Comparative effectiveness of larotrectinib versus entrectinib for the treatment of metastatic NTRK gene fusion cancers
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To extrapolate clinical trial results to estimate and compare expected progression-free and overall life years (LYs) and quality-adjusted LYs (QALYs) for larotrectinib and entrectinib in patients with colorectal cancer (CRC), soft tissue sarcoma (STS) and brain metastases prior to treatment with larotrectinib or entrectinib. Methods: A naive direct comparison of larotrectinib versus entrectinib was made using partitioned survival modeling methods from clinical trial data. Results: Larotrectinib resulted in an additional 1.58 LYs (1.17 QALYs), 5.81 LYs (2.02 QALYs) and 1.01 LYs in CRC, STS and baseline brain metastases, respectively, compared with entrectinib. Conclusion: Larotrectinib provided life expectancy and QALY gains compared with entrectinib. Additional studies will be beneficial as more patients are treated and survival data develop to better inform comparative effectiveness results.
To effectively treat metastatic cancers, systemic drugs are needed to reach every organ via the bloodstream [1]. This comes at a cost, as these drugs indiscriminately target both cancer and healthy cells, particularly those in the bone marrow and gastrointestinal tract. With continuous innovations in cancer treatment and a better understanding of signaling networks that control specific cellular activities (e.g., proliferation), treatments have been developed aimed at specific targets, such as growth factors. These specific targets are overexpressed in certain types of cancers. For example, HER2 is overexpressed in certain breast and stomach cancers and, therefore, targeted therapeutics were developed to attack these specific proteins [2].
The clinical development programs for these targeted therapeutics focused on specific tumor types based on the tissue of origin. This paradigm has now been challenged by tumor-agnostic agents and, specifically, a class of targeted agents that are histology agnostic, which target NTRK gene fusion-positive tumors across several tumor types. While NTRK gene fusions have a high prevalence in certain rare cancers such as secretory breast carcinoma (>90%), these genetic alterations are rare in common cancers such as lung, sarcoma and colorectal cancer (CRC; <1%) [3]. As a result, to accrue enough patients in clinical trial designs to adequately assess efficacy, basket designs where patients across several tumor sites were enrolled were implemented [4].
The first drug that targeted NTRK gene fusion-positive tumors and received approval by the FDA was larotrectinib in 2018, which had an overall response rate (ORR) of 75% (95% CI: 61–85%, independent review) in a pooled analysis of three phase I and II single-arm trials of 55 combined pediatric and adult patients [5]. An updated pooled analysis from these three phase I and II clinical trials of larotrectinib (NCT02122913, NCT02637687 and NCT02576431) resulted in an ORR of 75% (95% CI: 68–81%) based on an investigator review of 206 patients evaluable for response [6]. In 2019, entrectinib was also approved and a pooled analysis of three phase I and II studies showed an ORR of 57% (95% CI: 43–71%, independent review) in 54 adult patients [7]. Additional clinical studies demonstrated intracranial activity for both larotrectinib and entrectinib as NTRK gene fusions were detected in primary brain tumors and in cancers with a high risk for brain metastasis [8–11]. Having more viable treatment options for patients with brain metastasis is necessary as the prognosis for these patients is poor and represents a substantial mortality burden in advanced cancer [12,13].
As the obtained ORRs for larotrectinib and entrectinib were averaged across different tumor types, the underlying assumption was that the efficacy or effectiveness was the same regardless of histology. However, there was likely to be treatment effect heterogeneity by tumor type, and therefore patients would receive differential clinical benefits based on histology. While the sample sizes were smaller when looking at subgroups, determining the comparative effectiveness of larotrectinib and entrectinib based on available data is potentially beneficial, as choosing between the two treatment options is a likely scenario that clinicians and patients will face. Treatment guidelines vary in their recommendations on the use of larotrectinib and entrectinib. In non-small cell lung cancer (NSCLC), the National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology (NCCN Guidelines®) explicitly recommend trying either larotrectinib or entrectinib for NTRK 1/2/3 gene fusion-positive metastatic NSCLC, although both of these targeted therapy options are recommended [14]. Therefore, if only a single attempt can be made with either treatment, the decision in making the most effective choice would be aided by comparative studies that assess short- and long-term health outcomes [15].
To assess other tumor sites, the objective of the current study was to assess the potential long-term comparative effectiveness of larotrectinib versus entrectinib in CRC, soft tissues sarcoma (STS) and patients with brain metastases prior to starting TRK inhibitor treatment by extrapolating clinical trial data. This permitted the assessment of lifetime progression-free survival (PFS) and overall survival (OS) outcomes and estimate life years (LYs) and quality-adjusted life years (QALYs).
