Comparative effectiveness of avelumab versus chemotherapy in Merkel cell carcinoma: innovative use of patient insights
Abstract
Aim: To assess patient experience with chemotherapy and avelumab in metastatic Merkel cell carcinoma (mMCC). Methods: In the JAVELIN Merkel 200 trial, chemotherapy-refractory mMCC patients could participate in optional qualitative interviews at baseline documenting recollection of previous chemotherapy experience, and at weeks 13/25 documenting current experience with avelumab. Functional Assessment of Cancer Therapy subscale for melanoma questionnaire (FACT-M) was administered in parallel. Results: In our sample, chemotherapy was associated with an unpleasant experience. On selected FACT-M items addressing chemotherapy-impacted concepts, most patients receiving avelumab were improved or stable; few worsened. In addition, a few patients spontaneously reported experiencing less toxicity with avelumab than experienced during previous chemotherapy. Conclusion: This approach merging qualitative and quantitative data suggests that mMCC patients report a better experience with avelumab than with chemotherapy.
Merkel cell carcinoma (MCC) is a rare and aggressive skin cancer. In Europe, the incidence rate is 0.2–0.4 cases per 100,000 person-years, while in the USA it is 0.7 cases per 100,000 person-years [1,2]. MCC is associated with a poor prognosis. The 5-year overall survival rate with metastatic MCC (mMCC) is estimated at between 0 and 18% [3–6].
Two retrospective studies, one based on a European registry, the other one on a US registry, recently showed that chemotherapy, whether as first-line, second-line or later, was associated with only a brief duration of tumor response and a poor overall survival in most patients with mMCC, further demonstrating that chemotherapy is not considered a standard of care [7,8]. The short duration of response is in line with Voog et al. [6] who reported in their analysis of 72 patients with mMCC, that while 57% initially responded to chemotherapy treatment, the median overall survival from the date of initiation of chemotherapy was 9 months for patients with metastatic disease. The poor overall survival of patients treated with chemotherapy for metastatic disease has been previously reported. Santamaria et al. [5] reported that of 161 patients with MCC treated between 1980 and 2010, the 5-year survival rate of those diagnosed with stage IV metastatic disease was 0% and adjuvant (post surgery) treatments, such as radiation and chemotherapy, did not improve survival rates.
Given the high unmet medical need in patients with mMCC, avelumab, a fully human anti-PD-L1 monoclonal antibody, was approved in 2017 by the US FDA and EMA to treat patients 12 years and older with mMCC. These approvals were based on data from an open-label, single-arm, multi-center clinical trial (JAVELIN Merkel 200, NCT02155647), which demonstrated a clinically meaningful and durable overall response rate with a manageable safety profile [9,10].
In addition to documenting clinical effectiveness within clinical trials, in recent years it has become increasingly important to document treatment benefit and meaningfulness from the patient perspective [11]. There are a number of patient reported outcome (PRO) measures validated for use in clinical trials for cancer in general, and particularly for more prevalent cancers [12–14]. Of these, the Functional Assessment of Cancer Therapy subscale for melanoma (FACT-M) assesses three domains seen to be important for patients with skin cancer more generally [15]: physical well-being, emotional well-being and social well-being. At the time the study was conducted, there was no disease-specific PRO measure developed for MCC. As melanoma and MCC share many similarities, both being aggressive skin cancers, the FACT-M was administered to patients with mMCC and demonstrated acceptable psychometric properties; the questionnaire being valid, reliable and sensitive to changes over time in this disease population [16].
In the context of rare diseases, the patient perspective or PRO assessments are seldom documented, and was never reported for MCC prior to JAVELIN Merkel 200, a registrational, single-arm, multicenter, international Phase II trial (NCT02155647) [9]. In that trial, the FACT-M data were used to document a gain in quality of life for patients with non progressive mMCC during treatment with avelumab [17]. Further, investigational drug clinical trials in high unmet medical need disease lacking a standard of care treatment tend then to be single arm studies which do not allow assessment of comparative effectiveness using randomized data. This is the case for the JAVELIN Merkel 200 trial investigating the efficacy and tolerability of avelumab in patients with mMCC.
We propose here a mixed methods research-based innovative approach to explore and compare whether chemotherapy and related side effects impact patients’ quality of life to a greater or lesser extent than when compared with avelumab in mMCC. For this purpose, we used qualitative historic experience with chemotherapy along with quantitative and supportive qualitative data with avelumab from a single arm study. The use of mixed methods research, which combines qualitative and quantitative data, may be a viable method to inform understanding of treatment benefit from the patient perspective [18]. Specifically, the objective of this project was to assess patients’ recollection of experience with previous chemotherapy treatment, as described by patients using their own words (qualitative insights), and compare with patients’ current experience of avelumab as described using quantitative (FACT-M) outcomes and supportive qualitative follow-up interviews.
Patients & methods
Study design
88 patients with histologically confirmed mMCC were enrolled in JAVELIN Merkel 200 part A, a registrational, single-arm, multicenter, international Phase II trial [9]. Patients were 18 years of age or older, and chemotherapy-refractory with disease progression after at least one line of chemotherapy for mMCC prior to entering the trial [9]. Methodological details of the JAVELIN Merkel 200 part A trial, as well as efficacy and safety outcomes, have been previously reported by Kaufman et al. [9].
