Efficacy and safety of ustekinumab in the induction therapy of TNF-α-refractory Crohn's disease patients: a systematic review and meta-analysis
Abstract
Aim: The aim of the systematic review and meta-analysis was to assess the efficacy and safety of ustekinumab in the induction therapy of anti-TNF-α failure patients with Crohn's disease. Methods: A systematic literature search was conducted in Medline (PubMed), EMBASE, Cochrane Library until 30 December 2016. We included randomized controlled trials that compared efficacy (clinical response and remission) and safety profile of ustekinumab in TNF-α failure Crohn's disease patients; primary and secondary TNF-α nonresponders or intolerant patients were also assessed. Included studies were critically appraised according to the PRISMA statement protocol; data aggregation with a RevMan® software was performed. Results: Three randomized controlled trials were revealed in the systematic review but only two of them (CERTIFI and UNITI-1) were homogenous to be included in the meta-analysis; aggregation of data only for induction phase of therapy was possible. Clinical response was significantly higher for patients who received ustekinumab compared with placebo patients in a group of TNF-α antagonist failure patients (relative benefit [RB] = 1.62; 95% CI: 1.28–2.04) and in the following subgroups: secondary nonresponders (RB = 1.98; 95% CI: 1.49–2.63), intolerant patients (RB = 1.47; 95% CI: 1.01–2.13) and patients who failed at least two TNF-α antagonists (RB = 2.19; 95% CI: 1.53–3.14) but in case of primary nonresponders it occurred insignificant (RB = 1.22; 95% CI: 0.76–1.98). The clinical remission in TNF-α antagonist failure population was significantly higher for patients who received ustekinumab compared with placebo (RB = 1.72; 95% CI: 1.17–2.53). Pooled analysis revealed that risk of adverse events in induction phase of therapy was not significantly different (risk ratio = 0.96; 95% CI: 0.86–1.06) between ustekinumab and placebo groups. Conclusion: The clinical response was significantly higher for TNF-α antagonist failure patients who received ustekinumab as well as in subgroups of secondary nonresponders or intolerant patients but not in case of primary nonresponders. Ustekinumab occurred as safe as placebo in the induction as well as in a maintenance phase of therapy.
First draft submitted: 30 March 2017; Accepted for publication: 12 May 2017; Published online: 29 June 2017
Crohn's disease (CD) is an immune disorder with multiple predisposing factors and an unknown causative agent. The number of new cases of CD in the USA is estimated at 33,000 per year [1], while in Europe epidemiological studies report even higher values: 53,000 [2]. Available data indicate that CD impairs health-related quality of life but is also associated with substantial direct and indirect costs across the patient's lifespan [3].
Initial therapy usually consists of 5-aminosalycilate compounds (e.g., mesalazine), systemic corticosteroids, topical corticosteroids (e.g., budesonide) and immunomodulators (e.g., methotrexate, thiopurines). In some patients insufficient control of the disease or substantial adverse events (AEs) necessitate the use of biologic therapy including TNF-α inhibitors: infliximab, adalimumab, certolizumab pegol or golimumab, but also biologics with a different mechanism of action such as vedolizumab and ustekinumab.
TNF-α antagonists are standard drugs used in biologic therapy of CD. They have been shown to be effective in the treatment of CD by improving patients’ quality of life and reducing the rate of hospitalizations and surgeries [4]. However, around 10–30% of patients are refractory to the initial anti-TNF-α therapy (primary nonresponse), and 23–46% of patients lose response over time and require a switch to another treatment or dose escalation (secondary nonresponse) [4]. Primary nonresponders are often unlikely to benefit from another TNF-α antagonist, while patients with secondary nonresponse who switch to another TNF-α antagonist are less likely to respond than patients naive to TNF-α antagonist therapy [5]. This constitutes a significant clinical problem because the benefit of alternative anti-TNF-α therapy may be limited for such patients and biologics with different mechanisms of action (e.g., ustekinumab or vedolizumab) seem to be necessary for effective treatment.
In September 2016 the US FDA, and in November 2016 the European Commission (EC), approved the use of ustekinumab (Stelara®) for the treatment of adult patients with moderately to severely active CD who had an inadequate response, lost response, or were intolerant to either conventional or TNF-α antagonist therapy or had medical contraindications to such therapies [6]. Ustekinumab is a human monoclonal antibody targeting the IL-12/23 p40 subunit, thus inhibiting the activity of both interleukins known to play a key role in inflammatory and immune responses. It is indicated for the treatment of adult patients with moderately to severely active CD. Induction of therapy with an intravenous dose of 6 mg/kg of ustekinumab, followed at week 8 by the first subcutaneous administration of 90 mg, has been authorized by the FDA and EC; dosing every 12 weeks is recommended [6].
The aim of this systematic review and meta-analysis was to examine the efficacy and safety of ustekinumab, compared with placebo, for the treatment of patients with CD who fail to respond to TNF-α antagonist therapy. Additional analyzes were performed in the subgroups of CD patients classified according to failure in response to TNF-α antagonist therapy: primary nonresponders, secondary nonresponders, intolerant patients and those who failed to respond to at least two TNF-α antagonists.
Methods
Literature search strategy
The search strategy was based on the medical subject heading MeSH terms and EMTREE combined with Boole's logical operators (Table 1). The systematic literature review was conducted using the main electronic databases: Medline via PubMed, Embase and the Cochrane Central Register of Controlled Trials (CENTRAL), until 30 December, 2016. Medline via PubMed and Embase databases as well as The Cochrane Database of Systematic Reviews were also searched for review articles. Additional relevant studies were identified by searching websites of the British Society of Gastroenterology and the European Crohn's and Colitis Organization.
| MeSH subject headings | Keywords (combined with Boole's logical operator, OR) |
|---|---|
| Medical condition | Crohn disease OR Crohn's disease OR Crohns disease OR Crohn's enteritis OR regional enteritis OR granulomatous enteritis OR Ileocolitis OR granulomatous colitis OR terminal Ileitis OR regional ileitides OR regional ileitis OR regional enterocolitis OR cleron disease OR enteritis regionalis OR morbus Crohn |
| Intervention | ustekinumab OR Stelara® OR cnto-1275 OR cnto 1275 OR cnto1275 OR 1275, CNTO |
| Methodological limits | PubMed: Humans, Randomized Controlled Trial, Clinical Trial, Controlled Clinical Trial; |
| EMBASE: Humans, Controlled Clinical Trials, Randomized Controlled Trial, Embase only; | |
| Cochrane Central Register of Controlled Trials: No limits applied; word varia-tions have been searched | |
| Language limits | PubMed, EMBASE: English |
Last updated: 30 December 2016.