Methods
A naive direct comparison of larotrectinib versus entrectinib was performed using a partitioned survival modeling approach to extrapolate lifetime PFS and OS curves from available clinical trial data [16]. The models consisted of three health states: progression-free, progression and death. The proportion of patients in each state was determined by the extrapolated PFS and OS curves. PFS for both larotrectinib and entrectinib were assessed by an independent review committee (IRC). In the CRC and STS models, PFS and OS curves were extrapolated from subgroup data for larotrectinib and entrectinib using parametric curve fits (exponential, Weibull, log-logistic and log-normal) [17]. For both models, after examining the visual fit, clinical plausibility and Bayesian information criterion, the exponential fit was applied for both PFS and OS in both the CRC and STS models as well as for larotrectinib patients with baseline brain metastases. Given the lack of available PFS and OS curves for patients with baseline brain metastases on entrectinib, an exponential curve was fit through the median point for PFS and OS. This method was also applied to the CRC and STS models for entrectinib as a sensitivity analysis (see Supplementary Material). Patients were entered into the three models based on their median age from the clinical trials (Table 1).
| Larotrectinib (n = 8) [18] | Entrectinib (n = 7) [19] | |
|---|---|---|
| Colorectal cancer | ||
| Age, median (range) | 69 (54–84) | 59.5 (31–75)† |
| Male, n (%) | 3 (37.5) | 6 (50.0)† |
| Median PFS, months (95% CI) | NR | 2.4 (1.0, 16.0) |
| Median OS, months (95% CI) | NR | 16.0 (2.4, NR) |
| ORR | 37.5% | 28.6% |
| Stable disease | 62.5% | 0.0% |
| Larotrectinib (n = 23) [18] | Entrectinib (n = 16) [20] | |
|---|---|---|
| Soft tissue sarcoma | ||
| Age, median (range) | 41 (26–48) | 50.5 (21–81) |
| Male, n (%) | 11 (47.8) | 8 (50.0) |
| Median PFS, months (95% CI) | NR | 10.1 (6.5, 11.2) |
| Median OS, months (95% CI) | NR | 16.8 (10.6, 20.9) |
| ORR | 52.2% | 56.3% |
| Stable disease | 26.1% | 25.0% |
| Larotrectinib (n = 14) [18] | Entrectinib (n = 16) [21] | |
|---|---|---|
| Brain metastasis at baseline | ||
| Median PFS, months (95% CI) | NR | 6.7 (4.7, NR) |
| Median OS, months (95% CI) | NR | 14.3 (7.6, NR) |
| ORR | 85.7% | 50.0% |
| Stable disease | 7.1% | NA |
†
Based on gastrointestinal carcinomas (n = 12) as colorectal cancer-specific characteristics not presented.
NA: Not available; NR: Not reached; ORR: Overall response rate; OS: Overall survival; PFS: Progression-free survival.
US life tables were applied to prevent the possibility of higher age-adjusted survival rates for larotrectinib or entrectinib in the parametric curve tails [22]. The LYs and QALYs obtained from the model were discounted at a 3% rate [18]. One-way sensitivity analysis (OWSA) was performed to determine influential model input parameters. Probabilistic sensitivity analysis (PSA) with 10,000 simulations was run to obtain 95% credible intervals (CrI) around the LY and QALY estimates.
Larotrectinib survival data sources
Inputs for all three models were informed by updated July 2020 data assessed by an IRC for adult patients (≥18 years of age) from the larotrectinib clinical trials program (NCT02122913, NCT02637687 and NCT02576431) [19]. The survival curves for the CRC model were estimated from 8 patients who had received fluoropyrimidine-, oxaliplatin- and irinotecan-containing therapy, as appropriate, with or without anti-VEGF-directed therapy or anti-EGFR directed therapy. The ORR for CRC patients was 37.5%, with 1 patient having a complete response and 2 having a partial response, while 5 patients (62.5%) had stable disease as the best response (Table 1). The STS model survival inputs were derived from 23 patients, excluding those with gastrointestinal stromal tumors, who had received an anthracycline-containing chemotherapy regimen as a single agent or combination, as appropriate. The ORR was 52.2%, with 6 patients (26.1%) having a complete response, 1 (4.3%) with a surgical complete response, 5 (21.7%) with a partial response and 6 (26.1%) with stable disease as the best response. There were 14 patients with brain metastases prior to starting larotrectinib. The ORR in this subgroup was 85.7% with 1 patient (7.1%) having a complete response, 11 patients (78.6%) with partial responses and 1 (7.1%) with stable disease as the best response. The distribution of tumor histology was 7 for NSCLC, 4 for thyroid, 2 for melanoma and 1 for breast [19].
