Real-world comparison of treatment patterns and effectiveness of albiglutide and liraglutide
Abstract
Aim: To compare medication adherence, discontinuation and glycemic control in patients receiving albiglutide versus liraglutide. Patients & methods: Administrative claims data and glycated hemoglobin (HbA1c) results were analyzed from a sample of adult health plan members with Type 2 diabetes. Results: Patients were matched 1:1 in the albiglutide (n = 2213) and liraglutide (n = 2213) overall cohorts and in 244 patients with HbA1c results from each treatment group. Mean HbA1c change from baseline was −1.0% for both groups. At 6 months, mean ± standard deviation adherence was 0.69 ± 0.29 versus 0.64 ± 0.29 (p < 0.001), and discontinuation was 33.2 versus 37.8% (p = 0.002) with albiglutide versus liraglutide, but these were not statistically or clinically different at 12 months. Conclusion: Similar treatment patterns and clinically meaningful reductions in HbA1c were observed for both treatments in this real-world comparison.
First draft submitted: 11 May 2017; Accepted for publication: 31 July 2017; Published online: 17 August 2017
The recommended initial treatment for Type 2 diabetes mellitus (T2DM) involves significant lifestyle adjustments, such as changes in diet and physical activity, coupled with first-line treatment with metformin [1]. For patients who are unable to achieve glycemic goals with metformin alone, one or more additional antidiabetic agents are used in later lines of treatment, including oral and injectable therapies. Agents that target glucagon-like peptide-1 (GLP-1) may be recommended among several treatment choices in the second or later lines of treatment, and they may also be used as first-line treatment in patients in whom metformin is contraindicated or not tolerated [1,2].
The GLP-1 receptor agonist albiglutide (Tanzeum®) is a once-weekly (q.w.) subcutaneous injection that was approved by the US FDA in April 2014 as an adjunct to diet and exercise to improve glycemic control in adults with T2DM [3]. The recommended initial dosage of albiglutide is 30 mg q.w., and the dosage may be increased to 50 mg q.w. if there is inadequate glycemic response [3]. Several Phase III clinical trials have compared the improvement in glycated hemoglobin (HbA1c) levels with albiglutide versus that of placebo or other antidiabetic agents in different disease settings [4–11].
Liraglutide (Victoza®) is a once daily subcutaneously injectable GLP-1 receptor agonist that was approved by the FDA in January 2010 for use in adults with T2DM [12]. Like albiglutide, liraglutide is used as an adjunct to diet and exercise to improve glycemic control. The initiating dose is 0.6 mg, followed by dose escalation after 1 week to 1.2 mg, which may be increased to 1.8 mg if needed for glycemic control [12].
The multinational HARMONY Phase III clinical trial program [4–11] evaluated albiglutide alone or in combination with commonly used T2DM treatments. The HARMONY trials demonstrated that albiglutide can reduce HbA1c levels by −0.8 to −1.0%. HARMONY 7 compared albiglutide versus liraglutide in adult patients (aged ≥18 years) with inadequately controlled T2DM [7]. In this trial, albiglutide 30 mg q.w. was titrated to 50 mg at week 6, and liraglutide 0.6 mg once daily was titrated to 1.2 mg at week 1 and to 1.8 mg at week 2. The findings from this study showed clinically relevant glycemic lowering with both albiglutide and liraglutide, but noninferiority criteria were not met for albiglutide versus liraglutide.
Medication adherence is an important component of T2DM control and treatment because it is associated with improved glycemic control, fewer diabetes-related complications, lower healthcare costs and reduced mortality [13–15]. Real-world treatment patterns for liraglutide and exenatide q.w. have been examined previously [16,17], and the results showed that adherence, as measured by proportion of days covered (PDC), was lower for liraglutide compared with exenatide q.w. A more recent study indicated that adherence rates were lower, and discontinuation rates were higher for liraglutide, albiglutide and exenatide q.w. compared with dulaglutide [18]. However, to date, there are no comparative data for albiglutide versus other GLP-1 receptor agonists, such as liraglutide, in a real-world setting. In this retrospective claims data-based observational study, we used a large US health insurance claims database to assess treatment patterns, including adherence and discontinuation rates, among patients initiating GLP-1 receptor agonist therapy with albiglutide or liraglutide during a 6-month period. In a subset of patients, we also compared glycemic control between matched cohorts of commercially insured patients with T2DM receiving albiglutide or liraglutide.
Methods
Study design & data source
This study was a retrospective database analysis using administrative claims data from the Optum Research Database (ORD) to assess the treatment patterns and effectiveness of albiglutide and liraglutide in a real-world setting. All analyses were prespecified and were conducted as per the study protocol. The ORD includes enrollment information, medical and pharmacy claims, and linked laboratory test results for approximately 14 million enrollees in US commercial health insurance plans annually. The ORD is geographically diverse and representative of the commercially insured US population. Medical claims included International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) and International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) diagnosis and procedure codes, Current Procedural Terminology codes, Healthcare Common Procedure Coding System codes, revenue codes and site of service codes. Outpatient pharmacy claims included National Drug Codes for filled prescriptions, dosage form, fill date, days’ supply, and deidentified patient and prescriber codes. Laboratory test results were available for a subset of patients in the database. Because this was a noninterventional, retrospective study analyzing a de-identified dataset, approval by an institutional review board and patient informed consent were not necessary.
Study population
The study population included adult commercial health plan members with evidence of T2DM (ICD-9-CM or ICD-10-CM diagnosis code for T2DM in any diagnosis position or evidence of oral antidiabetic drug [OAD] use) and one or more pharmacy claims for albiglutide or liraglutide between 29 July 2014 and 31 December 2015. The first fill date for albiglutide or liraglutide was the index date. Patients were required to have continuous enrollment in the health plan for 6 months (182 days) prior to the index date (baseline period) and for 6 months (182 days) following and inclusive of the index date (follow-up period). While not the focus of this manuscript, patients with 12 months of follow-up data were available and included in a subset analysis reviewing those outcomes available at 12 months. Exclusion criteria included any pharmacy claim for a GLP-1 receptor agonist during the baseline period, evidence of a medical claim for Type 1 diabetes in any diagnosis position in combination with at least one claim for insulin, and evidence of pregnancy or gestational diabetes in any diagnosis position during the baseline or follow-up periods.
To be included in the HbA1c subset analysis, patient data had to contain one or more HbA1c laboratory test results during the baseline period through the index date +7 days, and one or more HbA1c results between 30 days prior to and following the end of the 6-month follow-up period (index date +151 through index date +211 days).
