Atezolizumab with chemotherapy in first-line treatment for metastatic urothelial cancer: a cost–effectiveness analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Purpose: To evaluate the cost–effectiveness of atezolizumab plus chemotherapy as first-line treatment for metastatic urothelial cancer (mUC). Materials & methods: A Markov model was established for the analysis. Parametric survival models were used to fit to progression-free survival and overall survival data in the IMvigor130 study. A series of one-way and probabilistic sensitivity analyses were performed to test the robustness of the model. Results: The incremental cost–effectiveness ratios for atezolizumab plus chemotherapy versus chemotherapy alone were US$475,633.17 and $207,488.17 per quality-adjusted life year in the USA and China, respectively. Utility for the progression-free survival and progressive disease states, the cost of atezolizumab had the most significant impact on the incremental cost–effectiveness ratio. Conclusion: Atezolizumab plus chemotherapy is not a cost–effective treatment option as a first-line treatment for metastatic urothelial cancer.
Urothelial cancer (UC), which can arise from upper or lower urinary tracts, results in significant morbidity, mortality and costs worldwide [1–3]. The vast majority of urothelial cancer cases are bladder urothelial carcinoma, whereas upper tract urothelial carcinoma accounts for merely 5–10% of all UCs [4]. Cisplatin-based chemotherapy regimens are the preferred first-line treatment for metastatic UC (mUC); however, approximately 50% of patients with mUC are not fit enough to tolerate cisplatin treatment because of poor performance status and impaired renal function [5–8]. In recent years, carboplatin plus gemcitabine has been applied for cisplatin-ineligible patients and gemcitabine monotherapy has also been regarded as another alternative option for patients ineligible for combination chemotherapy [9,10]. Despite this progress, improvements in the efficacy of currently available chemotherapies are still far from satisfactory. Thus, there is an urgent need for effective treatment regimens for first-line treatment of patients with mUC.
In the past few years, immunotherapy with anti-programmed death receptor 1 (PD-1) or anti-programmed death ligand 1 (PD-L1) inhibitors has shown benefits in patients with mUC ineligible for cisplatin treatment or who have progressed after platinum-based chemotherapy [11–14]. On the basis of these encouraging results, atezolizumab, a humanized monoclonal antibody against PD-L1, was firstly approved by the US FDA for the treatment of patients with locally advanced or metastatic UC failed to first-line platinum-based chemotherapy. The success of atezolizumab for the treatment of mUC that failed to first-line platinum-based chemotherapy encouraged investigators to extend the application of atezolizumab to first-line treatment for patients with mUC. Recently, the results of the IMvigor130 study, which evaluated the efficacy of atezolizumab alone or combined with platinum-based chemotherapy versus placebo plus platinum-based chemotherapy in patients with untreated mUC, were published [15]. Between 15 July 2016 and 20 July 2018, 451 patients were enrolled in the atezolizumab plus chemotherapy group and 400 patients were enrolled in the placebo plus chemotherapy group. The addition of atezolizumab to platinum-based chemotherapy as first-line treatment significantly prolonged median progression-free survival (PFS) in patients with mUC compared with placebo plus platinum-based chemotherapy (8.2 months, 95% CI 6.5–8.3 versus 6.3 months, 95% CI: 6.2–7.0; hazard ratio [HR]: 0.82, 95% CI 0.70–0.96; p = 0·007), indicating that atezolizumab plus platinum-based chemotherapy might be a novel standard treatment option in first-line treatment for mUC.
Although the addition of atezolizumab to platinum-based chemotherapy has achieved a significant survival benefit as first-line treatment for mUC, its high price (1200 mg, US$4956.62 in China and $11,032.84 in the USA) can also increase the cost of mUC treatment. In recent years, growing cancer care expenditures have become one of the greatest concerns for public health policy makers, doctors and patients worldwide [16]. In many countries, cost–effectiveness analyses have become a preferred method to evaluate novel treatment regimens from the pharmacoeconomic profile, which provides an important framework for doctors, payers, patients and policy makers [17]. The USA and China are the largest developed country and the largest developing country in the world, respectively. It is representative to evaluate the cost–effectiveness of novel treatment schemes in the USA and China. The objective of the current study was to investigate the cost–effectiveness of atezolizumab with chemotherapy as first-line therapy for the treatment of mUC from a Chinese and USA payer's perspective.
Methods
Model structure
To evaluate the cost–effectiveness of the addition of atezolizumab to chemotherapy as first-line treatment for patients with mUC, a Markov model including three mutually exclusive health states (PFS, progressive disease [PD] and death) was established to estimate health outcomes and costs. In this model, all patients were assumed to enter the model in the PFS state. When the model began to progress, these patients could remain in the starting health state until disease progression or death. Once in the PD state, patients could remain in that state or transition to death at the end of each cycle. Transition diagram among these health states is shown in Figure 1. Outcomes of the analysis include costs, quality-adjusted life years (QALYs) and incremental cost–effectiveness ratio (ICER). Willingness-to-pay (WTP) thresholds were set at US$28,988.40/QALY (3× per-capita GDP of China in 2018) for China and US$100,000.00/QALY for the USA, respectively [18,19]. Costs and health outcomes were discounted at an annual rate of 3% [19,20]. The lifetime horizon was set at 15 years, after which almost all hypothetical patients were expected to be dead. Model cycle of 3 weeks was used for the base case analysis [21]. The study was performed from a Chinese and US payer's perspective, and the model was developed and implemented with Microsoft Excel (Microsoft Corporation, WA, USA) and TreeAge software (TreeAge, MA, USA, 2011).

