Polymer-based drug-eluting stent treatment extends the time to reintervention for patients with symptomatic femoropopliteal artery disease: clinical evidence and potential economic value
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Use long-term follow-up data from the IMPERIAL study to determine whether drug-eluting polymer-based nitinol stent treatment can delay the time to repeat intervention for femoropopliteal artery disease and how such a delay may result in cost savings in a value-based episode of care. Patients & methods: The IMPERIAL randomized controlled trial was an international study of a paclitaxel-eluting polymer-coated stent (Eluvia, Boston Scientific, MA, USA) versus a polymer-free paclitaxel-coated stent (Zilver PTX, Cook Corporation, IN, USA) for treating lesions of the femoropopliteal arterial segment. Study patients (n = 465) had symptomatic lower limb ischemia. Safety and efficacy assessments were performed through 5 years. Mean time to first reintervention was calculated in post-hoc analysis for patients who underwent a clinically driven target lesion revascularization (CD-TLR) through 3 or 5 years following the index procedure. To simulate potential cost savings associated with differential CD-TLR burden over time, a cost-avoidance analysis using input parameters from IMPERIAL and US 100% Medicare standard analytical files was developed. Results: Among patients with a first CD-TLR through 3 years of follow-up, mean time to reintervention was 5.5 months longer (difference 166 days, 95% CI: 51, 282 days; p = 0.0058) for patients treated with Eluvia (n = 56) than for those treated with Zilver PTX (n = 30). Through the 5-year study follow-up period, CD-TLR rates were 29.3% (68/232) for Eluvia and 34.2% (39/114) for Zilver PTX (p = 0.3540) and mean time to first reintervention exceeded 2 years for patients treated with Eluvia at 737 days versus 645 days for the Zilver PTX group (difference 92 days, 95% CI: -85, 269 days; p = 0.3099). Simulated savings considering reinterventions occurring over 1 and 5 years following initial use of Eluvia over Zilver PTX were US $1,395,635 and US $1,531,795, respectively, when IMPERIAL CD-TLR rates were extrapolated to 1000 patients. Conclusion: IMPERIAL data suggest initial treatment with Eluvia extends the time patients spend without undergoing reintervention. This extension may be associated with cost savings in relevant time frames.
Shareable abstract
Long-term follow-up data from the randomized IMPERIAL trial showed that treatment with the Eluvia drug-eluting stent delayed lesion restenosis and extended the time before reintervention was needed. Such a delay could lead to cost savings depending on the surveillance period, as shown in cost-avoidance scenarios based on costs associated with reintervention episodes of care.
Plain language summary
What is this article about?
The IMPERIAL randomized controlled trial was an international clinical study of the Eluvia drug-eluting stent compared with the Zilver PTX drug-coated stent for treating lesions of the femoropopliteal arterial segment (i.e., arteries in the thigh).
What were the results?
Long-term follow-up data showed that treatment with Eluvia delayed lesion restenosis and extended the time before reintervention was needed.
What do the results mean?
The time patients spend without undergoing reintervention is a potentially useful parameter for healthcare stakeholders when comparing interventional options. Avoiding repeat hospitalization and invasive procedures is important to patients and such a delay could lead to cost savings depending on the surveillance period, as shown in cost-avoidance scenarios based on costs associated with reintervention episodes of care.
Peripheral artery disease (PAD) is the atherosclerotic narrowing or blockage of arteries, most commonly affecting vessels supplying the legs. Prevalence among adults over 40 years of age in the USA was reported as 10.7% in 2003–2008 [1] and 13.5% among adults over age 65 in 2012 [2]. Healthcare costs for PAD are high [3,4], and largely driven by hospitalizations [5] and lower limb revascularization procedures [6].
Limb ischemia due to PAD is characterized by exertional leg pain and, in severe cases, rest pain and tissue loss. Endovascular revascularization options for the femoropopliteal artery segment, which may be used in patients with lifestyle-limiting claudication for whom medical therapy has not improved symptoms, or who present with chronic limb-threatening ischemia (CLTI) [7,8], have recently come to include drug-coated balloons and drug-eluting stents [7–9]. These therapies expand stenotic (i.e., narrowed) or occluded areas of the diseased artery lumen to allow blood flow while delivering an antirestenotic agent to the artery wall to prevent restenosis due to an exuberant healing process. Drug-eluting therapies for the femoropopliteal artery segment have proven to be cost-effective and have reduced repeat intervention rates relative to bare therapies [10].
Success and durability of peripheral artery revascularization procedures is typically measured by clinically driven target lesion revascularization (CD-TLR; i.e., whether additional revascularization procedures are required due to restenosis and recurring symptoms) and vessel patency (i.e., the absence of restenosis by imaging and without repeat revascularization procedures) [11]. In clinical study populations, lower vessel patency rates correlate with greater TLR rates. Loss of patency following initial treatment may contribute to symptom recurrence leading to reintervention procedures, and failed initial therapy is additionally associated with significantly increased numbers of clinic visits, hospital days, imaging procedures and radiation exposure for patients [12].
