Longer disease progression milestone-free time in people with amyotrophic lateral sclerosis treated versus not treated with intravenous edaravone: results from an administrative claims analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To estimate time-to-progression milestones in people with amyotrophic lateral sclerosis (PALS) treated versus not treated with intravenous (IV) edaravone (Radicava® IV, Mitsubishi Tanabe Pharma America [MTPA], hereafter “IV edaravone”) in a real-world setting. Background: IV edaravone is US FDA approved for the treatment of ALS and was shown in clinical trials to slow the rate of physical functional decline. Patients & methods: This retrospective observational analysis included PALS continuously enrolled in Optum's Clinformatics® Data Mart between 8 August 2017 and 31 December 2021. Cases treated with IV edaravone and controls not treated with IV edaravone were propensity score matched for: age, sex, race, US region of residence, pre-index disease duration, insurance, riluzole prescription; and pre-index claims for cardiovascular disease, artificial nutrition/gastrostomy tube, noninvasive ventilation and all-cause hospitalization. The index date was the first IV edaravone claim for cases; for controls, the index date was randomly assigned after IV edaravone market availability. Restricted mean time lost was calculated for the following disease progression milestones: new use of canes/walkers/wheelchairs, artificial nutrition, noninvasive ventilation, invasive ventilation, speech-generating devices and hospice. Results: Cases (n = 395) were matched to controls (n = 395). Cases had less restricted mean time lost, indicating longer disease progression milestone-free time, for all disease progression milestones. From 0 to 24 months post index, more cases (n = 129) than controls (n = 103) reported no milestones and more controls (n = 232) than cases (n = 131) reported deaths. Conclusion: In a US-based real-world setting, IV edaravone-treated PALS had a longer time to disease progression milestone events and fewer deaths in 2 years compared with PALS not treated with IV edaravone.
Introduction
Amyotrophic lateral sclerosis (ALS) is a fatal neurodegenerative condition that causes neuron cell death and progressive muscular weakness [1]. There is no cure, and mean survival time is between 3 and 5 years after symptom onset [2]. In 2017, the estimated prevalence rate ranged from 5.5 to 9.9 per 100,000 people in the US and was highest in men, Whites and those 60–69 years of age [3]. At the time this study was conducted, the US FDA had approved riluzole and intravenous (IV) edaravone (Radicava® IV, Mitsubishi Tanabe Pharma America [MTPA], hereafter “IV edaravone”) for the treatment of ALS [4,5]. IV edaravone received FDA approval in May 2017 [5]. FDA approval of IV edaravone was based on a pivotal phase III trial (MCI186-19; Study 19) in which IV edaravone was shown to slow the rate of functional decline by 33% (p = 0.0013), as measured by the ALS Functional Rating Scale-Revised (ALSFRS-R), compared with placebo at 24 weeks [6]. Of note, since the completion of the real-world study we report here, the US FDA has approved oral edaravone (Radicava ORS®, MTPA) in May 2022 [5] and sodium phenylbutyrate and taurursodiol (PB-TURSO; approved September 2022 but removed from the market in April 2024 due to negative phase III trial results) [7] for the treatment of people with ALS (PALS), and tofersen for PALS with a mutation in the superoxide dismutase 1 (SOD1) gene in April 2023 [8].
Research studies employing real-world data (RWD) can supplement evidence obtained from randomized controlled trials (RCTs), particularly in rare, heterogeneous diseases like ALS [9,10]. The US FDA recently created a framework to evaluate the use of real-world evidence (RWE) to support evidence generation and the regulatory approval process [11]. As a result, regulators are now examining the use of noninterventional RWE studies to evaluate the effectiveness of therapeutics [12]. The objective of this study was to estimate time-to-progression milestones in propensity score-matched PALS treated versus not treated with IV edaravone using RWD collected from a large US administrative claims database.
Methods
Data source
This was a retrospective, observational, propensity score-matched, comparative effectiveness cohort study using health claims data from the Optum Clinformatics® Data Mart (CDM; Optum, Inc.). The CDM is statistically de-identified under the expert determination method consistent with the Health Insurance Portability and Accountability Act of 1996 and is managed according to Optum customer data use agreements. Therefore, it does not require an institutional review board assessment or approval for secondary analysis as it is not considered human patient research as defined in 45 CFR 46.102. The database includes approximately 17 to 19 million annual covered lives. The population is geographically diverse, spanning all 50 states, and is composed of members with commercial and Medicare Advantage plans. CDM administrative claims submitted for payment by providers and pharmacies are verified, adjudicated and de-identified prior to inclusion. These data, including patient-level enrollment information, are derived from claims submitted for all medical and pharmacy healthcare services with information related to healthcare costs and resource utilization.
Study population
Records from PALS who had previously been treated with IV edaravone (Radicava® IV) were included in the IV edaravone-treated case group if they met the following criteria:
■
Adults aged at least 18 years on the IV edaravone index date (date of the first claim for IV edaravone)
■
Diagnosis of ALS (International Classification of Diseases, 9th/10th Revision, Clinical Modification [ICD-10-CM] code G12.21; [ICD-9-CM] code 335.20) on any claim in any setting
■
Initiated IV edaravone between 8 August 2017 and 31 September 2021 (claim for IV edaravone using Healthcare Common Procedure Coding System [HCPCS] codes J1301, J3490, or C9493 or the National Drug Code [NDC] 70510-2171-xx)
■
May or may not have received treatment with riluzole
PALS may or may not have continued IV edaravone treatment until death or censoring. PALS not treated with IV edaravone were included in the control group if they met criteria 1, 2 and 4 above. For the control group, the index date was randomly assigned under the assumption that the index timepoint was uniformly distributed over the time interval between the diagnosis date and the last claim date.
Confirmation of ALS in individuals treated versus not treated with IV edaravone
Administrative claims for ALS-related symptoms and procedures identifying respiratory-, nerve-, limb- and bulbar-related symptoms in the pre-index period were tabulated for both individuals treated and not treated with IV edaravone and compared with the proportion of symptoms in the 2 groups [13]. These claims were extracted using ICD-9-CM and ICD-10-CM, Current Procedural Terminology (CPT), or HCPCS codes. HCPCS codes are a standardized coding system based on the American Medical Association's CPT that describe specific items and services.