Selection criteria
Studies were identified using the search strategy by two independent reviewers (P Kawalec and P Moćko). When there was uncertainty regarding eligibility, a third reviewer was consulted (I Malinowska-Lipien). Study selection was based on the title and abstract, and if necessary, full-text articles. References of identified studies were hand searched for other relevant studies. All eligible randomized controlled trials (RCT) were critically appraised and analyzed according to the PRISMA Statement protocol [7]. Studies were selected for inclusion in this analysis based on the following criteria: the intervention evaluated was ustekinumab; patients treated for CD; and RCT. Results from nonrandomized or uncontrolled else open-label studies were not incorporated into dataset. Full-text articles were included if they contain required information about study population, treatment regimen and necessary data. Abstracts or posters after screening were excluded. The reference lists of included studies and review articles were screened to identify additional eligible studies.
Data extraction
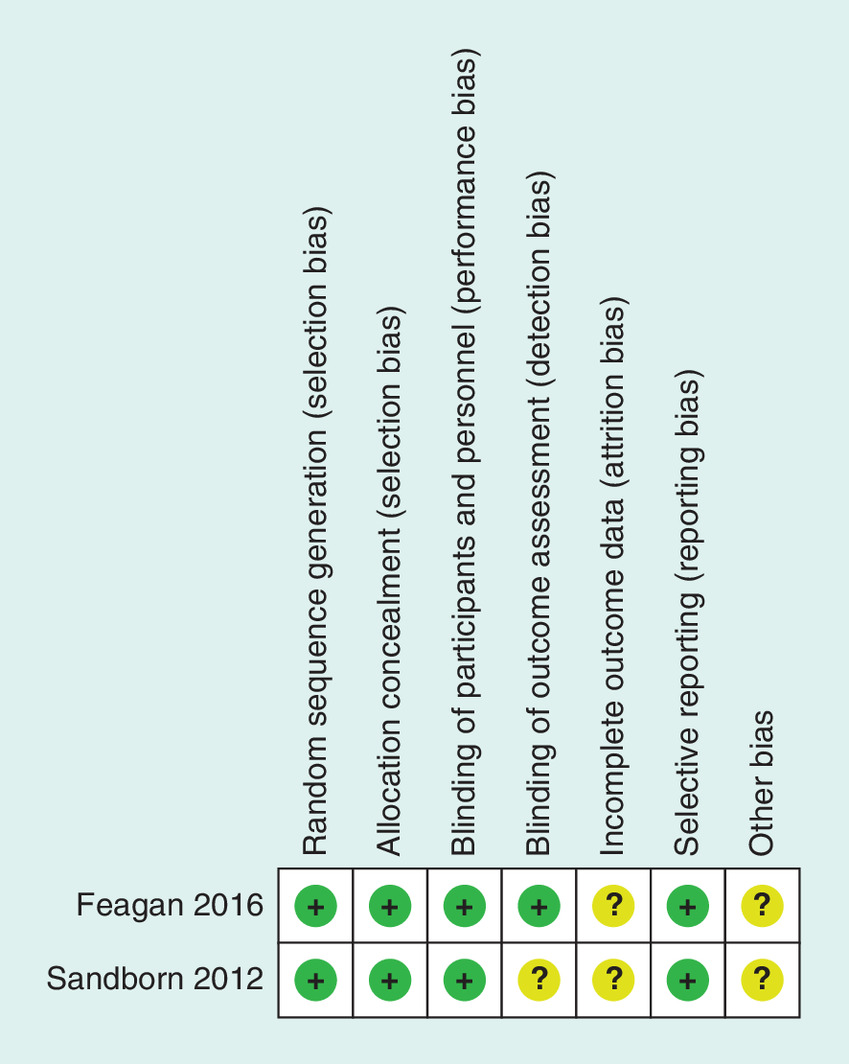
Data were also extracted using predefined data extraction forms by two independent reviewers. The following data were extracted from studies that met the inclusion criteria: characteristics of participants, intervention and regimen details, clinical end points, follow-up period and study design. For the efficacy analysis, data on clinical response and clinical remission were extracted. The safety analysis included the following data: any AEs, any serious AEs as well as risk of: arthralgia, headache, nausea, nasopharyngitis, abdominal pain, infusion or injection-site reactions, serious infections. The methodological quality of eligible RCTs was assessed using the Cochrane Collaboration's recommended tool for assessing risk of bias – domain-based evaluation. In assessing the risk of bias, ‘+’ is granted in the case of low risk of bias, ‘-’ indicates a high risk of bias, while the ‘?’ is unclear risk of bias [8].
Data analysis
Data were analyzed using intention-to-treat results from the included studies. The influence of intervention was expressed as a relative benefit (RB; described as risk ratio [RR]) on the graphs presented due to specific labeling of effect measurement in the statistical analysis software to the positive outcomes (clinical response; clinical remission) or a RR to the negative outcomes (the other analyzed end points), respectively. Meta-analysis was performed only for homogeneous data determined by degree of clinical and statistical heterogeneity. Clinical heterogeneity was assessed on the basis of characteristics of the included studies, whereas the statistical heterogeneity of the trial results was evaluated using the Chi2 test and the I2 test. Heterogeneity of study results was considered statistically significant at p < 0.1, and then the random-effects model was used, while at p ≥ 0.1 the fixed-effects model was applied. The analysis used a conservative approach, in which the value of the Chi2 test (p-value) below the threshold of 0.1 (the value of the low sensitivity of the test) indicates that differences are not accidental. For other calculations statistical significance was defined at p < 0.05. We performed a meta-analysis and all statistical tests and created forest plots using Review Manager 5.3 software. The graphic presentation of meta-analyzes applied forest plots on which the squares marked results of individual studies with the horizontal lines represent confidence interval and rhombus indicates the results of all studies pooled (meta-analysis).
Results
Description & quality of included studies
Results of the systematic review of medical databases were summarized in Figure 1. A total of 66 potentially relevant publications were identified in the literature search, 44 publications were excluded after the screening of titles and abstracts and 15 of them were removed on the basis of full-text papers; in case of remaining seven publications, duplicates were removed thus three publications for three RCTs [9–11] were finally included in the systemic review and considered for meta-analysis.