While drug coatings have reduced repeat intervention rates for the femoropopliteal artery, the first year following the initial intervention remains the peak reintervention period following drug-coated balloon [13] or drug-coated stent therapy [14]. Healthcare cost burden in vascular interventions for PAD is largely driven by reintervention procedures within the first 1 to 2 years [6,10,15–17].
In a value-based care environment, it is important to understand implications of use of different devices for treating PAD [18]. The Eluvia drug-eluting vascular stent system (Boston Scientific, MA, USA) has an antirestenotic paclitaxel drug coating designed to elute over approximately 1 year [19], and thereby prevent femoropopliteal artery lesion restenosis and the need for repeat interventions during the timeframe when they tend to occur following endovascular stent-based revascularization [20]. Eluvia's prolonged drug elution profile differs from that of the polymer-free paclitaxel-coated Zilver PTX stent (Cook Corporation, IN, USA), which delivers the antirestenotic agent for less than 2 months [21]. Performance of these two stents was compared in the randomized IMPERIAL study, which had primary objectives to investigate efficacy (i.e., patency in the treated area) and safety outcomes through 1 year [22]. The Eluvia stent was superior in terms of primary patency and non-inferior in terms of major adverse events through 1 year [22]. Systematic 5-year follow-up from the study contributes to the otherwise limited long-term data on drug-eluting stent (DES) placement in the femoropopliteal artery segment [14,23].
The objectives of the current analysis were to use long-term follow-up data from the IMPERIAL study to determine whether Eluvia treatment can shift the time to restenosis and repeat intervention as compared with Zilver PTX treatment, and explore implications of avoiding reintervention or prolonging the time until it is required by simulating cost savings that could be generated in value-based care episodes.
Methods
IMPERIAL study design & long-term follow-up
The IMPERIAL randomized controlled trial (RCT) was a prospective, multicenter, international study of the efficacy and safety of the Eluvia DES compared with the Zilver PTX stent for treating lesions of the superficial femoral and proximal popliteal arteries [22]. Patients had symptomatic lower limb ischemia categorized as claudication or early-stage chronic limb-threatening ischemia (Rutherford category 2–4). Study protocol approval was obtained from the institutional review board, independent ethics committee or research ethics board at each study site and patients provided written informed consent. IMPERIAL is registered with ClinicalTrials.gov, identifier NCT02574481.
Primary results were assessed at 1-year follow-up and have been reported previously [22]. Long-term follow-up was scheduled through 5 years and included assessments of mortality, major (i.e., above ankle) amputation, CD-TLR and primary patency based on core-laboratory assessed duplex ultrasound assessment without reintervention. Reinterventions for restenosis of the original treated artery segment in the presence of recurrent symptoms or diminished hemodynamics were considered CD-TLR, as described previously [22]. The all-cause mortality assessment included deaths reported and adjudicated through study channels as well as from other vital status records.
Statistical analysis
Event rates
Statistical analyses were performed with SAS (SAS Institute Inc, NC, USA) version 9.4. Safety event rates for IMPERIAL are reported through the upper limit of the 5-year follow-up window (i.e., 1855 days). Event rates were compared between treatment groups with the Chi-square test or Fisher's exact test. Kaplan-Meier analysis of primary patency was performed in the intention-to-treat analytic set.
Time to CD-TLR
Two time horizons were considered in post-hoc analysis of the mean time to first CD-TLR in the IMPERIAL RCT. First, the 3-year horizon included patients who underwent a first CD-TLR through 3 years following the index procedure. This time frame was chosen to encompass a period that is clinically meaningful for patients [24], in which most of the cost burden from repeat procedures is incurred [15,16], and is relevant to reduce total medical expenses associated with PAD care episodes [25]. Second, in order to capture the full study follow-up period, the 5-year horizon included all patients in the study who underwent a CD-TLR. The mean number of days to first CD-TLR and 95% confidence intervals were determined.
Restenosis timing
In post-hoc analysis, probability density analysis was used to visualize the time to anatomic restenosis in the RCT, similar to the analysis described by Iida et al. [20]. ‘Restenosis’ was based on core-lab duplex ultrasound assessment of the target lesion, or, if evaluable imaging was unavailable, first CD-TLR was considered indicative of restenosis.
Cost savings simulation
To illustrate the potential effect of differential reintervention burden over time in economic terms, an Excel-based (Microsoft Excel, WA, USA) cost-avoidance model was developed to assess the cost savings associated with reduced numbers of reinterventions over 1, 3 and 5 years following use of Eluvia or Zilver PTX. A deterministic simulation focused on reinterventions was used for simplicity and transparency of fixed input values. ‘Reintervention’ rates were based on CD-TLR rates from IMPERIAL data. Death or other adverse events were not included in the model. Input parameters are listed in Supplementary Table 1. Healthcare cost associated with a second femoropopliteal intervention was derived from a retrospective analysis of the US Medicare 100% standard analytical files (SAF); the procedure used to estimate this cost is described in Supplementary Figure 1. The estimated total cost per second revascularization includes all excess Medicare costs incurred around the second intervention, not restricted to direct revascularization procedure or encounter costs. Codes used to identify patients undergoing femoropopliteal stenting and subsequent revascularization procedures in Medicare data for the reintervention cost estimate are listed in Supplementary Table 2.
