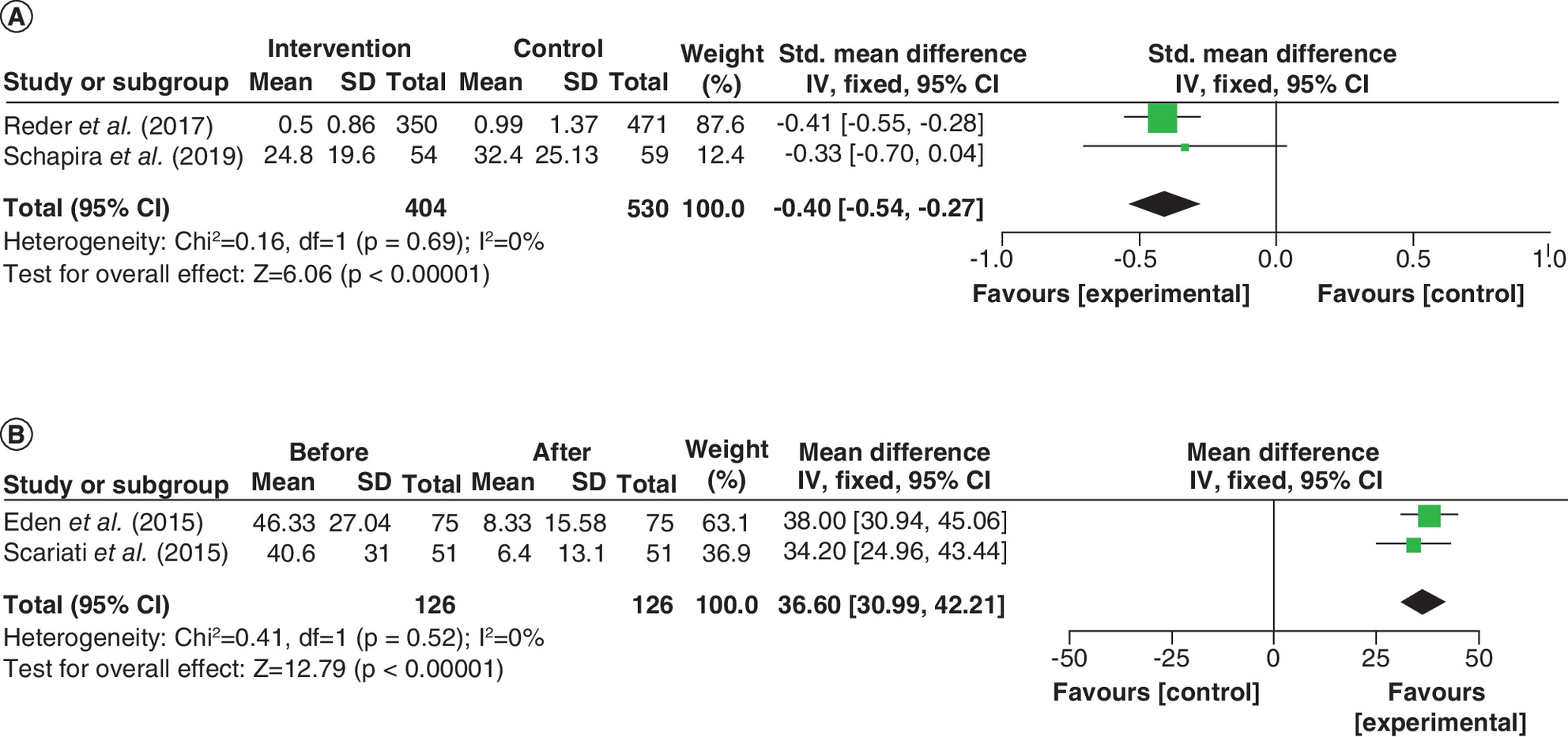
Figure 5. Forest plots of standardized mean differences for decision conflict and forest plots of mean differences for decision conflict.
(A) Randomized controlled trials, (B) Before–after study.
SD: Standard deviation.
Decision regret
Decision regret motivates people to undertake an action to avoid harmful future emotional consequences [44]. Indeed, decision regret is an indication to realize the self-reported health behaviors as well as objective behaviors such as attending for cancer screening. Two RCTs of the included studies reported the scores of decision regret. Reder et al. [30] used the Decision Regret Scale [45] to measure the scores of decision regret in the following 3 months, while Schapira et al. [31] used a 7-point Likert-type scale to measure the scores of decision regret in the next 12 months. The result showed no statically significant difference in overall decision regret scores, the SMD for pooled data from two RCTs was -0.03 (95% CI: -0.17 to 0.11, p = 0.66). The result showed that there was no significant heterogeneity among the studies (I2 = 0%, p = 0.66; Figure 6).

Figure 6. Forest plots of standardized mean differences for decision regret.
(A) Randomized controlled trials.
SD: Standard deviation.