Patient-reported outcomes
Qualitative interviews
As defined in the JAVELIN Merkel 200 trial protocol, study eligible patients were invited to participate in 30-minute semi-structured optional phone interviews at three predefined time-points during the trial. The first was at baseline prior to commencement of avelumab treatment, and the second and third were at study week 13 and 25 after avelumab initiation. Only patients still active in the trial and still willing to participate in interviews were interviewed at follow-up time-points.
Baseline interviews documented patient recollection of their previous experiences with chemotherapy and radiotherapy prior to study entry, and how these treatments impacted their everyday lives. Week 13 and 25 interviews documented patient current experiences, and impacts of avelumab as they progressed through treatment within the trial.
Nondirective interview techniques were employed to promote spontaneous answers from patients. As necessary, probing questions were used to collect additional follow-up details, explanations and examples. Interviews were audio-recorded, then transcribed verbatim. De-identified interview transcripts were then analyzed. A thematic approach was used for coding baseline interviews, which consisted of attributing a tag to represent the main ideas associated with words, phrases and paragraphs within the transcripts. These tags were then drawn out and compared with one another to identify concepts important to patients. For the Week 13 and Week 25 interviews, transcripts were coded at the individual level to explore the experience of each patient over time.
FACT-M
The FACT-M questionnaire includes 51 items, which are answered on 5-point Likert scales ranging from 0 (not at all) to 4 (very much) [15,19]. Patients were instructed to answer all items and select ‘not at all’ if they felt that the item was not applicable to them. The items are grouped into six subscales (Physical well-being, Social well-being, Emotional well-being, Functional well-being, Melanoma and Melanoma surgery). The FACT-M questionnaire was electronically completed at sites at baseline, week 13 and week 25. Psychometric properties of the FACT-M in the mMCC population have been demonstrated [16].
Mixed method research approach
In the absence of existing PRO data that document the impact of chemotherapy in mMCC population or randomized trial among this patient population to refer to, qualitative interviews were used to document the patients’ recollection of their experience with prior chemotherapy (baseline interviews) and their current experience with avelumab (follow-up interviews). Based on the analysis of the baseline interviews, a list of concepts patients reported around chemotherapy was developed. Subsequently the FACT-M was reviewed to select items matching these concepts. Next, these items were described over the course of the trial (week 13 and week 25) among patients with FACT-M data available, to explore if more patients remain the same or improve (change in the positive direction from baseline) than decline (change in the negative direction from baseline) on avelumab. The demographic and clinical characteristics, as well as the FACT-M response distribution at baseline of the interviewed patients were compared with the patients not interviewed using parametric tests (t-test for two-group comparison and ANOVA for comparisons between more than two groups).
Analyses
All qualitative analyses were performed using the Atlas.ti software package [20]. All statistical descriptive analyses of the FACT-M items were performed using SAS software for Windows (Version 9.4, SAS Institute Inc., NC, USA).
Results
Study population
In total, 88 patients were enrolled in the JAVELIN Merkel 200 part A; this population has been described elsewhere [9]. Seventy patients completed the FACT-M at baseline, 38 out of 57 at week 13 and 27 out of 45 at week 25.
Of the 88 patients, 19 patients accepted to participate in the optional baseline telephone interviews, out of which 18 completed the FACT-M. Nine patients completed both week 13 and week 25 follow-up interviews and had FACT-M data available.
Table 1 describes the characteristics of the subsample of interviewed patients overall and with FACT-M data and the subsample of patients not interviewed overall and with FACT-M data at baseline and follow-up. The two subsamples of interviewed and not interviewed patients with FACT-M data were not different demographically or clinically with regard to baseline metastatic tumor size and location, time since initial diagnosis and since first metastatic disease and number of previous therapy lines (p > 0.05). However, the interviewed sample consisted mainly of individuals from the USA, and as the sample sizes are small, the numerical differences in the site of tumor and tumor size may be important.
