Evaluation of a mobile social networking application for improving diabetes Type 2 knowledge: an intervention study using WhatsApp
Abstract
Aim: The aim of this study is to evaluate the WhatsApp social networking application for improving knowledge, self-efficacy and awareness about diabetes management. Methodology: The study was conducted with intervention and control groups at Teaching Hospital in Al-Khobar, Saudi Arabia. The intervention group received weekly educational messages using WhatsApp, while the control group received regular care. Results: Statistically, compared with the control group, the diabetes knowledge and self-efficacy of the intervention group increased significantly after the intervention with the WhatsApp application. Conclusion: The WhatsApp application can be effectively used for enhancing diabetes knowledge, self-efficacy and awareness among the Saudi population.
Diabetes mellitus is one of the most common chronic diseases worldwide, particularly in the Middle East. The disease is classified into two types: Type 1 and Type 2. In Type 1 diabetes, which is also called insulin-dependent diabetes, the body does not produce insulin [1]. This type is found among fewer people; approximately 5% of people suffer with this type of diabetes [1]. In Type 2 diabetes or noninsulin-dependent diabetes, the body does not use insulin properly [2]. This type is the most common among the diabetes population [2]. Various factors such as family history, high blood pressure, lack of physical activity, smoking, unhealthy eating habits, obesity and environmental agents, affect the disease's occurrence. Interestingly, most of the causal factors are related to behavioral aspects like eating habits and exercise [3].
With changes in lifestyles, the likelihood of the disease is also changing. According to the International Diabetes Federation, 387 million people were diagnosed with diabetes worldwide in 2014, which is projected to increase to 592 million by 2035 [4]. Among the 387 million identified with diabetes, 77% of them live in low and middle income countries, which reflect the large diabetes populations in these countries compared with developed countries. Also, an estimated 4.9 million deaths in 2014 were due to diabetes, and diabetes resulted in $612 billion in health expenditures [4]. About 37 million people in the Middle East and North Africa (MENA) region, or 1 in 10 adults, have been diagnosed with diabetes [5]. Saudi Arabia, which belongs to the MENA region, has an estimated diabetic population of 3.8 million, and ranks seventh in the world and first in the region in the prevalence of diabetes [6,7]. In Saudi Arabia, 78% of deaths are caused by chronic diseases, and about 5% of the deaths are caused by diabetes; additionally, expenditures of $1244 per person were incurred in treating diabetes in 2015 [8]. As there is a close relationship between diabetes and other chronic diseases like high blood pressure and coronary heart disease, the risk of developing diabetes is an important aspect that must be considered.
Contemporarily to the increase in its diabetic population, Saudi Arabia has recently been undergoing rapid changes in smartphone usage. Saudi Arabia has one of the highest mobile penetration rates in the world, at a level of 72.8%. More than 60% of mobile phone users in the country access the Internet on their mobile devices for various activities like checking emails and shopping online [9,10]. Also, usage of social networking applications like Facebook, Skype and WhatsApp on mobile devices is increasing rapidly. WhatsApp is a popular social networking mobile application with 500 million users worldwide. In Saudi Arabia, WhatsApp is one of the most popular mobile social networking platforms and is used by 56% of the population [11]. In connection with this work, WhatsApp is also an application that has been widely used in health and healthcare as it is shown in an overall review carried out by Kamel et al. [12]. Also, studies conducted in Mexico, Indonesia and London corroborate the usefulness of using WhatsApp as a tool to increase knowledge about diabetes and help manage the problems caused by this disease [13–15].
Social networking can be useful in various areas and play a significant role in sharing information and transferring knowledge. It can be used in managing chronic diseases like diabetes when there is an immediate need to raise awareness of various behavioral aspects of healthy diet, physical exercise and knowledge of self-management. People can be educated and their awareness levels can be increased through information sharing and discussions via mobile social networking applications, which are very convenient and easy to use. This can rapidly decrease healthcare expenditures in managing such chronic diseases and help people to self-manage their disease effectively.
On the impact of social networks on health outcomes, a review of the literature indicates that these media can contribute to increasing people's awareness of health, medical care and health policies [16]. In several cases it is observed that social networks allow direct communication and information between patients, doctors, nurses and relatives, to receive medical support, emotional support and education about various types of diseases. Another review of the literature presents some cases in which the use of social networks has allowed to transmit messages that can influence the health and behavior of the patient [17]. The work focuses on the acquisition of knowledge, attitudes, self-efficacy, motivation, emotions and changes in the patient's behavior. About this topic, a survey conducted among executives, doctors and directors of clinics, points out that social networks are potentially useful for the provision of health services in chronic diseases because through them communication between the patient and doctors is facilitated. The majority of respondents believe that the use of these means in healthcare is still incipient [18]. Another study presents several applications of mHealth technologies in the management of chronic diseases such as diabetes, cancer and cardiovascular diseases, among others [19]. Additional studies analyze the risks and benefits of social media in healthcare systems [20] or their impact on pharma and healthcare [21] or to promote health equity [22]. In general, these works show the potential of social networks to contribute to the improvement of health.