Quality assessments
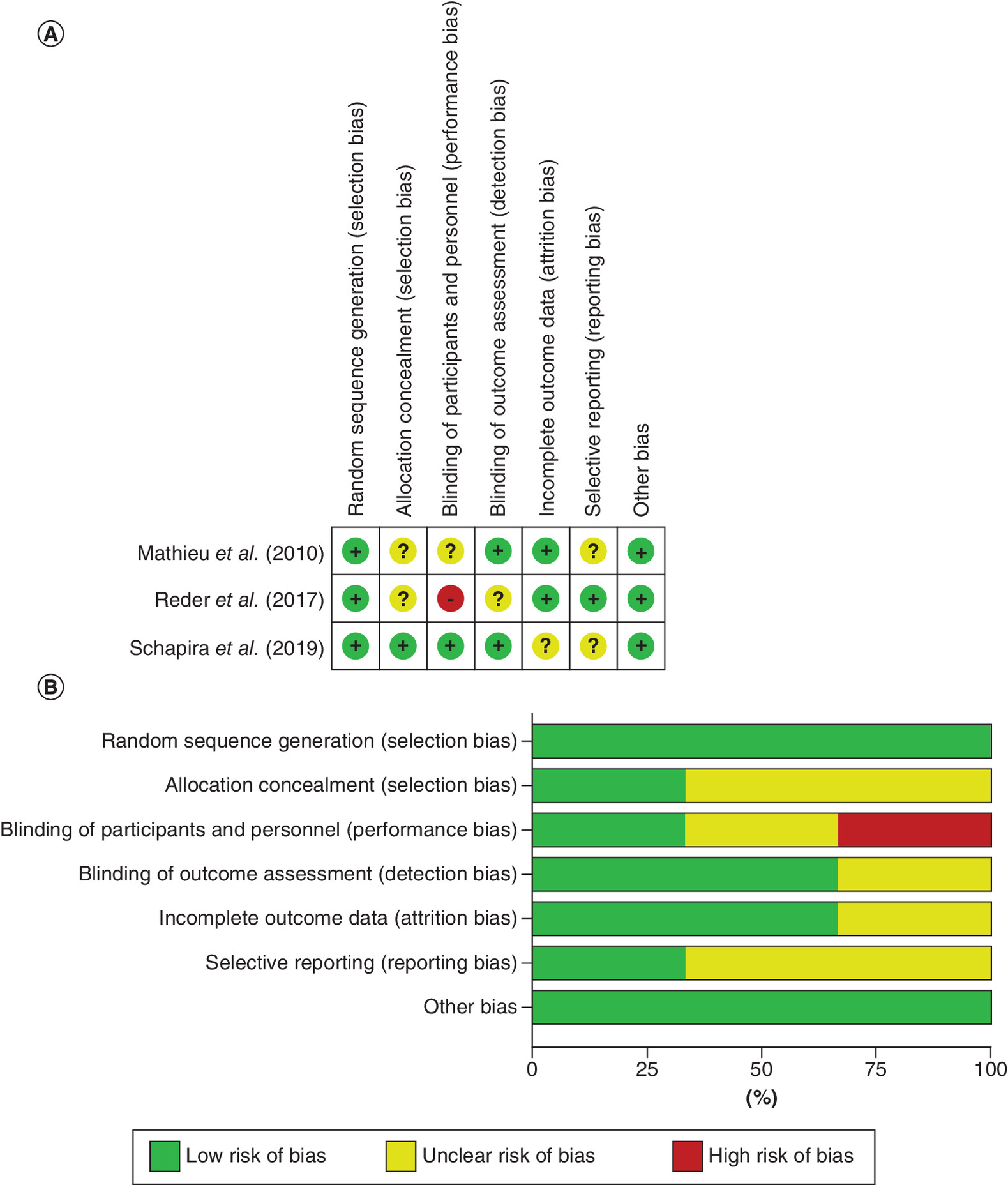
The included studies were limited by differences in outcomes, as well as by a potential lack of unifority in the educational information provided to the control groups. Random sequence generation was rated as being at low risk of bias in all of the RCTs [29–31]. Allocation concealment was considered low risk of bias in one RCT [31] and unclear risk in the remaining two RCTs [29,30]. Blinding of participants and personnel was assessed as being at unclear risk of bias in one RCT [29], high risk of bias in one RCT [30] and low risk of bias in one RCT [31]. Two RCTs [29,31] were evaluated as being a low risk of bias regarding blinding of outcome assessment and unclear risk of bias in one RCT [30]. Two RCTs were rated as low risk of attrition bias that relates to incomplete outcome data [29,30] and unclear risk of bias in one RCT [31]. Two RCTs [29,31] were classified as unclear risk of bias regarding selective reporting due to the lack of information about public registration of the trial protocol, the other one RCT [30] had a registered protocol and were rated as low risk of bias for the selective reporting parameter. When assessing other sources of bias, All RCTs [29-31] were rated as low or unclear risk of bias (Figure 7). Two before–after studies [32,33] in the domains confounding, deviations from intended interventions, selection of participants into the study, selection of the reported results, classification of interventions are at low risk and in missing data, measurement of outcomes are unclear. Overall, the quality analysis of RCTs showed that they had deficits concerning the blinding of participants, personnel, and/or outcome assessors (Figure 7). Two before–after studies were rated as having a low risk of bias. There were unclear in measurement of outcomes, the article did not provide sufficient information to judge the domain missing data. The bias in the other domains was rated as ‘low’.