| Timepoint | Characteristics | All patients | Patients with FACT-M data | ||||
|---|---|---|---|---|---|---|---|
| Interviewed patients | Patients not interviewed | p-value | Interviewed patients | Patients not interviewed | p-value | ||
| Baseline | n of patients | 19 | 69 | 18 | 52 | ||
| Gender (Male) - n (%): | 15 (78.9) | 50 (72.5) | 0.770 | 14 (77.8) | 38 (73.1) | 0.765 | |
| Age (years) - Mean (SDev) | 72.26 (8.18) | 69.01 (11.26) | 0.244 | 72.33 (8.41) | 69.46 (11.99) | 0.352 | |
| Country – n (%) | |||||||
| Australia | 0 (0.0) | 5 (7.2) | 0.110 | 0 (0.0) | 5 (9.6) | 0.048 | |
| Spain | 0 (0.0) | 2 (2.9) | 0 (0.0) | 1 (1.9) | |||
| France | 0 (0.0) | 10 (14.5) | 0 (0.0) | 6 (11.5) | |||
| Germany | 2 (10.5) | 6 (8.7) | 1 (5.6) | 6 (11.5) | |||
| Italy | 0 (0.0) | 8 (11.6) | 0 (0.0) | 7 (13.5) | |||
| Japan | 0 ( 0.0) | 3 (4.3) | 0 (0.0) | 3 (5.8) | |||
| Switzerland | 0 (0.0) | 1 (1.4) | 0 (0.0) | 1 (1.9) | |||
| USA | 17 (89.5) | 34 (49.3) | 17 (94.4) | 23 (44.2) | |||
| Body Mass Index (kg/m2) – Mean (SDev) | 29.42 (8.04) | 27.81 (5.35) | 0.308 | 29.49 (8.27) | 27.35 (5.27) | 0.210 | |
| ECOG PS – n (%) | |||||||
| 0 = Fully active | 10 (52.6) | 39 (56.5) | 0.763 | 10 (55.6) | 28 (53.8) | 0.900 | |
| 1 = Restricted in physically strenous activity | 9 (47.4) | 30 (43.5) | 8 (44.4) | 24 (46.2) | |||
| Site of primary tumor – n (%) | |||||||
| Non-Skin | 4 (21.1) | 10 (14.5) | 0.501 | 4 (22.2) | 5 (9.6) | 0.230 | |
| Skin | 14 (73.7) | 53 (76.8) | 13 (72.2) | 42 (80.8) | |||
| Missing | 1 (5.3) | 6 (8.7) | 1 (5.6) | 5 (9.6) | |||
| Tumor size at baseline (mm) – Mean (SDev) | 83.25 (49.89) | 105.62 (81.17) | 0.298 | 83.53 (51.63) | 110.26 (86.35) | 0.263 | |
| Years since initial diagnosis – Mean (SDev) | 2.32 (0.75) | 2.17 (0.79) | 0.483 | 2.28 (0.75) | 2.15 (0.83) | 0.577 | |
| Months since first metastatic disease – Mean (SDev) | 16.26 (10.37) | 16.46 (23.31) | 0.971 | 16.57 (10.58) | 17.07 (26.57) | 0.939 | |
| Number of previous therapy lines – Mean (SDev) | 1.32 (0.48) | 1.65 (0.89) | 0.117 | 1.33 (0.49) | 1.52 (0.75) | 0.333 | |
| Time since prior chemotherapy discontinuation (months) – Mean (SDev) | 1.39 (0.99) | 1.60 (1.58) | 0.602 | 1.35 (1.00) | 1.53 (1.08) | 0.556 | |
| Best response to prior chemotherapy – n (%) | |||||||
| CR | 3 (15.8) | 8 (11.6) | 0.379 | 2 (11.1) | 3 (5.8) | 0.259 | |
| PR | 3 (15.8) | 5 (7.2) | 3 (16.7) | 5 (9.6) | |||
| SD | 7 (36.8) | 15 (21.7) | 7 (38.9) | 9 (17.3) | |||
| PD | 6 (31.6) | 31 (44.9) | 6 (33.3) | 25 (48.1) | |||
| Missing | 0 (0.0) | 10 (14.5) | 0 (0.0) | 10 (19.2) | |||
| Week 13 | Still active in the study – n | 14 | 43 | 12 | 26 | ||
| Still on avelumab treatment – n (%) | 7 (50.0) | 19 (44.2) | 0.704 | 5 (41.7) | 16 (61.5) | 0.252 | |
| Best response by IERC to avelumab – n (%) | |||||||
| CR | 1 (7.1) | 7 (16.3) | 0.592 | 1 (8.3) | 5 (19.2) | 0.480 | |
| PR | 7 (50.0) | 13 (30.2) | 5 (41.7) | 12 (46.2) | |||
| SD | 1 (7.1) | 7 (16.3) | 1 (8.3) | 4 (15.4) | |||
| PD | 4 (28.6) | 11 (25.6) | 4 (33.3) | 3 (11.5) | |||
| Missing | 1 (7.1) | 5 (11.6) | 1 (8.3) | 2 (7.7) | |||
| Week 25 | Still active in the study – n (%) | 12 | 33 | 9 | 18 | ||
| Still on avelumab treatment – n (%) | 7 (58.3) | 19 (57.6) | 0.964 | 6 (66.7) | 14 (77.8) | 0.653 | |
| Best response by IERC to avelumab – n (%) | |||||||
| CR | 1 (8.3) | 7 (21.2) | 0.290 | 1 (11.1) | 5 (27.8) | 0.424 | |
| PR | 7 (58.3) | 11 (33.3) | 6 (66.7) | 7 (38.9) | |||
| SD | 0 (0.0) | 5 (15.2) | 0 (0.0) | 2 (11.1) | |||
| PD | 3 (25.0) | 5 (15.2) | 1 (11.1) | 1 (5.6) | |||
| Missing | 1 (8.3) | 5 (15.2) | 1 (11.1) | 3 (16.7) | |||
CR: complete response; FACT-M: Functional Assessment of Cancer Therapy subscale for melanoma; PD: progressive disease; PR: partial response; SD: stable disease; SDev: standard deviation.