The clinical trial reintervention rates and estimated cost associated with a second intervention were then scaled to three scenarios with increasing population size for comparison: the sample size of the Eluvia group in the IMPERIAL RCT; per 1000 patients; and the total number of Medicare beneficiaries with a femoropopliteal artery stent placement (based on 100% Medicare SAF). All costs are reported in 2023 US dollars; we assumed cost was linear and constant over time, thus costs were not discounted.
Results
IMPERIAL follow-up disposition through 5 years
The IMPERIAL study enrolled 465 patients (66% men, mean age 68 years), with high prevalence of diabetes (42%), hyperlipidemia (76%) and hypertension (83%) [22]. A total of 346 patients (74.4%) completed adequate follow-up (i.e., follow-up at least 1795 days or experienced a prior event) to be included in the 5-year assessments of CD-TLR and major amputation; of these, 296 patients completed the 60-month follow-up visit.
IMPERIAL safety & efficacy through 5 years
CD-TLR rates were 29.3% (68/232) for Eluvia and 34.2% (39/114) for Zilver PTX (p = 0.3540). Target limb major amputation rates were 3.4% (8/232) and 2.6% (3/114) for Eluvia and Zilver PTX, respectively (p > 0.99). The Kaplan-Meier analysis of primary patency in the RCT through the full 5-year follow-up window (i.e., 61 months) is shown in Supplementary Figure 2. The 5-year all-cause crude mortality rate was 18.8% (58/309) for Eluvia DES and 17.9% (28/156) for Zilver PTX (p = 0.8294).
Time to first CD-TLR in IMPERIAL
The time to first CD-TLR is shown in Figure 1. Among patients with a first CD-TLR through 3 years of follow-up, mean time to reintervention was significantly longer for patients treated with the Eluvia DES than for those treated with Zilver PTX (581 days vs 414 days; difference 166 days, 95%CI: 51, 282 days; p = 0.0058; Figure 1A). This equates to a mean time to CD-TLR of 19.4 months for patients treated with Eluvia, whereas the time for those treated with Zilver PTX was 13.8 months for a difference of approximately 5.5 months. In a 5-year time horizon, the time difference was 92 days or 3 months (95% CI: -85, 269 days; p = 0.3099; Figure 1B).
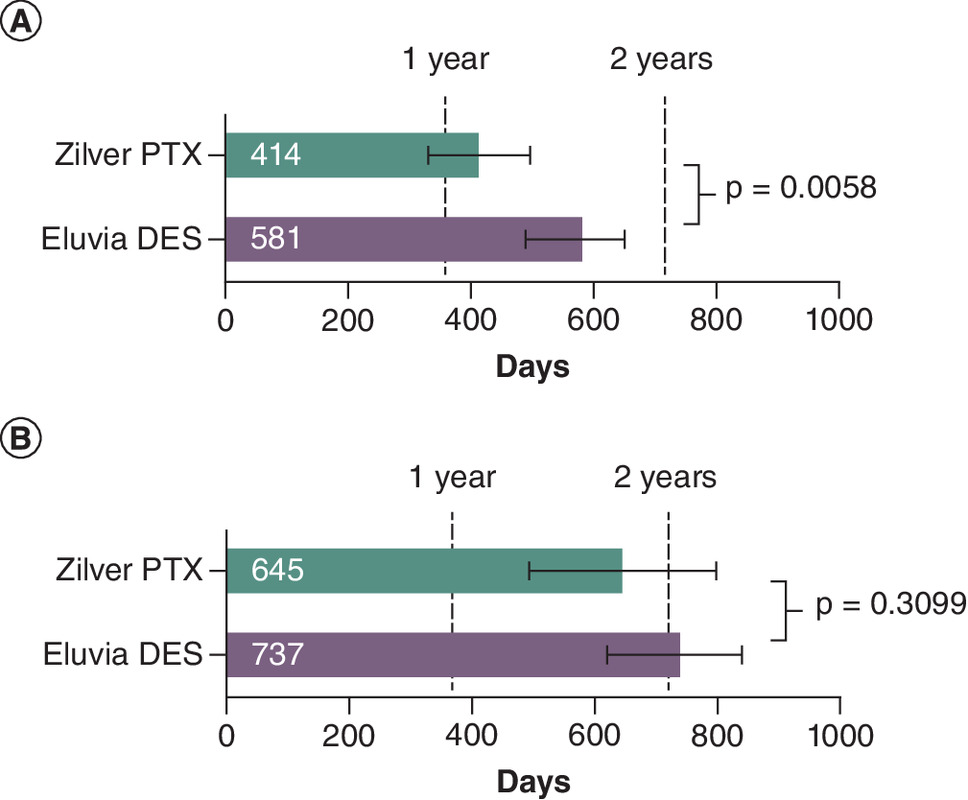
Figure 1. Time to first clinically driven target lesion revascularization in the IMPERIAL randomized controlled trial.
