Comparing the outcomes and costs of cardiac monitoring with implantable loop recorders and mobile cardiac outpatient telemetry following stroke using real-world evidence
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Patients with ischemic stroke (IS) commonly undergo monitoring to identify atrial fibrillation with mobile cardiac outpatient telemetry (MCOT) or implantable loop recorders (ILRs). The authors compared readmission, healthcare cost and survival in patients monitored post-stroke with either MCOT or ILR. Materials & methods: The authors used claims data from Optum's de-identified Clinformatics® Data Mart Database to identify patients with IS hospitalized from January 2017 to December 2020 who were prescribed ambulatory cardiac monitoring via MCOT or ILR. They compared the costs associated with the initial inpatient visit as well as the rate and causes of readmission, survival and healthcare costs over the following 18 months. Datasets were balanced using patient baseline and hospitalization characteristics. Multivariable generalized linear gamma regression was used for cost comparisons. Cox proportional hazard regression was used for survival and readmission analysis. Sub-cohorts were analyzed based on the severity of the index IS. Results: In 2244 patients, readmissions were significantly lower in the MCOT monitored group (30.2%) compared with the ILR group (35.4%) (hazard ratio [HR] 1.23; 95% CI: 1.04–1.46). Average cost over 18 months starting with the index IS was $27,429 (USD) lower in the MCOT group (95% CI: $22,353–$32,633). Survival difference bordered on statistical significance and trended to lower mortality in MCOT (8.9%) versus ILR (11.3%) (HR 1.30; 95% CI: 1:00–1.69), led by significance in patients with complications or comorbidities with the index event (MCOT 7.5%, ILR 11.5%; HR 1.62; 95% CI: 1.11–2.36). Conclusion: The use of MCOT versus ILR as the primary monitor following IS was associated with significant decreases in readmission, lower costs for the initial IS and total care over the next 18 months, significantly lower mortality for patients with complications and comorbidities at the index stroke, and a trend toward improved survival across all patients.
Shareable abstract
MCOT was associated with decreased readmissions (p = 0.016), lower healthcare costs (p < 0.001) and a trend toward lower mortality in patients with stroke (p = 0.051), when compared with ILR monitoring in an analysis of US insurance claims from Optum's de-identified Clinformatics® Data Mart Database.
#HEOR #healtheconomics #stroke #readmissions #healthcarecosts #mortality
Plain language summary
What is this study about?
This study compares the health and economic outcomes of using mobile cardiac outpatient telemetry (MCOT) and implantable loop recorders (ILRs) for long-term monitoring following an inpatient visit in patients who have had a stroke by analyzing Optum's de-identified Clinformatics® Data Mart Database claims for hospital admissions between 2017 and 2020.
What were the main results of the claims analysis?
The use of MCOT as the primary arrhythmia monitor following an initial stroke was associated with a decreased rate of readmissions across all patients, along with reduced healthcare costs for both the index stroke event and for total cost of care incurred over the 18 months following the index event. A significant reduction in mortality was seen in patients who suffered complications and comorbidities with the index stroke, with a trend toward improved survival across all patients.
What do the results mean?
Significant differences in readmission and healthcare costs were associated with the choice of post-stroke ambulatory arrhythmia monitoring.
Strokes are a costly and life-threatening medical emergency, with roughly 87% of all strokes classified as an ischemic stroke (IS) [1]. During 2019–2020, the estimated direct expenditure associated with stroke in USA amounted to $34.5 billion (USD), which included costs related to hospital outpatient visits or consultations, inpatient and emergency admissions, home healthcare services and prescribed medications [2]. In 2022, the Centers for Medicare and Medicaid Services (CMS) reported 30,827 inpatient admissions for IS, with average costs of $18,963 per admission and a mortality rate of 10% in the first 30 days, and up to 40% in the first year following the stroke [3,4]. Patients with atrial fibrillation (AF) and a history of stroke have a 15% risk of a recurrent stroke within 1 year of the initial stroke [5,6]. Two large cohort studies in USA found that 12.1% of patients with IS are readmitted within 30 days post-discharge, rising to 22.2% within 1 year, and that a fifth of these were unplanned readmissions that were primarily attributable to acute cerebrovascular diseases [7,8]. In an effort to prevent additional strokes, and ideally reduce stroke readmissions, patients with AF identified post-stroke are often initiated on oral anticoagulation medications, as recommended by the most recent American Heart Association/American Stroke Association guidelines on the diagnosis and management of AF [9]. To identify AF, patients are monitored for arrhythmias in a variety of ways, including admission electrocardiogram (ECG), serial resting ECGs, continuous inpatient cardiac telemetry, Holter monitoring, mobile cardiac outpatient telemetry (MCOT), external loop recording and implantable loop recording (ILR). The 2021 American Heart Association/American Stroke Association guideline on secondary prevention of IS recommends MCOT and ILR for long-term diagnostic monitoring post-IS, which can detect intermittent AF more readily than conventional follow-up through scheduled ECG monitoring [10–14].
ILRs are surgically implanted devices that measure cardiac electrical activity from underneath the skin of the chest. The device is programmed to record electrograms that reach pre-programmed rates or rhythms for overnight relay to the ILR manufacturers' data storage systems. The duration of fibrillation required to qualify as an AF detection by ILR is typically >2 min. ILRs are capable of monitoring up to 4.5 years [15,16].
MCOT is an externally worn monitor which measures electrical activity through a skin-surface ECG. The device continuously records and analyzes the incoming signal for AF with detection threshold duration typically at >30s. Detected events are relayed in near real-time to a 24/7 staffed monitoring center for evaluation and caregiver notification. In USA, reimbursement for MCOT allows for up to 30 days of continuous monitoring [17]. While MCOT is used for up 30 days, the ILR is intended to be used for years of monitoring. MCOT is a one-time billable test whereas ILR has a cost for the original device and implantation, eventual removal and monthly payments for ongoing recording and interpretation for the life of the device. ILR retains a ‘memory’ of discrete, dysrhythmic events, while MCOT maintains a continuous signal record. With the ILR, multiple arrhythmia detections result in a growing collection of arrhythmia event recordings, which may eventually fill the recorder's on-board memory. Once its memory is filled, the ILR either overwrites earlier events or ceases to record until cleared, while the MCOT continuous signal 30-day record is retained until the end of the service. These differences, particularly in the duration of AF required to qualify as an event, may lead to differences in detection capabilities which could in turn impact patient care [18]. For example, a 2015 meta-analysis of different diagnostic methods for identifying AF found no difference in the proportion of patients diagnosed with post-stroke AF between ILR and MCOT at 12 months (p = 0.91). However, at 21 days post-stroke only 9.6% of those who underwent ILR had been diagnosed with AF, compared with 19.1% with MCOT (p < 0.01) [13]. Similarly, a 2022 meta-analysis found that ILR monitoring achieved a pooled AF detection rate of 24.5% but this yield was not reached until after 36 months of ILR monitoring [19].
The authors aimed to compare the identifiable outcomes of readmission, healthcare costs and survival in patients monitored post-stroke with either MCOT or ILR.
Methods
Patient population
A retrospective database analysis was conducted using Optum's de-identified Clinformatics® Data Mart Database (CDM). Following the method outlined in Zachrison et al. for identifying stroke-related hospitalizations, inpatient records with a diagnosis related group (DRG) code from the following clusters were extracted for admissions initiated between 1 January 2017 and 31 December 2020 [20,21].
Craniotomy with major device implant or acute complex central nervous system primary diagnosis. DRG codes; 023, 024.
Peripheral, cranial nerve and other nervous system procedures. DRG codes; 040, 041, 042.
Ischemic stroke, precerebral occlusion or transient ischemia with thrombolytic agent. DRG codes; 061, 062, 063.
Intracranial hemorrhage or cerebral infarction. DRG codes; 064, 065, 066
Subject to further inclusion and exclusion criteria, these encounters were defined as the ‘index stay’, and the circumstances surrounding them as the ‘index event’ (Figure 1).
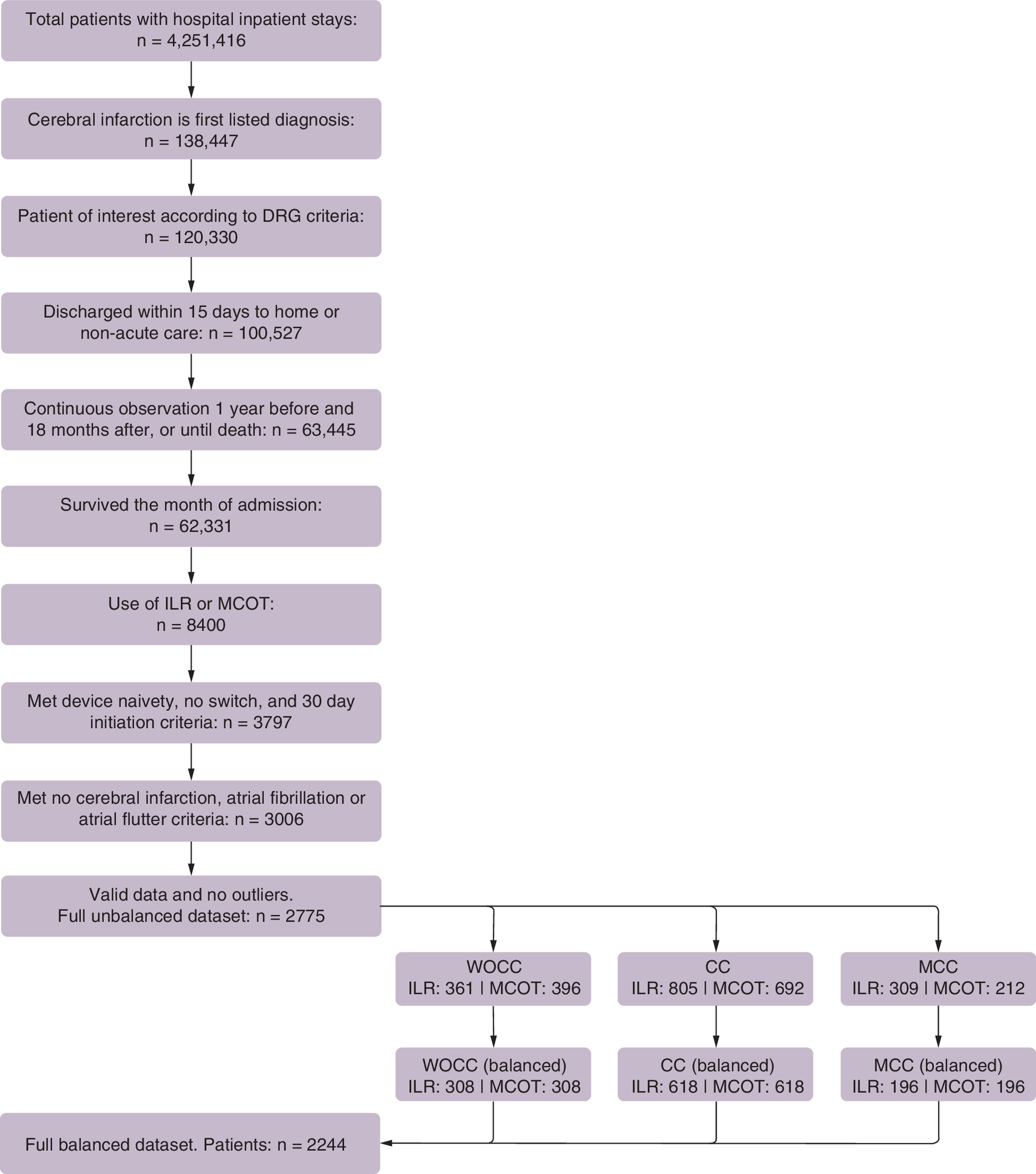
Figure 1. Sample population flowchart (patients).
