Progress of patients hospitalized with acute heart failure treated with empagliflozin
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To describe the epidemiological, clinical and laboratory characteristics and clinical progress of patients hospitalized with heart failure (HF) who started treatment with empagliflozin before discharge. Methods: We performed a retrospective observational study of patients aged ≥18 years admitted to the Internal Medicine Department of University Hospital Jaen, Jaen, Spain with acute HF between 1 May 2022 and 31 May 2023. Patients had to have a life expectancy of ≥1 year and have started treatment with empagliflozin during admission. Results: We included 112 patients (mean age, 85.2 ± 6.5 years; 67.9% women; 35.7 and 31.3% in NYHA functional classes III and IV; 73.2% with HF and preserved ejection fraction). Before admission, 80.4% were taking loop diuretics, 70.6% renin–angiotensin–aldosterone system inhibitors, 49.1% betablockers and 25% mineralocorticoid receptor antagonists. At admission, 94.6% were taking furosemide (15.2% at high doses, 36.6% at intermediate doses). The dose of furosemide was reduced at initiation of empagliflozin. At the end of follow-up, 13.4% of patients had died, 93.8% of the survivors continued treatment with empagliflozin and 26.8% had attended the emergency department with signs and symptoms of HF. Conclusion: Introduction of empagliflozin before discharge from hospital in patients admitted with HF made it possible to reduce the dose of diuretics during admission. The frequency of complications was as expected, and treatment was largely maintained.
Heart failure (HF) is a common condition whose frequency increases with age. The general prevalence of HF stands at around 2% of the adult population [1], although in persons aged >75 years, this figure reaches 16% [2]. HF is associated with high morbidity and mortality [3], and while survival seems to have improved in recent years, mortality continues to be very high [4]. Similarly, hospitalization for HF is the most common reason for admission among elderly patients in developed countries [5].
Hospitalization with HF is a key moment in the progress of affected patients, since it is associated with poor prognosis and an increased risk of repeated admission to hospital in the future. Therefore, early optimization of treatment is essential if we are to reverse this situation [6].
Patients with HF and reduced left ventricular ejection fraction (HFrEF) are recommended to undergo quadruple therapy with renin–angiotensin–aldosterone system (RAAS) inhibitors (preferably sacubitril–valsartan), betablockers, mineralocorticoid receptor antagonists and sodium-glucose cotransporter-2 inhibitors (SGLT2i) [7]. However, patients with HF and preserved ejection fraction (HFpEF) are poorly represented in clinical trials; therefore, treatment was limited to controlling cardiovascular risk factors and comorbid conditions. The publication of results from clinical trials showing the benefits of SGLT2i in reducing the risk of cardiovascular death or hospitalization for HF in patients with HFpEF [8,9] was followed by recommendations that include SGLT2i as a first-line treatment in this population [10,11].
The clinical trials EMPULSE and EMPA-RESPONSE-AHF have shown the clinical benefits of empagliflozin during hospitalization for HF [12,13]. Unfortunately, since real-world studies on SGLT2i are scarce, especially in patients with acute HF [14], specific studies are required.
The primary objective of the study was to describe the epidemiological, clinical and laboratory characteristics of patients hospitalized with HF in the Internal Medicine Department of University Hospital Jaen, Jaen, Spain who had started therapy with empagliflozin 10 mg/d during admission. The effectiveness of empagliflozin was also evaluated in terms of mortality, visits to the emergency department, adverse effects, persistence at 3 months and tolerability. Furthermore, the progress of patients who received high doses of furosemide upon admission.
Methods
Study design & population
In this observational retrospective study, a review was performed of the clinical history of all patients hospitalized with acute HF between 1 May 2022 and 31 May 2023 in the Internal Medicine Department of University Hospital Jaen. The study population comprised persons aged ≥18 years hospitalized with acute HF (decompensated or de novo) and who had been admitted with HF or had experienced a decompensation episode during admission to hospital for another reason. Life expectancy had to be ≥1 year depending on the patient's comorbid conditions, and the patient had to have started therapy with empagliflozin at 10 mg/d during admission. Data were obtained from the electronic records of the hospital's Archive and Clinical Documentation Department based on the ICD-9-CM and ICD-10-CM. The exclusion criteria were right heart failure, death during admission, discharge without SGLT2i and previous therapy with SGLT2i. The study was performed according to Law 14/2007 of 3 July on biomedical research, the principles of the Belmont report and the Declaration of Helsinki on biomedical research. Data confidentiality and patient anonymity were guaranteed. The study was evaluated by the Research Ethics Committee of the Province of Jaen. The Committee waived the requirement for patient informed consent owing to the nature and characteristics of the study.
