An indirect comparison of ustekinumab and vedolizumab in the therapy of TNF-failure Crohn's disease patients
Abstract
Aim: An indirect comparison of ustekinumab versus vedolizumab in patients with active moderate-to-severe Crohn's disease who were nonresponsive or intolerant to previous TNF-antagonist therapy. Methods: A systematic review was performed in Medline via PubMed, Embase, Cochrane Library, until 30 April 2017. Inclusion criteria were: randomized controlled trials, patients treated for Crohn's disease, ustekinumab or vedolizumab therapy. Included trials were critically appraised and afterward indirect comparison by Bucher was conducted; the manuscript was prepared in accordance to the PRISMA requirements. Results: Five randomized controlled trials were included and assessed for homogeneity; they occurred eligible for indirect comparison referring to induction or maintenance phase of TNF-antagonist failure population treatment; no statistically significant differences in clinical response (relative benefit [RB]: 1.14; 95% CI: 0.65–1.99; p = 0.64) as well as in clinical remission (RB: 1.16; 95% CI: 0.54–2.48; p = 0.71) in induction phase of therapy were revealed; no significant disparity was presented in a maintenance phase in clinical remission (RB: 0.72; 95% CI: 0.30–1.68; p = 0.44). No significant differences were also revealed in primary and secondary nonresponders subpopulations in clinical response. Indirect comparison of the safety profile presented no statistically significant difference between the biologics (relative risk [RR]: 0.93; 95% CI: 0.81–1.08; p = 0.35). Conclusion: No significant differences between vedolizumab and ustekinumab in clinical response and clinical remission for induction and remission in maintenance phase of TNF refractory patients therapy were revealed. In addition, no significant disparities in the risk of adverse events suggest a similar safety profile.
Crohn's disease (CD) is a chronic, autoimmune disease; it is a transmural, granulomatous inflammation of the GI tract of unknown etiology [1]. It usually develops in the age group from 15 to 30 years old [2]. The highest incidence was 20.2 per 100,000 person-years in North America, 12.7 per 100,000 person-years in Europe and 5.0 person-years in Asia and the Middle East [2]. The highest morbidity values for CD were reported for North America (319 per 100,000 persons) and Europe (322 per 100,000 persons) [2].
A range of pharmacotherapies can be used in CD patients; conventional therapies (5-aminosalycilate compounds, e.g., mesalazine, systemic corticosteroids, topical corticosteroids, e.g., budezonide and immunomodulators) remain limited because of inadequate control of the disease in a number of patients and this often leads to adverse events (AEs). Novel therapies include TNF-α antagonists (anti-TNFs or TNF antagonists) as: infliximab, adalimumab, golimumab or certolizumab pegol but also biologic of another way of activity as vedolizumab – a humanized monoclonal IgG1 antibody which inhibits migration and adhesion of leukocytes into the alimentary tract [3].
TNF-α antagonists are a standard biologic therapy of CD, of well-proven efficacy, providing reductions in hospitalizations and surgeries and improvement in patients’ quality of life [3,4]. However, around 10–30% of patients do not respond to the initial therapy (primary nonresponse) and 20–46% of patients lose response during therapy and need dose increase or providing another pharmacotherapy (secondary nonresponse) [4]. Primary nonresponders are less likely to benefit from another TNF-antagonist therapy but patients with secondary nonresponse who change to another TNF antagonist have lower probability to respond than TNF-naive patients [5]. This represents difficult clinical constraint as for such patients the clinical gain of alternative anti-TNF therapy may be reduced, so biologic drugs with other mechanisms of activity (such as ustekinumab or vedolizumab) seems to be necessary for effective therapy.
We focused on two novel biologic drugs considering their emerging position in the CD treatment, especially in TNF-antagonist-refractory subpopulations. Vedolizumab (Entyvio®) have been granted marketing authorization by the US FDA as well as the European Commission in 2014. In November 2016, the FDA as well as the European Commission has approved the use of ustekinumab (Stelara®) for the treatment of adult patients with moderately to severely active CD [6].
Ustekinumab is a fully human IgG1κ monoclonal antibody to IL-12/23 indicated for the treatment of adult patients with moderately to severely active CD; it's the first biologic therapy for CD that targets IL-12 and IL-23 cytokines, known to play a substantial role in inflammatory and immune responses. Intravenous dose of 6 mg/kg as induction therapy and afterwards the first subcutaneous 90 mg ustekinumab at week 8 should be administered. After this, subcutaneous 90 mg dosing every 12 weeks is recommended [6].
The use of vedolizumab is potentially less feasible to induce local or systemic adverse events than the use of other anti-α4 antibodies (e.g., natalizumab inducing progressive multifocal leukoencephalopathy in some patients) [7]; there is an evidence demonstrating a reduction in systemic adverse events of vedolizumab [8]; the authorized dose regimen is 300 mg administered intravenously at 0, 2 and 6 weeks and afterwards every 6 weeks [9].
Lack of evidence from head-to-head clinical trials comparing these biological drugs makes it necessary to perform indirect evaluations providing useful data about their relative efficacy. We applied a Bucher method – an adjusted indirect efficacy and safety comparison, recognized as a suitable and acceptable approach [10]. New therapeutic alternatives for patients with CD are urgently required, especially in case of primary or secondary nonresponders to standard biological therapy such as adalimumab or infliximab; therefore, the assessment of new promising molecules in the condition is critically important.
The objective of this indirect comparison was to evaluate the clinical efficacy and safety of two immunosuppressive monoclonal antibodies: ustekinumab and vedolizumab, in patients with active Crohn's disease who were intolerant or nonresponsive to previous TNF-antagonist treatment.
Methods
Literature search strategy
Randomized controlled trials (RCTs) comparing ustekinumab or vedolizumab with placebo in CD patients were included. The search strategy was based on the medical subject heading terms and EMTREE combined with Boole's logical operators (Table 1). A systematic review was performed in the following databases: Embase, Medline (via PubMed), Cochrane Central until 30 April 2017. Handsearching was also performed to screen the reference lists of the included papers to find additional relevant studies.
| Keywords (combined with Boole's logical operator, OR) | |
|---|---|
| Medical condition | Crohn disease OR Crohn's disease OR Crohns disease OR Crohn's enteritis OR regional enteritis OR granulomatous enteritis OR Ileocolitis OR granulomatous colitis OR terminal Ileitis OR regional ileitides OR regional ileitis OR regional enterocolitis OR cleron disease OR enteritis regionalis OR morbus Crohn |
| Intervention | Ustekinumab OR Stelara OR cnto-1275 OR cnto 1275 OR cnto1275 OR 1275, CNTO |
| Vedolizumab OR entyvio OR mln0002 OR mln 0002 OR mln 02 OR mln02 OR ldp 02 OR ldp02 | |
| Methodological limits | PubMed: humans, randomized controlled trial, clinical trial, controlled clinical trial; Embase: humans, controlled clinical trials, randomized controlled trial, Embase only; Cochrane Central Register of Controlled Trials: no limits applied; word variations have been searched |
| Language limits | PubMed, Embase: English |
Selection criteria
Two independent contributors (P Kawalec and P Moćko) used the same search strategy to identity relevant clinical trials. The study selection was based on the titles and abstracts and finally, on full-text articles.