Propensity score matching
Propensity score matching (PSM) estimates the effect of a treatment in nonrandomized, interventional studies by adjusting for potential confounding factors in a mixed population of treated or untreated individuals with varying characteristics to achieve a balanced covariate distribution between the treated and untreated groups [14]. After identifying PALS who had been treated versus not treated with IV edaravone as noted above and described in prior studies [13], a propensity score was estimated for each individual using extreme gradient boosting algorithm and accounted for the following covariates: age, sex, race, US region of residence, pre-index disease duration, insurance (Medicare Advantage vs commercial insurance), riluzole prescription; and pre-index claims for cardiovascular disease, artificial nutrition/gastrostomy tube placement, noninvasive ventilation and all-cause hospitalization. Pre-index disease duration was defined as the period between the date of first claim for ALS diagnosis and the first claim of IV edaravone for IV edaravone-treated PALS. For PALS who were not treated with IV edaravone, the pre-index disease duration was calculated between the date of first claim for ALS diagnosis and the randomly assigned index date. PALS in each group were then matched based on propensity score using the nearest-neighbor method with a caliper width equal to 0.1 of the SD of the logit scores [15] and PALS for whom no matching partner had been found were excluded. Each treated individual was allocated up to 1 untreated individual (in 1:1 matching) with the same (or a very similar) propensity score and treatment effect was evaluated in the matched groups. Standardized mean difference (SMD) was used to examine the balance of covariate distribution between groups treated versus not treated with IV edaravone [15]. SMDs of less than 10% were considered negligible imbalances.
Additional statistical analyses
Demographics and clinical variables were assessed descriptively using counts and percentages for categorical variables and measures of central tendency (mean/median/SD/interquartile range [IQR]) for continuous variables. Analysis of disease progression milestones and deaths used weighted estimates that considered the weights obtained from PSM and the time restriction, since weighted estimates may reduce bias and improve efficiency of the estimates, and thus provide better generalizability to the whole patient population [16].
Disease progression milestones
Six disease progression milestones, including 1) use of gait assistive devices (canes/walkers/wheelchairs), 2) artificial nutrition, 3) noninvasive ventilation, 4) invasive ventilation, 5) speech-generating devices and 6) hospice, were analyzed and their CPT, HCPCS, ICD-10-CM and revenue codes are reported (Table 1). The milestones are not listed in the order that they occurred.
| Milestone description | CPT codes | HCPCS codes | ICD-10-CM codes | Revenue codes |
|---|---|---|---|---|
| M1: Canes/walkers/wheelchairs | E0100, E0105-0159, E0950-E1298, E2201-E2397, E2601-E2625, K0001-K0899 | |||
| M2: Artificial nutrition | 43246, 43760, 43761, 44373, 49440, 49441, 49446, 49450, 49451, 49452, 97542 | B4034-B9998 | ||
| M3: Noninvasive ventilation | A7030-A7039, A7044-A7046, E0464, E0470, E0471 | |||
| M4: Invasive ventilation | 94002-94005 | A4611-A4613, A4623-A4626, A4629, A4483, A7501-A7527, E0460-E0461, E0463, E0472, E0450 | ||
| M5: Speech-generating devices | 92607, 92608, 92609 | E2500-E2599 | ||
| M6: Hospice | 99377, 99378 | V66.7 or Z 51.5 | 0650, 0651, 0655, 0656, 0657, 0659 |
CPT: Current procedural terminology; HCPCS: Healthcare Common Procedure Coding System; ICD-10-CM: International Classification of Diseases 10th Revision Clinical Modification.
Restricted mean time lost
Restricted mean time lost (RMTL) was measured and is defined as the increase/decrease in lost life expectancy due to a specific cause of death, or in the case of a non-fatal outcome, the difference in disease/milestone-free time, considering adjusting mortality as the competing risk [16]. RMTL is reported up to 24 months since the index date for each milestone, and differences in RMTL between groups are presented for controls not treated with IV edaravone and cases treated with IV edaravone. In both groups, PALS were analyzed as a group and also subdivided by whether they were covered by commercial or Medicare Advantage insurance.
A sensitivity analysis strategy proposed by Lin et al. was used to examine the robustness of calculated treatment effects for RMTL analyses to unmeasured confounding [17] using a strategy adapted from the E-value method [18,19]. For unmeasured binary confounder U, two sensitivity analysis parameters are defined: relative risk (RR) of the treatment on a level of U with a given propensity score value, and mean ratio (MR) of U on the RMTL outcome with a given propensity score value. For a pair of specified sensitivity parameters, corresponding 95% CI bounds can be calculated. The behavior of the 95% CI bounds shows the robustness of estimated treatment effects with respect to any unmeasured confounder.
All analyses were conducted using R (version 4.0.3, R Core Team, 2020). Propensity score estimating and matching were done using the MatchIt (version: 4.1.0, 2011) package.
Results
Study population selection & characteristics
Between 8 August 2017 and 31 December 2021, 15,099 adults with ALS in the Optum CDM had initiated IV edaravone, riluzole, or had no treatment (Figure 1). During 1:1 PSM, 7 out of 423 cases did not report sex information and were excluded. Additionally, there were no matches found for 21 patients. Therefore, the matching process resulted in a study population that included 395 PALS with at least 1 claim for IV edaravone and 395 controls not treated with IV edaravone. Demographic and clinical characteristics for both groups after PSM are presented in Table 2. Covariates were balanced between groups as indicated by an SMD of ≤0.1 for all variables. Median (IQR) IV edaravone treatment duration in the IV edaravone-treated group was 7.47 months (3.08, 14.55).

Figure 1. Patient disposition.
Identification and propensity score matching of adult PALS from the Optum CDM who initiated IV edaravone, riluzole, or had no treatment between 8 August 2017 and 31 December 2021.