Social networking platforms such as Facebook and Twitter have support groups in which people can share information and participate in discussions. This approach not only increases patients’ awareness levels but also motivates them to adopt healthy lifestyles to manage diabetes effectively. It can also help them to have a quality discussion with their doctors and enable them to receive and understand proper feedback and medication. Although mobile social networking applications provide various advantages, few studies focus on them in managing diabetes, especially in Saudi Arabia.
Using mobile phones to deliver healthcare services and manage diseases is referred to as mobile health (mHealth) [19]. Several developed countries have implemented mHealth to manage healthcare services, and studies have found positive results from its implementation [5,19]. However, such studies in developing regions are limited, and a gap exists between the understanding of diseases and the use of mobile applications to manage them.
Few studies conducted in Saudi Arabia investigate the effectiveness of mobile technology in managing diabetes. Yet, studies analyzing the use of mobile applications for both disease management and healthcare delivery have achieved positive results [1,3]. Also, similar studies have been conducted in the Middle East. A study on using mHealth systems for diabetes management in Iraq (n = 12) showed a significant reduction in HbA1C levels among the studied population [23]. In this research, the patient is equipped with a smartphone connected by an application to a glucose monitor. Glucose measurements and patient medical data are sent over the Internet to remote medical specialists. The installed application reminds patients of the programming of glucose readings and has a message menu to communicate with medical personnel. HbA1c levels are measured twice a day. As a consequence of this interaction, the HbA1c levels decreased during the intervention study. Likewise, the study found that the satisfaction levels of the patients using the application were significantly high, and the patients were happy to use the mobile application even after the study was over [23].
Another study used short messages services (SMS) to create awareness through education for Type 2 diabetic patients in Basra, Iraq. The study showed that the intervention significantly improved knowledge and awareness among the sample population (n = 50) and significantly reduced HbA1C levels in the patients [24]. A systematic review of similar studies focusing on mobile phone interventions for glycemic control in diabetes self-management found similar results. The study reviewed 22 trials, and a meta-analysis of 1657 participants showed reduced HbA1C values and significant evidence that Type 2 diabetes can be managed efficiently using mobile applications [25].
As well, in a feasibility investigation designed to evaluate the effectiveness of mobile technology (SMS) in Iraq for over 29 weeks, participants’ knowledge levels improved significantly. The mean knowledge score increased from 8.6 (standard deviation [SD]: 1.5) at the baseline to 9.9 (SD: 1.4) after the intervention study. All of the study's participants were highly satisfied with the service and wished to continue using the services even after the study ended [25].
In a nonrandomized controlled trial conducted in Riyadh, Saudi Arabia, the effectiveness of mobile technology (SMS) on improving glycemic control was evaluated by educating 100 participants on how to manage diabetes Type 2 effectively [26]. The intervention was education through SMS services. The study showed significant improvements in the patients’ diabetes knowledge and effective management of their HbA1C levels.
Also, Holtz and Lauckner reviewed 21 articles evaluating the features of mobile technology for managing diabetes [27]. About 71% of the reviewed studies showed significant improvements in HbA1C levels and self-efficacy scores.
Considering the complications associated with Type 2 diabetes as well as factors like increasing mobile penetration in Saudi Arabia, the primary aim of this study is to evaluate the use of a mobile application, WhatsApp, for increasing knowledge, self-efficacy and awareness about diabetes management among patients selected at Teaching Hospital in Al-khobar, Saudi Arabia.