All relevant RCTs were selected and critically appraised according to the PRISMA statement requirements [11]. The following criteria were used for study inclusion: first, RCTs; second, patients treated for CD; third, ustekinumab or vedolizumab therapy. We included full-text papers if they contained the necessary information about: methods used, treatment patterns and population characteristics. Abstracts were rejected due to the lack of detailed information about methods used, population and results; available data on file (www.clinicaltrials.gov) were searched. Nonrandomized as well as uncontrolled open-label studies were not included.
Data extraction
Data on clinical response and clinical remission were extracted both for induction and maintenance phases of therapy. The safety analysis embraced the following data: any AEs, serious AEs (SAEs), AEs associated with infusion or injection-site reactions/infusion reactions and infections. We have also extracted data as follows: population characteristics, study design (methodology), details on intervention and regimen, definition of outcomes as well as treatment duration and follow-up period. We considered only results for approved doses of ustekinumab (6 mg/kg) and vedolizumab (300 mg).
Data analysis & indirect comparison
The quality of the eligible RCTs was evaluated using the Cochrane Collaboration's recommended tool for assessing the risk of bias [12]. Results of indirect comparisons were presented as relative risks (RRs) with 95% CIs for considered efficacy outcomes and adverse events. The fixed effects model was used to calculate relative parameters when the statistical heterogeneity was not confirmed and the random effects model was used when heterogeneity was detected (p < 0.10). The impact of the intervention (for dichotomous data and positive outcomes, e.g., clinical response, clinical remission) was presented as a relative benefit – RB (described as RR) on the graphs with 95% CI. AEs as negative outcomes were summarized with RR. Statistical significance was defined at a p-value of less than 0.05 for the calculations performed. Indirect comparisons and statistical tests were presented as forest plots using Microsoft Excel® as well as the Stats Direct® and Review Manager, v.5.3 software. The indirect comparisons results were disclosed as figures; direct comparisons between ustekinumab and placebo or vedolizumab and placebo (solid squares) as well as results of indirect comparisons between ustekinumab and vedolizumab (blank rhombus) with 95% CIs (horizontal lines) were depicted.
Results
Results of systematic review & quality of studies included
The systematic review revealed five RCTs presented in five publications [13–17] (three studies compared ustekinumab and placebo: CERTIFI [13], UNITI-1 and IM-UNITI [14]), while two studies compared vedolizumab and placebo: GEMINI-2 [15] and GEMINI-3 [16]; additional post hoc analyses including results of [15] and [16] were also published [17] (Figure 1). The studies were homogeneous enough to perform an indirect comparison for the induction phase. For the maintenance phase, only two trials occurred eligible for the indirect comparison [14,15] (a heterogeneity analysis was presented in Supplementary Table 1).

Figure 1. Search flow diagram.
RCT: Randomized controlled trial.
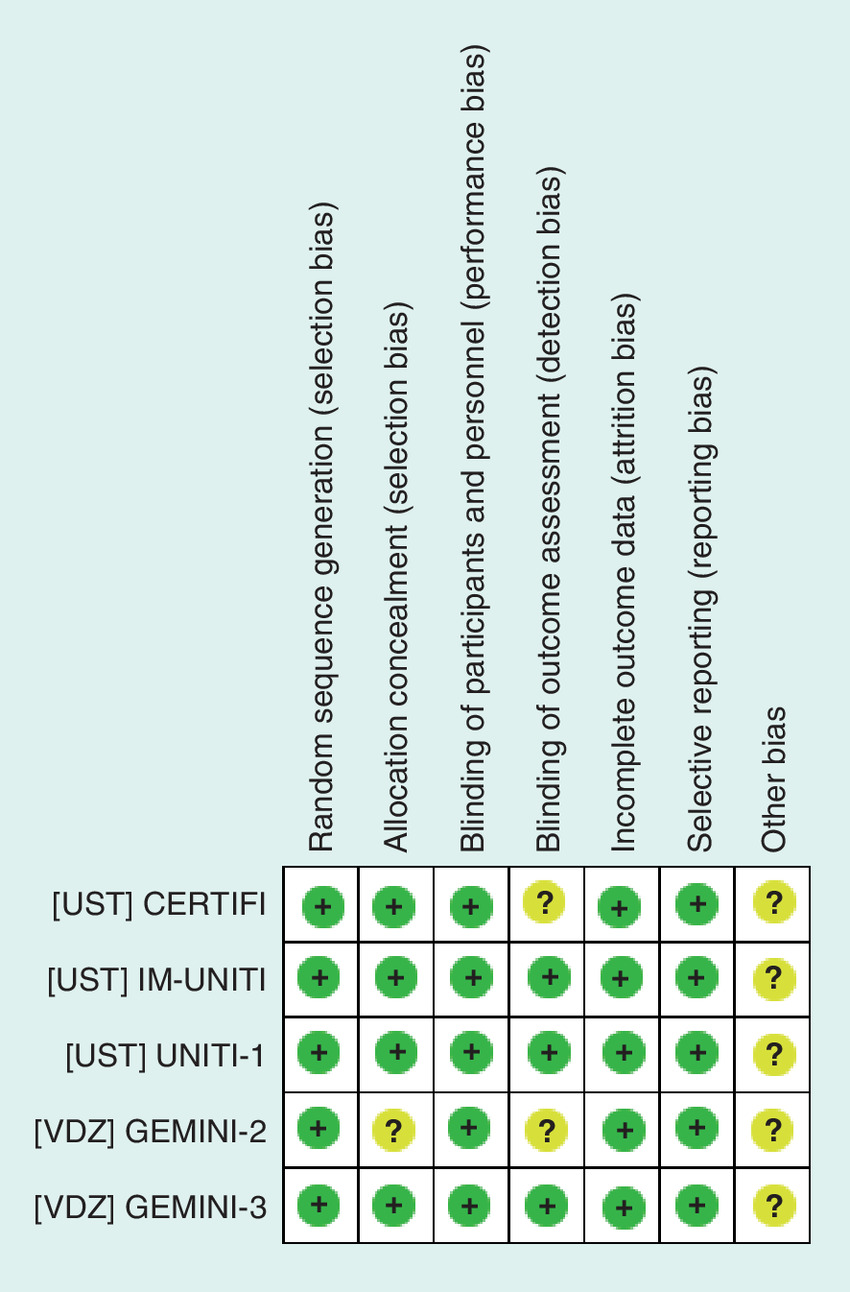
Included studies were randomized and double-blind. The methodological quality of the included RCTs was assessed as high as we revealed just some detection bias in case of two trials. A risk of bias in most domains was assessed as low (Figure 2).