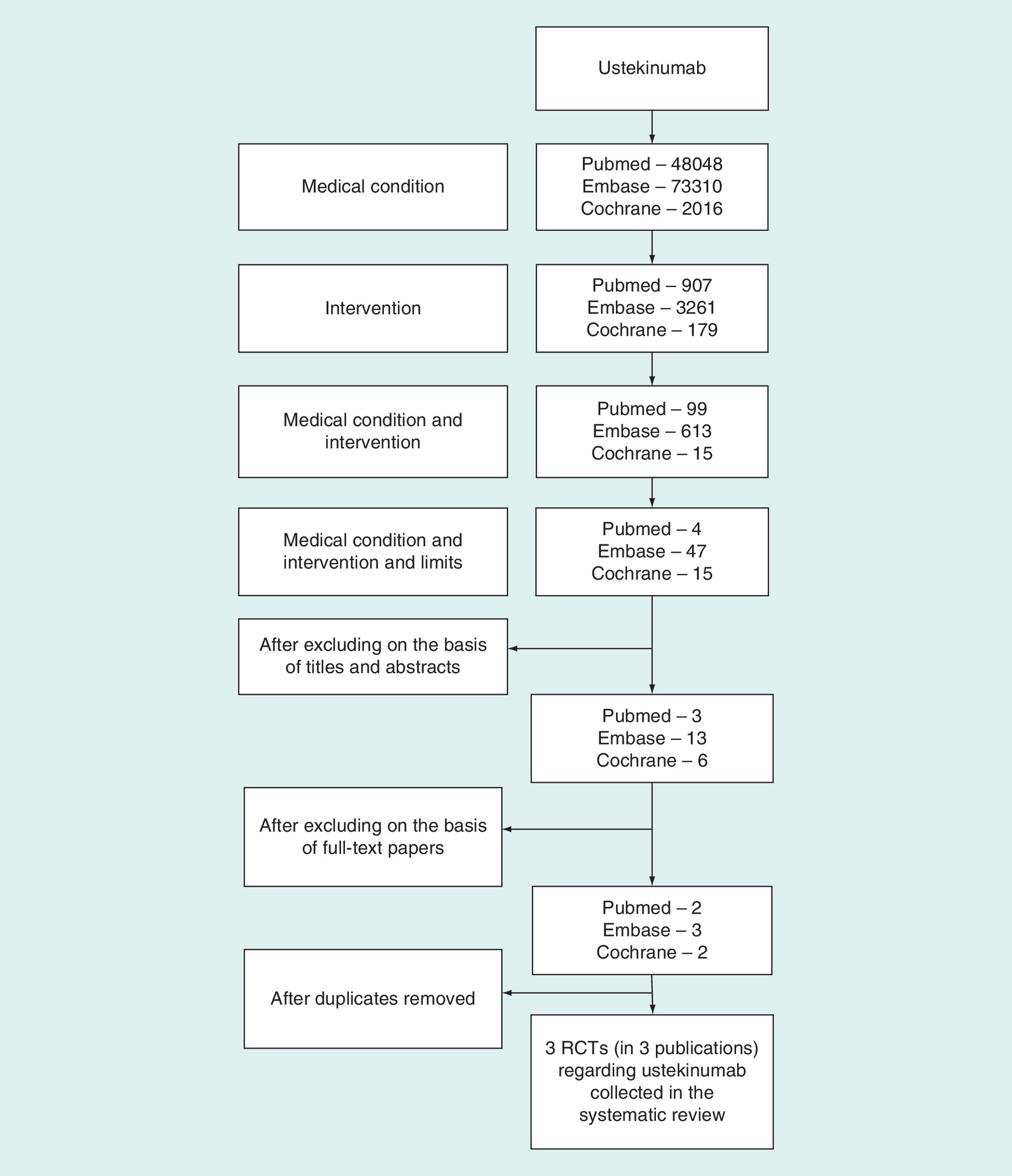
Figure 1. The literature search results of randomized controlled trials.
RCT: Randomized controlled trial.
Two of these studies [9,10] did not differ significantly in terms of population characteristics and drug administration regimen; the definitions of chosen end points: clinical response and clinical remission were the same as well as other methodology issues were similar, follow-up period for induction therapy assessment was the same – these two studies were homogeneous enough to be aggregated.
Table 2 summarizes characteristics of trials included in qualitative synthesis in a presented study. The methodological quality of the meta-analyzed RCTs was evaluated as high. The probability of occurrence of bias in most studies and domains was considered low (Figure 2). Both trials were randomized and double-blinded.
| Study (year) | Methodology | Patients | End points | Intervention | Follow-up period (efficacy) | Follow-up period (safety) | Ref. |
|---|---|---|---|---|---|---|---|
| Sandborn, (2012; CERTIFI) | RCT, multinational, multicenter, Phase III, parallel-group, double-blind, placebo-controlled | Patients at the age of at least 18 years and at least a 3-month history of CD with a score of 220 to 450 points on the CDAI | Clinical response (100-point decrease from the baseline CDAI score) at week 6 clinical remission (CDAI score <150 points) at week 6 | UST 1, 3 or 6 mg/kg or placebo during the induction phase (weeks 0–8); 526 patients were randomly assigned to receive intravenous UST UST (90 mg) or placebo at weeks 8 and 16, with efficacy assessed at week 22 during the maintenance phase (weeks 8–36), patients who had a response to UST as induction therapy and those who did not have a response underwent separate randomization to receive sc. | 6 weeks – induction phase, 22 weeks – maintenance phase | 6 weeks – induction phase, 22 weeks – maintenance phase | [9] |
| Feagan, (2016; UNITI-1 and IM-UNITI) | RCT, multinational, multi-center, Phase III, parallel-group, double-blind, placebo-controlled | Patients 18 years or older who had had CD for at least 3 months and had a score on the CDAI of 220 to 450 out of a possible range of 0 to 600 patients were required to have received one or more TNF antagonists at approved doses and to have met the criteria for primary nonresponse (the absence of a response) or secondary nonresponse (a response that was not maintained) or to have had unacceptable side effects | Clinical response at week 6 (decrease from baseline in CDAI score of at least 100 points or a total CDAI score less than 150) Clinical remission at week 8 (CDAI score <150) Clinical response at week 8 (decrease from baseline in CDAI score of at least 70 points at weeks 3 and 6) | UST iv. 130 or 6 mg/kg, or placebo during the induction phase UST sc. 90 mg every 8 or 12 weeks, or placebo through week 44 | 6 weeks – induction phase 52 weeks – maintenance phase (44 weeks of maintenance therapy and 8 weeks of therapy in induction phase) | 6 weeks – induction phase 52 weeks – maintenance phase (44 weeks of maintenance and 8 weeks of therapy in induction phase) | [10] |
CD: Crohn's disease; CDAI: Crohn's disease activity index; iv.: Intravenously; PLC: Placebo; RCT: Randomized controlled trial; sc.: Subcutaneously; UST: Ustekinumab; VDZ: Vedolizumab.
Meta-analysis
Clinical response rate
Clinical response was defined as a ≥100-point decrease in the Crohn's disease activity index score from output values in both revealed studies. In the TNF-α antagonist failure patients clinical response to ustekinumab was higher than in the placebo group. The fixed-effect model was used for analysis of the clinical response because there was no evidence of significant heterogeneity when data from the studies were pooled. The overall results of the meta-analysis demonstrated that ustekinumab was significantly superior to placebo in achieving the clinical response at week 6 of the treatment during induction phase in patients with active moderate to severe CD who were nonresponsive or intolerant to previous TNF-α antagonist therapy (RR = 1.62; 95% CI: 1.28–2.04; p < 0.0001; Figure 3). The meta-analysis in subpopulations of patients revealed that clinical response was significantly higher for patients who received ustekinumab compared with placebo patients in the following subgroups: secondary nonresponders, patients intolerant to TNF-α antagonist therapy, and patients failed to two previously used TNF-α antagonists, meanwhile no significant difference was revealed in primary responders group (Figure 4).
