US cost–effectiveness of polatuzumab vedotin, bendamustine and rituximab in diffuse large B-cell lymphoma
This article has been corrected.
VIEW CORRECTIONPublication: Journal of Comparative Effectiveness Research
Abstract
Aim: To evaluate the cost–effectiveness of polatuzumab vedotin (pola) + bendamustine + rituximab (BR) in relapsed/refractory diffuse large B-cell lymphoma based on the GO29365 trial from a US payer’s perspective. Materials & methods: A partitioned survival model used progression-free survival and overall survival data from the GO29365 trial. The base case analysis assumed overall survival was informed by progression-free survival; a mixture cure model estimated proportion of long-term survivors. Results: In the base case, pola + BR was cost-effective versus BR at US$35,864 per quality-adjusted life year gained. Probabilistic and one-way sensitivity analyses showed that the findings were robust. Conclusion: Pola + BR is cost-effective versus BR for the treatment of transplant-ineligible relapsed/refractory diffuse large B-cell lymphoma in the US.
Diffuse large B-cell lymphoma (DLBCL) is the most common subtype of non-Hodgkin lymphoma in the US, accounting for about 30% of non-Hodgkin lymphoma diagnoses each year [1]. The incidence of DLBCL is estimated to be 5.6 new cases per 100,000 per year and the estimated 5-year survival is 63.2% [2]. Most cases of DLBCL (74%) are diagnosed in patients aged 55 years and above, with a median age at diagnosis of 66 years [2].
As an aggressive lymphoma, DLBCL typically presents with progressive lymphadenopathy that requires immediate treatment in most cases [3]. Rituximab plus cyclophosphamide, doxorubicin, vincristine and prednisone (R-CHOP) remains the backbone of first-line therapy, with durable remissions achieved in more than half of treated patients [1,3]. However, relapse (progression following treatment) and refractory disease (resistant to last treatment) remain problematic, with high-dose chemotherapy followed by autologous hematopoietic stem cell transplantation (HSCT) providing a chance of cure in a minority of these patients [4,5]. In the remainder and in those who are ineligible for HSCT (e.g., due to advanced age or comorbidities) [6], the prognosis is poor [5,7,8]. For patients with DLBCL who do not undergo HSCT, one of the options recommended by the National Comprehensive Cancer Network (NCCN®) for second-line or later treatment is the chemotherapy regimen of bendamustine + rituximab (BR) (category 2B – there are no preferred options in this setting, in contrast to first-line therapy) [1]. BR has an acceptable toxicity profile and has shown modest efficacy in patients with relapsed/refractory (R/R) DLBCL [6]. In addition, CAR T-cell therapies are treatment options for patients with relapsed/refractory (R/R) DLBCL after two or more lines of systemic therapy [1].
Polatuzumab vedotin (pola) is a first-in-class CD79b-targeted antibody-drug conjugate that delivers monomethyl auristatin E, a potent microtubule inhibitor, directly to tumor cells. Pola was granted accelerated approval in June 2019 by the US FDA in combination with BR for the treatment of adult patients with R/R DLBCL after at least two prior therapies [9,10]. Approval was based on the results of the randomized Phase II cohort of the GO29365 clinical trial (ClinicalTrials.gov: NCT02257567), in which patients with R/R DLBCL who were ineligible for HSCT were randomized to receive either pola + BR (n = 40) or BR alone (n = 40), with stratification by duration of response to last therapy (≤12 vs >12 months). Pola + BR demonstrated a significantly higher independent review committee (IRC)-assessed complete response (CR) rate (40.0 vs 17.5%) and longer IRC-assessed progression-free survival (PFS) rate (median 9.5 vs 3.7 months; hazard ratio [HR]: 0.36; 95% CI: 0.21–0.63) and overall survival (OS) (median 12.4 vs 4.7 months; HR: 0.42; 95% CI: 0.24–0.75) with a median follow-up of 22.3 months [11]. Furthermore, pola + BR produced a longer IRC-assessed duration of response compared with BR (median 12.6 vs 7.7 months; HR: 0.47; 95% CI: 0.19–1.14) and had a manageable toxicity profile [11]. A recent analysis, which included an additional year of follow-up, found that PFS (investigator assessed) and OS remain significantly better for patients receiving pola + BR than BR alone [12]. Currently, pola ± B ± R ± BR are recommended by the 2020 NCCN guidelines as a preferred treatment option, with category 2A evidence, for patients with R/R DLBCL (after at least two prior therapies) who are ineligible for HSCT [1].
While clinical trial data have demonstrated the efficacy and safety of pola + BR in patients with R/R DLBCL, the cost–effectiveness of pola + BR has not yet been assessed. Therefore, this cost–effectiveness analysis (CEA) was conducted to examine the economic value of pola + BR versus BR alone for the treatment of patients with R/R DLBCL after ≥1 prior therapy who were ineligible for HSCT (based on the GO29365 clinical trial) from a US third-party payer’s perspective.
Materials & methods
Model overview
The goal was to assess the cost–effectiveness of pola + BR compared with BR for the treatment of transplant-ineligible patients with R/R DLBCL in the US over a lifetime horizon. The CEA was based on an updated analysis that included an additional year of follow-up [12]. OS and PFS were derived from the GO29365 trial (NCT02257567) [11]. Survival beyond the study observation period was extrapolated using a mixture cure model [13]. The cost–effectiveness model tracks drug acquisition and administration costs, supportive care costs before disease progression, medical costs after disease progression and adverse event (AE) costs. The model examined a lifetime horizon. The primary outcome of interest was the incremental cost–effectiveness ratio (ICER). The analysis was conducted from a US third party payer’s perspective and reports costs in 2020 US dollars (USD). Future medical costs, life years (LYs) and quality-adjusted life years (QALYs) are discounted at 3% per year. The model was built in Microsoft® Excel 2016.