Experience with chemotherapy
It is known that in mMCC, responses to chemotherapy are nondurable and almost all patients experience disease progression after chemotherapy [5–8]. Patients who entered the trial were patients who were previously treated with chemotherapy for their mMCC, but experienced disease progression. Although some patients recalled an initial benefit linked to chemotherapy treatment with the tumors shrinking or slowing of the disease progression, as their physicians had told them, most patients reported that the chemotherapy did not have long lasting effects. This disease progression happened weeks to months after the end of their chemotherapy treatment: “I realize now that they don't work. They're stuff that's proved etc., but they don't work in the short term and they hope they work, maybe they could work, but with Merkel cell they don't have a lasting effect” (patient 2).
Overall, 12 patients out of 19 (63%) spontaneously recalled experiencing fatigue and exhaustion following chemotherapy. The fatigue had a substantial impact on patients’ physical abilities and everyday lives as they were slowed down and had to rest much more than usual. “I was just, I mean I was just wiped out you know from… I had no energy […] I spent a lot of time in bed, just lying there… I just didn't feel like doing anything. I had, you know, a little bit of nausea” (patient 16). “I'd go outside to do some work outside in the yard and after about 20 minutes or so, I'd say I gotta go sit down” (patient 19). “It's slowed me down. I'm a very active person and we like to travel, probably abroad, and do things, but we haven't been able to travel, because of treatments” (patient 7).
Additionally, nine patients out of 19 (47%) spontaneously recalled nausea and/or vomiting. Appetite loss was reported by five (26%) patients and hair loss and sleep disturbances by three (16%) patients each. Other side effects were reported by one to three patients. In total, only two patients out of the 19 (11%) interviewed reported no adverse events from chemotherapy. Chemotherapy was described as ‘very disruptive’ (patient 3), ‘debilitating’ (patient 9) ‘devastating’ (patient 1) and compared to ‘poison’ (patient 5), or qualified as ‘nasty stuff’ (patient 11).
Avelumab versus chemotherapy based on quantitative (FACT-M items) data
Based on the analysis of the qualitative interview parts about patients’ recollection of experience with chemotherapy they had received in the past, the items of the FACT-M were screened. Items matching a concept raised during the qualitative interviews were selected. The analysis presented below explored the proportion of patients who were improved or stable or worsened on this selection of items after 13 and 25 weeks of treatment with avelumab. Given that the interviewed and not interviewed patients had no different demographic or key clinical characteristics (i.e., those defined above and presented in Table 1), the descriptive analysis was conducted on all patients with FACT-M data available at week 13 (n = 38) and at week 25 (n = 27). Selected items were related to physical functioning: “I have a lack of energy,” “I feel fatigued” and “I have to limit my physical activity because of my condition”; side effects: “I have nausea,” “I have a good appetite” and “I am bothered by side effects of treatment”; and other aspects of quality of life: “I am able to work (including work at home)”, “I am able to enjoy life”, “I am content with the quality of life right now,” “I have to limit my social activity because of my condition” and “I isolate myself from others because of my condition,” and “I have difficulty thinking clearly (remembering, concentrating).”
As shown in Figure 1, at both week 13 and week 25, the majority of patients were either stable or improved on all selected items. Approximately 10–40% of the participants reported some worsening varying at the two time-points, with one exception reporting some worsening in over 40% to nearly 50% of patients at both week 13 and 25 for the item “I am content with the quality of life right now.”