CDM: Clinformatics® Data Mart; IV: Intravenous; PALS: People with amyotrophic lateral sclerosis.
| Controls – not treated with IV edaravone | Cases – treated with IV edaravone | SMD | |
|---|---|---|---|
| n | 395 | 395 | |
| Age (years), mean (SD) | 63.7 (11.3) | 63.2 (10.4) | 0.0502 |
| Sex, n (%) Female Male | 156 (39.5) 239 (60.5) | 168 (42.5) 227 (57.5) | 0.0304 |
| Insurance, n (%) Commercial Medicare Advantage | 140 (35.4) 255 (64.6) | 154 (39.0) 241 (61.0) | 0.0354 |
| Race, n (%) White Black Other Unknown | 269 (68.1) 31 (7.8) 51 (12.9) 44 (11.1) | 292 (73.9) 22 (5.6) 46 (11.6) 35 (8.9) | 0.0582 0.0127 0.0127 0.0288 |
| Region, n (%) Midwest Northeast South West | 98 (24.8) 71 (18.0) 137 (34.7) 89 (22.5) | 103 (26.1) 69 (17.5) 132 (33.4) 91 (23.0) | 0.0127 0.0051 0.0127 0.0051 |
| Pre-index disease duration (months), mean (SD) | 6.9 (8.8) | 6.0 (8.7) | 0.1 |
| Riluzole prescription, n (%) | 230 (58.2) | 265 (67.1) | 0.0886 |
| Pre-index cardiovascular disease, n (%) | 52 (13.2) | 49 (12.4) | 0.0076 |
| Pre-index artificial nutrition/gastrostomy tube, n (%) | 68 (17.2) | 42 (10.6) | 0.0658 |
| Pre-index noninvasive ventilation, n (%) | 74 (18.7) | 64 (16.2) | 0.0253 |
| Pre-index all-cause hospitalization, n (%) | 112 (28.4) | 91 (23.0) | 0.0532 |
IV: Intravenous; PALS: People with amyotrophic lateral sclerosis; SMD: Standardized mean difference.
ALS-related symptoms & procedures
Claims for ALS-related symptoms and procedures were identified for both groups (Figure 2). These claims were not considered confounding factors and were evenly balanced between cases and controls – individuals in both groups reported a similar proportion of claims for ALS-related symptoms, including bulbar-, limb-, nerve- and respiratory-related symptoms, in the pre-index period. The most common symptoms for individuals in both groups were limb related. IV edaravone-treated PALS had more claims for the insertion of an IV catheter than PALS not treated with IV edaravone.
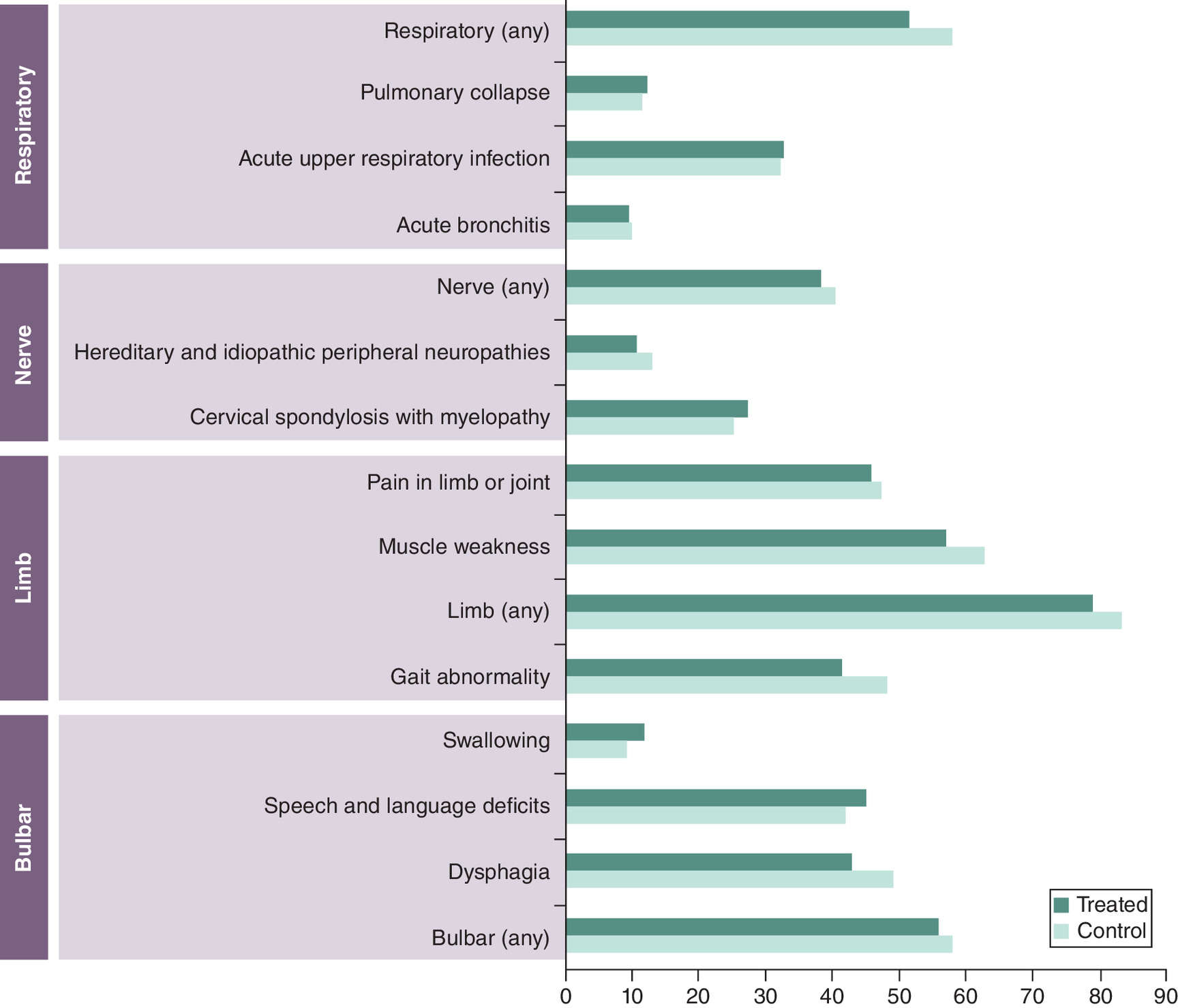
Figure 2. Claims for amyotrophic lateral sclerosis-related symptoms in the pre-index disease duration period.