A series of variables were collected from the electronic clinical history. These included demographic data (age, sex) and comorbid conditions such as smoking and alcohol consumption, cardiovascular risk factors, atrial fibrillation and type of HF (de novo or decompensated). The Charlson comorbidity index was calculated. Obesity was defined as a body mass index ≥30 kg/m2 [15], excess alcohol consumption as >80/60 g/d (male/female) in the previous year [15], cerebrovascular disease as a history of stroke or transitory ischemic attack, chronic kidney disease as a glomerular filtration rate <60 ml/min/1.73 m2 (3a, 45–59; 3b, 30–44; 4, 15–29 ml/min/1.73 m2), respiratory disease as chronic obstructive pulmonary disease or asthma and peripheral artery disease as intermittent claudication, peripheral vascular bypass, acute arterial ischemia or aortic aneurism (thoracic or abdominal) >6 cm in diameter. HF was classified according to left ventricular ejection fraction as <40% (HFrEF), 41–49% (HF with a slightly reduced ejection fraction) and ≥50% (HFpEF) [16].
Additional test findings included chest x-ray (cardiomegaly, pleural effusion, interstitial edema), echocardiogram (left ventricular ejection fraction), blood biochemistry (NT-proBNP, Ca125, serum creatinine, glomerular filtration and urine sodium at admission). As for pharmacologic treatment of HF, the data recorded included dose of furosemide at admission and at initiation of empagliflozin. Baseline treatment of HF (including RAAS inhibitors, betablockers, mineralocorticoid receptor antagonists, digoxin and other diuretics) was also recorded.
Follow-up data recorded included the proportion of patients who attended the emergency department and mortality at 3 months after discharge, adverse effects associated with empagliflozin and persistence over time, as well as reason for discontinuation (where applicable). Changes in the dose of diuretics and oral antidiabetic drugs were analyzed, and patients who had initiated empagliflozin at higher doses of diuretic than at admission were compared with patients whose dose was lower than at admission. Patients who had received empagliflozin early (within 2 days after admission) were also analyzed.
Statistical analysis
Qualitative variables are presented as number of cases and percentage; quantitative variables are presented as mean (and median, where applicable) and standard deviation (SD). The chi-squared test with continuity correction was to compare categorical variables and the t-test to compare 2 means. Logistic regression analysis was performed to control for the effects of confounders with mortality and readmission to hospital as dependent variables and those for which statistical significance was greater than p < 0.01 in the bivariate analysis as independent variables. Statistical significance was set at p < 0.05. The data were analyzed using IBM SPSS Statistics, Version 21.0 (IBM Corp., NY, USA).
Results
A total of 195 patients were admitted with HF between 1 May 2022 and 31 May 2023. Of these, 83 patients were excluded for various reasons. Therefore, the final study population comprised 112 patients (57.4%) who started treatment with empagliflozin before discharge; of these, 97 completed follow-up (15 patients died) (Figure 1). Since only two patients had started dapagliflozin at the end of the recruitment period, they were not included in the final analysis to avoid inconsistencies in the results.