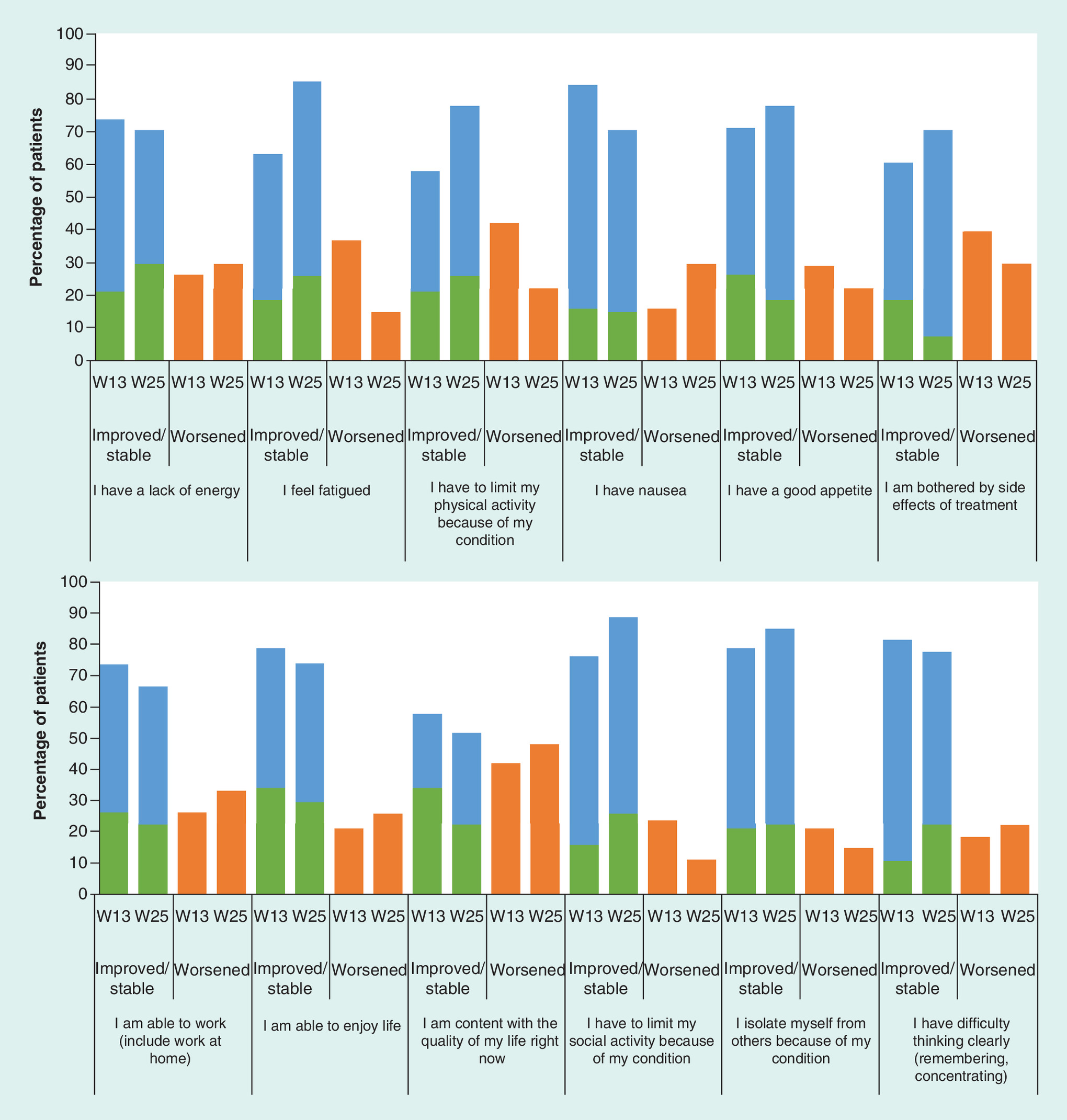
Figure 1. Change from baseline in chemotherapy-impacted concepts at week 13 (n = 38) and week 25 (n = 18).
Patients improved in green, stable in blue, worsened in orange.
Avelumab versus chemotherapy based on qualitative data
During the follow-up qualitative interviews, the nine interviewed patients did not report negative effects on their physical well-being or their daily activities while receiving avelumab, whereas at the study baseline interview they recalled chemotherapy having had negative effects on these. Among these nine patients, five patients reported some improvements and four reported no change on their physical functioning. “I have been able to go back to a lot of the stuff that I wasn't able to do before, once I had the chemo, I wasn't able to go to my exercise classes, now I'm slowly going back to all my classes” (patient 15). Still, fatigue forced some patients to rest more right after the infusion or after activities. “The only thing is, when I have the infusion, then there is something, it makes me really tired, and then I also fall asleep during the infusion, for around half an hour, three quarters of an hour, then I sleep” (patient 18).
Six patients out of nine interviewed at week 25 spontaneously compared their prior experience with chemotherapy to their current experience with avelumab. Overall, patients’ responses were very positive toward avelumab, reporting that they had fewer side effects with avelumab versus what they recalled from their experience with chemotherapy
“That was just, chemotherapy was nasty, I had, I had all sorts of, I mean fatigue and nausea and I lost all my hair and you know, I was just, and it was really, really hard on my body, and it was just very, because the drugs they gave me were really really strong, and it was just, it was nasty. So, but no, I mean with this drug [avelumab]…I don't have any, yeah, there's no side effects” (patient 4).
“[Avelumab] takes up a whole day, that's the only problem…Chemotherapy, I had to take that for three days in a row and I had to do it… what was it? Every three weeks? I can't remember now… anyway, I had to do a three day session each time, so… of course it didn't last as long each time getting the medication, but if I had to choose between the two routines, [avelumab] would be a much more preferable one” (patient 2).
In conclusion, interviewed patients at follow-up considered avelumab less burdensome than their previous chemotherapy.
Discussion
This novel project aimed to assess patients’ recollection of prior experience with chemotherapy, based on qualitative data (patient baseline interviews), with their current experience of avelumab based on quantitative data (FACT-M) and qualitative data (patient follow-up interviews).
To date, the quality of life of patients with mMCC receiving chemotherapy has not been documented in trials, preventing the possibility to perform a direct comparison to the quality of life data collected in patients with mMCC receiving avelumab. This innovative approach was proposed to address the limitations of comparing treatments in the context of a single arm study for a rare disease with high unmet medical need lacking a standard of care comparator.