Discussion
Summary & interpretation of main results
This systematic review and meta-analysis included three RCTs [29–31] and two before–after studies [31,33] assessing DAs given to women facing the decision to be screened with mammography. There are differences in the type and amount of information contained in DAs and the information provided to the control group, which may partially explain the significant heterogeneity in all assessment results. The overall conclusion from our review is that DAs, a key component of a high-quality decision-making process in SDM frameworks, significantly increase women's knowledge and the proportion of women making an informed choice, decrease the decision conflict, but do not significantly modify intentions toward screening and decrease decision regret.
Therefore, it is important not to overlook the basic principles of using DAs, that is, to help people participate in decision-making process in SDM frameworks, with the goal of promoting deliberation between patients, healthcare providers and other stakeholders [19]. They provide information about options and help patients construct, clarify, and communicate their personal values, thereby helping patients make high-quality decisions [19,20]. This review shows that compared with usual care, patients receiving DAs have more knowledge, and according to the three-dimensional classification framework of Marteau et al. [40] knowledge about the screening, attitude toward the screening and intention/uptake (depending on measurement point), knowledge is a key component of informed choice.
Our results are in line with those from other systematic reviews and meta-analyses indicating the superiority of DAs (in any format) in comparison with usual care [19,46–48]. Stacey et al., in a Cochrane meta-analysis of DAs for people facing screening or treatment issues, found DAs to improve people's knowledge, reduce decision conflict, promote an active patient role in decision making, and of 105 studies, seven studies assessed decision regret and only one reported statistically significant differences [19]. Only two studies measured decision regret and used different scales, which limited our conclusions. Recent literature suggested that decision regret may be an inducement in daily decision-making and cancer screening decisions, and may be an important basis for future research on DAs [44]. Therefore, it is recommended that future studies include decision regret into the outcome indicators, and use Decision Regret Scale with good reliability and validity to measure, so as to in-depth study of women's decision regret when facing breast cancer screening [45].
Montserrat et al. [46] indicated that DAs(in any format) for breast cancer screening can improve knowledge and promote informed choice, in accordance with their preferences, for women who face the decision of screening, but do not significantly modify attitudes or intentions toward screening and they found divergent results on decision conflict and decision confidence. We do not yet know how effectively women will use the web-based DAs on smartphones, or computers compared with their effective use of the paper-based or video-based. However, different forms of DAs can be used according to the patient's personal preferences. Therefore, it is one of research topics in future to compare the impact of these alternative DAs formats for women who are in face of breast cancer screening.
Eden et al. [32] stated that some clinics scanned the report of women from Mammopad and attached it to the electronic medical records (EMRs) for women facing breast cancer screening. Future research may provide a more seamless workflow, such as providing decision support through EMRs before they visit the Clinical staff. It is appropriate to use the EMRs to promote SDM, because the use of EMRs is high, with approximately 75% of Canadian and American doctors using EMRs [49]. Therefore, we hypothesize that in a busy daily practice environment, with limited time to have a conversation with patients, web-based DAs may have enormous potential to be linked or integrated into EMRs, thus providing a mechanism to ensuring a consistent approach to SDM and promoting continuity of care when women may be seen by multiple health professors, making it easy for patients to access and review materials prior to the encounter with the physician, which may facilitate the process of SDM [50]. Contrary to our result, Ivlev et al. revealed that the implementation of DAs for breast cancer screening in clinical practice at the national level may result in a 77% increase in the number of women aged 38–50 who would not want to begin mammography screening, compared with the corresponding number of women under usual care [47]. But our findings are consistent with Stacy et al. [18], except in the case of prostate cancer screening, with little evidence of the impact of DAs on the intention of screening.
