Meropenem/colistin versus meropenem/ampicillin–sulbactam in the treatment of carbapenem-resistant pneumonia
Abstract
Aim: Efficacy of colistin and ampicillin–sulbactam have not been compared in treatment of ventilator-associated pneumonia due to A. baumannii. Efficacy of colistin and ampicillin–sulbactam in combination with meropenem were compared in treatment of ventilator-associated pneumonia due to carbapenem-resistant A. baumannii. Method: 47 patients with ventilator-associated pneumonia due to carbapenem-resistant A. baumannii were randomized to receive meropenem/colistin or meropenem/ampicillin–sulbactam for 14 days. Clinical and microbiological responses and 28-day mortality were considered as outcomes. Results: Clinical response (75 vs 69.6%; p = 0.75) and microbial eradication (87.50 vs 91.3%; p = 0.59) were comparable between meropenem/colistin and meropenem/ampicillin–sulbactam groups, respectively. Conclusion: In this study, clinical and microbiological response were comparable between the meropenem/colistin and meropenem/ampicillin–sulbactam groups.
Lower respiratory tract infection is among the leading causes of mortality among infectious diseases. Unfortunately, its incidence has been increasing significantly since 1984 [1,2]. Ventilator-associated pneumonia (VAP) is one of the lower respiratory tract infections that is associated with prolonged mechanical ventilation, hospitalization, increased mortality and cost [3]. Each VAP episode leads to an increase in additional hospital costs by more than USD$10,000 [2,4]. Based on Magill's study, more than 39% of healthcare-associated pneumonias are VAPs [5]. At least 50% of these cases emerge as a result of antibiotic-resistant isolates [6]. Incidence of VAP caused by multidrug-resistant (MDR) A. baumannii was reported to be between 1.9 and 18.3% per 1000 ventilator days. Considering geographical area, population, assessment tools, diagnostic criteria and history of previous antibiotic exposure are factors that influenced the incidence of VAP. The incidence of VAP was reported in 20–30% of critically ill Iranian patients [7,8].
Acinetobacter species are aerobic Gram-negative coccobacilli and one of the common causes of VAP (17%) [9]. According the National Health Safety Network report, Acinetobacter species are considered as the fifth pathogen known in creating VAP [10]. Based on the recent Centers for Disease Control and Prevention report, 2% of all healthcare-associated infections were related to the Acinetobacter spp [11].
Significant changes in the antimicrobial susceptibility pattern of these isolates have been detected during the last four decades. Acinetobacter isolates were described for first time in 1911. Antimicrobial resistance rate of these isolates are increasing [12]. At present, Acinetobacter spp. are resistant to the most broad spectrum of antibacterial agents, even carbapenems [13]. The resistance rate to carbapenems increased from 9% in 1995 to 40% in 2004, and MDR isolates have been rapidly spreading in recent decades [9,14]. Approximately 63% of the Acinetobacter isolates are MDR pathogens [11].
Treatment of VAP due to resistant Acinetobacter species is a challenging issue as limited therapeutic options are available. Carbapenems, sulbactam, polymixins, aminoglycosides, tetracyclines and tigecycline were examined in some previous studies [9,15–17].
Following the introduction of new antibiotics and safety concerns, especially nephrotoxicity and neurotoxicity, systemic administration of polymixins was restricted for more than 60 years. However, colistin, as a member of polymixins group, is the only available option for the treatment of carbapenem-resistant A. baumannii [17].
Sulbactam is an irreversible inhibitor of β-lactamase, which has an intrinsic activity against A. baumannii. Sulbactam efficacy for the treatment of VAP was investigated in some studies [17–20].
The synergistic effects of carbapenems with other effective antibiotics have been reported in some studies for the treatment of carbapenem-resistanct A. baumannii infections [21]. The efficacy of colistin and ampicillin–sulbactam has not been compared in a head-to-head analysis in the treatment of VAP caused by A. baumannii. Therefore, the purpose of this study was to compare efficacy of colistin and ampicillin–sulbactam, in combination with meropenem in the treatment of VAP caused by carbapenem-resistant A. baumannii among critically ill patients.
Methods
Design
This open-label, randomized, clinical trial was conducted from October 2015 to October 2017 on critically patients admitted to the general intensive care unit (ICU) of Imam Khomeini hospital complex, Tehran, Iran. This study was registered in the Iranian Registry of Clinical Trials; a primary registry in the WHO registry network (registered code number: IRCT201509213449N19).
Ethical committee of Tehran University of Medical Sciences approved the study protocol (ethical code number: IR.TUMS.REC.1394.867).
Change in procalcitonin level following VAP treatment was considered for sample size calculation. Including α = 0.05 and β = 0.80, 23 patients were recruited in each group.
Study variables
Adult patients (18–75 years old) diagnosed with VAP (pneumonic following at least 48 h of mechanical ventilation) were screened. Clinical status, laboratory parameters and radiographic results were used for the diagnosis of pneumonia. The presence of at least two of the following parameters was main criteria: fever (T >38°C) or hypothermia (T <35.5°C), leukocytosis (WBC >12000 cells/ml) or leukopenia (WBC <4000 cells/ml) and positive tracheal culture or new or progressive infiltration in chest x-ray [22].
Patients with a history of hypersensitivity reactions to ampicillin–sulbactam, colistin, meropenem and tracheal aspiration isolates other than A. baumannii were excluded from the study.
Microbiology laboratory procedure
Endotracheal aspirates were collected in aseptic conditions from the patients with suspected VAP for further microbiological evaluation based on the recommendations by the Clinical and Laboratory Standard Institute [23].
Antimicrobial disks, such as ampicillin/sulbactam (10/10 μg), piperacillin/tazobactam (100/10 μg), ceftriaxone (30 μg), meropenem (10 μg), gentamicin (10 μg), ciprofloxacin (5 μg) and trimethoprim-sulfamethoxazole (1.25/23.75 μg) were tested against A. baumannii isolates. Zone diameters that were considered to be resistant are: ≤11 mm for ampicillin sulbactam, ≤17 mm for piperacillin tazobactam, ≤8 mm for ceftriaxone, ≤14 mm for meropenem, ≤12 mm for gentamicin, ≤15 mm for ciprofloxacin and ≤10 mm for trimethoprim sulfamethoxazole [23].