Clinical efficacy assessment
We extracted data for the considered subpopulation from ustekinumab studies [13,14] as well as vedolizumab trials [15–17]. The calculations for the maintenance phase were performed due to available data and were based on results presented in IM-UNITI [14] and GEMINI-2 [15]. The results from individual studies were presented in Supplementary Table 2. Additional comparisons for primary and secondary nonresponders were performed as we have found eligible data for the subpopulations [13–14,17].
Clinical response in induction phase of therapy
Clinical response was defined as a ≥100-point decrease in the Crohn's disease activity index [13–16] and was recorded in the induction phase of treatment (data revealed for week 6 of therapy; Supplementary Table 2). In a subgroup of patients, intolerant or refractory to anti-TNF therapy, clinical response in the vedolizumab group did not differ significantly from that in the ustekinumab treated. A comparison by Bucher revealed no statistically significant difference between ustekinumab and vedolizumab with regard to achieving clinical response at week 6 during induction phase of therapy. In addition, no significant disparities were revealed for primary and secondary nonresponders (Figure 3).
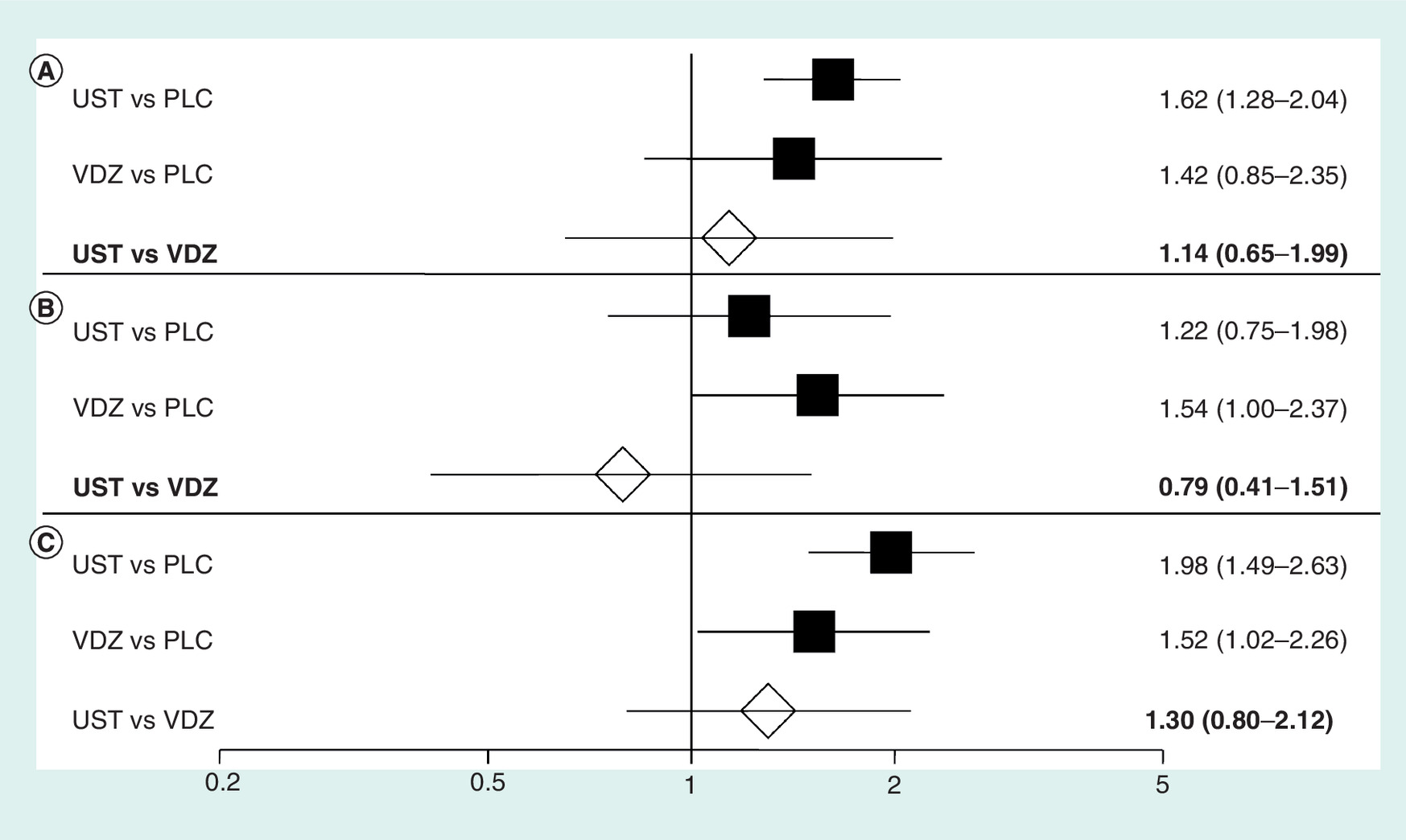
Figure 3. Indirect comparison of ustekinumab and vedolizumab for clinical response in induction phase of therapy (6 weeks).
(A) subpopulation of Crohn's disease patients with TNF treatment failure or intolerance; (B) primary nonresponders; (C) secondary nonresponders.
PLC: Placebo; UST: Ustekinumab; VDZ: Vedolizumab.
Clinical remission in induction phase of therapy
Clinical remission was defined as a Crohn's disease activity index of 150 or less and was analyzed in the induction phase of treatment [14,15] (data revealed for week 6; Supplementary Table 2). The overall results of the indirect comparison demonstrated that ustekinumab (for dosing regimen including 6 mg/kg) was as effective as vedolizumab (300 mg) for induction of clinical remission at week 6 (Figure 4).