Mean days to first CD-TLR (clinically driven target lesion revascularization) and 95%CI for those undergoing CD-TLR within 3 years (A), or within 5 years (B) of the stent implantation procedure; intention to treat population.
DES: Drug-eluting stent.
Timing of restenosis in IMPERIAL
Restenosis timing based on the probability density function is shown in Figure 2. Although both Zilver PTX and Eluvia had peaks in restenosis probability around 1 and 2 years (as expected given the scheduled duplex ultrasound evaluations at visits in those timeframes), the restenosis probability for patients treated with Eluvia was lower than that of Zilver PTX at both time points, and timing shifted later over the follow-up period.
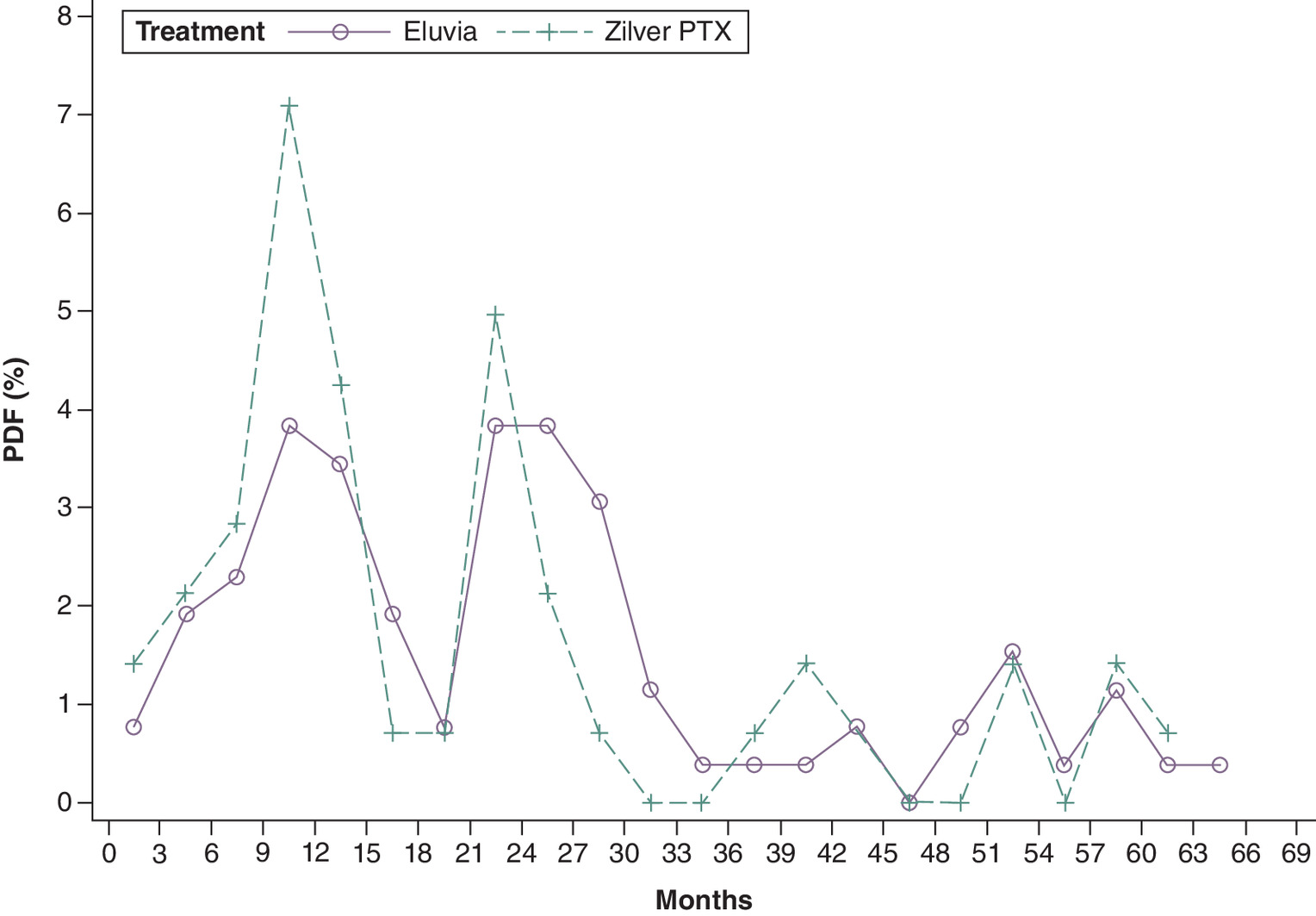
Figure 2. Probability density function for restenosis after Eluvia drug-eluting stent or Zilver PTX stent placement in the IMPERIAL randomized controlled trial.
The probability density of restenosis at 3-month intervals is shown.
PDF: Probability density function.