In their recent draft guidance on patient-centered research, presented on 18 December 2017, FDA clearly encourages the development of mixed methods research. Capturing the patient perspective in rare disease trials of new drugs with unique mechanism of action and subsequently with limited knowledge regarding their impact on patient's survival, functioning and feelings, is a challenge. Our innovative approach involves mixed methods research embedded in the clinical trial. This mixed methods research provides an assessment of the importance of specific aspects of treatment benefits to the patients – concepts of interest – the expectations and priorities and the nature and meaning of the change over time experienced by patients. This approach seems promising, and its full potential will need to be highlighted in other studies.
In our sample, chemotherapy was associated with an unpleasant experience with numerous side effects which negatively affected their activities of daily living. Patients used strong words to describe chemotherapy: one patient compared it used ‘poison,’ another to ‘nasty stuff.’ On the selection of FACT-M items addressing concepts impacted by chemotherapy, the majority of patients were stable or improved, and few reported some worsening at both week 13 and week 25. These quantitative findings were supported by the few patients who spontaneously compared, during follow-up interviews, their experience with avelumab to prior chemotherapy; all described avelumab overall as less burdensome, essentially due to less perceived toxicities and subsequently less deterioration of their physical functioning. Some patients even reported improvements in their physical health. We acknowledge that the number of interviewed patients with experience of both chemotherapy and avelumab was small. The qualitative data reported by these nine patients, who were all responders, are to be used as supportive data to inform the meaningfulness of the quantitative findings.
The selection of the FACT-M data focuses on items which were reported to be impacted by chemotherapy. FACT-M was developed at the time conventional chemotherapy were cancer standard treatments. In this trial, avelumab was associated with few grade 1–2 side effects [9]: 24% of the patients reported fatigue, 17% infusion-related reaction, 9% diarrhea and 9% nausea. While both fatigue and nausea are captured in the FACT-M, adverse events such as infusion-related reaction and diarrhea were not. Consequently, we cannot recognize that such side effects may be worse for chemotherapy than for avelumab. However, by weeks 13 and 25, 60 and 70%, respectively, of the patients still in the study at these time points reported an improvement or no change from baseline on the item “I am bothered by side effects of treatment”, suggesting that avelumab side-effects are less bothersome than chemotherapy side-effects.
This comparative effectiveness analysis attempted to explore aspects of ‘treatment experience’ while patients were on avelumab treatment and the patient's own comparison to prior treatment. The sample used in the analysis may have a selection bias against chemotherapy (i.e., all patients had disease progression after chemotherapy as per eligibility criteria), however, chemotherapy has not been shown to be an effective therapy with short tumor response duration and most patients will experience disease progression.
A limitation is the heterogeneity in this small study population; while enrolled patients shared the experience of prior chemotherapy, the number, the type and duration of previous chemotherapies varied. Another source of variability was the time since patients completed their prior chemotherapy; this ranged widely in number of months, which may have had an effect on patient recall when describing their experience with chemotherapy. During baseline interviews a few patients still described some degree of side effects they interpreted as due to chemotherapy, although screening assessments by physicians confirmed recovery of chemotherapy related adverse events (excluding hair loss).
A second limitation is the lack of comparability in the data collection methods. The baseline interviews were not designed to comprehensively collect patient experience with their chemotherapy to then map it to the FACT-M items and scoring. For example, the fatigue reported by patients was not quantified during the interview for chemotherapy the way it is quantified with the FACT-M. There was also no experience in reporting FACT-M data for a population of patients with mMCC or MCC treated with chemotherapy that could be used for comparison.
Another limitation was the small sample size which may limit the representativeness of the data to the general population of patients with mMCC. Not all 88 patients treated with avelumab in the study consented to be interviewed, and as such there is a potential self-selection bias of patients willing to discuss their personal experience more than other patients.
Conclusion
Data from this mixed methods research study suggest that most patients with mMCC reported no deterioration or improvements on their experience of treatment side effects and impact on their activities of daily living over the course of the trial when receiving avelumab, in contrast to what they recalled from their prior experience with chemotherapy.
Using an innovative mixed methods research approach, merging qualitative data and quantitative data may be appropriate in demonstrating patient reported treatment benefit by addressing challenges of a single arm study lacking an effective comparator treatment for diseases with high unmet medical need. While we believe this pilot study provides a powerful approach of benefit risk in line with patient-centred clinical research, we acknowledge the limitations related to the size of our sample which hinders generalization. Further study from another cohort of patients with mMCC treated with avelumab may substantiate this methodology attempted to describe the patient perceptions of the treatment experience for a rare disease of high unmet medical need.
Future perspective
No-one other than the patients themselves can report the true benefit of a treatment on both the disease and their lives. Patients’ involvement and input in clinical development and in drug approval is gaining importance and will keep doing so in the future years. With innovative clinical development pathways on the rise, creative methods to ascertain patient insights will increase.
Patients with metastatic Merkel cell carcinoma reported a better experience with avelumab, an immunotherapy agent recently approved for the treatment of Merkel cell carcinoma, than they did with chemotherapy.