CC: With complication or comorbidity; DRG: Diagnosis related group; ILR: Implantable loop recorder; MCC: With major complication or comorbidity; MCOT: Mobile cardiac outpatient telemetry; WOCC: Without complication or comorbidity.
For these encounters, the first listed diagnosis, serving as surrogate for a principal diagnosis, was required to correspond to a cerebral infarction, as indicated by any diagnosis code within the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) I63 group. Furthermore, the index events were characterized to correspond to the patients' first documented stroke. In this context, only the first stay for each patient was selected and patients with any I63 diagnosis in the year prior were excluded.
For inclusion, patients must have been initiated on ambulatory cardiac monitoring (ACM) with either ILR or MCOT anytime from the day of admission, up to 30 days after discharge. The procedural coding terminology used to identify these ACM can be found in the supplement. A 30-day cutoff was chosen to confidently associate the device with the identified stroke and to maintain comparability between the groups [22]. Continuous observation of 1 year before and 18 months after index admission, or until death, was required in order to compile history-based health profiles and to measure outcomes.
Patients monitored with more than one type of ACM device during the follow-up period, including extended wear Holter (EWH), were considered a distinct group outside the scope of this study, and thus, were excluded. Patients with evidence of ACM use in the year prior to the index admission were also excluded. The resulting data set from here on was composed of patients monitored with only one type of device, either ILR or MCOT, after the identified stroke event.
To focus on patients for whom ACM was used specifically for the detection of AF, patients with an ICD-10-CM I48 diagnosis, indicating atrial fibrillation or flutter, during the prior year were excluded. Furthermore, patients who died during the index month, who were transferred to hospice or long-term care, or had an index inpatient stay longer than 15 days, were excluded. Patients with poor early outcomes/cases were beyond the scope and intent of this study. However, the main motivation for these exclusion criteria was to mitigate biases related to device initiation timing [22,23]. Only patients 18 years of age and older were included.
Finally, patients were excluded based on outlier values in two baseline variables: prior year costs and age; and on outliers of two outcomes variables; index costs; and non-index post-index costs. Values at or above the 99th percentile were considered outliers.
Patient subgroups were formed based on the severity of the index hospitalization. These were primarily determined using the standardized DRG distinctions for complications and comorbidities as follows [24].
Major complication or comorbidity (MCC): This most severe category included patients discharged with DRGs 023, 040, 061, or 064, all of which are defined as ‘with major complication or comorbidity’.
Complication or comorbidity (CC): Encompassing less severe cases than MCC, this category included patients discharged with DRGs 041, 062 or 065, all of which are defined as ‘with complication or comorbidity’. Patients discharged with DRG 024, described as ‘without MCC’, were also assigned to the CC group based on the understanding that a major interventional procedure like craniotomy reaches a level of complexity beyond that of an IS without notable complications or comorbidities. Perfect balance regarding DRG 024 was ensured in the analysis data to account for potential misallocation.
Without CC/MCC (WOCC): Representing the least severe cases, this category includes patients discharged with DRGs 042, 063 and 066, all described as without CC or MCC.
For each patient, a health profile was assembled, consisting of Charlson summary measures, Charlson comorbidities and a set of additional health conditions [25–29]. These profiles were based on all diagnoses for the patient during the year preceding the index admission up to the date of the index discharge. This timeframe was chosen to encapsulate both the patient's health history and the characteristics of the index event. The additional conditions included in the health profile were hypertension, valvular disease, obesity, hyperlipidemia, obstructive sleep apnea, nicotine dependence and cigarette use [28,30]. The methodology used to identify these conditions is provided in the supplement.
The analysis used subsamples of the data in which all comparison groups were balanced according to patient health profiles, demographics, index event and stay characteristics as well as healthcare costs for the year preceding the index admission. For this, propensity scores, obtained via logistic regression and a matching greedy nearest neighbors' algorithm without replacement were used [31–34]. For adequate balance, an absolute standardized mean difference value (|SMD|) less than 0.10 was required for all variables reported in the balance tables (Table 1, and Supplemental Table A1) [25,30,32,33]. Also, when applicable, perfect balance was implemented for the three severity categories and for the DRGs 023 and 024.
| Unbalanced ILR, n = 1475; MCOT, n = 1300; total, n = 2775 | Balanced ILR, n = 1122; MCOT, n = 1122; total, n = 2244 | |||||
|---|---|---|---|---|---|---|
| Numerical characteristics | ILR mean | MCOT mean | |SMD| | ILR mean | MCOT mean | |SMD| |
| Age (years) | 72.91 | 75.79 | 0.314 | 74.81 | 75.08 | 0.032 |
| Length of stay (days) | 4.40 | 3.40 | 0.386 | 3.81 | 3.62 | 0.081 |
| Charlson comorbidities present | 3.67 | 3.53 | 0.075 | 3.57 | 3.57 | 0.002 |
| Charlson age-adjusted score | 5.59 | 5.77 | 0.074 | 5.67 | 5.72 | 0.023 |
| Year prior costs (2022 USD) | 15,952 | 15,601 | 0.012 | 16,198 | 15,689 | 0.018 |
| Qualitative characteristics | ILR, n (%) | MCOT, n (%) | |SMD| | ILR, n (%) | MCOT, n (%) | |SMD| |
| Demographics | ||||||
| Female | 767 (52.0) | 702 (54.0) | 0.040 | 595 (53.0) | 608 (54.2) | 0.023 |
| Male | 708 (48.0) | 598 (46.0) | 0.040 | 527 (47.0) | 514 (45.8) | 0.023 |
| Index hospitalization | ||||||
| Elective | 28 (1.9) | 16 (1.2) | 0.054 | 15 (1.3) | 13 (1.2) | 0.016 |
| Urgent | 184 (12.5) | 155 (11.9) | 0.017 | 132 (11.8) | 132 (11.8) | <0.001 |
| Emergency | 1263 (85.6) | 1129 (86.8) | 0.035 | 975 (86.9) | 977 (87.1) | 0.005 |
| Intensive care unit | 840 (56.9) | 668 (51.4) | 0.112 | 608 (54.2) | 600 (53.5) | 0.014 |
| Major surgery | 114 (7.7) | 63 (4.8) | 0.119 | 60 (5.3) | 61 (5.4) | 0.004 |
| DRG 023 | 45 (3.1) | 25 (1.9) | 0.072 | 25 (2.2) | 25 (2.2) | <0.001 |
| DRG 024 | 51 (3.5) | 32 (2.5) | 0.059 | 32 (2.9) | 32 (2.9) | <0.001 |
| WOCC | 361 (24.5) | 396 (30.5) | 0.134 | 308 (27.5) | 308 (27.5) | <0.001 |
| CC | 805 (54.6) | 692 (53.2) | 0.027 | 618 (55.1) | 618 (55.1) | <0.001 |
| MCC | 309 (20.9) | 212 (16.3) | 0.119 | 196 (17.5) | 196 (17.5) | <0.001 |
| Index year 2017 | 250 (16.9) | 201 (15.5) | 0.040 | 184 (16.4) | 178 (15.9) | 0.015 |
| Index year 2018 | 405 (27.5) | 318 (24.5) | 0.068 | 293 (26.1) | 276 (24.6) | 0.035 |
| Index year 2019 | 444 (30.1) | 383 (29.5) | 0.014 | 345 (30.7) | 333 (29.7) | 0.023 |
| Index year 2020 | 376 (25.5) | 398 (30.6) | 0.114 | 300 (26.7) | 335 (29.9) | 0.069 |
| Index discharge | ||||||
| Home, self-care | 747 (50.6) | 701 (53.9) | 0.066 | 604 (53.8) | 605 (53.9) | 0.002 |
| Home, assisted | 246 (16.7) | 285 (21.9) | 0.133 | 215 (19.2) | 222 (19.8) | 0.016 |
| SNF and like | 193 (13.1) | 139 (10.7) | 0.074 | 128 (11.4) | 130 (11.6) | 0.006 |
| Rehabilitation | 234 (15.9) | 153 (11.8) | 0.119 | 150 (13.4) | 144 (12.8) | 0.016 |
| Short-term care | 55 (3.7) | 22 (1.7) | 0.126 | 25 (2.2) | 21 (1.9) | 0.025 |
| Charlson comorbidities | ||||||
| AIDS/HIV | – | – | 0.042 | – | – | 0.024 |
| Acute myocardial infarction | 213 (14.4) | 171 (13.2) | 0.037 | 158 (14.1) | 154 (13.7) | 0.010 |
| Cancer any malignancy | 185 (12.5) | 152 (11.7) | 0.026 | 132 (11.8) | 130 (11.6) | 0.006 |
| Cerebrovascular disease | 1475 (100) | 1300 (100) | <0.001 | 1122 (100.0) | 1122 (100) | <0.001 |
| Congestive heart failure | 302 (20.5) | 279 (21.5) | 0.024 | 225 (20.1) | 236 (21.0) | 0.024 |
| COPD | 379 (25.7) | 340 (26.2) | 0.010 | 291 (25.9) | 293 (26.1) | 0.004 |
| Dementia | 123 (8.3) | 108 (8.3) | 0.001 | 104 (9.3) | 96 (8.6) | 0.025 |
| Diabetes uncomplicated | 591 (40.1) | 505 (38.8) | 0.025 | 436 (38.9) | 446 (39.8) | 0.018 |
| Diabetes complicated | 361 (24.5) | 334 (25.7) | 0.028 | 266 (23.7) | 291 (25.9) | 0.052 |
| Hemiplegia or paraplegia | 682 (46.2) | 511 (39.3) | 0.140 | 478 (42.6) | 461 (41.1) | 0.031 |
| Metastatic solid tumor | 23 (1.6) | 26 (2.0) | 0.033 | 15 (1.3) | 19 (1.7) | 0.029 |
| Mild liver disease | 85 (5.8) | 76 (5.8) | 0.004 | 57 (5.1) | 69 (6.1) | 0.046 |
| Moderate to severe liver disease | – | – | 0.037 | – | – | 0.057 |
| Peptic ulcer disease | 28 (1.9) | 16 (1.2) | 0.054 | 16 (1.4) | 14 (1.2) | 0.016 |
| Peripheral vascular disease | 489 (33.2) | 366 (28.2) | 0.109 | 349 (31.1) | 321 (28.6) | 0.055 |