Study measures
Demographics & clinical characteristics
Patient clinical characteristics were measured during the baseline period and included age in the index year, gender, geographic region, comorbidity based on the Quan–Charlson comorbidity score [19] and the Diabetes Complications Severity Index [20,21], use of OADs, use of insulin, use of pramlintide, antidiabetic therapy regimen (see below), all-cause and diabetes-related healthcare resource utilization, all-cause and diabetes-related healthcare costs, and specialty of the prescribing physician on the index pharmacy claim (defined as primary care [including obstetrics/gynecology], endocrinology, other specialty or unknown). Antidiabetic therapy regimens at baseline were categorized into the following groups: no therapy, OAD monotherapy (one OAD without insulin or other injectables), OAD combination therapy (two or more OADs without insulin or other injectables), injectable monotherapy (insulin or other injectables without OADs), or injectable with OAD combination therapy. Diabetes-related healthcare resource utilization at baseline was calculated for ambulatory visits (office and outpatient), emergency room visits and inpatient admissions. Visits were considered diabetes related if they had an ICD-9-CM or ICD-10-CM diagnosis code for diabetes in any diagnosis position. Diabetes-related costs at baseline were calculated using medical and pharmacy claims, and included both health plan payments and patient out-of-pocket payments. Costs for medical claims were considered diabetes related if they had an ICD-9-CM or ICD-10-CM diagnosis code for diabetes in any diagnosis position, and costs for pharmacy claims were considered diabetes related if they were for OADs, insulin or pramlintide. Costs were adjusted to 2015 US dollars using the annual medical care component of the Consumer Price Index [22] to reflect inflation. Baseline HbA1c level was the last measure in the baseline period through the index date + 7 days; the time between baseline HbA1c and the index date was also calculated. The valid range for HbA1c results was 3–20%.
Treatment patterns
GLP-1 receptor agonist treatment patterns were measured in the follow-up period. These included the type of GLP-1 receptor agonist initiated on the index date (albiglutide vs liraglutide), and the number of pharmacy fills for the index GLP-1 receptor agonist. Adherence, discontinuation and persistence of the index therapy were evaluated. Adherence was measured by PDC, which indicated the proportion of time over the course of treatment that a patient theoretically was in possession of the medication. The PDC was calculated using the number of days on which the index medication was available (based on days’ supply of filled prescriptions, inclusive of the index date) divided by the number of days in the follow-up period. A PDC of 0.80 or greater was defined as adherent, while a PDC of less than 0.80 was defined as nonadherent. Discontinuation of therapy was defined as a gap in therapy of the index drug of more than 60 days. The date of discontinuation was defined as the run-out date of the last prescription filled prior to the gap in therapy. Persistence on therapy was measured as the number of days to discontinuation of the index therapy. The 12-month outcomes were only available for treatment patterns.
Glycemic control
In the subset of patients included in the HbA1c analysis, follow-up HbA1c outcomes were measured as a continuous variable using the first HbA1c level test result in the period from the index date + 151 days through index date + 211 days. A categorical measure was created by grouping follow-up HbA1c level results into four groups: <7.0, 7.0 to <8.0, 8.0 to <9.0 and ≥9.0%. The time (in days) between the index date and the date of the follow-up HbA1c result was also calculated. The change in HbA1c from baseline to follow-up was calculated as the baseline HbA1c result minus the follow-up HbA1c result.
Propensity score matching
To enable comparison of outcomes between patient cohorts with similar patient characteristics, and to minimize confounding bias when estimating the effect of treatment, propensity score matching was used to match patients in the albiglutide and liraglutide cohorts [23].
Propensity scores were estimated by unconditional logistic regression analyses that incorporated potential predictors of therapy as independent variables in a regression model, with cohort (i.e., albiglutide versus liraglutide) as the outcome. The final list of variables included in the propensity score model was determined following the review of the prematching descriptive analysis of patient characteristics and other baseline measures. Covariates for the logistic regression model included index quarter and year, age, gender, geographic region, baseline comorbidity, index drug prescriber specialty, baseline diabetes-related medication (OADs, insulin and pramlintide) use, medication count (all-cause), baseline diabetes-related utilization and costs, and – in the subset of patients with HbA1c results – baseline HbA1c level.
Patients were matched in a 1:1 ratio for each comparison group (i.e., matching was conducted separately for the overall cohort and for the subset of patients with HbA1c results). A standardized difference of greater than 10% was used to indicate significant practical differences in the cohort comparison [24].
Following propensity score matching, between-cohort differences in study outcomes were analyzed using paired t-tests for continuous variables and McNemar tests for categorical variables. Statistical significance was defined as p < 0.05. Statistical analyses were performed using SAS (version 9.4, SAS Institute, Inc., NC, USA).
Results
Subject demographics & baseline characteristics
Figure 1 shows the sample selection and attrition flowchart. There were 4426 patients identified in the postmatched study sample (n = 2213 each in the albiglutide and liraglutide groups); 488 patients were included in the HbA1c subset analysis sample of patients with both baseline and follow-up HbA1c results (n = 244 each in the albiglutide and liraglutide groups; Figure 1).
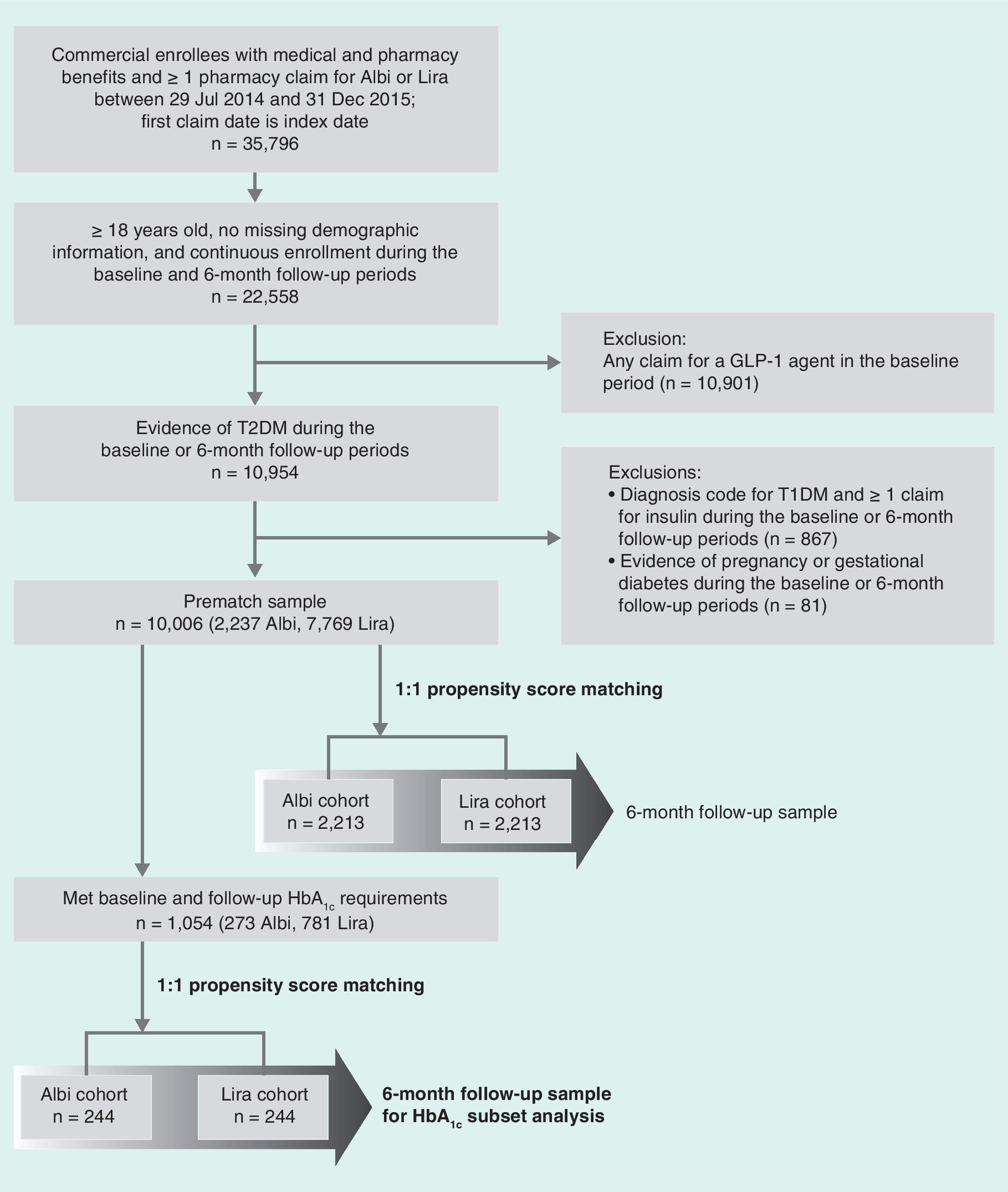
Figure 1. Sample selection and attrition flowchart.