Meropenem and colistin Minimum Inhibitory Concentration (MICs) were determined using the E-test method for A. baumannii isolates. E-test strips were obtained from the Liofilchem Company, Roseto Dgli Abruzzi, Italy. MIC ≥ 8 μg/dl and MIC ≥ 2 μg/dl were considered as the breakpoints, based on Clinical and Laboratory Standard Institute and European Committee on Antimicrobial Susceptibility Testing for meropenem and colistin resistance, respectively [23,24].
Therapeutic regimens
Using the simple randomization method via random number generator, 47 patients with VAP caused by carbapenem-resistant A. baumannii were assigned to receive either meropenem/colistin or meropenem/ampicillin–sulbactam. ampicillin–sulbactam and colistin were administered with a daily dose of 12/6 g (divided in 6 equal doses during a 1-h intravenous [iv.] infusion) and 9 million international units as loading dose and then daily (divided in 2 equal doses, during 1-h iv. infusion) respectively [25,26]. Both the groups also received meropenem 2 g three-times a day and each dose was administered during 4 h iv. infusion [27]. Doses of the antibiotics were adjusted according to the patients’ renal function.
Demographic data
Demographic (sex, age and weight) and primary characteristics (baseline diseases, cause of hospital and ICU admission, history of antibiotic use and concomitant medications) were collected from each patient's medical chart. Clinical status, oxygenation and hemodynamic parameters of the patients were assessed daily during the 14 days of antibiotic therapy. To assess the response to these treatment regimens, clinical data, such as sequential organ failure assessment (SOFA) and Clinical pulmonary infection score, laboratory variables such as complete blood count, erythrocyte sedimentation rate, C-reactive protein, and serum procalcitonin and microbiological findings were used.
The culture of endotracheal samples for each patient were repeated at days 7 and 14. Follow-up of the patients was carried out for 28 days. Clinical and microbiological responses were considered as the primary outcome. Clinical response at the end of treatment course was classified either as a success or a failure. Complete resolution of the signs of VAP was defined as clinical success. The patient was categorized as a partial responder when at least two signs of VAP were resolved. Persistence or worsening of VAP signs was considered as clinical failure [28]. Microbiological response was categorized as eradication or persistent. Absence or presence of the pretreatment pathogen 1 or 2 weeks after VAP treatment was defined as eradication and persistence, respectively [16].
Incidence of acute kidney injury (AKI) was detected based on the KDIGO definition [29]. An increase of ≥0.3 mg/dl in serum creatinine within 48 h of therapy or 1.5-times increase in the baseline within 7 days or urine volume of less than 0.5 ml/kg/h for 6 h were all considered as AKI definitions.
The duration of hospitalization in the ICU and 28-day mortality were defined as the secondary outcomes of this study.
Statistical analysis
Statistical Package for Social Sciences (SPSS) 21.0 program was used for data analysis. Continuous and categorical variables were reported as mean ± standard deviation and numbers or percentages, respectively. The Mann–Whitney rank sum test was performed to compare the continuous data between the groups. Fisher's Chi-square tests were used for the assessment of clinical and microbiological responses. The time between treatment initiation to death or ICU discharge was defined as the survival time. Survival analysis was performed for the regimens with the help of the Kaplan–Meier test. A p-value of less than 0.05 was considered to be statistically significant.
Results
Out of the 891 patients who were admitted to the ICU, 125 (14.03%) developed VAP. Among them, 78 (62.4%) patients were not eligible for further evaluation. The consort flow diagram of the study has been depicted in Figure 1. Endotracheal aspirate samples were negative (culture-negative VAP) and positive (culture-positive VAP) in 38/125 (30.4%) and 87/125 (69.6%) of the patients, respectively. A. baumannii (47/125), Klebsiella spp. (22/125), P. aueroginosa (10/125), Enterobacter spp. (2/125), E. coli (2/125), Staphylococcus. aureus (2/125), Staphylococcus. epidermidis (1/125) and Streptococcus spp. (1/125) were the isolated pathogens in the culture-positive patients. All A. baumannii isolates were resistant to third-generation cephalosporins, fluoroqinolones, aminoglycosides, piperacillin-tazobactam and meropenem. According to the antibiotic susceptibility tests, all were carbapenem-resistant isolates. Resistance of the isolates toward meropenem was confirmed through the MIC test. All the isolates had meropenem MIC values ≥32 μg/ml. Colistin MIC values of A. baumannii isolates were between 0.25 and 2 μg/ml.

Figure 1. The CONSORT flow diagram of the study.
MIU: Million international units; TDS: Ter die sumendim (three times daily).
Demographic, laboratory and clinical characteristics of the patients have been shown in Table 1. Considering these variables, there was no significant difference between the groups. Also, baseline diseases and concomitant medications were similar between the groups (Table 2). Only baseline cardiovascular diseases were more common in meropenem/colistin as compared with the meropenem/ampicillin–sulbactam groups (p = 0.008). Based on regression analysis, cardiovascular diseases had no effect on primary and secondary outcome.