| Renal disease | 370 (25.1) | 347 (26.7) | 0.037 | 294 (26.2) | 293 (26.1) | 0.002 |
| Rheumatoid disease | 102 (6.9) | 52 (4.0) | 0.129 | 61 (5.4) | 50 (4.5) | 0.045 |
| Other comorbidities | ||||||
| Hypertension complicated | 486 (32.9) | 456 (35.1) | 0.045 | 374 (33.3) | 386 (34.4) | 0.023 |
| Hypertension uncomplicated | 1347 (91.3) | 1176 (90.5) | 0.030 | 1029 (91.7) | 1021 (91.0) | 0.025 |
| Obesity | 429 (29.1) | 295 (22.7) | 0.146 | 288 (25.7) | 265 (23.6) | 0.048 |
| Valvular disease | 752 (51.0) | 603 (46.4) | 0.092 | 559 (49.8) | 528 (47.1) | 0.055 |
| Hyperlipidemia | 1235 (83.7) | 1075 (82.7) | 0.028 | 946 (84.3) | 929 (82.8) | 0.041 |
| Obstructive sleep apnea | 194 (13.2) | 161 (12.4) | 0.023 | 141 (12.6) | 141 (12.6) | <0.001 |
| Nicotine dependence | 280 (19.0) | 222 (17.1) | 0.050 | 201 (17.9) | 195 (17.4) | 0.014 |
| Cigarette smoking | 217 (14.7) | 168 (12.9) | 0.052 | 157 (14.0) | 147 (13.1) | 0.026 |
An en rule (–) denotes that one or more values have been suppressed to mask counts within the 1–10 range in adherence to patient privacy guidelines.
DRGs 023 and 024 involve cases of craniotomy with major device implant or an acute complex central nervous system principal diagnosis. DRG 024 pertains to cases without MCC, whereas DRG 023 pertains to cases with MCC.
Data sets were balanced via a nearest neighbors algorithm using propensity scores, which were obtained via logistic regressions. Comorbidities and summary measures were determined based on all patient diagnoses from 1 year prior to the index admission up to the date of index discharge. Adequate balance required |SMD| <0.10 for all listed covariates. The three severity categories as well as cases with DRGs 023 and 024 were perfectly balanced.
CC: With complication or comorbidity; COPD: Chronic obstructive pulmonary disease; DRG: Diagnosis related group; ILR: Implantable loop recorder; MCC: With major complication or comorbidity; MCOT: Mobile cardiac outpatient telemetry; n: Patient count; |SMD|: Absolute standardized mean difference; SNF: Skilled nursing facility; WOCC: Without complication or comorbidity.
The resulting outcomes analyzed in this study were average total healthcare costs; survival at the end of the 18-month follow-up period; and inpatient readmissions, more precisely, the rates of patients who had one or more inpatient hospital readmissions during follow-up. These outcomes were compared between covariate balanced groups of the patients monitored with ILR and of the patients monitored with MCOT.
Readmissions were defined as any hospital inpatient admission during the 18-month post-index period, excluding the index stay. These were grouped into three categories based on the triage/acuity types reported as follows.
All inpatient: all inpatient hospital admissions, including those with unreported or unknown acuity.
Inpatient non-elective: hospital inpatient admissions reported as urgent, emergent or via a trauma center.
Inpatient emergency: hospital inpatient admissions reported as emergent or via a trauma center.
The definitions of urgent, emergent and trauma center correspond to those outlined in the CMS Manual System [24].
Additionally, readmissions were analyzed according to three cause categories: all cause, cerebrovascular, which includes diagnoses within any of the ICD-10-CM groups I60-I69, all of which correspond to cerebrovascular diseases and cerebral infarction, which includes diagnoses specifically in the ICD-10-CM I63 group. For this study, the cause of readmission was determined solely by the first listed diagnosis.
The readmissions analysis compared unique patient readmissions between the groups; that is, the measured unit corresponded to patients readmitted and each patient was counted at most once. For each cause and admission type combination, rates and adjusted probabilities of readmission were analyzed. These rates correspond to the simple proportion of patients readmitted during the 18-month follow-up period, whereas the adjusted probabilities were estimated using cox proportional hazard (CPH) regressions [35–37]. Hazard ratios (HRs) obtained from these regressions were used to assess statistical differences in readmissions between the device groups.
Survival and adjusted survival were computed for the end of the 18th month post-index. The estimates for adjusted survival were obtained via the failure function and estimated cumulative hazards derived using CPH regressions. HRs obtained from these regressions were used to assess statistical differences in survival, or more precisely, mortality, between the device groups.
Costs provided in the CDM are standardized figures, which, according to the documentation, were derived using proprietary algorithms. Per the data descriptions, these standardized costs are intended to reflect the intensity of care provided and to facilitate comparisons by equating cost differences to variations in utilization [38]. These costs should be interpreted as the sum of all payments made to healthcare providers, including amounts paid by the primary insurer, any coinsurance, and any payments made by the beneficiary. All cost amounts correspond to 2022 US Dollars.
In this analysis, healthcare costs refer to the sum of all costs in the CDM within the specified event or timeframe, associated with the patient. This also applies to costs for the year preceding the index admission, which are used as a baseline characteristic. For outcomes comparisons, costs were aggregated in three different ways:
1.
Index to end of follow-up: includes all costs reported from the date of the index admission through the end of the follow-up.
2.
Index visit: includes all costs directly associated with the index hospitalization.
3.
Follow-up: corresponds to the difference between the index to end of follow-up cost and the index visit cost.
Generalized linear model (GLM) gamma regressions with log-links were used to estimate and compare average costs between the groups [8,39–41]. To account for differences in survival, where they existed, inverse probability of survival weights, computed using CPH regressions, were incorporated into the cost regressions. For all GLM and CPH regressions, the following covariates were considered for inclusion as confounding variables: age, length of stay (LOS), two Charlson summary measures (comorbidity count, and age-adjusted score), year prior cost, sex, discharge to location, admission to an intensive care unit, major surgery, the 17 Charlson comorbidities, 8 additional comorbidities, DRG severity and the craniotomy DRGs (as applicable). However, to ensure successful execution, the final set of covariates included in each regression were algorithmically selected based on the number of observations, variance, mutual information and explanatory ability. Age-adjusted Charlson comorbidity score was included in all regressions [27,29].
Throughout the analysis, Wald's tests were used for hypothesis testing involving HRs. In all these cases, the null hypothesis was Ho: HR = 1. For all ratios, the numerator corresponded to the ILR group and the denominator to MCOT group. 95% confidence intervals (CIs) for all HRs were constructed using Wald's method. For averages, differences were evaluated using Student's t-test. P-values less than 0.05 were used to determine statistical significance throughout the study. Bootstrapping with replacement methods were used to estimate the 95% CIs for the differences in costs and for the CPH survival functions. Eicker-Huber-White heteroskedasticity-consistent standard errors, specifically the HC3 variant, were used in all hypothesis tests and CIs calculations.
All data processing and statistical analysis was conducted using Python (Python Software Foundation, DE, USA) version 3.10 [42].
Results
Patient & index characteristics
Patient demographics and characteristics by monitoring method before and after covariate balancing are provided in Tables 1 and 2.
| Unbalanced | Balanced | |||||
|---|---|---|---|---|---|---|
| ILR | MCOT | All | ILR | MCOT | All, n (%) | |
| Patients (n) | 1475 | 1300 | 2775 | 1122 | 1122 | 2244 |
| Days index to device (mean) | 5.98 | 11.73 | 8.67 | 5.86 | 12.02 | 8.94 |
| Days discharge to device (mean) | 1.59 | 8.33 | 4.75 | 2.06 | 8.4 | 5.23 |
| ILR, n (%) | MCOT, n (%) | All, n (%) | ILR, n (%) | MCOT, n (%) | All, n (%) | |
| Device before discharge | 1209 (82.0) | 438 (33.7) | 1647 (59.4) | 900 (80.2) | 378 (33.7) | 1278 (57.0) |
| DRG cluster: 040, 041, 042 | 1083 (73.4) | – (<1.0) | ∼1090 (∼39.0) | 816 (72.7) | – (<1.0) | ∼820 (∼37.0) |
| DRG cluster: 061, 062, 063 | 40 (2.7) | ∼140 (∼11.0) | ∼180 (∼7.0) | 30 (2.7) | ∼130 (∼11.0) | ∼160 (∼7.0) |
| DRG cluster: 064, 065, 066 | 256 (17.4) | 1098 (84.5) | 1354 (48.8) | 219 (19.5) | 936 (83.4) | 1155 (51.5) |
An en rule (–) denotes that one or more values have been suppressed to mask counts within the 1–10 range in adherence to patient privacy guidelines. A tilde (∼) denotes that an approximate value in lieu of the exact value was provided to prevent the reconstruction of a masked count.
