Clinical manifestations and healthcare utilization before diagnosis of transthyretin amyloidosis
Publication: Journal of Comparative Effectiveness Research
Abstract
Introduction: Initial clinical manifestations of transthyretin amyloidosis (ATTR) are not well understood, making timely diagnosis challenging. Methods: Patients aged ≥68 years newly diagnosed with ATTR were identified using Medicare Research Identifiable Files. Symptom manifestation and healthcare utilization were measured during 3 years pre-diagnosis; demographics and comorbidity index during 1-year pre-diagnosis. Controls (ATTR-free) were matched 1:1 to patients with ATTR based on age, sex and region; same index date and enrollment as match. Results: We identified 552 matched ATTR-control pairs: mean age 78.3 (standard deviation 6.3) and 64.5% male. Among patients with ATTR (vs controls), cardiovascular conditions (92.9 vs 75.9%) and hospitalization (54.0 vs 35.5%) were frequent during 3 years pre-diagnosis. Conclusion: Patients with ATTR have multiple symptoms and hospitalizations pre-diagnosis, recognition of which may facilitate earlier diagnosis and treatment.
Transthyretin amyloidosis (ATTR) is a progressive, debilitating condition caused by multisystem infiltration of transthyretin (TTR) amyloid fibrils. Extracellular deposition of amyloid fibrils triggered by dissociation and misfolding of TTR protein can result from heritable mutations in the TTR gene (mutant or variant [ATTRv]) or aging-related misfolding (wild-type [ATTRwt]), giving rise to two distinct subtypes of the condition [1,2]. Cardiomyopathy, bilateral carpal tunnel syndrome and progressive symmetric sensorimotor neuropathy are the primary manifestations of ATTR [3,4]. As the condition progresses, amyloid deposits in the gastrointestinal tract, eyes and other tissues can lead to additional multisystem symptoms [5]. The presence and extent of cardiac involvement is a major cause of morbidity and significantly affects overall survival and quality of life [6,7]. Progressive heart failure, frequently with preserved left ventricular ejection fraction, ventricular hypertrophy in the absence of hypertension, arrhythmias (especially atrial fibrillation), conduction system disorders and intracardiac thrombus causing systemic embolization are major manifestations of ATTR cardiomyopathy (ATTR-CM) [6–8].
Diagnosis of ATTR is often delayed or missed due to multiple overlapping and nonspecific clinical manifestations, symptom variability and low disease awareness. Delayed diagnosis can lead to symptom worsening, impaired function and poor quality of life due to disease progression [6,7]. A prospective evaluation of 916 patients with ATTR-CM established a diagnostic delay of more than 4 years after cardiac symptom presentation in 42% of cases evaluated. Significant functional impairment, worsening of cardiac disease, greater decline in quality of life and poorer survival were noted at the time of diagnosis [7]. The heterogeneity in symptom manifestation further mandates multidisciplinary care, frequent hospital visits and high rate of healthcare utilization [5,9,10].
New disease-modifying agents such as the TTR silencers (inotersen and patisiran) and stabilizers (tafamidis, diflunisal and acoramidis) that inhibit TTR protein production or prevent its aggregation to amyloid fibrils have demonstrated significant improvement in clinical outcomes [11–16]. Treatment with inotersen and patisiran is associated with reduced polyneuropathy and improved quality of life; tafamidis with reduced cardiovascular (CV) mortality and CV-related hospitalization; and diflunisal with reduced progression of neurologic impairment and preserved quality of life [11–15]. Given the availability of effective treatment, there is an emerging need to better understand the initial clinical presentation of this previously untreatable condition to facilitate earlier diagnosis and prompt treatment.
Limited research exists about patient symptoms and experiences before diagnosis of ATTR. A previous study evaluated patient clinical characteristics and healthcare utilization before ATTRv diagnosis through retrospective analysis of a large commercial claims database [17]. However, a key limitation of that study was the underrepresentation of older patients, who are more likely to be affected by the disease. Thus, this study was designed to understand the pattern of patient clinical characteristics and healthcare utilization in the years leading up to diagnosis of ATTR among Medicare beneficiaries.
Methods & materials
Study design & data source
This was a retrospective, descriptive analysis of the Medicare claims database, Research Identifiable Files (RIFs) during an 8-year study period between 1 January 2011 and 31 December 2018. The Medicare RIFs database is the most comprehensive Medicare data source capturing all Medicare-enrolled beneficiaries from all census regions in the US. The database includes patient information on demographics, enrollment and administrative claims-level data for more than 55 million Medicare enrolled beneficiaries as of 2015 [18]. Detailed information on inpatient and outpatient services, diagnoses and procedures (International Classification of Diseases [ICD] versions 9/10), prescription drugs, skilled nursing facility and home health care, hospice care, durable medical equipment, dates of service and provider charges and characteristics can be obtained for analyses [19]. In addition, Medicare RIFs include a unique, encrypted beneficiary identifier that allows linkage across files and time [19]. As the database allows for the largest possible sample size of beneficiaries it is well suited for studying rare diseases [20]. This study received approval for full waiver of Health Insurance Portability and Accountability Act authorization from the Western Institutional Review Board. Partnership for Health Analytic Research, LLC, a health services research company, was hired by Akcea Pharmaceuticals to conduct this study.
Patient population & time frame
Clinical characteristics and healthcare utilization data of patients ≥68 years old (age requirement allowed for an adequate sample size among Medicare enrollees who are primarily 65 years and older, taking into account the chosen pre-index observation period defined below), before ATTR diagnosis (ATTRv or ATTRwt) during the identification (ID) period (1 January 2011 to 31 December 2018) were extracted through RIFs. Patients with newly diagnosed ATTR, defined as those having one or more inpatient or two or more outpatient medical claims with a diagnosis code for ATTR (ICD-10, Clinical Modification [ICD-10-CM]: E85.1, E85.2, E85.82) were included in the study. Patients diagnosed with other amyloidosis diagnosis code (ICD-10-CM: E85.0, E85.89, E85.9), except light chain, secondary systemic and organ-limited amyloidosis, during any time in the study period (2011–2018) were included if they had one or more medical claim (inpatient or outpatient) with a diagnosis code for congestive heart failure (CHF), cardiomyopathy (restrictive or hypertrophic) or neuropathy and had no claims for chemotherapy or stem cell transplant. Among those identified, patients with evidence of dementia at any time in the study period (2011–2018) were excluded to omit patients with amyloid angiopathy, which may be observed in patients with dementia and was not an amyloidosis type of interest [21–23]. The index date was defined as the date of the first claim with an ATTR diagnosis code during the ID period. A disease-free control group of patients without history of diagnosis of amyloidosis was derived from a 5% random sample of enrollees between 1 January 2011 to 31 December 2018. Patients in the control group were matched 1:1 to patients identified as newly diagnosed with ATTR (i.e., cases) based on age, sex and region and were assigned the same index date as their matched ATTR case. The baseline period was defined as the 1-year period before the index date. In addition, a 3-year period before the index date was used to examine manifestation of clinical characteristics and healthcare utilization of interest before the index diagnosis. All patients were required to have continuous enrollment in fee-for-service Medicare Parts A (hospital insurance) and B (medical insurance) and Part D (prescription drug coverage) during the 3 years before diagnosis to ensure completeness of available clinical data for included patients.