Methodology
Study setting & participants
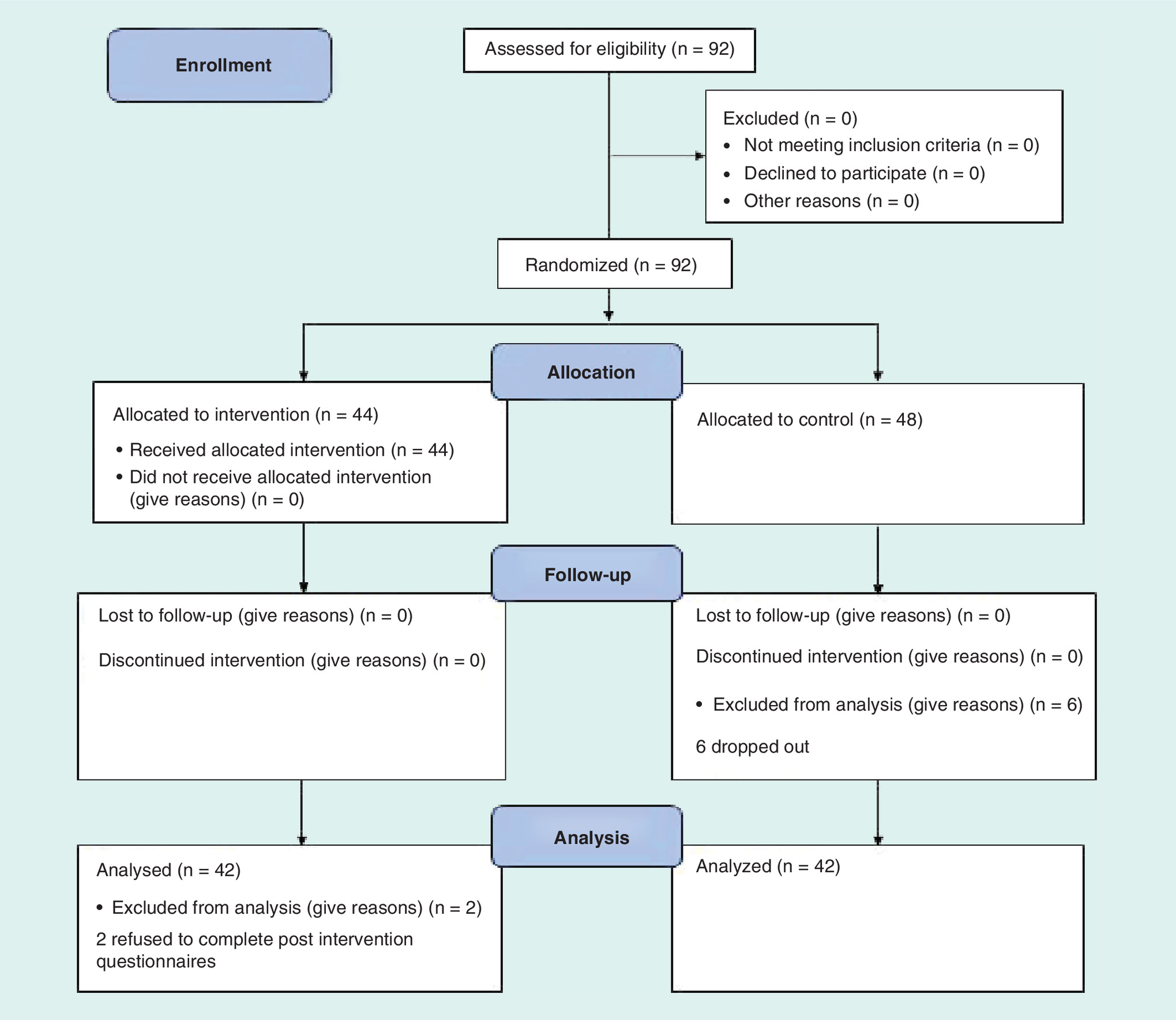
An intervention study was conducted with female Type 2 diabetic patients. We focused on female patients because the prevalence of diabetes Type 2 is higher in women than in men. The participants were selected randomly at Teaching Hospital in Al-Khobar, Eastern Province, Saudi Arabia, on Wednesdays and Thursdays for 6 weeks. The participants were asked to take part in a face-to-face interview, during which the details of the study were explained to them. After providing their consent, the participants were selected and divided into two groups: the control group, whose participants followed their regular diabetes treatment; and the intervention group, whose participants were allowed to use WhatsApp mobile application for increasing their awareness about the disease. The ethical consent for this study was given by the Dammam University, Saudi Arabia. The selection process included enrollment, allocation, follow-up and analysis steps, and the results are shown in Figure 1.
Sampling
A total sample of 82 participants was required, based on the G*Power3.1 software package (www.gpower.hhu.de/fileadmin/redaktion/Fakultaeten/Mathematisch-Naturwissenschaftliche_Fakultaet/Psychologie/AAP/gpower/GPower3-BRM-Paper.pdf). The sample was increased to 92 to account for dropouts. The participants were randomly divided into two groups: the control group (n = 48) and the intervention group (n = 44).
Inclusion & exclusion criteria
Inclusion criterion: female participants with Type 2 diabetes who were not pregnant and without diabetes complications.
Exclusion criterion: pregnant females and males.