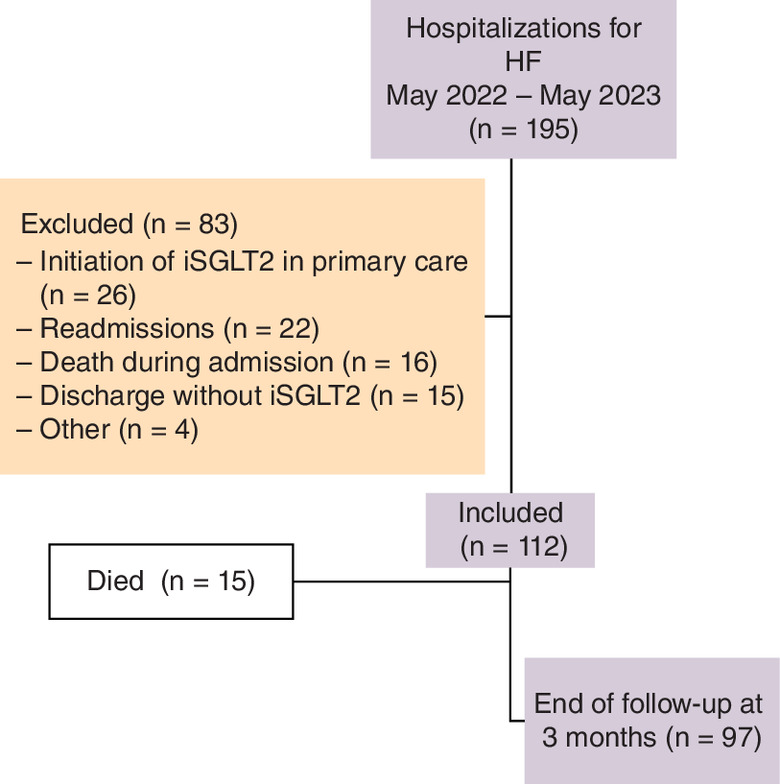
Figure 1. Patient flowchart.
HF: Heart failure; SGLT2i: Sodium-glucose cotransporter 2 inhibitor.
The baseline characteristics of the population are shown in Table 1. Mean age was 85.2 ± 6.5 years, and 67.9% of patients were women. Most patients were in NYHA functional class III (35.7%) or IV (31.3%), 73.2% had HFpEF, and most cases (85.7%) involved an exacerbation in patients previously diagnosed with HF. As for the presence of other comorbidities, 89.3% had arterial hypertension, 51.8% had atrial fibrillation, 40.1% chronic kidney disease, 38.4% diabetes and 10.7% a history of myocardial infarction.
| Biodemographic characteristics | |
|---|---|
| Age (years), mean (±SD) | 85.2 ± 6.5 |
| Female sex, n (%) | 76 (67.9) |
| Charlson comorbidity index, mean (±SD) | 6.5 ± 1.8 |
| Alcoholism, n (%) | 4 (3.6) |
| HF data | |
|---|---|
| NYHA functional class, n (%) I II III IV ND | 12 (10.7) 21 (18.8) 40 (35.7) 35 (31.3) 4 (3.6) |
| Type of HF, n (%) HFpEF HFmrEF HFrEF NA | 82 (73.2) 18 (16.1) 8 (7.1) 4 (3.6) |
| Type of admission, n (%) Exacerbation De novo | 96 (85.7) 16 (14.3) |
| Physical examination, n (%) Crackles, n (%) Edema, n (%) | 84 (75.0) 66 (58.9) |
| Chest x-ray, n (%) Interstitial edema Pleural effusion Cardiomegaly | 59 (52.7) 45 (40.2) 4 (3.6) |
| Echocardiogram, n (%) During admission Before admission | 63 (56.3) 53 (47.3) |
| Biochemistry NT-proBNP (at admission), pg/ml Median Ca125, U/ml Median Urine sodium (at admission) (n = 32), mEq/l Median | 7.790.0 ± 8.438.9 4.536 55.6 ± 55.1 34.1 66.3 ± 43.9 62.5 |
| Cardiovascular risk factors | |
|---|---|
| Hypertension, n (%) | 100 (89.3) |
| Dyslipidemia, n (%) | 50 (44.6) |
| Type 2 diabetes, n (%) | 43 (38.4) |
| Obesity, n (%) | 30 (26.8) |
| Vascular disease | |
|---|---|
| Chronic kidney disease, n (%) 3a 3b 4 Creatinine (at admission), mg/dl Median Glomerular filtration rate (at admission), ml/min/1.73m2 Median | 45 (40.1) 22 (19.6) 15 (13.4) 8 (7.1) 1.4 ± 0.7 1.2 50.7 ± 20.8 48.5 |
| Previous myocardial infarction, n (%) | 12 (10.7) |
| Cerebrovascular disease, n (%) | 9 (8.0) |
| Peripheral artery disease, n (%) | 5 (4.5) |
| Other comorbid conditions | |
|---|---|
| Atrial fibrillation, n (%) | 58 (51.8) |
| Respiratory diseases, n (%) | 40 (35.7) |
| Chronic cognitive impairment, n (%) | 17 (15.2) |
| Cancer, n (%) | 4 (3.6) |
| Treatment before admission | |
|---|---|
| Diuretics, n (%) Furosemide (oral) No furosemide 20 mg 40 mg 60 mg 80 mg 120 mg Other loop diuretics Hydrochlorothiazide | 31 (27.7) 1 (0.9) 51 (45.5) 5 (4.5) 11 (9.8) 4 (3.6) 9 (8.1) 28 (25.0) |
| Renin–angiotensin–aldosterone system inhibitors, n (%) ACEI/ARA II Sacubitril/valsartan | 79 (70.6) 75 (67.0) 4 (3.6) |
| Betablockers, n (%) | 55 (49.1) |
| Mineralocorticoid receptor antagonists, n (%) | 28 (25.0) |
| Digoxin, n (%) | 2 (1.8) |
ACEI: Angiotensin-converting enzyme inhibitor; ARA II: Angiotensin II receptor antagonist; HF: Heart failure; HFpEF: Heart failure with preserved ejection fraction; HFmrEF: Heart failure with mildly reduced ejection fraction; HFrEF: Heart failure with reduced ejection fraction; NA: Not available; NYHA: New York Heart Association.