Study measures & statistical analysis
Baseline characteristics including patient demographics (age, sex and geographic region), physician characteristics including diagnosing physician specialty at index date (physician associated with index claim) and frequently visited physician specialty during the baseline period (hematologist/oncologist, nephrologist, cardiologist, gastroenterologist, neurologist, primary care physician, and other) were described. To examine severity of comorbidity burden, the Charlson Comorbidity Index (CCI) was calculated [24]; and the number of chronic conditions was counted using the Healthcare Cost and Utilization Project chronic condition indicator [25].
In each pre-index year during the 3 years before diagnosis, the occurrence of selected comorbid conditions and symptoms, with one or more claims, potentially related to ATTR (nervous system, CV, ocular, musculoskeletal, gastrointestinal, and metabolic conditions and multiorgan failures/dysfunctions) was identified. Proportions of patients with CV conditions and carpal tunnel syndrome, spinal stenosis and/or aortic stenosis and interquartile mean time between first evidence of CV condition and index diagnosis were also calculated. Healthcare utilization including proportion of patients with an indication for undergoing selected diagnostic testing (blood/urine testing, cardiac imaging, tissue biopsy, genetic testing, nerve conduction study, gastric emptying, and mass spectrometry), therapeutic services (defibrillator/pacemaker [cardiac implantable electronic device], stent, cardiac ablation, cardioversion) and CV-related inpatient hospitalization and emergency department (ED) visits and mean number of outpatient physician visits and prescription fills were calculated. Utilization was considered CV-related if its billing claim included a primary diagnosis code for one of the selected CV conditions.
All data transformations and statistical analyses were performed using SAS version 9.4. A two-sided p-value <0.05 was considered statistically significant. Patient clinical characteristics and healthcare utilization in each pre-index year over the 3 years before diagnosis were summarized through descriptive statistics (mean, standard deviation [SD] and range). Continuous variables were summarized as means and SD, and categorical variables were described as frequencies and percentages. All outcomes were compared between cases versus matched controls. Results are reported in accordance with the Centers for Medicare & Medicaid Services cell size suppression policy, which stipulates that no cell with a value <11 (not including 0) can be directly reported [26].
Results
Of the 1359 Medicare claims patients identified during the ID period, 371 fulfilled the criteria for the 3-year look-back period (≥68 years) with a specific diagnostic code for ATTRv or ATTRwt. Among 11,755 Medicare claims patients identified with diagnostic code for other amyloidosis types (except light chain, secondary systemic and organ-limited amyloidosis), 921 fulfilled the inclusion criteria for ATTR. Following the exclusion of those with a diagnosis code of dementia, the final cohort consisted of 552 patients with ATTR, who were matched with 552 ATTR free controls (Table 1).
| Criteria for identifying patients with ATTR amyloidosis | Final ATTR cohort with 3-year look-back period |
|---|---|
| A. Had ≥1 inpatient or ≥2 outpatient medical claims during the ID period (1/1/2016–31/12/2018) with a diagnosis code for hereditary or wild-type forms of amyloidosis and had no amyloidosis diagnosis before the index date (the first diagnosis date in ID period) | 1359 |
| A1. Among A, who were continuously enrolled in the 3 years before the index date | 389 |
| A2. Among A1, who were at least 68 years old on the index date | 371 |
| B. Had ≥1 inpatient or ≥2 outpatient medical claims in the specific CY with a diagnosis code for another form of amyloidosis (except light chain, secondary systemic, and organ-limited amyloidosis) and had no amyloidosis diagnosis before the index date (the first diagnosis date in ID period) | 11,755 |
| B1. Among B, who were continuously enrolled in the 3 years before the index date | 3667 |
| B2. Among B1, who were at least 68 years old on the index date | 3490 |
| B3. Among B2, had ≥1 medical claim with a diagnosis code for CHF, cardiomyopathy, or neuropathy in study period (2011–2018) | 2758 |
| B4. Among B3, lack evidence of chemotherapy or stem cell transplant in study period | 979 |
| B5. Among B4, lack evidence of a diagnosis of light chain amyloidosis in study period | 921 |
| C. A2 or B5 | 1228 |
| D. Among C, had no evidence of dementia in study period | 552 |
ATTR: Transthyretin amyloidosis; CHF: Congestive heart failure; CY: Claim year; ID: Identification.
Comorbidity & treating physician characteristics
The mean (SD) age among patients with ATTR and matched controls was 78.3 (6.3) years, with more patients belonging to the age group 75–85 years (50.9%). Overall, 35.5% of patients were female, and a predominance of White race beneficiaries was observed in both the groups of interest (ATTR vs control: 83.9 vs 91.5%; p < 0.001) (Table 2). Patients with ATTR presented with significant comorbidity burden in the year before diagnosis, with a mean (SD) CCI of 3.1 (2.5) and 5.4 (2.0) chronic conditions relative to a CCI of 2.0 (2.4) and 4.3 (2.0) chronic conditions in matched controls. In the year before diagnosis, primary care physicians were the most commonly seen physician type by patients with ATTR (48.0 vs 44.4% in matched controls), followed by cardiologists (17.9 vs 10.0%), dermatologists (3.8 vs 7.1%), hematologist/oncologists (3.1%) and orthopedic surgeons (2.0 vs 2.9%). Cardiologists were the diagnosing physician in 16.1% of patients, followed by hematologist/oncologists (9.6%), primary care physicians (9.4%), pathologists (6.5%) and radiologists (4.9%) (Table 3).
| ATTR | Matched DF controls† | p-value | |
|---|---|---|---|
| N | 552 | 552 | |
| Age in years, mean (SD) | 78.3 (6.3) | 78.3 (6.3) | NA‡ |
| 68–69, n (%) | 29 (5.3) | 29 (5.3) | |
| 70–74, n (%) | 149 (27.0) | 149 (27.0) | |
| 75–84, n (%) | 281 (50.9) | 281 (50.9) | |
| 85+, n (%) | 93 (16.8) | 93 (16.8) | |
| Female, n (%) | 196 (35.5) | 196 (35.5) | NA‡ |
| Race, n (%) | <0.001 | ||
| White | 463 (83.9) | 505 (91.5) | |
| Black | 67 (12.1) | 30 (5.4) | |
| Other/unknown | 22 (4.0) | 17 (3.1) | |
| Region, n (%) | NA‡ | ||
| Midwest | 149 (27.0) | 149 (27.0) | |
| Northeast | 163 (29.5) | 163 (29.5) | |
| South | 146 (26.4) | 146 (26.4) | |
| West | 94 (17.0) | 94 (17.0) | |
| Year of index date, n (%) | NA‡ | ||
| 2016 | 165 (29.9) | 165 (29.9) | |
| 2017 | 167 (30.3) | 167 (30.3) | |
| 2018 | 220 (39.9) | 220 (39.9) |
†
Matched with age, gender and region.
‡
Matched exactly.