Intervention tools
The WhatsApp mobile social networking application was used as the intervention tool. This tool is a messenger application for smartphones and employ Internet to send and receive messages, images, videos and other documents for free [28]. The application allows users to send and receive messages for free using an Internet connection that also allows the exchange of image, video and audio files. The participants utilized their own phones and had experience using the WhatsApp mobile social application. The intervention process is designed for a bidirectional communication and there was not any tailoring to age or education.
The period of intervention was 8 weeks and the study was carried out at Teaching Hospital in Al-Khobar, Eastern Province of Saudi Arabia. During this period, free messages via WhatsApp were sent to the intervention group weekly, but they could be more frequent if it was necessary. The messages were written in Arabic language and had been reviewed by a specialist in diabetes. Its content was about general diabetes care knowledge, diabetes signs and symptoms, pathophysiology, etiology, diet therapy, exercising and other topics. The main educational goal was to improve the level of knowledge of diabetic patients. Meanwhile, the control group did not receive this information and followed their usual diabetes care.
Measurements tools
The Diabetic Knowledge Test (DKT) – a questionnaire comprising 24 items – was used to test general diabetes knowledge among the participants and was adapted from the Diabetes Education Study, TX, USA [29]. The questionnaire was translated into Arabic language so that the participants could easily answer it. Each question had three possible answers: ‘yes’, ‘no’ and ‘I do not know’. One point was awarded for every correct answer and 0 points were awarded for every wrong answer. Each participant took the DKT after the intervention study and at the baseline. After the completion of the intervention, the Dutch/US Diabetes Management Self-Efficacy Scale (DMSES) translated into Arabic was used to measure each patient's efficacy expectations for engaging in 20 self-management Type 2 diabetes activities [26]. The score was recorded on a 1–10 point numerical scale, with higher scores indicating greater levels of self-efficacy. The measurement tools were applied at the baseline and at the end of the study.
Behavioral change model
About the behavioral change model used in our research, we adopted in a general way ‘The Integrated Theory of Health Behavior Change’ which suggests that health behavior change can be enhanced by fostering knowledge and beliefs, increasing self-regulation skills and abilities and enhancing social facilitation [30]. The model indicates that we need an instrument to improve knowledge, self-efficacy and awareness among the participants. In this sense, we use WhatsApp as the intervention tool to send messages about diabetes knowledge in order to promote a behavioral change among the participants. According to the model, when participants receive, analyze and assimilate the information about diabetes, provided through the messages of WhatsApp, improves their knowledge, self-efficacy and awareness, and there is a change in the attitude and behavior of the patient regarding the management of the disease.
In our work, the application of the DKT and the Dutch/US DMSES allow us to measure objectively the behavioral change in terms of knowledge and self-efficacy. In this context, the knowledge of diabetes is connected to the understanding that patients have about this disease and is revealed in the responses that they give in the DKT to 22 specific questions such as signs of the disease, symptoms, medical treatment and physical exercise, among others [31].
In the case of diabetes, self-efficacy is related to the confidence that people have in their abilities to carry out the treatment of diabetes that requires diet, exercise and medical treatment [30]. In this study, self-efficacy is measured by the DMSES engaging participants in 20 self-management Type 2 diabetes activities. In a general way, self-efficacy is a person's ability to perform a practical action successfully. When the individual believes that he is capable of doing something he does it, but if he believes that he cannot do it, he does not.
Concerning awareness about diabetes, it is associated with the perception, understanding and knowledge of the disease, its problems and treatment alternatives [32].
Statistical analysis
The data collected before and after the intervention study were analyzed using the Statistical Package for the Social Sciences (SPSS) version 23 (www.ibm.com/analytics/spss-statistics-software and www.spss-tutorials.com/spss-what-is-it/). The study's findings were considered statistically significant if the probability (p) is less than 0.05 or p < 0.05. The participants’ diabetes knowledge and self-efficacy scores were the primary outcomes of the study. The total number of participants from both groups was 92. G*Power 3.1 was used for power calculation and indicated that 41 participants in each group would result in 80% power for the paired samples t-test when comparing the pre- and post-intervention study scores. The differences between the control and intervention groups were tested using the t-test. Nominal data among the independent groups were compared using the χ2 test.
Results
A total of 84 patients out of 92 participated in the study, with 42 participants in the control group and the other 42 in the intervention group. Of the eight excluded participants, two of them from the intervention group did not complete the poststudy questionnaires, and the remaining six participants dropped out from the study.