DRGs 040, 041 and 042 involve peripheral, cranial nerve, and other nervous system procedures.
DRGs 061, 062 and 063 involve ischemic stroke, precerebral occlusion or transient ischemia with thrombolytic agent.
DRGs 064, 065 and 066 involve intracranial hemorrhage or cerebral infarction.
DRG: Diagnostic-related group; ILR: Implantable loop recorder; MCOT: Mobile cardiac outpatient telemetry.
Table 1 contains summary statistics for patient and index stay characteristics that were considered for balance. The left side of the table accounts for all 2775 patients that met the inclusion criteria prior to the balancing process: 1475 for ILR and 1300 for MCOT. The average age of patients utilizing ILR (72.91) was 2.88 years younger than those on MCOT (75.79). MCOT had a higher proportion of female patients (54 vs 52%). The mean LOS of the index hospitalization for patients with ILR (4.40 days) was a full day longer than MCOT (3.40 days). Overall, most index hospitalizations for both monitoring methods included emergency admissions (ILR 85.6%, MCOT 86.8%), with an average of 3.67 Charlson comorbidities in the ILR group, and 3.53 in the MCOT group. These comorbidities, found in Table 1, are most prominently cerebrovascular disease, hemiplegia/paraplegia, diabetes and renal disease.
The number of patients in the data set after balancing was 2244 (Table 1, right side), divided equally between the device groups (ILR 1122, MCOT 1122 patients). The difference in age between the groups decreased from nearly 3 years to under 0.3 years, though ILR patients were still younger on average. The difference in LOS for the index hospitalization was reduced to under one fifth of a day. The three severity categories became equally represented in both device groups (308, 618 and 196 patients in the WOCC, CC and MCC subgroups, respectively, for MCOT and ILR). According to |SMD| values, differences between the groups with respect to Charlson age-adjusted scores, comorbidity counts, demographics and most other covariates were further reduced. Exceptions were year prior costs, the index year of 2019, hyperlipidemia and four Charlson comorbidities for which there were slight difference increases. The criteria for adequate balance, |SMD| <0.10, was met in all instances (Table 1, last column).
Table 2 provides descriptive statistics for characteristics that were not targeted for balance, including the timing to device initiations and the distribution of patients across the different DRG clusters. The majority of ILR patients were discharged with a DRG in the 040–042 cluster (73% in both the unbalanced and balanced datasets), whereas the majority of MCOT patients were discharged with a DRG in the 064–066 cluster (85% and 83% in the unbalanced and balanced datasets, respectively). Most device initiations in the ILR group took place before discharge (>80% in the unbalanced and balanced datasets) whereas this was only the case for the minority of MCOT patients (34% in both unbalanced and balanced datasets).
Patients readmitted
Results for the readmissions analysis are shown in Table 3. When considering all-cause readmissions of any type across all patients, those in the MCOT group were less likely to be readmitted (30.2%) compared with ILR (35.4%) (HR 1.23; 95% CI: 1.04–1.46; p = 0.016). All-cause readmissions of any type were significantly lower for MCOT patients within the MCC severity subgroup (33.7% vs 46.7%; HR 1.59; 95% CI: 1.10–2.28; p = 0.012), but not significantly lower for the WOCC and CC subgroups. All-cause emergency readmissions were also significantly lower for MCOT patients in the CC and MCC subgroups (HR 1.32; 95% CI: 1.00–1.74; p = 0.046; and HR 1.77; 95% CI: 1.14–2.76; p = 0.011; respectively), while there was no significant difference between MCOT and ILR for patients in the WOCC subgroup.
| Observed rates | Adjusted probabilities | HRs | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Severity | Cause | Admission type | ILR (%) | MCOT (%) | ILR (%) | MCOT (%) | HR | HR, 95% CI | p-value |
| All patients ILR, n: 1122 MCOT, n: 1122 | All cause | Inpatient | 39.2 | 34.3 | 35.4 | 30.2 | 1.23† | (1.04, 1.46) | 0.016 |
| Inp. Non-elect. | 34.0 | 28.5 | 31.5 | 25.8 | 1.29† | (1.07, 1.55) | 0.008 | ||
| Inp. Emerg. | 30.7 | 25.0 | 28.8 | 23.2 | 1.31† | (1.06, 1.62) | 0.012 | ||
| Cerebrovascular I60–169 | Inpatient | 15.2 | 10.4 | 15.7 | 10.7 | 1.53† | (1.20, 1.96) | <0.001 | |
| Inp. Non-elect. | 12.1 | 8.6 | 12.8 | 9.1 | 1.46† | (1.11, 1.91) | 0.006 | ||
| Inp. Emerg. | 10.7 | 7.7 | 11.4 | 8.1 | 1.45† | (1.07, 1.98) | 0.018 | ||
| Cerebral infarction I63 | Inpatient | 11.9 | 7.6 | 12.7 | 8.0 | 1.65† | (1.26, 2.16) | <0.001 | |
| Inp. Non-elect. | 11.1 | 7.1 | 11.9 | 7.5 | 1.63† | (1.23, 2.17) | <0.001 | ||
| Inp. Emerg. | 9.9 | 6.4 | 10.6 | 6.8 | 1.60† | (1.18, 2.17) | 0.002 | ||
| WOCC ILR, n: 308 MCOT, n: 308 | All cause | Inpatient | 26.9 | 28.2 | 24.0 | 25.4 | 0.93 | (0.63, 1.38) | 0.726 |
| Inp. Non-elect. | 22.1 | 23.1 | 20.1 | 21.5 | 0.92 | (0.60, 1.42) | 0.721 | ||
| Inp. Emerg. | 19.8 | 21.1 | 18.3 | 19.8 | 0.91 | (0.58, 1.42) | 0.682 | ||
| Cerebrovascular I60–169 | Inpatient | 13.0 | 10.4 | 12.8 | 10.4 | 1.26 | (0.68, 2.36) | 0.463 | |
| Inp. Non-elect. | 9.7 | 8.8 | 9.9 | 8.9 | 1.13 | (0.59, 2.18) | 0.710 | ||
| Inp. Emerg. | 9.4 | 8.1 | 9.4 | 8.4 | 1.14 | (0.48, 2.66) | 0.770 | ||
| Cerebral infarction I63 | Inpatient | 10.1 | 7.8 | 10.3 | 7.9 | 1.33 | (0.74, 2.40) | 0.342 | |
| Inp. Non-elect. | 9.7 | 7.8 | 10.0 | 7.9 | 1.29 | (0.69, 2.42) | 0.431 | ||
| Inp. Emerg. | 9.4 | 7.1 | 9.3 | 7.5 | 1.27 | (0.58, 2.77) | 0.555 | ||
| CC ILR, n: 618 MCOT, n: 618 | All cause | Inpatient | 41.3 | 36.2 | 36.7 | 31.2 | 1.24 | (0.99, 1.56) | 0.062 |
| Inp. Non-elect. | 35.9 | 30.7 | 33.0 | 27.3 | 1.28† | (1.00, 1.62) | 0.045 | ||
| Inp. Emerg. | 32.0 | 26.2 | 29.9 | 24.0 | 1.32† | (1.00, 1.74) | 0.046 | ||
| Cerebrovascular I60–169 | Inpatient | 16.0 | 10.2 | 16.3 | 10.2 | 1.70† | (1.23, 2.34) | 0.001 | |
| Inp. Non-elect. | 13.3 | 9.1 | 13.9 | 9.3 | 1.55† | (1.09, 2.21) | 0.014 | ||
| Inp. Emerg. | 11.5 | 7.9 | 12.2 | 8.3 | 1.53† | (1.01, 2.31) | 0.044 | ||
| Cerebral infarction I63 | Inpatient | 12.8 | 7.9 | 13.4 | 8.3 | 1.69† | (1.18, 2.41) | 0.004 | |
| Inp. Non-elect. | 12.1 | 7.4 | 12.8 | 7.8 | 1.71† | (1.19, 2.46) | 0.004 | ||
| Inp. Emerg. | 10.5 | 6.8 | 11.3 | 7.2 | 1.63† | (1.09, 2.45) | 0.017 | ||
| MCC ILR, n: 196 MCOT, n: 196 | All cause | Inpatient | 52.0 | 37.8 | 46.7 | 33.7 | 1.59† | (1.10, 2.28) | 0.012 |
| Inp. Non-elect. | 46.4 | 30.1 | 42.8 | 28.0 | 1.78† | (1.15, 2.77) | 0.010 | ||
| Inp. Emerg. | 43.4 | 27.6 | 40.1 | 26.0 | 1.77† | (1.14, 2.76) | 0.011 | ||
| Cerebrovascular I60–169 | Inpatient | 16.3 | 11.2 | 17.5 | 11.9 | 1.54 | (0.81, 2.92) | 0.191 | |
| Inp. Non-elect. | 12.2 | 7.1 | 13.2 | 7.8 | 1.74 | (0.93, 3.28) | 0.084 | ||
| Inp. Emerg. | 10.2 | 6.1 | 11.0 | 6.8 | 1.68 | (0.84, 3.37) | 0.146 | ||
| Cerebral infarction I63 | Inpatient | 12.2 | 6.1 | 13.7 | 6.6 | 2.18† | (1.10, 4.30) | 0.025 | |
| Inp. Non-elect. | 10.2 | 5.1 | 11.9 | 5.6 | 2.25† | (1.07, 4.69) | 0.031 | ||
| Inp. Emerg. | 8.7 | 4.1 | 9.7 | 4.5 | 2.27† | (1.04, 4.98) | 0.041 | ||
†
Statistically significant at the 0.05 level.