Figure 1. Markov model diagram for patients with untreated metastatic urothelial cancer.
PD: Progressive disease; PFS: Progression-free survival.
Patients & treatment regimens
The target population for the model was modeled consistent with the patient population in the IMvigor130 study [15]. These patients had locally advanced or metastatic UC and had not received previous systemic therapy in the metastatic setting. Meanwhile, patients in the model were eligible for platinum-based chemotherapy. Key baseline characteristics of the patients in the IMvigor130 study were presented in Table 1. Patients in the atezolizumab plus chemotherapy group received gemcitabine (1000 mg/m2 body surface area [BSA; 21-day cycles, days 1 and 8 of each cycle]), plus either carboplatin (area under the curve of 4.5 mg/ml per min) or cisplatin (70 mg/m2 BSA) on day 1 of each cycle. Atezolizumab was administered intravenously at a dose of 1200 mg on day 1 of each cycle. Patients in the comparator group (chemotherapy alone) received the same chemotherapy regimens as those in the atezolizumab plus chemotherapy group.
| Parameters | Atezolizumab + chemotherapy | Chemotherapy | Ref. |
|---|---|---|---|
| Baseline characteristics | |||
| Age group, years | |||
| <65 | 34% | 38% | [15] |
| ≥65 | 66% | 62% | [15] |
| Sex | |||
| Male | 75% | 75% | [15] |
| Female | 25% | 26% | [15] |
| Race | |||
| White | 77% | 76% | [15] |
| Other | 23% | 24% | [15] |
| Primary tumor site | |||
| Bladder | 69% | 73% | [15] |
| Other | 31% | 67% | [15] |
| PD-L1 status | |||
| IC2/3 | 24% | 23% | [15] |
| IC1 | 43% | 45% | [15] |
| IC0 | 33% | 33% | [15] |
| Survival data | |||
| HR for OS | 0.83 (95% CI: 0.69–1.00) | – | [15] |
| HR for PFS | 0.82 (95% CI: 0.70–0.96) | – | [15] |
| Median OS (months) | 16.0 (95% CI: 13.9–18.9) | 13.4 (95% CI: 12.0–15.2) | [15] |
| Median PFS (months) | 8.2 (95% CI: 6.5–8.3) | 6.3 (95% CI: 6.2–7.0) | [15] |
| Grade 3–4 AEs, rate (range) | |||
| Anemia | 0.40 (0.32–0.48) | 0.38 (0.304–0.456) | [15] |
| Neutropenia | 0.37 (0.296–0.444) | 0.30 (0.24–0.36) | [15] |
| Neutrophil count decreased | 0.21 (0.168–0.252) | 0.24 (0.192–0.288) | [15] |
| Platelet count decreased | 0.21 (0.168–0.252) | 0.25 (0.20–0.30) | [15] |
| Thrombocytopenia | 0.21 (0.168–0.252) | 0.18 (0.144–0.216) | [15] |
| Utility | |||
| PFS | 0.842 (0.6736–1) | 0.842 (0.6736–1) | [21] |
| PD | 0.800 (0.640–0.96) | 0.800 (0.640–0.96) | [21] |
AEs: Adverse events; HR: Hazard ratio; OS: Overall survival; PD: Progressive disease; PD-L1: Programmed death-ligand 1; PFS: Progression-free survival.
Efficacy & safety
In this analysis, parametric survival models were used to fit to PFS and OS Kaplan–Meier data in the IMvigor130 study (Table 1). Survival data in each group were extracted from the Kaplan–Meier survival curves using a plot digitizer software (DigitizeIt, version 2.0, www.digitizeit.de) because individual patient data were not available. The probability for transition from PFS to a PD state was derived from the modeled PFS curves, and the probability for transition from any state to the death state was derived from the modeled OS curves (Figure 2). Grade 3–4 treatment-related adverse events (AEs) with an incidence of ≥5% were derived from the IMvigor130 study (Table 1). Meanwhile, a specific quality-of-life adjustment weight (utility scores, where 1 is full health and 0 is death) was assigned for each health state. Health utilities for health states were derived from previous literature [21]. The utility scores were 0.842 for the PFS state and 0.800 for the PD state (Table 1).