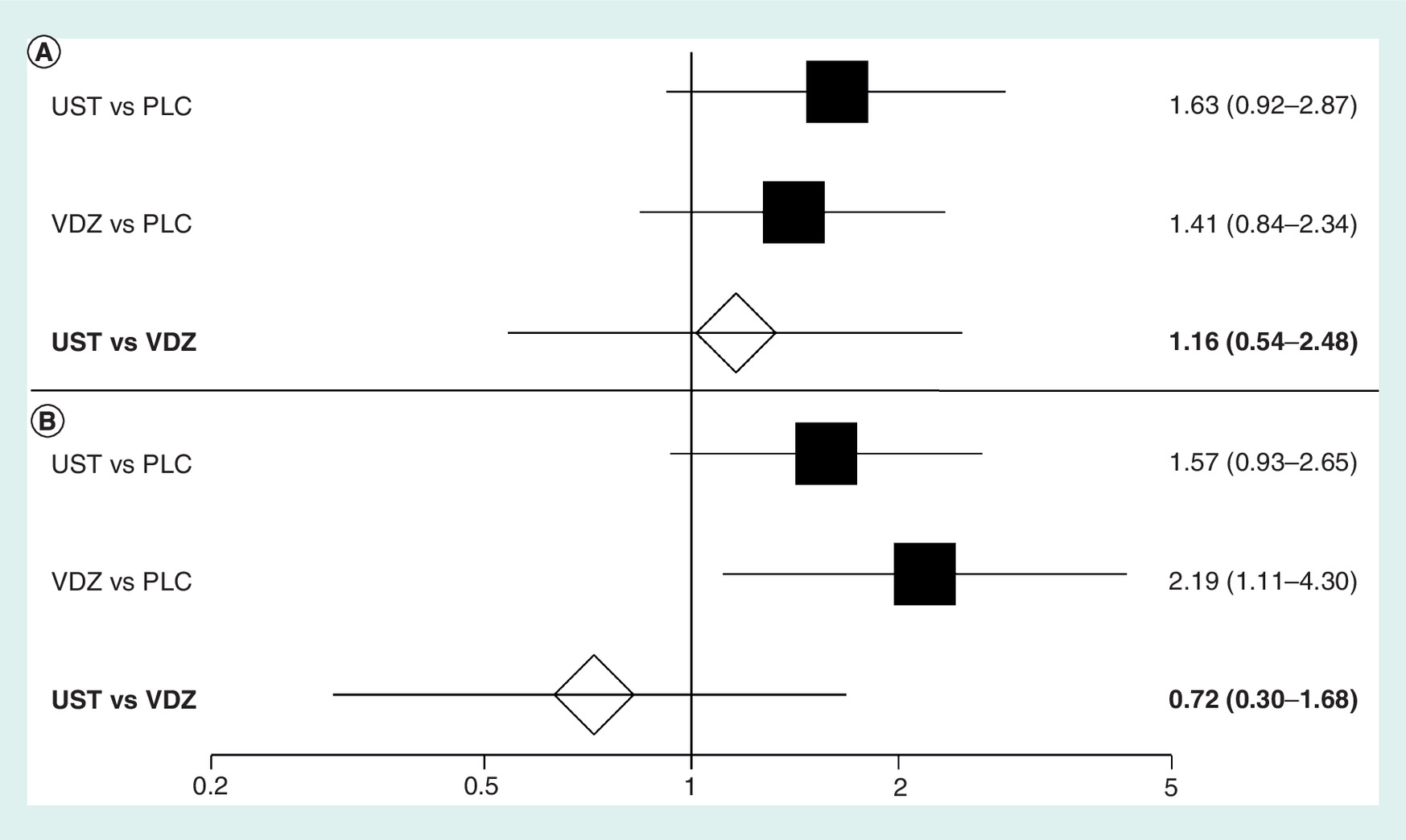
Figure 4. Indirect comparison of ustekinumab and vedolizumab for clinical remission in a subpopulation of Crohn's disease patients with TNF treatment failure or intolerance.
(A) Induction phase of therapy; (B) Maintenance phase of therapy.
PLC: Placebo; UST: Ustekinumab; VDZ: Vedolizumab.
Clinical remission in maintenance phase of therapy
In the maintenance phase, there was no significant difference between ustekinumab and vedolizumab for clinical remission after a total of 52 weeks of treatment in a subpopulation of patients who were intolerant or refractory to TNF-antagonist treatment (Figure 4).
Safety assessment in the induction phase of therapy
In regard to the risk of any AEs during short-term induction phase of treatment (6–10 weeks) no significant difference between ustekinumab and vedolizumab was revealed; there were also no significant differences in the frequency of any SAEs, serious infections or infusion-related reactions in the induction phase of therapy (Figure 5).