| Parameter | Meropenem/colistin group (n = 24) | Meropenem/ampicillin–sulbactam group (n = 23) | p-value |
|---|---|---|---|
| Age (mean ± SD) | 60.63 ± 12/97 | 56.26 ± 11/50 | 0.44 |
| Gender Male (%) Female (%) | 16/24 (66.7%) 8/24 (33.3%) | 19/23 (82.6%) 4/23 (17.4%) | 0.32 |
| Weight (kg) | 70.63 ± 9.24 | 70.87 ± 10.19 | 0.93 |
| Recent surgery (during past 30 days) | 6/24 (25%) | 7/23 (30.4%) | 0.75 |
| Previous antibiotic therapy (during past 30 days) | 22/24 (91.7%) | 20/23 (87%) | 0.67 |
| Charlson comorbidity score (median/range) | 4 (0–9) | 3 (0–10) | 0.52 |
| Duration of hospital stay before ICU admission (median/range) | 5.5 (0–45) | 5 (0–60) | 0.71 |
| Duration of ICU stay before VAP diagnosis (median/range) | 10 (2–51) | 8 (2–27) | 0.067 |
| SOFA score (median/range) | 5.5 (0–12) | 6.5 (0–19) | 0.21 |
| Predicted mortality rate (%) (based on SOFA score) | 39.13 ± 13.81 | 48.14 ± 23.68 | 0.19 |
| CPIS score (median/range) | 8.5 (6–11) | 8 (5–11) | 0.61 |
| Procalcitonin (median/range) | 1.22 (0.08–44.74) | 0.75 (0.14–90.76) | 0.66 |
| CRP [mg/l] (mean ± SD) | 72.39 ± 38.04 | 90.52 ± 43.97 | 0.16 |
| ESR [mm/h] (mean ± SD) | 67 ± 34.52 | 54.95 ± 35.43 | 0.27 |
| WBC (mean ± SD) | 15.76 ± 5.63 | 15.34 ± 10.58 | 0.87 |
| HR [bpm] (median/range) | 97 (69–148) | 103 (57–135) | 0.74 |
| RR [bpm] (median/range) | 22 (12–30) | 22 (11–42) | 0.10 |
| MAP [mmHg] (mean ± SD) | 87.75 ± 15.96 | 95 ± 20.3 | 0.18 |
| Temperature [°C] (mean ± SD) | 38.04 ± 1.17 | 37.65 ± 0.79 | 0.058 |
CPIS: Clinical pulmonary infection assessment; CRP: C-reactive protein; ESR: Erythrocyte sedimentation rate; ICU: Intensive care unit; MAP: Mean arterial pressure; RR: Respiratory rate; SD: Standard deviation; SOFA: Sequential organ failure assessment; VAP: Ventilator-associated pneumonia; WBC: White blood cells.
| Parameter | Meropenem/colistin group (n = 24) | Meropenem/ampicillin–sulbactam group (n = 23) | p-value |
|---|---|---|---|
| Baseline diseases | |||
| Cardiovascular diseases | 15/24 (62.5%) | 5/23 (21.7%) | 0.008 |
| Respiratory diseases | 6/24 (25%) | 2/23 (8.7%) | 0.24 |
| CVA | 4/24 (16.7%) | 2/23 (8.7%) | 0.67 |
| Neurological diseases | 3/24 (12.5%) | 2/23 (8.7%) | > 0.99 |
| Solid tumors | 2/24 (8.3%) | 6/23 (26.1%) | 0.14 |
| Genetic disorders | 2/24 (8.3%) | 1/23 (4.3%) | > 0.99 |
| IV drug user | 2/24 (8.3%) | 1/23 (4.3%) | > 0.99 |
| Thyroid disorders | 1/24 (4.2%) | – | > 0.99 |
| Diabetes mellitus | 9/24 (37.5%) | 4/23 (17.4%) | 0.19 |
| Rheumatologic disorders | – | 1/23 (4.3%) | 0.49 |
| Hematologic disorders | 1/24 (4.2%) | 1/23 (4.3%) | > 0.99 |
| Genitourinary problems | 2/24 (8.3%) | – | 0.49 |
| CKD | 1/24 (4.2%) | 1/23 (4.3%) | > 0.99 |
| Gasterointestinal diseases | – | 1/23 (4.3%) | 0.49 |
| Psychiatric problems | 1/24 (4.2%) | – | > 0.99 |
| Concurrent medications | |||
| Vancomycin | 10/24 (41.7%) | 7/23 (30.4%) | 0.55 |
| Caspofungin | 3/24 (12.5%) | 3/23 (13%) | >0.99 |
| Linezolide | 1/24 (4.2%) | – | >0.99 |
| Vasopressor | 11/24 (45.8%) | 9/23 (39.1%) | 0.77 |
| NAC | 2/24 (8.3%) | 2/23 (8.7%) | >0.99 |
| Atorvastatin | 8/24 (33.3%) | 5/23 (21.7%) | 0.52 |
| Corticosteroid | 5/24 (20.8%) | 3/23 (13%) | 0.7 |
| Immunosuppresants | 1/24 (4.2%) | – | >0.99 |
CKD: Chronic kidney disease; CVA: Cerebrovascular accident; IV: Intravenous; NAC: N-acetyl-L-cysteine.
All the recruited patients had at least one risk factor for developing MDR VAP. Prior antibiotic use (89.36%) and at least 5 days of hospitalization before VAP (95.74%) were identified as risk factors.
Clinical pulmonary infection score and procalcitonin decreased significantly within both the groups at the end of treatment course as compared with the baseline values. However, the change was not very different intergroup. Although SOFA score decreased in both the groups, but the changes were not significant for both intergroup and intragroup. Serum C-reactive protein and erythrocyte sedimentation rate decreased significantly within the meropenem/ampicillin–sulbactam (p = 0.04) and meropenem/colistin groups (0.01), respectively. However, the intergroup changes were comparable (Table 3).