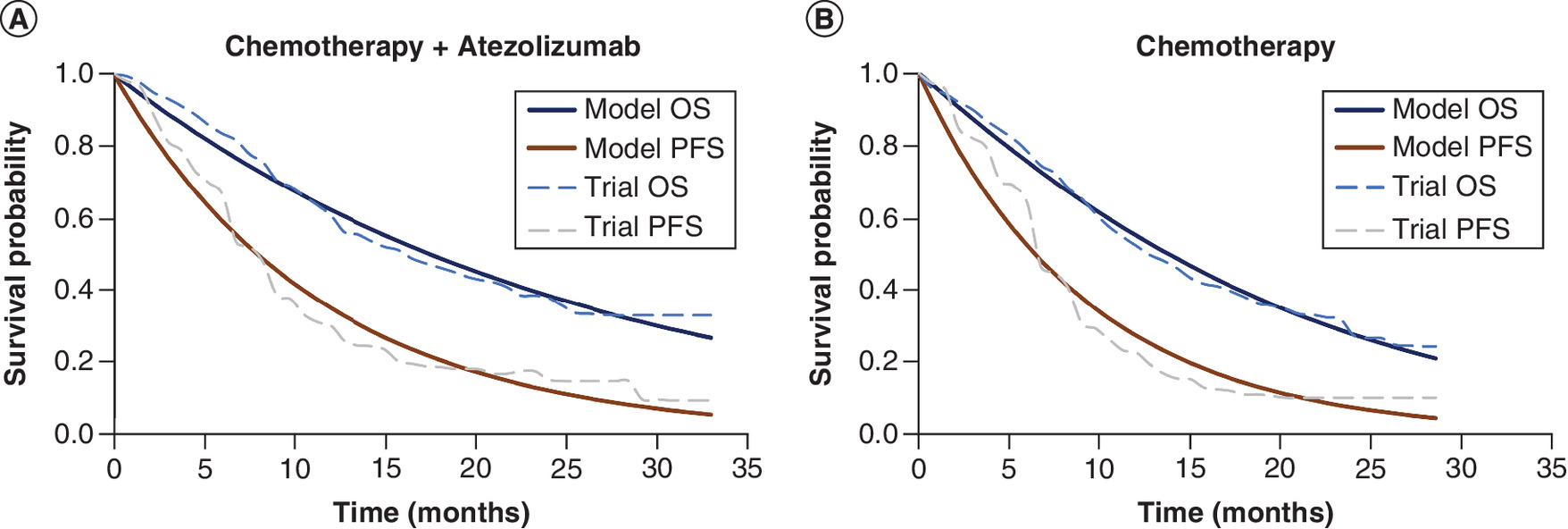
Figure 2. Modeled survival curves for each treatment groups.
(A) Atezolizumab plus chemotherapy group. (B) Chemotherapy alone group.
OS: Overall survival; PFS: Progression-free survival.
Cost input
In the current analysis, only direct medical costs, which included costs of drug, tests, AE-related treatments, best-supportive care (BSC) and follow-up, were considered. The unit prices of drugs in China were retrieved from the national drug prices or our hospital and the unit prices for the drugs were based on the wholesale acquisition costs from the AnalySource database RED BOOK Online (Table 2). The unit cost of tests, drug administration, follow-up, tests, AE-related treatments and BSC were retrieved from the CMS clinical laboratory fee schedule files and previously published literature (Table 2) [22–28]. To calculate doses of drugs, we used a mean BSA of 2.1 or 1.72 m2 for patients in the USA and China, respectively [26,29]. All costs were converted to US dollars (1 US dollar = 6.6118 CNY, 2018).
| Parameters | Value (US$) | Range | Resource | Ref. |
|---|---|---|---|---|
| Gemcitabine (200 mg) | 36.65 (China) | 26.92–40.38 | Local estimate | |
| 25.91 (USA) | 20.728–31.092 | RED BOOK | ||
| Carboplatin (50 mg) | 4.59 (China) | 3.672–5.508 | Local estimate | |
| 44.4 (USA) | 35.52–53.28 | RED BOOK | ||
| Cisplatin (30 mg) | 2.89 (China) | 2.312–3.468 | Local estimate | |
| 31.2 (USA) | 24.96–37.44 | RED BOOK | ||
| Atezolizumab (1200 mg) | 4956.62 (China) | 3965.296–5947.944 | Local estimate | |
| 11032.84 (USA) | 8826.272–13239.408 | RED BOOK | ||
| Laboratory tests | 30.68 (China) | 24.544–36.816 | Local estimate | |
| 76 (USA) | 60.8–91.2 | [28] | ||
| Computed tomography | 211.56 (China) | 169.248–253.872 | Local estimate | |
| 828 (USA) | 662.4–993.6 | [28] | ||
| Anemia | 508.2 (China) | 406.56–609.84 | [22] | |
| 4368 (USA) | 3494.4–5241.6 | [27] | ||
| Neutropenia | 466 (China) | 372.8–559.2 | [23] | |
| 5937 (USA) | 4749.6–7124.4 | [26] | ||
| Neutrophil count decreased | 466 (China) | 372.8–559.2 | [23] | |
| 5937 (USA) | 4749.6–7124.4 | [26] | ||
| Platelet count decreased | 3395 (China) | 2716–4074 | [22] | |
| 4014 (USA) | 3211.2–4816.8 | [27] | ||
| Thrombocytopenia | 3395 (China) | 2716–4074 | [22] | |
| 4014 (USA) | 3211.2–4816.8 | [27] | ||
| Cost of supportive care per cycle | 117.1 (China) | 93.68–140.52 | [23] | |
| 1213 (USA) | 970.4–1455.6 | [27] | ||
| Routine follow-up of patients per unit | 51.5 (China) | 41.2–61.8 | [25] | |
| 422 (USA) | 337.6–506.4 | [27] |
Sensitivity analysis
A series of one-way sensitivity analyses are performed to test the robustness of the model by varying each parameter to its lower and upper bounds. All parameters were assumed to range between ±20%, and the results of the one-way sensitivity analyses are shown as tornado diagrams. In addition, probabilistic sensitivity analyses were also performed with each key parameter randomly varied within its distribution range simultaneously for 1000 iterations.