Potential cost savings
The estimated total cost to Medicare for a second intervention was $34,040 per patient (Supplementary Table 1 & Supplementary Figure 1). Potential savings associated with avoiding reinterventions due to initial placement of Eluvia over Zilver PTX are shown in Table 1. Savings to Medicare per 1000 patients initially receiving Eluvia over Zilver PTX were simulated as $1,395,635 through 1 year and $1,531,795 through 5 years (Table 1, Scenario 2). Extending this model to a population equal to the number of Medicare beneficiaries with femoropopliteal stent placements (n = 94,321), projected savings totaled $144,499,333 through 5 years (Table 1, Scenario 3).
| Year 1 | Year 3 | Year 5 | ||||
|---|---|---|---|---|---|---|
| Eluvia | Zilver PTX | Eluvia | Zilver PTX | Eluvia | Zilver PTX | |
| Scenario 1: IMPERIAL Eluvia group sample size for each time period | ||||||
| Patients with CD-TLR | 14 | 26 | 56 | 59 | 68 | 78 |
| Calculated costs | $476,558 | $885,037 | $1,906,234 | $2,008,354 | $2,314,713 | $2,655,111 |
| Incremental savings† | $408,479 | $102,120 | $340,399 | |||
| Scenario 2: Per 1000 patients | ||||||
| Patients with CD-TLR | 47 | 88 | 220 | 234 | 297 | 342 |
| Calculated costs | $1,599,875 | $2,995,510 | $7,488,776 | $7,965,334 | $10,109,847 | $11,641,642 |
| Incremental savings† | $1,395,635 | $476,558 | $1,531,795 | |||
| Scenario 3: Medicare beneficiaries with femoropopliteal stent placement (n = 94,321)‡ | ||||||
| Patients with CD-TLR | 4433 | 8300 | 20,751 | 22,071 | 28,013 | 32,258 |
| Calculated costs | $150,898,832 | $282,531,087 | $706,361,757 | $751,294,412 | $953,559,439 | $1,098,058,772 |
| Incremental savings† | $131,632,255 | $44,932,655 | $144,499,333 | |||
†
Zilver PTX – Eluvia.
‡
Includes both bare metal and drug-eluting stent placement.
CD-TLR: Clinically driven target lesion revascularization.
Discussion
For patients with symptomatic femoropopliteal PAD lesions treated with DES, polymer-coated Eluvia provided statistically significant and clinically meaningful extension of the time to first reintervention, which has implications for both patients and the healthcare system when practicing in a value-based environment. The potential economic value of differential reintervention burden in various time frames was illustrated from a Medicare perspective, with cost savings apparent through the 1-, 3- and 5-year horizons represented in the simulation.
The restenosis timing analysis provides mechanistic support for the observed delay in the need for reintervention. Restenosis following Eluvia use did not predominantly occur within 1 year, in contrast to Zilver PTX and in a previous evaluation for bare metal stents [20]. The delayed restenosis timing pattern for Eluvia was consistent with a prolonged antirestenotic effect, as expected with the sustained drug elution of the polymer-based Eluvia DES [19]. The observed peaks around the scheduled visit windows are explained by use of duplex ultrasound imaging to identify restenosis; this imaging was typically obtained during study visits.
Eluvia cost effectiveness through 2 years has previously been reported, demonstrating an economic advantage to payers responsible for total medical expenses [26]. Through further long-term clinical follow-up, more than two-thirds of patients in IMPERIAL did not require a repeat intervention at all within 5 years after femoropopliteal stenting, while increasing the time to reintervention also has potential economic and clinical implications. Our analysis of Medicare cost data provides a basic example of real-world opportunity cost savings associated with initial use of Eluvia instead of Zilver PTX. Currently, healthcare cost burden associated with vascular interventions for PAD is largely driven by repeat revascularization procedures [10,11], and a 2-year timespan has been suggested by the Society for Vascular Surgery as meaningful for assessment of clinical improvement among patients with intermittent claudication [17]. Treatment that extends the time to reintervention beyond 1 year benefits patients and demonstrates healthcare quality improvement over the current state. Repeat revascularization procedures suggest symptom recurrence, may require hospitalization, and, like all invasive procedures, have associated risks and reduced quality of life. Furthermore, patients with PAD have serious comorbidities [3,27] and symptomatic PAD is associated with increased mortality risk compared with no PAD [28]. In an analysis of a Swedish national registry [29], 3.4–20.5% (depending on PAD severity) of patients requiring revascularization died within 1 year, accumulating to 7.5–31.7% within 2 years. Our findings suggest durability of the initial DES therapy may be maintained beyond the life expectancy of a portion of patients with severe PAD, meaningfully impacting their quality of life.
Limitations of the clinical analysis include the reduced sample size in long-term follow-up, which was similar between the RCT study groups. The study was not designed primarily as an economic analysis and the deterministic model utilized does not differentiate factors such as resources, device costs, mortality and other cost parameters that could influence the true cost to Medicare or the magnitude of potential cost savings from other perspectives. Costs were not discounted. The assumption of similar base cost associated with reintervention does not account for potential between-group cost variation and true ‘re’-interventions in the same artery cannot be determined from Medicare data. The volume of Medicare beneficiaries undergoing femoropopliteal artery stenting includes both bare metal and drug-eluting stent procedures due to coding limitations, and thus the scenario based on this number overestimates costs related to initial DES use. Last, extrapolating findings from clinical trial data or smaller samples to larger populations (e.g., Medicare beneficiaries) introduces uncertainties, as outcomes in real-world settings may differ.