Claims for ALS-related symptoms, including bulbar-, limb-, nerve- and respiratory-related symptoms, are reported in the pre-index period for the groups treated with IV edaravone (treated; dark blue) versus not treated with IV edaravone (control; light blue). The pre-index disease duration period was defined as the period between the date of ALS diagnosis and the first claim of IV edaravone for IV edaravone-treated cases. For PALS not treated with IV edaravone, the index date was randomly assigned starting on 8 August 2017 (date IV edaravone was available on the market) and ending on 30 September 2021, assuming the index date was uniformly distributed over the time interval between the diagnosis date and last claim date, and pre-index disease duration was calculated based on this assigned index date.
ALS: Amyotrophic lateral sclerosis; IV: Intravenous.
RMTL for reported disease progression milestones
RMTL was calculated for 6 disease progression milestones, including new use of canes/walkers/wheelchairs, artificial nutrition, noninvasive ventilation, invasive ventilation, speech-generating devices and hospice (Table 3). For all milestones, IV edaravone-treated cases had a smaller amount of time lost due to reaching disease progression milestones than controls not treated with IV edaravone based on RMTL for PALS overall, and when grouping PALS based on commercial or Medicare Advantage insurance coverage.
| Commercial Insurance | |||||
|---|---|---|---|---|---|
| Milestone† | Not treated with IV edaravone | Treated with IV edaravone | Difference in RMTL (95% CI) | ||
| n (%) | RMTL (95% CI) | n (%) | RMTL (95% CI) | ||
| Canes/walkers/wheelchairs | 37.0 (24.0) | 12.66 (8.95, 16.38) | 29.7 (19.3) | 6.29 (4.39, 8.19) | 6.37 (2.2, 10.55) |
| Artificial nutrition | 39.0 (25.3) | 11.11 (7.3, 14.92) | 23.2 (15.1) | 5.02 (3.27, 6.77) | 6.09 (1.9, 10.28) |
| Noninvasive ventilation | 31.0 (20.1) | 10.61 (6.41, 14.81) | 24.1 (15.7) | 5.91 (4.04, 7.78) | 4.7 (0.1, 9.29) |
| Invasive ventilation | 5.0 (3.2) | 1.65 (-0.81, 4.12) | 1.0 (0.7) | 1.1 (0.14, 2.06) | 0.55 (-2.09, 3.2) |
| Speech-generating devices | 31.0 (20.1) | 5.98 (2.05, 9.92) | 16.0 (10.4) | 2.83 (1.34, 4.31) | 3.15 (-1.05, 7.36) |
| Hospice | 18.0 (11.7) | 4.79 (1.6, 7.97) | 13.8 (9.0) | 2.09 (0.79, 3.39) | 2.7 (-0.74, 6.14) |
| Medicare Advantage | |||||
| Milestone† | Not treated with IV edaravone | Treated with IV edaravone | Difference in RMTL (95% CI) | ||
| n (%) | RMTL (95% CI) | n (%) | RMTL (95% CI) | ||
| Canes/walkers/wheelchairs | 56.0 (23.2) | 10.02 (7.32, 12.72) | 42.4 (17.5) | 5.39 (4.1, 6.67) | 4.63 (1.64, 7.62) |
| Artificial nutrition | 61.0 (25.3) | 9.32 (6.4, 12.24) | 48.8 (20.2) | 5.42 (4.08, 6.75) | 3.9 (0.69, 7.12) |
| Noninvasive ventilation | 37.0 (15.4) | 6.87 (4.31, 9.42) | 24.5 (10.1) | 3.99 (2.81, 5.17) | 2.88 (0.06, 5.7) |
| Invasive ventilation | 7.0 (2.9) | 4.15 (1.71, 6.59) | 3.1 (1.3) | 0.58 (0.09, 1.07) | 3.57 (1.08, 6.06) |
| Speech-generating devices | 27.0 (11.2) | 3.18 (0.96, 5.4) | 14.0 (5.8) | 1.52 (0.74, 2.29) | 1.66 (-0.69, 4.02) |
| Hospice | 24.0 (10.0) | 3.87 (1.47, 6.27) | 37.5 (15.5) | 2.43 (1.47, 3.39) | 1.44 (-1.14, 4.02) |
| Overall | |||||
| Milestone† | Not treated with IV edaravone | Treated with IV edaravone | Difference in RMTL (95% CI) | ||
| n (%) | RMTL (95% CI) | n (%) | RMTL (95% CI) | ||
| Canes/walkers/wheelchairs | 93.0 (23.5) | 10.9 (8.73, 13.07) | 72.1 (18.2) | 5.68 (4.61, 6.74) | 5.22 (2.8, 7.64) |
| Artificial nutrition | 100.0 (25.3) | 8.2 (5.95, 10.44) | 72.0 (18.2) | 4.6 (3.59, 5.61) | 3.6 (1.13, 6.06) |
| Noninvasive ventilation | 68.0 (17.2) | 3.52 (1.67, 5.38) | 48.6 (12.3) | 0.75 (0.29, 1.2) | 2.78 (0.87, 4.69) |
| Invasive ventilation | 12.0 (3.0) | 4.02 (2.05, 5.98) | 4.2 (1.1) | 1.94 (1.23, 2.66) | 2.07 (-0.02, 4.17) |
| Speech-generating devices | 58.0 (14.7) | 9.78 (7.46, 12.1) | 30.0 (7.6) | 5.27 (4.21, 6.33) | 4.51 (1.95, 7.07) |
| Hospice | 42.0 (10.6) | 4.16 (2.29, 6.02) | 51.3 (13.0) | 2.32 (1.55, 3.09) | 1.83 (-0.19, 3.85) |
†
Milestones are not listed in the order they occurred.
CI: Confidence interval; IV: Intravenous; PALS: People with amyotrophic lateral sclerosis; RMTL: Restricted mean time lost.