Results
Base case results
The results of the cost–effectiveness analysis are shown in Table 3. Over a 15-year lifetime horizon, patients in the atezolizumab plus chemotherapy group achieved longer survival than those in the chemotherapy alone group (1.43 vs 1.07 QALYs) after adjusting for quality of life. From the US payer's perspective, the costs of atezolizumab plus chemotherapy and chemotherapy alone were US$221,092.77 and $49,864.83, respectively. From China payer's perspective, the costs of the atezolizumab plus chemotherapy and chemotherapy alone groups were US$89,513.33 and $14,817.59, respectively. The ICERs of atezolizumab plus chemotherapy versus chemotherapy alone were US$475,633.17 and $207,488.17 per QALY in the USA and China, respectively.
| Model outcomes | Atezolizumab + chemotherapy | Chemotherapy |
|---|---|---|
| USA | ||
| Total costs (US$) | 221,092.77 | 49,864.83 |
| Incremental costs | 171,227.94 | – |
| Total effectiveness (QALYs) | 1.43 | 1.07 |
| Incremental effectiveness (QALYs) | 0.36 | – |
| ICER ($/QALY) | 475,633.17 | |
| China | ||
| Total costs (US$) | 89,513.33 | 14,817.59 |
| Incremental costs | 74,695.74 | – |
| Total effectiveness (QALYs) | 1.43 | 1.07 |
| Incremental effectiveness (QALYs) | 0.36 | – |
| ICER (US$/QALY) | 207,488.17 | – |
ICER: Incremental cost–effectiveness ratio; QALY: Quality-adjusted life year.
Sensitivity analysis
On the basis of the results of the one-way sensitivity analysis, utility for the PFS and PD states, the cost of atezolizumab had the most significant impacts on the ICERs in both the USA and China (Figure 3). The cost of chemotherapy drugs, cost of AE-related treatment, cost of tests, cost of supportive care and cost of follow-up had little impact on the results of the model. In the probabilistic sensitivity analyses, the proportions of atezolizumab plus chemotherapy being cost–effective compared with chemotherapy alone at the WTP thresholds of US$100,000.00/QALY in the USA and US$28,988.40/QALY in China were 0%.
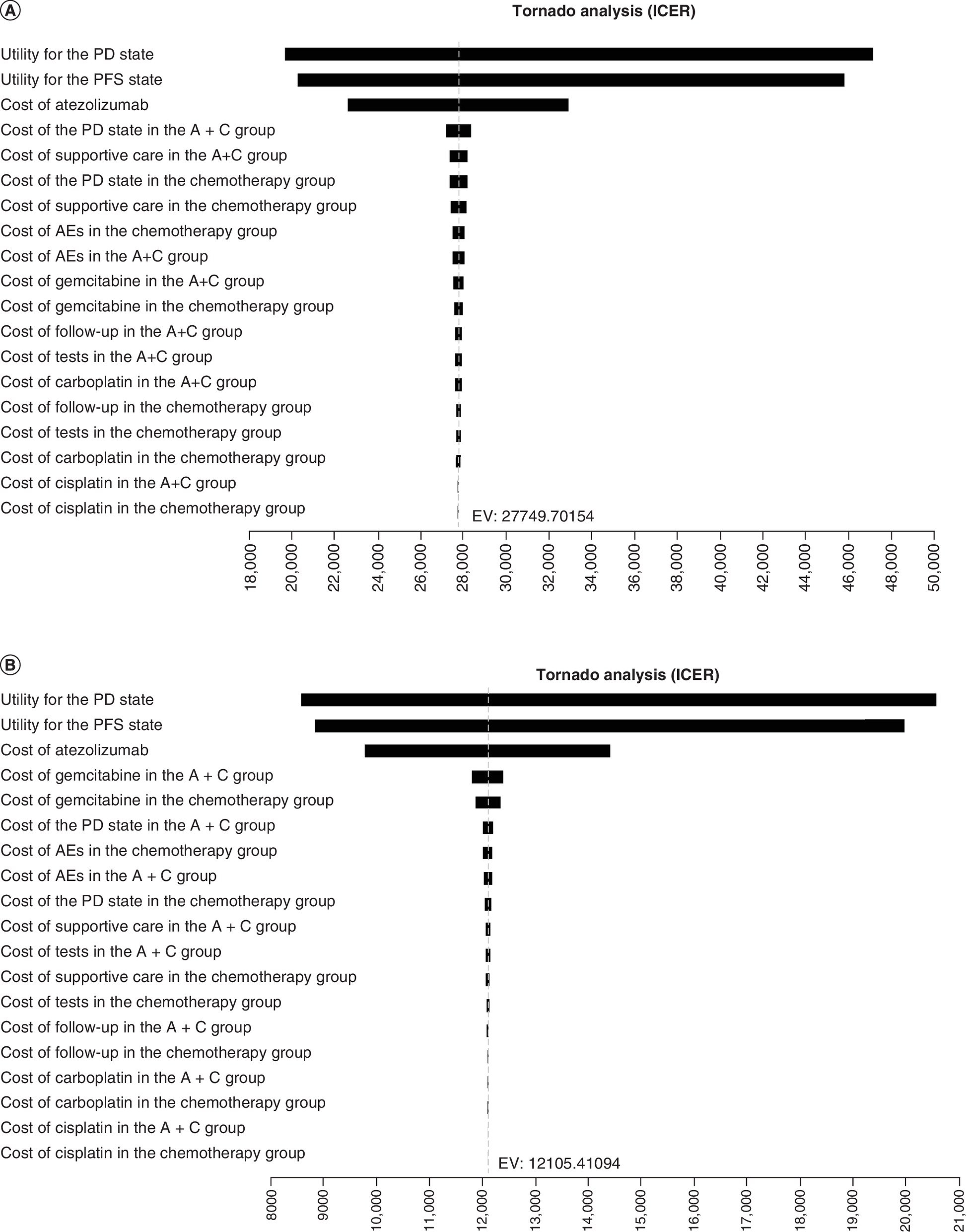
Figure 3. Tornado diagram for one-way sensitivity analyses.