I60–I69 refer to the ICD-10-CM range of diagnosis code groups for cerebrovascular diseases. I63 refers to the group of diagnosis codes specific to cerebral infarctions.
Adjusted probabilities and hazard statistics were estimated using Cox proportional hazards regressions while controlling for demographics, index event and stay characteristics and patients' health profiles. Observed rates correspond to the simple proportions of patients who were readmitted during the follow-up period. Only the first readmission, if any, for each patient was counted in all calculations.
Hazard ratio: (hazard in ILR group) / (hazard in MCOT group).
95% CIs were estimated using Wald's method.
p-values correspond to Wald's test.
Heteroskedasticity-consistent standard errors were used for hypothesis tests and confidence intervals.
CC: With complication or comorbidity; CI: Confidence interval; CPH: Cox proportional hazards; Emerg.: Emergency; HR: Hazard ratio; ILR: Implantable loop recorder; Inp.: Inpatient; MCC: With major complication or comorbidity; MCOT: Mobile cardiac outpatient telemetry; N: Count; Non-elect.: Non-elective; WOCC: Without complication or comorbidity.
Cerebrovascular readmissions of any type across all patients showed a similar pattern; patients in the MCOT group had fewer readmissions than those in the ILR group (ILR 15.7%, MCOT 10.7%; HR 1.53; 95% CI: 1.20–1.96; p < 0.001). While there was no significant difference in this readmissions category between MCOT and ILR for patients in the WOCC or MCC subgroups, ILR patients in the CC subgroup were more likely to be readmitted (HR 1.70; 95% CI: 1.23–2.34; p < 0.001). Emergency readmissions for cerebrovascular causes were significantly lower for MCOT monitored patients overall (HR 1.45; 95% CI: 1.07–1.98; p = 0.018) and in the CC subgroup (HR 1.53; 95% CI: 1.01–2.31; p = 0.044).
Readmissions specific to cerebral infarction across all patients were significantly lower in the MCOT monitored group (8.0%) compared with ILR (12.7%) (HR 1.65; 95% CI: 1.26–2.16; p < 0.001), with fewer emergency readmissions (HR 1.60; 95% CI: 1.18–2.17; p = 0.002). As in the broader cerebrovascular group, there was no significant difference between MCOT and ILR monitored patients in the WOCC subgroup. However, overall readmissions specific to cerebral infarction in the CC and MCC subgroups were significantly lower for MCOT monitored patients than for ILR monitored patients (HR 1.69; 95% CI: 1.18–2.41; p = 0.004 for CC; and HR 2.18; 95% CI: 1.10–4.30; p = 0.025 for MCC), and also with respect to emergency readmissions (HR 1.63; 95% CI: 1.09–2.45; p = 0.017 for CC; and HR 2.27; 95% CI: 1.04–4.98; p = 0.041 for MCC).
Numerically, in the WOCC subgroup, patients monitored with ILR had relatively fewer all cause readmissions than MCOT monitored patients across admission types; however, none of these differences showed statistical significance (HR 0.93; 95% CI: 0.63–1.38; p = 0.726 for all inpatient; HR 0.92; 95% CI: 0.60–1.42; p = 0.721 for non-elective; and HR 0.91; 95% CI: 0.58–1.42; p = 0.682 for emergency).
Healthcare costs
The results from the cost analysis are reported in Table 4; these correspond to the GLM gamma regression adjusted standardized costs denoted in 2022 US Dollars. Across all patients, the adjusted average cost from the initial admission to the end of the 18-month follow-up period was $27,429 less for patients in the MCOT group compared with the ILR group (95% CI: $22,353–$32,633; p < 0.001). Costs for patients in the MCOT group were also lower both with respect to the index visit (difference $19,424; 95% CI: $17,896–$21,110; p < 0.001), and also with respect to follow-up care (difference $9,825, CI; $4,512–$14,825; p < 0.001), when compared with those in the ILR group. Broken down by the severity category of the index event, the total cost from index to end of follow-up was lower for the MCOT patient groups; specifically, these costs were $21,503 (95% CI: $14,322–$29,661; p < 0.001), $28,810 (95% CI: $22,619–37,301; p < 0.001), and $35,528 (95% CI: $22,382–$51,648; p < 0.001) lower for MCOT patients in the WOCC, CC and MCC subgroups, respectively. Similarly, index visit costs were $14,298 (95% CI: $12,606–$15,840; p < 0.001), $17,917 (95% CI: $15,686–$20,331; p < 0.001), and $28,918 (95% CI: $22,376–$34,892; p < 0.001) lower for MCOT patients in the WOCC, CC and MCC subgroups, respectively. Follow-up costs were significantly lower for MCOT patients in the CC subgroup (difference $12,161; 95% CI: $6,026–$19,805; p < 0.001), but, while trending lower, no statistically significant differences were associated with the WOCC and MCC subgroups.
| ILR | MCOT | Difference | Difference 95% CI | p-value | |
|---|---|---|---|---|---|
| Index to end of follow-up | |||||
| All patients | 111,896 | 84,467 | 27,429† | (22,353, 32,633) | <0.001 |
| WOCC | 79,970 | 58,467 | 21,503† | (14,322, 29,661) | <0.001 |
| CC | 114,400 | 85,590 | 28,810† | (22,619, 37,301) | <0.001 |
| MCC | 154,994 | 119,736 | 35,258† | (22,382, 51,648) | <0.001 |
| Index visit | |||||
| All patients | 52,837 | 33,413 | 19,424† | (17,896, 21,110) | <0.001 |
| WOCC | 33,737 | 19,439 | 14,298† | (12,606, 15,840) | <0.001 |
| CC | 52,135 | 34,218 | 17,917† | (15,686, 20,331) | <0.001 |
| MCC | 82,429 | 53,511 | 28,918† | (22,376, 34,892) | <0.001 |
| Follow-up | |||||
| All patients | 60,443 | 50,618 | 9825† | (4512, 14,825) | <0.001 |
| WOCC | 46,400 | 39,488 | 6912 | (-878, 15,337) | 0.078 |
| CC | 63,414 | 51,253 | 12,161† | (6026, 19,805) | <0.001 |
| MCC | 77,078 | 63,195 | 13,883 | (-988, 30,248) | 0.053 |
Index to end of follow-up refers to all costs from the date of index admission to the end of follow-up; Index visit includes all costs associated with the initial hospitalization; Follow-up cost is the difference between Index to End of follow-up and index visit cost.
†
Statistically significant at the 0.05 level.
Patient counts: ILR (WOCC: 308, CC: 618, MCC: 196, Total ILR: 1122), MCOT (WOCC: 308, CC: 618, MCC: 196, Total MCOT: 1122)
Means and differences in means were estimated using GLM gamma regressions while controlling for demographics, index event and stay characteristics, patients' health profiles and survival when applicable.
95% CIs were estimated using bootstrapping methods.
p-values correspond to Student's t-test.
Heteroskedasticity-consistent standard errors were used for hypothesis tests and confidence intervals.
CC: With complication or comorbidity; CI: Confidence interval; GLM: Generalized Linear Model; ILR: Implantable loop recorder; MCC: With major complication or comorbidity; MCOT: Mobile cardiac outpatient telemetry; WOCC: Without complication or comorbidity.
Survival
As reported in Table 5 and shown in Figure 2A, across all patients, adjusted survival for the 18 months after index was numerically higher in the MCOT group (91.1%) compared with the ILR group (88.7%), however, this difference did not meet the established significance standard (HR 1.30; 95% CI: 1.00–1.69; p = 0.051) (Table 5). Figure 2B shows a slightly higher numerical survival for ILR among WOCC patients with a substantial 95% CI: overlap. The trend toward improved survival was driven by a statistically significantly lower mortality among MCOT patients in the CC subgroup (ILR 11.5%, MCOT 7.5%; HR 1.62; 95% CI: 1.11–2.36; p = 0.012) (Table 5 & Figure 2C). There were no statistically significant differences in survival, or more precisely, in mortality, between the two device groups within the WOCC (HR 0.86; 95% CI: 0.46–1.61; p = 0.632), and the MCC (HR 1.04; 95% CI: 0.66–1.66; p = 0.855) subgroups. For the MCC subgroup, survival is virtually indistinguishable between the MCOT and ILR groups, as indicated by the almost complete overlap of the 95% CIs in Figure 2D.
| Patient counts | Observed 18 m. survival | Adjusted 18 m. survival | Adjusted 18 m. mortality | Hazard ratios | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ILR | MCOT | ILR (%) | MCOT (%) | ILR (%) | MCOT (%) | ILR % | MCOT (%) | HR | HR, 95% CI | p-value | |
| All patients | 1122 | 1122 | 88.8 | 90.8 | 88.7 | 91.1 | 11.3 | 8.9 | 1.30 | (1.00, 1.69) | 0.051 |
| WOCC | 308 | 308 | 94.2 | 93.8 | 94.5 | 93.6 | 5.5 | 6.4 | 0.86 | (0.46, 1.61) | 0.632 |
| CC | 618 | 618 | 88.5 | 92.2 | 88.5 | 92.5 | 11.5 | 7.5 | 1.62† | (1.11, 2.36) | 0.012 |
| MCC | 196 | 196 | 81.1 | 81.6 | 81.3 | 82.0 | 18.7 | 18.0 | 1.04 | (0.66, 1.66) | 0.855 |
†
Statistically significant at the 0.05 level.
Adjusted survival, mortality and hazard statistics were estimated using CPH regressions while controlling for demographics, index event and stay characteristics and patients' health profiles. Observed survival correspond to the simple proportions of patients who survived the 18 month post-index period.
Hazard Ratio = (Hazard in ILR group) / (Hazard in MCOT group).