Disease progression milestones & deaths from 0 to 24 months
Disease progression milestones and deaths are reported from 0 to 12 months, 12 to 24 months and 0 to 24 months after the index date (Table 4). Weights were estimated from the propensity score model and the resulting estimated percentages may be generalized to the patient population. Overall, more IV edaravone-treated cases (n = 129) reported an absence of milestones than controls not treated with IV edaravone (n = 103) from 0 to 24 months after the index date. Fewer deaths occurred in IV edaravone-treated cases (n = 131) than in controls not treated with IV edaravone (n = 232) from 0 to 24 months after the index date.
| (a) | Not treated with IV edaravone | Treated with IV edaravone | ||
|---|---|---|---|---|
| 0–12 months | 12–24 months | 0–12 months | 12–24 months | |
| Absence of milestones, n (%) | 47.6 (26.0) | 55.8 (45.7) | 67.0 (34.7) | 62.0 (55.4) |
| Deaths, n (%) | 136.8 (74.9) | 94.7 (77.5) | 79.0 (40.9) | 52.0 (46.4) |
| (b) | Not treated with IV edaravone | Treated with IV edaravone | ||
| 0–24 months | 0–24 months | |||
| Absence of milestones, n (%) | 103 (33.9) | 129 (42.3) | ||
| Deaths, n (%) | 232 (75.9) | 131 (43.0) | ||
IV: Intravenous.
Sensitivity analyses
In Figure 3, contour plots show the lower bounds of 95% CI for use of canes/walkers/wheelchairs, artificial nutrition, noninvasive ventilation and speech-generating devices, which had relatively large estimated treatment effects. The gray scales represent different lower bound values of the lower 95% confidence bound of the treatment effect, with the lighter shades indicating large effect values and darker shades indicating negative values. The solid curve in the middle of the plots represents when the lower bound of the lower 95% confidence bound of the treatment effect is zero. For the disease progression milestones including use of canes/walkers/wheelchairs and artificial nutrition, the benefit of IV edaravone treatment still holds under RR <2 and MR <2, as the lower bound of the 95% confidence bounds of the treatment effect is above the solid zero curves. This indicates the estimated treatment effects for these 2 milestones are tolerable to relatively high deviations from the ignorability assumption, i.e., no unmeasured confounder. The RR <1.6 and MR <2 for noninvasive ventilation to hold the above-zero treatment effect also indicates a moderate robustness to unmeasured confounding.
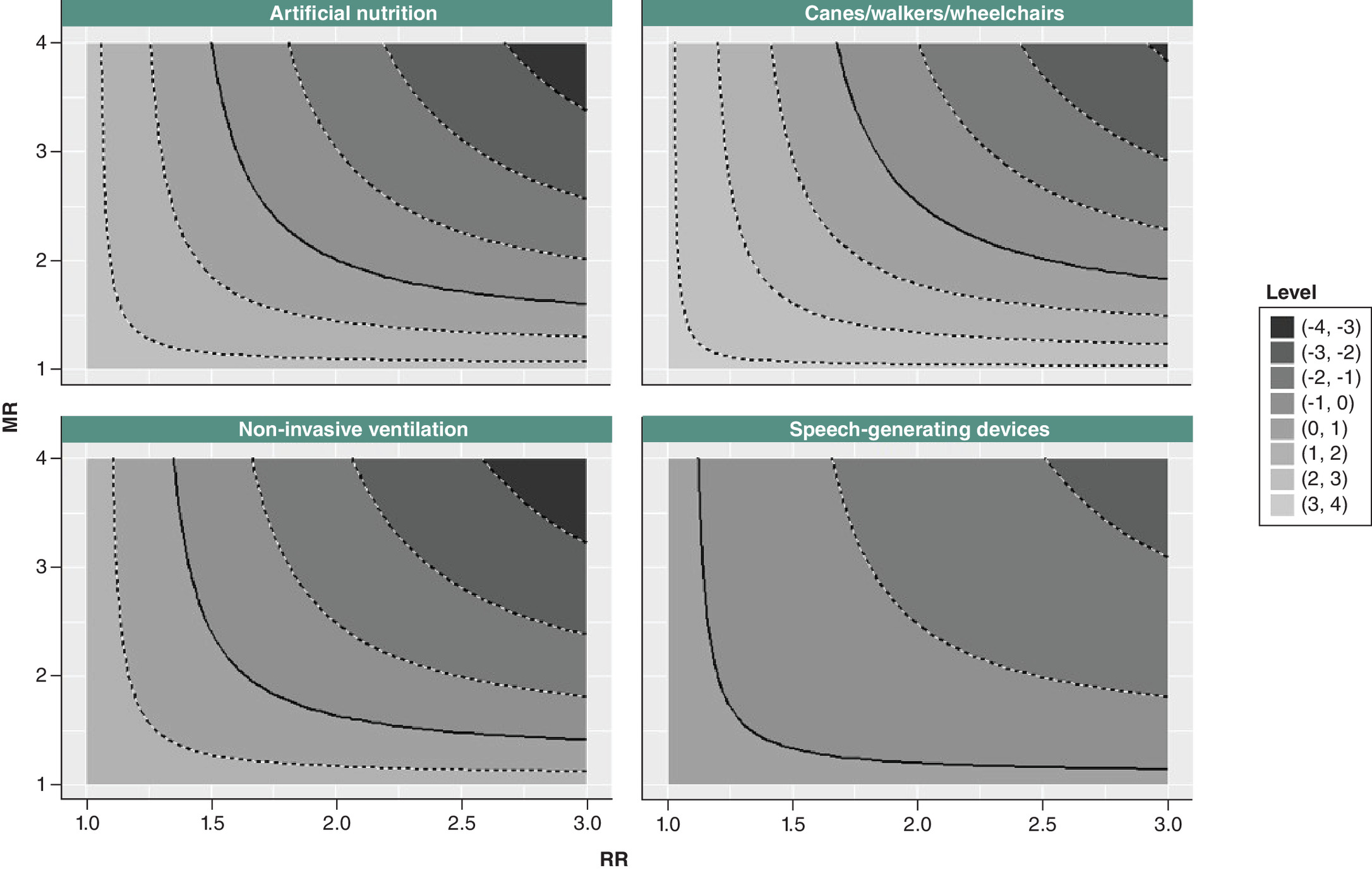
Figure 3. Contour plots for lower bounds of treatment effect by milestones.