| Parameter | Baseline vs week 4 | |
|---|---|---|
| SOFA score Mean (95% CI) difference value within meropenem/colistin group [p-value] Mean (95% CI) difference value within meropenem/ampicillin–sulbactam group [p-value] Mean (95% CI) difference value between meropenem/colistin and Meropenem/ampicillin–sulbactam groups [p-value] | 0.15 (-0.18 to 1.11) [0.74] 0.83 (-1.31 to 2.98) [0.41] 1.51 (-4.15 to 1.12) [0.24] | |
| CPIS Mean (95% CI) difference value within meropenem/colistin group [p-value] Mean (95% CI) difference value within meropenem/ampicillin–sulbactam group [p-value] Mean (95% CI) difference value between meropenem/colistin and meropenem/ampicillin–sulbactam groups [p-value] | 3.76 (3.07 to 4.45) [<0.001] 3.68 (2.59 to 4.78) [<0.001] 0.26 (-0.72 to 1.25) [0.59] | |
| Procalcitonin Mean (95% CI) difference value within meropenem/colistin group [p-value] Mean (95% CI) difference value within meropenem/ampicillin–sulbactam group [p-value] Mean (95% CI) difference value between meropenem/colistin and meropenem/ampicillin–sulbactam groups [p-value] | 3.72 (-5.06 to 12.46) [0.008] 7.29 (-4.27 to 18.86) [0.03] -1.55 (-11.35 to 8.23) [0.74] | |
| ESR Mean (95% CI) difference value within meropenem/colistin group [p-value] Mean (95% CI) difference value within meropenem/ampicillin–sulbactam group [p-value] Mean (95% CI) difference value between meropenem/colistin and meropenem/ampicillin–sulbactam groups [p-value] | 23.13 (5.20 to 41.07) [0.01] 3.80 (-9.84 to 17.44) [0.56] 7.42 (-13.33 to 27.81) [0.47] | |
| CRP Mean (95% CI) difference value within meropenem/colistin group [p-value] Mean (95% CI) difference value within meropenem/ampicillin–sulbactam group [p-value] Mean (95% CI) difference value between meropenem/colistin and meropenem/ampicillin–sulbactam groups [p-value] | 2.21 (-21.99 to 26.43) [0.85] 33.20 (2.13 to 64.27) [0.04] -4.55 (-22.52 to 13.41) [0.61] |
CI: Confidence interval; CPIS: Clinical pulmonary infection score; CRP: C-reactive protein; ESR: Erythrocyte sedimentation rate; SOFA: Sequential organ failure assessment.
During the study period, AKI occurred in three and one patients in the meropenem/colistin and meropenem/ampicillin–sulbactam groups, respectively (p = 0.11).
Clinical improvement of pneumonia was achieved in 18/24 (75%) and 16/23 (69.6%) of patients in the meropenem/colistin and meropenem/ampicillin–sulbactam group, respectively (p = 0.75) (Table 4). During the antibiotic treatment course, cultures of endotracheal samples became negative in 5/24 (87.50%) and 5/23 (91.30%) of patients in the meropenem/colistin and meropenem/ampicillin–sulbactam groups, respectively (p = 0.59).
| Type of regimen | Clinical response | 28-day mortality | ||||
|---|---|---|---|---|---|---|
| Improvement | Failure | p-value | Yes | No | p-value | |
| Meropenem/colistin (n = 24) | 18/24 (75%) | 6/24 (25%) | 0.75 | 10/24 (41.67%) | 14/24 (58.33%) | 0.99 |
| Meropenem/ampicillin–sulbactam (n = 23) | 16/23 (69.6%) | 7/23 (30.4%) | 9/23 (39.13%) | 14/23 (60.87%) | ||
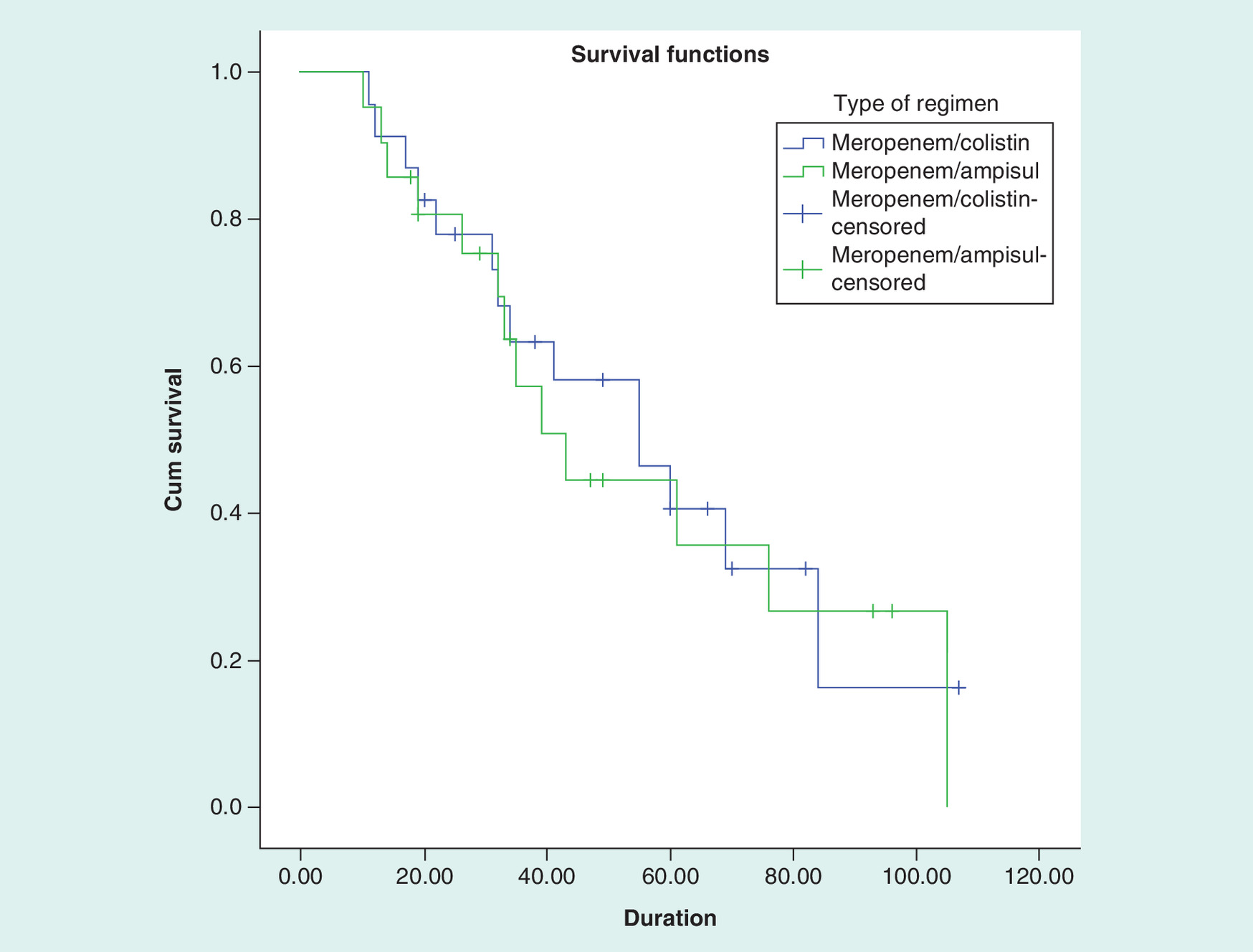
The 28-day mortality (Table 5) was not different between the meropenem/colistin and meropenem/ampicillin–sulbactam groups (10/24 [41.67%] and 9/23 [39.13%], p >0.99). No significant difference in mortality was found between the groups in the survival analysis (p = 0.78) during hospitalization at the ICU (Figure 2).