As for treatment of HF before admission, 80.4% were taking a loop diuretic, mainly furosemide, 70.6% were taking a RAAS inhibitor, 49.1% were taking betablockers, and 25% were taking mineralocorticoid receptor antagonists (Table 1).
Median time to starting empagliflozin during admission was 3 days (IQR, 0–269). At admission, 94.6% were taking furosemide (15.2% at high doses [≥60 mg/24 h]; 36.6% at intermediate doses [>40-<60 mg/24 h]). On initiating empagliflozin, 12.5% were taking high doses of furosemide and 26.8% were taking intermediate doses. The dose of furosemide was reduced in 12.4% of patients (Supplementary Table 1).
As for the events recorded, 26.8% of patients (n = 30) had attended the emergency department and 13.4% (n = 15) had died 3 months after discharge. Patients who had started empagliflozin with diuretics at higher doses than those prescribed at onset of the episode that led them to be hospitalized did not progress more poorly, more frequently die, visit the emergency room more often, or experience worse adverse effects during follow-up (Supplementary Table 2).
Of the patients who remained alive, 93.8% were still taking empagliflozin at 3 months of follow-up. The reasons for withdrawal (n = 22; 19.6%) were death (15 patients [13.4%]), discontinuation of therapy for unknown reasons (4 [3.6%]), intolerance (1 [0.9%]), urinary discomfort (1 [0.9%]) and palliative care (1 [0.9%]). Type of acute HF, obesity, hypertension, Type 2 diabetes and edema were included as potential confounding factors in the logistic regression analysis, although no statistically significant findings were recorded.
Discussion
This real-world study, which involved more than 100 patients admitted to a Spanish internal medicine department with HF, showed that it was feasible to initiate empagliflozin before discharge from hospital and that treatment was maintained by a large number of participants during follow-up.
In the study sample, mean age was high (85 years), most patients were in NYHA functional class III or IV, and up to 75% had HFpEF. Moreover, patients had numerous comorbid conditions. In the RICA registry, which included patients aged ≥50 years admitted with HF to internal medicine departments in Spain between 2008 and 2019, the mean age was 80 years, up to a third of patients were in functional class III, more than 60% had HFpEF, and comorbidity was very common [17]. Various studies have indicated that in clinical practice, a high number of patients with HF would be eligible for treatment with SGLT2i [18,19]. In fact, in a recent study that analyzed the eligibility of the four pharmacologic pillars for treatment of HFrEF at discharge from hospital, SGLT2i were more frequently prescribed than RAAS inhibitors and mineralocorticoid receptor antagonists, with kidney failure being the main factor limiting prescription of these agents, in contrast with SGLT2i [20]. Furthermore, major differences can be observed in the clinical profile and type of HF depending on the specialist treating the patient (e.g., internal medicine vs cardiology). Older age, more comorbid conditions, and a higher frequency of HFpEF also play a role [21]. Additionally, there are relevant differences with clinical trials. For example, whereas in the EMPA-RESPONSE-HF studies the presence of chronic kidney disease with estimated glomerular filtration rate ≤30 ml/min was an exclusion criterion, and EMPULSE included up to 20 ml/min. In our cohort, 7.1% of patients had a history of G4 chronic kidney disease. Moreover, at the time of admission, 19.6 and 4.5% of patients had an estimated glomerular filtration rate <30 and <20 ml/min, respectively. Patients were older, with more comorbidities and a higher Charlson index. Moreover, the present study showed that 73.2% had HFpEF, whereas in the EMPULSE trial only 28.7% had HF with EF >40%, and in EMPA-RESPONSE-HF, the mean left ventricular ejection fraction was 36 ± 17%, indicating that the phenotype of patients hospitalized in the internal medicine department differs from that shown in clinical trials [12,13]. Consequently, the information provided in the present study is relevant, since the sample is representative of patients with acute HF admitted to internal medicine departments in Spain and treated early with an SGLT2i before discharge to ensure they obtain the maximum benefit from treatment, as recommended in clinical practice guidelines [6,10,11].