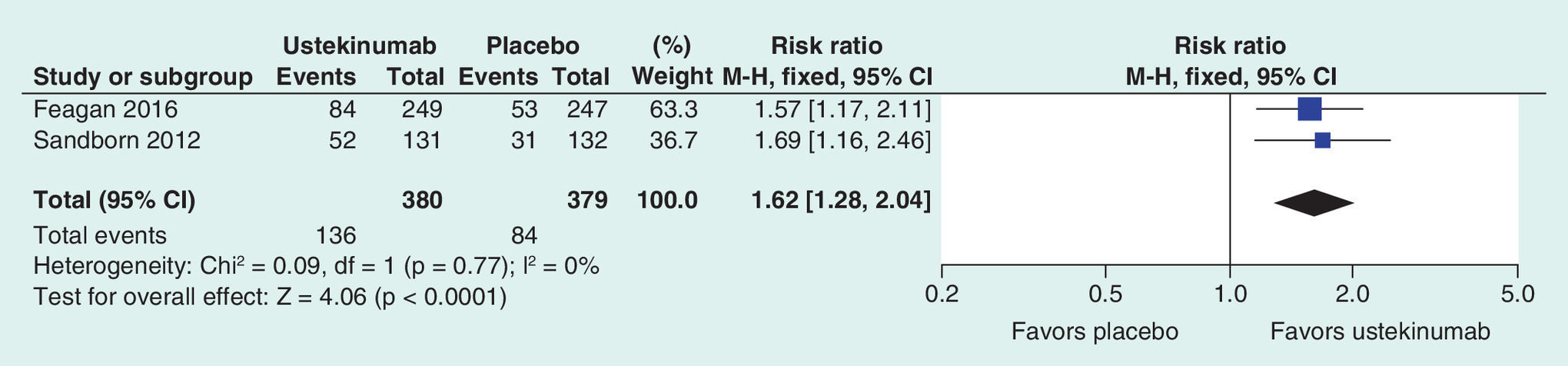
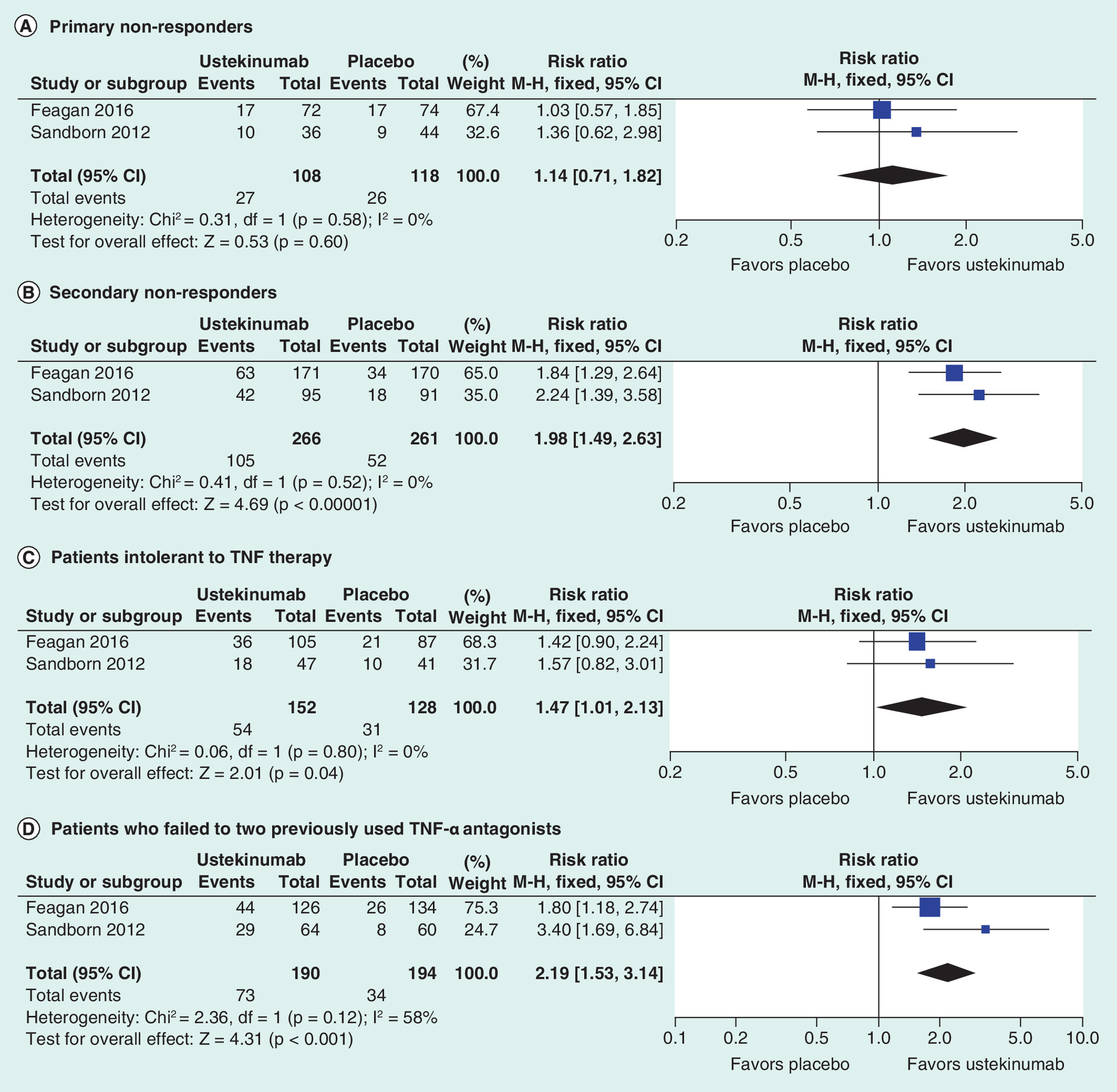
Figure 4. Forest plot of meta-analysis for ustekinumab versus placebo of response to treatment at week 6.
(A) Primary nonresponders, (B) secondary nonresponders, (C) patients intolerant to TNF-α therapy, (D) patients who failed to two previously used TNF-α antagonists.