Strengths & limitations
Several limitations must be considered while analyzing our conclusions. First, the number of qualified studies is small, so it is difficult to assess publication bias and when the meta-analysis contains relatively few studies, therefore, these conclusions should be preliminary. Second, the broad theories and frameworks that guide the development of DAs fail to explore the impact of specific theories on patients' decision in detail [31,32]. Hence, more research are needed to better understand how the theoretic underpinnings of DAs influence their effectiveness and address the gap between theory and practice [51]. Third, the broad definition of DAs was used and the content of DAs used in the studies was not developed and evaluated according to IPDAS. Some studies have shown that low-quality DAs can negatively affect patients. Durand et al. assessed 30 DAs for breast cancer, prostate cancer and colon cancer screening with IPDAS, of which 25 met the qualified criteria and only 3 met the certification criteria, suggesting the need to improve the quality of DAs [52]. Fourth, compared with control groups, more studies are needed to determine which patient groups are most likely to benefit from DAs. For example, it is recommended to develop, use and evaluate DAs for people with lower literacy [53]. It is worth noting that most of trials in this review focused on highly educated, with more health conscious than the general population. Research shows that effectively using DAs may be affected by the user's health literacy [54]. People with lower health literacy are less likely to benefit from health education materials, because they may have difficulties in understanding information and are therefore less likely to acquire new knowledge [52]. Importantly, women with low health literacy also lack the numeracy skills to understand the likelihood of benefits and harms of mammography screening. For example, Davis et al. demonstrated that lower performance on the Rapid Estimate of Adult Literacy in Medicine (REALM) was associated with lower screening mammography knowledge [55]. More trials should target these populations and investigate the delivery of DAs in different clinical settings. Fifth, many health-related decisions, such as screening decisions, have a long duration, breast cancer screening decision may have to be made by women multiple times in their lifetime, so the lack of long-term follow-up in the included studies also limits people's understanding of the impact of Web-based DAs over time. Schapira et al. was the study with the longest follow-up (12 months) [31]. A longer follow-up and longitudinal outcomes would have made it possible to assess knowledge decline or retention, and the long-term impact on screening participation. Our results remind us that even if statistical information are effectively communicated, participants may not make estimates of the same order of magnitude after a few weeks.
Future research
On the one hand, one advantage of DAs is to promote the process of SDM between clinicians, patients and other stakeholders [18]. Clinicians is one of the main bodies of SDM, and their cognitive degree of DAs determines whether DAs can be provided to patients at the right time and in the right situation [56]. The higher degree the medical staff's awareness of DAs, the greater the probability recommended to patients, the higher the utilization rate of decision-making assistance in clinical practice [57]. However, Wyatt et al. reported that clinicians used DAs in clinical setting only partially and inconsistently [58], so, to increase the compliance of screening women with DAs, clinical training on the use of DAs and SDM practices for clinicians may be required to facilitate the implementation of DAs and promote a more ideal-type of SDM [59]. On the other hand, as the treatment routine will be continuously improved with the development of medical treatment technology, any DAs, whether fully validated or not, needs to be updated regularly to incorporate new research findings and advances in modes of treatment and prevention, as well as new recommendations put forth by professional groups, so as to ensure the effectiveness of DAs and its relevance with clinical practice. In summary, the technological capabilities of mobile technology are continuing to develop at high speed, and provide us with an unprecedented opportunity to apply digital technology to prevent and manage health conditions [60]. There are potential economic benefit because it is easy to provide web-based DAs to a large number of people (for example, mobile technology applications can be easily downloaded, and automated systems can provide a large number of people with low-cost website links). This technology makes the DAs more personalized and interactive [20]. However, despite the fact that the Internet has become an easily accessible tool, a persistent digital divide still exists [61]. Therefore, special attention should be paid to the socio-demographic characteristics of the population, and more medical infrastructure resources should be built for underserved communities, and free or discounted Wi-Fi connections and mobile devices should be provided for low-income areas. These actions, in combination with the popularity of smart phone users, these measures may narrow the digital divide [62,63].
Conclusion
This is the first systematic review and meta-analysis which test the effectiveness of web-based DA for women who are in face of breast cancer screening. Our work indicates that DAs may support women during their decision process for choosing a preventive measure. This is mainly achieved by improving decision-related outcomes. In the last several years, the internet has become even more widespread and easy to use with many public places providing it at no cost, which may be an important feature to increase access to DAs. There is growing demand for tools to support SDM in practice; a growing use of the Internet by users; and a need to build upon the numerous paper-based tools that have already been developed, tested, and implemented into care settings. Above all, the use of web-based DAs depends on the ability of computer access and technology, and if it is a web-based tool, it depends on the availability of good Internet services. The efficiency of web-based information tools may be hindered due to resource constraints, or even due to residential limitations (poor Internet access). Therefore, it should be addressed when studying the implementation of these tools in practice in the future.
•
Mammography has been found to reduce breast cancer mortality by about 20% for women of different ages at general risk, but these data and increasing evidence about the harms of mammography screening have generated controversy.
•
Because guidelines for screening for breast cancer for certain age groups are controversial, many experts have advocated the use of shared decision making (SDM) using validated decision aids (DAs), which can be presented in different formats (e.g., paper, multimedia and web-based).
•
How to communicate balanced information about the pros and cons of mammography screening to women facing screening, and encourage them to share decision making with healthcare professionals has become the focus of global attention.
•
According to the International Patient Decision Aids Standards (IPDAS) Collaboration, DAs are defined as evidence-based tools designed to help people participate in decision making about healthcare options.
•
‘Delivering DAs on the Web’ is defined as the process of using the internet to provide some or all components of DAs to help individuals (e.g., patients, caregivers, etc.) involved in the process of choosing between two or more medically-appropriate healthcare options (e.g., preference-sensitive care).