The present study showed that before admission, 70.6% of patients were taking a RAAS inhibitor, 49.1% a betablocker and 25.0% a mineralocorticoid receptor antagonist. A recent study performed in Spain and including patients with HFpEF up to 2019 found that 79.8% were taking RAAS inhibitors (12% sacubitril–valsartan), 65.9% were taking betablockers, 27.7% mineralocorticoid receptor antagonists and only 5.1% SGLT2i [1]. A study performed in France showed that 73.7% were taking RAAS inhibitors, 80.3% were taking betablockers, and 21.6% mineralocorticoid receptor antagonists [22]. Despite having improved the percentage of patients taking treatment recommended for HF compared with previous studies, there is still considerable room for improvement in the form of a more favorable prognosis and reduced risk of readmission with HF, especially when treatment is started early, including both before and after discharge, which is the most vulnerable period for affected patients [6,23–25]. Furthermore, the EMPULSE study found that the benefit of adding empagliflozin before discharge was independent of the underlying treatment the patient was taking for HF [26]. In any case, SGLT2i are underused in clinical practice, and clinical findings indicate that these drugs should be prescribed more frequently [27,28].
The EMPULSE study [12] randomized patients during admission when they were hemodynamically stable (mean time from admission to randomization, 3 days). In fact, before randomization, patients had to be treated with a minimum single dose of 40 mg of iv. furosemide (or equivalent iv. loop diuretic, defined as 20 mg of torasemide or 1 mg of bumetanide). The EMPA-RESPONSE-AHF trial [13] was a randomized, placebo-controlled, double-blind, parallel group, multicenter pilot study, in which 80 acute HF patients with and without diabetes were randomized to receive either empagliflozin 10 mg/d or placebo for 30 days. Of note, patients had to be treated with loop diuretics at screening. In the present study, prior to admission, 25% of patients were taking thiazide diuretics and 25% mineralocorticoid receptor antagonists that were maintained during admission. At initiation of empagliflozin, 17.9% were taking high-dose furosemide (≥60 mg), 2.7% were taking hydrochlorothiazide, and 5.4% did not receive any diuretic treatment because the drug was started the day before hospital discharge. The median time until initiation of empagliflozin was 3 days, although patients who started earlier did not experience more complications during follow-up. Similarly, the results of the present study revealed no differences in clinical profile, indicating that empagliflozin could be used when the patient's condition stabilizes during admission. As for the dose of furosemide, while not recommended by guidelines [6,10,11], this study revealed that starting empagliflozin with higher doses of furosemide than at admission did not imply a poorer prognosis, possibly because empagliflozin leads to osmotic diuresis that does not interfere with other treatments or involves more clinical risks than usual in a patient admitted with HF [25,26].
With respect to events at 3 months after discharge, 26.8% of patients had attended the emergency department (at 6 months) and 13.4% had died. In the EMPULSE trial, cardiovascular death or worsening of HF occurred in 34 (12.8%) patients in the empagliflozin group and in 49 (18.5%) in the placebo group (HR: 0.69; 95% CI: 0.45–1.08). In the EMPA-RESPONSE-HF trial, death, re-hospitalization for HF, or worsening HF during hospitalization was reported in four patients (10%) in the empagliflozin group and in 13 patients (33%) in the placebo group (p = 0.014). The findings of the present study can be explained by the profile of patients with acute HF admitted to internal medicine, namely, older age with more comorbidities, a higher Barthel index and more complex management requirements than those recruited in the pivotal clinical trials, thus highlighting the importance of the results reported here.