Conclusion
IMPERIAL data suggest treatment with Eluvia may contribute to value improvement in a value-based payment environment by avoiding or delaying the need for reintervention relative to other stent therapies, which is important to patients and may lead to cost savings depending on the surveillance period. In addition to traditional measures such as rates of repeat intervention or clinical improvement, the time patients spend without undergoing reintervention is a potentially useful parameter for healthcare stakeholders when comparing interventional options for PAD.
Summary points
•
The IMPERIAL randomized controlled trial compared femoropopliteal arterial segment treatment with the Eluvia paclitaxel-eluting polymer-coated stent with that of the Zilver PTX polymer-free paclitaxel-coated stent with patient follow-up up to 5 years.
•
The average time to reintervention (i.e., re-revascularization following the index study treatment) was prolonged among patients treated with Eluvia, with a difference ranging from approximately 5.5 months through 3 years following stent implantation to 3 months through 5 years of follow-up.
•
The relative delay in time to reintervention among Eluvia-treated patients was consistent with imaging-based analysis of time to lesion restenosis, which showed an earlier peak for patients treated with Zilver PTX.
•
Potential cost savings were estimated using cost data from Medicare 100% Standard Analytical Files and clinically driven target lesion revascularization rates from IMPERIAL.
•
Simulated savings generated for use of Eluvia over Zilver PTX were up to US $1,531,795 over 5 years among 1000 patients undergoing femoropopliteal stent placement.
•
Avoiding repeat hospitalization and invasive procedures is important to patients and may result in cost savings.
Author contributions
WA Gray and S Müller-Hülsbeck contributed to the IMPERIAL study conception and design; WA Gray, S Müller-Hülsbeck, Y Soga, M Fujihara, O Iida, A Babaev, D Kawasaki, T Zeller and D O'Connor were responsible for acquisition of data. All authors were responsible for data interpretation, contributed to drafting the work or reviewing it critically for important intellectual content; final approval of the version to be published; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments
The authors thank the IMPERIAL investigators, and the following Boston Scientific employees for their assistance: N Kilburn (clinical trial management), A Sanyal (statistical analysis management), A Williams (economic analysis) and EJ Davis (medical writing). Results were presented at CRT 2023, 26 February 2023, Washington DC, USA.
Financial disclosure
IMPERIAL was sponsored and funded by Boston Scientific Corporation (MA, USA). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
WA Gray is a consultant, advisory board member and has received institutional research support from Boston Scientific Corporation. Y Soga serves as an advisor to Boston Scientific. M Fujihara is a consultant for Boston Scientific Corporation. O Iida is a consultant for Boston Scientific Corporation. A Babaev reports receiving honoraria for physician training from Boston Scientific and Medtronic. D Kawasaki is a consultant for Boston Scientific Corporation. T Zeller reports receiving honoraria from: Abbott Vascular, Veryan, Biotronik, Boston Scientific Corp., Cook Medical, Gore & Associates, Medtronic, TriReme, Shockwave, B. Braun, Efemoral, consulting for: Boston Scientific Corp., Cook Medical, Gore & Associates, Medtronic, Veryan, Intact Vascular. D O'Connor reports receiving honoraria for physician training from Cardiovascular Systems Incorporated, Abbott and Boston Scientific. MR Jaff is an employee of Boston Scientific, is a board member of Access Vascular, and is a consultant for Gilde Healthcare. He has equity interest in Efemoral, R3 Vascular. AM Chavez is an employee of and owns stock in Boston Scientific. S Müller-Hülsbeck serves as a consultant and has received honoraria and travel grants from Boston Scientific, Eurocor, Alvimedica, and has received fees from Terumo. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing and editorial support were provided by EJ Davis an employee of Boston Scientific Corporation.
Ethical conduct of research
The authors state that approval for the research described was obtained from the institutional review board, independent ethics committee or research ethics board at each study site. Written informed consent was obtained from the patients for their participation in the study.
Data sharing statement
The authors certify that this manuscript reports original clinical trial data. The data will not be made publicly available.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary material.docx)
- Download
- 99.28 KB
References
Papers of special note have been highlighted as: • of interest
1.
Tsao CW, Aday AW, Almarzooq ZI et al. Heart disease and stroke statistics – 2023 update: a report from the American Heart Association. Circulation 147(8), e93–e621 (2023).
2.
Kalbaugh CA, Kucharska-Newton A, Wruck L et al. Peripheral artery disease prevalence and incidence estimated from both outpatient and inpatient settings among Medicare fee-for-service beneficiaries in the Atherosclerosis Risk in Communities (ARIC) study. J. Am. Heart Assoc. 6(5), e003796 (2017).
3.