Entrectinib data sources
Model inputs for entrectinib were informed by published literature and scientific conference proceedings. In the CRC model, an updated, integrated analysis of three phase I and II clinical trials had 7 patients with a 28.6% ORR consisting of 2 patients with a partial response and no patients with stable disease as the best response (Table 1) [20]. Model inputs for the STS model were also from an updated integrated analysis of 16 patients with a 56.3% ORR consisting of 9 patients with a partial response and 4 (25.0%) with stable disease as the best response [21]. In the model for patients with baseline brain metastases, 6.7 months was used for median PFS and 14.3 months was used for median OS from a subgroup of 16 patients [23]. The distribution of tumor histology was eight for NSCLC, four for thyroid, two for sarcoma and one for breast. The ORR in this subgroup was 50.0%, with four patients (25.0%) having either a complete or partial response and one patient (6.3%) with stable disease as the best response.
Health state utility values for estimation of QALYs
Health state utility values were obtained from the literature for CRC and STS (Table 2). In the CRC model, the utilities were from a cross-sectional study that assessed 508 Finnish CRC patients using the EQ-5D and the values were 0.82 for progression-free and 0.64 for progressive disease [24]. For the STS model, utilities were used from a study that assessed 207 members of the general public in the UK using the time trade-off method [25]. A utility of 0.43 was used for progression-free and 0.30 for progressive disease. Across both CRC and STS models, on-treatment utilities were calculated as a weighted average of the utility for those in progression-free, with and without responsive disease based on the response rate for each treatment. For the model with patients who had brain metastases prior to TRK inhibitor treatment, given the differences in primary tumor distributions for both larotrectinib and entrectinib, QALYs were not estimated in this model.
| Progression-free/stable disease | Progressive disease | Ref. | |
|---|---|---|---|
| Colorectal cancer, base case (95% CI) | 0.82 (0.78, 0.86) | 0.64 (0.55, 0.75) | [23] |
| Larotrectinib on-treatment utility | 0.83 | ||
| Entrectinib on-treatment utility | 0.83 | ||