ATTR: Transthyretin amyloidosis; DF: Disease free; NA: Not available; SD: Standard deviation.
| ATTR | Matched DF controls‡ | p-value | |
|---|---|---|---|
| N | 552 | 552 | |
| Charlson Comorbidity Index, mean (SD) | 3.1 (2.5) | 2.0 (2.4) | <0.001 |
| Number of chronic conditions, mean (SD) | 5.4 (2.0) | 4.3 (2.0) | <0.001 |
| Physician specialty, n (%) | <0.001 | ||
| Primary care | 265 (48.0) | 245 (44.4) | |
| Cardiology | 99 (17.9) | 55 (10.0) | |
| Dermatology | 21 (3.8) | 39 (7.1) | |
| Orthopedic surgery | 11 (2.0) | 16 (2.9) | |
| Hematology/oncology | 17 (3.1) | –§ | |
| Urology | –§ | 16 (2.9) | |
| Other specialty¶ | 115 (20.8) | 126 (22.8) | |
| No evaluation and management services | 17 (3.1) | 48 (8.7) | |
| Provider associated with index claim, n (%) | NA | ||
| Facility claims, unknown specialty | 214 (38.8) | NA | |
| Cardiology | 89 (16.1) | NA | |
| Hematology/oncology | 53 (9.6) | NA | |
| Primary care | 52 (9.4) | NA | |
| Pathology | 36 (6.5) | NA | |
| Diagnostic radiology | 27 (4.9) | NA | |
| Other specialty | 81 (14.7) | NA |
†
During 1 year before the index date.
‡
Matched with age, gender and region.
§
Reported per Centers for Medicare & Medicaid Services cell size suppression policy (i.e., frequency <11).
¶
Included all other specialties with frequency <2% and podiatry (2.4%, n = 26).
ATTR: Transthyretin amyloidosis; DF: Disease free; NA: Not available; SD: Standard deviation.
In the 3 years leading up to ATTR diagnosis, occurrence of the selected comorbidities was more frequent among patients with ATTR relative to matched controls (Figure 1, Table 4). A statistically significant difference (p < 0.05) in the observed comorbidities was noticed between patients with ATTR and matched controls in CV conditions (92.9 vs 75.9%), musculoskeletal conditions (62.9 vs 42.2%), gastrointestinal conditions (49.1 vs 36.8%), metabolic conditions (46.6 vs 37.1%), nervous system conditions (37.7 vs 22.1%), ocular conditions (33.0 vs 25.9%) and organ dysfunction or failure (28.3 vs 15.4%). In patients with nervous system conditions, a statistically significant difference between cases and matched controls was observed only for peripheral neuropathy (29.2 vs 11.8%; ATTR vs matched controls; p < 0.001), whereas other neurological symptoms including urinary incontinence (12.5 vs 13.6%) and fecal incontinence (2.4 vs 2.0%) were not statistically significant. Among the musculoskeletal conditions, percentage of patients with ATTR who developed spinal stenosis (28.8 vs 14.7%) and carpel tunnel syndrome (16.7 vs 6.2%) were statistically higher than matched controls. In the case of gastrointestinal conditions, a statistically significant difference was observed among the percentage of patients who experienced constipation (21.9 vs 13.6%) (Table 4).
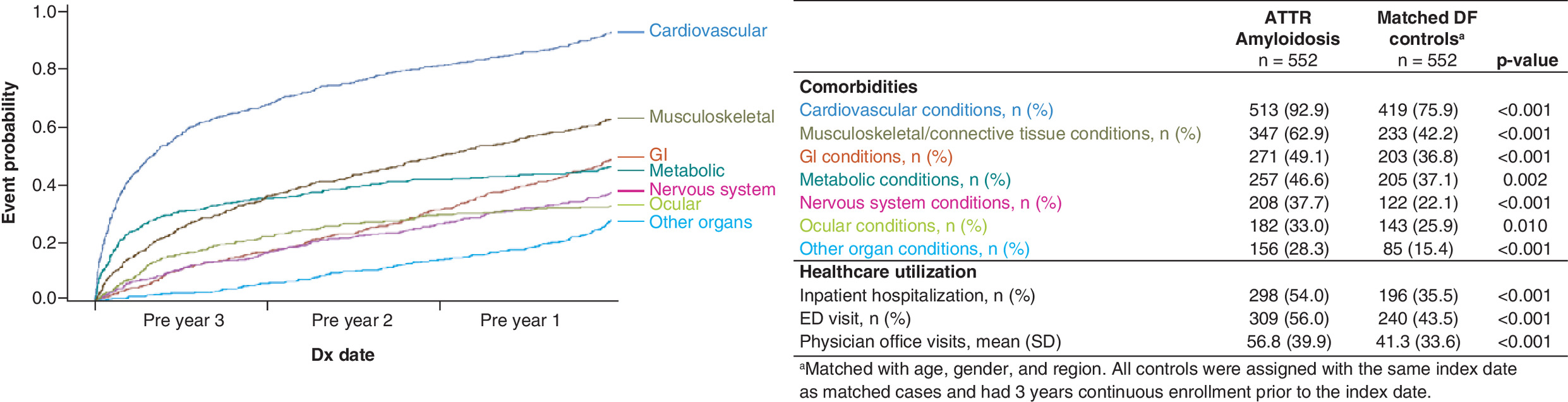
Figure 1. First observed occurrence of comorbidity by organ system during 3 years prior to ATTR diagnosis (left) and aggregate comorbidity and healthcare utilization in pre-diagnosis period (right).
In the 3 years leading up to ATTR diagnosis, occurrence of the selected comorbidities and healthcare utilization was more frequent among patients with ATTR relative to matched controls.
ATTR: Transthyretin amyloidosis; DF: Disease free; Dx: Diagnosis; ED: Emergency department; GI: Gastrointestinal; SD: Standard deviation.