The demographic information and the clinical characteristics of the participants are presented in Table 1. According to the table, the application of the Chi-square statistical test expressed in terms of (χ2) and the corresponding probability p indicate that there areno statistical differences in age, education and marital status between the participants of the intervention and control group. However, the duration of diabetes among the participants of the intervention and control group shows a significant statistical difference.
| Variable | Control group (n = 48) | Intervention group (n = 44) | Test statistics | p-value |
|---|---|---|---|---|
| Age (n (%)) ≤40 years ≥41 years | 11 (22.9%) 37 (77.1%) | 11 (25%) 33 (75%) | χ2 = 0.485 | 0.486 |
| Education (n (%)) Diploma or less University | 38 (79.2%) 10 (20.8%) | 34 (77.3%) 10 (22.7%) | χ2 = 0.470 | 0.492 |
| Marital status (n (%)) Married Divorced/widowed Single | 36 (75%) 10 (20.8%) 2 (4.2%) | 30 (68.2%) 8 (18.2%) 6 (13.6%) | χ2 = 4.366 | 0.112 |
| Duration of diabetes (n (%)) ≤5 years 6–10 years 11–15 years ≥15 years | 15 (31.3%) 11 (22.9%) 2 (4.2%) 20 (41.7%) | 17 (38.6%) 6 (13.6%) 11 (25%) 10 (22.7%) | χ2 = 21.766 | < 0.001 |
The pre- and post-scores of both groups underwent paired comparison using paired t-test to compare the change in diabetes knowledge and self-efficacy, as shown in Table 2. These results indicate that there was a statistically significant change in diabetes knowledge and self-efficacy between the baseline and the end of the study in the intervention group, but not in the control group.
| Group | Outcome measure | Mean ± SD | 95% CI | p-value |
|---|---|---|---|---|
| Control | Preknowledge Postknowledge Pre self-efficacy Post self-efficacy | 13.81 ± 1.96 13.85 ± 1.81 5.97 ± 2.05 6.02 ± 2.01 | -0.78–0.86 -0.83–0.93 | 0.92 0.91 |
| Intervention | Preknowledge Postknowledge Pre self-efficacy Post self-efficacy | 14.45 ± 2.38 21.28 ± 1.59 6.65 ± 1.47 7.34 ± 1.26 | 5.95–7.71 0.10–1.23 | < 0.001 < 0.001 |
SD: Standard deviation.
Table 3 compared the changes of knowledge and self-efficacy between the control and the intervention group using the t-test. The findings suggest that if compared with the control group, the intervention group had a significantly greater improvement in knowledge and self-efficacy.
| Outcome measure | Group | Mean ± SD | 95% CI | p-value |
|---|---|---|---|---|
| Post knowledge level | Control Intervention | 13.85 ± 1.81 21.8 ± 1.59 | 7.21–8.69 | <0.001 |
| Post self-efficacy level | Control Intervention | 6.02 ± 2.01 7.34 ± 1.26 | 0.59–2.05 | < 0.001 |
SD: Standard deviation.
From above Tables, for knowledge and self-efficacy of the control group were p = 0.92 and 0.91, respectively. While, for the intervention group p-values were < 0.001 for both knowledge and self-efficacy.
Discussion
According to this work, the statistical results obtained from the application of the χ2 shown in Table 1 indicate that there are no significant differences between the demographic characteristics such as age, marital status and education of both groups. However, the diabetes duration presents significant statistical differences among both groups. In general, the average pre-intervention scores of the participants were 13–14.5 for diabetes knowledge and 6 for self-efficacy.
Similarly, the pre- and post-scores of both groups analyzed by the t-test displayed in Table 2 show that the mean diabetes knowledge of the intervention group at the baseline was 14.45 (SD: 2.38), and increased to 21.28 (SD: 1.59) after the intervention. In the same way, the mean self-efficacy of the intervention group at the baseline was 6.65 (SD: 1.47) and increased to 7.34 (SD: 1.26) after the intervention process. In addition, the statistical information demonstrates that the control group does not show a significant improvement in diabetes knowledge and self-efficacy. In other words, the intervention group with the WhatsApp social networking application revealed a significant increase in diabetes knowledge and self-efficacy levels (p < 0.001), compared with no significant improvement in the control group.
Analogously, the change of scores between the control and intervention groups described in Table 3 points out that related to the control group there is a statistically significant increase in diabetes knowledge and self-efficacy in the intervention group, after the utilization of the WhatsApp social networking application (p-value < 0.05).
In consequence, Tables 1, 2 & 3 show that diabetes knowledge and self-efficacy levels increased significantly with the WhatsApp social networking application in the intervention group. Regarding the control group, where the WhatsApp social networking application was not used, diabetes knowledge and self-efficacy levels did not improve meaningfully.