Patient population & model structure
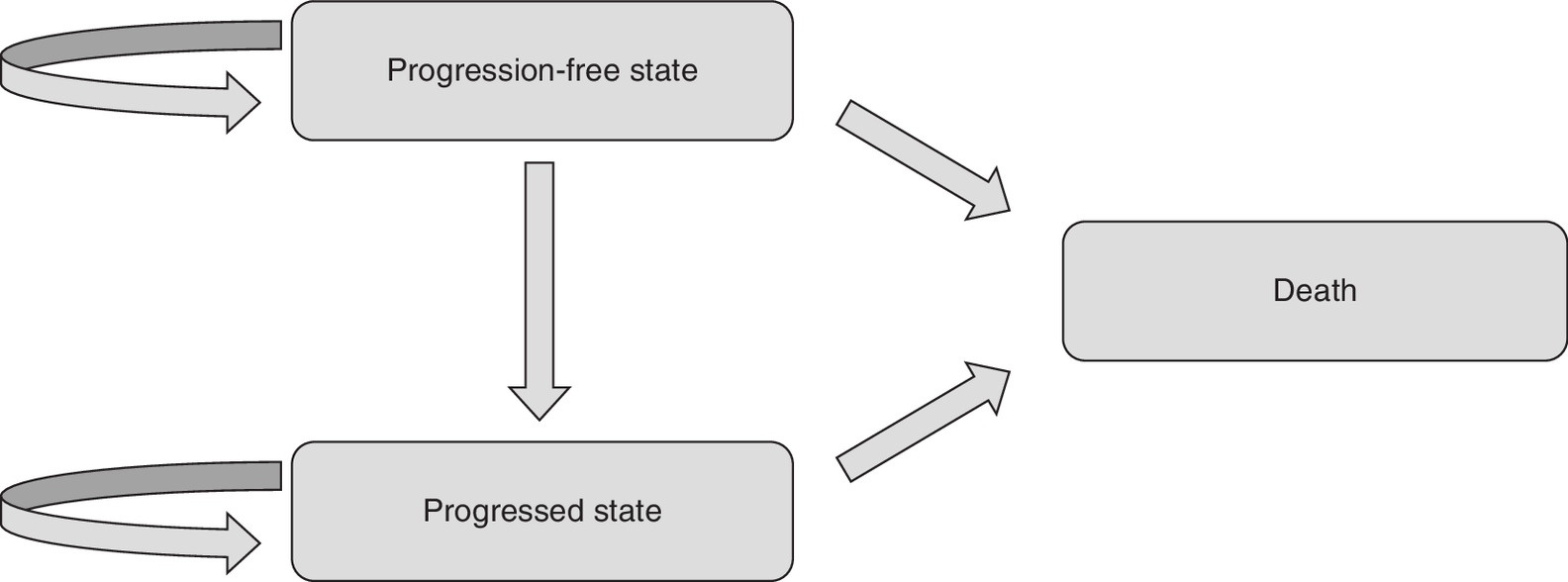
The target population consisted of adult patients (≥18 years) with R/R DLBCL (after ≥1 prior therapy) who were ineligible for HSCT, based on the GO29365 trial [11]. The model used a partitioned survival framework, which has been used in previous CEA studies of DLBCL [14,15]. The model consisted of three health states: progression free, defined as the time from the initiation of therapy for R/R DLBCL until disease progression; progressed disease (PD), defined as the time from disease progression until death from any cause; and death, defined as the absorbing state (Figure 1). Time-to-event data were used to model the proportion of patients who were in the progression-free, PD and death states dependent on time since trial initiation. OS was partitioned into PFS and PD. The proportion of patients in the PD health state at a given point in time was calculated as the difference between the proportion of patients who were alive and the proportion of patients who were progression free.
The two comparison arms (pola + BR vs BR) were defined based on the GO29365 trial (data cutoff: 15 March 2019) [11], in which treatment was administered for six cycles of 21 days each. For patients in the pola + BR arm, pola 1.8 mg/kg was administered on day 2 of cycle 1 and day 1 of cycles 2–6, bendamustine 90 mg/m2/day was administered on days 2 and 3 of cycle 1 and days 1 and 2 of cycles 2–6 and rituximab 375 mg/m2 was administered on day 1 of cycles 1–6. For patients in the BR arm, bendamustine 90 mg/m2/day was administered on days 2 and 3 of cycle 1 and days 1 and 2 of cycles 2–6, while rituximab 375 mg/m2 was administered on day 1 of cycles 1–6.
Patients were modeled with one-week cycles over a 50-year time horizon, to reflect a lifetime horizon for this disease population. Patients with R/R DLBCL entered the model in the progression-free health state for both the pola + BR and BR arms. In each weekly cycle, patients were redistributed among the three health states, with death being the absorbing state. A half-cycle correction was applied to costs and effectiveness. Since the model was developed from a US third-party payer’s perspective, only direct costs were considered. Model inputs and data sources are provided in Table 1 and described below.
| Model input | Value | Notes/sources | Ref. |
|---|---|---|---|
| Population characteristics | |||
| – Average bodyweight (kg) | 78.88 | Genentech, data on file | [21] |
| – Average BSA (m2) | 1.93 | ||
| Utility | |||
| – Progression-free state | 0.83 | JULIET study | [18,19] |
| – PD state | 0.71 | ||
| Drug acquisition costs per mg‡($) | |||
| – Pola | 105.00 | Genentech, data on file, CMS ASP Pricing File 2020 | [21,22] |
| – Bendamustine | 20.95 | ||
| – Rituximab | 8.81 | ||
| Drug administration costs ($) | |||
| – Pola administration cost per infusion, first infusion | 174.07 | CMS Physician Fee Schedule 2019 | [23] |
| – Pola administration cost per infusion, subsequent infusions | 143.08 | ||
| – Bendamustine cost per infusion | 143.08 | ||
| – Rituximab cost per infusion | 174.07 | ||
| Medical unit costs ($) | |||
| – Medical history and physical exam | 75.32 | CMS physician fee schedule, CPT code: 99213 | [23] |
| – CBC with differential | 8.63 | CMS lab fee schedule, CPT code: 85025 | [24] |
| – LDH | 6.71 | CMS lab fee schedule, CPT code: 83615 | [24] |
| – Comprehensive metabolic panel | 11.74 | CMS lab fee schedule, CPT code: 80053 | [24] |
| – CT scan | 121.81 | CMS lab fee schedule, CPT code: 78815 | [24] |
| – Medical cost of progression per weekly cycle | 1135.12 | Huntington et al. | [25] |
| – Terminal care cost (one-time) | 24,994.11 | Chastek et al. | [26] |
| Frequency of HRU per weekly cycle during PFS | |||
| – CT scan, up to 2 years after 6 cycles of treatment | 0.038 | NCCN guidelines | [1] |
| – Other resources, up to 2 years after 6 cycles of treatment | 0.077 | ||
| – CT scan, years 2–5 after 6 cycles of treatment | 0.019 | ||
| – Other resources, years 2–5 after 6 cycles of treatment | 0.077 | ||
| – CT scan, 5 years after 6 cycles of treatment | 0.019 | ||
| – Other resources, 5 years after 6 cycles of treatment | 0.019 | ||
| AE unit costs ($) | |||
| – Anemia | 7130.86 | The list of AEs was derived from the pola package insert; cost inputs for each AE were obtained from HCUP | [9,27] |
| – Diarrhea | 7661.39 | ||
| – Hypokalemia | 6960.60 | ||
| – Hypophosphatemia | 7854.71 | ||
| – Infections | 6955.11 | ||
| – Lymphopenia | 7176.99 | ||
| – Neutropenia | 13,451.09 | ||
| – Thrombocytopenia | 11,260.87 | ||
| AE rates, pola + BR†(%) | |||
| – Anemia | 18.00 | The list of AEs and associated rates were derived from the pola package insert | [9] |
| – Diarrhea | 4.40 | ||
| – Hypokalemia | 11.00 | ||
| – Hypophosphatemia | 7.00 | ||
| – Infections | 16.00 | ||
| – Lymphopenia | 87.00 | ||
| – Neutropenia | 61.00 | ||
| – Thrombocytopenia | 31.00 | ||
| AE rates, BR†(%) | |||
| – Anemia | 10.00 | The list of AEs and associated rates were derived from the pola package insert | [9] |
| – Diarrhea | 5.00 | ||
| – Hypokalemia | 5.00 | ||
| – Hypophosphatemia | 8.00 | ||
| – Infections | 2.60 | ||
| – Lymphopenia | 82.00 | ||
| – Neutropenia | 33.00 | ||
| – Thrombocytopenia | 26.00 | ||
†
The model considered all-cause grade 3 or higher AEs occurring in >10% of patients with R/R DLBCL and ≥5% of the pola + BR arm and selected grade 3–4 laboratory abnormalities worsening from baseline in patients with R/R DLBCL and ≥5% of the pola + BR arm based on the pola US FDA package insert.
