MOMENT registry: Patients with advanced non-small-cell lung cancer harboring MET exon 14 skipping treated with systemic therapy
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: MET exon 14 (METex14) skipping occurs in 3–4% of non-small-cell lung cancer (NSCLC) cases. Low frequency of this alteration necessitated open-label, single-arm trials to investigate MET inhibitors. Since broad MET biomarker testing was only recently introduced in many countries, there is a lack of historical real-world data from patients with METex14 skipping NSCLC receiving conventional therapies. Given the rarity of this population and limitations of existing real-world data sources, the MOMENT registry aims to prospectively collect uniform, comprehensive, high-quality data from patients with METex14 skipping advanced NSCLC treated in routine clinical practice, which can support clinical and regulatory decision making. Patients & methods: MOMENT is a multinational, non-interventional disease registry collecting data on patients with METex14 skipping advanced NSCLC receiving any systemic anticancer therapy. Newly diagnosed patients and those already receiving treatment are eligible. Patients with previous participation in a clinical trial can be included if they receive at least one subsequent therapy line in a routine clinical setting. Eligible systemic treatment includes all available anticancer therapies (approved, conditionally approved or provided through Early Access). Data collection includes biomarker testing results, demographics, baseline clinical characteristics, treatment details and effectiveness, safety information and imaging. Registry site inclusion is dependent on confirmation that local METex14 skipping detection methods are sufficient to confirm METex14 skipping status. MOMENT is currently active at more than 60 sites across Europe and North America and approximately 700 patients are expected to be enrolled within the next 4 years. The first patient was enrolled on 4 October 2022. After completion of data collection, MOMENT data can be shared with external parties to conduct non-interventional studies. Discussion/conclusion: The MOMENT registry collects comprehensive, high-quality real-world data from patients with METex14 skipping advanced NSCLC receiving systemic anticancer treatment in a routine clinical setting, to enable future studies informing regulatory decisions and optimal care for this rare population.
Clinical Trial Registration: NCT05376891 (ClinicalTrials.gov); EUPAS47602 (EU PAS register no.)
Plain language summary
What is the MOMENT Registry?
The MOMENT registry is a multi-national, large-scale, disease registry designed to gather high quality information on people with a rare type of advanced non-small-cell lung cancer (NSCLC), called MET exon 14 (METex14) skipping, who have received any type of anticancer treatment which affects the whole body.
Who can be included in this registry?
People who have been newly diagnosed with METex14 skipping advanced NSCLC and those who are already receiving treatment for the disease can be included. People who have previously taken part in a clinical trial can be included, if they are due to receive further cancer treatment in the clinic.
How many people are expected to be enrolled?
The MOMENT registry includes people from cancer treatment centers from over 60 locations across 14 countries in Europe and North America. The registry is expected to enroll about 700 people in the next 4 years.
What type of data does the registry collect?
The registry collects information on cancer biomarker test results, the characteristics of people who develop METex14 skipping advanced NSCLC, the effectiveness of the anticancer treatment that they receive and any side effects that they experience with these treatments.
Why is this registry needed?
The high-quality data collected in the MOMENT registry will allow a better understanding of METex14 skipping advanced NSCLC and the effectiveness of the anticancer treatment that people receive. It will serve as a database for future analysis of this rare disease.
Background
Mesenchymal–epithelial transition factor (MET) tyrosine kinase receptor exon 14 (METex14) skipping is a MET alteration that leads to the dysregulation of MET signaling in 3–4% of patients with non-small-cell lung cancer (NSCLC) [1,2]. Highly-selective MET inhibitors, such as tepotinib, capmatinib and savolitinib are a new class of treatment targeting this alteration [3]. Due to the low frequency of this alteration and therefore the limited number of patients, MET inhibitors have typically been investigated in open-label, single-arm trials [4–6].
Although MET inhibitors are currently available as treatment options for patients in routine clinical practice around the world, MET biomarker testing has only recently been introduced, globally. Since 2021, treatment guidelines such as the American Society of Clinical Oncology and Ontario Health (Cancer Care Ontario), NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) and the European Society for Medical Oncology Clinical Practice Guidelines, began including recommendations for testing for METex14 skipping in patients with NSCLC [7–9]. Therefore, there are currently limited historical data on METex14 skipping NSCLC in real-world data (RWD) sources, and the characteristics, biomarker testing, treatment patterns and treatment outcomes of these patients are not yet well-described in the published literature. High-quality RWD on patients with METex14 skipping NSCLC treated in routine clinical care are important to enable research that helps to better understand and treat these patients. Such research may also help to contextualize and strengthen the results from single-arm clinical trials. Most regulatory agencies consider RWD as complementary to clinical trial data for regulatory decisions. Importantly, published guidelines highlight data quality as a key factor in determining their usability, especially for regulatory purposes [10–12].
Previous descriptive studies of patients with METex14 skipping NSCLC using RWD have highlighted general challenges to research in this population, such as suboptimal data quality and limited availability of oncology-specific clinical parameters, which are not always recorded when using secondary data from routine clinical care settings [13,14] (i.e., data that are not collected for specific research purposes) [15]. Primary RWD, which are prospectively and systematically collected for research purposes, have the potential to deliver more comprehensive and higher quality information from routine clinical care than is typically available in secondary RWD sources [15,16]. The collection of RWD can enable analyses that better inform clinical and regulatory decision making, including those relating to indications that are rare or not yet well researched.