(A) The US payer's perspective. (B) The Chinese payer's perspective.
A+C: Atezolizumab plus chemotherapy; AE: Adverse event; EV: Expected value; ICER: Incremental cost–effectiveness ratio; PD: Progressive disease; PFS: Progression-free survival.
Discussion
UC is one of the most commonly diagnosed cancers worldwide. Despite the availability of platinum-based chemotherapy, the efficacy of current treatment regimens is still limited and most patients will experience disease progression within the short term. Recently, the addition of atezolizumab to platinum-based chemotherapy was demonstrated to achieve a significant survival benefit as a first-line treatment for mUC in the IMvigor130 study; however, treatment with atezolizumab may also pose significant clinical and economic burdens on healthcare systems. In this study, we performed a cost–effectiveness analysis to compare atezolizumab plus chemotherapy versus chemotherapy in first-line treatment for mUC from the USA and Chinese payer perspectives. Our model-based analysis showed that the addition of atezolizumab to chemotherapy achieved 0.36 QALYs compared with chemotherapy; however, the addition of atezolizumab significantly increased the expenditures both in the USA and China, thus resulting in an ICER of atezolizumab plus chemotherapy versus chemotherapy of US$475,633.17 and $207,488.17 per QALY in the USA and China, respectively. At the WTP thresholds of US$100,000.00 and $28,988.40 per QALY in the USA and China, respectively, the addition of atezolizumab to chemotherapy is not a cost-effective treatment option in first-line treatment for mUC from the pharmacoeconomic perspective.
This is the first study to evaluate the pharmacoeconomic profile of atezolizumab plus chemotherapy in the first-line treatment of mUC. In addition to atezolizumab, a series of other immune checkpoint inhibitors, including pembrolizumab and nivolumab, were also approved for the treatment of advanced UC [11–14]. The cost–effectiveness of these novel drugs was also investigated in previous studies. Patterson et al. assessed the cost–effectiveness of pembrolizumab for first-line treatment of urothelial carcinoma ineligible for cisplatin-based therapy in patients with strongly PD-L1-positive tumors in Sweden. Pembrolizumab improved the effectiveness by 1.71 and 1.75 QALYs compared with carboplatin plus gemcitabine and gemcitabine monotherapy, respectively. On the other hand, pembrolizumab increased the cost by US$90,520.00 versus carboplatin plus gemcitabine and US$95,055.00 versus gemcitabine, yielding ICERs of US$53,055.00 and $54,415.00 per QALY, respectively [21]. Ren et al. performed a cost–effectiveness study to evaluate pembrolizumab for locally advanced or mUC where cisplatin is unsuitable. The results of the cost–effectiveness analysis performed by the manufacturer (Merck Sharp & Dohme) showed that the ICER for pembrolizumab compared with carboplatin plus gemcitabine was estimated to be £37,081.00 per QALY, indicating pembrolizumab as a cost-effective treatment option for NICE's criteria for locally advanced or metastatic urothelial carcinoma ineligible for cisplatin-based therapy. However, the independent Evidence Review Group (ERG) performed the cost–effectiveness analysis by defining a new base case that included multiple adjustments to the original base case based on identified errors, violations and alternative judgments. Ultimately, the base-case ICER of ERG was £67,068.00 per QALY, suggesting that the ICER was highly uncertain [30]. The ICERs in these studies were much lower than those in our study. There could be several reasons for this. First, patients in these studies were diagnosed with UCs with strongly PD-L1-positive. These patients could achieve more favorable benefits from the treatment of immune checkpoint inhibitor (ICIs). Second, patients included in these studies with the following criteria were ineligible for cisplatin-based therapy: Eastern Cooperative Oncology Group performance status 2, creatinine clearance 30–60 ml/min, grade ≥2 audiometric hearing loss, grade ≥2 peripheral neuropathy or New York Heart Association Class III heart failure. These patients may benefit less from the treatment of chemotherapy. Third, these studies were conducted based on single-arm trials, and there were no head-to-head trials comparing pembrolizumab with other treatments. Studies directly comparing pembrolizumab with other treatments would help address some of the uncertainties in the future.