HR 95% CIs were estimated using Wald's method and p-values correspond to Wald's test.
Heteroskedasticity-consistent standard errors were used for hypothesis tests and confidence intervals.
18 m: 18-month; CC: With complication or comorbidity; CI: Confidence interval; CPH: Cox Proportional Hazards; HR: Hazard ratio; ILR: Implantable loop recorder; MCC: With major complication or comorbidity; MCOT: Mobile cardiac outpatient telemetry; WOCC: Without complication or comorbidity.
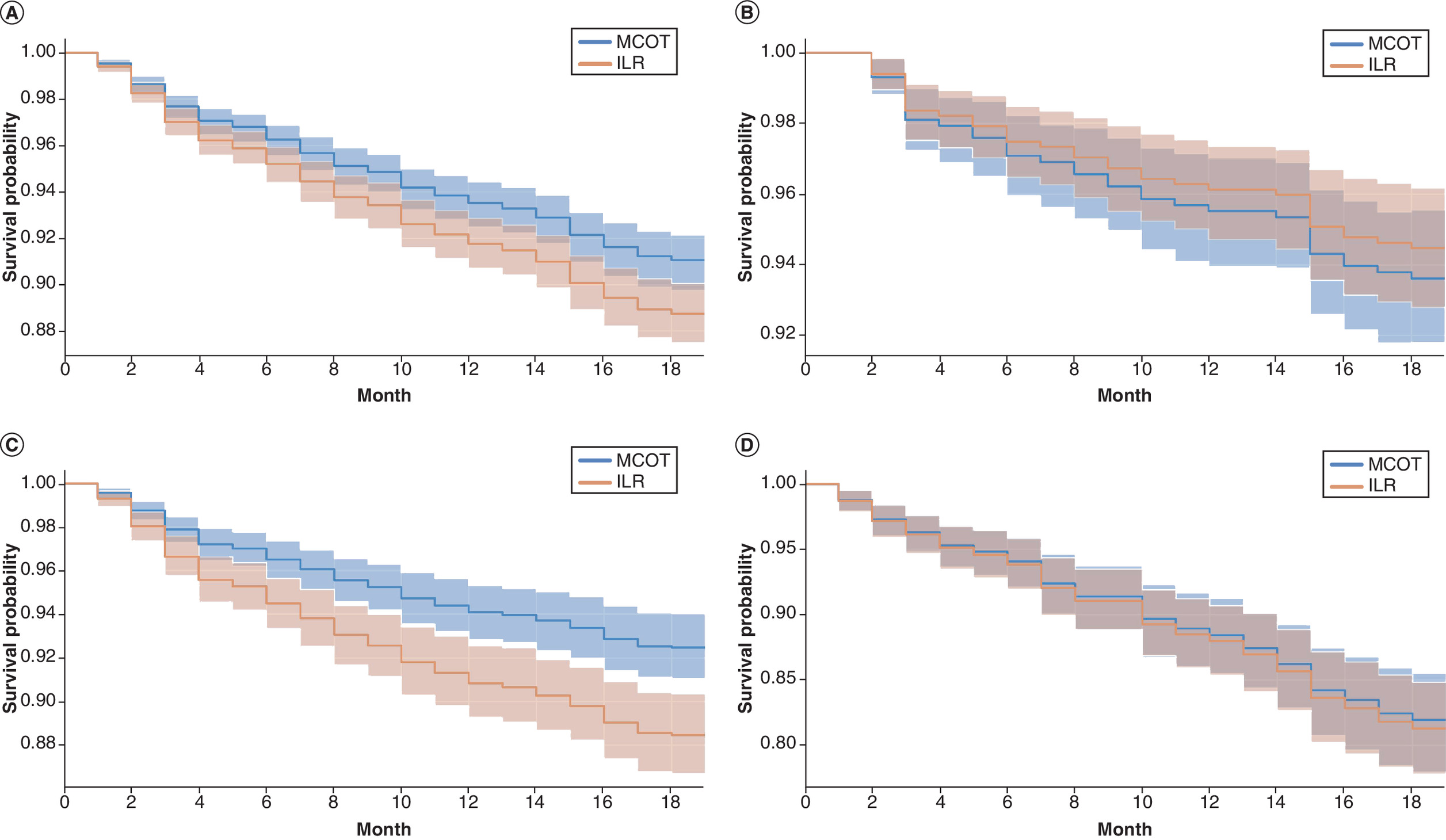
Figure 2. Cox proportional hazards adjusted survival for implantable loop recorder and mobile cardiac outpatient telemetry patients.
(A) CPH adjusted survival ILR versus MCOT. All severities. (B) CPH adjusted survival ILR versus MCOT. severity; WOCC. (C) CPH adjusted survival ILR versus MCOT. Severity; CC. (D) CPH adjusted survival ILR versus MCOT. Severity; MCC . Survival rates were calculated for each of the 18 months post-index using CPH regressions, taking into account demographics, health profiles, and index hospitalization details. Shaded areas represent 95% confidence intervals. To mitigate bias from differences in device initiation timing, patients who died in the index month were excluded throughout the analysis.
CC: With complication or comorbidity; CPH: Cox proportional hazards; ILR: Implantable loop recorder; MCC: With major complication or comorbidity; MCOT: Mobile cardiac outpatient telemetry; WOCC: Without complication or comorbidity.
Discussion
The findings of this study address several gaps in the literature and add to the body of existing evidence by quantifying readmission rates and emergency department utilization, providing data on patient survival and clinical outcomes, and offering a more recent insight into the economic burden of stroke in this patient population. The authors compared common methods of post-stroke discharge monitoring in the US – MCOT and ILR. It revealed that MCOT monitoring was associated with significantly fewer hospital readmissions and lower total cost of care. Readmissions were 5% lower for the MCOT patient group, with similar reductions in readmissions specific to cerebrovascular and cerebral infarct care. A concomitant reduction in emergency department utilization of 5% was also shown. Total costs for the stroke admission and the following 18 months were found to be $27,429 lower for those monitored with MCOT, including $9,825 lower costs for post-discharge care. Overall patient survival throughout the 18 months following discharge was numerically superior for those monitored with MCOT and it reached statistically significant levels within the subgroup that experienced CC during their initial stroke hospitalization.
The benefit of long-term monitoring for AF in patients post-stroke has been previously established in the literature [13]. Prior studies have predominantly concentrated on the length of monitoring time, detection of AF, the initiation frequency of oral anticoagulation therapy and rates of stroke recurrence.
The STROKE-AF trial, a randomized trial involving 496 patients with IS from large- or small-vessel disease, demonstrated 1-year post-stroke AF detection rate of 12.1% in patients monitored with ILR, in stark contrast to 1.8% in those receiving site-specific conventional care (including 12-lead EKG, Holter or event recorders). However, the incidence of new stroke at 12 months did not differ significantly. The study found 7.2% IS recurrence for the ILR group versus 9.8% for the control group, with a p-value of 0.30 [43]. Similarly, the PER-DIEM trial, comparing the efficacy of ILR with that of external loop recorders (ELR) in 300 patients with recent IS, found a 12-month AF detection rate of 15.3% in the ILR group compared with 4.7% in the ELR group. Yet, it also reported no significant difference in stroke recurrence rates between groups, with 3.3% for ILR and 5.3% for ELR, with a p-value of 0.40 [44]. In a retrospective analysis from 2023, Boriani et al. evaluated the effectiveness of ILR versus external cardiac monitors (including short-term Holter monitors, event monitors, and MCOT) using Medicare insurance claims data in IS patients. This study observed a higher two-year AF detection rate in the ILR-monitored patients (33.9%) compared with those with external devices (13.3%). Despite the higher detection rate, the rate of recurrent strokes was slightly lower in the group with externally-worn monitoring (7.9%) than in the ILR group (8.4%), with a marginal difference in mortality rates (11.1% for external monitors vs 9.1% for ILR) [45]. Across these studies, a higher propensity for anticoagulant initiation was noted in ILR groups. Although increased detection of AF and initiation of anticoagulation therapy were achieved through long-term cardiac monitoring, a significant reduction in recurrent strokes has not been conclusively shown, underscoring the need for continued research in the treatment and prevention of secondary strokes in this patient population.
In addition to identifying AF in this population, research indicates there is a correlation between multimorbidity and complications and elevated mortality rates in both the short and long term. The estimated prevalence of multimorbidity among stroke patients ranges from 43% to 94% [46]. Nonetheless, the link between multimorbidity in stroke and its health-related outcomes remains limited, which is in part due to the ongoing need to refine the definitions of comorbidity and multimorbidity, including whether to incorporate risk factors and stroke sequalae within these definitions [46].
In patients monitored with MCOT post-stroke, survival trended toward improvement when including patients of all stroke severities compared with ILR monitored patients, a finding driven by statistically significant lower mortality among MCOT prescribed patients in the CC subgroup. Possible explanations for this finding could be due to differences in the detection methods, with MCOT detecting AF of shorter durations and allowing for near real-time notifications, compared with the generally longer durations required to detect AF with ILR (>2 min) and delayed event transmission and analysis inherent with ILR data communications. The etiology of this observation should be investigated further given the relevance of potentially impacting mortality post-stroke.
The significant effects upon readmissions associated with MCOT monitoring were strongly evident across all patients in this study, and most evident in all-cause, cerebrovascular, and cerebral infarction diagnosis. Interestingly, the significance within each of the readmission causes was driven by patients who suffered complications post-stroke (all-cause driven by the MCC subgroup, cerebrovascular caused readmissions driven by CC subgroup and cerebral infarction driven by both CC and MCC subgroups).
Perhaps a timelier intervention stemming from detection of other rhythms by MCOT precipitated more effective outpatient treatment. Of import, not only were inpatient admissions seen less frequently with the MCOT group, but the costlier emergency visits were significantly less frequent for all stroke severities and readmission causes in this group; predominantly driven by improvements in the CC and MCC subgroups. Further analysis to better understand readmission rates and survival trends in this population is warranted.