According to this research, the changes in knowledge and self-efficacy scores, in addition to being statistically significant, are also meaningful because it makes sense to conclude that the participants of the intervention group who received information about diabetes were able to improve their diabetes knowledge, thanks to the system of messages sent through WhatsApp. On the other hand, we can expect that the participants in the control group, who did not use WhatsApp to receive any information about this disease, did not improve their knowledge and self-efficacy. These results are in agreement with the behavioral change model employed in this research [31].
Other studies have shown significant improvement in diabetes management after deploying mobile technologies to deliver healthcare {1,3,7,10]. However, despite these results, the research on adopting mobile technologies for healthcare delivery in Saudi Arabia is limited, although a few studies have been conducted in the MENA region [3,25–27].
Regarding this work, it is pertinent to comment that it presents some limitations since it mainly focuses on diabetes knowledge and self-efficacy while neglecting other healthcare services like reminders, general support messages and appointment reminders. Also, the HbA1C levels of the patients were not used in the analysis process. Another limitation of our work is that we did not evaluate the effect of ‘participant contact’ from the intervention content.
The scope for further research may involve many aspects that can be included and analyzed in future studies. For example, we may use WhatsApp interconnected with a similar system to that employed in Iraq study to measure the Hb1Ac levels of participants; then, the HbA1C levels of the patients and general support messages can be used as a measurement tool for effective analysis of the intervention [23]. In addition, different behavioral therapies can be integrated with mobile applications to analyze their impact on diabetes management. Also, future research may also focus on expanding the service areas offered through mobile applications, which could lead to a major breakthrough for healthcare service delivery in Saudi Arabia. Finally, future mHealth research work in this area is currently underway to conduct a larger scale study.
Conclusion
Considering the increasing adoption of mobile technologies in Saudi Arabia, this study investigates the scope of mobile technologies, specifically social networking applications like WhatsApp, in diabetes management, and shows that this technology is significantly operative in managing this disease. The results indicate that the WhatsApp messenger mobile application can be used as an effective tool to improve diabetes knowledge and self-efficacy. Up to the level of knowledge of the author, this is the first study of this type applied in Saudi Arabia.
This work evaluates the use of WhatsApp for improving knowledge, self-efficacy and awareness about diabetes management.
The study was conducted with an intervention and control groups at Teaching Hospital in Al-Khobar, Eastern Province, Saudi Arabia.
Pre- and post-intervention scores on diabetes knowledge and self-efficacy from both groups were analyzed using the χ2 and the t-test.
At the baseline, the mean diabetes knowledge of the intervention group was 14.45 (SD: 2.38) and this value increased to 21.28 (SD: 1.59) after the intervention with the WhatsApp application.
The mean self-efficacy of the intervention group rose from 6.65 (SD: 1.47) to 7.34 (SD: 1.26) during the intervention.
Related to the control group, there is a statistically significant increase in diabetes knowledge and self-efficacy in the intervention group.
No significant improvements were noted in the control group.
The observed changes in the intervention group were meaningful and statistically significant.
WhatsApp can be used as an effective tool to provide knowledge, self-efficacy and awareness about diabetes management among the Saudi population.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Alanzi TM, Istepanian RS, Philip N, Sungoor A. A study on perception of managing diabetes mellitus through social networking in the kingdom of Saudi Arabia. In: XIII Mediterranean Conference on Medical and Biological Engineering and Computing 2013 2014. Roa Romero L (Ed.). Springer, Cham, 1907–1910 (2014).
2.
International Diabetes Federation. Diabetes Atlas released on World Diabetes Day (5th Edition) (2015). http://www.diabetesatlas.org/.
3.
Alanzi T, Istepanian R, Philip N. Design and usability evaluation of social mobile diabetes management system in the Gulf region. JMIR Res. Protoc. 5(3), e93 (2016).
4.
International Diabetes Federation. Key findings 2014 (2016). http://www.idf.org/diabetesatlas/update-2014.
5.
Rehalia A, Prasad S. Global harnessing of advanced mHealth for community mobilization. mHealth 2, 7 (2016).
6.
Sherif S. Economic development and diabetes prevalence in MENA countries: Egypt and Saudi Arabia comparison. World J. Diabetes 6(2), 304 (2015).
7.
Majeed A, El-Sayed A, Khoja T, Alshamsan R, Millett C, Rawaf S. Diabetes in the Middle-East and North Africa: an update. Diabetes Res. Clin. Prac. 103(2), 218–222 (2014).
8.