Albi: Albiglutide; GLP-1: Glucagon-like peptide-1; HbA1c: Glycated hemoglobin; Lira: Liraglutide; T1DM: Type 1 diabetes mellitus; T2DM: Type 2 diabetes mellitus.
The propensity score-matched albiglutide and liraglutide cohorts were well balanced (a standardized difference of <10%) with respect to the key characteristics shown in Tables 1 & 2. Patient demographic characteristics are shown in Table 1. Mean patient age was approximately 52 years in the albiglutide and liraglutide cohorts, and approximately 53 years in the HbA1c subset. Both samples contained slightly higher proportions of men than women. A majority of the patients (>60%) were from the south geographic region.
| Characteristic | Postmatch full sample | Postmatch HbA1c subset analysis† | ||||
|---|---|---|---|---|---|---|
| Albi (n = 2213) | Lira (n = 2213) | Stand diff‡ (%) | Albi (n = 244) | Lira (n = 244) | Stand diff‡ (%) | |
| Age, year, mean (SD) | 52.4 (8.9) | 52.4 (9.1) | 0.50 | 53.3 (8.9) | 52.5 (9.2) | 8.46 |
| Male, n (%) | 1187 (53.6) | 1168 (52.8) | 1.72 | 131 (53.7) | 127 (52.1) | 3.28 |
| Geographic region, n (%) | ||||||
| Northeast | 85 (3.8) | 86 (3.9) | −0.23 | 8 (3.3) | 8 (3.3) | 0.00 |
| Midwest | 452 (20.4) | 476 (21.5) | −2.66 | 28 (11.5) | 30 (12.3) | −2.53 |
| South | 1417 (64.0) | 1402 (63.4) | 1.41 | 177 (72.5) | 171 (70.1) | 5.44 |
| West | 259 (11.7) | 249 (11.3) | 1.42 | 31 (12.7) | 35 (14.3) | −4.79 |
†Patients had at least one baseline and one follow-up HbA1c test result.
‡By convention, a standardized difference of less than 10% indicates that the cohorts are well matched for that variable [24].
Albi: Albiglutide; HbA1c: Glycated hemoglobin; Lira, Liraglutide; SD: Standard deviation; Stand diff: Standardized difference.
Baseline patient clinical characteristics are shown in Table 2. The majority of patients in each sample had Quan–Charlson comorbidity scores of 0, and the mean Diabetes Complications Severity Index score in each sample was <1. Approximately half of the prescribers of the index pharmacy claim were in the primary care specialty. Approximately 30% of patients used insulin in the baseline period, and most patients were on OAD-only therapy (monotherapy or oral combination therapy). In the HbA1c subset analysis sample, 16.8% of patients in the albiglutide cohort and 18.4% of patients in the liraglutide cohort had baseline HbA1c levels of less than 7.0%, while 39% of patients in both the albiglutide and liraglutide cohorts had baseline HbA1c levels of at least 9.0%.
| Baseline characteristic | Postmatch full sample | Postmatch HbA1c subset analysis† | ||||
|---|---|---|---|---|---|---|
| Albiglutide (n = 2213) | Liraglutide (n = 2213) | Stand diff‡ (%) | Albiglutide (n = 244) | Liraglutide (n = 244) | Stand diff‡ (%) | |
| Quan–Charlson comorbidity score category, n (%) | ||||||
| – 0 | 1428 (64.5) | 1399 (63.2) | 2.73 | 150 (61.5) | 152 (62.3) | −1.69 |
| – 1–2 | 662 (29.9) | 684 (30.9) | −2.16 | 76 (31.2) | 76 (31.2) | 0 |
| – 3–4 | 101 (4.6) | 108 (4.9) | −1.49 | 13 (5.3) | 12 (4.9) | 1.86 |
| – ≥5 | 22 (1.0) | 22 (1.0) | 0 | 5 (2.1) | 4 (1.6) | 3.05 |
| DCSI score, mean (SD) | 0.68 (1.1) | 0.68 (1.2) | 0.12 | 0.7 (1.2) | 0.7 (1.1) | 2.85 |
| Index provider specialty, n (%) | ||||||
| – Primary care | 1118 (50.5) | 1110 (50.2) | 0.72 | 141 (57.8) | 138 (56.6) | 2.48 |
| – Endocrinology | 565 (25.5) | 540 (24.4) | 2.61 | 53 (21.7) | 60 (24.6) | −6.80 |
| – Other | 171 (7.7) | 175 (7.9) | −0.67 | 12 (4.9) | 11 (4.5) | 1.93 |
| – Unknown | 359 (16.2) | 388 (17.5) | −3.50 | 38 (15.6) | 35 (14.3) | 3.45 |
| HbA1c, %, mean (SD) | – | – | – | 8.8 (2.0) | 8.6 (1.8) | 9.25 |
| – <7.0, n (%) | – | – | – | 41 (16.8) | 45 (18.4) | −4.30 |
| – 7.0 to <8.0, n (%) | – | – | – | 54 (22.1) | 51 (20.9) | 2.99 |
| – 8.0 to <9.0, n (%) | – | – | – | 55 (22.5) | 52 (21.3) | 2.97 |
| – ≥9.0, n (%) | – | – | – | 94 (38.5) | 96 (39.3) | −1.68 |
| Insulin use, n (%) | 680 (30.7) | 668 (30.2) | 1.18 | 71 (29.1) | 65 (26.6) | 5.49 |
| Count of OAD classes, mean (SD) | 1.6 (1.1) | 1.6 (1.1) | 0.37 | 1.7 (1.2) | 1.8 (1.2) | −1.79 |
| Antidiabetic therapy regimen, n (%) | ||||||
| – None | 261 (11.8) | 260 (11.8) | 0.14 | 25 (10.3) | 21 (8.6) | 5.61 |
| – OAD monotherapy | 452 (20.4) | 457 (20.7) | −0.56 | 44 (18.0) | 48 (19.7) | −4.19 |
| – OAD combination therapy | 820 (37.1) | 828 (37.4) | −0.75 | 104 (42.6) | 110 (45.1) | −4.96 |
| – Injectable monotherapy | 135 (6.1) | 153 (6.9) | −3.30 | 14 (5.7) | 15 (6.2) | −1.73 |
| – Injectable + OAD combination therapy | 545 (24.6) | 515 (23.3) | 3.18 | 57 (23.4) | 50 (20.5) | 6.94 |
| Diabetes-related healthcare resource utilization by visit count per patient, mean (SD) | ||||||
| – Ambulatory visits | 3.2 (2.6) | 3.3 (3.6) | −1.41 | 3.2 (2.5) | 3.2 (2.6) | 0.48 |
| – ER visits | 0.1 (0.4) | 0.1 (0.5) | −0.39 | 0.1 (0.4) | 0.2 (0.5) | −9.56 |
| – Inpatient stays | 0 (0.2) | 0 (0.2) | 0.83 | 0 (0.2) | 0 (0.2) | 0 |
| Total diabetes-related healthcare costs per patient, US dollars, mean (SD) | 2863 (7895) | 3070 (8257) | −2.56 | 2579 (5166) | 2406 (4280) | 3.64 |
†Patients had at least one baseline and one follow-up HbA1c test result.