The objective of the ongoing Met nOn sMall cEll caNcer regisTry (MOMENT) registry, which applies primary data collection, is to enable future analyses of uniform, comprehensive and high-quality data on patients with METex14 skipping advanced NSCLC. MOMENT data are intended to allow better understanding of characteristics and treatment outcomes of this rare patient population, and to adequately complement and strengthen existing evidence from clinical trials.
Methods
Registry design
MOMENT (ClinicalTrials.gov identifier: NCT05376891; EU PAS register no.: EUPAS47602) is a multinational, non-interventional disease registry that utilizes longitudinal follow-up to prospectively collect high-quality, standardized, and contemporaneous data on patients with METex14 skipping advanced NSCLC, who are receiving any type of systemic anticancer therapy in routine clinical practice. The disease registry design applies available recommendations from the European Medicines Agency (EMA) on disease registries and registry-based studies to ensure collection of high-quality harmonized and standardized data with quantifiable quality indicators in terms of completeness, accuracy, validity, consistency and integrity (EMA/426390/2021) [10]. The registry protocol was developed in collaboration with physicians, principal investigators and regulatory agencies to incorporate input on selection of core data elements and other registry design elements such as quality control measures. The registry was designed to closely emulate interventional clinical trial data collection processes as far as possible without imposing treatment decisions or patient follow-up requirements. For example, data are continuously and prospectively checked for errors or omissions via automated system processes, and epidemiological and medical data are reviewed at specified timepoints based on an Epidemiological and Medical Data Monitoring plan. Written favorable opinion or approval of the relevant Independent Ethics Committee (IEC)/Institutional Review Board (IRB) will be obtained before commencement of the registry at each participating site. Further quality measures are described below.
Data are collected on patient and clinical characteristics (including biomarker data), treatment patterns and effectiveness and safety outcomes. To enable adequate follow-up, the registry will operate for a minimum of 5 years and patient enrollment is planned to continue until 6 months prior to the end of data collection. All quality measures are intended to assure the robustness of results of the future non-interventional studies that utilize the data to support decisions by healthcare providers and regulatory agencies.
Eligibility criteria & description of treatments
The MOMENT population includes patients with advanced stage (IIIB–IV) NSCLC and confirmed METex14 skipping, who agree to participate and sign an informed consent form, and who are initiating or are currently treated with at least one systemic therapy (i.e., both newly diagnosed patients and those already receiving therapy are potentially eligible) (Figure 1). Patients currently enrolled in a clinical trial are not eligible. However, patients with prior clinical trial participation can be included if they are currently receiving at least one subsequent line of therapy in a routine clinical setting. Patients can also enter any clinical trial, non-interventional study, registry or expanded access program after enrollment into the MOMENT registry; in such cases, treatment will be blinded while the patient receives any investigational drug in that second study.
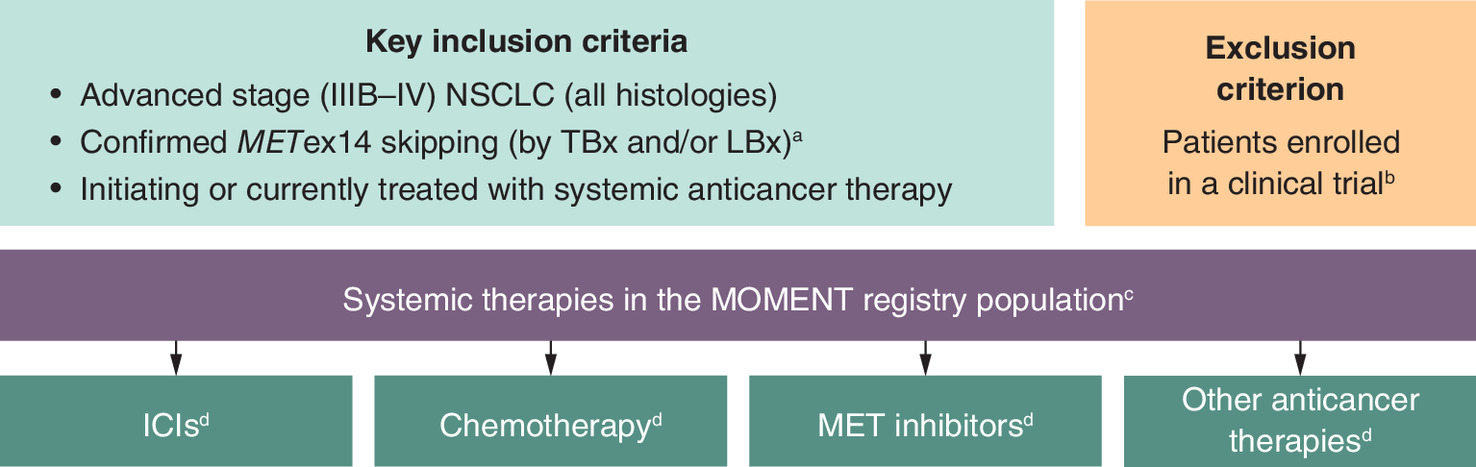
Figure 1. Eligibility criteria.