Among patients with Functional Assessment of Cancer Therapy subscale for melanoma data at weeks 13 and 25 (67 and 60% of study patients, respectively), most patients were stable or improved on the Functional Assessment of Cancer Therapy subscale for melanoma items matching concepts that patients had qualitatively reported to be worsened with chemotherapy.
We describe an alternative innovative approach merging qualitative and quantitative data that could help address challenges linked to demonstrate treatment benefit in the absence of comparator arms in rare disease clinical trial.
Acknowledgements
The authors would like to thank all participants, patients and investigator sites, for their contribution in this project. The authors would also like to thank G Thomson (Mapi) for her medical writing assistance and editorial support in manuscript preparation and M Henry-Szatkowski (Mapi) for his contribution in the statistical analysis.
Author contributions
All authors meet all authorship criteria.
Financial & competing interests disclosure
This study was funded by and is part of an alliance between Merck KGaA and Pfizer, Inc, NY, USA. M Bharmal is an employee of Merck KGaA, Darmstadt, Germany; M Hennessy is an employee of EMD Serono, US; A Marrel, B Arnould, F Fofana and J Lambert are paid consultants to Merck KGaA, Darmstadt, Germany.
G Thomson (Mapi) provided medical writing assistance and editorial support in manuscript preparation and M Henry-Szatkowski (Mapi) contributed to the statistical analysis.
Ethical conduct of research
The clinical trial protocol, including description of the qualitative interviews, was approved by all relevant independent ethics committees and institutional review boards at each site and was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice. A written informed consent was obtained from all the patients who agreed to be interviewed.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Lebbe C, Becker JC, Grob JJ et al. Diagnosis and treatment of Merkel Cell Carcinoma. European consensus-based interdisciplinary guideline. Eur. J. Cancer 51(16), 2396–2403 (2015).
2.
Paulson KG, Park SY, Vandeven NA et al. Merkel cell carcinoma: Current US incidence and projected increases based on changing demographics. J. Am. Acad. Dermatol. 78(3), 457.e2–463.e2 (2017).
3.
Allen PJ, Bowne WB, Jaques DP, Brennan MF, Busam K, Coit DG. Merkel cell carcinoma: prognosis and treatment of patients from a single institution. J. Clin. Oncol. 23(10), 2300–2309 (2005).
4.
Tai PT, Yu E, Winquist E et al. Chemotherapy in neuroendocrine/Merkel cell carcinoma of the skin: case series and review of 204 cases. J. Clin. Oncol. 18(12), 2493–2499 (2000).
5.
Santamaria-Barria JA, Boland GM, Yeap BY, Nardi V, Dias-Santagata D, Cusack JC Jr. Merkel cell carcinoma: 30-year experience from a single institution. Ann. Surg. Oncol. 20(4), 1365–1373 (2013).
6.
Voog E, Biron P, Martin JP, Blay JY. Chemotherapy for patients with locally advanced or metastatic Merkel cell carcinoma. Cancer 85(12), 2589–2595 (1999).
7.
Becker JC, Lorenz E, Ugurel S et al. Evaluation of real-world treatment outcomes in patients with distant metastatic Merkel cell carcinoma following second-line chemotherapy in Europe. Oncotarget 8(45), 79731–79741 (2017).
•• Article supporting the limited efficacy of chemotherapy in Merkel cell carcinoma (MMC) patients.
8.
Cowey CL, Mahnke L, Espirito J, Helwig C, Oksen D, Bharmal M. Real-world treatment outcomes in patients with metastatic Merkel cell carcinoma treated with chemotherapy in the USA. Future Oncol. 13(19), 1699–1710 (2017).
•• Article supporting the limited efficacy of chemotherapy in MMC patients.
9.
Kaufman HL, Russell J, Hamid O et al. Avelumab in patients with chemotherapy-refractory metastatic Merkel cell carcinoma: a multicentre, single-group, open-label, Phase 2 trial. Lancet Oncol. 17(10), 1374–1385 (2016).
• The article is presenting the efficacy and safety results from the trial.
10.
Kaufman HL, Russell JS, Hamid O et al. Durable responses to avelumab (anti-PD-L1) in patients with Merkel cell carcinoma progressed after chemotherapy: 1-year efficacy update. Presented at: 2017 AACR Annual Meeting. WAUSA, 1–5 April 2017.
11.
U.S. Department of Health and Human Services. Guidance for Industry Patient Reported Outcome Measures: Use in Medicinal Product Development to Support Labelling Claims (2009).
12.
Scott NW, Fayers PM, Aaronson NK et al. EORTC QLQ-C30. EORTC, Belgium (2008). http://groups.eortc.be/qol/eortc-qlq-c30.
13.
Dueck AC, Mendoza TR, Mitchell SA et al. Validity and reliability of the US National Cancer Institute's Patient-Reported Outcomes Version of the Common Terminology Criteria for Adverse Events (PRO-CTCAE). JAMA Oncol. 1(8), 1051–1059 (2015).
14.
Cleeland CS. The M.D. Anderson Symptom Inventory. The University of Texas Anderson Cancer Center, TX, USA (2016).
15.