Contour plots show the lower bounds of the 95% confidence interval for use of artificial nutrition, canes/walkers/wheelchairs, noninvasive ventilation and speech-generating devices. The gray scales represent different lower bound values of the lower 95% confidence bound of the treatment effect, with lighter shades indicating large effect values and darker shades indicating negative values. The solid curve in the middle of the plots represents when the lower bound value of the lower 95% confidence bound of the treatment effect is zero.
MR: Mean ratio; RR: Relative risk.
Discussion
In this case–control study of PALS with commercial and Medicare Advantage insurance in a large database, IV edaravone-treated cases had a smaller amount of time lost due to reaching disease progression milestones than controls not treated with IV edaravone based on RMTL for all milestones: new use of canes/walkers/wheelchairs, artificial nutrition, noninvasive ventilation, invasive ventilation, speech-generating devices and hospice. Additionally, more IV edaravone-treated cases reported an absence of disease progression milestones or death from 0 to 24 months after the index date than controls who were not treated with IV edaravone.
The ALSFRS-R is a 12 item questionnaire aimed at assessing function in daily activities [20]. It is used to track ALS progression, and the degree of impairment and speed of progression varies by patient, with some patients experiencing severe limb symptoms but few bulbar (speech and swallowing) symptoms, and vice versa [21–26]. However, the ALSFRS-R does not directly report the timing of certain ALS milestones, such as the need for assistive devices used for walking or breathing, which are key to a patient's quality of life. Additionally, the King's and Milano-Torino Staging (MiToS) ALS staging systems do not provide much information about the timing of these critical milestones [27]. A more recent tool to describe ALS progression called the Tollgate-based ALS Staging System (TASS) measures ALS progression and consists of 27 tollgates, or critical clinical events, including the need for a walker/wheelchair or communication device [28]. One group developed and applied an ALSFRS-R-to-TASS mapping methodology to a large database to estimate tollgate-based time trajectories that may be used to inform patients and clinicians about these life-changing milestones [29], since most databases do not provide patient records pertaining to TASS information. Due to the small amount of data in the ALS field regarding time-to-milestone progression, the current study helps to fill the knowledge gap by providing RWD on the general timing to milestones in PALS using different treatment regimens.
In this study, RMTL was selected to represent the treatment effect for 2 reasons, even though alternative approaches – the cause-specific hazard function (which calculates the cause-specific hazard ratio [cHR]) and the subdistribution hazard function (which calculates the subdistribution hazard ratio [sHR]) – are generally used for competing risk analysis based on hazards. First, estimations and statistical analyses based on cHR and sHR have several limitations; these limitations have been previously described [30]. Second, in our study, disease progression milestones competed with each other, and death was another competing event. Median survival would no longer be useful as it would become a biased parameter in the scenario with competing risks. By contrast, RMTL is estimated as the area under the cumulative incidence function (CIF) curve up to a certain time. As the CIF curve can identify the probability of one event occurring in a given time period in the presence of other events, the analysis captured the mean amount of time lost due to a particular cause Therefore, RMTL was analyzed in this study, and may be better understood by clinicians and PALS.
In 2023, a literature review that discussed the epidemiology and economic burden of ALS in the US highlighted costs associated with ALS stratified by disease stage/milestone and reported substantially higher costs for later-stage milestones as compared with earlier-stage milestones [31]. Additional studies examining the association of treatment for ALS with time-to-milestone progression and survival, together with an understanding of the economic burden of these factors, would be beneficial for ongoing clinical trials and cost-effectiveness models for ALS treatments.
In line with this, the current study assessed time to milestones, and additionally provided RWD on the mortality of PALS who were treated versus not treated with IV edaravone, adding to our previous RWD study reporting that PALS who were prescribed IV edaravone and continued using it over 31 months after the index date survived longer than those who were not treated with IV edaravone [13]. That study contained similar limitations to the current study, which are described below.
When evaluating the results of this study, we do need to consider several limitations. The current study was comprised only of PALS who had commercial health coverage or Medicare Advantage plans. Therefore, results of this analysis may not be generalizable to PALS who have different or no health insurance coverage. Another limitation is that administrative claims data, upon which this study is based, may be impacted by social determinants of health, which were not collected for adjustment in this analysis. Additionally, administrative claims data may be impacted by coding limitations and entry error. Also, selection bias and/or smaller sample sizes may have resulted from underdiagnosis of ALS, as some PALS were excluded from this analysis, including untreated PALS, those without an appropriately recorded diagnosis and those not enrolled in the Optum CDM during the post-index period. While PSM was used to help control differences between cohorts, adjustment was restricted to measurable administrative claims characteristics. Consequently, PALS in our study may have been healthier than the total cohort of PALS in the database.
At the same time, this is a large, carefully conducted retrospective analysis with a number of strengths. The analysis drew from a large, real-world population of PALS during a similar time frame using the Optum CDM administrative claims database, following them for up to 2 years after their index date. To minimize differences due to the heterogeneity of ALS, individuals from the treated and control groups were propensity score matched on 12 items to ensure balance. This methodology is meant to overcome as many potential limitations as possible. Future studies could assess time to disease progression milestones and survival analyses in other large retrospective datasets, including electronic medical records or other insurance databases, to corroborate these results.
Conclusion
This retrospective, observational, propensity score-matched study suggests that MTPA IV edaravone treatment in PALS in a real-world setting is associated with fewer reported disease progression milestones and deaths during the first 2 years after the index date. These results provide an example of real-world impact of IV edaravone in PALS that supports the findings of a 33% slowing of functional loss, as measured by the ALSFRS-R in the pivotal RCT of IV edaravone [6]. This RWD may be useful to payers, healthcare providers, PALS and caregivers in evaluating the real-world impact of edaravone treatment.
Summary points
•
Intravenous (IV) edaravone has been FDA approved for the treatment of amyotrophic lateral sclerosis (ALS) and was shown in clinical trials to slow the rate of physical functional decline.