aPrior to the initiation of a trial site, local METex14 skipping detection methods will be assessed.
bPatients with previous participation in any clinical trial can be included, provided they receive at least one subsequent therapy line in a routine clinical setting. If a patient enters a clinical trial after enrollment into the registry, treatment will be blinded for data entry in the eCRF during the time the patient receives any investigational drug.
cAll available anticancer therapies, including those approved, conditionally approved, or available through early access.
dGiven as monotherapy or in combination with other systemic therapies.
eCRF: Electronic case report form; ICI: Immune checkpoint inhibitor; LBx: Liquid biopsy; MET: Mesenchymal–epithelial transition factor, METex14: MET exon 14; NSCLC: Non-small-cell lung cancer; TBx: Tissue biopsy.
Written informed consent must be obtained from patients before participation in the MOMENT registry; adequate information must be provided to the patient, including a subject information sheet in the local language. All relevant aspects of the registry will also be verbally explained to the patient in easily understandable terms. The informed consent form must be signed and dated by both the patient and the investigator, with the signed form kept at the investigator's site and a copy given to the patient. If new information arises that could impact consent, the subject information sheet and other materials will be revised, reviewed and approved before being sent to patients, with explanations of any changes provided by the investigator. Patients may withdraw consent and discontinue participation at any time.
Eligible systemic treatments for the registry population include all available anticancer therapies that are approved, conditionally approved, or available through early access in routine clinical care. During follow-up across different lines of therapy for advanced disease, systemic anticancer treatment classes expected to be recorded in the registry, either as monotherapy or in combination regimens, include chemotherapy, immune checkpoint inhibitors, targeted therapies (such as MET inhibitors) and other anticancer therapies.
Planned enrollment & registry sites
Approximately 700 patients are expected to be enrolled in the MOMENT registry within 4 years. Enrollment of approximately 200 patients who receive tepotinib is targeted but not required. The first patient was enrolled on 4 October 2022.
Participating sites include oncology and radiotherapy sites, both in academic and community oncology settings, to increase representativeness of the patient sample. The registry is currently operating at more than 60 sites in 14 countries across Europe and North America, including Austria, Belgium, Canada, the Czech Republic, France, Germany, Israel, Italy, the Netherlands, Portugal, Spain, Sweden, the UK and the USA (Figure 2).
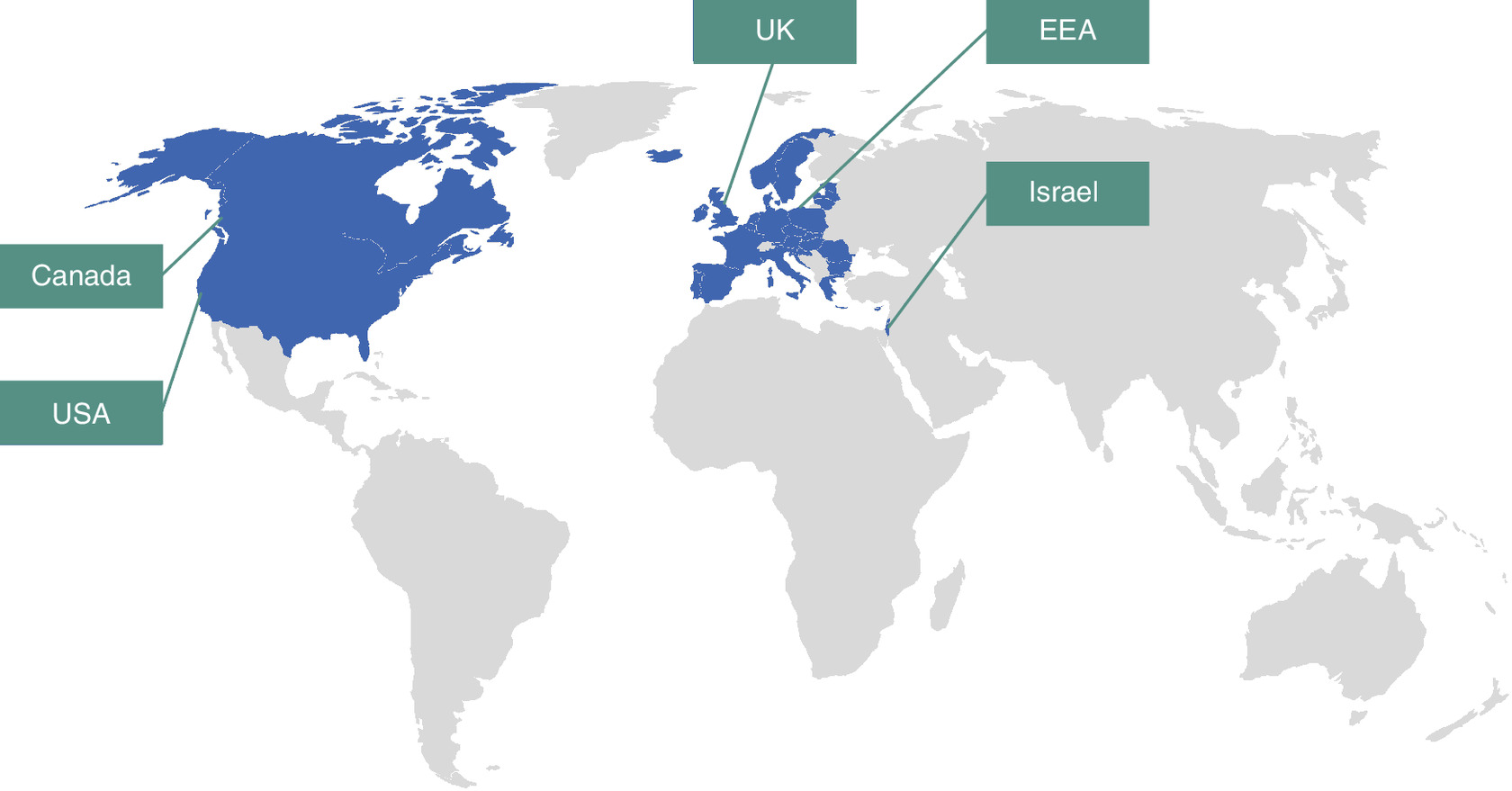
Figure 2. MOMENT registry participating countries.