Criqui MH, Matsushita K, Aboyans V et al. Lower extremity peripheral artery disease: contemporary epidemiology, management gaps, and future directions: a scientific statement from the American Heart Association. Circulation 144(9), e171–e191 (2021).
4.
Jaff MR, Cahill KE, Yu AP, Birnbaum HG, Engelhart LM. Clinical outcomes and medical care costs among Medicare beneficiaries receiving therapy for peripheral arterial disease. Ann. Vasc. Surg. 24(5), 577–587 (2010).
5.
Kohn CG, Alberts MJ, Peacock WF, Bunz TJ, Coleman CI. Cost and inpatient burden of peripheral artery disease: findings from the national inpatient sample. Atherosclerosis 286, 142–146 (2019).
6.
Hasvold P, Nordanstig J, Kragsterman B et al. Long-term cardiovascular outcome, use of resources, and healthcare costs in patients with peripheral artery disease: results from a nationwide Swedish study. Eur. Heart J. Qual. Care Clin. Outcomes 4(1), 10–17 (2018).
7.
Bailey SR, Beckman JA, Dao TD et al. ACC/AHA/SCAI/SIR/SVM 2018 Appropriate use criteria for peripheral artery intervention: a report of the American College of Cardiology Appropriate Use Criteria Task Force, American Heart Association, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, and Society for Vascular Medicine. J. Am. Coll. Cardiol. 73(2), 214–237 (2019).
8.
Aboyans V, Ricco JB, Bartelink MEL et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries. Endorsed by: the European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur. Heart J. 39(9), 763–816 (2017).
9.
Feldman DN, Armstrong EJ, Aronow HD et al. SCAI consensus guidelines for device selection in femoral-popliteal arterial interventions. Catheter. Cardiovasc. Interv. 92(1), 124–140 (2018).
10.
Sridharan ND, Boitet A, Smith K et al. Cost-effectiveness analysis of drug-coated therapies in the superficial femoral artery. J. Vasc. Surg. 67(1), 343–352 (2018).
11.
Patel MR, Conte MS, Cutlip DE et al. Evaluation and treatment of patients with lower extremity peripheral artery disease: consensus definitions from Peripheral Academic Research Consortium (PARC). J. Am. Coll. Cardiol. 65(9), 931–941 (2015).
12.
Zielinski LP, Chowdhury MM, Coughlin PA. Patient and institutional costs of failure of angioplasty of the superficial femoral artery. Ann. Vasc. Surg. 72, 218–226 (2021).
13.
Briody H, Kearns CA, Lee MJ. Mortality, safety and efficacy of paclitaxel-containing balloons and stents in the femoropopliteal artery: systematic review and meta-analysis of randomized controlled trials since 2018. J. Vasc. Interv. Radiol. (2024) (Epub ahead of print).
14.
Dake MD, Ansel GM, Jaff MR et al. Durable clinical effectiveness with paclitaxel-eluting stents in the femoropopliteal artery: 5-year results of the Zilver PTX Randomized Trial. Circulation 133(15), 1472–1483 (2016).
15.
Pietzsch JB, Geisler BP, Garner AM, Zeller T, Jaff MR. Economic analysis of endovascular interventions for femoropopliteal arterial disease: a systematic review and budget impact model for the United States and Germany. Catheter. Cardiovas. Interv. 84(4), 546–554 (2014).
• Budget impact model based on first-generation drug-eluting therapies for lower extremity peripheral artery disease (PAD) highlights the importance of promoting a shift from low- to high-value treatments.
16.
Mahoney EM, Wang K, Keo HH et al. Vascular hospitalization rates and costs in patients with peripheral artery disease in the United States. Circ. Cardiovasc. Qual. Outcomes 3(6), 642–651 (2010).
17.
Williams A, McGovern AM, Danese M, Griffiths RI. POSB37 Real-world costs of reintervention in stenting with femoropopliteal artery revascularization [ISPOR Europe Abstract]. Value in Health 25(1), S67 (2021).
18.
Duwayri YM, Woo K, Aiello FA et al. The Society for Vascular Surgery Alternative Payment Model Task Force report on opportunities for value-based reimbursement in care for patients with peripheral artery disease. J. Vasc. Surg. 73(4), 1404–1413; e2 (2021).
• Overview of aspects of value-based care in PAD treatment and challenges in evaluating PAD care.
19.
Müller-Hülsbeck S. Eluvia peripheral stent system for the treatment of peripheral lesions above the knee. Expert Opin. Drug Deliv. 13(11), 1639–1644 (2016).
20.
Iida O, Uematsu M, Soga Y et al. Timing of the restenosis following nitinol stenting in the superficial femoral artery and the factors associated with early and late restenoses. Catheter. Cardiovasc. Interv. 78(4), 611–617 (2011).
21.
Dake MD, Van Alstine WG, Zhou Q, Ragheb AO. Polymer-free paclitaxel-coated Zilver PTX Stents–evaluation of pharmacokinetics and comparative safety in porcine arteries. J. Vasc. Interv. Radiol. 22(5), 603–610 (2011).