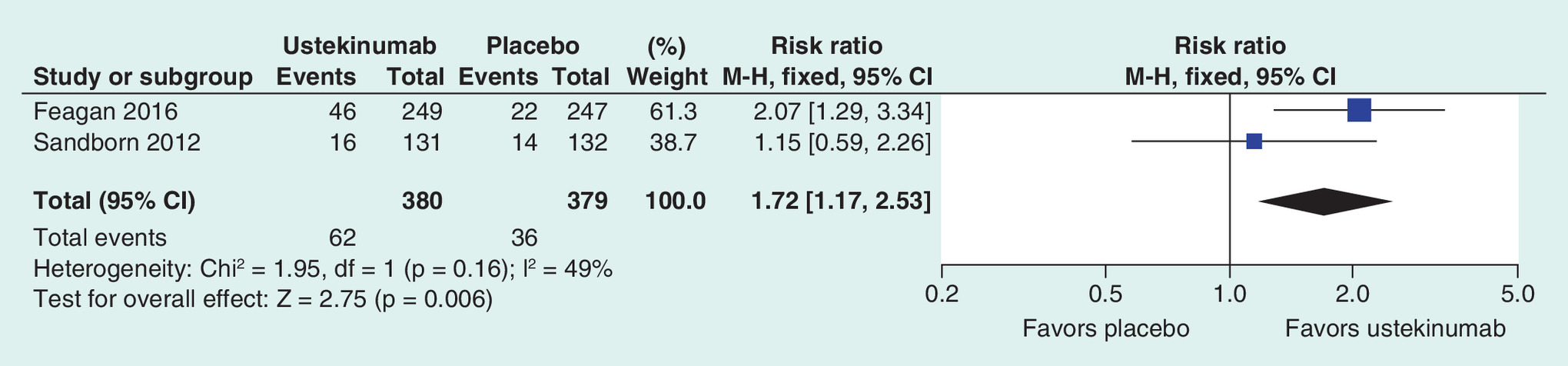
Clinical remission
Clinical remission was defined in both reference studies as a Crohn's disease activity index score of ≤150 points. There was no evidence of significant heterogeneity when data from the studies were pooled, therefore, a fixed-effect model was used for analysis of the clinical remission. Meta-analysis revealed that clinical remission was significantly higher for patients who received ustekinumab as compared with placebo patients. During the induction phase ustekinumab was significantly more effective than placebo in relation to the percentage of patients who achieved clinical remission at week 6 of treatment (RR = 1.72; 95% CI: 1.17–2.53; p = 0.006; Figure 5).
In a study [9], maintenance end points were assessed at 22 weeks so it was contraindicated to perform a data aggregation with the second study [10] providing maintenance phase results for 44 weeks of therapy. Due to follow-up period differences and population characteristics constraints we were unable to perform an aggregation of maintenance phase data for both pivotal trials [9,10].
Adverse events
In the overall meta-analysis, there were no statistically significant differences between ustekinumab and placebo in the frequency of any AEs (RR = 0.96; 95% CI: 0.86–1.06; p = 0.40), as well as in the risk of serious AEs (RR = 1.03; 95% CI: 0.61–1.73; p = 0.91) during the induction phase of therapy. In terms of serious infections there was also no statistically significant difference between groups although a trend was revealed suggesting impact of ustekinumab therapy on the end point rate (RR = 2.98; 95% CI: 0.97–9.13; p = 0.06; Figure 6).
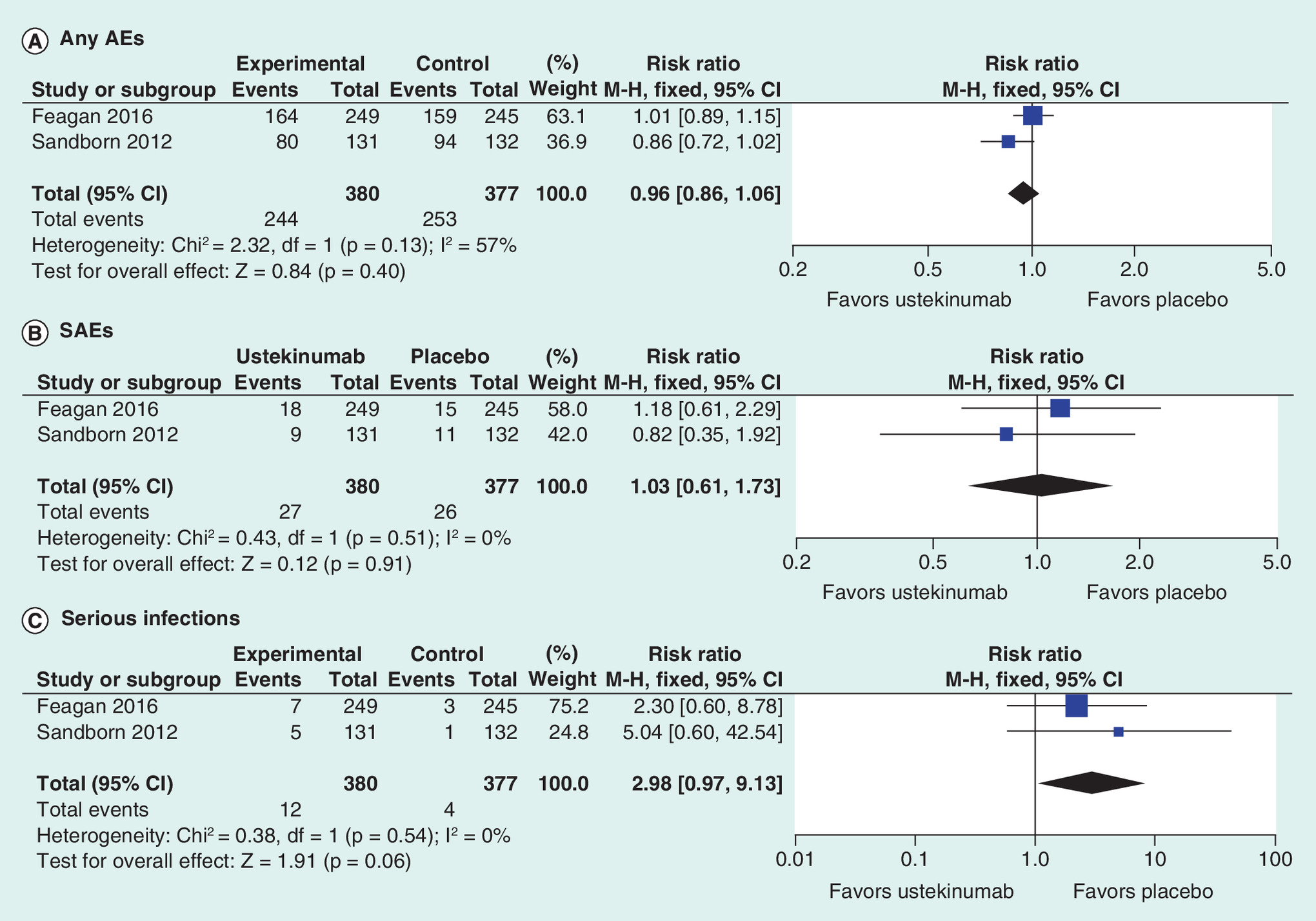
Figure 6. Forest plot of meta-analysis of adverse events for ustekinumab versus placebo.