EEA: European Economic Area.
Data elements & data collection
For enrolled patients, sites are expected to collect data routinely and continuously from enrollment into the registry until death, loss to follow-up (drop-out), withdrawal of consent, or the end of the data collection period. Data elements are standardized and thereby harmonized according to EMA recommendations of international terminologies (e.g., Medical Dictionary for Regulatory Activities [MedDRA], Eastern Cooperative Oncology Group [ECOG] and National Cancer Institute Common Terminology Criteria for Adverse Events [NCI-CTCAE]) (Figure 3).
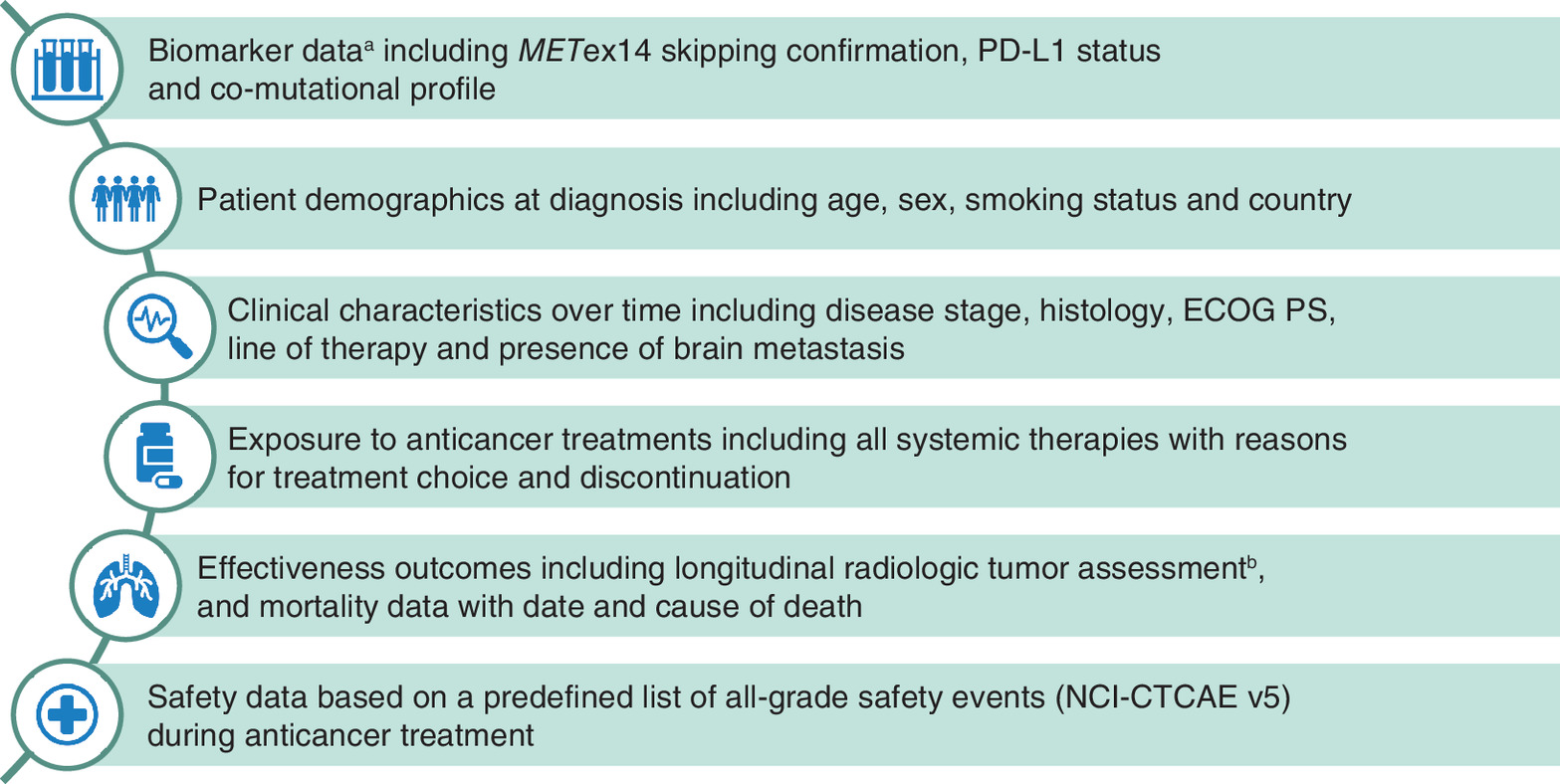
Figure 3. Core data elements of the MOMENT registry.