Finally, most patients continued treatment with empagliflozin during the 3-month follow-up. The frequency of adverse events was similar to that described in clinical trials [8,28,29]. These results could prove even more relevant if we consider the older age, comorbid conditions and frailty that characterize the study patients, since suspending treatment that has proven clinically beneficial is associated with a poorer prognosis and greater risk of complications [30,31].
The present study is subject to a series of limitations. Given its retrospective design, the only data collected were those already included in the patients' electronic clinical history, thus favoring the loss of some variables of clinical interest. However, it is very unlikely that visits to the emergency department, death and changes in treatments, including withdrawal, were not detected, since the health system in Andalusia, Spain is completely computerized and information is readily available, including changes in treatment (drug withdrawal and/or dose modification), which are detected quickly and in real time. Furthermore, the absence of a comparison group limits the generalization of the results obtained. Finally, it would be necessary to replicate these results in other populations with similar characteristics in multicenter studies.
Conclusion
Despite this study has relevant limitations (i.e., small sample size and lack of comparative group), our data suggest that in clinical practice it may be feasible to introduce empagliflozin before discharge in patients admitted to internal medicine with HF. The frequency of complications was as expected owing to the highly complex nature of the patients, and treatment was largely maintained during follow-up.
Summary points
•
While the clinical trials EMPULSE and EMPA-RESPONSE-AHF showed that initiation of empagliflozin during acute heart failure (HF) hospitalization was effective and safe, real-world data remain scarce.
•
This study analyzed the epidemiological, clinical and laboratory characteristics and clinical progress of patients admitted for acute HF who started treatment with empagliflozin before discharge.
•
This retrospective and observational study analyzed 112 adult patients admitted for HF to an Internal Medicine Department at a University hospital in Spain.
•
Mean age was 85.2 ± 6.5 years, 67.9% of patients were women and 73.2% had heart failure with preserved ejection fraction (HFpEF).
•
Before admission, 80.4% were taking loop diuretics, 70.6% renin–angiotensin–aldosterone system inhibitors, 49.1% betablockers and 25% mineralocorticoid receptor antagonists.
•
Median time to starting empagliflozin during admission was 3 days. The dose of furosemide was reduced in 12.4% of patients during hospitalization.
•
At 3 months after discharge, 13.4% of patients died and 26.8% attended the emergency department due to HF.
•
Of the patients who remained alive, 93.8% were taking empagliflozin at 3 months of follow-up.
•
In summary, the initiation of empagliflozin before discharge from hospital in patients admitted with HF was possible and safe in clinical practice.
Financial disclosure
Funded by the Fundación para la investigación biosanitaria de Andalucía Oriental – Alejandro Otero (FIBAO), though an unrestricted grant from Boehringer Ingelheim (BI) – Lilly Alliance. BI was given the opportunity to review the manuscript for medical and scientific accuracy as it relates to Boehringer Ingelheim substances, as well as intellectual property considerations. M Raya-Cruz has given talks, attended conferences and participated in clinical trials sponsored by AstraZeneca, Boehringer Ingelheim, Eli Lilly and Company, Pfizer, Cantabria Labs and Rovi. J Gascón Jurado has attended lectures sponsored by Pfizer. G Olalla de la Torre Peregrín has attended lectures sponsored by Rovi. N Montúfar has attended conferences sponsored by Rovi, Pfizer and Janssen. F Gómez Delgado has given talks, attended conferences and participated in clinical trials sponsored by Ferrer, Esteve, Boehringer Ingelheim, Eli Lilly and Company, Daiichi Sankyo, Novartis, GSK, Pfizer, Janssen-Cilag, Amgen, Viatrix and Sanofi. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
Content Ed Net (Madrid, Spain) provided editorial assistance in the preparation of this manuscript, which was funded by the Fundación para la investigación biosanitaria de Andalucía Oriental – Alejandro Otero (FIBAO).