| ATTR | Matched DF controls† | p-value | |
|---|---|---|---|
| N | 552 | 552 | |
| Cardiovascular conditions, n (%) | 513 (92.9) | 419 (75.9) | <0.001 |
| First evidence occurred | <0.001 | ||
| No evidence | 39 (7.1) | 133 (24.1) | |
| Pre-Y3 | 375 (67.9) | 313 (56.7) | |
| Pre-Y2 | 74 (13.4) | 57 (10.3) | |
| Pre-Y1 | 64 (11.6) | 49 (8.9) | |
| Dyspnea | 396 (71.7) | 208 (37.7) | <0.001 |
| Congestive heart failure | 348 (63.0) | 121 (21.9) | <0.001 |
| Edema | 279 (50.5) | 121 (21.9) | <0.001 |
| Atrial fibrillation/flutter | 267 (48.4) | 128 (23.2) | <0.001 |
| Ventricular hypertrophy | 248 (44.9) | 81 (14.7) | <0.001 |
| Chest pain | 231 (41.8) | 142 (25.7) | <0.001 |
| Other hemorrhages‡ | 218 (39.5) | 160 (29.0) | <0.001 |
| Coronary artery disease | 207 (37.5) | 163 (29.5) | 0.005 |
| Aortic stenosis | 143 (25.9) | 87 (15.8) | <0.001 |
| Bradycardia | 131 (23.7) | 96 (17.4) | 0.009 |
| Hypotension | 114 (20.7) | 62 (11.2) | <0.001 |
| Syncope | 93 (16.8) | 81 (14.7) | 0.322 |
| Myocardial infarction | 80 (14.5) | 34 (6.2) | <0.001 |
| Restrictive cardiomyopathy | 63 (11.4) | 18 (3.3) | <0.001 |
| Hypertrophic cardiomyopathy | 44 (8.0) | –§ | <0.001 |
| Ischemic stroke | 43 (7.8) | 41 (7.4) | 0.820 |
| Hemorrhagic stroke | –§ | –§ | 0.999 |
| Musculoskeletal/connective tissue conditions, n (%) | 347 (62.9) | 233 (42.2) | <0.001 |
| First evidence occurred | <0.001 | ||
| No evidence | 205 (37.1) | 319 (57.8) | |
| Pre-Y3 | 202 (36.6) | 138 (25.0) | |
| Pre-Y2 | 75 (13.6) | 54 (9.8) | |
| Pre-Y1 | 70 (12.7) | 41 (7.4) | |
| Spinal stenosis | 159 (28.8) | 81 (14.7) | <0.001 |
| Low bone mineral density | 113 (20.5) | 95 (17.2) | 0.166 |
| Osteoporosis | 107 (19.4) | 84 (15.2) | 0.067 |
| Carpal tunnel syndrome | 92 (16.7) | 34 (6.2) | <0.001 |
| Fibromyalgia | 50 (9.1) | 28 (5.1) | 0.010 |
| Biceps rupture | 22 (4.0) | 14 (2.5) | 0.175 |
| Hip/knee arthroscopy | –§ | –§ | 0.435 |
| Gastrointestinal conditions, n (%) | 271 (49.1) | 203 (36.8) | <0.001 |
| First evidence occurred | <0.001 | ||
| No evidence | 281 (50.9) | 349 (63.2) | |
| Pre-Y3 | 96 (17.4) | 72 (13.0) | |
| Pre-Y2 | 79 (14.3) | 75 (13.6) | |
| Pre-Y1 | 96 (17.4) | 56 (10.1) | |
| Constipation | 121 (21.9) | 75 (13.6) | <0.001 |
| Nausea | 110 (19.9) | 95 (17.2) | 0.246 |
| Diarrhea | 104 (18.8) | 72 (13.0) | 0.009 |
| Unintentional weight loss | 78 (14.1) | 62 (11.2) | 0.148 |
| Gastroparesis | –§ | –§ | 0.094 |
| Metabolic conditions, n (%) | 257 (46.6) | 205 (37.1) | 0.002 |
| First evidence occurred | <0.001 | ||
| No evidence | 295 (53.4) | 347 (62.9) | |
| Pre-Y3 | 197 (35.7) | 166 (30.1) | |
| Pre-Y2 | 36 (6.5) | 22 (4.0) | |
| Pre-Y1 | 24 (4.3) | 17 (3.1) | |
| Diabetes | 257 (46.6) | 205 (37.1) | 0.002 |
| Nervous system conditions, n (%) | 208 (37.7) | 122 (22.1) | <0.001 |
| First evidence occurred | <0.001 | ||
| Pre Y3 | 93 (16.8) | 63 (11.4) | |
| Pre Y2 | 55 (10.0) | 35 (6.3) | |
| Pre Y1 | 60 (10.9) | 24 (4.3) | |
| Neuropathy | 161 (29.2) | 65 (11.8) | <0.001 |
| Incontinence | 78 (14.1) | 81 (14.7) | 0.797 |
| Urinary incontinence | 69 (12.5) | 75 (13.6) | 0.592 |
| Fecal incontinence | 13 (2.4) | 11 (2.0) | 0.680 |
| Ocular conditions, n (%) | 182 (33.0) | 143 (25.9) | 0.010 |
| First evidence occurred | 0.024 | ||
| No evidence | 370 (67.0) | 409 (74.1) | |
| Pre-Y1 | 16 (2.9) | 21 (3.8) | |
| Pre-Y2 | 41 (7.4) | 28 (5.1) | |
| Pre-Y3 | 125 (22.6) | 94 (17.0) | |
| Glaucoma | 111 (20.1) | 75 (13.6) | 0.004 |
| Vitreous opacification | 55 (10.0) | 40 (7.2) | 0.107 |
| Blindness/loss of vision | 49 (8.9) | 43 (7.8) | 0.514 |
| Abnormal conjunctival vessels | –§ | –§ | 0.317 |
| Pupillary abnormalities | –§ | –§ | 0.179 |
| Other organ conditions, n (%) | 156 (28.3) | 85 (15.4) | <0.001 |
| First evidence occurred | <0.001 | ||
| No evidence | 396 (71.7) | 467 (84.6) | |
| Pre-Y3 | 35 (6.3) | 31 (5.6) | |
| Pre-Y2 | 45 (8.2) | 31 (5.6) | |
| Pre-Y1 | 76 (13.8) | 23 (4.2) | |
| Renal failure | 145 (26.3) | 71 (12.9) | <0.001 |
| Multiple organ dysfunction syndrome | 32 (5.8) | 32 (5.8) | 1.000 |
| Organ transplant¶ | –§ | –§ | 0.315 |
†
Matched with age, gender, and region.
‡
Included extracranial (e.g., gastrointestinal, genitourinary, retroperitoneal) and intracranial hemorrhages (e.g., intracerebral, subarachnoid, subdural).
§
Reported per Centers for Medicare & Medicaid Services cell size suppression policy (i.e., frequency <11).
¶
Included codes related to cardiac, kidney, liver, lung and pancreas transplant (including transplant status, after care, rejection, failure and complications).
ATTR: Transthyretin amyloidosis; DF: Disease free.
CV conditions
CV conditions were the most commonly seen comorbidity (92.9 vs 75.9%) in patients with ATTR in the 3 years leading to diagnosis. Dyspnea (71.6 vs 37.7%), congestive heart failure (63.0 vs 21.9%), edema (50.5 vs 21.9%), atrial fibrillation (48.4 vs 23.2%), ventricular hypertrophy (44.9 vs 14.7%), chest pain (41.8 vs 25.7%), hemorrhage (39.5 vs 29.0%), aortic stenosis (25.9 vs 15.8%), hypotension (20.7 vs 11.2%), myocardial infarction (14.5 vs 6.2%) and restrictive cardiomyopathy (11.4 vs 3.3%) were significantly more common in patients with ATTR in the 3 years before diagnosis compared with controls (Table 4). In particular, coronary artery disease, atrial fibrillation/flutter and restrictive cardiomyopathy were observed more than 2 years before ATTR diagnosis (Table 5). CV conditions in conjunction with spinal stenosis (29.4%), aortic stenosis (27.9%) and carpal tunnel syndrome (16.2%) were also observed in patients with ATTR in the 3 years leading to diagnosis (results not displayed).
| ATTR | ||
|---|---|---|
| No. of patients with event | IQM (days) | |
| Cardiovascular conditions | 513 | 966.2 |
| Coronary artery disease | 207 | 943.9 |
| Atrial fibrillation/flutter | 267 | 809.2 |
| Restrictive cardiomyopathy | 63 | 804.5 |
| Bradycardia | 131 | 744.6 |
| Dyspnea | 396 | 634.2 |
| Ischemic stroke | 43 | 591.0 |
| Aortic stenosis | 143 | 575.1 |
| Edema | 279 | 570.3 |
| Congestive heart failure | 348 | 569.2 |
| Other hemorrhages | 218 | 538.1 |
| Syncope | 93 | 482.5 |
| Chest pain | 231 | 442.2 |
| Ventricular hypertrophy | 248 | 424.6 |
| Hypotension | 114 | 394.4 |
| Hemorrhagic stroke | –‡ | 388.7 |
| Myocardial infarction | 80 | 331.3 |
| Hypertrophic cardiomyopathy | 44 | 259.0 |
†
Median values not reported per Centers for Medicare & Medicaid Services cell size suppression policy (i.e., frequency <11); interquartile means reported as a proxy of median.