aBased on tests performed to confirm biomarker status and genomic alterations (laboratory report data including test type, method, results, interpretation).
bIncluding imaging needed to mimic RECIST v1.1 response assessment following clinical practice. Imaging data proposed to be sent to an independent review committee (if feasible) to independently assess tumor response (impact of any differences could be assessed during data analyses) per RECIST v1.1.
ECOG PS: Eastern Cooperative Oncology Group Performance Status; MET: Mesenchymal–epithelial transition factor; METex14: MET exon 14; NCI-CTCAE: National Cancer Institute Common Terminology Criteria for Adverse Event; PD-L1: Programmed death-ligand 1: RECIST: Response Evaluation Criteria in Solid Tumors.
An electronic case report form (eCRF) is used for data collection, which includes biomarker testing assay types and results, demographics, baseline clinical characteristics, treatment details for each line of therapy, treatment effectiveness and safety information (Figure 3, Table 1). Historical data are extracted from the patient's medical record at enrollment. In addition, baseline and follow-up imaging data, including tumor images, are collected continuously from patient enrollment, to enable future studies using MOMENT data to incorporate independent review committee assessments.
| Data collected | Timing of data collection | |
|---|---|---|
| Biomarker data | • METex14 skipping information • Information on ALK mutation, BRAF, CDK6 amplification and mutation, EGFR mutation, KRAS mutation, ROS1 fusions and mutation • PD-L1 information • MET amplification status | At enrollment |
| Demographics | • Age, sex, country, smoking status, weight, height | At enrollment |
| Clinical characteristics | • Medical history – Comorbid conditions – Malignant cancer history, prior treatment, response to prior treatment – Prior trial/current early access participation – Diagnosis of NSCLC details | At enrollment |
| • Medical history – Metastases (distant and brain) – Performance status (ECOG PS, KPS, other) | At enrollment and during follow-up | |
| Treatment exposure | • Treatment regimen details • Reasons for treatment choice/change or discontinuation • Concomitant supportive care • Brain metastases management | From enrollment or start of systemic therapy |
| • Brain metastases management outcome | At enrollment and during follow-up | |
| Effectiveness | • Tumor response per investigator per timepoint for each treatment line (based on RECIST-like criteria†): – Response: complete or partial, stable disease, progressive disease – Not evaluable – Non-complete response/non-progressive disease‡ • Imaging data are collected at baseline, and follow-up for central review and independent assessment of response and progression • Mortality data, including date and cause of death | From enrollment and during follow-up |
| Safety | • Data on adverse reactions for each patient include: – Timing – Severity/seriousness – Management (hospitalization, dose reductions, treatment interruptions/discontinuation) – Outcome | From enrollment (as of consent form signature), and during follow-up |
†
Future studies may incorporate assessment of response according to RECIST v1.1, per IRC if required, based on the imaging data collected.
‡
Used in case of non-measurable disease at baseline assessment of tumor.
AE: Adverse event; ECOG PS: Eastern Cooperative Oncology Group Performance Status; eCRF: Electronic case report form; IRC: Independent review committee; KPS: Karnofsky performance status; METex14: MET exon 14; NSCLC: Non-small-cell lung cancer; PD-L1: Programmed death-ligand 1; RECIST: Response Evaluation Criteria in Solid Tumors.
All data collected will be processed, evaluated and stored in a de-identified form (using unique assigned patient numbers) in accordance with applicable General Data Protection Regulations (GDPR) or other relevant local regulations. Patients will be informed accordingly and will be requested to give their consent on data handling procedures, in accordance with local regulations. In case verification of data is required, original medical records will be archived at the registry site for the longest time permitted by local regulations, or for at least 5 years after the end of registry data collection.
Use of MOMENT data
The primary objective of the MOMENT registry is to provide high-quality data for non-interventional studies, which aim to inform clinical and regulatory decisions. Indeed, examples of potential future applications for data collected in the MOMENT registry include providing more comparable external controls for single-arm intervention studies of patients with METex14 skipping NSCLC, characterization of the natural history of METex14 skipping NSCLC, assessing the safety of treatment options for these patients, as well as possible identification of eligible patients for future clinical trials for this rare disease population [13,17]. Therefore, in addition to the already planned studies by the sponsor, MOMENT data will be made available for external research and research applications after the end of data collection, as guided by the MOMENT charter. Future MOMENT registry-based analyses or non-interventional studies need a pre-defined study protocol and statistical analysis plan approved by a governance committee. To ensure compliance with the Health Insurance Portability and Accountability Act of 1996 (HIPAA) and the GDPR, access to de-identified data will be provided through a secure channel only to qualified persons for a limited timeframe.