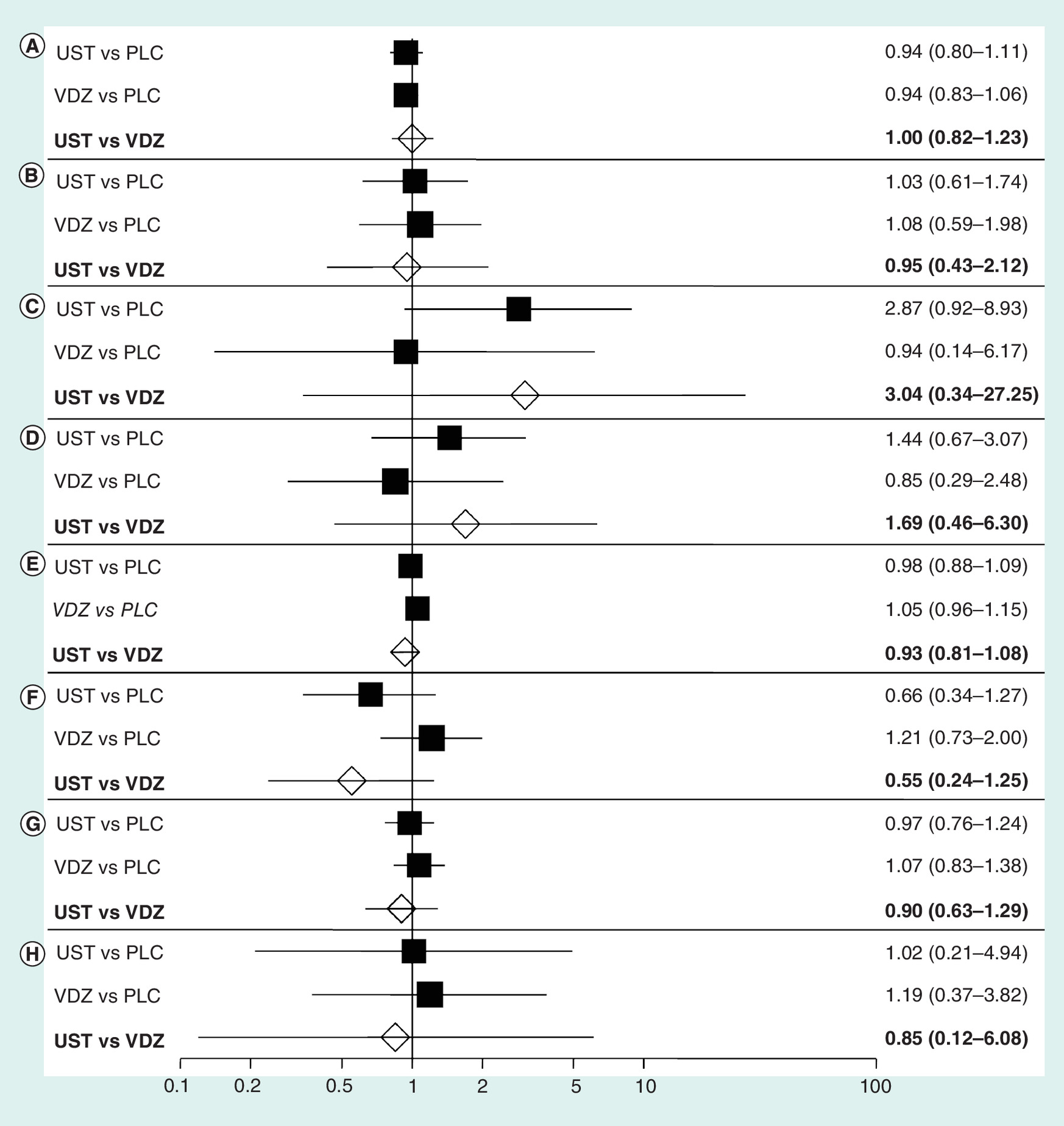
Figure 5. Indirect comparison of safety profile of ustekinumab and vedolizumab in Crohn's disease patients.
(A) any adverse events (AEs); (B) any serious adverse events (SAEs); (C) serious infections; (D) injection-site reactions (results for A–D in induction phase of therapy); (E) any AEs; (F) any SAEs; (G) any infections; (H) serious infections (results for E-H in maintenance phase of therapy).
PLC: Placebo; UST: Ustekinumab; VDZ: Vedolizumab.
The safety analysis for induction phase indicated the lack of statistically significant differences in case of the following common (reported by at least 5% of the patients) AEs: pyrexia, nasopharyngitis, abdominal pain, arthralgia, headache, nausea and fatigue (Table 2).
| UST 6 mg/kg | VDZ 300 mg | ||
|---|---|---|---|
| Feagan 2016 (UNITI-1) [14] UST (n = 249) vs PLC (n = 245); 8 weeks | Sandborn 2013 CERTIFI [13] UST n = 131) vs PLC n = 132); 8 weeks | Sands 2014 GEMINI-3 [16] VDZ (n = 209) vs PLC (n = 207); 10 weeks | Sandborn 2013 GEMINI-2 [15] VDZ (n = 220†) vs PLC (n = 148†); 6 weeks |
| Arthralgia | |||
| 15 (6.0%) vs 18 (7.3%) | 6 (4.6%) vs 5 (3.8%) | 10 (5%) vs 9 (4%) | – |
| RR: 0.82 (95% CI: 0.29–2.34); p = 0.71 | |||
| Headache | |||
| 20 (8.0%) vs 22 (9.0%) | 13 (9.9%) vs 8 (6.1%) | 11 (5%) vs 15 (7%) | 19 (9%) vs12 (8%) |
| RR: 1.25 (95% CI: 0.58–2.68); p = 0.57 | |||
| Nausea | |||
| 13 (5.2%) vs 18 (7.3%) | 8 (6.1%) vs 11 (8.3%) | 12 (6%) vs 5 (2%) | 11 (5%) vs 9 (6%) |
| RR: 0.53 (95% CI: 0.17–1.73); p = 0.29 | |||
| Pyrexia | |||
| 15 (6.0%) vs 15 (6.1%) | – | 7 (3%) vs 13 (6%) | 9 (4%) vs 2 (1%) |
| RR: 0.87 (95% CI: 0.14–5.37); p = 0.87 | |||
| Nasopharyngitis | |||
| 11 (4.4%) vs 13 (5.3%) | 8 (6.1%) vs 6 (4.5%) | 9 (4%) vs 8 (4%) | – |
| RR: 0.89 (95% CI: 0.29–2.73); p = 0.84 | |||
| Abdominal pain | |||
| 13 (5.2%) vs 13 (5.3%) | 7 (5.3%) vs 9 (6.8%) | 9 (4%) vs 6 (3%) | – |
| RR: 0.61 (95% CI: 0.19–1.97); p = 0.40 | |||
| Fatigue | |||
| 9 (3.6%) vs 13 (5.3%) | – | 6 (3%) vs 2 (<1%) | – |
| RR: 0.23 (95% CI: 0.04–1.38); p = 0.10 | |||
Safety assessment in the maintenance phase of therapy
An indirect comparison revealed no statistically significant differences between ustekinumab and vedolizumab in the frequency of any AEs and SAEs in the maintenance phase. Moreover, during 52 weeks of treatment the risk of any infections or the probability of serious infections (Figure 5) occurred similar in ustekinumab and vedolizumab groups.
Discussion
Vedolizumab is currently used in emerging group of patients with inflammatory bowel diseases due to high efficacy and good safety profile [18,19] while ustekinumab is a novel biologic drug just approved in the therapy of CD [6]. In currently published literature neither efficacy nor safety profile comparisons between ustekinumab and vedolizumab were performed. Due to lack of direct clinical comparisons, the positioning of ustekinumab and vedolizumab in the therapeutic paradigm of CD patients refractory or intolerant to TNF antagonists should be based on indirect comparisons both for clinical efficacy (clinical response, induction and maintenance of remission) and for safety profile.