‡
Reported per Centers for Medicare & Medicaid Services cell size suppression policy (i.e., frequency <11).
ATTR: Transthyretin amyloidosis; IQM: Interquartile mean.
Healthcare utilization
Analysis of healthcare utilization data showed that the occurrence of selected diagnostic testing and procedures, ED visits and hospitalizations were more frequent among patients with ATTR in the 3 years leading up to diagnosis relative to matched controls in a similar time frame (Supplementary Tables). Cardiac imaging (81.7 vs 48.2%), blood/urine examination (45.8 vs 18.3%) and nerve condition studies (19.2 vs 8.5%) were more frequent among patients with ATTR (p < 0.001); notably, echocardiogram (81.5 vs 48.2%) was the most frequently prescribed cardiac imaging modality for diagnosing CV conditions in patients with ATTR. Data concerning therapeutic procedures in the 3 years before diagnosis showed that patients with ATTR received defibrillator/pacemaker (cardiac implantable electronic device; 16.3 vs 7.2%), cardioversion (12.5 vs 2.4%) and cardiac ablation (5.1%) more frequently than matched controls (p < 0.001). Inpatient hospitalizations (54.0 vs 35.5%; p < 0.001) and ED visits (56.0 vs 43.5%; p < 0.001) during the 3 years before diagnosis were more frequent among patients with ATTR. Patients with ATTR had a greater number of physician outpatient visits (56.8 [39.9] vs 41.3 [33.6]; p < 0.001]) and prescriptions (100.0 [62.8] vs 87.4 [73.9]; p = 0.002) than matched controls in the 3 years leading to diagnosis. Additionally, CV-related inpatient hospitalizations (29.3 vs 11.4%; p < 0.001) and ED visits (22.8 vs 13.0%; p < 0.001) were more common among the patients with ATTR (Supplementary Tables).
Cumulative probability plots (Figures 1–3) show consistent results for patients with ATTR with the first occurrence of selected comorbidities and selected diagnostic testing often being early in the 3 years before diagnosis.
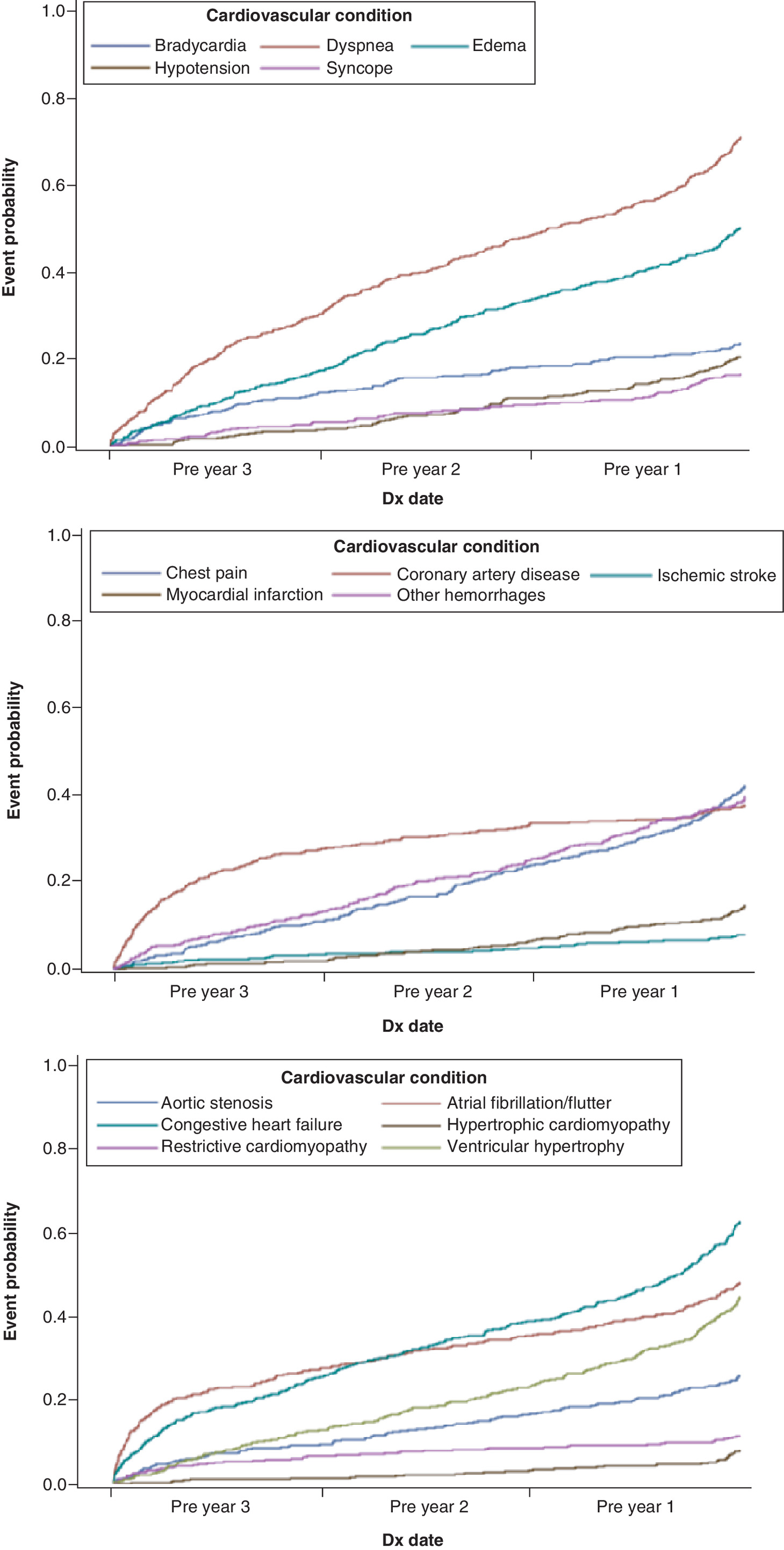
Figure 2. First observed occurrence of cardiovascular conditions† during the 3 years before transthyretin amyloidosis diagnosis.
(A) Frequency of occurrence in the years before transthyretin amyloidosis (ATTR) diagnosis of cardiovascular conditions commonly associated with ATTR. (B) Frequency relative to ischemic cardiovascular conditions. (C) Frequency for findings and conditions associated with ventricular hypertrophy.
†Hemorrhagic stroke was not plotted due to small count of patients (i.e., <11) with condition, as per the Centers for Medicare & Medicaid Services cell size suppression policy.
Dx: Diagnosis.

Figure 3. First observed occurrence of diagnostic testing during 3 years prior to transthyretin amyloidosis diagnosis.
Selected diagnostic testing is often early in the 3 years prior to diagnosis.
Dx: Diagnosis.