Bahijri SM, Jambi HA, Al Raddadi RM, Ferns G, Tuomilehto J. The prevalence of diabetes and prediabetes in the adult population of Jeddah, Saudi Arabia – a community-based survey. PLoS ONE 11(4), e0152559 (2016).
9.
AlQulaity M, Bajaber W. In: The Growth of E-commerce in Saudi Arabia and its Influence on Saudi women (1st Edition). GRIN Verlag, Germany (2015). https://books.google.com.sa/books/about/The_Growth_of_E_Commerce_in_Saudi_Arabia.html?id=V0iRDAAAQBAJ&redir_esc=y&hl=en.
10.
Jamal A, Temsah M, Khan S et al. Mobile phone use among medical residents: a cross-sectional multicenter survey in Saudi Arabia. JMIR MHealth UHealth. 4(2), 61 (2016).
11.
WhatsApp: mobile usage penetration by country | Statista (2016). https://www.statista.com/statistics/291540/mobile-internet-user-whatsapp/.
12.
Kamel M, Giustini D, Wheeler S. Instagram and WhatsApp in health and healthcare: an overview. Future Internet 8(3), 37 (2016).
• Analyzes the use of WhatsApp as a healthcare tool.
13.
Saavedra J. Social networks as a means of monitoring patients with hypertension and diabetes success story. Int. J. Integr. Care. 15, 74–77 (2015).
• Analyzes the use of WhatsApp as a healthcare tool.
14.
Ekadinata N, Widyandana D. Health promotion using WhatsApp-based images and texts for voluntary primary health workers. Berita Kedokteran Masyarakat. 33(11), (2017) (Epub ahead of print).
• Analyzes the use of WhatsApp as a healthcare tool.
15.
Blackstock S, Solomon S, Kumar P. Using WhatsApp messaging to improve engagement of young adolescents with Type 1 diabetes mellitus. Endocrine J. 39, (2015) (Epub ahead of print).
• Analyzes the use of WhatsApp as a healthcare tool.
16.
Griffiths F, Dobermann T, Cave J et al. The impact of online social networks on health and health systems: a scoping review and case studies. Policy Internet 7(4), 473–496 (2015).
17.
Welch V, Petkovic J, Simeon R. Interactive social media interventions for health behaviour change, health outcomes, and health equity in the adult population. Cochrane Public Health Group (2018). http://cochranelibrary-wiley.com/doi/10.1002/14651858.CD012932/abstract;jsessionid=FAC457D64680DFE8EED3BF5869A56AEC.f04t03.
18.
Volppk K, Molita N. Social networks to improve patient health. Insights Report. NEJM Catalyst (2017). https://catalyst.nejm.org/.
19.
Istepanian RSH, Woodward B. mHealth: Fundamentals and Applications. Wiley – IEEE Press, NJ, USA (2016).
•• This is an interesting book about the applications of mHealth technologies.
20.
Kotsilieris T, Pavlaki A, Christopolou S, Anagnostopoulos I. The impact of social networks on healthcare. Social Network Analysis and Mining 7(1), 18 (2017).
21.
Limaye N, Saraogi A. How social media is Transforming Pharma and Healthcare. Applied. Clinical. Trials. 27(2), (2018).
22.
Welch V, Petkovic J, Pardo J et al. Interactive social media interventions to promote health equity: an overview of reviews. Health Promot. Chronic. Dis. Prev. Can. 36(4), 63–75 (2016).
23.
Istepanian R, Mousa A, Haddad N et al. The potential of m-health systems for diabetes management in post-conflict regions a case study from Iraq. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2014, 3650–3653 (2014).
•• This study describes the improving Hb1Ac levels with mHealth technologies.
24.
Mulvaney D, Woodward B, Datta S et al. Development of m-health monitoring systems in India and Iraq. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2012, 288–291 (2012).
25.
Haddad NS, Istepanian R, Philip N et al. A feasibility study of mobile phone text messaging to support education and management of Type 2 diabetes in Iraq. Diabetes Technol. Ther. 16(7), 454–459 (2014).
26.
Bijl J, Poelgeest-Eeltink A, Shortridge-Baggett L. The psychometric properties of the diabetes management self-efficacy scale for patients with Type 2 diabetes mellitus. J. Adv. Nurs. 30(2), 352–359 (1999).
27.
Holtz B, Lauckner C. Diabetes management via mobile phones: a systematic review. Telemed. J. E. Health 18(3), 175–184 (2012).
28.
WhatsApp. www.whatsapp.com/.
29.
Garcia A, Villagomez E, Brown S, Kouzekanani K, Hanis C. The Starr County Diabetes Education Study: development of the Spanish language diabetes knowledge questionnaire. Diabetes Care. 24(1), 21–22 (2001).