Discussion
In this pilot, randomized, clinical trial, the meropenem/colistin and meropenem/ampicillin–sulbactam groups showed similar efficacy and renal safety in critically ill patients with VAP caused by carbapenem-resistant A. baumannii. Clinical and microbiological responses, episodes of AKI, duration of ICU hospitalization and 28-day mortality were comparable among the groups.
Based on a large multicenter study in VAP patients, Klebsiella species was the most common isolate, followed by P. aeroginosa or A. baumannii pathogens [30,31]. During the years 2003–2008, the incidence rate of carbapenem-resistant A. baumannii increased 57% in the USA hospitals. ampicillin–sulbactam also showed same change in its antimicrobial susceptibility pattern [32]. In Iran, more than 70% of A. baumannii isolates were carbapenem-resistant [33]. In this study, all of the A. baumannii isolates were resistant to carbapenem. In a recent paper with published data from 348 hospitals of diverse geographical areas in USA, the prevalence of MDR A. bauamnnii isolates was reported as 36.3%. Most of the MDR A. baumannii was detected in midwest (44.4%), followed by west (42.5%), northeast (40.5%) and south (29.5%) [34]. The prevalence of colistin-resistant A. baumannii was reported as ranging from 0 to 40.6% over the world. The highest values were attributed to Asian and European countries [35–37]. According to the results of the E-test method in this study, the rate of colistin resistance in A. baumannii isolates was about 2%.
There are limited therapeutic options for the treatment of VAP caused by carbapenem-resistant A. baumannii. Although carbapenem-resistant isolates are increasing, however carbapenem-heteroresistant should be considered. Heteroresistant isolates are genetically homogenous microorganisms but have different antimicrobial susceptibility pattern. Synergistic effects of a carbapenem with other antimicrobial agents are proposed for carbapenem-resistant isolates [38–40].
In a prospective cohort study in Greece, the efficacy and safety of sulbactam and colistin as monotherapy were found to be comparable for the treatment of MDR A. baumannii-associated VAP in a population of debilitated patients. The clinical response rate of sulbactam and colistin was similar in our study with others [41].
Colistin caused renal injury was detected in 0–57% of the recipients [42]. Patient features, such as age, obesity, comorbidities, concomitant nephrotoxic medications, serum concentration and dose of colistin, were defined as important risk factors for the development of colistin-induced nephrotoxicity [43]. In this study, all the patients with AKI during the colistin therapy were old-age individuals and received vancomycin concomitantly with colistin.
Unfortunately, colistin-resistant Gram-negative pathogens have emerged following the overuse of this antibiotic during the recent years. The increasing resistance to colistin is a serious threat around the word. In an era of colistin resistance, inhaled antibiotics may be the last viable option for the treatment of severe pneumonia. The efficacy of different antimicrobial agents, such as colistin and aminoglycosides, as inhalation therapy was assessed for the treatment of VAP. Combination regimens consisting of a systemic or nebulized aminoglycosides were reviewed. Nebulized aminoglycoside is recommended due to its better penetration and lesser toxicity [44].
Increased rate of treatment failure and mortality due to MDR infections is a global issue. The estimation of the directly attributed mortality of these infections is difficult. Patient comorbidities (malignancies, renal and liver disorders, genetic and neurological problems), delay in start of effective antibiotic regimens, inappropriate selection of antimicrobial regimens, septic shock, resistant pathogens, concurrent infections, previous antibiotic and corticosteroid therapies, high APACHEII and SOFA scores were significant risk factors of mortality in patients with MDR A. baumannii-associated VAP [7,45–47].
In this study, the 28-day all-cause mortality was similar to previous studies. Global mortality related to VAP was reported in the range of 20–50% of critically ill patients. However, in a large meta-analysis, the direct attributable mortality of VAP was reported as 13% [48].
The mortality rates of MDR A. baumannii-associated pneumonia were estimated as 7.8–23 and 10–43% in patients who were hospitalized in the wards and the ICU, respectively [18,48].
The efficacy and the safety of colistin and high-dose ampicillin/sulbactam were comparable in the treatment of VAP caused by MDR A. baumannii in critically ill patients [41]. However, in a retrospective comparison study, higher microbiological failure and mortality were detected in the colistin group in comparison with the ampicillin–sulbactam group [49].
Ampicillin–sulbactam may be as a suitable alternative for colistin in the treatment of VAP caused by carbapenem-resistant A. baumannii in critically ill patients. However, the limitations of this study should also be considered. This was a pilot, single-center, randomized, clinical trial without a considerable sample size. Sulbactam is not commercially available in Iran and, therefore, ampicillin–sulbactam was used instead of sulbactam. The main activity of ampicillin–sulbactam against A. baumannii is attributed to the sulbactam component. The ampicillin moiety of this compound may restrict the dose of ampicillin–sulbactam in clinical practice. Efficacy and safety of different doses of sulbactam may be examined in well-designed, randomized, clinical trials for the treatment of VAP, resulting from carbapenem-resistant pathogens. Increasing incidence rate of infections due to MDR producing carbapenemase Gram-negative pathogens especially A. baumannii should be in mind when an empirical antibiotic regimen for empiric therapy of VAP is selected. Availability and cost are other deterring factors in selecting an appropriate antibiotic especially in developing countries. As discussed earlier, colistin is not an ideal antibiotic due to its limitations.
Conclusion
In this study clinical and microbiological response, duration of intensive care unit stay and 28-day mortality were compared between the meropenem/colistin and meropenem/ampicillin–sulbactam in critically ill patients with pneumonia due to A. baumannii. Sulbabtam (or ampicillin–sulbactam) may be a potential option for treatment of infections due to carbapenem-resistant A. baumannii. Therefore, further clinical trials are needed for the conclusion.