| Soft tissue sarcoma, base case (95% CI) | 0.43 (0.39, 0.47) | 0.30 (0.26, 0.34) | [24] |
| Larotrectinib on-treatment utility | 0.50 | ||
| Entrectinib on-treatment utility | 0.50 |
Results
In the base case CRC model, treatment with larotrectinib resulted in 1.16 LYs (95% CrI: 0.50–2.28) and 0.95 LYs (95% CrI: 0.00–4.03) in the progression-free and postprogression states, respectively (Figure 1A & Table 3). This led to a gain of 0.81 LYs and 0.77 LYs in the progression-free and postprogression states, respectively, compared with entrectinib. Larotrectinib use had a lifetime addition of 1.58 total LYs and 1.17 total QALYs compared with entrectinib (Table 3). The most influential parameters in the OWSA were survival input estimates (see Supplementary Material). Using just the median PFS and OS point estimates for entrectinib resulted in an incremental gain of 0.26 LYs and 0.34 QALYs for larotrectinib (see Supplementary Material).
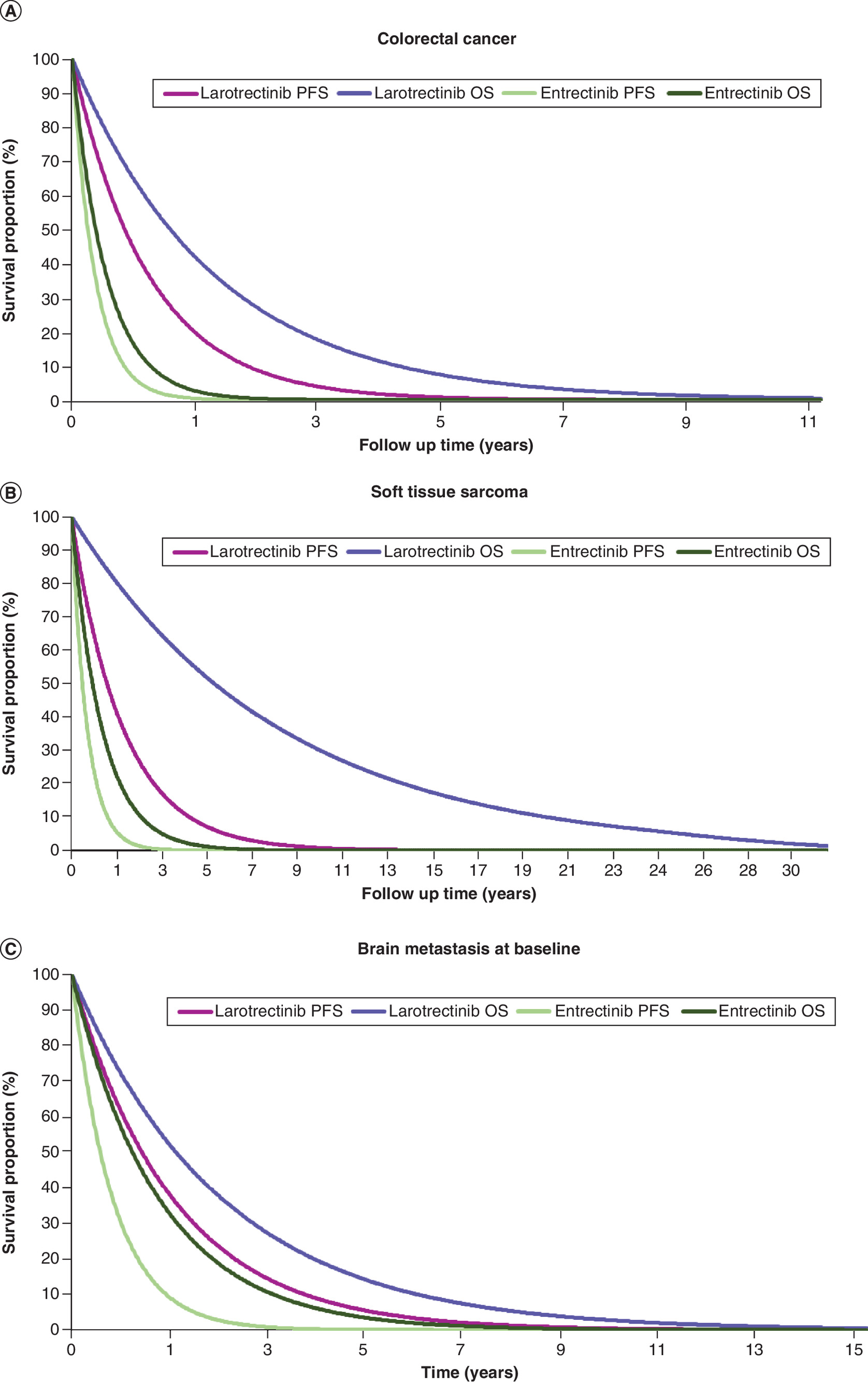
Figure 1. Parametric extrapolations of progression-free and overall survival.
(A) Colorectal cancer. (B) Soft tissue sarcoma. (C) Brain metastasis at baseline.
OS: Overall survival; PFS: Progression-free survival.
| Larotrectinib | Entrectinib | |
|---|---|---|
| Colorectal cancer | ||
| Life years, mean (95% CrI) | ||
| Progression free | 1.16 (0.50, 2.28) | 0.35 (0.14, 0.64) |
| Postprogression | 0.95 (0.00, 4.03) | 0.18 (0.00, 1.25) |
| Total | 2.11 (0.84, 5.10) | 0.53 (0.17, 1.60) |
| QALYs, mean (95% CrI) | ||
| Progression free | 0.97 (0.41, 1.90) | 0.29 (0.12, 0.53) |
| Postprogression | 0.61 (0.00, 2.52) | 0.11 (0.00, 0.82) |
| Total | 1.58 (0.66, 3.47) | 0.41 (0.14, 1.10) |
| Soft tissue sarcoma | ||
| Life years, mean (95% CrI) | ||
| Progression free | 2.08 (1.22, 3.41) | 0.66 (0.37, 1.12) |
| Postprogression | 4.99 (1.00, 10.30) | 0.60 (0.00, 1.81) |
| Total | 7.07 (3.31, 12.34) | 1.26 (0.64, 2.44) |
| QALYs, mean (95% CrI) | ||
| Progression free | 1.03 (0.61, 1.72) | 0.33 (0.18, 0.56) |
| Postprogression | 1.50 (0.31, 3.16) | 0.18 (0.00, 0.54) |
| Total | 2.53 (1.40, 4.21) | 0.51 (0.30, 0.88) |
| Brain metastasis at baseline | ||
| Life years | ||
| Progression free | 1.91 | 0.80 |
| Postprogression | 0.85 | 0.86 |
| Total | 2.76 | 1.66 |
CrI: Credible interval; QALY: Quality-adjusted life year.