In recent years, immune checkpoint inhibitors, such as nivolumab and pembrolizumab, have significantly improved survival and quality of life for patients in a series of malignancies. However, not all patients can benefit from this novel treatment. In the one-way sensitivity analyses of our analysis, the most influential parameters in the model were utility for the PFS state and the PD state and it is essential to find the most suitable patients with best survival benefits for the immune checkpoint inhibitors. In recent years, several biomarkers, including PD-L1 expression and tumor mutation burden, have been demonstrated to predict the response to ICIs [31–33]. In the subgroup analysis of the IMvigor130 study, age ≥65 years, male, White race, Eastern Cooperative Oncology Group performance status score = 0, PD-L1 status of 2 or 3 and no previous adjuvant or neoadjuvant regimen were considered biomarkers favoring the treatment of atezolizumab plus chemotherapy. The pharmacoeconomic profile of atezolizumab plus chemotherapy in these patients may be more cost-effective. In addition, the high cost of atezolizumab was another parameter that significantly influenced the model, which suggested that the production of drugs with lower prices and higher efficacy is also urgently needed. With the development of the drug industry, ICIs with favorable efficacy but lower prices are emerging, which could significantly decrease the ICER of atezolizumab plus chemotherapy versus chemotherapy in the first-line treatment of patients with mUC.
Several limitations of the analysis should be addressed. First, the model included grade 3–4 AEs, and the cost of grade 1–2 AEs was excluded. Fortunately, AE-related treatment was not considered a significant influencing parameter in the one-way sensitivity analyses. Second, the study merely investigated the cost–effectiveness of atezolizumab plus chemotherapy versus chemotherapy for mUC; however, a series of other immune checkpoint inhibitors were also approved for the treatment of advanced UC. However, these ICIs were approved for patients with mUC ineligible for cisplatin-based therapy and there are no head-to-head trials comparing atezolizumab with these treatments; thus, we did not evaluate the cost–effectiveness among these treatment regimens. Finally, the results and conclusions were conducted based on data from USA and China and they should be interpreted with caution for other countries.
Conclusion
On the basis of the data derived from the IMvigor130 study and the current price of atezolizumab, the addition of atezolizumab to chemotherapy is unlikely to be a cost-effective treatment option at the WTP threshold of US$100,000.00 and $28,988.40 per QALY in the USA and China, respectively. To the best of our knowledge, this is the first analysis evaluating the cost–effectiveness of atezolizumab plus chemotherapy versus chemotherapy in first-line mUC setting, which may contribute to the value assessment for these novel drugs and help in the decision-making of doctors, patients and healthcare financial structures.
Future perspective
In the past few years, immunotherapy with anti-programmed death receptor 1 or anti-programmed death ligand 1 inhibitors has shown benefits in patients with mUC. However, high-priced immunotherapy also increases the cost of mUC treatment and brings new issues to society. Currently, the growing financial burden of healthcare has become one of the greatest concerns for public health policy makers, doctors and patients worldwide. Thus, it has become increasingly important to evaluate a novel treatment regimen from efficacy and the pharmacoeconomic profile. Thus, an increasing number of cost–effectiveness analyses evaluating novel treatment regimens from the pharmacoeconomic profile may become one of the standard methods for novel treatment regimen evaluation and provide an important framework for doctors, payers, patients and policy makers.
•
The IMvigor130 study demonstrated that the addition of atezolizumab to platinum-based chemotherapy can significantly prolong median progression-free survival in patients with metastatic urothelial cancer (mUC), indicating that atezolizumab plus platinum-based chemotherapy might be a novel standard treatment option in first-line treatment for mUC.
•
However, the high cost of atezolizumab may significantly increase the cost of treatment for mUC.
•
In this study, we evaluated the cost–effectiveness of atezolizumab with chemotherapy as a first-line treatment for patients with mUC from the perspective of Chinese and USA societies.
•
Over a lifetime horizon, incremental cost–effectiveness ratios for atezolizumab plus chemotherapy versus chemotherapy alone were US$475,633.17 and $207,488.17 per quality-adjusted life-year in the USA and China, respectively.
•
Utility for the progression-free survival and progressive disease states, the cost of atezolizumab had the most significant impact on the incremental cost–effectiveness ratios.
•
On the basis of the data derived from the IMvigor130 study and the current price of atezolizumab, the addition of atezolizumab to chemotherapy is unlikely to be a cost-effective treatment option at the willingness to pay threshold of US$100,000.00 and $28,988.40 per quality-adjusted life-year in the USA and China, respectively.
Author contributions
PF Zhang and Q Li designed the study; PF Zhang, F Wen, QJ Wu and L Zhang collected and analyzed the data; PF Zhang and F Wen drafted the manuscript. All authors reviewed the manuscript draft and approved the final manuscript.