•
This systematic review and meta-analysis included three randomized controlled trials and two before–after studies assessing DAs given to women facing the decision whether to be screened using mammography.
•
The overall conclusion from our review is that DAs, a key component of a high-quality decision-making process in SDM frameworks, significantly increase women's knowledge and the proportion of women making an informed choice, decrease decision conflict, but do not significantly modify intentions toward screening or affect decision regret.
•
Web-based DAs are dynamic, tailored and interactive. Therefore, in the future, more internet devices and free or larger discount WI-FI should be established to ensure more women can benefit from this effective tool.
Author contributions
L Yu and W Zhang contributed to the conception and design of this study; L Yu and S Yang performed the statistical analysis and drafted the manuscript; P Li greatly helped in the manuscript revision process; N Liu, J Wang, PP Guo, XH Zhang and W Zhang critically reviewed the manuscript and supervised the whole study process. All the authors read and approved the final manuscript.
Acknowledgments
The authors thank to the students who took the time to become involved in the investigation.
Financial & competing interests disclosure
This research was financed by the China Postdoctoral Science Foundation (2019T120242). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Data sharing statement
The authors certify that this manuscript reports the secondary analysis of clinical trial data that have been shared with them, and that the use of this shared data is in accordance with the terms (if any) agreed upon their receipt. The source of this data is cited in the manuscript.
Supplementary Material
File (suppl_file.docx)
- Download
- 17.41 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Lauby-Secretan B, Scoccianti C, Loomis D et al. Breast cancer screening – viewpoint of the IARC Working Group. N. Engl. J. Med. 372(24), 2353–2358 (2015).
•• The pros and cons of breast cancer screening
2.
Lannin DR. Effect of screening mammography on breast cancer incidence. N. Engl. J. Med. 368(7), 677–678 (2013).
•• The pros and cons of breast cancer screening
3.
Myers ER, Moorman P, Gierisch JM et al. Benefits and harms of breast cancer screening: a systematic review. JAMA 314(15), 1615–1634 (2015).
•• The pros and cons of breast cancer screening.
4.
Mandelblatt JS. Effects of mammography screening under different screening schedules: model estimates of potential benefits and harms. Ann. Intern. Med. 151(10), 738 (2009).
•• The pros and cons of breast cancer screening
5.
Bond M, Garside R, Hyde C. A crisis of visibility: the psychological consequences of false-positive screening mammograms, an interview study. Br. J. Health Psychol. 20(4), 792–806 (2015).
•• The pros and cons of breast cancer screening
6.
Brodersen J, Schwartz LM, Heneghan C et al. Overdiagnosis: what it is and what it isn't. BMJ Evid. Based Med. 23(1), 1–3 (2018).
•• The pros and cons of breast cancer screening
7.
Qaseem A, Lin JS, Mustafa RA et al. Screening for breast cancer in average-risk women: a guidance statement from the American College of Physicians. Ann. Intern. Med. 170(8), 547–560 (2019).
•• The pros and cons of breast cancer screening
8.
Kerlikowske K, Zhu W, Hubbard RA et al. Breast Cancer Surveillance Consortium. Outcomes of screening mammography by frequency, breast density, and postmenopausal hormone therapy. JAMA Intern. Med. 173(9), 807–816 (2013).
•• The pros and cons of breast cancer screening
9.
Hubbard RA, Kerlikowske K, Flowers CI et al. Cumulative probability of false-positive recall or biopsy recommendation after 10 years of screening mammography: a cohort study. Ann. Intern. Med. 155(8), 481–492 (2011).
•• The pros and cons of breast cancer screening
10.
Waller J, Osborne K, Wardle J. Enthusiasm for cancer screening in Great Britain: a general population survey. Br. J. Cancer 112(3), 562–566 (2015).
•• The pros and cons of breast cancer screening
11.
Sutkowi-Hemstreet A, Vu M, Harris R et al. Adult patients' perspectives on the benefits and harms of overused screening tests: a qualitative study. J. Gen. Intern. Med. 30(11), 1618–1626 (2015).
•• The pros and cons of breast cancer screening
12.
Allen SV, Nes LS, Marnach ML et al. Patient understanding of the revised USPSTF screening mammogram guidelines: need for development of patient decision aids. BMC Womens Health 12, 36 (2012).
•• The pros and cons of breast cancer screening
13.
Nelson HD, Pappas M, Cantor A et al. Harms of breast cancer screening: systematic review to update the 2009 U.S. Preventive Services Task Force recommendation. Ann. Intern. Med. 164(4), 256 (2016).
•• The current status of screening guidelines
14.
Qaseem A, Lin JS, Mustafa RA et al. Screening for breast cancer in average-risk women: a guidance statement from the American College of Physicians. Ann. Intern. Med. 170(8), 547–560 (2019).
•• The current status of screening guidelines
15.
Oeffinger KC, Fontham ETH, Etzioni R et al. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA 314(15), 1599–1614 (2015).