For the base case STS model, estimated pre- and postprogression survival for patients treated with larotrectinib was 2.08 LYs (95% CrI: 1.22–3.41) and 4.99 (95% CrI: 1.00–10.30), respectively (Figure 1B & Table 3). These resulted in 1.42 and 4.39 LYs gained in the progression-free and postprogression states, respectively, compared with entrectinib. Compared with entrectinib, 2.02 QALYs were gained for larotrectinib. Survival inputs were the most influential parameters from the OWSA (see Supplementary Material). In the sensitivity analysis using median PFS and OS point estimates for entrectinib, there was a gain of 5.14 LYs and 1.71 QALYs for larotrectinib. In the model that assessed patients with baseline brain metastases, estimated PFS for patients treated with larotrectinib was 1.91 LYs compared with 0.80 LYs for entrectinib (Table 3). Total LYs for larotrectinib patients was 2.76 LYs compared with 1.66 LYs for entrectinib. These estimates yielded an incremental gain of 1.11 LYs for larotrectinib versus entrectinib.
Discussion
Given that the clinical trial programs for larotrectinib and entrectinib were single-armed studies that were unable to directly assess comparative and long-term outcomes, we projected lifetime PFS, OS and QALYs for larotrectinib and entrectinib in advanced CRC, STS and patients with baseline brain metastases to estimate the comparative effectiveness between the two treatments. Our intent was to provide an initial assessment of comparative health benefits while patient data matures or other study designs become feasible. Best practices were used in fitting the parametric models to available data, assessing statistical tests, visual fit and considering clinical plausibility [26]. The results, though limited by the nature of the comparisons and the small sample sizes, demonstrated consistently improved health outcomes for patients receiving larotrectinib versus entrectinib, although the magnitude of benefit varied across tumor types.
Currently, these two treatment options are often used after standard first-line or later treatments have failed. In these patients, there is a strong rationale for the use of larotrectinib or entrectinib, as NTRK gene fusions are believed to be the primary oncogenic driver of their cancers [27]. NTRK gene fusions are rare, but with increasing awareness in the clinical community and scientific societies publishing newer guidelines including recommendations for testing NTRK genomic alterations, more patients with metastatic cancers will likely discover that they are eligible to be treated with larotrectinib or entrectinib [28,29].
While treatment with larotrectinib or entrectinib might offer substantial health benefits to certain patients, selection between the two treatments will be necessary. This is evidenced by the explicit recommendation that only one TRK inhibitor be used for eligible patients with NTRK 1/2/3 gene-fusion positive NSCLC in the NCCN Guidelines® [14]. Patients with NSCLC accounted for the majority of tumor types in the brain metastases model. In addition to guideline recommendations, there is a mechanistic rationale for carefully selecting between the two available TRK inhibitors in that acquired resistance in some patients has been reported [30,31]. In the modeling results, treatment with larotrectinib resulted in different magnitudes of health gains compared with entrectinib but consistently performed better across CRC, STS and in patients with baseline brain metastases. This suggests that if patients only have one chance to use a TRK inhibitor, larotrectinib may be the appropriate option to maximize health gains.
The appropriate selection of therapy is particularly relevant when choosing between the treatment options in patients with brain metastasis. Given the harmful effects on survival and quality of life from brain metastasis, more effective systemic treatment options are sorely needed [32]. Having demonstrated CNS activity, larotrectinib and entrectinib provide additional viable treatment options for patients with baseline brain metastases. While the samples were small and baseline characteristics were not adjusted, the distribution of the primary tumor histologies in both treatment groups with baseline brain metastases were similar, supporting the comparison. The direct comparison of the two treatment options showed patients on larotrectinib gaining an additional year of OS compared with entrectinib in this group. Improvements in patients with brain metastases are continuously being made using systemic therapies, and these results signal that larotrectinib may provide substantial benefit for eligible patients.
The only other published study comparing larotrectinib and entrectinib used similar modeling methods to assess the long-term comparative effectiveness in NSCLC patients for larotrectinib and entrectinib [15]. This study found a gain of 4.77 LYs and 3.36 QALYs for larotrectinib in the base case, and even a favorable scenario analysis for entrectinib found 2.38 LYs and 2.03 QALYs gained for larotrectinib. Similar to the current study, however, the NSCLC model was also limited to a naive, cross-trial comparison of small samples. Further evidence to support the use of larotrectinib is limited to case reports given the novelty of larotrectinib and the rarity of NTRK gene fusions [33,34].
Limitations
There are several limitations to this study. As the clinical trials for larotrectinib and entrectinib were single-armed studies, our study was a naive, direct (cross-trial) comparison of survival for the two treatments. Patients' baseline and clinical characteristics were not randomized, matched or adjusted for, which could have impacted the results. The median age when simulated patients entered into the models between larotrectinib and entrectinib varied slightly, which may have contributed to the projected improved survival with larotrectinib. However, given that PFS and OS were short across the models, this difference in starting median age likely did not have a significant impact. Furthermore, sample sizes across all three models were small. Consequently, there is considerable uncertainty about how the model results will translate to clinical practice outside of phase I and II trials. We attempted to characterize the uncertainty as much as possible by running OWSA, PSA and sensitivity analyses for entrectinib. Additionally, we did not evaluate comparative safety differences between the two TRK inhibitors. Due to these limitations, the results should be considered a first-stage comparison and be interpreted with appropriate caution.