Discussion
ATTR is often unheeded or misdiagnosed early in its course due to its nonspecific and heterogeneous clinical presentation [27]. This retrospective analysis of Medicare health claims showed that patients with ATTR exhibit numerous symptoms and multisystem comorbidities in the 3 years before diagnosis. Many conditions and symptoms were more frequent among patients with ATTR compared with disease-free matched controls, suggesting that these comorbidities may be associated with ATTR. Patients with ATTR experienced a greater number of chronic conditions and a higher CCI score compared with matched controls, indicating the progressive nature of this condition. Analysis of healthcare utilization data also showed that patients with ATTR had more frequent diagnostic and therapeutic procedures, ED visits and hospitalizations than matched controls during a similar time frame.
In the 3 years before ATTR diagnosis, the selected conditions were more frequently observed among the patients with ATTR than matched controls. In particular, coronary artery disease, atrial fibrillation/flutter and restrictive cardiomyopathy were observed as early as 2–3 years before ATTR diagnosis. Spinal stenosis and carpal tunnel syndrome were the most commonly seen musculoskeletal comorbidities in patients with ATTR and their occurrence in combination with CV conditions was also frequently noticed.
This study provides a granular picture of the symptom burden experienced by patients with ATTR before diagnosis and may be of clinical significance for several reasons. The occurrence of the selected conditions, sometimes years before a diagnosis of ATTR, could indicate early markers of disease that, if recognized, could allow for earlier diagnosis and treatment. As prognosis is dependent on early intervention, timely diagnosis and treatment is critical. In addition, although the frequent manifestation of CV and neurologic conditions was expected, the occurrence of gastrointestinal and musculoskeletal conditions suggests the multisystem nature of clinical presentation even in earlier stages of disease. It is also important to acknowledge that diagnostic errors are common in this disease [28,29] and can lead to initiation of an inappropriate treatment in two-thirds of the patients [30]. Finally, the higher frequency of comorbid conditions and healthcare utilization (therapeutic devices, ED visits and hospitalization) in these older patients with ATTR compared with controls suggests a high disease burden associated with the condition that could potentially be attenuated with earlier diagnosis and initiation of therapy.
The findings of the present study are consistent with previously published reports. The analysis of healthcare utilization data of ATTRv patients enrolled in the APOLLO study showed that, in the year before study enrollment, patients with ATTRv averaged 7.6 visits to general practitioners (once every 7 weeks) and 8.8 visits to specialists (once every 6 weeks) [31]. Approximately 23% of patients had at least one ED visit in the year before enrollment, and 28% of patients reported at least one overnight hospitalization. Moreover, patients in later stages of disease experienced more ED visits and hospitalizations than those in earlier stages [31]. Analysis of 10-year data from the National Inpatient Sample (2005–2014) revealed 41 hospitalizations per 100,000 and longer inpatient stays (7.5 ± 9.2 days vs 6.2 ± 8.1 days, p < 0.001) in patients with a diagnosis of amyloidosis [32]. These findings indicate that ATTR presents with significant comorbidity and healthcare expenditure in the years before diagnosis.
The Transthyretin Amyloidosis Outcome Survey demonstrated widespread cardiac involvement among the patients with ATTR. Signs and symptoms of cardiac involvement were seen in 94% of patients with ATTRwt [5]. The present study showed that patients with ATTR suffered from multiple CV symptoms with twice as many inpatient hospitalizations and ED visits due to CV-related events over the 3 years before diagnosis than controls. A similar observation was made by Lane et al., who reported that ATTR-CM patients presented with a minimum of 4 years of delayed diagnosis and a median 17 healthcare encounters in the 3 years before diagnosis [7]. An international cardiac amyloidosis patient survey analyzing delays and errors in the diagnostic pathway showed that patients visited three to five physicians before a diagnosis of amyloidosis was made [28]. A 2019 analysis of the National Inpatient Sample showed that heart failure was present in 34.7% of patients with amyloidosis (p = 0.001) and was associated with higher morbidity and mortality. Moreover, that study also showed that patients with ATTR with a concomitant diagnosis of heart failure were more likely to undergo right heart catheterization, endomyocardial biopsy or have a pacemaker or defibrillator implanted [32]. In a retrospective claims analysis of commercial and Medicare supplemental databases, Reddy et al. further showed that CV procedures like electrocardiography and echocardiogram were the most common cardiac diagnostic procedures in ATTRv patients in the year after diagnosis [9].
The results presented in the current study are to be interpreted in the context of several limitations. First, the patient identification algorithm used in this study has not been validated using medical records; however, the majority of patients included in the final sample had specific codes for ATTR (E85.1, E85.2 or E85.82). Second, the 3-year look-back period limited the ability to examine earlier manifestations of disease; however, this time frame was chosen in favor of a longer look-back period that yielded a much smaller sample size. Third, the ATTR population included in the present study did not show a high frequency of ATTRwt (i.e., ~23% of those identified in 2018), as would be expected given recent availability of this diagnostic code with respect to study period; therefore, the study findings are likely more representative of patients with ATTRv than ATTRwt. Moreover, the percentage (12.1%) of African–American beneficiaries in our study, albeit higher than in the underlying population of fee-for-service Medicare beneficiaries (9.2% in 2019), was lower than expected as the V122I variant associated with African ancestry is the predominant cause of ATTRv in the USA. The observed percentage could be the result of genetics, inequality in access to genetic testing, or provider knowledge. Fourth, as new treatments have emerged since the study identification period (2016–2018), increased awareness for a more treatable condition may yield different patterns of care leading up to diagnosis. Fifth, although age of onset of ATTR amyloidosis varies among patients, the study findings may not be generalizable to patients who are younger than 68 years of age at diagnosis. Sixth, although patients with ATTR were compared with a matched reference cohort representing beneficiaries without the condition, we did not adjust for all observed differences between the groups, limiting our ability to directly link pre-diagnosis patterns with ATTR amyloidosis. Finally, claims data lack clinical information, such as genotype or severity of illness, to help further characterize patients with an ATTR diagnosis and the associated comorbidity, manifestations and patterns of care leading up to diagnosis [33].
Despite the limitations discussed, the current study presented valuable insights on the unmet needs and healthcare utilization patterns in the years before an ATTR diagnosis. The high rate of ED visits and hospitalizations over the 3 years before diagnosis points to an elevated need for acute care before diagnosis of ATTR. The overlapping symptom complex observed in the ATTR patient population can make early diagnosis challenging. Future analyses focusing on long-term healthcare utilization in the years following ATTR diagnosis are imperative to gain a comprehensive understanding of burden of illness in this population.
Conclusion
Older patients with ATTR have a highly variable symptom presentation. Multisystem involvement, particularly CV and nervous system conditions, are observed among Medicare beneficiaries as early as 3 years before diagnosis. This constellation of conditions, together with multiple physician visits, hospitalization and investigational and therapeutic procedures lead to considerable burden of illness even before a clinical diagnosis of ATTR is established. Increased awareness of characteristic signs and symptoms of ATTR, including CV-related symptoms, may lead to earlier recognition of the disease and diagnosis and timely access to disease-modifying therapies.
•
Patients with transthyretin amyloidosis (ATTR) often experience multiple clinical manifestations and symptom variability, which makes diagnosis in the early stages of the disease challenging.
•
Patients facing a delayed diagnosis of ATTR can experience symptom worsening, impaired function, poor quality of life and poorer survival due to disease progression, further resulting in higher healthcare utilization and costs.