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary material.docx)
- Download
- 27.26 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Escobar C, Palacios B, Varela L et al. Prevalence, characteristics, management and outcomes of patients with heart failure with preserved, mildly reduced, and reduced ejection fraction in Spain. J. Clin. Med. 11(7), 5199 (2022).
• More than 2% of patients attended in Spain have heart failure (HF), of which around 50% have HF with reduced ejection fraction. The risk of outcomes, particularly HF hospitalization, are high in this population.
2.
Lippi G, Sanchis-Gomar F. Global epidemiology and future trends of heart failure. AME Med. J. 5, 15 (2020).
3.
Gerber Y, Weston SA, Redfield MM et al. A contemporary appraisal of the heart failure epidemic in Olmsted County, Minnesota, 2000 to 2010. JAMA Intern. Med. 175(6), 996–1004 (2015).
4.
Chen S, Huang Z, Liang Y et al. Five-year mortality of heart failure with preserved, mildly reduced, and reduced ejection fraction in a 4880 Chinese cohort. ESC Heart. Fail. 9(4), 2336–2347 (2022).
• In China, one-sixth individuals with HF died in 5 years.
5.
Roger VL. Epidemiology of heart failure. a contemporary perspective. Circ. Res. 128(10), 1421–1434 (2021).
6.
Fernández-Rodríguez JM, Casado J, Formiga F et al. Executive summary of the 2023 update on the consensus regarding basic conduct during hospital admission for patients with acute heart failure. Rev. Clin. Esp. (Barc) 223(8), 499–509 (2023).
7.
McDonagh T, Metra M, Adamo M et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 42(36), 3599–3726 (2021).
8.
Anker SD, Butler J, Filippatos G et al. Empagliflozin in heart failure with a preserved ejection fraction. N. Engl. J. Med. 385(16), 1451–1461 (2021).
•• In patients with heart failure with preserved ejection fraction (HFpEF), the addition of empagliflozin translated into a reduction in the risk of cardiovascular death or HF hospitalization.
9.
Solomon SD, McMurray JJV, Claggett B et al. Dapagliflozin in heart failure with mildly reduced or preserved ejection fraction. N. Engl. J. Med. 387(12), 1089–1098 (2022).
10.
Kittleson MM, Panjrath GS, Amancherla K et al. 2023 ACC Expert Consensus decision pathway on management of heart failure with preserved ejection fraction: a report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 81(18), 1835–1878 (2023).
11.
McDonagh T, Metra M, Adamo M et al. 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure, Developed by the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 44(37), 3627–3639 (2023).
12.
Voors AA, Angermann CE, Teerlink JR et al. The SGLT2 inhibitor empagliflozin in patients hospitalized for acute heart failure: a multinational randomized trial. Nat. Med. 28(3), 568–574 (2022).
•• This clinical trial showed that among patients admitted for HF, initiation of empagliflozin was effective and safe.
13.
Damman K, Beusekamp JC, Boorsma EM et al. Randomized, double-blind, placebo-controlled, multicentre pilot study on the effects of empagliflozin on clinical outcomes in patients with acute decompensated heart failure (EMPA-RESPONSE-AHF). Eur. J. Heart Fail. 22(4), 713–722 (2020).
14.
López-Vilella R, Trenado VD, Cervera BG et al. Sodium-glucose cotransporter 2 inhibitors reduce cardiovascular events in acute heart failure. A real-world analysis. Eur. J. Intern. Med. 104, 128–130 (2022).
15.
Mostaza JM, Pintó X, Armario P et al. SEA 2022 Standards for Global Control of Cardiovascular Risk. Clin. Investig. Arterioscler. 34(3), 130–179 (2022).
16.
Lam CSP, Solomon SD. Classification of Heart Failure According to Ejection Fraction: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 77(25), 3217–3225 (2021).
17.
Montero-Pérez-Barquero M, Escobar-Cervantes C, Dávila-Ramos MF et al. Benefits of dapagliflozin in the whole spectrum of heart failure in clinical practice: the RICA registry. Future Cardiol. 19(6), 323–332 (2023).
18.
Håkansson E, Norberg H, Själander S et al. Eligibility of dapagliflozin and empagliflozin in a real-world heart failure population. Cardiovasc. Ther. 2021, 1894155 (2021).
19.