(A) any adverse events, (B) serious adverse events, (C) serious infections.
AE: Adverse event; SAE: Serious adverse event.
Additionally, the meta-analysis on the basis of two RCTs revealed no statistically significant differences between ustekinumab and placebo with regard to the risk of: arthralgia, headache, nausea, nasopharyngitis, abdominal pain, and AEs associated with infusion or injection-site reactions during induction treatment (Table 3).
| Outcome | Feagan 2016 (UNITI-1) [10]† | Sandborn 2012 (CERTIFI) [9]‡ |
|---|---|---|
| Arthralgia | 15 (6.0%) vs 18 (7.3%) RR = 0.90 [95% CI: 0.51–1.6]; p = 0.61 | 6 (4.6%) vs 5 (3.8%) |
| Headache | 20 (8.0%) vs 22 (9.0%) RR = 1.09 [95% CI: 0.68–1.75]; p = 0.72 | 13 (9.9%) vs 8 (6.1%) |
| Nausea | 13 (5.2%) vs 18 (7.3%) RR = 0.72 [95% CI: 0.42–1.24]; p = 0.23 | 8 (6.1%) vs 11 (8.3%) |
| Nasopharyngitis | 11 (4.4%) vs 13 (5.3%) RR = 0.99 [95% CI: 0.53–1.84]; p = 0.98 | 8 (6.1%) vs 6 (4.5%) |
| Abdominal pain | 13 (5.2%) vs 13 (5.3%) RR = 0.90 [95% CI: 0.50–1.63]; p = 0.73 | 7 (5.3%) vs 9 (6.8%) |
| AEs associated with infusion or injection site reactions | 9 (3.6%) vs 5 (2.0%) RR = 1.45 [95% CI: 0.68–3.08]; p = 0.34 | 7 (5.3%) vs 6 (4.5%) |
†Ustekinumab 6 mg/kg (n = 249) versus placebo (n = 245).
‡Ustekinumab 6 mg/kg (n = 131) versus placebo (n = 132).
AE: Adverse event; RR: Risk ratio.
Discussion
The results of this meta-analysis including two RCTs [9,10] showed that the rates of clinical response and remission in the induction phase of therapy were significantly higher for patients treated with ustekinumab as compared with those treated with placebo in the population of patients refractory to anti-TNF-α therapy as well as in secondary nonresponders, patients intolerant to previous TNF-α antagonist therapy or those who failed to respond to two previously used TNF-α antagonists. No significant differences in clinical response were revealed in the subgroup of patients with previous failure in response to TNF-α antagonist therapy (primary nonresponders).
In our research we focused on the assessment of the effects of novel biologic drugs in primary nonresponders to TNF-α antagonist therapy because these patients have the lowest chances to benefit from biologic therapy, and providing alternatives for infliximab, adalimumab and certolizumab pegol seems to be a priority. As suggested in other publications [4,12], secondary nonresponders are more likely to get alternative treatment than patients refractory to induction TNF-α antagonist therapy, constituting a significant proportion of patients. Treatment failure with the use of the first TNF-α antagonist is associated with a lower rate of clinical response to subsequent therapies with alternative TNF-α antagonists, thus limiting the available treatment options for patients with CD [4,12,13].
We were interested to see whether the aggregation of data would affect the results presented in both single RCTs [9,10] for primary nonresponders if no significant clinical benefit for the use of ustekinumab was revealed. Therefore, we performed a sophisticated search for exclusive results for nonresponder subpopulations and aggregated the results, which is a novel approach and, to our knowledge, such findings have not been published before.
The results of our study suggest that although ustekinumab seems to be an appropriate therapeutic approach in patients with CD who fail to respond to TNF-α antagonist therapy, the best clinical effect can be observed for secondary nonresponders to previous TNF-α antagonist treatment and intolerant patients, while still no significant benefit in terms of clinical response was revealed for patients with primary nonresponse. This finding is important for future therapeutic approach to patients with CD and should influence the development of biologic therapy regimens in these patients. According to the aggregated data, ustekinumab seems to be not a valuable alternative treatment in case of the lack of effective biologic therapy for primary nonresponders, further research is necessary to confirm our conclusions. An important advantage of ustekinumab is the subcutaneous way of administration because this generally requires a reduced amount of the drug to maintain efficacy and is more convenient for patients.
In a systematic review we identified three placebo-controlled RCTs evaluating the use of ustekinumab in the therapy of CD [9–11].
A pivotal study [9] revealed that patients with moderate to severe CD resistant to TNF-α antagonists showed an increased rate of response to induction therapy with ustekinumab, as compared with placebo. Moreover, patients with an initial response to ustekinumab had significantly increased rates of response and remission with ustekinumab as maintenance therapy during the maintenance phase; 145 patients who responded to therapy with ustekinumab at 6 weeks were again randomized to receive either subcutaneous injections of ustekinumab (90 mg) or placebo at weeks 8 and 16 [9]. Maintenance therapy with ustekinumab, as compared with placebo, resulted in significantly increased rates of clinical remission and response at 22 weeks. Patients with an initial response to ustekinumab had significantly increased rates of response and remission with ustekinumab as maintenance therapy [9].
The pivotal study published in 2016 [10] was a phase-3 development program for the treatment of CD with ustekinumab consisting of two 8-week induction trials (UNITI-1 and UNITI-2) and one 44-week maintenance trial (IM-UNITI), representing 52 weeks of therapy. In UNITI-1, patients were required to have received one or more TNF-α antagonists at approved doses and to have met the criteria for primary or secondary nonresponse or to have shown unacceptable side effects. In UNITI-2, patients were required to have shown treatment failure or unacceptable side effects when treated with immunosuppressants or glucocorticoids and could have previously received one or more TNF-α antagonists. In our study, we did not include the UNITI-2 trial because we focused on the subpopulation of patients who failed to respond to TNF-α antagonist therapy. Patients who completed UNITI-1 or UNITI-2 and had a clinical response to induction therapy with ustekinumab could be enrolled in the IM-UNITI maintenance trial. A high percentage of patients with response to ustekinumab at induction were in clinical remission during maintenance, despite having received only a single intravenous induction dose of ustekinumab. This finding might indicate that ustekinumab has a long duration of action. The rates of AEs were similar for subcutaneous maintenance therapy with ustekinumab and placebo, and there was no apparent relationship between dose and safety. The AEs observed in those trials were consistent with 5 years of cumulative data acquired for patients with psoriasis (who received subcutaneous doses of ≤90 mg) and 2 years of safety data for patients with psoriatic arthritis. No deaths, serious opportunistic infections, tuberculosis or major cardiovascular AEs were reported, but large studies of longer duration are needed to assess uncommon AEs [10].