•• The current status of screening guidelines
16.
Mango V, Bryce Y, Morris EA et al. ACOG practice bulletin July 2017: breast cancer risk assessment and screening in average-risk women. Br. J. Radiol. 91(1090), 20170907 (2018).
•• The current status of screening guidelines
17.
Klarenbach S, Sims-Jones N, Lewin G et al. Recommendations on screening for breast cancer in women aged 40–74 years who are not at increased risk for breast cancer. Can. Med. Assoc. J. 190(49), E1441–E1451 (2018).
•• the current status of screening guidelines
18.
Elwyn G, O'Connor A, Stacey D et al. Developing a quality criteria framework for patient decision aids: online international Delphi consensus process. BMJ 333(7565), 417 (2006).
•• A quality criteria framework for patient decision aids
19.
Stacey D, Légaré F, Lewis K et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst. Rev. 4(4), CD001431 (2017).
•• Application effect of decision aids
20.
Hoffman AS, Volk RJ, Saarimaki A et al. Delivering patient decision aids on the internet: definitions, theories, current evidence, and emerging research areas. BMC Med. Inform. Decis. Mak. 13(Suppl. 2), S13 (2013).
• Overview of web-based decision aids
21.
Rose AS, Tosteson ANA. Shared Decision Making. Encyclopedia of Medical Decision Making. Kattan MW (Ed.). 1036–1041 Sage Publications, CA, USA (2009).
• Overview of web-based decision aids
22.
Syrowatka A, Krömker D, Meguerditchian AN, Tamblyn R. Features of computer-based decision aids: systematic review, thematic synthesis, and meta-analyses. J. Med. Internet Res. 18(1), e20 (2016).
• Overview of web-based decision aids
23.
Liberati A, Altman DG, Tetzlaff J et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 339, b2700 (2009).
• Methodology of meta analysis
24.
Elwyn G, O'Connor AM, Bennett C et al. Assessing the quality of decision support technologies using the International Patient Decision Aid Standards instrument (IPDASi). PLoS ONE 4(3), e4705 (2009).
• Methodology of meta analysis
25.
Baptista S, Sampaio ET, Heleno B et al. Web-based versus usual care and other formats of decision aids to support prostate cancer screening decisions: systematic review and meta-analysis. J. Med. Internet Res. 20(6), e228 (2018).
• Methodology of meta analysis
26.
Higgins J, Green S. Cochrane Collaboration. Cochrane Handbook for Systematic Reviews for Interventions. Cochrane Database Syst. Rev. 2011(2), S38 (2011).
• Methodology of meta analysis
27.
Sterne JA, Hernan MA, Reeves BC et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 355, i4919 (2016).
• Methodology of meta analysis
28.
Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics 50(4), 1088–1101 (1995).
• Methodology of meta analysis
29.
Mathieu E, Barratt AL, McGeechan K, Davey HM, Howard K, Houssami N. Helping women make choices about mammography screening: an online randomized trial of a decision aid for 40-year-old women. Patient Educ Couns. 81(1), 63–72 (2010).
• Detailed content of web-based decision aids
30.
Maren R, Petra K. Does a decision aid improve informed choice in mammography screening? Results from a randomised controlled trial. PLoS ONE 12(12), e0189148 (2017).
• Detailed content of web-based decision aids
31.
Schapira MM, Hubbard RA, Seitz HH et al. The impact of a risk-based breast cancer screening decision aid on initiation of mammography among younger women: report of a randomized trial. MDM Policy Pract. 4(1), 2381468318812889 (2019).
• Detailed content of web-based decision aids
32.
Eden KB, Scariati P, Klein K et al. Mammography decision aid reduces decisional conflict for women in their forties considering screening. J. Womens Health (Larchmt). 24(12), 1013–1020 (2015).
• Detailed content of web-based decision aids
33.
Scariati P, Nelson L, Watson L, Bedrick S, Eden KB. Impact of a decision aid on reducing uncertainty: pilot study of women in their 40s and screening mammography. BMC Med. Inform. Decis. Mak. 15, 89 (2015).
• Detailed content of web-based decision aids
34.
Zillmann D. Exemplification effects in the promotion of safety and health. J. Commun. 56(S1), S221–S237 (2006).
• Detailed content of web-based decision aids
35.
Mundorf N, Zillmann D. Effects of story sequencing on affective reactions to broadcast news. J. Broadcast. Electron. Media 35(2), 197–211 (1991).
• Detailed content of web-based decision aids
36.
Tversky A, Kahneman D. Judgment under uncertainty: heuristics and biases. Science 185(4157), 17–34 (1974).
• Detailed content of web-based decision aids
37.
Tversky A, Kahneman D. The framing of decisions and the psychology of choice. Science 211(4481), 453–458 (1981).
• Detailed content of web-based decision aids
38.
Durand MA, Stiel M, Boivin J et al. Where is the theory? Evaluating the theoretical frameworks described in decision support technologies. Patient Educ. Couns. 71(1), 125–135 (2008).