‡By convention, a standardized difference of less than 10% indicates that the cohorts are well matched for that variable [24].
DCSI: Diabetes Complications Severity Index; ER: Emergency room; HbA1c: Glycated hemoglobin; OAD: Oral antidiabetic agent; SD: Standard deviation; Stand diff: Standardized difference.
Treatment pattern outcomes
For the 6-month follow-up treatment pattern outcomes, adherence as measured by PDC was significantly higher in the albiglutide cohort compared with the liraglutide cohort. The mean (standard deviation [SD]) PDC was 0.69 (0.29) for albiglutide versus 0.64 (0.29) for liraglutide (p < 0.001) (Table 3). A larger proportion of albiglutide initiators had a PDC of ≥0.80 compared with liraglutide initiators (48.3 vs 42.3%, respectively; p < 0.001) (Table 3). The albiglutide cohort also had a significantly higher number of index drug fills (mean 4.6 vs 3.8), longer persistence (mean 142.1 vs 134.7 days), and a lower proportion of discontinuers (33.2 vs 37.8%) versus the liraglutide cohort, respectively (all p ≤ 0.002) (Table 3). The 12-month follow-up treatment pattern outcomes were not statistically or clinically different for the albiglutide and liraglutide cohorts. Adherence mean (SD) PDC was 0.59 (0.32) for albiglutide versus 0.58 (0.32) for liraglutide; persistence was 227.6 (137.4) days for albiglutide versus 223.9 (143.8) days for liraglutide, and the proportion of discontinuers was 55.4% for albiglutide versus 54.1% for liraglutide.
| Outcome‡ | Postmatch full sample | Postmatch HbA1c subset analysis† | ||||
|---|---|---|---|---|---|---|
| Albiglutide (n = 2213) | Liraglutide (n = 2213) | p-value | Albiglutide (n = 244) | Liraglutide (n = 244) | p-value | |
| Index drug PDC, mean (SD) | 0.69 (0.29) | 0.64 (0.29) | <0.001 | 0.75 (0.25) | 0.68 (0.29) | <0.001 |
| – PDC <0.80, n (%) | 1144 (51.7) | 1277 (57.7) | <0.001 | 109 (44.7) | 131 (53.7) | 0.007 |
| – PDC ≥0.80, n (%) | 1069 (48.3) | 936 (42.3) | <0.001 | 135 (55.3) | 113 (46.3) | 0.007 |
| Number of index drug fills, mean (SD) | 4.6 (2.1) | 3.8 (2.1) | <0.001 | 5.0 (2.0) | 3.9 (2.0) | <0.001 |
| Persistence on index drug, days, mean (SD)§ | 142.1 (60.8) | 134.7 (64.7) | <0.001 | 150.2 (54.8) | 139.0 (63.2) | 0.004 |
| Discontinuation of index drug, n (%)¶ | 734 (33.2) | 836 (37.8) | 0.002 | 69 (28.3) | 85 (34.8) | 0.101 |
†Patients had at least one baseline and one follow-up HbA1c test result.
‡Dosage at baseline and follow-up was the same for the albiglutide and liraglutide cohorts.
§Persistence on therapy was measured as the number of days to discontinuation of the index therapy.
¶Discontinuation of therapy was defined as a gap in therapy of the index drug of more than 60 days.
HbA1c: Glycated hemoglobin; PDC: Proportion of days covered; SD: Standard deviation.
In the 6-month follow up, 11.7% of albiglutide initiators had only a single fill of the index drug during follow-up, compared with 18.7% of liraglutide initiators (p < 0.001) (Figure 2), and significantly more albiglutide initiators had six or more index drug fills compared with liraglutide initiators (p < 0.001). The proportions of patients using the lowest and highest dosages of either GLP-1 receptor agonist were similar. Albiglutide dosages of 30 and 50 mg, respectively, were used by 72.9 and 27.1% of patients at index and by 55.7 and 44.3% at last dose; liraglutide 0.6/1.2 and 1.8 mg dosages, respectively, were used by 73.1 and 26.9% of patients at index and by 54.4 and 45.6% at last dose. Adherence and persistence findings were similar for the subset of patients with baseline and follow-up HbA1c level test results (p ≤ 0.007) and except that the proportion of discontinuations was not significantly different between the albiglutide and liraglutide cohorts (p = 0.101) (Table 3).