Future perspective
Treatment of infections due to Gram-negative pathogens especially A. baumannii is a challenging issue. Introducing appropriate antibiotic regimens for treatment of these infections should be considered in future well-designed multicenter studies with adequate sample sizes.
Aim
Sulbactam efficacy for the treatment of ventilator-associated pneumonia (VAP) was investigated in some studies.
The efficacy of colistin and ampicillin–sulbactam has not been compared in the treatment of VAP caused by A. baumannii.
Methods
47 patients with VAP caused by carbapenem-resistant A. baumannii were assigned to receive either meropenem/colistin or meropenem/ampicillin–sulbactam. Clinical response at the end of treatment course was classified either as a success or a failure. Microbiological response was categorized as eradication or persistent.
Results
Clinical improvement of pneumonia was achieved in 75 and 69.6% of patients in the meropenem/colistin and meropenem/ampicillin–sulbactam group, respectively. During the antibiotic treatment course, cultures of endotracheal samples became negative in 87.50 and 91.30% of patients in the meropenem/colistin and meropenem/ampicillin–sulbactam groups, respectively.
Conclusion
Sulbabtam (or ampicillin–sulbactam) may be a potential option for treatment of infections due to carbapenem-resistant A. baumannii.
Acknowledgements
The authors would like to thank the nursing staff of general ICU of Imam Khomeini Hospital, Iran for their kind support.
Financial & competing interests disclosure
The office of vice-chancellor for research of Tehran University of Medical Sciences, Tehran, Iran supported this work. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Craig CP, Connelly S. Effect of intensive care unit nosomial pneumonia on duration of stay and mortality. Am. J. Infect. Control. 12(4), 233–238 (1984).
2.
Safdar N, Dezfulian C, Collard HR, Saint S. Clinical and economic consequences of ventilator-associated pneumonia: a systematic review. Crit. Care Med. 33(10), 2184–2193 (2005).
•• A systematic review on ventilator-associated pneumonia.
3.
Gales AC, Jones RN, Sader HS. Contemporary activity of colistin and polymyxin B against a worldwide collection of Gram-negative pathogens: results from the SENTRY antimicrobial surveillance program (2006–09). J. Antimicrob. Chemother. 66(9), 2070–2074 (2011).
4.
Warren DK, Shukla SJ, Olsen MA et al. Outcome and attributable cost of ventilator-associated pneumonia among intensive care unit patients in a suburban medical center. Crit. Care Med. 31(5), 1312–1317 (2003).
5.
Magill SS, Edwards JR, Bamberg W et al. Multistate point-prevalence survey of healthcare–associated infections. N. Engl. J. Med. 370(13), 1198–1208 (2014).
6.
Jones RN. Resistance patterns among nosocomial pathogens: trends over the past few years. Chest J. 119(Suppl. 2), 397S–404S (2001).
7.
Almomani BA, McCullough A, Gharaibeh R, Samrah S, Mahasneh F. Incidence and predictors of 14-day mortality in multidrug-resistant Acinetobacter baumannii in ventilator-associated pneumonia. J. Infect. Dev. Ctries 9(12), 1323–1330 (2015).
8.
Afhami S, Hadadi A, Khorami E, Seifi A, Bazaz NE. Ventilator-associated pneumonia in a teaching hospital in Tehran and use of the Iranian Nosocomial infections surveillance software. East Mediterr. Health J. 19(10), 883 (2013).
9.
Munoz-Price LS, Weinstein RA. Acinetobacter infection. N. Engl. J. Med. 358(12), 1271–1281 (2008).
• Review of Acinetobacter infection.
10.
Weiner LM, Webb AK, Limbago B et al. Antimicrobial-resistant pathogens associated with healthcare-associated infections: summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2011–2014. Infect. Control Hosp. Epidemiol. 37(11), 1288–1301 (2016).
11.
Centres for Disease Control and Prevention. Antibiotic resistance threats in the United States (2013). www.cdc.gov/drugresistance/pdf/ar-threats-2013-508.pdf.
12.
Peleg AY, Seifert H, Paterson DL. Acinetobacter baumannii: emergence of a successful pathogen. Clin. Microbiol. Rev. 21(3), 538–582 (2008).
13.
Lolans K, Rice TW, Munoz-Price LS, Quinn JP. Multicity outbreak of carbapenem-resistant Acinetobacter baumannii isolates producing the carbapenemase OXA-40. Antimicrob. Agents Chemother. 50(9), 2941–2945 (2006).
14.
Centres for Disease Control and Prevention. Multidrug-resistant organism & Clostridium difficile infection (MDRO/CDI) module. National Healthcare Safety Network. Atlanta USA, 2013. www.cdc.gov/nhsn/PDFs/pscManual/12pscMDRO_CDADcurrent.pdf.
15.
Betrosian AP, Douzinas EE. ampicillin–sulbactam: an update on the use of parenteral and oral forms in bacterial infections. Expert Opin. Drug Metab. Toxicol. 5(9), 1099–1112 (2009).
16.
Bhavnani SM, Rubino CM, Hammel JP et al. Pharmacological and patient-specific response determinants in patients with hospital-acquired pneumonia treated with tigecycline. Antimicrob. Agents Chemother. 56(2), 1065–1072 (2012).
17.
Chu H, Zhao L, Wang M, Liu Y, Gui T, Zhang J. Sulbactam-based therapy for Acinetobacter baumannii infection: a systematic review and meta-analysis. Braz. J. Infect. Dis. 17(4), 389–394 (2013).
•• A systematic review on sulbactam-based therapy for Acinetobacter baumannii infection.
18.
Lin H-S, Lee M-H, Cheng C-W et al. Sulbactam treatment for pneumonia involving multidrug-resistant Acinetobacter calcoaceticus–Acinetobacter baumannii complex. J. Infect. Dis. 47(6), 370–378 (2015).
•• Evaluating sulbactam-based therapy for multidrug-resistant Acinetobacter.
19.