Conclusion
Based on this modeling study that was informed by parametric extrapolations of in-trial survival data, treatment with larotrectinib led to gains in LYs and QALYs compared with entrectinib in patients with NTRK gene fusion. Limitations of this study included small samples of patients in each subgroup and a cross-trial comparison. Updated analysis with larger samples and more mature survival data could help reduce uncertainty in future studies assessing the comparative effectiveness of larotrectinib and entrectinib.
Background
•
Larotrectinib and entrectinib are TRK inhibitors that are indicated for multiple tumor types.
•
Larotrectinib demonstrated improvements in life expectancy and health utility in patients with TRK fusion-positive metastatic non-small cell lung cancer compared with entrectinib.
•
Larotrectinib also demonstrated improvements in life expectancy and health utility compared with standard of care in patients with differentiated thyroid cancer, colorectal cancer (CRC) and soft tissue sarcoma (STS).
•
No study has evaluated the comparative effectiveness of larotrectinib versus entrectinib in other metastatic cancers, specifically CRC and STS, and prior brain metastases.
What this study adds
•
Larotrectinib clinical trial data and published literature were used to inform simulation modeling of life expectancy and quality-adjusted life years (QALYs) to assess the comparative effectiveness of larotrectinib against entrectinib across TRK fusion-positive metastatic CRC, STS and prior brain metastases.
•
The modeling results showed larotrectinib is expected to provide additional life-years and QALYs compared with entrectinib in TRK fusion-positive metastatic CRC, STS and prior brain metastases.
•
As the survival data for larotrectinib and entrectinib mature and additional patients are treated, future studies should reassess the comparative effectiveness.
Impact on clinical practice
•
This evidence will help clinicians and decision-makers assess the relative clinical value of larotrectinib and entrectinib.
Financial & competing interests disclosure
K Suh, JJ Carlson and SD Sullivan report personal fees from Bayer US LLC during the conduct of the study. F Xia and T Williamson are employees of Bayer US LLC. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
Data sharing statement
The authors certify that this manuscript reports the secondary analysis of clinical trial data that have been shared with them and that the use of this shared data is in accordance with the terms (if any) agreed upon their receipt. The source of this data is Bayer US LLC, data on file.
Supplementary Material
File (supplementary materials (8).docx)
- Download
- 86.50 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Chabner BA, Roberts TG Jr. Timeline: chemotherapy and the war on cancer. Nat. Rev. Cancer 5(1), 65–72 (2005).
2.
Hyman DM, Taylor BS, Baselga J. Implementing genome-driven oncology. Cell 168(4), 584–599 (2017).
3.
Chen Y, Chi P. Basket trial of TRK inhibitors demonstrates efficacy in TRK fusion-positive cancers. J. Hematol. Oncol. 11(1), 78 (2018).
4.
Woodcock J, LaVange LM. Master protocols to study multiple therapies, multiple diseases, or both. N. Engl. J. Med. 377(1), 62–70 (2017).
5.
Drilon A, Laetsch TW, Kummar S et al. Efficacy of larotrectinib in TRK fusion-positive cancers in adults and children. N. Engl. J. Med. 378(8), 731–739 (2018).
• Across three clinical trials, larotrectinib demonstrated promising efficacy results.
6.
Hong DS, DuBois SG, Kummar S et al. Larotrectinib in patients with TRK fusion-positive solid tumours: a pooled analysis of three phase 1/2 clinical trials. Lancet Oncol. 21(4), 531–540 (2020).
7.
Doebele RC, Drilon A, Paz-Ares L et al. Entrectinib in patients with advanced or metastatic NTRK fusion-positive solid tumours: integrated analysis of three phase 1–2 trials. Lancet Oncol. 21(2), 271–282 (2020).
8.
Cocco E, Scaltriti M, Drilon A. NTRK fusion-positive cancers and TRK inhibitor therapy. Nat. Rev. Clin. Oncol. 15(12), 731–747 (2018).
9.
Farago AF, Le LP, Zheng Z et al. Durable clinical response to entrectinib in NTRK1-rearranged non-small cell lung cancer. J. Thorac. Oncol. 10(12), 1670–1674 (2015).
10.
Rosen EY, Schram AM, Young RJ et al. Larotrectinib demonstrates CNS efficacy in TRK fusion-positive solid tumors. JCO Precis. Oncol. 3, 19.00009 (2019).
