A network meta-analysis of immunotherapy-based treatments for advanced nonsquamous non-small cell lung cancer
Publication: Journal of Comparative Effectiveness Research
Abstract
Introduction: In the absence of head-to-head trials comparing immunotherapies for advanced nonsquamous non-small-cell lung cancer (NsqNSCLC), a network meta-analysis (NMA) was conducted to compare the relative efficacy of these treatments. Materials & methods: A systematic literature review of randomized controlled trials evaluating first-line-to-progression and second-line treatments for advanced NsqNSCLC informed Bayesian NMAs for overall survival (OS) and progression-free survival (PFS) end points. Results: Among first-line-to-progression treatments, pembrolizumab + pemetrexed + platinum showed the greatest OS benefit versus other regimens and a PFS benefit versus all but three regimens. Among second-line treatments, an OS benefit was seen for atezolizumab, nivolumab and pembrolizumab versus docetaxel. Conclusion: Pembrolizumab + pemetrexed + platinum showed the maximum OS benefit in the first-line setting. In the second-line setting, anti-PD-1/anti-PD-L1 monotherapies were better than docetaxel.
Lung cancer is the leading cause of cancer-related mortality worldwide [1]. Non-small-cell lung cancer (NSCLC) is a major subtype of lung cancer comprising 80–90% of all classified lung cancer cases [2]. Historically, platinum-based chemotherapy has been the standard-of-care treatment for advanced NSCLC; however, the introduction of targeted therapies and immunotherapies has changed the treatment landscape in this population [3]. Currently, platinum-based chemotherapy combined with immunotherapy is considered the standard first-line treatment option for patients with advanced NSCLC without a molecular biomarker [2]. Evidence of significantly increased survival rates with PD-1/PD-L1 inhibitors nivolumab (NIV), pembrolizumab (PEMBRO) and atezolizumab (ATEZ) compared with chemotherapy (docetaxel [DOC]) led to their approval as second-line therapies for advanced NSCLC in previously treated disease [4–7]. Subsequently, PEMBRO was approved as a single agent for the first-line treatment of patients with metastatic NSCLC whose tumors express a PD-L1 tumor proportion score (TPS) ≥50% and with no EGFR mutation or ALK gene rearrangement, based on significantly improved progression-free survival (PFS) compared with platinum-based doublet chemotherapy [8]. More recently, it was approved for the first-line treatment of patients with stage III NSCLC who are not candidates for surgical resection or definitive chemoradiation or metastatic NSCLC without EGFR or ALK genomic aberrations and with PD-L1 TPS ≥1%, based on significantly improved overall survival (OS) compared with chemotherapy [9].
Recent clinical trials have evaluated the efficacy and safety of PD-1/PD-L1 inhibitors in combination with traditional chemotherapy regimens as first-line therapy for advanced NSCLC. In the randomized, open-label, phase 2 KEYNOTE-021 Cohort G, the addition of PEMBRO to carboplatin and pemetrexed (PEM) in chemotherapy-naive patients with advanced, nonsquamous NSCLC without targetable EGFR or ALK genetic aberrations showed a significantly improved objective response rate (ORR) and prolonged PFS compared with carboplatin and PEM alone [10]. Based on these results, this PEMBRO combination was granted accelerated approval in this setting. An updated analysis showed that these significant improvements in PFS and ORR were maintained after a 24-month median follow-up [11]. Furthermore, the phase 3 KEYNOTE-189 study in patients with previously untreated metastatic NSCLC confirmed the survival benefit of PEMBRO in combination with PEM and platinum chemotherapy [12], leading to full approval of PEMBRO plus chemotherapy for first-line treatment of metastatic nonsquamous NSCLC. More recently, ATEZ in combination with bevacizumab (BEV), paclitaxel and carboplatin was approved based on findings from the phase 3 IMpower150 study [13]. Patients with metastatic nonsquamous NSCLC with no EGFR or ALK genetic aberrations treated with this ATEZ combination in the first-line setting showed significantly longer OS compared with those treated with BEV only plus chemotherapy. Additionally, immunotherapy + immunotherapy combinations such as NIV and ipilimumab (IPI) have gained first-line approval in patients with PD-L1 TPSs ≥1% without EGFR or ALK genomic aberrations based on the efficacy observed in the CHECKMATE-227 trial. Patients with PD-L1 TPSs ≥1% receiving NIV in combination with IPI experienced a statistically significant improvement in OS compared with those receiving platinum chemotherapy.
Second-line treatment options evaluated by clinical trials include PD-1/PD-L1 inhibitors (PEMBRO, NIV and ATEZ) and chemotherapy-based options such as ramucirumab (RAM) plus DOC or PEM monotherapy. DOC and RAM combination showed improved OS compared with DOC in the REVEL [14] trial. Monotherapy PEM [15] (for nonsquamous histology only) and DOC [16] have demonstrated improved OS. KEYNOTE-010 [4], a phase II/III trial, showed significantly better OS and PFS for patients randomized to the PEM arm. NIV significantly improved OS in patients with metastatic nonsquamous NSCLC in the CHECKMATE-057 [5] study. Finally, ATEZ in the OAK [7] study showed better OS compared with DOC.