22.
Gray WA, Keirse K, Soga Y et al. A polymer-coated, paclitaxel-eluting stent (Eluvia) versus a polymer-free, paclitaxel-coated stent (Zilver PTX) for endovascular femoropopliteal intervention (IMPERIAL): a randomised, non-inferiority trial. Lancet 392(10157), 1541–1551 (2018).
23.
Torsello GF, Stavroulakis K, Bisdas T et al. Treatment of femoropopliteal artery disease with polymer-coated drug-eluting stent: 5-year results of a prospective, non-randomized study including the Halo phenomenon. Cardiovasc. Intervent. Radiol. 47(2), 177–185 (2024).
24.
Society for Vascular Surgery Lower Extremity Guidelines Writing Group; Conte MS, Pomposelli FB, Clair DG et al. Society for Vascular Surgery practice guidelines for atherosclerotic occlusive disease of the lower extremities: management of asymptomatic disease and claudication. J. Vasc. Surg. 61(Suppl. 3), S2–S41 (2015).
25.
Duwayri YM, Aiello FA, Tracci MC et al. Defining the 90-day cost structure of lower extremity revascularization for alternative payment model assessment. J. Vasc. Surg. 73(2), 662–673; e3 (2021).
26.
Gray WA, Griffiths RI, Elroy PWM et al. Cost–effectiveness of a paclitaxel-eluting stent (Eluvia) compared to Zilver PTX for endovascular femoropopliteal intervention. J. Med. Econ. 25(1), 880–887 (2022).
• Cost–effectiveness model of Eluvia compared with Zilver PTX.
27.
Norgren L, Hiatt WR, Dormandy JA et al. Inter-society consensus for the management of peripheral arterial disease (TASC II). J. Vasc. Surg. 45(Suppl. S), S5–S67 (2007).
28.
Sigvant B, Lundin F, Wahlberg E. The risk of disease progression in peripheral arterial disease is higher than expected: a meta-analysis of mortality and disease progression in peripheral arterial disease. Eur. J. Vasc. Endovasc. Surg. 51(3), 395–403 (2016).
29.
Baubeta Fridh E, Andersson M, Thuresson M et al. Amputation rates, mortality, and pre-operative comorbidities in patients revascularised for intermittent claudication or critical limb ischaemia: a population based study. Eur. J. Vasc. Endovasc. Surg. 54(4), 480–486 (2017).
Information & Authors
Information
Published In
Copyright
© 2024 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 23 February 2024
Accepted: 26 March 2024
Published online: 12 April 2024
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Polymer-based drug-eluting stent treatment extends the time to reintervention for patients with symptomatic femoropopliteal artery disease: clinical evidence and potential economic value. (2024) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0025
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Aniol Bosch, Pauline Champion, Joaquim Ciurana, Antonio J. Guerra, Additively manufactured reinforced polymeric stents for peripheral artery disease: design, manufacture and performance evaluation, 3D Printing in Medicine, 10.1186/s41205-026-00328-8, 12, 1, (2026).
- Tsuyoshi Shibata, Naoki Fujimura, Shigeo Ichihashi, Yutaka Iba, Masami Shingaki, Terutoshi Yamaoka, Comparison of Clinical Presentation and In Stent Re-stenosis Morphology between Polymer Free and Polymer Coated Paclitaxel Based Stents, European Journal of Vascular and Endovascular Surgery, 10.1016/j.ejvs.2026.04.041, (2026).
- M. Lourdes Del Río-Solá, Joan Roedan-Oliver, Sergio Asensio-Rodriguez, Sandra Perez-Fernandez, Álvaro Revilla-Calavia, Efficacy of Pacitaxel-Eluting Stents in Femoropopliteal Disease: A Systematic Review and Meta-Analysis, Annals of Vascular Surgery, 10.1016/j.avsg.2025.11.128, 124, (299-311), (2026).
- Raphaël Coscas, Jos C. van den Berg, There Is No Light Without Shadow, European Journal of Vascular and Endovascular Surgery, 10.1016/j.ejvs.2025.03.036, 69, 6, (874-875), (2025).
- Tsuyoshi Shibata, Yutaka Iba, Masami Shingaki, Osamu Yamashita, Yoshinori Tsubakimoto, Fumiaki Kimura, Atsutoshi Hatada, Fuminori Kasashima, Kyohei Ueno, Nobuyoshi Kawaharada, Editor's Choice – Comparative Analysis of Three Year Results of Two Paclitaxel Related Stents for the Management of Femoropopliteal Disease in a Real World Setting, European Journal of Vascular and Endovascular Surgery, 10.1016/j.ejvs.2025.03.010, 69, 6, (865-873), (2025).
- Manasi Tannu, W. Schuyler Jones, Rajesh V. Swaminathan, Jennifer A. Rymer, J. Antonio Gutierrez, Femoropopliteal Endovascular Intervention: A Review of the Current Landscape, Circulation: Cardiovascular Interventions, 10.1161/CIRCINTERVENTIONS.124.014024, 18, 5, (2025).