•
People with amyotrophic lateral sclerosis (PALS) continuously enrolled in Optum's Clinformatics® Data Mart (CDM) between 8 August 2017 and 31 December 2021 were included in this retrospective observational analysis.
•
Cases treated with IV edaravone (n = 395) and controls not treated with IV edaravone (n = 395) were propensity score matched for: age, sex, race, US region of residence, pre-index disease duration, Medicare Advantage versus commercial insurance, riluzole prescription; and pre-index claims for cardiovascular disease, artificial nutrition/gastrostomy tube placement, noninvasive ventilation and all-cause hospitalization.
•
Restricted mean time lost (RMTL) was calculated for the following 6 disease progression milestones up to 24 months after the index date: new use of canes/walkers/wheelchairs, artificial nutrition, noninvasive ventilation, invasive ventilation, speech-generating devices and hospice.
•
Cases had a smaller amount of time lost due to reaching disease progression milestones than controls based on RMTL for all six milestones.
•
More cases (n = 129) than controls (n = 103) reported no milestones from 0 to 24 months after the index date.
•
More controls (n = 232) than cases (n = 131) reported deaths from 0 to 24 months after the index date.
•
The results of these analyses provide evidence of a real-world impact of IV edaravone and may help payers and clinicians when assessing the utility of edaravone use.
Author contributions
All authors contributed to the study's conception and design. M Ciepielewska and M Hagan performed data collection. J Zhang and Y Liu performed data analysis and interpretation. All authors drafted, reviewed, revised and commented on previous versions of the article. All authors read and approved the final version to be published.
Acknowledgments
Previously presented at 2022 Northeast Amyotrophic Lateral Sclerosis Consortium, 2022 Academy of Managed Care Pharmacy Nexus, 2022 International Symposium on ALS/MND, 2023 California ALS Research Summit, 2023 Muscular Dystrophy Association, 2023 American Academy of Neurology, 2023 Neuromuscular Study Group, 2023 Northeast Amyotrophic Lateral Sclerosis Consortium, 2023 World Congress of Neurology, 2023 International Symposium on ALS/MND.
Financial disclosure
This study was sponsored by Mitsubishi Tanabe Pharma America, Inc. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
JD Berry reports research funding from Alexion, Biogen, Mitsubishi Tanabe Pharma America, Inc. (MTPA), Brainstorm Cell Therapeutics, Amylyx Pharmaceuticals, nQ Medical, MT Pharma Holdings of America (MTPHA), Transposon Therapeutics, RAPA Therapeutics, National Institute of Neurological Disorders and Stroke, Muscular Dystrophy Association, ALS Finding a Cure, ALS Association and ALS One. He has consulted on scientific advisory boards for Amylyx, MTPA, MTPHA. He has acted as a consultant for Amylyx, Alexion and Biogen. He is a member of a DSMB for Sanofi and a trial support committee for Biogen. And, he has been an educational speaker for Projects in Knowledge, Inc. M Hagan is a former employee of MTPA. J Zhang and Y Liu are employees of Princeton Pharmatech, which has received consultancy fees from MTPA. M Ciepielewska is an employee of MTPA. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
The authors thank p-value communications for editorial assistance and I Brody of p-value communications (NJ, USA) for providing medical writing support, which was funded by Mitsubishi Tanabe Pharma America, Inc. (NJ, USA) in accordance with Good Publication Practice Guidelines 2022.
Data sharing statement
All data generated or analyzed during this study are included in this published article.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Brown RH, Al-Chalabi A. Amyotrophic lateral sclerosis. N. Engl. J. Med. 377(2), 162–172 (2017).
2.
Brooks BR, Jorgenson JA, Newhouse BJ, Shefner JM, Agnese W. Edaravone in the treatment of amyotrophic lateral sclerosis: efficacy and access to therapy – a roundtable discussion. Am. J. Manag. Care 24(Suppl. 9), S175–S186 (2018).
• This article reported on a collaborative roundtable discussion on use of Mitsubishi Tanabe Pharma America (MTPA) edaravone in the treatment of amyotrophic lateral sclerosis (ALS), with a focus on the edaravone clinical development program, efficacy of edaravone and access to therapy.
3.
Mehta P, Raymond J, Punjani R et al. Prevalence of amyotrophic lateral sclerosis in the United States using established and novel methodologies, 2017. Amyotroph. Lateral Scler. Frontotemporal Degener. 24(1–2), 108–116 (2023).
4. .
Rilutek® (riluzole). Prescribing information. Covis Pharmaceuticals, Inc, NC, USA (2016).
5. .
Radicava® (edaravone) injection and Radicava ORS® (edaravone) oral suspension. Prescribing Information. Mitsubishi Tanabe Pharma Corporation, NJ, USA (2022).
6.
Writing Group; Edaravone (MCI-186) ALS 19 Study Group. Safety and efficacy of edaravone in well defined patients with amyotrophic lateral sclerosis: a randomised, double-blind, placebo-controlled trial. Lancet Neurol. 16(7), 505–512 (2017).
•• This is the pivotal phase III study that assessed the safety and efficacy of MTPA IV edaravone for an enriched subpopulation of patients with ALS.
7. .
Relyvrio® (sodium phenylbutyrate and taurursodiol). Prescribing information. Amylyx Pharmaceuticals, Inc, MA,USA (2022).
8. .
QALSODY® (tofersen) injection. Prescribing information. Biogen MA Inc, MA, USA (2023).
9.
Berger ML, Sox H, Willke RJ et al. Good practices for real-world data studies of treatment and/or comparative effectiveness: recommendations from the joint ISPOR-ISPE Special Task Force on real-world evidence in health care decision making. Pharmacoepidemiol. Drug Saf. 26(9), 1033–1039 (2017).
10.
Beaulieu-Jones BK, Finlayson SG, Yuan W et al. Examining the use of real-world evidence in the regulatory process. Clin. Pharmacol. Ther. 107(4), 843–852 (2020).
11.
US Food and Drug Administration. Framework for FDA's real-world evidence program. (2018) (Accessed 10 February 2023). https://www.fda.gov/media/120060/download
12.