Discussion
Data quality goals
The eCRF design and prospective data collection enhance data quality and ensure that registry protocol-specified data are obtained in a complete, accurate, standardized and timely manner. The completeness and quality of the prospective data collection are warranted through extensive registry quality control procedures with continuous monitoring, quality checking, data cleaning and maintenance of a validated database. Quality control procedures are applied at each stage of data handling to ensure reliability and correct processing. Discrepancies, inconsistencies, implausibility, or omissions of key data, as identified during periodic data reviews and automated data checks, are clarified or resolved by queries to the sites. Additionally, based on the Epidemiological and Medical Data Monitoring plan, summary statistics will be computed for key variables to check for outliers and abnormal values or distributions according to registry guidelines [10].
Innovative registry elements
Many secondary RWD sources, including single-country databases, are often associated with various limitations when used to conduct comparative studies [13,18]; the design of the MOMENT study aims to overcome many of these limitations.
Data on mortality can be robustly collected and analyzed if the date and cause of death are available. However, there are inherent challenges in using RWD sources to assess response-based outcomes such as objective response rate and duration of response, which require accurate tumor response and progression assessments. For example, while the Response Evaluation Criteria in Solid Tumors (RECIST v1.1) guidelines are often used to standardize tumor response assessment in interventional clinical trials, these criteria are not necessarily used by physicians in real-world clinical practice [13]. Instead, data in real-world clinical records are often limited to the physician's assessment of tumor response and potentially the supporting scan report. Imaging data are rarely available in RWD sources. MOMENT collects the physicians' tumor response assessments in the eCRF, and retrieves images and imaging data (including site radiology reports, ultrasound reports, etc.), which enables independent assessment of tumor response for registry-based non-interventional studies using MOMENT registry data. The availability of images and imaging data will enable future studies that use MOMENT data to perform a second, independent and blinded assessment of tumor response to all treatment regimens through an independent read committee. Completeness of these data helps provide more accurate evidence to assess the effectiveness of available therapies.
Biomarker testing in real-world, routine clinical practice is often heterogeneous, with the wide variety of commercial or in-house assays leading to differences in standards between sites [19]. Since MOMENT collects data in countries across Europe and North America, some level of heterogeneity is anticipated. However, biomarker data, including assay types and results, are monitored, continuously queried and used to confirm patient eligibility based on METex14 skipping status. Ultimately, this process aims to minimize heterogeneity and enhance data quality.
Conclusion
The availability of high-quality key data, including information on patient characteristics, biomarkers and imaging data from tumor assessments, is critical to enable meaningful analyses of this rare disease. Such data can ensure that patients selected for analyses of treatment outcomes can be adequately compared with clinical trial results to support regulatory and clinical decisions. The prospective design and the innovative elements of MOMENT enable the collection of comprehensive, high-quality RWD from patients with advanced NSCLC harboring METex14 skipping undergoing systemic anticancer treatment in a routine clinical setting, to support future studies informing the optimal care for this rare patient population.
Summary points
•
MET inhibitors like tepotinib, capmatinib and savolitinib target non-small-cell lung cancer (NSCLC) harboring MET exon 14 (METex14) skipping, but have been studied mainly in single-arm trials due to the relative rarity of this alteration, present in approximately 3–4% of patients with NSCLC.
•
High-quality real-world data are therefore crucial for understanding and treating patients with METex14 skipping NSCLC and for complementing clinical trial data.
•
The MOMENT registry aims to collect high-quality, standardized and comprehensive data on patients with METex14 skipping advanced NSCLC.
•
MOMENT includes patients with advanced NSCLC and confirmed METex14 skipping, who are receiving any systemic anticancer therapy and are not currently participating in clinical trials.
•
The registry is currently operating at more than 60 sites in 14 countries and approximately 700 patients are expected to be enrolled within the next 4 years.
•
MOMENT collects robust mortality data, prospective imaging data and monitors heterogeneous biomarker testing to enhance data quality.
•
Data collection is standardized and harmonized according to European Medicines Agency recommendations, with continuous quality control measures.
•
MOMENT aims to improve the understanding and treatment of advanced NSCLC with METex14 skipping by providing comprehensive, high quality real-world data.
Author contributions
The authors confirm contribution to the manuscript as follows: conceptualization: M Thomas, P Christopoulos, WT Iams, F Audhuy, K Berghoff, SP Eggleton, F Fries, M Hildenbrand, P Liu, SH Mahmoudpour, C Menzel, D Oksen; investigation: M Thomas, P Christopoulos, WT Iams, J Mazières, AB Cortot, N Peled, G Minuti, EF Smit; methodology: M Thomas, P Christopoulos, M Hildenbrand, SH Mahmoudpour, C Menzel, D Oksen; supervision: M Thomas, P Christopoulos, WT Iams. All authors reviewed the manuscript and approved the final version.
Acknowledgments
The authors thank patients, all investigators and co-investigators and the teams at all participating centers and at Merck.
Financial disclosure
This trial was sponsored by Merck (Crossref funder ID: 10.13039/100009945). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing support was provided by Ifigeneia Mavragani, PhD, of Syneos Health, UK and funded by Merck (Crossref funder ID: 10.13039/100009945).