Betrosian AP, Frantzeskaki F, Xanthaki A, Georgiadis G. High-dose ampicillin–sulbactam as an alternative treatment of late-onset VAP from multidrug-resistant Acinetobacter baumannii. Scand. J. Infect. Dis. 39(1), 38–43 (2007).
20.
Jeong IB, Na MJ, Son JW, Kwon SJ. High-dose sulbactam treatment for ventilator-associated pneumonia caused by carbapenem-resistant Acinetobacter baumannii. Korean J. Crit. Care Med. 31(4), 308–316 (2016).
21.
Liu X, Zhao M, Chen Y et al. Synergistic killing by meropenem and colistin combination of carbapenem-resistant Acinetobacter baumannii isolates from Chinese patients in an in vitro pharmacokinetic/pharmacodynamic model. Int. J. Antimicrob. Agents 48(5), 559–563 (2016).
22.
Centers for Disease Control and Prevention. Pneumonia (ventilator-associated [VAP] and nonventilator-associated pneumonia [PNEU]) event. Device-associated Module PNEU/VAP (2015). www.cdc.gov/nhsn/pdfs/pscmanual/6pscvapcurrent.pdf.
23.
Wayne P. Performance Standards for Antimicrobial Susceptibility Testing, 26th Ed. CLSI supplement M100S. Clinical and Laboratory Standards Institute, CLSI, PA, USA (2016). http://shop.clsi.org/site/Sample_pdf/M100S26_sample.pdf.
24.
Magiorakos AP, Srinivasan A, Carey R et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 18(3), 268–281 (2012).
• An international expert proposal for interim standard definitions for acquired resistance.
25.
Kift EV, Maartens G, Bamford C. Systematic review of the evidence for rational dosing of colistin. S. Afr. Med. J. 104(3), 183–186 (2014).
26.
Levin AS, Levy CE, Manrique AEI, Medeiros EA, Costa SF. Severe nosocomial infections with imipenem-resistant Acinetobacter baumannii treated with ampicillin/sulbactam. Int. J. Antimicrob. Agents 21(1), 58–62 (2003).
• Treatment of carbapenem-resistant Acinetobacter.
27.
Jaruratanasirikul S, Sriwiriyajan S, Punyo J. Comparison of the pharmacodynamics of meropenem in patients with ventilator-associated pneumonia following administration by 3-h infusion or bolus injection. Antimicrob. Agents Chemother. 49(4), 1337–1339 (2005).
28.
Valachis A, Samonis G, Kofteridis DP. The role of aerosolized colistin in the treatment of ventilator-associated pneumonia: a systematic review and meta-analysis. Crit. Care Med. 43(3), 527–533 (2015).
29.
Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin. Pract. 120(4), C179–C184 (2012).
30.
Koulenti D, Tsigou E, Rello J. Nosocomial pneumonia in 27 ICUs in Europe: perspectives from the EU-VAP/CAP study. Eur. J. Clin. Microbiol. Infect. Dis. 36(11), 1999–2006 (2017).
31.
Camargo LF, De Marco FV, Barbas CS et al. Ventilator associated pneumonia: comparison between quantitative and qualitative cultures of tracheal aspirates. Crit Care. 8(6), R422 (2004).
32.
Roy S, Dalal BS, Mitra S, Dalal BS, Dasgupta R. Study of the isolates of suspected VAP, prevalence of the different organisms and mic patterns in a tertiary care hospital. Morb. Mortal. Wkly Rep. 4(09), 505–508 (2017).
33.
Haeili M, Ghodousi A, Nomanpour B, Omrani M, Feizabadi MM. Drug resistance patterns of bacteria isolated from patients with nosocomial pneumonia at Tehran hospitals during 2009–2011. J. Infect. Dev. Ctries 7(04), 312–317 (2013).
34.
Ho PL, Ho AY, Chow KH, Cheng VC. Surveillance for multidrug-resistant Acinetobacter baumannii: a lesson on definitions. Int. J. Antimicrob. Agents 36(5), 469–471 (2010).
35.
Arroyo LA, Mateos I, González V, Aznar J. In vitro activities of tigecycline, minocycline and colistin-tigecycline combination against multi-and pandrug-resistant clinical isolates of Acinetobacter baumannii group. Antimicrob. Agents Chemother. 53(3), 1295–1296 (2009).
36.
Ko KS, Suh JY, Kwon KT et al. High rates of resistance to colistin and polymyxin B in subgroups of Acinetobacter baumannii isolates from Korea. J. Antimicrob. Chemother. 60(5), 1163–1167 (2007).
37.
Cai Y, Chai D, Wang R, Liang B, Bai N. Colistin resistance of Acinetobacter baumannii: clinical reports, mechanisms and antimicrobial strategies. J. Antimicrob. Chemother. 67(7), 1607–1615 (2012).
38.
El-Halfawy OM, Valvano MA. Antimicrobial heteroresistance: an emerging field in need of clarity. Clin. Microbiol. Rev. 28(1), 191–207 (2015).
39.
Laishram S, Anandan S, Devi BY et al. Determination of synergy between sulbactam, meropenem and colistin in carbapenem-resistant Klebsiella pneumoniae and Acinetobacter baumannii isolates and correlation with the molecular mechanism of resistance. J. Chemother. 28(4), 297–303 (2016).
40.
Liu X, Zhao M, Chen Y et al. Synergistic killing by meropenem and colistin combination of carbapenem-resistant Acinetobacter baumannii isolates from Chinese patients in an in vitro pharmacokinetic/pharmacodynamic model. Int. J. Antimicrob. Agents 48(5), 559–563 (2016).
41.
Betrosian AP, Frantzeskaki F, Xanthaki A, Douzinas EE. Efficacy and safety of high-dose ampicillin/sulbactam vs. colistin as monotherapy for the treatment of multidrug resistant Acinetobacter baumannii ventilator-associated pneumonia. J. Infect. 56(6), 432–436 (2008).
• High-dose ampicillin/sulbactam for the treatment of multidrug-resistant Acinetobacter.
42.
Gauthier TP, Lantz E, Frederick C et al. Variability within investigations of intravenous colistin: the scope of the problem. Clin. Infect. Dis. 58(9), 1340–1342 (2014).