30.
Dehghan H, Charkazi A, Kouchaki G et al. General self-efficacy and diabetes management self-efficacy of diabetic patients referred to diabetes clinic of Aq Qala, North of Iran. J. Diabetes Metab. Disord. 16, 8 (2017).
31.
Tawalbeh L, Gharaibeh B. Diabetes knowledge among university nursing students in the North of Jordan. Pakistan J. Nutr. 13(12), 728–734 (2014).
•• This work presents an interesting analysis of the behavioral change model.
32.
Diabetes awareness. www.diabetes.co.uk/diabetes-awareness.html.
Information & Authors
Information
Published In
Copyright
© 2018 Future Medicine Ltd.
History
Received: 2 April 2018
Accepted: 7 June 2018
Published online: 26 June 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Evaluation of a mobile social networking application for improving diabetes Type 2 knowledge: an intervention study using WhatsApp. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0028
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Anstan Saldanha, Anna Boggis, Anna Sofia Serlachius, Digital health interventions for improving mental health outcomes and wellbeing for adults with diabetes: A systematic review, Patient Education and Counseling, 10.1016/j.pec.2026.109659, 149, (109659), (2026).
- EunSeok Cha, Meihua Ji, Colleen Dawkins, Xiaoyan Qi, Hyesun Jang, Melissa Spezia Faulkner, Characteristics of behavior change techniques in theory-based self-management education and support interventions for adults with type 2 diabetes using digital technology: A scoping review, DIGITAL HEALTH, 10.1177/20552076261443759, 12, (2026).
- Shan Chen, Emma Mirza Wati Mohamad, Arina Anis Azlan, Xixi Zhao, Instant messaging-based digital health interventions for diabetes management: a domain-structured systematic review and meta-analysis of randomized controlled trials, Frontiers in Public Health, 10.3389/fpubh.2026.1780625, 14, (2026).
- Hwee Wen Ong, Khairul Anwar Ayob, David Siew-Kit Choon, Virginia Hartono, Metabolic Optimisation in Total Joint Arthroplasty: A Single-Centre Retrospective Cohort Pilot Study on the Safety and Feasibility of a Digitally Supported Perioperative Diet Modification, Journal of Clinical Medicine, 10.3390/jcm15051948, 15, 5, (1948), (2026).
- Ola Sukkarieh, Leonard Egede, Mona Osman, Maya Bassil, Myrna A. A. Doumit, Reimagined diabetic care approach: A qualitative study on the acceptability of mhealth interventions in a LMIC, PLOS One, 10.1371/journal.pone.0343711, 21, 2, (e0343711), (2026).
- Michelli Caroliny de Oliveira, Inara Pereira da Cunha, Karine Laura Cortellazzi, Gláucia Maria Bovi Ambrosano, Fernanda Dandara Marques Gomes de Morais, Luciane Miranda Guerra, Antonio Carlos Pereira, Jaqueline Vilela Bulgareli, Using social media application associated with active learning methodologies for adherence to dental treatment, Brazilian Journal of Oral Sciences, 10.20396/bjos.v24i00.8668221, 24, (e258221), (2025).
- Manoela Vieira Gomes da Costa, Renata Puppin Zandonadi, Verônica Cortez Ginani, Silvana Schwerz Funghetto, Luciano Ramos de Lima, Tania Cristina Morais Santa Barbara Rehem, Marina Morato Stival, Connecting Health and Technology: Validation of Instant Messaging for Use as Diabetes Mellitus Control Strategy in Older Brazilian Adults, International Journal of Environmental Research and Public Health, 10.3390/ijerph22020282, 22, 2, (282), (2025).
- Ali Safdari, Nazi Nejat, Abdollah Abolfathi, Fatemeh Mehrabi, Fatemeh Rafiei, Effect of social media-based education on self-care status, health literacy, and glycated hemoglobin in patients with type 2 diabetes, Frontiers in Public Health, 10.3389/fpubh.2025.1507726, 13, (2025).
- Fatemeh Abbasian, Mohammad Mehdi Naghizadeh, Leila Ahmadian, Effect of WhatsApp Messenger-based education on the knowledge of health ambassadors about home care for minor illnesses, BMC Health Services Research, 10.1186/s12913-024-11988-9, 24, 1, (2024).
- Pedro F. Castillo-Valdez, Marisela Rodriguez-Salvador, Yuh-Shan Ho, Research Landscape of Diabetes mHealth Technologies, Foresight and STI Governance, 10.17323/2500-2597.2024.1.19.32, 18, 1, (19-32), (2024).
- See more