In the third RCT [11] ustekinumab showed efficacy in patients with moderate to severe CD, particularly among patients previously receiving infliximab. In the induction phase of this Phase IIA study, patients were randomly assigned to receive intravenous ustekinumab (at a dose of 6 mg/kg of body weight) or placebo at week 0. During the maintenance phase, patients who responded to ustekinumab therapy at 6 weeks underwent a second randomization to receive subcutaneous injections of ustekinumab (90 mg) or placebo at weeks 8 and 16. Intravenous ustekinumab induction therapy in patients with CD refractory to treatment with TNF-α antagonists (primary or secondary lack of response) showed a significant benefit in terms of clinical response but not remission, and subcutaneously administered maintenance doses of ustekinumab were shown to be efficacious during a period of 22 weeks [11]. Patients with moderate to severe CD that were resistant to TNF-α antagonists had an increased rate of response to induction with ustekinumab, as compared with placebo. Patients with an initial response to ustekinumab had significantly increased rates of response and remission with ustekinumab as maintenance therapy [11]. However, the trial differed from the pivotal studies [9,10] in terms of treatment regimen, cross-over design and duration of therapy; therefore, we could not include its results in the current meta-analysis.
The efficacy of ustekinumab was also assessed in observational studies. One retrospective observational study included 45 patients with CD refractory to TNF-α antagonist therapy and treated with ustekinumab with the use of a novel subcutaneous dosing regimen designed to simulate the intravenous load used in clinical trials. It revealed that ustekinumab was effective in improving clinical, laboratory and endoscopic markers of disease activity in patients with severe refractory CD [14]. Another retrospective observational study collected data on 122 consecutive patients with active CD refractory to TNF-α antagonist therapy, who received at least one subcutaneous injection of ustekinumab and were followed for at least 3 months. The primary outcome was clinical benefit, defined as a reduction in symptoms and the levels of biochemical markers of CD and complete weaning from steroids, without surgery or immunosuppressant therapies. The outcome was achieved in 65% of the patients within 3 months of ustekinumab therapy [15]. Another retrospective multicenter open-label study [16], which included patients with CD resistant to conventional immunosuppressants and anti-TNF-α drugs, revealed that ustekinumab was an effective and safe treatment option. Clinical response after a loading ustekinumab dose was achieved in 84% of the patients, while the clinical benefit at 6 months, 12 months and at the end of the follow-up was 76, 64 and 58%, respectively. Dose escalation was effective in 73% of the patients. The initial response to ustekinumab and previous use of more than two immunosuppressant drugs were associated with an improvement in clinical response to ustekinumab maintenance therapy. AEs were reported in 9.5% of the patients, but none of them required drug withdrawal [16].
We identified only one network meta-analysis including studies on ustekinumab [17], but it concerned only biologic-naive patients and thus was not within the scope of our analysis.
Our systematic review and meta-analysis has a number of limitations. The primary limitation is the fact that only two RCTs were available for inclusion. The RCTs differed in the duration of the follow-up periods (22 [9] and 44 weeks [10]), but to overcome the problem of heterogeneity, only the results for induction phase (6 weeks of treatment in both clinical trials) were aggregated and analyzed in our study. Another important limitation of our meta-analysis is the duration of the follow-up period (6 weeks), which was too short to assess the safety profile and all possible AEs of therapy.
The strengths of this systematic review and meta-analysis include strict methodology, which follows the methods and recommendations from the PRISMA Statement [7] concerning clear search strategy and predefined criteria for inclusion of studies in a systematic review and meta-analysis. Moreover, data extraction and calculations were conducted independently by two researchers. Furthermore, only RCTs were considered for inclusion. The analyzes were performed on the basis of intention-to-treat data, and depending on data heterogeneity, an appropriate statistical model was applied (fixed or random). Clinical outcomes were assessed using exactly the same definitions in both studies. Finally, the meta-analysis covered high-quality RCTs with a large number of patients.
Conclusion
In summary, the results of this systematic review and meta-analysis demonstrated that ustekinumab therapy has a beneficial effect in patients with CD, excluding primary nonresponders, when compared with placebo. Based on the safety analysis, there was no evidence for an increase in the incidence of any AEs. Our study supports the use of ustekinumab for the treatment of patients with CD refractory to TNF-α antagonists.
Efficacy and safety of ustekinumab in the induction therapy of anti-TNF-α failure patients with Crohn's disease was assessed.
Clinical response was significantly higher for patients who received ustekinumab compared with placebo patients in a group of TNF-α antagonist failure patients.
Clinical response was significantly higher for patients in the following subgroups: secondary nonresponders, intolerant patients and patients who failed at least two TNF-α antagonists.
In case of primary nonresponders clinical response occurred insignificant.
The clinical remission in TNF-α antagonist failure population was significantly higher for patients who received ustekinumab compared with placebo.
Risk of adverse events in the induction phase of therapy was not significantly higher compared with placebo.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
The Crohn's & Colitis Foundation of America. The Facts About Inflammatory Bowel Diseases. www.ccfa.org/assets/pdfs/updatedibdfactbook.pdf.
2.
Burisch J, Tine J, Martinato M. The burden of inflammatory bowel disease in Europe. J. Crohn's Colitis 7(4), 322–337 (2013).
3.
Floyd DN, Langham S. The economic and quality-of-life burden of Crohn's disease in Europe and the United States, 2000 to 2013: a systematic review. Dig. Dis. Sci. 60, 299–312 (2015).
4.
Roda G, Jharap B, Neeraj N et al. Loss of response to Anti-TNF-As: definition, epidemiology, and management. Clin. Transl. Gastroenterol. 7(1), e135 (2016).
5.
Colombel JF, Sandborn WJ, Rutgeerts P et al. Adalimumab for maintenance of clinical response and remission in patients with Crohn's disease: the CHARM trial. Gastroenterology 132, 52–65 (2007).
• Summary of product characteristics for Stelara® (ustekinumab).
6.
Moher D, Liberati A, Tetzlaff J, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 6, e1000097 (2009).
7.
Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions. John Wiley & Sons, NJ, USA (2008).
8.
Sandborn W, Gasink C, Long-Long G et al. Ustekinumab induction and maintenance therapy in refractory Crohn's disease. N. Engl. J. Med. 367, 1519–1528 (2012).
• Pivotal clinical trial in ustekinumab assessment.
9.
Feagan BG, Sandborn WJ, Gasink C et al. Ustekinumab as induction and maintenance therapy for Crohn's disease. N. Engl. J. Med. 375, 1946–1960 (2016).
• Pivotal clinical trial in ustekinumab assessment.
10.
Sandborn WJ, Feagan BG, Fedorak RN et al. A randomized trial of ustekinumab, a human interleukin-12/23 monoclonal antibody, in patients with moderate to severe Crohn's disease. Gastroenterology 135(4), 1130–1141 (2008).
•• Additional clinical trial in ustekinumab efficacy in Crohn's disease (CD) assessment.
11.