The most understandable component of this analysis is the resulting healthcare costs. Decreases in the index visits costs, significant across the entire MCOT group and each stroke severity subgroup. Costs attributed to the ILR purchase, $4,500–$6,000, and the increased procedural costs associated with the inpatient surgical placement of the ILR, would have an expected increase in costs for ILR over MCOT. Following discharge, the lower costs associated with MCOT are likely at least in part due to the reduced number of readmissions, particularly for expensive emergency readmissions of MCC subgroup with associated cerebral infarction, which occurred 53% less often with those using MCOT. Moreover, as ILRs are designed to last several years, with ongoing charges of up to $275 per month, total expenses would be expected to be higher compared with the one-time cost of MCOT, at approximately $900 [47].
Prior work from Medic et al. in 2021 found lower per-patient costs when monitoring with MCOT followed by ILR versus the use of ILR alone. In that study the cost per patient with detected AF was almost 8x lower than when ILR alone was used [47]. That study adds to previous work in this space by directly comparing the clinical and economic outcomes of the two methods used and exploring various scenarios where each might offer greater benefits, such as considering MCOT for use prior to the implantation of ILR, with ILR being reserved for patients in which MCOT did not identify AF.
The differences noted between MCOT and ILR with respect to readmissions, healthcare costs and survival could lie in the differential significance of AF identified on these distinctly different forms of monitoring. Data from the ASSERT trial, which monitored for AF with cardiac implantable devices (CIEDs) that continuously monitor for years, indicated that only AF episodes >24 hours in duration were significantly linked to an increased risk of stroke [48]. However, McIntyre et al. when modeling scenarios that predicted stroke risk from 14-day external monitors, found that episodes of AF lasting >6-minutes pose a recurrent stroke risk comparable to the episodes >24-h detected with CIEDs [49]. The disparity in AF duration in predicting stroke has been attributed to the varying degrees of AF burden and their associated risk. Thus, AF identified through sporadic, non-invasive monitoring modalities, even if shorter in duration, is representative of higher AF burden and higher risk when compared with longer duration AF events identified on ILR devices. Identification of AF, even brief episodes, detected on intermediate duration (30-day) monitoring modalities such as MCOT, may therefore represent AF of greater clinical relevance than AF reported by ILRs and thus factor into the findings on readmission, healthcare costs and survival noted in this analysis.
Strengths & limitations
The strengths of this study can be attributed to the authors' use of large-scale, real-world data sets with multi-year patient care continuity. The longitudinal continuity allowed for accurate identification and exclusion of patients with prior AF diagnoses, or incomplete claims records. Furthermore, the outcomes studied (readmissions, costs and survival) are visible in the data set analyzed. The authors did not rely on changes in the ICD-10 diagnostic codes over time, or the initiation of therapies, both of which are influenced by patient and physician preference. As a result, the reported values are applicable to the overall post-stroke monitoring patient population, not only those patients with measurable AF. As noted above there is little in the literature showing a causal link between monitoring, AF detection and improved patient outcomes.
This study is subject to limitations and risks of bias inherent to the utilization of data derived from claims databases. It is important to note that claims are considered retrospectively, and their primary purpose was for reimbursement [50]. Some of the documented potential biases include DRG or procedural upcoding and the underreporting of ICD-10 diagnoses not relevant to the payment [51,52]. Thus, the inability to determine the intent behind patient care limits conclusions that could be drawn with regard to detection and treatment for AF following these monitoring approaches.
Correspondingly, the lack of information regarding medical necessity, utility and more importantly non-futility, made a suitable non-ACM population difficult to identify. Analysis was not undertaken on the non-ACM population, and it is unknown how MCOT and ILR fare with respect to readmissions, healthcare costs and survival with respect to a non-ACM group.
It should be noted that despite the statistical strength and persistence of some observed patterns, this analysis alone cannot directly attribute the outcomes differences on readmissions, follow-up healthcare costs and survival to the choice of the ACM device. Future studies should aim to explore intermediate channels which may be linked to both the device and the outcomes.
Finally, the development of optimal strategies to exploit the advantages of both MCOT and ILR would benefit from a prospective study where patients potentially begin monitoring using MCOT before transitioning to long-term invasive monitoring with ILR if there is residual need. This could also help in establishing the temporal associations of AF development and whether it is a result of the stroke process or simply develops over time.
Conclusion
In this analysis of medical insurance claims following stroke hospitalization, compared with ILR, the use of MCOT as an arrhythmia monitor was associated with significant decreases in the rate of hospital readmissions, and reduced healthcare costs for both the index event and total costs incurred over the following 18 months. Additionally, MCOT monitored patients showed a noticeable trend toward improved survival that bordered on statistical significance across all patient stroke severities, driven by a significant reduction in mortality for patients who suffered complications and comorbidities during the index stroke admission.
The size of this study cohort and the significant differences in both readmission and cost of patient care merit its inclusion in the development of medical policy and the ongoing evolution of patient care following a stroke.
Summary points
•
Ambulatory cardiac monitoring is commonly undertaken to assess for atrial fibrillation (AF) after a stroke event so initiation of stroke prophylaxis can be considered.
•
The 2023 American Heart Association/American Stroke Association guidelines consider long-term monitoring to detect for recurrent AF beneficial, whether that be with either mobile cardiac outpatient telemetry (MCOT), implantable loop recorder (ILR) or another approach.
•
MCOT is an external method of arrhythmia monitoring for assessing the development of AF over the course of 30 days, while ILR is implanted through a minimally invasive procedure and monitors for AF over a period of several years.
•
This study utilized deidentified claims data included in the Optum’s de-identified Clinformatics® Data Mart Database from 2017 to 2020.
•
The study population included 2244 patients who were admitted for IS and were prescribed either MCOT or ILR monitors following discharge.
•
The analysis looked at overall trends and differences in patient outcomes based on the severity of their admission DRG code, grouping inpatient admissions by those without complications or comorbidities (WOCC), with complications and comorbidities (CC) and those with major complications and comorbidities (MCC).
•
Across all patients, the cost of the index visit for patients monitored with MCOT was $19,424 less than the initial visit for those monitored with ILR (p < 0.001), while across all severities, the total medical costs to the end of observation, excluding the index visit, were $9825 lower when MCOT was used as opposed to an ILR (p < 0.001).
•
Across all stroke admission severities, MCOT was associated with a lower mortality rate, which bordered on statistical significance (ILR 11.3%; MCOT 8.9%; HR 1.30; 95% CI 1:00–1.69; p = 0.051), while a significant reduction in mortality was observed in MCOT-monitored patients who suffered CC with the index stroke (MCOT 7.5%; ILR 11.5%; HR 1.62; 95% CI: 1.11– 2.36; p = 0.012).
•
Readmissions across patients were significantly lower for those monitored with MCOT (30.2%) than with ILR (35.4%) (HR 1.23; 95% CI: 1.04–1.46; p = 0.016)). Emergency readmissions due to cerebral infarction were significantly higher among ILR monitored patients than MCOT monitored patients in the CC (ILR 11.3%; MCOT 7.2%; HR 1.63; 95% CI: 1.09-2.45; p = 0.017), and MCC (ILR 9.76%; MCOT 4.5%; HR 2.27; 95% CI: 1.04-4.98; p = 0.041) severity categories.
Author contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Acknowledgments
Special thanks to M Kyriakakos from Veranex for providing drafting and editorial assistance in the preparation of the manuscript, N Mark and M Amarapala from Veranex for providing editorial assistance, and J Ferrara from Veranex for supporting in the conceptual guidance of the manuscript.
Financial disclosure
This study was funded by Koninklijke Philips NV, Amsterdam, Netherlands. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
G Medic, A Dunn, R Vazquez and V Norlock are the employees of Philips. Philips is a producer of MCOT. M Kyriakakos and C Siegfried are employees of Veranex. Veranex received funding from Philips to write the manuscript. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Writing support was provided by Veranex and was funded by Koninklijke Philips NV (Amsterdam, The Netherlands).
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary table.xlsx)
- Download
- 28.62 KB
References
1.
Tsao CW, Aday AW, Almarzooq ZI et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics – 2023 Update: a report from the American Heart Association. Circulation 147(8), e93–e621 (2023).
2.
Martin SS, Aday AW, Almarzooq ZI et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. 2024 Heart Disease and Stroke Statistics: a report of US and global data from the American Heart Association. Circulation 149(8), e347–e913 (2024).
3.
Wang G, Zhang Z, Ayala C, Dunet DO, Fang J, George MG. Costs of hospitalization for stroke patients aged 18–64 years in the United States. J. Stroke Cerebrovasc. Dis. 23(5), 861–868 (2014).
4.
Moraes MA, Jesus PAP, Muniz LS et al. Mortalidade por acidente vascular cerebral isquêmico e tempo de chegada a hospital: análise dos primeiros 90 dias. Rev. Esc. Enferm. USP 57, e20220309 (2023).
5.
Cardiogenic brain embolism. The second report of the Cerebral Embolism Task Force. Arch. Neurol. 46(7), 727–743 (1989).
6.
Stroke Risk in Atrial Fibrillation Working Group. Independent predictors of stroke in patients with atrial fibrillation: a systematic review. Neurology 69(6), 546–554 (2007).
7.
Vahidy FS, Donnelly JP, McCullough LD et al. Nationwide estimates of 30-day readmission in patients with ischemic stroke. Stroke 48(5), 1386–1388 (2017).
8.
Zhou LW, Lansberg MG, de Havenon A. Rates and reasons for hospital readmission after acute ischemic stroke in a US population-based cohort. PLOS ONE 18(8), e0289640 (2023).
9.
Joglar JA, Chung MK, Armbruster AL et al. Peer Review Committee Members. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 149(1), e1–e156 (2024).
10.
Sanna T, Diener HC, Passman RS et al. CRYSTAL AF Investigators. Cryptogenic stroke and underlying atrial fibrillation. N. Engl. J. Med. 370(26), 2478–2486 (2014).
11.
Gladstone DJ, Spring M, Dorian P et al. EMBRACE Investigators and Coordinators. Atrial fibrillation in patients with cryptogenic stroke. N. Engl. J. Med. 370(26), 2467–2477 (2014).