43.
Ortwine JK, Sutton JD, Kaye KS, Pogue JM. Strategies for the safe use of colistin. Expert Rev. Anti Infect. Ther. 13(10), 1237–1247 (2015).
44.
Kalil AC, Metersky ML, Klompas M et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 63(5), e61–e111 (2016).
45.
Choi J, Park Y, Kim C et al. Mortality risk factors of Acinetobacter baumannii bacteraemia. Intern. Med. 35(10), 599–603 (2005).
46.
Liu C-P, Shih S-C, Wang N-Y et al. Risk factors of mortality in patients with carbapenem-resistant Acinetobacter baumannii bacteremia. J. Microbiol. Immunol. Infect. 49(6), 934–940 (2016).
47.
Chiang D-H, Wang C-C, Kuo H-Y et al. Risk factors for mortality in patients with Acinetobacter baumannii bloodstream infection with genotypic species identification. J. Microbiol. Immunol. Infect. 41(5), 397–402 (2008).
48.
Melsen WG, Rovers MM, Groenwold RH et al. Attributable mortality of ventilator-associated pneumonia: a meta-analysis of individual patient data from randomized prevention studies. Lancet Infect. Dis. 13(8), 665–671 (2013).
49.
Zalts R, Neuberger A, Hussein K et al. Treatment of carbapenem-resistant Acinetobacter baumannii ventilator-associated pneumonia: retrospective comparison between intravenous colistin and intravenous ampicillin–sulbactam. Am. J. Ther. 23(1), e78–e85 (2016).
Information & Authors
Information
Published In
Copyright
© 2018 Future Medicine Ltd.
History
Received: 23 April 2018
Accepted: 6 June 2018
Published online: 7 September 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Meropenem/colistin versus meropenem/ampicillin–sulbactam in the treatment of carbapenem-resistant pneumonia. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0037
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Ajaree Rayanakorn, Thitiya Lukkunaprasit, Shaun Lee Wen Huey, Wasan Katip, Comparative efficacy and safety of colistin-based and alternative antibiotic regimens for multidrug-resistant Gram-negative infections: A systematic review and network meta-analysis, International Journal of Infectious Diseases, 10.1016/j.ijid.2026.108909, 170, (108909), (2026).
- Subhash Todi, Bharat G Jagiasi, Deven Juneja, Justin A Gopaldas, Kapil D Soni, Sunil Karanth, Ritu Singh, Mohit Kharbanda, Ashutosh Bhardwaj, Tapas K Sahoo, Shilpushp Bhosale, Sharmili Sinha, Manish Bharti, Anuj M Clerk, Amit Kumar, Bram Rochwerg, Vinod K Singh, Pradip K Bhattacharya, Indian Society of Critical Care Medicine Guidelines on Evidence-based Recommendations for the Treatment of Carbapenem-resistant Enterobacterales, Carbapenem-resistant Acinetobacter baumannii, and Carbapenem-resistant Pseudomonas aeruginosa in Critically Ill Patients: A GRADE-guided Approach, Indian Journal of Critical Care Medicine, 10.5005/jp-journals-10071-25216, 30, 6, (472-517), (2026).
- Francesco Nappi, Sulbactam–Durlobactam for Carbapenem-Resistant Acinetobacter baumannii–calcoaceticus Complex, Pathogens, 10.3390/pathogens15040449, 15, 4, (449), (2026).
- L.V. Zgrzheblovska, I.R. Malysh, I.M. Berezenko, Cefoperazone-sulbactam in combination with meropenem versus colistin in combination with meropenem in treatment of ventilator-associated pneumonia caused by carbapenem-resistant Acinetobacter baumannii, Infusion & Chemotherapy, 10.32902/2663-0338-9-2026-1-11-16, 9, 1, (11-16), (2026).
- Mostafa Mansouri, Jalal Mardaneh, Kiana Yahaei, Yeganeh Ahrari Roodi, Mohsen Sahebanmaleki, Combination Antibiotic Therapy with Colistin, Meropenem, and Ampicillin-Sulbactam for Carbapenem-Resistant Acinetobacter Infections: A Randomized Controlled Trial, Jundishapur Journal of Microbiology, 10.5812/jjm-164182, 19, 2, (2026).
- Natália Kehl Moreira, Mariana Preussler Mott, Luana Silva Dornelles, Caroline Collioni Constante, Larissa Lutz, Patricia Orlandi Barth, Rodrigo Minuto Paiva, Afonso Luís Barth, Juliana Caierão, Carbapenem Resistance among Enterobacterales Intrinsically Resistant to Polymyxin B in Southern Brazil, Brazilian Archives of Biology and Technology, 10.1590/1678-4324-2026250135, 69, (2026).
- Iman Karimzadeh, Sandra L. Kane-Gill, Binglei Ma, Anti-Infective-Associated AKI: A Narrative Review of the Epidemiology, Mechanisms, Risk Factors, Biomarkers, Clinical Course, Monitoring, Prevention, and Therapeutic Strategies, Antibiotics, 10.3390/antibiotics14111138, 14, 11, (1138), (2025).
- Chahat Choudhary, Vikas Kumar, Gyan Vardhan, Ashish Kumar, Puneet Dhamija, Combating carbapenem-resistant organisms with colistin-sparing regimens, Indian Journal of Physiology and Pharmacology, 10.25259/IJPP_356_2024, 69, (203-210), (2025).
- Mohananasunthari Poornachandran, Sabariah Noor Harun, Teh Sin Yin, Noorfatimah Yahaya, Siti Maisharah Sheikh Ghadzi, Population Pharmacokinetic Models of Ampicillin–Sulbactam Among Adult Patients with Infectious Diseases: A Systematic Review, Therapeutic Drug Monitoring, 10.1097/FTD.0000000000001380, 48, 1, (60-70), (2025).
- Jutima Baruah, Laishram Shantikumar Singh, Thounaojam Salvia, Debashree Bhowmik, Escalating threat of Acinetobacter baumannii : Resistance mechanisms and mitigation strategies a perspective , Journal of Laboratory Physicians, 10.25259/JLP_31_2025, 17, (235-246), (2025).
- See more