‡
The recommended dose of pola is 1.8 mg/kg every 21 days for six cycles in combination with bendamustine 90 mg/m2/day on day 1 and 2 and rituximab 375 mg/m2 on day 1 of each cycle, based on the pola FDA package insert.
AE: Adverse event; ASP: Average sales price; BSA: Body surface area; BR: Bendamustine + rituximab; CBC: Complete blood count; CMS: Centers for Medicare & Medicaid; CPT: Current Procedural Terminology; CT: Computed tomography; DLBCL: Diffuse large B-cell lymphoma; HCUP: Healthcare Cost and Utilization Project; HRU: Healthcare resource utilization; NCCN: National Comprehensive Cancer Network; PD: Progressed disease; Pola: Polatuzumab vedotin; R/R: Relapsed/refractory.
Model inputs
Efficacy inputs
Observed OS and investigator-assessed PFS were derived from the GO29365 trial [11,21]. Figure 2 shows the predicted PFS and OS curves for each treatment, as used in the base-case analysis. Based on observed data and clinical opinion, a mixture cure model was deemed appropriate for modeling PFS and OS informed by PFS [13]. This statistical model assumes that the patient population consists of long-term survivors (patients who have not died from DLBCL) and patients who progress and die from the disease [13]. Parametric functions were also applied to model the distribution among stable disease, PD and death based on the patient-level data of the GO29365 trial, assuming a long-term survival rate [16]. Distributions explored included the exponential, Weibull, log-logistic, log-normal, generalized gamma and Gompertz functions. Based on visual inspection, the Akaike information criterion and the Bayesian information criterion, a log-normal distribution provided the best fit to the observed data for both PFS and OS. The estimated proportions of long-term survivors were 22% for pola + BR vs 0% for the BR arm [13].

Figure 2. Observed and predicted (A) progression-free survival and (B) overall survival for each treatment arm in GO29365.
BR: Bendamustine + rituximab; OS: Overall survival; PFS: Progression-free survival; Pola: Polatuzumab vedotin.
The base-case model used PFS to inform OS. Scenario analyses were performed to test the impact of a mixture cure model based on OS only (as described by Bansal et al. [17]) and standard parametric techniques (non-mixture cure).
Utility inputs
Utility inputs for the progression-free and PD health states were obtained from JULIET, a Phase II study of tisagenlecleucel in patients with DLBCL that was refractory to first and second-line therapies or that had relapsed after HSCT [18,19]. The JULIET study incorporated the SF-36 which was converted to SF-6D scores [20]. The utility was 0.83 for the progression-free health state (assumed to be the same for all patients regardless of treatment arm) and 0.71 for the PD health state.
Cost inputs
Costs considered in this model included treatment costs, medical costs associated with each health state, AE costs and end-of-life costs (Table 1). All costs were in 2020 USD. If applicable, the medical care component of the Consumer Price Index was used to inflate the original cost inputs to 2020 USD [28].
Drug acquisition costs
Drug acquisition costs were estimated based on average body surface area (BSA), dosing schedules and number of doses per treatment cycle. The full weight distribution of the patient cohort was used in the model instead of the mean to more accurately capture the cost of pola using variations of the 30 mg vial in addition to 140 mg vials of pola (no vial sharing was assumed). The average weight of DLBCL patients in the Flatiron Health data (derived from Genentech, data on file [21]) was 78.9 kg and given the available vial of 140 mg and a dosing of 1.8 mg/kg, the average patient would use one vial. However, when considering the full weight distribution of DLBCL patients in Flatiron, patients used variations of 30 and 140 mg vials of pola to allow precise weight-based dosing (e.g., dose of 30, 60, 90, 120, 140, 150, etc.).
Treatments other than pola are dosed according to BSA. An average BSA of 1.93 m2 was derived from Genentech, data on file [21]. The dosages received for rituximab were calculated using a minimum dosage strength of 100 mg based on the FDA package insert [29]. Bendamustine was assumed to have no dose wastage since the administration is through multi-use vials.
Unit drug costs were based on Average Sales Price (ASP). Drug costs related to dose wastage (no vial sharing) were considered. The dosing schedule and number of doses per treatment cycle were based on the FDA package inserts for pola [9], rituximab [29], bendamustine [30], as well as the GO29365 trial [11]. The ASP unit prices were obtained by dividing payment amounts in the 2020 Medicare Part B Drug ASP Pricing Files (effective 1 July 2020 to September 2020 [22]) by 1.06 because Medicare pays physicians and suppliers for most part B-covered drugs based on their ASP plus 6%. The unit ASP price for pola is US$105.00 per mg. The expected drug acquisition costs per patient were calculated using time to off treatment curves and the average drug costs per treatment weekly model cycle. The mean number of treatment cycles based on trial data were 4.2 and 2.7 for the pola + BR and BR arms, respectively [21].
Drug administration costs
Lengths of administration for each regimen were obtained from package inserts and the corresponding unit administration costs were obtained from the Centers for Medicare & Medicaid Services (CMS) 2019 Physician Fee schedule (Table 1) [9,23,29,30]. The expected drug administration costs per patient were calculated using time to off treatment curves and the average drug administration costs per treatment weekly cycle.
Medical costs
Medical costs included medical costs associated with health states and terminal care costs. The resource use per week in the progression-free health state was estimated based on the NCCN guidelines for patients with DLBCL, which recommend that patients complete a medical history and physical exam and lab tests every 3–6 months for 5 years and a computed tomography scan every 6 months for 2 years after treatment completion [1]. These rates were translated into weekly frequencies in the model, assuming patients completed the medical history and physical exam and lab tests every 3 months. The unit costs of routine follow-up were obtained from the CMS 2019 Physician Fee and Clinical Laboratory Fee schedule [23,24].