Sandborn WJ, Rutgeerts P, Enns R et al. Adalimumab induction therapy for Crohn disease previously treated with infliximab: a randomized trial. Ann. Intern. Med. 146, 829–838 (2007).
12.
Sandborn WJ. Clinical perspectives in Crohn's disease. Moving forward with anti-TNF-A-alpha therapy: current needs and future treatments. Rev. Gastroenterol. Disord. 7(Suppl. 2), S23–S35 (2007).
13.
Harris KA, Horst S, Gadani A et al. Patients with refractory Crohn's disease successfully treated with ustekinumab. Inflamm. Bowel Dis. 22(2), 397–401 (2016).
14.
Wils P, Bouhnik Y, Michetti P et al. Subcutaneous ustekinumab provides clinical benefit for two-thirds of patients with Crohn's disease refractory to anti-tumor necrosis factor agents. Clin. Gastroenterol. Hepatol. 14(2), 242–250 (2016).
•• Additional clinical trial in ustekinumab efficacy in CD assessment.
15.
Khorrami S, Ginard D, Marín-Jiménezet I et al. Ustekinumab for the treatment of refractory Crohn's disease: the Spanish experience in a large multicentre open-label cohort. Inflamm. Bowel Dis. 22(7), 1662–1669 (2016).
•• Additional clinical trial in ustekinumab efficacy in CD assessment.
16.
Singh S, Garg SK, Pardi D et al. Comparative efficacy of biologic therapy in biologic-naïve patients with Crohn disease: a systematic review and network meta-analysis. Mayo Clin. Proc. 89(12), 1621–1635 (2014).
17.
Singh S, Garg SK, Pardi D et al. Comparativeefficacy of biologic therapy in biologic-naïve patients with Crohn disease: asystematic review and network meta-analysis. Mayo Clin. Proc. 89(12), 1621–1635 (2014).
Information & Authors
Information
Published In
Copyright
© Future Medicine Ltd.
History
Published online: 29 June 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Efficacy and safety of ustekinumab in the induction therapy of TNF-α-refractory Crohn's disease patients: a systematic review and meta-analysis. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0022
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Mahmoud H. Mosli, Badr Al-Bawardy, Turki AlAmeel, Nahla A. Azzam, Shakir A. Bakkari, Othman R. Alharbi, Abdulelah Almutairdi, Yaser K. Meeralam, Omar I. Saadah, Majid A. Almadi, Waleed Alhazzani, Haifa F. Alotaibi, Khalidah A. Alenzi, Bedor A. Al-Omari, Hajer Y. Almudaiheem, Ahmed H. Al-Jedai, Practical guidelines on medical management of adults with moderate-to-severe inflammatory bowel disease, Saudi Journal of Gastroenterology, 10.4103/sjg.sjg_277_25, 32, 4, (254-297), (2025).
- Ahmed G. Alghamdi, Hadeel S. Aldofaian, Mohammed S. Alahmari, Bashaar K. Alibrahim, Mishal A. Alshowair, Hussam A. Alhamidi, Abdullah H. Bawazir, Amal M. Aseri, Alaa A. Aldeibani, Mohanned M. AlRaddadi, Reem O. Almutairi, Sultan S. Alshahrani, Abdullah D. Alenezi, Rakan H. Alshala, Abeer M. Alhuraibi, Renad M. Alharbi, Patterns and predictors of biologic therapy switching in inflammatory bowel disease at a tertiary care center: A retrospective observational study, Saudi Journal of Gastroenterology, 10.4103/sjg.sjg_169_25, (2025).
- Hongkun Li, Yuyue Zhang, Simin Du, Jinghan Shen, Xingyan Liu, Jie Jing, “Remodeling the intestinal immune microenvironment”: immune regulation and tissue regeneration by mesenchymal stem/stromal cells in the repair microenvironment of inflammatory bowel disease, Frontiers in Immunology, 10.3389/fimmu.2025.1543702, 16, (2025).
- Jildou van der Werf, Nicholas Ian Fleming, Are single nucleotide polymorphisms underutilized for guiding treatment of inflammatory bowel disease?, Immunology & Cell Biology, 10.1111/imcb.70029, 103, 6, (551-562), (2025).
- Richard Silva, José Nunes de Azevedo, Jorge Pereira Machado, Jorge Magalhães Rodrigues, Placebo-Controlled Trials in the Management of Crohn’s Disease: An Umbrella Review of Meta-Analyses, Medical Sciences, 10.3390/medsci13010012, 13, 1, (12), (2025).
- Mahesh Krishna, Ellen J. Spartz, Laura Maas, Vivy Cusumano, Sowmya Sharma, Berkeley Limketkai, Alyssa Parian, Retrospective Cohort Study on the Predictive Value of Primary Non-response to Initial Biologic for Future Biologic Use in Patients with Inflammatory Bowel Disease, Digestive Diseases and Sciences, 10.1007/s10620-024-08816-9, 70, 2, (746-753), (2025).
- Sunil Samnani, Emily C L Wong, Hasan Hamam, Parambir S Dulai, John K Marshall, Vipul Jairath, Walter Reinisch, Neeraj Narula, Outcomes of Patients With Prior Biologic Intolerance Are Better Than Those With Biologic Failure in Clinical Trials of Inflammatory Bowel Disease, Journal of Crohn's and Colitis, 10.1093/ecco-jcc/jjae151, 19, 3, (2024).
- Omar I. Saadah, Turki AlAmeel, Ahmed Al Sarkhy, Mohammed Hasosah, Abdulrahman Al-Hussaini, Majid A. Almadi, Badr Al-Bawardy, Talal A. Altuwaijri, Mohammed AlEdreesi, Shakir A. Bakkari, Othman R. Alharbi, Nahla A. Azzam, Abdulelah Almutairdi, Khalidah A. Alenzi, Bedor A. Al-Omari, Hajer Y. Almudaiheem, Ahmed H. Al-Jedai, Mahmoud H. Mosli, Saudi consensus guidance for the diagnosis and management of inflammatory bowel disease in children and adolescents, Saudi Journal of Gastroenterology, 10.4103/sjg.sjg_171_24, 31, 3, (107-136), (2024).
- Yaqing Bai, Yinghao Sun, Qi He, Xiaoyin Bai, Hong Yang, Comparative effectiveness and safety of ustekinumab at different intervals of maintenance phase in inflammatory bowel disease: a systematic review and meta-analysis, European Journal of Gastroenterology & Hepatology, 10.1097/MEG.0000000000002718, 36, 4, (359-370), (2024).
- Yago González-Lama, Elena Ricart, Daniel Carpio, Guillermo Bastida, Daniel Ceballos, Daniel Ginard, Ignacio Marin-Jimenez, Luis Menchen, Fernando Muñoz, Controversies in the management of anti-TNF therapy in patients with Crohn’s disease: a Delphi consensus, BMJ Open Gastroenterology, 10.1136/bmjgast-2023-001246, 11, 1, (e001246), (2024).
- See more