•
This analysis utilized Medicare Research Identifiable Files (2011–2018) to examine patient clinical characteristics and healthcare utilization in the years leading up to a diagnosis of ATTR.
•
The final cohort consisted of 552 matched ATTR–control pairs, with a mean (standard deviation) age of 78.3 (6.3).
•
In the 3 years leading up to ATTR diagnosis, a statistically significant difference (p < 0.05) in the observed comorbidities was found between patients with ATTR and matched controls in cardiovascular conditions (92.9 vs 75.9%), musculoskeletal conditions (62.9 vs 42.2%), gastrointestinal conditions (49.1 vs 36.8%), metabolic conditions (46.6 vs 37.1%), nervous system conditions (37.7 vs 22.1%), ocular conditions (33.0 vs 25.9%) and organ dysfunction or failure (28.3 vs 15.4%).
•
The occurrence of selected diagnostic testing and procedures, ED visits and hospitalizations was more frequent among patients with ATTR in the 3 years leading up to diagnosis relative to matched controls in a similar time frame.
•
Results were consistent with published ATTR literature, in particular, by showing the common manifestation of cardiovascular symptoms in the early stages of disease.
•
High ATTR disease burden in the population of Medicare enrollees points to an opportunity for earlier diagnosis and intervention.
•
This study highlights the potential for earlier diagnosis of ATTR; future research on long-term healthcare utilization among patients with ATTR would add to our understanding of the burden faced by this population.
Author contributions
J Native-Nicolau, NM Fine, JT Ortiz Perez, D Brown, M Vera-Llonch: design of the work; interpretation of data; revising the work for important intellectual content; final approval. SR Reddy and E Chang: design of the work; acquisition and analysis of data; interpretation of data; drafting and revising the work for important intellectual content; final approval. MH Tarbox: acquisition of data; drafting and revising the work for important intellectual content; final approval.
Financial & competing interests disclosure
Funding for this study and publication-related fees was received from Akcea Therapeutics. D Brown and M Vera-Llonch are employees of and own stock in Ionis Pharmaceuticals Inc. SR Reddy, E Chang and MH Tarbox are employees of PHAR (Partnership Health Analytic Research), which was paid by Akcea to perform the research described in this manuscript. SR Reddy, E Chang and MH Tarbox report other from AbbVie, other from ASPC, other from Amgen, other from AstraZeneca, other from BMS, other from Boston Scientific Corporation, other from Celgene, other from Eisai, other from Ethicon, other from GRAIL, other from Helsinn, other from Illumina, other from Innovation and Value Initiative, other from Ionis, other from Jazz, other from Kite, other from Novartis, other from Otsuka, other from Pathnostics, other from PhRMA, other from Prothena, other from Sage, other from Verde Technologies, other from Genentech, Inc., other from Greenwich Biosciences, Inc., other from Mirum Pharmaceuticals, Inc., grants and other from Dompe US, Inc., other from Sanofi US Services, Inc. and other from Takeda, all outside the submitted work. JT Ortiz Perez received advisory board fees from Akcea and speaker fees for Astra-Zeneca, Boehringer and GE outside of the submitted work. J Native-Nicolau received funding for clinical trials for Pfizer, Akcea and Eidos; educational grants from Pfizer; and has been a consultant for Pfizer, Eidos, Akcea and Alnylam. NM Fine received consulting and research support from Akcea, Alnylam, Pfizer and Eidos. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplemental material.docx)
- Download
- 19.73 KB
References
1.
Sekijima Y. Transthyretin (ATTR) amyloidosis: clinical spectrum, molecular pathogenesis and disease-modifying treatments. J. Neurol. Neurosurg. Psychiatry 86(9), 1036–1043 (2015).
2.
Ihse E, Ybo A, Suhr O et al. Amyloid fibril composition is related to the phenotype of hereditary transthyretin V30M amyloidosis. J. Pathol. 216(2), 253–261 (2008).
3.
Gertz MA, Mauermann ML, Grogan M, Coelho T. Advances in the treatment of hereditary transthyretin amyloidosis: a review. Brain Behav. 9(9), e01371 (2019).
4.
Nakagawa M, Sekijima Y, Yazaki M et al. Carpal tunnel syndrome: a common initial symptom of systemic wild-type ATTR (ATTRwt) amyloidosis. Amyloid 23(1), 58–63 (2016).
5.
Coelho T, Maurer MS, Suhr OB. THAOS – The Transthyretin Amyloidosis Outcomes Survey: initial report on clinical manifestations in patients with hereditary and wild-type transthyretin amyloidosis. Curr. Med. Res. Opin. 29(1), 63–76 (2013).
6.
Swiecicki PL, Zhen DB, Mauermann ML et al. Hereditary ATTR amyloidosis: a single-institution experience with 266 patients. Amyloid 22(2), 123–131 (2015).
7.
Lane T, Fontana M, Martinez-Naharro A et al. Natural history, quality of life, and outcome in cardiac transthyretin amyloidosis. Circulation 140(1), 16–26 (2019).
8.
Ruberg FL, Grogan M, Hanna M et al. Transthyretin amyloid cardiomyopathy. J. Am. Coll. Cardiol. 73(22), 2872–2891 (2019).
9.
Reddy SR, Chang E, Tarbox MH et al. The clinical and economic burden of newly diagnosed hereditary transthyretin (ATTRv) amyloidosis: a retrospective analysis of claims data. Neurol. Ther. 9(2), 473–482 (2020).
10.
Stewart M, Shaffer S, Murphy B et al. Characterizing the high disease burden of transthyretin amyloidosis for patients and caregivers. Neurol. Ther. 7(2), 349–364 (2018).
11.
Keohane D, Schwartz J, Gundapaneni B et al. Tafamidis delays disease progression in patients with early stage transthyretin familial amyloid polyneuropathy: additional supportive analyses from the pivotal trial. Amyloid 24(1), 30–36 (2017).
12.
Maurer MS, Schwartz JH, Gundapaneni B et al. Tafamidis treatment for patients with transthyretin amyloid cardiomyopathy. N. Engl. J. Med. 379(11), 1007–1016 (2018).
13.
Benson MD, Waddington-Cruz M, Berk JL et al. Inotersen treatment for patients with hereditary transthyretin amyloidosis. N. Engl. J. Med. 379(1), 22–31 (2018).
14.
Adams D, Gonzalez-Duarte A, O'Riordan WD et al. Patisiran, an RNAi therapeutic, for hereditary transthyretin amyloidosis. N. Engl. J. Med. 379(1), 11–21 (2018).
15.
Castaño A, Helmke S, Alvarez J et al. Diflunisal for ATTR cardiac amyloidosis. Congest. Heart Fail. Greenwich Conn 18(6), 315–319 (2012).
16.
Fox JC, Hellawell JL, Rao S et al. First-in-human study of AG10, a novel, oral, specific, selective, and potent transthyretin stabilizer for the treatment of transthyretin amyloidosis: a phase 1 safety, tolerability, pharmacokinetic, and pharmacodynamic study in healthy adult volunteers. Clin. Pharmacol. Drug Dev. 9(1), 115–129 (2020).
17.
Vera-Llonch M, Reddy SR, Chang E et al. The patient journey toward a diagnosis of hereditary transthyretin (ATTRv) amyloidosis. Orphanet J. Rare Dis. 16(1), 25 (2021).