Financial & competing interests disclosure
This work was funded by the National Natural and Scientific Foundation of China (No. 81572988) and Science & Technology Department of Sichuan Province Funding Project (2018SZ0117). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Data sharing statement
The data generated in the current study are available from the corresponding author on reasonable request.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Wong MCS, Fung FDH, Leung C et al. The global epidemiology of bladder cancer: a joinpoint regression analysis of its incidence and mortality trends and projection. Sci. Rep. 8(1), 1129 (2018).
• Current epidemiology of bladder cancer.
2.
Kamat AM, Hahn NM, Efstathiou JA et al. Bladder cancer. Lancet 388(10061), 2796–2810 (2016).
3.
Sullivan R, Peppercorn J, Sikora K et al. Delivering affordable cancer care in high-income countries. Lancet Oncol. 12(10), 933–980 (2011).
4.
Ferlay J, Soerjomataram I, Dikshit R et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 136(5), E359–E386 (2015).
• Current epidemiology of cancers worldwide.
5.
Loehrer PJ, Einhorn LH, Elson PJ et al. A randomized comparison of cisplatin alone or in combination with methotrexate, vinblastine, and doxorubicin in patients with metastatic urothelial carcinoma: a cooperative group study. J. Clin. Oncol. 10(7), 1066–1073 (1992).
6.
Von Der Maase H, Sengelov L, Roberts JT et al. Long-term survival results of a randomized trial comparing gemcitabine plus cisplatin, with methotrexate, vinblastine, doxorubicin, plus cisplatin in patients with bladder cancer. J. Clin. Oncol. 23(21), 4602–4608 (2005).
7.
Bamias A, Tzannis K, Harshman LC et al. Impact of contemporary patterns of chemotherapy utilization on survival in patients with advanced cancer of the urinary tract: a Retrospective International Study of Invasive/Advanced Cancer of the Urothelium (RISC). Ann. Oncol. 30(11), 1841 (2019).
8.
Galsky MD, Chen GJ, Oh WK et al. Comparative effectiveness of cisplatin-based and carboplatin-based chemotherapy for treatment of advanced urothelial carcinoma. Ann. Oncol. 23(2), 406–410 (2012).
9.
Carles J, Nogué M. Gemcitabine/Carboplatin in Advanced Urothelial Cancer. Semin Oncol 28, 19–24 (2001).
10.
Park JH, Lee SW, Kim HS et al. Combination of gemcitabine and carboplatin as first line treatment in elderly patients or those unfit for cisplatin-based chemotherapy with advanced transitional cell carcinoma of the urinary tract. Cancer Chemother. Pharmacol. 71(4), 1033–1039 (2013).
11.
Gartrell BA, He T, Sharma J, Sonpavde G. Update of systemic immunotherapy for advanced urothelial carcinoma. Urol. Oncol. 35(12), 678–686 (2017).
• Current update of immunotherapy for advanced urothelial carcinoma.
12.
Balar AV, Galsky MD, Rosenberg JE et al. Atezolizumab as first-line treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: a single-arm, multicentre, phase 2 trial. Lancet 389(10064), 67–76 (2017).
13.
Balar AV, Castellano D, O'Donnell PH et al. First-line pembrolizumab in cisplatin-ineligible patients with locally advanced and unresectable or metastatic urothelial cancer (KEYNOTE-052): a multicentre, single-arm, phase 2 study. Lancet Oncol. 18(11), 1483–1492 (2017).
14.
Powles T, Durán I, Van Der Heijden MS et al. Atezolizumab versus chemotherapy in patients with platinum-treated locally advanced or metastatic urothelial carcinoma (IMvigor211): a multicentre, open-label, phase 3 randomised controlled trial. Lancet 391(10122), 748–757 (2018).
• Full publication of the IMvigor211 study.
15.
Galsky MD, Arija JÁA, Bamias A et al. Atezolizumab with or without chemotherapy in metastatic urothelial cancer (IMvigor130): a multicentre, randomised, placebo-controlled phase 3 trial. Lancet 395(10236), 1547–1557 (2020).
•• Full publication of the IMvigor130 study.
16.
Dieleman JL, Templin T, Sadat N et al. National spending on health by source for 184 countries between 2013 and 2040. Lancet 387(10037), 2521–2535 (2016).
• A key publication that describes the future and potential spending on healthcare worldwide.
17.
Kadom N, Itri JN, Trofimova A et al. Cost-effectiveness analysis: an overview of key concepts, recommendations, controversies, and pitfalls. Acad. Radiol. 26(4), 534–541 (2019).
• The guideline on how to establish a cost–effectiveness analysis.
18.
Murray CJL, Evans DB, Acharya A, Baltussen RMPM. Development of WHO guidelines on generalized cost-effectiveness analysis. Health Econ 9(3), 235–251 (2000).
•• This is the guideline on how to establish a cost–effectiveness analysis.
19.
Criss SD, Mooradian MJ, Watson TR et al. Cost-effectiveness of atezolizumab combination therapy for first-line treatment of metastatic nonsquamous non-small cell lung cancer in the United States. JAMA Netw. Open 2(9), e1911952–e1911952 (2019).