For patients who progressed on the study treatment, medical costs associated with PD were assigned (US$1135.12 per weekly cycle), based on a Medicare analysis of patients with DLBCL [25].
For patients who died, a one-time terminal care cost (US$24,994.11) corresponding to the incremental costs of hospice care and inpatient care during the last month of life was assigned based on Chastek et al. [26].
AE costs
Patients in the progression-free state incurred costs associated with the management of AEs. The model considered all-cause grade ≥3 AEs occurring in >10% of patients with R/R DLBCL and ≥5% more in the pola-BR arm and selected grade 3–4 laboratory abnormalities worsening from baseline in patients with R/R DLBCL and ≥5% in the pola-BR arm based on the pola FDA package insert [9].
Model outputs
Base-case analyses
Using the base case model inputs, the costs and utilities for each treatment arm were calculated and compared. The outcomes included total costs and its cost components (i.e., treatment costs, medical costs associated with health states, terminal care costs and AE costs) and effectiveness measured as total LYs and QALYs. The total incremental costs, total incremental LYs, total incremental QALYs and ICERs (presented as incremental cost per LY and incremental cost per QALY) were also calculated comparing the pola + BR versus BR arms.
Sensitivity & scenario analyses
Deterministic sensitivity analyses (DSA) were conducted to assess the impact of individual model inputs on the results. The DSA varied one model input at a time, including discount rate, utility, average patient BSA, average patient weight and medical costs. Inputs included in the DSA are shown in Table 2.
| Parameter | Base-case input | DSA input |
|---|---|---|
| Patient baseline characteristics | ||
| – Average weight at baseline (kg) | 78.88 | ±20% of base case |
| – Average BSA at baseline (m2) | 1.93 | |
| Drug administration cost per treatment cycle (US$) | ||
| – First cycle, pola + BR | 634.30 | ±20% of base case |
| – Subsequent cycle, pola + BR | 603.31 | 20th and 80th percentile values from PSA distribution |
| – First cycle, BR | 460.23 | ±20% of base case |
| – Subsequent cycle, BR | 460.23 | 20th and 80th percentile values from PSA distribution |
| Supportive care cost during PFS per weekly cycle (US$) | ||
| – Supportive care cost in PFS for the first 2 years | 12.52 | 20th and 80th percentile values from PSA distribution |
| – Supportive care cost in PFS from year 2 to year 5 | 10.18 | 20th and 80th percentile values from PSA distribution |
| – Supportive care cost in PFS after 5 years | 4.30 | 20th and 80th percentile values from PSA distribution |
| Other medical costs (US$) | ||
| – PD cost per weekly cycle | 1135.12 | 20th and 80th percentile values from PSA distribution |
| – AE cost, pola + BR (one-time) | 21,989.99 | 20th and 80th percentile values from PSA distribution |
| – AE cost, BR (one-time) | 15,505.21 | 20th and 80th percentile values from PSA distribution |
| – Terminal care cost (one-time) | 24,994.11 | ±20% of base case |
| Health state utility | ||
| – PFS utility | 0.830 | 20th and 80th percentile values from PSA distribution |
| – PD utility | 0.710 | 20th and 80th percentile values from PSA distribution |
| Discount rate (US%) | ||
| – Discount rate for costs | 3.0 | 0.0%, 6.0% |
| – Discount rate for utilities | 3.0 | 0.0%, 6.0% |
AE: Adverse event; BR: Bendamustine + rituximab; BSA: Body surface area; DSA: Deterministic sensitivity analyses; PD: Progressed disease; PFS: Progression-free survival; Pola: Polatuzumab vedotin; PSA: Probabilistic sensitivity analyses.
Probabilistic sensitivity analyses (PSA) were conducted to estimate the probability for the pola + BR arm to be cost-effective compared with the BR arm based on different willingness-to-pay (WTP) thresholds. A Monte-Carlo simulation with 1000 iterations was conducted. In each iteration, the model inputs were randomly drawn from the specified distributions. Inputs included in the PSA are shown in Supplementary Table 1.
The base-case model was a mixture cure model where PFS informed OS. Scenario analyses examined a mixture cure model where PFS did not inform OS as well as a non-mixture cure model (non-proportional hazard model for enhanced flexibility) using standard parametric techniques. For the non-mixture cure model, we used feedback from clinical experts and visual inspection with Akaike information criterion and Bayesian information criterion to determine that a generalized gamma distribution provided the best fit for the observed data for PFS and a log-normal distribution for OS.
Results
Base case analyses
In the base-case analysis (using a discount rate of 3% per year for costs and utilities), pola + BR was associated with greater utility compared with BR, including 3.09 (4.04 vs 0.95) incremental LYs and 2.57 (3.31 vs 0.73) incremental QALYs over a 50-year time horizon (Table 3).
| Pola + BR | BR | Pola + BR vs BR | |
|---|---|---|---|
| Costs (2020 $)† | |||
| Total costs | 210,418 | 118,088 | 92,329 |
| – Total treatment costs | 139,717 | 47,944 | 91,773 |
| – Pola acquisition costs | 68,991 | 0 | 68,991 |
| – Bendamustine acquisition costs | 34,438 | 23,548 | 10,890 |
| – Rituximab acquisition costs | 33,426 | 22,856 | 10,570 |
| – Drug administration costs | 2862 | 1540 | 1322 |
| – Supportive care costs associated with PFS | 1445 | 274 | 1171 |
| – Medical costs associated with PD | 24,954 | 29,804 | -4849 |
| – Terminal care costs | 22,313 | 24,561 | -2248 |
| – AE costs | 21,989 | 15,505 | 6484 |
| Effectiveness† | |||
| – Total LYs | 4.04 | 0.95 | 3.09 |
| – Total QALYs | 3.31 | 0.73 | 2.57 |
| ICER | |||
| – Incremental cost per LY gained | $29,881/LY | ||
| – Incremental cost per QALY gained | $35,864/QALY | ||
†
Discount rate 3% per year.
AE: Adverse event; BR: Bendamustine + rituximab; ICER: Incremental cost–effectiveness ratio; LY: Life year; PFS: Progression-free survival; PD: Progressed disease; Pola: Polatuzumab vedotin; QALY: Quality-adjusted life year.
Over the same time horizon, patients in the pola + BR arm incurred higher treatment costs compared with patients in the BR arm (US$139,717 vs 47,944, difference = US$91,773; Table 3). Conversely, due to lower progression and death rates, patients in the pola + BR arm incurred lower post-progression medical costs (US$24,954 vs US$29,804; difference = -US$4849) and terminal care costs (US$22,313 vs 24,561; difference = -US$2248). The total costs over a lifetime were estimated to be US$210,418 for patients in the pola + BR arm and $118,088 for patients in the BR arm, leading to a total incremental cost of US$92,329 (pola + BR vs BR).