Cormier JN, Davidson L, Xing Y, Webster K, Cella D. Measuring quality of life in patients with melanoma: development of the FACT-melanoma subscale. J. Support. Oncol. 3(2), 139–145 (2005).
16.
Bharmal M, Fofana F, Barbosa CD et al. Psychometric properties of the FACT-M questionnaire in patients with Merkel cell carcinoma. Health Qual. Life Outcomes 15(1), 247 (2017).
• Presents the psychometric validation of the Functional Assessment of Cancer Therapy - Melanoma questionnaire in MMC population.
17.
Kaufman HL, Hunger M, Hennessy M, Schlichting M, Bharmal M. Nonprogression with avelumab treatment associated with gains in quality of life in metastatic Merkel cell carcinoma. Future Oncol. 14(3), 255–266 (2018).
18.
Curry L, Nunez-Smith M. Mixed Methods in Health Sciences Research: A Practical Primer. SAGE Publications (2014).
19.
Cormier JN, Ross MI, Gershenwald JE et al. Prospective assessment of the reliability, validity, and sensitivity to change of the functional assessment of cancer Therapy-Melanoma questionnaire. Cancer 112(10), 2249–2257 (2008).
20.
Friese S, Ringmayr TG. ATLAS.ti. 7 User Manual. Berlin: ATLAS.ti Scientific Software Development GmbH (2013). https://atlasti.com/wp-content/uploads/2014/05/atlasti_v7_manual_201312.pdf?q=/uploads/media/atlasti_v7_manual_201312.pdf.
Information & Authors
Information
Published In
Copyright
© 2018 Merck KGaA, Darmstadt, Germany.
History
Received: 25 May 2018
Accepted: 27 July 2018
Published online: 15 August 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparative effectiveness of avelumab versus chemotherapy in Merkel cell carcinoma: innovative use of patient insights. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0048
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Catherine S. Valukas, Sunandana Chandra, Jaehyuk Choi, Jeffrey D. Wayne, Contemporary Management of Merkel Cell Carcinoma, Hematology/Oncology Clinics of North America, 10.1016/j.hoc.2025.07.009, 40, 1, (101-115), (2026).
- Michael Soileau, Rajeev Kumar, Ashwini Parab, Triza Brion, Kailee White, Connie H. Yan, Megha B. Shah, Pavnit Kukreja, Maurizio F. Facheris, Anand Shewale, Jason Aldred, Patients’ experience with and perspectives on long-term use of continuous subcutaneous infusion of foslevodopa/foscarbidopa in Parkinson’s disease, Journal of Neurology, 10.1007/s00415-025-13123-y, 272, 6, (2025).
- Raphael Yip, Gaston Arnolda, Klay Lamprell, Bróna Nic Giolla Easpaig, Renuka Chittajallu, Geoff Delaney, Ian Olver, Winston Liauw, Jeffrey Braithwaite, Experience of patients considering or using checkpoint inhibitors in cancer treatment: a systematic review of qualitative research, Journal for ImmunoTherapy of Cancer, 10.1136/jitc-2023-007555, 12, 1, (e007555), (2024).
- Catherine S. Valukas, Sunandana Chandra, Jaehyuk Choi, Jeffrey D. Wayne, Contemporary Management of Merkel Cell Carcinoma, Advances in Oncology, 10.1016/j.yao.2023.01.003, 3, 1, (37-46), (2023).
- Matteo Scampa, Rastine Merat, Evangelia Tzika, Daniel F. Kalbermatten, Carlo M. Oranges, Survival outcomes and epidemiology of Merkel cell carcinoma of the lower limb and hip: A Surveillance, Epidemiology, and End Results analysis 2000-2018, JAAD International, 10.1016/j.jdin.2021.12.010, 7, (13-21), (2022).
- Jérémy Lambert, Alexia Marrel, Sandra P. D’Angelo, Melissa A. Burgess, Bartosz Chmielowski, Nicola Fazio, Thilo Gambichler, Jean-Jacques Grob, Céleste Lebbé, Caroline Robert, Jeffrey Russell, Gülseren Güzel, Murtuza Bharmal, Patient Experiences with Avelumab in Treatment-Naïve Metastatic Merkel Cell Carcinoma: Longitudinal Qualitative Interview Findings from JAVELIN Merkel 200, a Registrational Clinical Trial, The Patient - Patient-Centered Outcomes Research, 10.1007/s40271-020-00428-5, 13, 4, (457-467), (2020).
- Giancarlo A. Garcia, Andrea L. Kossler, Avelumab as an Emerging Therapy for Eyelid and Periocular Merkel Cell Carcinoma, International Ophthalmology Clinics, 10.1097/IIO.0000000000000306, 60, 2, (91-102), (2020).
- Cecilia Vellani, Daniela D’Ambrosio, Luca Licata, Ilaria Vacchieri, Antonio Bernardo, Giuseppe Trifirò, Monitoring response of advanced Merkel cell carcinoma to Avelumab with 18F-FDG PET/CT, European Journal of Nuclear Medicine and Molecular Imaging, 10.1007/s00259-018-4230-x, 46, 5, (1197-1198), (2018).