In a systematic review, we have found three randomized, placebo-controlled clinical trials evaluating ustekinumab in CD therapy. In a Phase IIA study [20], ustekinumab presented efficacy in patients with moderate-to-severe CD, especially in a group of patients on prior infliximab therapy; the drug regimen used and cross-over study project made the trial heterogeneous to pivotal studies [13–16] thus, made it impossible to include its results to indirect comparisons. In a Phase IIB trial, intravenous ustekinumab induction therapy in CD patients refractory to TNF-antagonist therapy had significantly more often a clinical response but not remission, and maintenance doses of ustekinumab administered subcutaneously occurred effective during a period of 22 weeks [13].
The pivotal study published in 2016 [14] was a Phase III development program for the treatment of CD with ustekinumab embraced two 8-week induction trials (UNITI-1 and UNITI-2) and one 44-week maintenance trial (IM-UNITI), providing results for 52 weeks of therapy. In UNITI-1, patients received one or more TNF antagonists at approved doses and have met the criteria for primary or secondary nonresponse or to have had unacceptable AEs. In UNITI-2, treatment failure or unacceptable AEs when treated with immunosuppressants or glucocorticoids were inclusion criteria; patients could have received prior TNF antagonists; we have not taken the study into consideration as we focused on specific subpopulation. Patients who terminated UNITI-1 or UNITI-2 and had a clinical response to ustekinumab induction therapy were enrolled to the IM-UNITI maintenance trial. When exploring data for maintenance phase of therapy we considered only results for UNITI-1 population; the patients with a response to ustekinumab at induction were likely to sustain a clinical remission during maintenance, despite having received just a single intravenous induction dose of ustekinumab. This finding could indicate that ustekinumab has a long duration of action. No deaths, serious opportunistic infections or major adverse cardiovascular events were revealed and the rates of drug-specific antibodies were low [13,14].
The efficacy, safety and tolerability of vedolizumab induction and maintenance therapies in CD were revealed in the pivotal GEMINI-2 [15] and GEMINI-3 [16] studies. The meta-analysis presented that clinical response was significantly higher for vedolizumab-treated patients compared with placebo in the overall population and in both considered subgroups: patients with previous failure of anti-TNF treatment as well as TNF-naive patients. The clinical remission in the overall population and subpopulation of TNF-antagonist-naive patients was significantly higher for vedolizumab group compared with placebo while the risk of AEs, SAEs and serious infections occurred similar [19].
Clinical effects of vedolizumab in induction and maintenance therapy in TNF-naive or TNF-failure subgroups were evaluated in a pooled analysis of data from GEMINI-2 and GEMINI-3 [17]. In TNF-failure patients, the effects of vedolizumab induction of clinical remission in week 6 remained unproved but it became significant in week 10. Remission rates remained higher than placebo with vedolizumab maintenance through week 52 in both TNF-naive and TNF-failure populations, illustrating the potential value of vedolizumab as a first-line biologic as well as treatment alternative in those who are TNF antagonists nonresponsive. Compared with placebo, vedolizumab generally showed similar efficacy irrespective of the type of prior TNF-antagonist failure but response and remission rates were higher in TNF-naive population than in patients who had experienced TNF failure [17].
In our research we focused on assessment of the biologics in primary nonresponders to TNF-antagonist therapy as this group of patients have the lowest chances to get an effective therapy so providing alternatives for infliximab, adalimumab and certolizumab pegol seems to be a priority. As suggested in other publications [4,21], secondary nonresponders are more likely to benefit from alternative treatment compared with patients refractory to induction TNF-antagonist therapy. Treatment failure of the first TNF antagonist is connected with a lower rate of clinical response to subsequent TNF-α antagonists, limiting available treatment options for patients with CD [4,21–22]. We performed a sophisticated research for exclusive results for primary and secondary nonresponders subpopulations and have found relevant data for ustekinumab (UNITI-1 study) [14] as well as pooled data referring to vedolizumab trials (GEMINI-2 or GEMINI-3) [17]. No significant additional benefit in response rate in a subgroup of primary nonresponders in UNITI-1 study was revealed but in vedolizumab group a significant difference compared with placebo was shown in week 6 and 10 [17] but it ceased in 52 weeks; results presented for vedolizumab [17] were revealed as post hoc analysis of lower credibility and some additional research is necessary to provide more robust data.
Due to some heterogeneity in methodology between reference studies [14,17] as well as limited number of end points and periods available for comparison (only response rate for 6 weeks) some further clinical research in relevant subpopulations of TNF-failure patients is necessary (e.g., mucosal healing as an efficacy end point would be interesting but impossible for assessment due to lack of relevant data).
The Bucher method is an indirect comparison of two interventions, adjusted according to the results of their direct comparisons with a common therapy or placebo. The results of indirect comparisons have limited credibility but provides the most worthwhile data until direct comparisons are performed [10,23]; until recently, no clinical trials comparing ustekinumab with vedolizumab are currently being conducted or even planned.
We faced with some differences between studies for evaluated biologics. Although in case of ustekinumab trials [CERTIFI 13, UNITI-1 14] drugs were administered for 8 weeks while in case of vedolizumab trials for 6 weeks [15] or 10 weeks [16], all results were presented for the same follow-up of 6 weeks thus enabling indirect comparisons. Moreover, in general population characteristics also differences occurred as specified in Supplementary Table 1 but we extracted only data for relevant subpopulations indicating only TNF-antagonist-failure patients; we considered results from UNITI-1 [14] study and in case of vedolizumab trials – extracted data only for subpopulation of patients with prior anti-TNF failure [15–17].
Maintenance extension of study [16] was open-label so data were excluded from analysis and in case of [13] maintenance, outcomes were assessed at 22 weeks (after a total 30 weeks of treatment) so results for this study were also omitted.
Due to significant differences in follow-up period for reported outcomes, the only studies suitable for safety profile comparisons were [14] and [15] assessing vedolizumab and ustekinumab in 6 weeks of induction therapy (in study [13] and [16] safety data at week 52 was unavailable).
The indirect comparison showed no significant differences for any of the studied safety outcomes although a trend favoring vedolizumab in serious infections rate (Figure 5C) and favoring ustekinumab in any serious adverse effects (Figure 5F) was revealed. We have made an indirect safety analysis but it could be limited due to the potential gut-selective immunosuppressive properties of vedolizumab.
A possibility to conduct a network meta-analysis (NMA; mixed-treatment comparison) instead of an indirect comparison by the Bucher method was analyzed. The NMA is a sophisticated technique providing comparisons of considered therapeutic options, including results of direct and indirect comparisons for compared drugs. Nevertheless, the use of the NMA could be risky as studies included are often methodologically and clinically heterogeneous [24]. According to the recommendations of European network for Health Technology Assessment, the choice of indirect comparison method should be considered based on available evidence [25]. In our opinion, the available RCTs and relevant data placed Bucher's method over NMA so we used a more transparent way to provide the best available evidence for the comparison of considered biological drugs in CD therapy.