• Detailed content of web-based decision aids
39.
Frosch DL, Legare F, Fishbein M, Elwyn G. Adjuncts or adversaries to shared decision-making? Applying the integrative model of behavior to the role and design of decision support interventions in healthcare interactions. Implement Sci. 4, 73 (2009).
• Detailed content of web-based decision aids
40.
Marteau TM, Dormandy E, Michie S. A measure of informed choice. Health Expect. 4(2), 99–108 (2001).
• Detailed content of web-based decision aids
41.
Linder SK, Swank PR, Vernon SW, Mullen PD, Morgan RO, Volk RJ. Validity of a low literacy version of the Decisional Conflict Scale. Patient Educ. Couns. 85(3), 521–524 (2011).
• Detailed content of web-based decision aids
42.
O'Connor AM. Validation of a decisional conflict scale. Med. Decis. Making 15(1), 25–30 (1995).
• Detailed content of web-based decision aids
43.
Ferron Parayre A, Labrecque M, Rousseau M et al. Validation of SURE, a four-item clinical checklist for detecting decisional conflict in patients. Med. Decis. Making 34(1), 54–62 (2014).
• Detailed content of web-based decision aids
44.
Zeelenberg CM. Regret in decision making. Curr. Direct. Psychol. Sci. 11(6), 212–216 (2002).
• Detailed content of web-based decision aids
45.
Brehaut JC, O'Connor AM, Wood TJ et al. Validation of a decision regret scale. Med. Decis. Making 23(4), 281–292 (2013).
• Detailed content of web-based decision aids
46.
Martínez-Alonso M, Carles-Lavila M, Pérez-Lacasta MJ et al. Assessment of the effects of decision aids about breast cancer screening: a systematic review and meta-analysis. BMJ Open 7(10), e016894c (2017).
• Application effect of decision aids in breast cancer screening
47.
Ivlev I, Hickman EN, McDonagh MS, Eden KB. Use of patient decision aids increased younger women's reluctance to begin screening mammography: a systematic review and meta-analysis. J. Gen. Intern. Med. 32(7), 803–812 (2017).
• Application effect of decision aids in breast cancer screening
48.
Collier R. National Physician Survey: EMR use at 75%. CMAJ 187(1), E17–E18 (2015).
• The future development of web-based decision aids
49.
Davis S, Roudsari A, Raworth R et al. Shared decision-making using personal health record technology: a scoping review at the crossroads. J. Am. Med. Inform. Assoc. 24(4), 857–866 (2017).
• The future development of web-based decision aids
50.
Durand MA, Stiel M, Boivin J et al. Where is the theory? Evaluating the theoretical frameworks described in decision support technologies. Patient Educ. Couns. 71(1), 125–135 (2008).
• The future development of web-based decision aids
51.
Bush N, Vanderpool R, Cofta-Woerpel L, Wallace P. Profiles of 800,000 users of the National Cancer Institute's Cancer Information Service since the debut of online assistance, 2003–2008. Prev. Chronic Dis. 7(2), A31 (2010).
• The future development of web-based decision aids
52.
McCaffery KJ, Holmes-Rovner M, Smith SK et al. Addressing health literacy in patient decision aids. BMC Med. Inform. Decis. Mak. 13(Suppl. 2), S10 (2013).
• The future development of web-based decision aids
53.
Von Wagner C, Steptoe A, Wolf MS et al. Health literacy and health actions: a review and a framework from health psychology. Health Educ. Behav. 36(5), 860–877 (2009).
• The future development of web-based decision aids
54.
Davis TC, Arnold C, Berkel H et al. Knowledge and attitude on screening mammography among low-literate, low-income women. Cancer 78(9), 1912–1920 (1996).
• The future development of web-based decision aids
55.
Graham ID, Logan J, Bennett CL et al. Physicians' intentions and use of three patient decision aids. BMC Med. Inform. Decis. Mak. 7(1), 20 (2007).
• The future development of web-based decision aids
56.
Friesen-Storms JH, Bours GJ, van der Weijden T, Beurskens AJ. Shared decision making in chronic care in the context of evidence based practice in nursing. Int. J. Nurs. Stud. 52(1), 393–402 (2015).
• The future development of web-based decision aids
57.
Wyatt KD, Branda ME, Anderson RT et al. Peering into the black box: a meta-analysis of how clinicians use decision aids during clinical encounters. Implement. Sci. 9(1), 1–10 (2014).
• The future development of web-based decision aids
58.
Kristina T, Nathan DS, Anna MJ et al. ‘They leave at least believing they had a part in the discussion’: understanding decision aid use and patient-clinician decision-making through qualitative research. Patient Educ. Couns. 93(1), 86–94 (2013).
• The future development of web-based decision aids
59.
Borrelli B, Ritterband LM. Special issue on eHealth and mHealth: challenges and future directions for assessment, treatment, and dissemination. Health Psychol. 34S, 1205–1208 (2015).