12.
Hermans ANL, Gawalko M, Dohmen L et al. Mobile health solutions for atrial fibrillation detection and management: a systematic review. Clin. Res. Cardiol. 111(5), 479–491 (2022).
13.
Sposato LA, Cipriano LE, Saposnik G et al. Diagnosis of atrial fibrillation after stroke and transient ischaemic attack: a systematic review and meta-analysis. Lancet Neurol. 14(4), 377–387 (2015).
14.
Kleindorfer DO, Towfighi A, Chaturvedi S et al. 2021 Guideline for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack: a Guideline From the American Heart Association/American Stroke Association. Stroke 52(7), e364–e467 (2021).
15.
LINQ II LNQ22. Clinical manual. Medtronic Inc, Dublin, Ireland (2022).
16.
LUX-Dx. User's manual. Boston Scientific Corporation, MA,USA (2019).
17.
Miller DJ, Khan MA, Schultz LR et al. Outpatient cardiac telemetry detects a high rate of atrial fibrillation in cryptogenic stroke. J. Neurol. Sci. 324(1–2), 57–61 (2013).
18.
Centers for Medicare & Medicaid Services. Billing and coding: electrocardiographic (EKG or ECG) monitoring (Holter or real-time monitoring). Article ID: A57576 (2023).
19.
Jiang H, Tan SY, Wang JK et al. A meta-analysis of extended ECG monitoring in detection of atrial fibrillation in patients with cryptogenic stroke. Open Heart 9(2), e002081 (2022).
20.
Zachrison KS, Li S, Reeves MJ et al. Strategy for reliable identification of ischaemic stroke, thrombolytics and thrombectomy in large administrative databases. Stroke Vasc. Neurol. 6(2), 194–200 (2021).
21.
Centers for Medicare & Medicaid Services. ICD-10-CM/PCS MS-DRG v37.0 definitions manual (2019). www.cms.gov/icd10m/version37-fullcode-cms/fullcode_cms/P0001.html
22.
Lévesque LE, Hanley JA, Kezouh A, Suissa S. Problem of immortal time bias in cohort studies: example using statins for preventing progression of diabetes. BMJ 340, b5087 (2010).
23.
Wang J, Peduzzi P, Wininger M, Ma S. Statistical methods for accommodating immortal time: a selective review and comparison. arXiv Available at: https://arxiv.org/abs/2202.02369 (2022).
24.
Centers for Medicare and Medicaid Services. CMS manual system pub 100-04 Medicare claims processing (2009). www.cms.gov/regulations-and-guidance/guidance/manuals/internet-only-manuals-ioms-items/cms018912
25.
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J. Chronic Dis. 40(5), 373–383 (1987).
26.
Quan H, Sundararajan V, Halfon P et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 43(11), 1130–1139 (2005).
27.
Austin SR, Wong YN, Uzzo RG, Beck JR, Egleston BL. Why summary comorbidity measures such as the Charlson Comorbidity Index and Elixhauser Score Work. Med. Care 53(9), e65–e72 (2015).
28.
Gasparini A. comorbidity: an R package for computing comorbidity scores. J. Open Source Software 3(23), 648 (2018).
29.
Zhang N, Lin Q, Jiang H, Zhu H. Age-adjusted Charlson Comorbidity Index as effective predictor for in-hospital mortality of patients with cardiac arrest: a retrospective study. BMC Emerg. Med. 23(1), 7 (2023).
30.
Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med. Care 36(1), 8–27 (1998).
31.
Rosenbaum PR, Rubin DB. The central role of the propensity score in observational studies for causal effects. Biometrika 70(1), 41–55 (1983).
32.
Austin PC. A comparison of 12 algorithms for matching on the propensity score. Stat. Med. 33(6), 1057–1069 (2014).
33.
Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav. Res. 46(3), 399–424 (2011).
34.
Normand ST, Landrum MB, Guadagnoli E et al. Validating recommendations for coronary angiography following acute myocardial infarction in the elderly: a matched analysis using propensity scores. J. Clin. Epidemiol. 54(4), 387–398 (2001).
35.
Cox DR. Regression models and life-tables. J. Royal Stat. Soc. B (Methodological) 34(2), 187–202 (1972).
36.
Basu A, Manning WG, Mullahy J. Comparing alternative models: log vs Cox proportional hazard? Health Econ. 13(8), 749–765 (2004).
37.
Davidson-Pilon C. Lifelines: survival analysis in Python. (2019).
38.
Optum's de-identified Clinformatics® Data Mart Database. User Manual. Version 9.0. (September 2023).
39.
Malehi AS, Pourmotahari F, Angali KA. Statistical models for the analysis of skewed healthcare cost data: a simulation study. Health Econ. Rev. 5, 11 (2015).
40.
Seabold S, Perktold J. Statsmodels: Econometric and Statistical Modeling with Python. Proceedings of the 9th Python in Science Conference. 92–96 https://doi.org/10.25080/Majora-92bf1922-011 (2010).
41.
Onukwugha E, Bergtold J, Jain R. A primer on marginal effects-part II: health services research applications. Pharmacoeconomics 33(2), 97–103 (2015).
42.
Python Software Foundation. Python 3.10 Documentation (2023). https://docs.python.org/3/
43.
Bernstein RA, Kamel H, Granger CB et al. STROKE-AF Investigators. Effect of long-term continuous cardiac monitoring vs usual care on detection of atrial fibrillation in patients with stroke attributed to large- or small-vessel disease: the STROKE-AF randomized clinical trial. JAMA 325(21), 2169–2177 (2021).
44.
Buck BH, Hill MD, Quinn FR et al. Effect of implantable vs prolonged external electrocardiographic monitoring on atrial fibrillation detection in patients with ischemic stroke: the PER DIEM randomized clinical trial. JAMA 325(21), 2160–2168 (2021).
45.
Boriani G, Auricchio A, Botto GL et al. Insertable cardiac monitoring results in higher rates of atrial fibrillation diagnosis and oral anticoagulation prescription after ischaemic stroke. Europace 25(9), euad212 (2023).
46.
Gallacher KI, Jani BD, Hanlon P, Nicholl BI, Mair FS. Multimorbidity in stroke. Stroke 50(7), 1919–1926 (2019).
47.
Medic G, Kotsopoulos N, Connolly MP et al. Mobile cardiac outpatient telemetry patch vs implantable loop recorder in cryptogenic stroke patients in the US – cost-minimization model. Med. Devices (Auckl). 14, 445–458 (2021).
48.
Van Gelder IC, Healey JS, Crijns HJGM et al. Duration of device-detected subclinical atrial fibrillation and occurrence of stroke in ASSERT. Eur. Heart J. 38(17), 1339–1344 (2017).
49.
McIntyre WF, Wang J, Benz AP et al. Estimated incidence of previously undetected atrial fibrillation on a 14-day continuous electrocardiographic monitor and associated risk of stroke. Europace 24(7), 1058–1064 (2022).
50.
Ferver K, Burton B, Jesilow P. The use of claims data in healthcare research. Open Public Health J. 2(1), 11–24 (2009).
51.
Geruso M, Layton T. Upcoding: evidence from Medicare on squishy risk adjustment. J. Polit. Econ. 12(3), 984–1026 (2020).
52.
Konrad R, Zhang W, Bjarndóttir M, Proaño R. Key considerations when using health insurance claims data in advanced data analyses: an experience report. Health Syst. (Basingstoke) 9(4), 317–325 (2019).
Information & Authors
Information
Published In
Copyright
© 2024 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 26 January 2024
Accepted: 22 March 2024
Published online: 11 April 2024
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparing the outcomes and costs of cardiac monitoring with implantable loop recorders and mobile cardiac outpatient telemetry following stroke using real-world evidence. (2024) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0008
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Pierantonio Russo, Ramaa Nathan, Mostafa Shokoohi, Erik Hendrickson, Ken Boyle, Mintu Turakhia, Brent Wright, All-cause healthcare cost differences across ambulatory cardiac monitoring modalities in Medicare beneficiaries: a real-world claims-based study using entropy balancing, Journal of Medical Economics, 10.1080/13696998.2026.2707021, 29, 1, (2076-2085), (2026).
- Ewelina Młynarska, Katarzyna Hossa, Natalia Krupińska, Hanna Pietruszewska, Aleksandra Przybylak, Kinga Włudyka, Jacek Rysz, Beata Franczyk, Atrial Fibrillation in COVID-19: Mechanisms, Clinical Impact, and Monitoring Strategies, Biomedicines, 10.3390/biomedicines13122889, 13, 12, (2889), (2025).
- Jia-Yi Wang, Stephanie Vu, Matthew McGuinness, Ryan Barrette, Stephen Trudeau, Hayley Price, Peter Zimetbaum, Magdy Selim, Jennifer Dearborn-Tomazos, Factors associated with increased atrial fibrillation detection in patients with embolic stroke of undetermined source, Journal of Stroke and Cerebrovascular Diseases, 10.1016/j.jstrokecerebrovasdis.2025.108343, 34, 7, (108343), (2025).
- Biswaranjan Senapati, Bharat S. Rawal, Sensor-Based Technique for The Identification of Cardiac Disorders Utilising Feature Extraction and Artificial Neural Networks, 2025 Third International Conference on Microwave, Antenna and Communication (MAC), 10.1109/MAC64480.2025.11140541, (1-6), (2025).
- Nidhi Yadav, Ananya Tiwari, Alok Pandya, Shubhita Tripathi, Next-generation biosensors for infectious disease surveillance: Innovations, challenges, and global health impact, undefined, 10.1016/bs.pmbts.2025.05.010, (2025).
- Md. Alamin Talukder, Majdi Khalid, Mohsin Kazi, Nusrat Jahan Muna, Mohammad Nur-e-Alam, Sajal Halder, Nasrin Sultana, A hybrid cardiovascular arrhythmia disease detection using ConvNeXt-X models on electrocardiogram signals, Scientific Reports, 10.1038/s41598-024-81992-w, 14, 1, (2024).