An increasing number of patients with CD make it necessary to develop new drugs to effectively induce and maintain remission, improve quality of life and prevent surgery in these patients. Increasing demand for new therapeutic options in patients with CD, especially in case of primary or secondary nonresponders to TNF antagonists is obvious. More and more patients are intolerant or unresponsive to standard biologic anti-TNF therapy; due to their ineffectiveness in a number of patients, the search for alternative biologic therapies should be released.
Conclusion
No statistically significant differences between ustekinumab and vedolizumab in clinical response and clinical remission for induction and remission in maintenance phase of therapy were revealed in the TNF-antagonist failure population as well as in primary and secondary nonresponders. In addition, a similar safety profile was revealed for the considered drugs.
Efficacy and safety of ustekinumab and vedolizumab assessment in patients with active moderate-to-severe Crohn's disease who were nonresponsive or intolerant to previous TNF-antagonist therapy is important in clinical practice.
No direct comparison of these two novel drugs was performed up to date, so indirect comparison by Bucher was performed.
No statistically significant differences in clinical response as well as in clinical remission in induction phase of therapy were revealed.
No significant differences were presented in a maintenance phase in clinical remission.
No significant differences were also revealed in primary and secondary nonresponder subpopulations in clinical response.
No significant differences in the risk of adverse events suggest a similar safety profile.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Supplementary Material
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Baumgart DC, Sandborn WJ. Crohn's disease. Lancet 380(9853), 1590–1605 (2012).
2.
Molodecky NA, Soon IS, Rabi DM et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology 142(1), 46–54 (2012).
3.
Gomollon F, Dignass A, Vito A et al. 3rd European evidence based consensus on the diagnosis and management of Crohn's disease 2016: Part 1: Diagnosis and medical management. J. Crohns Colitis 11(1), 3–25 (2017).
4.
Roda G, Jharap B, Neeraj N, Colombel JF. Loss of response to anti-TNFs: definition, epidemiology, and management. Clin. Transl. Gastroenterol. 7(1), e135 (2016).
5.
Colombel JF, Sandborn WJ, Rutgeerts P et al. Adalimumab for maintenance of clinical response and remission in patients with Crohn's disease: the CHARM trial. Gastroenterology 132, 52–65 (2007).
6.
Summaryof Product Characteristics for Entyvio (vedolizumab). (Accessed 2 August 2017). www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000958/WC500058513.pdf.
7.
Tilg H, Kaser A. Vedolizumab, a humanizedmab against the alpha4beta7 integrin for the potential treatment of ulcerativecolitis and Crohn's disease. Curr. Opin. Investig. Drugs 11(11), 1295–1304 (2010).
8.
Wyant T, Leach T, Sankoh S et al. Vedolizumab affectsantibody responses to immunisation selectively in the gastrointestinal tract:randomised controlled trial results. Gut 64(1), 77–83 (2015).
9.
Summaryof Product Characteristics for Entyvio (vedolizumab). (Accessed 7 August 2017). https://ec.europa.eu/health/documents/community-register/2014/20140522128514/anx_128514_en.pdf.
10.
Bucher HC, Guyatt GH, Griffith LE, Walter SD. The results of direct andindirect treatment comparisons in meta-analysis of randomized controlled trials. J. Clin. Epidemiol. 50(6), 683–691 (1997).
11.
Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 6(7), e1000097 (2009).
12.
Higgins JP, Green S. Cochrane handbook forsystematic reviews of interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration (2011).
13.
Sandborn WJ, Gasink C, Long-Long G et al. Ustekinumab induction andmaintenance therapy in refractory Crohn's disease. N. Engl. J. Med. 367, 1519–1528 (2012).
• Pivotal input for indirect comparisons performed.
14.
Feagan BG, Sandborn WJ, Gasink C et al. Ustekinumab as inductionand maintenance therapy for Crohn's disease. N. Engl. J. Med. 375, 1946–1960 (2016).
• Pivotal input for indirect comparisons performed.
15.
Sandborn WJ, Feagan BG, Rutgeerts P et al. Vedolizumab as inductionand maintenance therapy for Crohn's disease. N. Engl. J. Med. 369(8), 711–721 (2013).
• Pivotal input for indirect comparisons performed.
16.
Sands BE, Feagan BG, Rutgeerts P et al. Effects of vedolizumabinduction therapy for patients with Crohn's disease in whom tumor necrosisfactor antagonist treatment failed. Gastroenterology 147(3), 618–627 (2014).
• Pivotal input for indirect comparisons performed.
17.
Sands BE, Sandborn WJ, Van Assche G et al. Vedolizumab as inductionand maintenance therapy for Crohn's disease in patients naïve to or who havefailed tumor necrosis factor antagonist therapy. Inflamm. Bowel Dis. 23(1), 97–106 (2017).
• Pivotal input for indirect comparisons performed.
18.
Feagan BH, Patel H, Colombel JF et al. Effectsof vedolizumab on health-related quality of life in patients withulcerative colitis: results from the randomised GEMINI 1 trial. Aliment Pharmacol. Ther. 45(2), 264–275 (2017).
19.
Moćko P, Kawalec P, Smela-Lipińska B, Pilc A. Effectiveness and safety ofvedolizumab for treatment of Crohn's disease: a systematic review andmeta-analysis. Arch. Med. Sci. 12(5), 1088–1096 (2016).
•• Additional data on pivotal studies included to indirect comparisons.
20.
Sandborn WJ, Feagan BG, Fedorak RN et al. A randomized trial ofustekinumab, a human interleukin-12/23 monoclonal antibody, in patients withmoderate-to-severe Crohn's disease. Gastroenterology 135(4), 1130–1141 (2008).
•• Additional data on pivotal studies included to indirect comparisons.
21.
Sandborn WJ. Clinical perspectives inCrohn's disease. Moving forward with anti-TNF-alpha therapy: current needs andfuture treatments. Rev. Gastroenterol. Disord. 7(Suppl. 2), S23–S35 (2007).
22.
Sandborn WJ, Rutgeerts P, Enns R et al. Adalimumab inductiontherapy for Crohn disease previously treated with infliximab: a randomizedtrial. Ann. Intern. Med. 146, 829–838 (2007).
23.