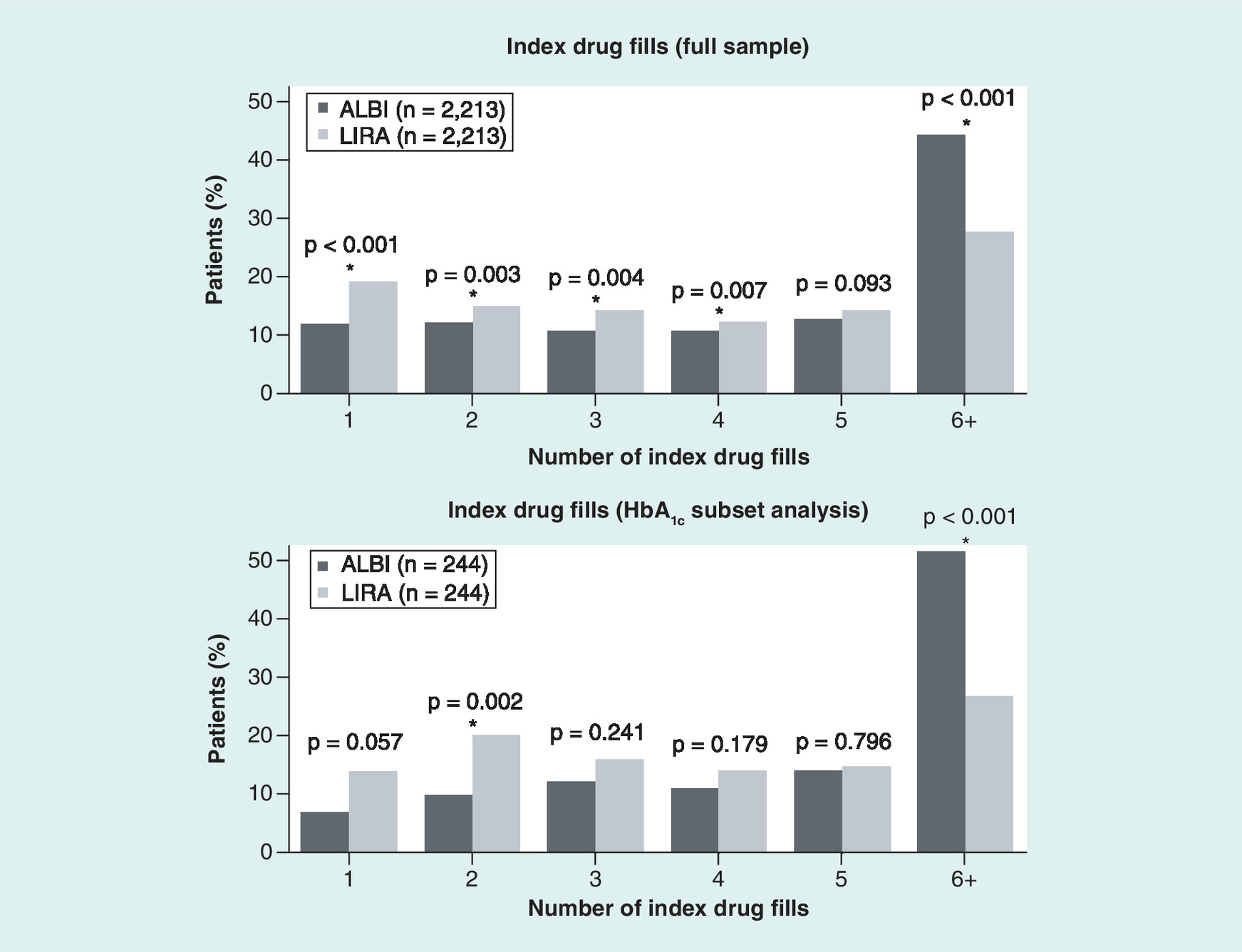
Figure 2. Index drug fills.
ALBI: Albiglutide; HbA1c: Glycated hemoglobin; LIRA: Liraglutide.
HbA1c outcomes
During the 6-month follow-up period, 36.5% of albiglutide initiators and 39.3% of liraglutide initiators achieved a glycemic target of HbA1c <7.0% (Figure 3 & Table 4), compared with 16.8 and 18.4% of patients, respectively, who had this HbA1c level at baseline. On the other hand, over 18.0% of patients in both cohorts had HbA1c levels that met or exceeded 9.0% in the follow-up period. The results for albiglutide and liraglutide were similar across the HbA1c strata. For both cohorts, the mean HbA1c change from baseline was −1.0%. The differences between the albiglutide and liraglutide cohorts in mean follow-up HbA1c, follow-up HbA1c distribution and mean change in HbA1c were not statistically significant, as shown in Table 4.
| Outcome | Albiglutide (n = 244) | Liraglutide (n = 244) | p-value |
|---|---|---|---|
| Follow-up HbA1c level, %, mean (SD) | 7.8 (1.7) | 7.6 (1.5) | 0.276 |
| – <7.0, n (%) | 89 (36.5) | 96 (39.3) | 0.500 |
| – 7.0 to <8.0, n (%) | 68 (27.9) | 57 (23.4) | 0.113 |
| – 8.0 to <9.0, n (%) | 38 (15.6) | 47 (19.3) | 0.230 |
| – ≥9.0, n (%) | 49 (20.1) | 44 (18.0) | 0.498 |
| Change from baseline in HbA1c, mean (SD) | −1.0 (1.7) | −1.0 (1.6) | 0.847 |
HbA1c: Glycated hemoglobin; PDC, Proportion of days covered; SD: Standard deviation.
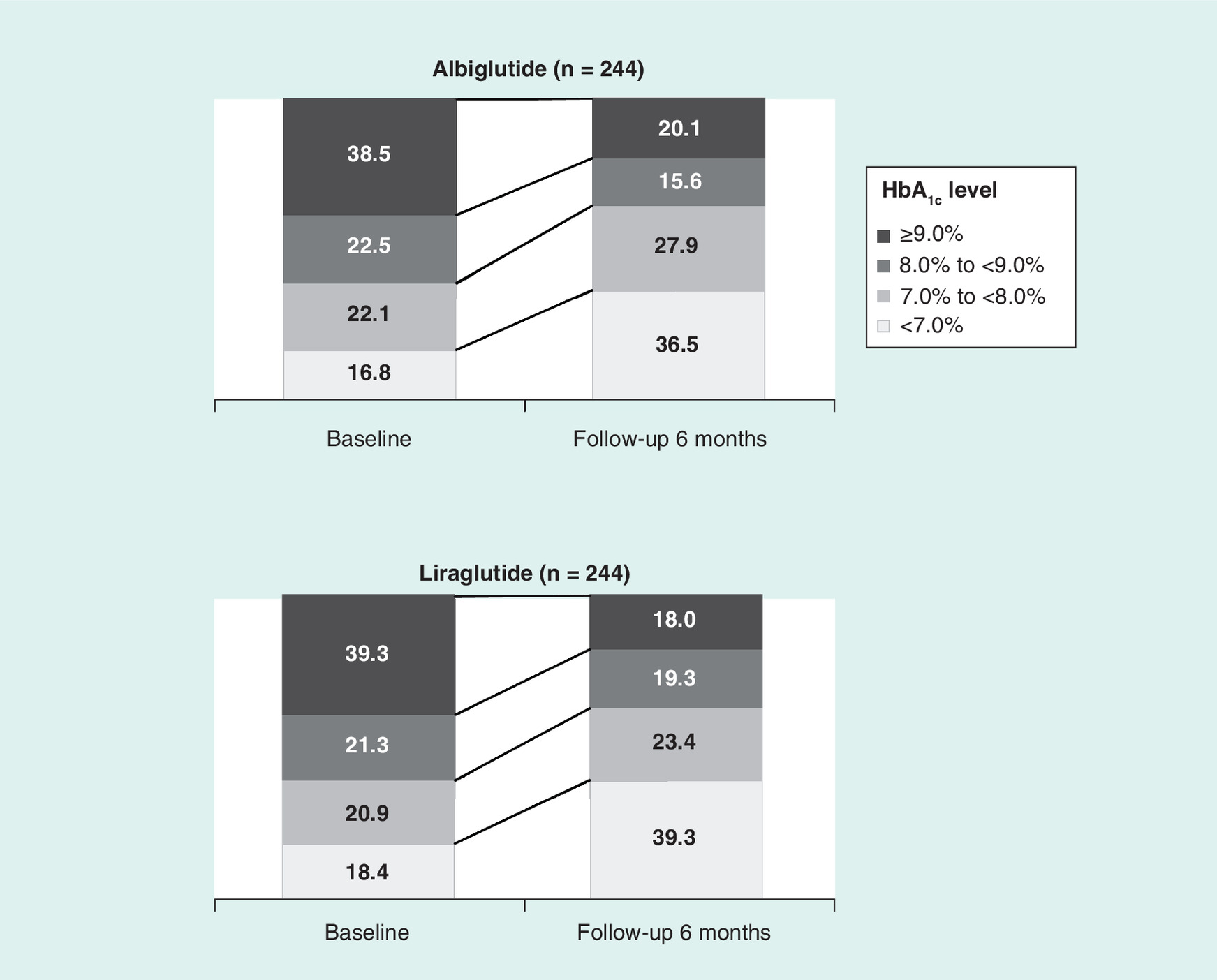
Figure 3. Distribution of baseline and follow-up glycated hemoglobin levels.