Competing interests disclosure
M Thomas: Honoraria/advisory board: Amgen, AstraZeneca, BeiGene, Bristol Myers Squibb, Boehringer Ingelheim, Celgene, Chugai, Daiichi Sankyo, GlaxoSmithKline, Janssen Oncology, Lilly, Merck, MSD, Novartis, Pfizer, Roche, Sanofi, Takeda; research funding (institution): AstraZeneca, Bristol Myers Squibb, Merck, Roche, Takeda; non-financial support (travel costs): AstraZeneca, Bristol Myers Squibb, Boehringer Ingelheim, Daiichi Sankyo, Janssen Oncology, Lilly, Merck, MSD, Novartis, Pfizer, Roche, Sanofi, Takeda. P Christopoulos: Research funding from Amgen, AstraZeneca, Boehringer Ingelheim, Merck, Novartis, Roche, Takeda; advisory board/lecture fees: AstraZeneca, Boehringer Ingelheim, Chugai, Daiichi Sankyo, Gilead, Novartis, Pfizer, Roche, Takeda, Thermo Fisher Scientific. WT Iams: Consulting or advisory role: EMD Serono Research & Development Institute, Inc., Billerica, MA, USA, an affiliate of Merck KGaA, Janssen, Takeda, Bristol Myers Squibb, Mirati, Chardan Consulting, Curio Science, Defined Health, G1 Therapeutics, Genentech, Jazz Pharmaceuticals, Outcomes Insights. J Mazières: Advisory boards: Roche, Bristol Myers Squibb, MSD, AstraZeneca, Pfizer, Novartis, Merck, Amgen, Takeda, Daiichi Sankyo; research funding (institution): Roche/Genentech, AstraZeneca, Bristol Myers Squibb. AB Cortot: Research funding: Novartis, Merck; honoraria: AstraZeneca, Bristol Myers Squibb, Novartis, MSD, Pfizer, Roche, Takeda; consulting or advisory role: AstraZeneca, Bristol Myers Squibb, Novartis, Pfizer, Roche, Takeda; travel expenses: AstraZeneca, MSD, Novartis, Pfizer, Roche, Takeda. N Peled: Advisor, honoraria and research funding: Bristol Myers Squibb, Eli Lilly, Foundation Medicine, Guardant Health, Merck Serono Ltd., Herzliya, Israel, an affiliate of Merck KGaA, MSD, Novartis, NovellusDx, Pfizer, Roche, Takeda. G Minuti: Consulting/advisory role: AstraZeneca, Bristol Myers Squibb, Roche. EF Smit: Advisory/consultancy (institution): Lilly, AstraZeneca, Boehringer Ingelheim, Roche/Genentech, Bristol Myers Squibb, Merck, MSD, Takeda, Bayer, Regeneron, Novartis, Daiichi Sankyo, Seattle Genetics; research funding (institution): Boehringer Ingelheim, Bayer, Roche/Genentech, AstraZeneca, Bristol Myers Squibb. F Audhuy: Employee of Merck Serono S.A.S., Lyon, France, an affiliate of Merck KGaA. K Berghoff, F Fries, M Hildenbrand, SH Mahmoudpour, C Menzel, D Oksen: Employees of Merck. SP Eggleton: Employee of Merck Serono Ltd., Feltham, UK, an affiliate of Merck KGaA. P Liu: Employee of Merck Serono Pharmaceutical R&D Co., Ltd., Beijing, China, an affiliate of Merck KGaA. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Ethical conduct of research
An unconditional prerequisite for a patient's participation in the registry is their written informed consent which must be given before any registry-related activities are carried out. Prior to commencement of the registry at a given site, the protocol will be submitted together with its associated documents (consent form, patient information) to the relevant Independent Ethics Committee (IEC)/Institutional Review Board (IRB) for its opinion/approval. The registry must not start at a site before a written confirmation of favorable opinion/approval from the concerned IEC/IRB has been obtained. The protocol and any applicable documentation (Subject Information and Consent Form) will be submitted or notified to the National Health Authorities in accordance with the regulations of the countries involved in the registry.
Data sharing statement
Any requests for data by qualified scientific and medical researchers for legitimate research purposes will be subject to Merck's (CrossRef Funder ID: 10.13039/100009945) Data Sharing Policy. All requests should be submitted in writing to Merck's data sharing portal (https://www.merckgroup.com/en/research/our-approach-to-research-and-development/healthcare/clinical-trials/commitment-responsible-data-sharing.html). When Merck has a co-research, co-development, or co-marketing or co-promotion agreement, or when the product has been out-licensed, the responsibility for disclosure might be dependent on the agreement between parties. Under these circumstances, Merck will endeavor to gain agreement to share data in response to requests.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest
1.
Awad MM, Oxnard GR, Jackman DM et al. MET exon 14 mutations in non-small-cell lung cancer are associated with advanced age and stage-dependent MET genomic amplification and c-Met overexpression. J. Clin. Oncol. 34(7), 721–730 (2016).
2.
Reungwetwattana T, Liang Y, Zhu V, Ou S-HI. The race to target MET exon 14 skipping alterations in non-small-cell lung cancer: The why, the how, the who, the unknown, and the inevitable. Lung Cancer 103, 27–37 (2017).
• Underscores the emerging significance of MET exon 14 in non-small-cell lung cancer, the efficacy of various MET-targeted TKIs in clinical and preclinical settings and the anticipated challenges of resistance to these therapies.