Kawalec P, Moćko P, Pilc A, Radziwon Zalewska M, Malinowska-Lipień I. Vedolizumab compared withcertolizumab in the therapy of Crohn's disease: a systematic review and indirectcomparison. J. Human Pharmacol. Drug Ther. 36(8), 861–869 (2016).
24.
Brignardello-Petersen R, Rochwerg B, Guyatt GH et al. What is a networkmeta-analysis and how can we use it to inform clinical practice? Pol. Arch. Med. Wewn. 124(12), 659–660 (2014).
25.
European Network for Health Technology Assessment. Guideline: comparators and comparisons. Direct and Indirect Comparisons (2013). (Accessed 2 August 2017). www.eunethta.eu/sites/5026.fedimbo.belgium.be/files/Direct%20and%20indirect%20comparisons.pdf.
Information & Authors
Information
Published In
Copyright
© 2018 Future Medicine Ltd.
History
Received: 12 June 2017
Accepted: 11 August 2017
Published online: 8 November 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
An indirect comparison of ustekinumab and vedolizumab in the therapy of TNF-failure Crohn's disease patients. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0041
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Paweł Moćko, Magdalena Koperny, Katarzyna Śladowska, Przemysław Holko, Iwona Kowalska‐Bobko, Paweł Kawalec, Efficacy and safety of mirikizumab compared with currently approved biologic drugs for the treatment of ulcerative colitis: A systematic review and network meta‐analysis, Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy, 10.1002/phar.4611, 44, 10, (811-821), (2024).
- Ahmad Alamer, Lina H Al Lehaibi, Mukhtar Alomar, Fahad Aldhuwayan, Saleh Alshouish, Anfal Y Al-Ali, Zakia Almudhry, Abdulaziz Almulhim, Abdulhamid Althagafi, Saad Aldosari, Turki AlAmeel, Short term effectiveness of ustekinumab versus vedolizumab in Crohn’s disease after failure of anti-TNF agents: An observational comparative study design with a Bayesian analysis, Saudi Journal of Gastroenterology, 10.4103/sjg.sjg_101_24, 30, 5, (324-334), (2024).
- Andreas Sturm, Raja Atreya, Dominik Bettenworth, Bernd Bokemeyer, Axel Dignass, Robert Ehehalt, Christoph-Thomas Germer, P. C. Grunert, Ulf Helwig, Karoline Horisberger, Klaus Herrlinger, Peter Kienle, Torsten Kucharzik, Jost Langhorst, Christian Maaser, Johann Ockenga, Claudia Ott, Britta Siegmund, Sebastian Zeißig, Andreas Stallmach, Aktualisierte S3-Leitlinie „Diagnostik und Therapie des Morbus Crohn“ der Deutschen Gesellschaft für Gastroenterologie, Verdauungs- und Stoffwechselkrankheiten (DGVS) (Version 4.1) – living guideline, Zeitschrift für Gastroenterologie, 10.1055/a-2309-6123, 62, 08, (1229-1318), (2024).
- Patrick Gagnon-Sanschagrin, Myrlene Sanon, Mikhaïl Davidson, Cynthia Willey, Sumesh Kachroo, Timothy Hoops, Dominik Naessens, Annie Guerin, Martin Cloutier, The economic impact of suboptimal treatment and treatment switch among patients with Crohn’s disease treated with a first-line biologic – A US retrospective claims database study, Journal of Medical Economics, 10.1080/13696998.2024.2374645, 27, 1, (931-940), (2024).
- Michael Chiorean, Jeanne Jiang, Ninfa Candela, Grace Chen, Hela Romdhani, Dominick Latremouille-Viau, Sherry Shi, Rebecca Bungay, Annie Guerin, Tao Fan, Real-world clinical outcomes and healthcare costs in patients with Crohn’s disease treated with vedolizumab versus ustekinumab in the United States, Current Medical Research and Opinion, 10.1080/03007995.2024.2326585, 40, 5, (877-885), (2024).
- Klaudia Farkas, Hajnal Székely, Péter Bacsur, Balázs Bánky, Zsuzsa Bianka Élthes, László Harsányi, Katalin Edit Müllner, Ágnes Milassin, Károly Palatka, Patrícia Sarlós, Tamás Szamosi, Tamás Molnár, Pál Miheller, A Crohn-betegég terápiás stratégiája, Orvosi Hetilap, 10.1556/650.2024.33020, 165, Supplement-1, (1-36), (2024).
- Mahmoud H. Mosli, Hajer Y. Almudaiheem, Turki AlAmeel, Shakir A. Bakkari, Othman R. Alharbi, Khalidah A. Alenzi, Amr M. Khardaly, Maha A. AlMolaiki, Bedor A. Al-Omari, Rayan G. Albarakati, Ahmed H. Al-Jedai, Omar I. Saadah, Majid A. Almadi, Badr Al-Bawardy, Saudi Arabia consensus guidance for the diagnosis and management of adults with inflammatory bowel disease, Saudi Journal of Gastroenterology, 10.4103/sjg.sjg_277_22, 29, Suppl 1, (S1-S35), (2022).
- Andreas Sturm, Raja Atreya, Dominik Bettenworth, Bernd Bokemeyer, Axel Dignaß, Robert Ehehalt, Christoph Germer, Philip C. Grunert, Ulf Helwig, Klaus Herrlinger, Peter Kienle, Martin E. Kreis, Torsten Kucharzik, Jost Langhorst, Christian Maaser, Johann Ockenga, Claudia Ott, Britta Siegmund, Sebastian Zeißig, Andreas Stallmach, Aktualisierte S3-Leitlinie „Diagnostik und Therapie des Morbus Crohn“ der Deutschen Gesellschaft für Gastroenterologie, Verdauungs- und Stoffwechselkrankheiten (DGVS) – August 2021 – AWMF-Registernummer: 021-004, Zeitschrift für Gastroenterologie, 10.1055/a-1713-3941, 60, 03, (332-418), (2022).
- Laurène Parrot, Catherine Dong, Franck Carbonnel, Antoine Meyer, Systematic review with meta‐analysis: the effectiveness of either ustekinumab or vedolizumab in patients with Crohn's disease refractory to anti‐tumour necrosis factor, Alimentary Pharmacology & Therapeutics, 10.1111/apt.16714, 55, 4, (380-388), (2021).
- Javier P. Gisbert, María Chaparro, Primary Failure to an Anti-TNF Agent in Inflammatory Bowel Disease: Switch (to a Second Anti-TNF Agent) or Swap (for Another Mechanism of Action)?, Journal of Clinical Medicine, 10.3390/jcm10225318, 10, 22, (5318), (2021).