HbA1c: Glycated hemoglobin.
Discussion
The present study evaluated treatment patterns among patients with T2DM initiating albiglutide versus liraglutide in the first real-world comparison of albiglutide with another GLP-1 receptor agonist (liraglutide). After 6 months of follow-up, the albiglutide initiators cohort had higher adherence rates, longer persistence and lower discontinuation rates compared with the liraglutide initiators cohort. One of the key findings was that both the albiglutide and liraglutide cohorts had a clinically meaningful −1% change from baseline in HbA1c levels; these findings were within the ranges of HbA1c changes from baseline observed in a head-to-head clinical trial comparing albiglutide with liraglutide (HARMONY 7) [7].
The goal of diabetes treatment is to maintain blood glucose at normal levels to reduce the risk of diabetes complications, and HbA1c level is a particularly strong predictor for diabetes complications [25,26]. Each 1% reduction in HbA1c level is associated with a 37% decreased risk for microvascular complications and a 21% decreased risk for any end point or death related to diabetes [26]. The HARMONY 7 trial assessed HbA1c change from baseline to week 32 for albiglutide and liraglutide. The mean change in HbA1c was −0.78% (95% CI: −0.87 to −0.69) in the albiglutide group and −0.99% (95% CI: −1.08 to −0.90) in the liraglutide group. The criteria for noninferiority of albiglutide versus liraglutide were not met [7]. In a real-world analysis, our finding in the subset analysis of patients with baseline and follow-up HbA1c test results showed a −1.0% mean change in HbA1c in both the albiglutide and liraglutide cohorts. This finding was also similar to that observed in another real-world analysis of liraglutide (HbA1c change from baseline −1.08% [27]) during a postindex period of the same duration. The differences in HbA1c outcomes between the albiglutide and liraglutide cohorts after 6 months of follow-up were not significantly different in this study.
Medication adherence is an important consideration in making treatment decisions for patients with T2DM, as better adherence is associated with greater reductions in HbA1c levels, improved clinical outcomes and lower healthcare costs [13,14]. In the present study, we found that adherence rates, as measured by PDC values, were statistically significantly higher for albiglutide (PDC 0.69) compared with liraglutide (PDC 0.64) at 6 months. However, this difference may not be clinically meaningful because the statistically significant differences observed at 6 months were not observed at 12 months. Although it may be difficult to compare adherence outcomes between studies because of differences in methodology, our findings were in agreement with real-world analyses of other GLP-1 receptor agonists. A retrospective cohort study using US insurance claims data showed that over a 6-month period after initiation of GLP-1 receptor agonists, the exenatide q.w. cohort had slightly greater adherence compared with the liraglutide cohort (mean PDC 0.68 for exenatide q.w. vs 0.67 for liraglutide) [16]. Yu et al. [17] also reported a PDC of approximately 0.69 for both liraglutide and exenatide q.w. over a 6-month follow-up period using US insurance claims data [17]. A recent study using Truven Health MarketScan Research Databases and the Medicare Supplemental and Coordination of Benefits Databases found that adherence as measured by mean PDC was 0.67 for liraglutide and 0.61 for exenatide q.w. versus approximately 0.70 for dulaglutide during a 6-month postindex period [18]. In that study, the odds ratio for adherence to albiglutide compared with dulaglutide was 0.63 (95% CI: 0.55–0.73), while it was 0.65 (95% CI: 0.49–0.71) for liraglutide compared with dulaglutide [18]. However, there are at least three important differences between the study by Alatorre et al. [18] and the present study: first, the main focus of the study by Alatorre et al. was on dulaglutide, exenatide q.w. and liraglutide, whereas the focus of the present study was on albiglutide and liraglutide because, at the time our study was conducted, the only GLP-1 receptor agonists that were tier 2 co-preferred with the same copay were albiglutide and liraglutide. Exenatide was at the tier 3 copay level, and dulaglutide was not on the health insurance plans’ formularies at the time of our study. Second, Alatorre et al. did not assess HbA1c outcomes, whereas our analysis included follow-up HbA1c outcomes in a subset of patients with data available. Third, Alatorre et al. used data from Truven Health's MarketScan Research Databases, which included Medicare patients, whereas the present study included patients from commercial health insurance plans only, and no Medicare patients were included.
It is worth noting that because both groups of patients in our study were in a tier 2 co-preferred status for most plans included in the study database, their out-of-pocket costs for albiglutide versus liraglutide were similar; therefore, it is unlikely that cost affected adherence rates. We also found that significantly fewer albiglutide initiators had only a single fill of the index drug during the follow-up period compared with liraglutide initiators, and there was a lower discontinuation rate in the albiglutide cohort compared with the liraglutide cohort. A recent meta-analysis also found that patients using albiglutide had the lowest treatment discontinuation rates of patients using all currently available GLP-1 receptor agonists [28]. However, Alatorre et al. [18] recently reported lower discontinuation rates for patients using dulaglutide over a 6-month postindex period compared with those using albiglutide, exenatide q.w. and liraglutide [18]. Although the reasons for the differences in the rates of adherence, persistence and discontinuation between cohorts are unknown, it is possible that differences in side effects, dosing schedules, gastrointestinal tolerability, medication costs or patient preference may have contributed to the observed treatment patterns. Future research is warranted to explore the reasons for discontinuation of or nonadherence to GLP-1 receptor agonist therapy.
The main strength of the present study is that it contributes important real-world data to the existing evidence supporting the use of albiglutide for improving glycemic control among patients with T2DM. Our findings also suggest the need for additional comparative studies of outcomes associated with albiglutide versus other GLP-1 receptor agonists, as well as other classes of antidiabetic therapies.