Considering both cost and utility outcomes, the ICERs comparing the pola + BR versus BR arms were estimated to be US$29,881 per LY gained and US$35,864 per QALY gained (Table 3).
Sensitivity & scenario analyses
DSA
The DSA results indicate that the results were robust in key scenarios. Figure 3 shows the top eight most sensitive parameters, with ICERs ranging from US$25,679 to US$46,271. The model was most sensitive to the discount rate considered for effectiveness. Specifically, when a discount rate of 6% was selected, the ICER increased to US$46,271/QALY gained. Other key drivers of the model included utility in PFS and average patient BSA. In contrast, the model was not sensitive to AE costs, supportive care cost in PFS and terminal care cost.

Figure 3. Deterministic sensitivity analysis results for pola + bendamustine + rituximab versus bendamustine + rituximab alone.
BR: Bendamustine + rituximab; BSA: Body surface area; PD: Progressed disease; PFS: Progression-free survival; Pola: Polatuzumab vedotin; QALY: Quality-adjusted life year.
PSA
The cost–effectiveness plane showing the incremental costs and incremental QALYs in the comparison of the pola + BR arm versus the BR arm based on 1000 simulations of the model is presented in Figure 4. The average incremental cost and QALYs were US$88,481 and 2.61, respectively. The average cost per QALY gained was US$42,612/QALY.

Figure 4. Incremental cost–effectiveness plane for pola + bendamustine + rituximab versus bendamustine + rituximab alone.
The average incremental cost and QALYs were US$88,481 and 2.61, respectively. The average cost per QALY gained was US$42,612/QALY.
BR: Bendamustine + rituximab; Pola: Polatuzumab vedotin; QALY: Quality-adjusted life year.
The cost–effectiveness acceptability curve is presented in Figure 5. The pola + BR arm was considered cost-effective relative to the BR arm in 68% of replications at a WTP threshold of US$50,000 per QALY and in 97% of replications at a WTP threshold of US$100,000 per QALY.
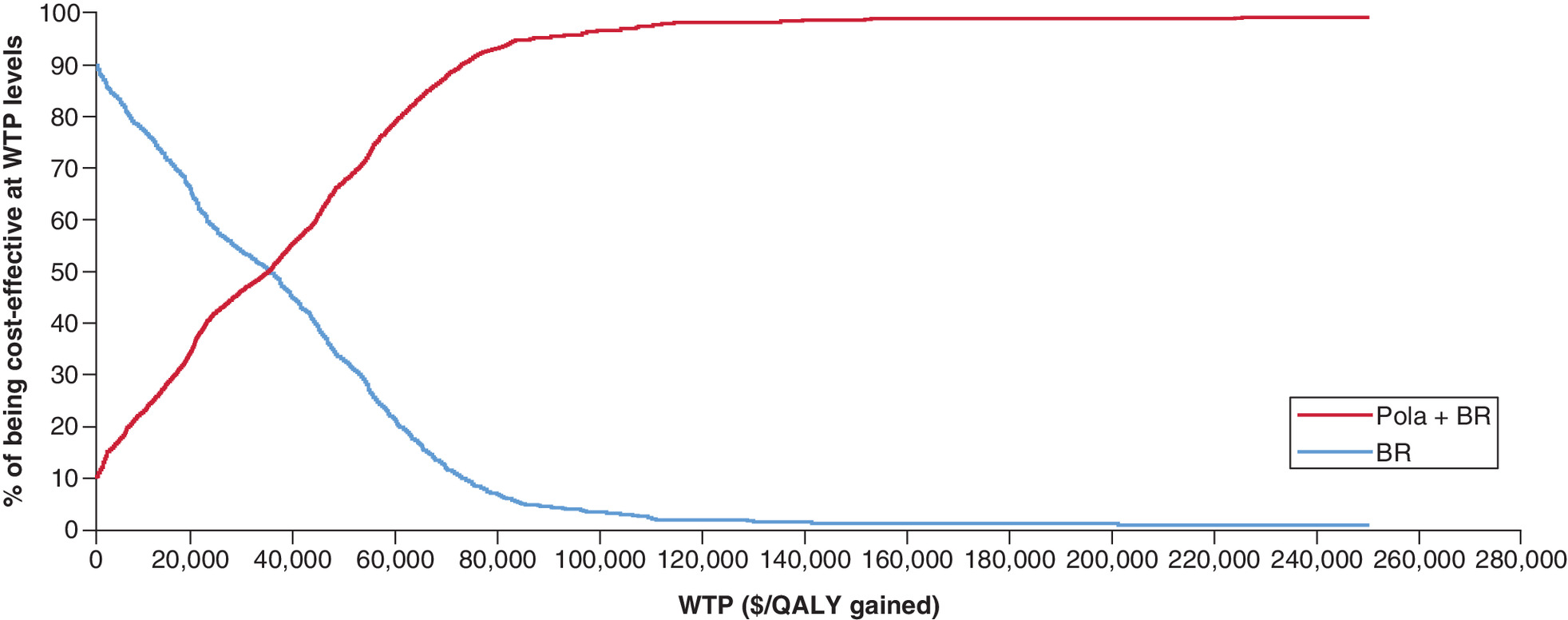
Figure 5. Cost–effectiveness acceptability curve (willingness-to-pay per quality-adjusted life year).
BR: Bendamustine + rituximab; Pola: Polatuzumab vedotin; QALY: Quality-adjusted life year; WTP: Willingness-to-pay.
Additional scenario analyses resulted in ICERs of US$41,442 per QALY when OS was modeled separately from PFS (mixture cure) and US$72,166 per QALY when using standard parametric methods (non-mixture cure). Both ICERs were below the US acceptable WTP threshold of US$150,000 per QALY gained [31].
Discussion
Following the recent approval of pola + BR in the US for the treatment of adult patients with R/R DLBCL, not otherwise specified, after at least two prior therapies, it is important for payers to understand the economic benefits of this regimen compared with the existing recommended standards of care. In the randomized Phase II cohort of GO29365, pola + BR showed a significantly higher CR rate and improved OS and PFS compared with BR [11]. In the present study, we assessed the cost–effectiveness of pola +BR versus BR using model inputs from the GO29365 trial [11] and the literature or other publicly available data. The results from the base-case analysis showed that pola + BR was associated with a greater health benefit compared with BR over a lifetime (50 years), as evidenced by a gain of 2.57 QALYs. The incremental cost per QALY gained over a lifetime was estimated at US$35,864, which was below the US-acceptable WTP threshold of US$150,000 per QALY gained [31]. Moreover, in the sensitivity analyses, the cost–effectiveness results were found to be robust in key scenarios, with pola + BR being cost-effective relative to BR in 97% of cases at a WTP threshold of US$100,000/QALY gained.