3.
Hong L, Zhang J, Heymach JV, Le X. Current and future treatment options for MET exon 14 skipping alterations in non-small-cell lung cancer. Ther. Adv. Med. Oncol. 13, 1–16 (2021).
4.
Wolf J, Seto T, Han J-Y et al. Capmatinib in MET exon 14–mutated or MET-amplified non–small-cell lung cancer. N. Engl. J. Med. 383(10), 944–957 (2020).
5.
Lu S, Fang J, Li X et al. Once-daily savolitinib in Chinese patients with pulmonary sarcomatoid carcinomas and other non-small-cell lung cancers harbouring MET exon 14 skipping alterations: A multicentre, single-arm, open-label, Phase II study. Lancet Respir. Med. 9(10), 1154–1164 (2021).
6.
Paik P, Felip E, Veillon R et al. Tepotinib in non-small-cell lung cancer with MET exon 14 skipping mutations. N. Engl. J. Med. 383(10), 931–943 (2020).
7.
Hendriks LE, Kerr KM, Menis J et al. Oncogene-addicted metastatic non-small-cell lung cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 34(4), 339–357 (2023).
8. .
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for non-small-cell Lung Cancer V7.2024. © National Comprehensive Cancer Network, Inc. (2024) (Accessed July 2024).
9.
Hanna NH, Robinson AG, Temin S et al. Therapy for stage IV non–small-cell lung cancer without driver alterations: ASCO and OH (CCO) joint guideline update. J. Clin. Oncol. 39(9), 1040–1091 (2021).
10.
European Medicines Agency. EMA/426390/2021. Guideline on registry-based studies. (2021). https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-registry-based-studies_en-0.pdf
11.
US Food and Drug Administration. Real-World Data: Assessing Registries to Support Regulatory Decision-Making for Drug and Biological Products. Guidance for Industry. (2021). https://www.fda.gov/media/154449/download
12.
Miksad RA, Abernethy AP. Harnessing the power of real-world evidence (RWE): a checklist to ensure regulatory-grade data quality. Clin. Pharmacol. Ther. 103(2), 202–205 (2018).
• Highlights the importance of real-world evidence in bridging the gap between clinical trial results and real-world clinical decisions, particularly in complex cancer care.
13.
Oksen D, Prince P, Boutmy E et al. Treatment effectiveness in a rare oncology indication: lessons from an external control cohort study. Clin. Transl. Sci. 15(8), 1990–1998 (2022).
• Reported lessons learned provide important considerations for the conduct of external control studies in rare oncology indications, and may be applicable to research in other rare conditions.
14.
Blonde L, Khunti K, Harris SB, Meizinger C, Skolnik NS. Interpretation and impact of real-world clinical data for the practicing clinician. Adv. Ther. 35(11), 1763–1774 (2018).
15.
De Lusignan S, Crawford L, Munro N. Creating and using real-world evidence to answer questions about clinical effectiveness. J. Innov. Heal. Informatics. 22(3), 368–378 (2015).
16.
Christopoulos P, Schlenk R, Kazdal D et al. Real-world data for precision cancer medicine—A European perspective. Genes Chromosom. Cancer 62(9), 557–563 (2023).
• Emphasizes the significance of integrating high-quality real-world data to enhance precision oncology research and clinical practice, thereby improving patient outcomes and supporting regulatory decisions.
17.
Pisa F, Arias A, Bratton E, Salas M, Sultana J. Real world data for rare diseases research: the beginner's guide to registries. Expert Opin. Orphan Drugs 11(1), 9–15 (2023).
• Highlights the significance of registries as a source of real-world data, which are crucial for addressing the challenges associated with research on rare diseases.
18.
Rolfo C, Hess LM, Jen M-H et al. External control cohorts for the single-arm LIBRETTO-001 trial of selpercatinib in RET+ non-small-cell lung cancer. ESMO Open 7(4), 100551 (2022).
19.
van de Ven M, Koffijberg H, Retèl V et al. Real-world utilization of biomarker testing for patients with advanced non–small cell lung cancer in a tertiary referral center and referring hospitals. J. Mol. Diagn. 23(4), 484–494 (2021).
• Provides insights into the real-world implementation and patterns of biomarker testing in patients with advanced non-small-cell lung cancer, highlighting gaps and opportunities for optimizing personalized treatment strategies in clinical practice.
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 8 August 2024
Accepted: 17 December 2024
Published online: 21 January 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
MOMENT registry: Patients with advanced non-small-cell lung cancer harboring MET exon 14 skipping treated with systemic therapy. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0127
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Tsai Ling Ting, Shiuan-Chih Chen, Durable Benefit Beyond Response: Reinterpreting Amivantamab Efficacy in METex14 NSCLC Subgroups, Journal of Thoracic Oncology, 10.1016/j.jtho.2025.06.006, 20, 10, (e108-e109), (2025).
- Paul K. Paik, Wade T. Iams, Hatim Husain, Richard M. O’Hara, Emmanuel Adewusi, Xiuning Le, Tepotinib in patients with MET exon 14 skipping non-small cell lung cancer, Cancer Treatment Reviews, 10.1016/j.ctrv.2025.102990, 139, (102990), (2025).