18.
Centers for Medicare & Medicaid Services. On its 50th anniversary, more than 55 million Americans covered by Medicare (2015). www.cms.gov/newsroom/press-releases/its-50th-anniversary-more-55-million-americans-covered-medicare
19.
Virnig B. Strengths and Limitations of CMS Administrative Data in Research (2018). www.resdac.org/articles/strengths-and-limitations-cms-administrative-data-research
20.
Siedelman L. Differences between RIF, LDS, and PUF Data Files (2016). www.resdac.org/articles/differences-between-rif-lds-and-puf-data-files
21.
Ghiso J, Frangione B. Cerebral amyloidosis, amyloid angiopathy, and their relationship to stroke and dementia. J. Alzheimers Dis. 3(1), 65–73 (2001).
22.
Keage HA, Carare RO, Friedland RP et al. Population studies of sporadic cerebral amyloid angiopathy and dementia: a systematic review. BMC Neurol. 9(1), 3 (2009).
23.
Chen S-J, Tsai H-H, Tsai L-K et al. Advances in cerebral amyloid angiopathy imaging. Ther. Adv. Neurol. Disord. 12, 1756286419844113 (2019).
24.
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J. Chronic Dis. 40(5), 373–383 (1987).
25.
Agency for Healthcare Research and Quality. HCUP Chronic Condition Indicator (2015). www.hcup-us.ahrq.gov/toolssoftware/chronic/chronic.jsp
26.
ResDAC, Waruiru Mburu. CMS Cell Size Suppression Policy (2017). https://resdac.org/articles/cms-cell-size-suppression-policy
27.
Nativi-Nicolau JN, Karam C, Khella S, Maurer MS. Screening for ATTR amyloidosis in the clinic: overlapping disorders, misdiagnosis, and multiorgan awareness. Heart Fail. Rev. (2021).
28.
Lousada I, Maurer MS, Warner MT et al. Amyloidosis research consortium cardiac amyloidosis survey: results from patients with AL and ATTR amyloidosis and their caregivers. J. Card. Fail. 25(8), S69 (2019).
29.
Witteles RM, Bokhari S, Damy T et al. Screening for transthyretin amyloid cardiomyopathy in everyday practice. JACC Heart Fail. 7(8), 709–716 (2019).
30.
Maurer MS, Elliott P, Comenzo R et al. Addressing common questions encountered in the diagnosis and management of cardiac amyloidosis. Circulation 135(14), 1357–1377 (2017).
31.
Schmidt H, Lin H, Agarwal S et al. Impact of hereditary transthyretin-mediated amyloidosis on use of health care services: an analysis of the APOLLO study. Presented at: The 16th International Symposium on Amyloidosis (ISA). Kumamoto, Japan, 26–29 March 2018.
32.
Sperry BW, Saeed IM, Raza S et al. Increasing rate of hospital admissions in patients with amyloidosis (from the National Inpatient Sample). Am. J. Cardiol. 124(11), 1765–1769 (2019).
33.
Tyree PT, Lind BK, Lafferty WE. Challenges of using medical insurance claims data for utilization analysis. Am. J. Med. Qual. Off. J. Am. Coll. Med. Qual. 21(4), 269–275 (2006).
Information & Authors
Information
Published In
Pages: 1031 - 1044
PubMed: 35993313
Copyright
© 2022 Jose Nativi-Nicolau. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 12 April 2022
Accepted: 29 July 2022
Published online: 22 August 2022
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Clinical manifestations and healthcare utilization before diagnosis of transthyretin amyloidosis. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0074
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Joshua D. Mitchell, Kevin M. Alexander, Hanh Dung Dao, Elizabeth Nagelhout, Neil Lamarre, Margarita Udall, Richard K. Cheng, Diagnostic Trends and Geographic Health Care Disparities Among Patients With Transthyretin Amyloid Cardiomyopathy, Journal of the American Heart Association, 10.1161/JAHA.125.048943, 15, 12, (2026).
- Kevin M. Alexander, Shun Kohsaka, Steen Hvitfeldt Poulsen, Astrid J. Terkelsen, J. Gustav Smith, Johan Sundström, Jason Wright, Krister Järbrink, Arti Gauvri Bhimjiyani, Laura Davis, Yuya Matsue, Lisa J. Anderson, Björn Pilebro, Contemporary Description of Clinical Characteristics and Outcomes in Patients with Hereditary ATTR Amyloidosis: Results from the Multicountry OverTTuRe Study, Cardiology and Therapy, 10.1007/s40119-026-00450-y, 15, 2, (201-229), (2026).
- Gabriela Spencer-Bonilla, Jun Fan, Paul Cheng, Anubodh Varshney, Natasha Din, Fatima Rodriguez, Mia A. Papas, Marie Davies, John Venditto, Joanna Huang, Ronald M. Witteles, Paul A. Heidenreich, Kevin M. Alexander, Alexander T. Sandhu, Delayed Diagnosis of Transthyretin Amyloid Cardiomyopathy in the Veterans Health Administration, JACC, 10.1016/j.jacc.2025.10.021, 87, 5, (533-545), (2026).
- Craig I. Coleman, Randy Martinez, Sophia A. Torres, Methods of identifying transthyretin amyloid cardiomyopathy in secondary data sources: a systematic review, Current Medical Research and Opinion, 10.1080/03007995.2025.2596820, 41, 11, (2013-2024), (2025).
- Noel Dasgupta, Steen Hvitfeldt Poulsen, Michele Emdin, Amrut V. Ambardekar, Keyur B. Shah, Liana Hennum, Rohit Marwah, Melissa Allison, Pruthviraj Shivanna, Suresh Siddhanti, Jean-François Tamby, Heather Falvey, Justin L. Grodin, Contemporary Oral Medication Use and Frequency in Patients with Transthyretin Amyloid Cardiomyopathy, American Journal of Cardiovascular Drugs, 10.1007/s40256-025-00752-x, 25, 6, (829-839), (2025).
- Svetlana N. Nasonova, Igor V. Zhirov, Anastasiya A. Shoshina, Yulia F. Osmolovskaya, Alexey A. Ansheles, Olga Ya. Tchaikovskaya, Svetlana V. Dobrovolskaya, Vladimir B. Sergienko, Marina A. Saidova, Sergey N. Tereshchenko, Sergey A. Boytsov, Expert Center for cardiac amyloidosis: reality and perspectives, Terapevticheskii arkhiv, 10.26442/00403660.2024.04.202677, 96, 4, (321-329), (2024).
- Loris Poli, Beatrice Labella, Stefano Cotti Piccinelli, Filomena Caria, Barbara Risi, Simona Damioli, Alessandro Padovani, Massimiliano Filosto, Hereditary transthyretin amyloidosis: a comprehensive review with a focus on peripheral neuropathy, Frontiers in Neurology, 10.3389/fneur.2023.1242815, 14, (2023).
- Efstratios A. Apostolou, Anna-Maria Fontrier, Georgios K. Efthimiadis, Efstathios Kastritis, John Parissis, Panos Kanavos, The patient pathway in ATTR-CM in Greece and how to improve it: A multidisciplinary perspective, Hellenic Journal of Cardiology, 10.1016/j.hjc.2023.05.004, 73, (73-80), (2023).