20.
Nguyen C, Lairson DR, Swartz MD, Du XL. Cost-effectiveness of adding androgen deprivation therapy to radiation therapy for men with advanced prostate cancer from a U.S. payer's perspective. J. Manag. Care Spec. Pharm. 25(2), 225–234 (2019).
21.
Patterson K, Prabhu V, Xu R et al. Cost-effectiveness of pembrolizumab for patients with advanced, unresectable, or metastatic urothelial cancer ineligible for cisplatin-based therapy. Eur. Urol. Oncol. 2(5), 565–571 (2019).
22.
Chongqing T, Liubao P, Xiaohui Z et al. Cost–utility analysis of the newly recommended adjuvant chemotherapy for resectable gastric cancer patients in the 2011 Chinese National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology: Gastric Cancer. Pharmacoeconomics 32(3), 235–243 (2014).
23.
Bai Y, Xu Y, Wu B. Cost-effectiveness and budget impact analysis of apatinib for advanced metastatic gastric cancer from the perspective of health insurance system. Gastroenterol. Res. Pract. 2017, 2816737 (2017).
24.
Shi G, Park SH, Ren H et al. Cost analysis for different sequential treatment regimens for metastatic renal cell carcinoma in China. J. Med. Econ. 21(12), 1150–1158 (2018).
25.
Wu B, Ye M, Chen H, Shen JF. Costs of trastuzumab in combination with chemotherapy for HER2-positive advanced gastric or gastroesophageal junction cancer: an economic evaluation in the Chinese context. Clin. Ther. 34(2), 468–479 (2012).
26.
Ramamurthy C, Handorf EA, Correa AF et al. Cost-effectiveness of abiraterone versus docetaxel in the treatment of metastatic hormone naïve prostate cancer. Urol. Oncol. 37(10), 688–695 (2019).
27.
Wu B, Zhang Q, Sun J. Cost-effectiveness of nivolumab plus ipilimumab as first-line therapy in advanced renal-cell carcinoma. J. Immunother. Cancer 6(1), 124 (2018).
28.
Chen Q, Ayer T, Nastoupil LJ et al. Comparing the cost-effectiveness of rituximab maintenance and radioimmunotherapy consolidation versus observation following first-line therapy in patients with follicular lymphoma. Value Health 18(2), 189–197 (2015).
29.
Wu B, Li T, Cai J et al. Cost-effectiveness analysis of adjuvant chemotherapies in patients presenting with gastric cancer after D2 gastrectomy. BMC Cancer 14, 984–984 (2014).
30.
Ren S, Squires H, Hock E et al. Pembrolizumab for locally advanced or metastatic urothelial cancer where cisplatin is unsuitable: an evidence review group perspective of a NICE single technology appraisal. Pharmacoeconomics 37(9), 1073–1080 (2019).
31.
Gibney GT, Weiner LM, Atkins MB. Predictive biomarkers for checkpoint inhibitor-based immunotherapy. Lancet Oncol. 17(12), e542–e551 (2016).
32.
Bai R, Lv Z, Xu D, Cui J. Predictive biomarkers for cancer immunotherapy with immune checkpoint inhibitors. Biomarker Res. 8, 34 (2020).
33.
Strickler JH, Hanks BA, Khasraw M. Tumor mutational burden as a predictor of immunotherapy response: is more always better? Clin. Cancer Res. 27(5), 1236–1241 (2021).
Information & Authors
Information
Published In
Pages: 1021 - 1030
PubMed: 35924662
Copyright
© 2022 Future Medicine Ltd.
History
Received: 28 March 2022
Accepted: 15 July 2022
Published online: 4 August 2022
Keywords:
Topics
Authors
Funding Information
National Natural and Scientific Foundation of China: 81572988
Science & Technology Department of Sichuan Province Funding Project: 2018SZ0117
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Atezolizumab with chemotherapy in first-line treatment for metastatic urothelial cancer: a cost–effectiveness analysis. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0064
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Hao Cheng, Jun Li, Ningying Mao, Cost-effectiveness analysis of Enfortumab vedotin and pembrolizumab for advanced urothelial carcinoma, Medicine, 10.1097/MD.0000000000048312, 105, 15, (e48312), (2026).
- Heng Xiang, Zhihua She, Liting Wang, Ye Peng, Lei Zhang, Chongqing Tan, Comparison of Atezolizumab plus Aevacizumab and Atezolizumab plus Aabozantinib for advanced hepatocellular carcinoma: A cost-effectiveness analysis, PLOS One, 10.1371/journal.pone.0337606, 20, 12, (e0337606), (2025).
- Mingye Zhao, Taihang Shao, Yue Yin, Hongshu Fang, Hanqiao Shao, Wenxi Tang, Adverse Event Costs and Cost-Effectiveness Analyses of Anticancer Drugs, JAMA Network Open, 10.1001/jamanetworkopen.2025.12455, 8, 5, (e2512455), (2025).
- ZhiYao HE, Min LUO, Li YANG, HongXin DENG, YuQuan WEI, Advances in tumor immunotherapy and gene therapy, SCIENTIA SINICA Vitae, 10.1360/SSV-2022-0160, (2022).