Thorvaldsen T, Ferrannini G, Mellbin L et al. Eligibility for dapagliflozin and empagliflozin in a real-world heart failure population. J. Card. Fail. 28(7), 1050–1062 (2022).
20.
D'Amario D, Rodolico D, Delvinioti A et al. Eligibility for the 4 pharmacological pillars in heart failure with reduced ejection fraction at discharge. J. Am. Heart Assoc. 12(13), e029071 (2023).
• Showed that in clinical practice, around 46% of patients could receive the four foundational drugs at discharge of patients with HFrEF admitted for HF, up to 71% in the case of SGLT2i.
21.
Álvarez-García J, Salamanca-Bautista P, Ferrero-Gregori A et al. Prognostic impact of physician specialty on the prognosis of outpatients with heart failure: propensity matched analysis of the REDINSCOR and RICA registries. Rev. Esp. Cardiol. (Engl Ed.) 70(5), 347–354 (2017).
22.
Rastogi T, Duarte K, Huttin O et al. The prescription pattern of heart failure medications in reduced, mildly reduced, and preserved ejection fractions. J. Clin. Med. 12(1), 99 (2022).
23.
Trullàs JC, Formiga F, Casado J et al. Initiation, maintenance and withdrawal of disease-modifying treatment during an acute heart failure decompensation. Rev. Clin. Esp. (Barc) 219(8), 464–466 (2019).
24.
Iguchi M, Wada H, Martínez F et al. When should we start sodium-glucose co-transporter inhibitors in patients with heart failure? The importance of early intervention. Eur. Cardiol. 18, e41 (2023).
25.
Greene SJ, Butler J, Fonarow GC. In-hospital initiation of quadruple medical therapy for heart failure: making the post-discharge vulnerable phase far less vulnerable. Eur. J. Heart Fail. 24(1), 227–229 (2022).
26.
Ferreira JP, Blatchford JP, Teerlink JR et al. Mineralocorticoid receptor antagonist use and the effects of empagliflozin on clinical outcomes in patients admitted for acute heart failure: findings from EMPULSE. Eur. J. Heart Fail. 25(10), 1797–1805 (2023).
• Showed that initiation of empagliflozin in patients admitted for acute heart failure was effective and safe, regardless of background treatment with mineralocorticoid receptor antagonists.
27.
Ray GM, Bermudez SR, Anderson JR et al. Utilization rates and predictors of sodium glucose cotransporter 2 inhibitor use in patients with heart failure with or without Type 2 diabetes. Am. J. Health Syst. Pharm. 80(24), 1787–1795 (2023).
• Showed that in clinical practice, despite current guideline recommendations, the use of SGLT2i remains unacceptably low.
28.
Ferreira JP, Zannad F, Butler J et al. Recency of heart failure hospitalization, outcomes, and the effect of empagliflozin: an EMPEROR-Pooled Analysis. JACC Heart Fail. 11(6), 702–712 (2023).
29.
Packer M, Anker SD, Butler J et al. Cardiovascular and renal outcomes with empagliflozin in heart failure. N. Engl. J. Med. 383(15), 1413–1424 (2020).
30.
Bhagat AA, Greene SJ, Vaduganathan M et al. Initiation, continuation, switching, and withdrawal of heart failure medical therapies during hospitalization. JACC Heart Fail. 7(1), 1–12 (2019).
31.
Schrage B, Lund LH, Benson L et al. Association between a hospitalization for heart failure and the initiation/discontinuation of guideline-recommended treatments: an analysis from the Swedish Heart Failure Registry. Eur. J. Heart Fail. 25(7), 1132–1144 (2023).
• Showed that in clinical practice, the early re-/initiation of guideline-directed medical HF therapy was associated with better survival.
Information & Authors
Information
Published In
Copyright
© 2024 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 4 March 2024
Accepted: 26 April 2024
Published online: 24 May 2024
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Progress of patients hospitalized with acute heart failure treated with empagliflozin. (2024) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0027
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Zuyuan Huang, Guoxing Ling, Chen Fang, Zimin Wu, Shigao Ye, Chuanliang Zhang, Cheng Luo, Baoshi Zheng, Mechanisms and Therapeutic Potential of Sodium–Glucose Cotransporter 2 Inhibitors in Heart Failure, Reviews in Cardiovascular Medicine, 10.31083/RCM45833, 27, 4, (2026).