Franklin JM, Patorno E, Desai RJ et al. Emulating randomized clinical trials with nonrandomized real-world evidence studies: first results from the RCT DUPLICATE initiative. Circulation 143(10), 1002–1013 (2021).
13.
Brooks BR, Berry JD, Ciepielewska M et al. Intravenous edaravone treatment in ALS and survival: an exploratory, retrospective, administrative claims analysis. EClinicalMedicine 52, 101590 (2022).
•• This real-world analysis evaluated overall survival in US patients with ALS treated with MTPA IV edaravone compared with those not treated with MTPA IV edaravone.
14.
Austin PC. Statistical criteria for selecting the optimal number of untreated subjects matched to each treated subject when using many-to-one matching on the propensity score. Am. J. Epidemiol. 172(9), 1092–1097 (2010).
15.
Stuart EA, Lee BK, Leacy FP. Prognostic score-based balance measures can be a useful diagnostic for propensity score methods in comparative effectiveness research. J. Clin. Epidemiol. 66(Suppl. 8), S84–S90; e1 (2013).
16.
Conner SC, Trinquart L. Estimation and modeling of the restricted mean time lost in the presence of competing risks. Stat. Med. 40(9), 2177–2196 (2021).
• This study illustrated estimation and statistical modeling of restricted mean time lost (RMTL) in the presence of competing risks.
17.
Lin Z, Ni A, Lu B. Matched design for marginal causal effect on restricted mean survival time in observational studies. J. Caus. Infer. 11(1), 20220035 (2023).
18.
Ding P, VanderWeele TJ. Sensitivity analysis without assumptions. Epidemiology 27(3), 368–377 (2016).
19.
VanderWeele TJ, Ding P. Sensitivity analysis in observational research: introducing the E-value. Ann. Intern. Med. 167(4), 268–274 (2017).
20.
Cedarbaum JM, Stambler N, Malta E et al. The ALSFRS-R: a revised ALS functional rating scale that incorporates assessments of respiratory function. BDNF ALS Study Group (phase III). J. Neurol. Sci. 169(1–2), 13–21 (1999).
21.
Proudfoot M, Jones A, Talbot K, Al-Chalabi A, Turner MR. The ALSFRS as an outcome measure in therapeutic trials and its relationship to symptom onset. Amyotroph. Lateral Scler. Frontotemporal Degener. 17(5–6), 414–425 (2016).
22.
Beghi E, Chio A, Couratier P et al. The epidemiology and treatment of ALS: focus on the heterogeneity of the disease and critical appraisal of therapeutic trials. Amyotroph. Lateral Scler. 12(1), 1–10 (2011).
23.
Balendra R, Jones A, Jivraj N et al. Estimating clinical stage of amyotrophic lateral sclerosis from the ALS Functional Rating Scale. Amyotroph Lateral Scler Frontotemporal Degener. 5(3–4), 279–284 (2014).
24.
Chio A, Mora G, Leone M et al. Early symptom progression rate is related to ALS outcome: a prospective population-based study. Neurology 59(1), 99–103 (2002).
25.
Kollewe K, Mauss U, Krampfl K, Petri S, Dengler R, Mohammadi B. ALSFRS-R score and its ratio: a useful predictor for ALS-progression. J. Neurol. Sci. 275(1–2), 69–73 (2008).
26.
Roche JC, Rojas-Garcia R, Scott KM et al. A proposed staging system for amyotrophic lateral sclerosis. Brain 135(Pt 3), 847–852 (2012).
27.
Fang T, Al Khleifat A, Stahl DR et al. Comparison of the King's and MiToS staging systems for ALS. Amyotroph. Lateral Scler. Frontotemporal Degener. 18(3–4), 227–232 (2017).
28.
Dalgic OO, Erenay FS, Pasupathy KS, Ozaltin OY, Crum BA, Sir MY. Tollgate-based progression pathways of ALS patients. J. Neurol. 266(3), 755–765 (2019).
29.
Dalgic OO, Wu H, Safa Erenay F et al. Mapping of critical events in disease progression through binary classification: application to amyotrophic lateral sclerosis. J. Biomed. Inform. 123, 103895 (2021).
30.
Wu H, Yuan H, Yang Z, Hou Y, Chen Z. Implementation of an alternative method for assessing competing risks: restricted mean time lost. Am. J. Epidemiol. 191(1), 163–172 (2022).
• This article recommends use of RMTL and the difference in RMTL in analyses of competing risks data, mostly focusing on clinical and epidemiological studies where there is a comparison of treatment effects between two groups for survival data.
31.
Berry JD, Blanchard M, Bonar K et al. Epidemiology and economic burden of amyotrophic lateral sclerosis in the United States: a literature review. Amyotroph. Lateral Scler. Frontotemporal Degener. 24(5-6), 436–448 (2023).
• This literature review provides an up-to-date understanding of the epidemiology and cost/healthcare resource use burden of ALS in the US, including a discussion of costs associated with ALS stratified by disease stage/milestone.
Information & Authors
Information
Published In
Copyright
© 2025 Mitsubishi Tanabe Pharma America, Inc. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 31 January 2024
Accepted: 3 December 2024
Published online: 21 January 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Longer disease progression milestone-free time in people with amyotrophic lateral sclerosis treated versus not treated with intravenous edaravone: results from an administrative claims analysis. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0007
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Yihan Shen, Siyu Shen, Zhen-Ge Luo, Gene-targeted versus broad-spectrum therapies in ALS: comparative lessons and strategic outlook, Journal of Genetics and Genomics, 10.1016/j.jgg.2026.01.012, 53, 7, (1159-1179), (2026).
- Tifenn Charbonnel, Elodie Richard, Adrien Dupuis, Maelys Palla, Patrick Vourc’h, Philippe Corcia, Yara Al Ojaimi, Hélène Blasco, The preclinical discovery and development of edaravone for the treatment of amyotrophic lateral sclerosis: what lessons have we learnt?, Expert Opinion on Drug Discovery, 10.1080/17460441.2026.2619067, 21, 2, (147-160), (2026).