The results of this study should be interpreted in light of several limitations common to claims-based analyses. First, the presence of a claim for a filled prescription does not indicate that the medication was consumed or that it was administered as prescribed, and medications filled over the counter or provided as samples by a physician are not included in claims data. Furthermore, we assessed whether or not the medications were being prescribed and refilled as indicated in the prescribing information. This analysis was based on adjudicated prescription claims data. Thus, we do not know how the patient was using the drug or whether it was used off-label. Also, this analysis looked specifically at the intent-to-treat use of albiglutide and liraglutide. Thus, patients may have switched or augmented their treatments with other therapies during the follow-up period. We controlled for baseline diabetes-related medication use (OADs, insulin and pramlintide) during the propensity score matching process. Second, the presence of a diagnosis code on a medical claim does not prove the presence of disease, as diagnoses may be incorrectly coded or included as rule-out criteria. It should be noted, however, that the potential for disease misidentification was minimized in this study by the requirement that patients have pharmacy claims for medications expressly indicated to treat T2DM. Furthermore, we evaluated a focused set of outcomes and did not examine healthcare resource utilization, costs, concomitant medications or other changes in characteristics that could have changed over the course of the study. We also could not account for patient use of coupons that may lower costs and impact medication use patterns because this information was not available in the database. Additional limitations are that HbA1c results were available for only a subset of the patient population and may have been incomplete for those patients who did have results. Also, only HbA1c results obtained from laboratory testing conducted at a central laboratory during a patient visit were available for analysis; those obtained in a physician's office or otherwise not processed by a laboratory for which data were submitted were not included in the laboratory results data. Because of these limitations, the HbA1c subset analysis may not be a complete representation of HbA1c outcomes in this patient population. It is also possible that the requirement of HbA1c results from specific time windows (i.e., the baseline and follow-up periods) created a selection bias by restricting the HbA1c analysis to patients who visit their physicians more frequently or on a reliable schedule. Furthermore, the results of paired t-tests may have been biased if the likelihood of a patient having missing HbA1c data was not random. Finally, because this study was conducted in a commercial managed care population, the results may not be generalizable to other populations, such as patients who are uninsured or enrolled in Medicare.
Conclusion
In this first real-world comparison of patients with T2DM initiating treatment with albiglutide versus liraglutide, adherence, persistence and discontinuation rates were similar for albiglutide and liraglutide initiators after 12 months. In a subset of patients with baseline and 6-month follow-up HbA1c test results, HbA1c levels did not differ between cohorts, with both cohorts achieving −1% change from baseline in HbA1c values. Because randomized clinical trials may not necessarily reflect the real-world use of GLP-1 receptor agonists, here we provide real-world evidence to support the use of albiglutide for improving glycemic control among patients with T2DM. Our findings suggest the need for additional comparative studies of outcomes associated with albiglutide versus other GLP-1 receptor agonists, as well as versus other classes of antidiabetic therapies.
The glucagon-like peptide-1 (GLP-1) receptor agonist albiglutide is a once-weekly subcutaneous injection used as an adjunct to diet and exercise to improve glycemic control in adults with Type 2 diabetes mellitus (T2DM).
There are no real-world comparative data for albiglutide versus other GLP-1 receptor agonists in T2DM patients.
The goals were to determine treatment patterns and compare glycemic control in patients with T2DM receiving albiglutide versus the GLP-1 receptor agonist liraglutide based on data from a US health insurer.
Baseline characteristics including comorbidity, glycated hemoglobin (HbA1c), insulin use and antidiabetic regimens were well balanced using propensity score matching methods.
Both albiglutide and liraglutide were associated with similar and clinically meaningful −1% change from baseline in HbA1c levels.
The real-world HbA1c findings were within the ranges of HbA1c changes from baseline observed in the HARMONY 7 clinical trial.
Although albiglutide users had significantly higher adherence rates and lower discontinuation rates than liraglutide users after 6 months, this difference was not maintained to 12 months.
This study provides real-world evidence of generally similar treatment patterns and improvement of glycemic control in patients with T2DM using albiglutide or liraglutide.
Acknowledgements
Authorship: All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval to the version to be published.
Data availability: A redacted report of aggregate data for the current study will be posted on GSK's Clinical Trial Registry (www.gskclinicalstudyregister.com/study/207267?search=study&#ps).
Financial & competing interests disclosure
Funding for this study and article processing charges were provided by GlaxoSmithKline. M Sikirica, A Joshi and M Bogart are employees of and stockholders in GlaxoSmithKline. E Buysman, SW Thayer and M DuCharme are employees of Optum, which received funding from GlaxoSmithKline in relation to this work. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing and editorial assistance in the preparation of this manuscript was provided by G Bijur and N Price of AOIC, LLC. Support for this assistance was funded by GlaxoSmithKline.
Ethical conduct of research
Because this was a noninterventional, retrospective study, and the analysis was of a deidentified dataset, approval from an institutional review board and patient informed consent were not necessary.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Inzucchi SE, Bergenstal RM, Buse JB et al. Management of hyperglycemia in Type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 38(1), 140–149 (2015).
2.
Harris KB, McCarty DJ. Efficacy and tolerability of glucagon-like peptide-1 receptor agonists in patients with Type 2 diabetes mellitus. Ther. Adv. Endocrinol. Metab. 6(1), 3–18 (2015).
3.
TANZEUM (Albiglutide) Prescribing Information. GlaxoSmithKline, DE, USA (2016). www.gsksource.com/pharma/content/dam/GlaxoSmithKline/US/en/Prescribing_Information/Tanzeum/pdf/TANZEUM-PI-MG-IFU-COMBINED.PDF.
4.
Home PD, Shamanna P, Stewart M et al. Efficacy and tolerability of albiglutide versus placebo or pioglitazone over 1 year in people with Type 2 diabetes currently taking metformin and glimepiride: HARMONY 5. Diabetes Obes. Metab. 17(2), 179–187 (2015).
5.
Ahrén B, Johnson SL, Stewart M et al. HARMONY 3 Study Group. HARMONY 3: 104-week randomized, double-blind, placebo- and active-controlled trial assessing the efficacy and safety of albiglutide compared with placebo, sitagliptin, and glimepiride in patients with Type 2 diabetes taking metformin. Diabetes Care 37(8), 2141–2148 (2014).
6.
Weissman PN, Carr MC, Ye J et al. HARMONY 4: randomised clinical trial comparing once-weekly albiglutide and insulin glargine in patients with Type 2 diabetes inadequately controlled with metformin with or without sulfonylurea. Diabetologia 57(12), 2475–2484 (2014).
7.
Pratley RE, Nauck MA, Barnett AH et al. Once-weekly albiglutide versus once daily liraglutide in patients with Type 2 diabetes inadequately controlled on oral drugs (HARMONY 7): a randomised, open-label, multicentre, non-inferiority Phase III study. Lancet Diabetes Endocrinol. 2(4), 289–297 (2014).
•• HARMONY 7 was a noninferiority Phase III clinical trial comparing albiglutide versus liraglutide in Type 2 diabetes mellitus (T2DM) patients.
8.
Rosenstock J, Fonseca VA, Gross JL et al. Advancing basal insulin replacement in Type 2 diabetes inadequately controlled with insulin glargine plus oral agents: a comparison of adding albiglutide, a weekly GLP-1 receptor agonist, versus thrice-daily prandial insulin lispro. Diabetes Care 37(8), 2317–2325 (2014).
9.
Nauck MA, Stewart MW, Perkins C et al. Efficacy and safety of once-weekly GLP-1 receptor agonist albiglutide (HARMONY 2): 52 week primary endpoint results from a randomised, placebo-controlled trial in patients with Type 2 diabetes mellitus inadequately controlled with diet and exercise. Diabetologia 59(2), 266–274 (2016).
10.