While patients in the pola + BR arm incurred higher costs, including those associated with treatment, AE management and supportive care due to longer survival time, these increases were partially offset by the lower post-progression medical costs and terminal care costs. This offset may be explained by the lower rates of progression and death observed with pola + BR in the GO29365 trial, where pola + BR reduced the risk of death by 58% compared with BR alone [11]. This improvement was supported by a significantly higher CR rate with pola + BR versus BR (40 vs 18%; p < 0.05), as well as a manageable toxicity profile [11]. Thus, the present study suggests that despite having higher treatment-related costs, pola + BR is more cost-effective relative to BR for the treatment of patients with R/R DLBCL who are ineligible for HSCT in the US.
Additional therapies have also recently been approved for this difficult-to-treat population, including the CAR-T therapies axicabtagene ciloleucel and tisagenlecleucel based on the results from the Phase II clinical trials ZUMA-1 and JULIET [18,32]. A few studies have assessed the cost–effectiveness of CAR-T therapy for R/R DLBCL [33–35]. Lin et al. built a decision analytic Markov and suggested that in optimistic scenarios, the ICERs of axicabtagene ciloleucel and tisagenlecleucel were US$129,000 and 168,000 per QALY gained, respectively, compared with chemoimmunotherapy and HSCT in adult patients with R/R DLBCL [33]. In a separate study, Whittington et al. used a decision tree and semi-Markov model and estimated ICERs ranging between US$100,400 and 289,000 per QALY gained when comparing axicabtagene ciloleucel with chemotherapy in adult patients with R/R DLBCL [34]. In addition, Roth et al. used a mixture cure regression analysis to estimate an incremental cost of US$58,146 per QALY gained with axicabtagene ciloleucel compared with chemotherapy in patients with R/R large B-cell lymphoma (including DLBCL) [35].
The estimated ICER of US$35,864 per QALY gained in the current analysis of pola + BR versus BR was lower than the ICERs in each of the three published CAR-T models in R/R DLBCL. The patient population in the pola GO29365 trial varies from the patient populations of other trials in the R/R DLBCL setting. Patients in the GO29365 trial were on average older with a poorer prognosis (based on International Prognostic Index score) and a higher proportion were more heavily pretreated or refractory to prior treatment than those enrolled in clinical trials of axicabtagene ciloleucel and tisagenlecleucel (e.g., ZUMA-1 and JULIET [11,18,32]). It is therefore positive that pola + BR was found to be cost-effective (with a relatively low ICER under the US$150,000/QALY gained threshold) versus BR in a difficult-to-treat DLBCL population with few remaining treatment options. Compared with CAR-T therapies, pola can be characterized as a readily available, ‘off-the-shelf’ treatment; a recent discrete event simulation model found that increased wait times associated with CAR-T treatment can result in worse outcomes for patients with R/R DLBCL [36]. Increased wait times may further impact the cost–effectiveness for CAR-T therapies as well.
The results of this cost–effectiveness model should be interpreted in light of some limitations. First, the sample size was small since the model was based on a randomized Phase II clinical trial. Second, cost inputs used in this model might vary in different patient populations and were based on available data. However, a PSA varying different model inputs was conducted and demonstrated the robustness of results. Furthermore, the validity and robustness of partitioned survival models beyond the observed trial duration is dependent on the maturity of the used survival data. Since the results are sensitive to long-term survival results (which at this point have to be extrapolated), future CEAs based on survival data with a longer follow-up time are warranted.
Conclusion
The results of this CEA model suggest that, from the perspective of a US third-party payer, pola + BR represents a cost-effective option compared with BR alone for the treatment of patients with R/R DLBCL who are ineligible for HSCT. This cost–effectiveness was robust in sensitivity analyses.
•
Addition of polatuzumab vedotin (pola) to bendamustine + rituximab (BR) was associated with a significantly improved complete response rate and a 58% reduction in the risk of death in patients with transplant-ineligible relapsed/refractory diffuse large B-cell lymphoma (R/R DLBCL) in the GO29365 trial (ClinicalTrials.gov: NCT02257567).
•
The current study evaluated the cost–effectiveness of pola + BR for the treatment of R/R DLBCL from a US third-party payer's perspective based on GO29365 trial data.
•
A partitioned survival model was developed using progression-free survival (PFS) and overall survival (OS) data from the GO29365 trial. The base-case analysis assumed OS was informed by PFS and used a mixture cure model to estimate the proportion of long-term survivors (pola + BR: 21%; BR: 0%) based on a recent analysis.
•
In the base case, pola + BR was associated with higher utility than BR alone (3.09 incremental life years [LY], 2.57 incremental quality-adjusted life years [QALY]).
•
Estimated total lifetime costs (including drug acquisition/administration, adverse events, PFS routine care, progressed disease medical care and end-of-life care) were US$210,418 with pola + BR and $118,088 with BR, leading to a total incremental cost of US$92,329.
•
Driven predominately by higher PFS and OS and higher estimated proportion of long-term survivors, pola + BR is more cost-effective than BR for the treatment of transplant-ineligible R/R DLBCL in the US, with incremental costs per LY and per QALY gained of US$29,881/LY and $35,864/QALY.
•
Probabilistic sensitivity analyses testing model robustness showed that, at US willingness-to-pay thresholds of US$50,000 and 100,000, pola + BR was more cost-effective than BR in 68 and 97% of cases, respectively.
Author contributions
All authors were involved in the development of the economic model and the analysis, review and approval of the manuscript.
Acknowledgments
We would like to thank SJ Hong of the University of Washington and Genentech, Inc. for his assistance with model design and manuscript review.
Financial & competing interests disclosure
The study was sponsored by Genentech, Inc.; Analysis Group, Inc. was paid to develop the economic model. AS Masaquel, M Schulz and J Li are employees of Genentech, Inc. and own stocks/stock options in F. Hoffmann La Roche Ltd. F Felizzi and P Thuresson are employees of F. Hoffmann La Roche Ltd; P Thuresson owns shares in F. Hoffmann La Roche Ltd. KA Betts, EX Du and I Dieye are employees of Analysis Group, Inc., which has received consulting fees from the sponsor.
Editorial assistance, under the guidance of K Betts and A Masaquel, was provided by R Hubbard of Gardiner-Caldwell Communications and was funded by F. Hoffmann-La Roche Ltd.
Data sharing statement
Qualified researchers may request access to individual patient-level data through the clinical study data request platform (www.clinicalstudydatarequest.com). Further details on Roche’s criteria for eligible studies are available here (https://clinicalstudydatarequest.com/Study-Sponsors/Study-Sponsors-Roche.aspx). For further details on Roche’s Global Policy on the Sharing of Clinical Information and how to request access to related clinical study documents, see here: (https://www.roche.com/research_and_development/who_we_are_how_we_work/clinical_trials/our_commitment_to_data_sharing.htm).