11.
Ziegler DS, Wong M, Mayoh C et al. Brief report: potent clinical and radiological response to larotrectinib in TRK fusion-driven high-grade glioma. Br. J. Cancer 119(6), 693–696 (2018).
12.
Hatiboglu MA, Wildrick DM, Sawaya R. The role of surgical resection in patients with brain metastases. Ecancermedicalscience 7, 308 (2013).
13.
Liu Q, Tong X, Wang J. Management of brain metastases: history and the present. Chin. Neurosurg. J. 5(1), 1 (2019).
14.
Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Non-Small Cell Lung Cancer (V.6.2021). © National Comprehensive Cancer Network, Inc. 2021 All rights reserved. Accessed [September 30, 2021]. To view the most recent and complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.
15.
Roth JA, Carlson JJ, Xia F, Williamson T, Sullivan SD. The potential long-term comparative effectiveness of larotrectinib and entrectinib for second-line treatment of TRK fusion-positive metastatic lung cancer. J. Manag. Care Spec. Pharm. 26(8), 981–986 (2020).
•• In a prior analysis of larotrectinib and entrectinib using similar methods, larotrectinib was projected to gain additional life years and quality-adjusted life years compared to entrectinib in patients with TRK fusion-positive metastatic lung cancer.
16.
Kim H, Gurrin L, Ademi Z, Liew D. Overview of methods for comparing the efficacies of drugs in the absence of head-to-head clinical trial data. Br. J. Clin. Pharmacol. 77(1), 116–121 (2014).
• In the absence of head-to-head trials or the ability to directly compare two treatments, naive direct comparisons can be performed as outlined here.
17.
Hoyle MW, Henley W. Improved curve fits to summary survival data: application to economic evaluation of health technologies. BMC Med. Res. Methodol. 11, 139 (2011).
18.
Cost-Effectiveness in Health and Medicine (2nd Edition). Neumann P, Sanders G, Russell L, Siegel J, Ganiats T. (Eds). Oxford University Press, NY, USA (2017).
19.
Bayer US LLC. Data on file. (2020).
20.
Patel M, Siena S, Demetri G et al. Efficacy and safety of entrectinib in NTRK fusion-positive gastrointestinal cancers: updated integrated analysis of three clinical trials (STARTRK-2, STARTRK-1 and ALKA-372-001). Ann. Oncol. 31, S232–S233 (2020).
21.
Chawla S, Paz-Ares L, Patel M et al. An updated analysis of the clinical efficacy and safety of entrectinib in NTRK fusion-positive sarcoma. Presented at: 2020 CTOS Virtual Meeting, November 18–21, 2020.
22.
Centers for Disease Control and Prevention. United States life tables, 2018. Natl Vital Stat. Rep. 69(13), 1–83 (2021).
23.
Rolfo CD, De Braud FG, Doebele RC et al. Efficacy and safety of entrectinib in patients (pts) with NTRK-fusion-positive (NTRK-fp) solid tumors: an updated integrated analysis. J. Clin. Oncol. 38(Suppl. 15), 3605 (2020).
24.
Färkkilä N, Sintonen H, Saarto T et al. Health-related quality of life in colorectal cancer. Colorectal Dis. 15(5), e215–e222 (2013).
25.
Guest JF, Sladkevicius E, Gough N, Linch M, Grimer R. Utility values for advanced soft tissue sarcoma health states from the general public in the United Kingdom. Sarcoma 2013, 863056 (2013).
26.
Latimer NR. Survival analysis for economic evaluations alongside clinical trials – extrapolation with patient-level data: inconsistencies, limitations, and a practical guide. Med. Decis. Making 33(6), 743–754 (2013).
27.
Rosen EY, Goldman DA, Hechtman JF et al. TRK fusions are enriched in cancers with uncommon histologies and the absence of canonical driver mutations. Clin. Cancer Res. 26(7), 1624–1632 (2020).
28.
Demetri GD, Antonescu CR, Bjerkehagen B et al. Diagnosis and management of tropomyosin receptor kinase (TRK) fusion sarcomas: expert recommendations from the World Sarcoma Network. Ann. Oncol. 31(11), 1506–1517 (2020).
29.
Marchiò C, Scaltriti M, Ladanyi M et al. ESMO recommendations on the standard methods to detect NTRK fusions in daily practice and clinical research. Ann. Oncol. 30(9), 1417–1427 (2019).
30.
Drilon A, Li G, Dogan S et al. What hides behind the MASC: clinical response and acquired resistance to entrectinib after ETV6-NTRK3 identification in a mammary analogue secretory carcinoma (MASC). Ann. Oncol. 27(5), 920–926 (2016).