Reusch J, Stewart MW, Perkins CM et al. Efficacy and safety of once-weekly glucagon-like peptide 1 receptor agonist albiglutide (HARMONY 1 trial): 52-week primary endpoint results from a randomized, double-blind, placebo-controlled trial in patients with Type 2 diabetes mellitus not controlled on pioglitazone, with or without metformin. Diabetes Obes. Metab. 16(12), 1257–1264 (2014).
11.
Leiter LA, Carr MC, Stewart M et al. Efficacy and safety of the once-weekly GLP-1 receptor agonist albiglutide versus sitagliptin in patients with Type 2 diabetes and renal impairment: a randomized Phase III study. Diabetes Care 37(10), 2723–2730 (2014).
12.
Victoza (Liraglutide) Prescribing Information. Novo Nordisk A/S, Bagsvaerd, Denmark (2015). www.accessdata.fda.gov/drugsatfda_docs/label/2016/022341s025lbl.pdf.
13.
Wild H. The economic rationale for adherence in the treatment of Type 2 diabetes mellitus. Am. J. Manag. Care 18(3 Suppl.), S43–S48 (2012).
14.
Jha AK, Aubert RE, Yao J, Teagarden JR, Epstein RS. Greater adherence to diabetes drugs is linked to less hospital use and could save nearly $5 billion annually. Health Aff. (Millwood) 31(8), 1836–1846 (2012).
• This analysis showed that improved medicine adherence among T2DM patients resulted in significant healthcare cost reduction.
15.
Asche C, LaFleur J, Conner C. A review of diabetes treatment adherence and the association with clinical and economic outcomes. Clin. Ther. 33(1), 74–109 (2011).
16.
Johnston SS, Nguyen H, Felber E et al. Retrospective study of adherence to glucagon-like peptide-1 receptor agonist therapy in patients with Type 2 diabetes mellitus in the United States. Adv. Ther. 31(11), 1119–1133 (2014).
• Used US administrative claims data comparing adherence in T2DM patients initiating exenatide once-weekly (q.w.), exenatide two-times a day (b.i.d.), or once daily liraglutide.
17.
Yu M, Xie J, Fernandez Lando L, Kabul S, Swindle RW. Liraglutide versus exenatide once weekly: persistence, adherence, and early discontinuation. Clin. Ther. 38(1), 149–160 (2016).
• Examined real-world comparisons of adherence and persistence in T2DM patients initiating liraglutide or exenatide (q.w. or b.i.d.) using U.S. insurance claims data.
18.
Alatorre C, Fernández Landó L, Yu M et al. Treatment patterns in patients with Type 2 diabetes mellitus treated with glucagon-like peptide-1 receptor agonists: higher adherence and persistence with dulaglutide compared with once-weekly exenatide and liraglutide. Diabetes Obes. Metab. 19(7), 953–961 (2017).
•• Compared adherence, persistence and treatment patterns among T2DM patients initiating dulaglutide, liraglutide, exenatide (q.w. or b.i.d.) or albiglutide.
19.
Quan H, Li B, Couris CM et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 173(6), 676–682 (2011).
20.
Young BA, Lin E, Von Korff M et al. Diabetes complications severity index and risk of mortality, hospitalization, and healthcare utilization. Am. J. Manag. Care 14(1), 15–23 (2008).
21.
Chang HY, Weiner JP, Richards TM, Bleich SN, Segal JB. Predicting costs with diabetes complications severity index in claims data. Am. J. Manag. Care 18(4), 213–219 (2012).
22.
Bureau of Labor Statistics. Chained Consumer Price Index. Medical Care. Series ID: SUUR0000SAM. United States Department of Labor (2017). https://data.bls.gov/cgi-bin/surveymost?su.
23.
Rosenbaum PR, Rubin DB. The central role of the propensity score in observational studies for causal effects. Biometrika 70(1), 41–55 (1983).
24.
Normand ST, Landrum MB, Guadagnoli E et al. Validating recommendations for coronary angiography following acute myocardial infarction in the elderly: a matched analysis using propensity scores. J. Clin. Epidemiol. 54(4), 387–398 (2001).
25.
Albers JW, Herman WH, Pop-Busui R et al. Effect of prior intensive insulin treatment during the Diabetes Control and Complications Trial (DCCT) on peripheral neuropathy in Type 1 diabetes during the Epidemiology of Diabetes Interventions and Complications (EDIC) Study. Diabetes Care 33(5), 1090–1096 (2010).
26.
Stratton IM, Adler AI, Neil HA et al. Association of glycaemia with macrovascular and microvascular complications of Type 2 diabetes (UKPDS 35): prospective observational study. BMJ 321(7258), 405–412 (2000).
• Evaluated the relationship between glycated hemoglobin levels and the risk of macrovascular or microvascular complications in T2DM patients.
27.
Lee WC, Dekoven M, Bouchard J, Massoudi M, Langer J. Improved real-world glycaemic outcomes with liraglutide versus other incretin-based therapies in Type 2 diabetes. Diabetes Obes. Metab. 16(9), 819–826 (2014).
• Showed that real-world analysis of liraglutide glycated hemoglobin change from baseline was -1.08%, which was equivalent to the finding in the present study.
28.
Li Z, Zhang Y, Quan X et al. Efficacy and acceptability of glycemic control of glucagon-like peptide-1 receptor agonists among Type 2 diabetes: a systematic review and network meta-analysis. PLoS ONE 11(5), e0154206 (2016).
Information & Authors
Information
Published In
Copyright
© 2018 Erin Buysman.
History
Published online: 17 August 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Real-world comparison of treatment patterns and effectiveness of albiglutide and liraglutide. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0032
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Xi Tan, Brenna L. Brady, Lin Xie, Yurek Paprocki, Healthcare Resource Utilization and Costs in Individuals Who Discontinue Liraglutide and Who Switch from Liraglutide to Once-Weekly Injectable Semaglutide, Diabetes Therapy, 10.1007/s13300-025-01741-8, 16, 7, (1417-1433), (2025).
- A.B.M. Kamrul-Hasan, Deep Dutta, Lakshmi Nagendra, Saptarshi Bhattacharya, Rajiv Singla, Sanjay Kalra, Efficacy and safety of albiglutide, a once-weekly glucagon-like peptide-1 receptor agonist, in patients with type 2 diabetes: A systematic review and meta-analysis, Medicine, 10.1097/MD.0000000000038568, 103, 25, (e38568), (2024).
- Humaira Hussein, Clareece R. Nevill, Anna Meffen, Keith R. Abrams, Sylwia Bujkiewicz, Alex J. Sutton, Laura J. Gray, Double-counting of populations in evidence synthesis in public health: a call for awareness and future methodological development, BMC Public Health, 10.1186/s12889-022-14213-6, 22, 1, (2022).
- Erin R. Weeda, Alyssa K. Muraoka, Matthew D. Brock, Jessica M. Cannon, Medication adherence to injectable glucagon‐like peptide‐1 (GLP‐1) receptor agonists dosed once weekly vs once daily in patients with type 2 diabetes: A meta‐analysis, International Journal of Clinical Practice, 10.1111/ijcp.14060, 75, 9, (2021).