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_data.zip)
- Download
- 21.46 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
National Comprehensive Cancer Network (NCCN). NCCN clinical practice guidelines in oncology (NCCN guidelines) B-Cell lymphomas. V4.2020. 1–297 (2020). https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf
2.
National Cancer Institute (NCI) Surveillance, Epidemiology, and End Results Program (SEER). Cancer stat facts: NHL - Diffuse large B-Cell lymphoma (DLBCL) 2019. (2019). https://seer.cancer.gov/statfacts/html/dlbcl.html
3.
Liu Y, Barta SK. Diffuse large B-cell lymphoma: 2019 update on diagnosis, risk stratification, and treatment. Am. J. Hematol. 94(5), 604–616 (2019).
• This review article provides an overview of diffuse large B-cell lymphoma (DLBCL), including current diagnosis, risk stratification and treatments. The focus is how cell-of-origin and molecular features are being used to guide treatment of front-line and relapsed/refractory DLBCL.
4.
Crump M, Kuruvilla J, Couban S et al. Randomized comparison of gemcitabine, dexamethasone, and cisplatin versus dexamethasone, cytarabine, and cisplatin chemotherapy before autologous stem-cell transplantation for relapsed and refractory aggressive lymphomas: NCIC-CTG LY.12. J. Clin. Oncol. 32(31), 3490–3496 (2014).
5.
Gisselbrecht C, Glass B, Mounier N et al. Salvage regimens with autologous transplantation for relapsed large B-cell lymphoma in the rituximab era. J. Clin. Oncol. 28(27), 4184–4190 (2010).
6.
Vacirca JL, Acs PI, Tabbara IA et al. Bendamustine combined with rituximab for patients with relapsed or refractory diffuse large B cell lymphoma. Ann. Hematol. 93(3), 403–409 (2014).
7.
van Den Neste E, Schmitz N, Mounier N et al. Outcome of patients with relapsed diffuse large B-cell lymphoma who fail second-line salvage regimens in the International CORAL study. Bone Marrow Transplant. 51(1), 51–57 (2016).
• This article reports updated outcomes of the Collaborative Trial in Relapsed Aggressive Lymphoma (CORAL) study, for patients who could not proceed to scheduled autologous stem cell transplantation (ASCT). Median overall survival was significantly improved for patients with lower tertiary IPI, those responding to third-line treatment, and those who were eventually transplanted.
8.
Crump M, Neelapu SS, Farooq U et al. Outcomes in refractory diffuse large B-cell lymphoma: results from the international SCHOLAR-1 study. Blood. 130(16), 1800–1808 (2017).
9.
Genentech, Inc. POLIVY™ (polatuzumab vedotin-piiq) for injection, for intravenous use. (2019). https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/761121s000lbl.pdf
10.
US FDA. FDA approves polatuzumab vedotin for diffuse large B-cell lymphoma 2019. (2019). https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-polatuzumab-vedotin-piiq-diffuse-large-b-cell-lymphoma
11.
Sehn LH, Herrera AF, Flowers CR et al. Polatuzumab vedotin in relapsed or refractory diffuse large B-cell lymphoma. J. Clin. Oncol. 38(2), 155–165 (2020).
• This original article reports on the Phase Ib/II trial of polatuzumab vedotin plus benamustine + obinutuzumab (BG), or polatuzumab vedotin plus bendamustine + rituximab (BR) versus BR alone in patients with transplant-ineligible relapsed/refractory DLBCL. Polatuzumab vedotin plus BR resulted in a significantly higher CR rate and reduced risk of death compared with BR alone.
12.
Sehn LH, Matasar MJ, Flowers CR et al. Polatuzumab vedotin plus bendamustine with rituximab in relapsed/refractory diffuse large B-cell lymphoma: updated results of a Phase Ib/II randomized study. Poster presented at ASH 2019 (P-4081) (2019).
• This poster reports the updated results of the Phase II trial of polatuzumab vedotin plus BR in relapsed/refractory DLBCL with an additional year of follow-up. No new safety signals were identified. Progression-free survival and overall survival remain significantly better for patients receiving polatuzumab vedotin plus BR versus BR, and 38% patients treated with polatuzumab vedotin plus BR had response durations ≥12 months.
13.
Sehn LH, Flowers CR, McMillan A et al. Estimation of long-term survival with polatuzumab vedotin plus bendamustine and rituximab for patients with relapsed/refractory diffuse large B-cell lymphoma (R/R DLBCL). Hematol. Oncol. 37(S2), 257–258 (2019).
14.
National Institute for Health and Care Excellence (NICE). Axicabtagene ciloleucel for treating diffuse large B-cell lymphoma and primary mediastinal large B-cell lymphoma after 2 or more systemic therapies (TA559). (2019). https://www.nice.org.uk/Guidance/TA559
15.
National Institute for Health and Care Excellence (NICE). Tisagenlecleucel for treating relapsed or refractory diffuse large B-cell lymphoma after 2 or more systemic therapies (TA567). (2019). https://www.nice.org.uk/Guidance/TA567
16.
Lambert PC. Modeling of the cure fraction in survival studies. Stata J. 7(3), 351–375 (2007).
17.
Bansal A, Sullivan SD, Lin VW et al. Estimating long-term survival for patients with relapsed or refractory large B-cell lymphoma treated with chimeric antigen receptor therapy: a comparison of standard and mixture cure models. Med. Decis. Making. 39(3), 294–298 (2019).
• This estimated long-term survival for patients with relapsed or refractory large B-cell lymphoma treated with chimeric antigen receptor therapy. Standard parametric models were compared with mixture cure models. Based on the findings, they suggest that mixture cure models may provide a more accurate estimate of long-term survival compared with standard models, with sufficient follow-up.
18.
Schuster SJ, Bishop MR, Tam CS et al. Tisagenlecleucel in adult relapsed or refractory diffuse large B-cell lymphoma. N. Engl. J. Med. 380(1), 45–56 (2019).
19.
United Kingdom National Institute for Health and Care Excellence. Single technology appraisal. Tisagenlecleucel-T for treating relapsed or refractory diffuse large B-cell lymphoma [ID 1166] 2018. (2019). https://www.nice.org.uk/guidance/ta567
20.
Rowen D, Brazier J, Roberts J. Mapping SF-36 onto the EQ-5D index: how reliable is the relationship? Health. Qual Life. Outcomes. 7(27), (2009).
21.
Genentech, Inc. Data on File.
22.
United States Centers for Medicare & Medicaid Services (CMS). ASP pricing file (effective 01/01/2019 - 03/31/2019). (2019). https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Part-B-Drugs/McrPartBDrugAvgSalesPrice/2019ASPFiles.html
23.
United States Centers for Medicare & Medicaid Services (CMS). Physician fee schedule search. (2019). https://www.cms.gov/apps/physician-fee-schedule/overview.aspx
24.