31.
Russo M, Misale S, Wei G et al. Acquired resistance to the TRK inhibitor entrectinib in colorectal cancer. Cancer Discov. 6(1), 36–44 (2016).
32.
Peters S, Bexelius C, Munk V, Leighl N. The impact of brain metastasis on quality of life, resource utilization and survival in patients with non-small-cell lung cancer. Cancer Treat. Rev. 45, 139–162 (2016).
33.
Percy C, Schubert T, Galant C, Kirchgesner T, Mazzeo F. Larotrectinib in a NTRK-rearranged soft tissue sarcoma in the neoadjuvant setting: a case report. Clin. Case Rep. 9(3), 1694–1698 (2021).
34.
Rabban JT, Devine WP, Sangoi AR et al. NTRK fusion cervical sarcoma: a report of three cases, emphasising morphological and immunohistochemical distinction from other uterine sarcomas, including adenosarcoma. Histopathology 77(1), 100–111 (2020).
Information & Authors
Information
Published In
Pages: 1011 - 1019
PubMed: 35993247
Copyright
© 2022 Future Medicine Ltd. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 14 October 2021
Accepted: 15 July 2022
Published online: 22 August 2022
Keywords:
Topics
Authors
Funding Information
Bayer US LLC
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparative effectiveness of larotrectinib versus entrectinib for the treatment of metastatic NTRK gene fusion cancers. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0247
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Filipa Mascarenhas-Melo, Rafael Pinheiro, Francis Victor, Maria Eugénia Pina, Ana Figueiras, Pharmaceutical Compounding as a Pillar of Personalized Oncology: Current Applications, Emerging Technologies, and Future Perspectives, Pharmaceuticals, 10.3390/ph19071077, 19, 7, (1077), (2026).
- Shahd Hamran, Zaineh Alnoubani, Aly Mostafa Hassan, Amani A. Al-Rajhi, Humam Emad Rajha, Munirah Altaissan, Giridhara R. Babu, Zoran Gatalica, Semir Vranić, NTRK1-3 fusions in sarcomas: prevalence, significance, and clinical implications – a systematic review , Future Oncology, 10.1080/14796694.2025.2597405, 21, 30, (4011-4024), (2025).
- Nasim Izadi, Aneta Fried, Sarka Sevcikova, Johana Strmiskova, Ludmila Moranova, Susana Campuzano, Martin Bartosik, Electrochemical detection of fusion genes: Advancing cancer diagnosis and therapy, Electrochimica Acta, 10.1016/j.electacta.2025.147472, 542, (147472), (2025).
- Sara Polajžer, Katarina Černe, Precision Medicine in High-Grade Serous Ovarian Cancer: Targeted Therapies and the Challenge of Chemoresistance, International Journal of Molecular Sciences, 10.3390/ijms26062545, 26, 6, (2545), (2025).
- Seungmee Lee, Yu-Ra Jeon, Changmin Shin, Sun-Young Kwon, Sojin Shin, Pan-TRK positive uterine sarcoma in immunohistochemistry without neurotrophic tyrosine receptor kinase gene fusions: A case report, World Journal of Clinical Cases, 10.12998/wjcc.v13.i2.96876, 13, 2, (2025).
- Kangho Suh, Ashley Kang, Gilbert Ko, Todd Williamson, Nick Liao, Sean D. Sullivan, Projecting long-term clinical outcomes with larotrectinib compared with immune checkpoint inhibitors in metastatic nonsmall cell lung cancer and differentiated thyroid cancer, Journal of Managed Care & Specialty Pharmacy, 10.18553/jmcp.2024.30.6.581, 30, 6, (581-587), (2024).
- Akanksha Dessai, Usha Yogendra Nayak, Yogendra Nayak, Precision nanomedicine to treat non-small cell lung cancer, Life Sciences, 10.1016/j.lfs.2024.122614, 346, (122614), (2024).
- Svetlana N. Aleksakhina, Alexander O. Ivantsov, Evgeny N. Imyanitov, Agnostic Administration of Targeted Anticancer Drugs: Looking for a Balance between Hype and Caution, International Journal of Molecular Sciences, 10.3390/ijms25074094, 25, 7, (4094), (2024).
- Gang Wang, Zhi Min Zhu, Kun Wang, Integrative analysis of PTEN ‐related hub genes and validating drug targets for colorectal cancer , Precision Medical Sciences, 10.1002/prm2.12126, 13, 1, (4-20), (2024).
- Daohong Chen, Biomarkers navigate drug development: Pharmacology, effectiveness and safety, Medicine in Drug Discovery, 10.1016/j.medidd.2023.100174, 21, (100174), (2024).