• The future development of web-based decision aids
60.
Alicia HY, Jinmyoung C. Has the digital health divide widened? Trends of health-related internet use among older adults from 2003 to 2011. J. Gerontol. B Psychol. Sci. Soc. Sci. 72(5), 856–863 (2017).
• The future development of web-based decision aids
61.
Karin M, Shadiya L. How feasible is multiple time point web-based data collection with individuals experiencing street homelessness? J. Urban Health 94(1), 64–74 (2017).
• The future development of web-based decision aids
62.
Hong YA, Zhou Z. A profile of eHealth behaviors in China: results from a national survey show a low of usage and significant digital divide. Front. Public Health 6, 274 (2018).
• The future development of web-based decision aids
63.
Alvarez-Galvez J, Salinas-Perez JA, Montagni I et al. The persistence of digital divides in the use of health information: a comparative study in 28 European countries. Int. J. Public Health 65(3), 64 (2020).
• The future development of web-based decision aids
Information & Authors
Information
Published In
Pages: 985 - 1002
PubMed: 33025800
Copyright
© 2020 Future Medicine Ltd.
History
Received: 4 April 2020
Accepted: 6 August 2020
Published online: 7 October 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Web-based decision aids to support breast cancer screening decisions: systematic review and meta-analysis. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0052
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Yang Chen, Chuanmei Zhu, Linna Li, Juejin Li, Qianwen Yan, Xiaolin Hu, Effects of Decision Aids on Decision Knowledge, Conflict, and Satisfaction Among Patients With Cancer: A Systematic Review and Meta‐Analysis, Journal of Nursing Management, 10.1155/jonm/6436400, 2026, 1, (2026).
- Effie Simou, Dimitrios Tseronis, Konstantina Zoupidou, Dimitrios Boumpas, Development of a Web-Based Multimedia Patient Decision Aid for Rheumatoid Arthritis: A User-Centered Design, Healthcare, 10.3390/healthcare14080983, 14, 8, (983), (2026).
- Rongyi Wu, Safa Elkefi, Health Informatics in Promoting Breast Cancer Screening: A Systematic Review of Benefits and Challenges, JCO Clinical Cancer Informatics, 10.1200/CCI-25-00174, 9, (2025).
- Chunbing Wang, Xiongqi Guo, RE: Personalized starting age of gastric cancer screening based on individuals’ risk profiles: a population-based, prospective study, JNCI: Journal of the National Cancer Institute, 10.1093/jnci/djaf206, 117, 10, (2138-2139), (2025).
- Jie Zhong, Wei Liang, Tongyao Wang, Pui Hing Chau, Nathan Davies, Junqiang Zhao, Ho Nee Connie Chu, Chia Chin Lin, Digital Decision Aids to Support Decision-Making in Palliative and End-of-Life Dementia Care: Systematic Review and Meta-Analysis, Journal of Medical Internet Research, 10.2196/71479, 27, (e71479), (2025).
- Phoebe Ullrich, Henrike Voß, Laura Unsöld, Michael Thomas, Matthias Villalobos, Web-based educational tools and decision aids for patients with advanced cancer: A systematic review, Patient Education and Counseling, 10.1016/j.pec.2025.108706, 134, (108706), (2025).
- Jun-Ming Su, Huey-Liang Kuo, Kai-Ling Yang, Chih-Jung Wu, Ya-Fang Ho, Interactive decision aid on therapy decision making for patients with chronic kidney disease: A prospective exploratory pilot study, DIGITAL HEALTH, 10.1177/20552076251332832, 11, (2025).
- Anna Rose Johnson, Grace Anne Longfellow, Clara N Lee, Benjamin Ormseth, Gary B Skolnick, Mary C Politi, Yonaira M Rivera, Terence Myckatyn, Social Media as a Platform for Cancer Care Decision-Making Among Women: Internet Survey-Based Study on Trust, Engagement, and Preferences, JMIR Cancer, 10.2196/64724, 11, (e64724), (2025).
- Patricia Villain, Laura Downham, Alice Le Bonniec, Charlotte Bauquier, Olena Mandrik, Tom Nadarzynski, Lorie Donelle, Raúl Murillo, Eleni L Tolma, Sonali Johnson, Patricia Soler-Michel, Robert Smith, Impact of Online Interactive Decision Tools on Women’s Decision-Making Regarding Breast Cancer Screening: Systematic Review and Meta-Analysis, Journal of Medical Internet Research, 10.2196/65974, 27, (e65974), (2025).
- Francis D. Graziano, Donovan R. White, Ethan L. Plotsker, Ronnie L. Shammas, Elizabeth Smith‐Montes, Jonas A. Nelson, Carrie S. Stern, Enhancing Patient Decision‐Making in Breast Reconstruction: A Systematic Review of Decision Aid Efficacy, Journal of Surgical Oncology, 10.1002/jso.28038, 131, 6, (1222-1235), (2024).
- See more