United States Centers for Medicare & Medicaid Services (CMS). Clinical Laboratory Fee Schedule (CLFS) public use file (Updated 01/15/19). (2019). https://www.cms.gov/Medicare/Medicare-Fee-for-ServicePayment/ClinicalLabFeeSched/Clinical-Laboratory-Fee-Schedule-Files.html
25.
Huntington S, Keshishian A, McGuire M et al. Costs of relapsed diffuse large B-cell lymphoma among Medicare patients. Leuk. Lymphoma. 59(12), 2880–2887 (2018).
• This observational study used Medicare claims to analyze the variation in health care costs for patients with diffuse large B-cell lymphoma treated in front-line and the relapsed settings. The results confirmed that older adults with relapsed diffuse large B-cell lymphoma incur higher medical costs, and suggest improving front-line treatment would reduce likelihood of relapse, but would contain health care costs.
26.
Chastek B, Harley C, Kallich J et al. Health care costs for patients with cancer at the end of life. J. Oncol. Pract. 8(6), 75s–80s (2012).
27.
Agency for Healthcare Research and Quality. Healthcare Cost and Utilization Project (HCUP). 2015 HCUPnet (2019). https://hcupnet.ahrq.gov/#setup
28.
United States Bureau of Labor Statistics. Consumer price index – all urban consumers medical care in U.S. city average, all urban consumers, not seasonally adjusted . (2019). https://data.bls.gov/timeseries/CUUR0000SAM
29.
Genentech, Inc. RITUXAN® (rituximab) highlights of prescribing information. (2019). https://www.gene.com/download/pdf/rituxan_prescribing.pdf
30.
Teva Pharmaceuticals USA, Inc. BENDEKA® (bendamustine hydrochloride injection) highlights of prescribing information. (2018). https://www.accessdata.fda.gov/drugsatfda_docs/label/2015/208194s000lbl.pdf
31.
Institute for Clinical and Economic Review (ICER). Overview of the ICER assessment framework and update for 2017–2019. (2019). https://icer-review.org/wp-content/uploads/2018/03/ICER-value-assessment-framework-update-FINAL-062217.pdf
32.
Neelapu SS, Locke FL, Bartlett NL et al. Axicabtagene ciloleucel CAR T-cell therapy in refractory large B-cell lymphoma. N. Engl. J. Med. 377(26), 2531–2544 (2017).
33.
Lin JK, Muffly LS, Spinner MA et al. Cost effectiveness of chimeric antigen receptor T-cell therapy in multiply relapsed or refractory adult large B-cell lymphoma. J. Clin. Oncol. 37(24), 2105–2119 (2019).
34.
Whittington MD, McQueen RB, Ollendorf DA et al. Long-term survival and cost–effectiveness associated with axicabtagene ciloleucel vs chemotherapy for treatment of B-cell lymphoma. JAMA Netw Open. 2(2), e190035 (2019).
35.
Roth JA, Sullivan SD, Lin VW et al. Cost–effectiveness of axicabtagene ciloleucel for adult patients with relapsed or refractory large B-cell lymphoma in the United States. J. Med. Econ. 21(12), 1238–1245 (2018).
36.
Tully S, Feng Z, Grindrod K et al. Developing a discrete-event simulation to study the influence of waiting times on the effectiveness and cost–effectiveness of chimeric antigen receptor (CAR) T-cell therapy in large B-cell lymphoma. Value. In. Health. 22(S521), (2019).
Information & Authors
Information
Published In
Pages: 1003 - 1015
PubMed: 33028076
Copyright
© 2020 Keith A Betts et al. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 9 April 2020
Accepted: 18 August 2020
Published online: 8 October 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
US cost–effectiveness of polatuzumab vedotin, bendamustine and rituximab in diffuse large B-cell lymphoma. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0057
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Matthew Matasar, Javier Sanchez Alvarez, Hélène Parisé, Eric Zuk, Danilo Di Maio, Sheila Shapouri, Eunice Kim, Shih-Wen Lin, Cost-effectiveness analysis of mosunetuzumab for treatment of relapsed or refractory follicular lymphoma after two or more lines of systemic therapy in the United States, Journal of Medical Economics, 10.1080/13696998.2024.2352820, 27, 1, (766-776), (2024).
- Jee H. Choe, Tianzhou Yu, Jeremy S. Abramson, Mohamed Abou-el-Enein, Cost-effectiveness of second-line lisocabtagene maraleucel in relapsed or refractory diffuse large B-cell lymphoma, Blood Advances, 10.1182/bloodadvances.2023011793, 8, 2, (484-496), (2024).
- Fei Fei Liu, Meaghan Bartlett, Samantha Craigie, A Systematic Literature Review of Health-Related Quality of Life Outcomes and Associated Utility Values in Relapsed and/or Refractory Large B Cell Lymphoma, PharmacoEconomics - Open, 10.1007/s41669-023-00464-5, 8, 2, (171-190), (2024).
- Amar H. Kelkar, Edward R. Scheffer Cliff, Caron A. Jacobson, Gregory A. Abel, Stijntje W. Dijk, Eline M. Krijkamp, Robert Redd, Joanna C. Zurko, Mehdi Hamadani, M.G. Myriam Hunink, Corey Cutler, Second-Line Chimeric Antigen Receptor T-Cell Therapy in Diffuse Large B-Cell Lymphoma, Annals of Internal Medicine, 10.7326/M22-2276, 176, 12, (1625-1637), (2023).
- Matthew Matasar, Anthony Masaquel, Rodrigo S. Ho, Aino Launonen, Carmen D. Ng, Rongrong Wang, David Fox, Farah Hossain, Jia Li, John M. Burke, US cost-effectiveness analysis of polatuzumab vedotin in previously untreated diffuse large B-cell lymphoma, Journal of Medical Economics, 10.1080/13696998.2023.2254640, 26, 1, (1134-1144), (2023).
- Melina Sophie Kurte, Ann‐Cathrine Siefen, Florian Jakobs, Bastian von Tresckow, Hans Christian Reinhardt, Florian Kron, Cost‐effectiveness analysis of transplant‐ineligible relapsed or refractory diffuse large B‐cell lymphoma treatment options—Experience of the efficiency frontier approach, European Journal of Haematology, 10.1111/ejh.14095, 111, 6, (895-908), (2023).
- Colin Thomas, Sameep Thapa, Connor McLaughlin, Molly Halloran, Pierluigi Porcu, Point and counterpoint: Polatuzumab vedotin in the front-line therapy for diffuse large B- cell lymphoma, Frontiers in Oncology, 10.3389/fonc.2022.1098375, 12, (2023).
- Adding polatuzumab vedotin cost effective in large B-cell lymphoma, PharmacoEconomics & Outcomes News, 10.1007/s40274-020-7194-6, 864, 1, (4-4), (2020).