The first-line and second-line treatment landscapes for nonsquamous advanced NSCLC are dynamic and rapidly evolving. Such expansion of the treatment armamentarium adds to the complexity of decision-making for healthcare practitioners and patients in this setting. The objective of this study was to identify and collate specific evidence for first-line-to-progression and second-line treatments for advanced nonsquamous NSCLC by conducting a systematic literature review (SLR) and then using those findings in a network meta-analysis (NMA) to compare treatments with regard to their relative efficacies.
Materials & methods
Systematic literature review
An SLR was conducted in accordance with the guidelines set out by the Centre for Reviews and Dissemination [17], Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement [18] and Cochrane guide for SLRs [19]. The SLR was performed to identify studies published up to 13 June 2018.
Data sources & search strategies
Searches for relevant full publications were carried out using the following electronic databases: Embase, MEDLINE and Cochrane Central Register of Controlled Trials. Full search strategies are provided in Supplementary Table 1. In addition, recent conference proceedings for the American Association for Cancer Research, European Lung Cancer Conference, World Conference on Lung Cancer, European Society for Medical Oncology (ESMO), ESMO Immuno-Oncology Congress and American Society for Clinical Oncology up to 23 July 2018 were searched to identify abstracts reporting unpublished studies of interest.
Study selection & data extraction
Study eligibility criteria were specified in terms of patients, interventions, comparators, outcomes and study design (PICOS; Supplementary Table 2 includes a full PICOS statement). The population inclusion criteria for the SLR were aimed to identify a population consisting of first-line-to-progression patients and another of second-line patients with locally advanced or metastatic nonsquamous NSCLC (stage IIIB or IV). Studies consisting of mixed squamous and nonsquamous histological populations were included if results were reported specifically for the nonsquamous NSCLC population. Exceptions were made for the CHECKMATE 227 [20], KEYNOTE-042 [9] and KEYNOTE-024 [8] studies where mixed squamous and nonsquamous efficacy data were extracted in an effort to include the best available data, despite the potential introduction of heterogeneity. Although these studies contained mixed squamous and nonsquamous efficacy data, the majority of patients were nonsquamous. Studies were included irrespective of PD-L1 expression level, whereas studies including only a mutation-positive-specific population (i.e., EGFR+, ALK+) were excluded. All abstracts and full articles were reviewed according to the eligibility criteria by two systematic reviewers; any differences in opinion were resolved through consultation with a third reviewer and a consensus was reached. From the identified eligible studies, the following data were extracted: study characteristics, patient characteristics, key inclusion/exclusion criteria, treatments, efficacy end points and safety end points. Investigator-assessed OS and PFS were the efficacy end points of interest. Where PFS was not reported in the publication, time-to-progression, event-free survival and failure-free survival data were extracted, if available; however, only studies that used PFS as a definition were considered for the NMA. All data were extracted by a single reviewer and then independently verified and validated by a second reviewer. Risk-of-bias assessments were carried out for each study reported in peer-reviewed publications according to Cochrane risk-of-bias guidance [19]. Studies were assessed on biases relating to sequence generation, allocation concealment, blinding, incomplete outcome data and selective reporting. The identified studies were categorized as follows:
•
First-line-to-progression: studies investigating the treatment of patients who had received no prior systemic therapy. As part of the treatment regimen, patients could go on to receive maintenance therapy based on their response to first-line induction treatment.
•
Second-line: studies investigating the treatment of patients who had received at least one prior systemic therapy.
Studies that only included data for first-line induction, where the treatment was not given until progression, were not included, as the treatment effect from these regimens is considered to be different from those treated until progression. Furthermore, the number of treatment cycles in the studies differed (i.e., four cycles vs a maximum number of cycles), therefore, only those studies with comparable exposure were analyzed in the first-line setting. In the current analyses, the regimens were named according to the time period of treatment given and are denoted by “i” for induction only and “c” for therapies continued from induction into maintenance.
Network meta-analysis
An NMA was conducted to assess the relative efficacy of therapies in terms of survival end points (OS and PFS). Network plots are presented for each end point to illustrate how the studies and treatments are connected. The NMA was conducted in a Bayesian framework, as recommended by the NICE Decision Support Unit (DSU) technical support documents [21] using the OpenBUGS software (London, Scotland, UK) package version 3.2.3 [22]. Fixed-effects (FE) and random-effects (RE) NMAs were conducted for each end point. Models described by Woods were used to simultaneously analyze hazard ratios (HRs) and median survival estimates reported for PFS and OS end points [21,23]. The models analyzed the data on the log-hazard scale and accounted for correlations in multiarm trials. HRs represent the relative difference in the hazard rate for each treatment compared with the reference treatment. Observed data (reported HRs and corresponding standard errors [SEs] on the log scale) were included in the model using a normal likelihood (Supplementary Materials). The deviance information criterion (DIC) and total residual deviance were used to compare the fit and complexity of the FE and RE models [24]. Markov chain Monte Carlo (MCMC) simulation was used to simulate from the posterior distributions; using two MCMC chains, this estimator was run for 100,000 burn-in simulations and monitored for a further 150,000 simulations. Convergence was assessed by a combination of visual inspection of MCMC trace, Gelman–Rubin statistics and autocorrelation diagnostic plots [22]. This Woods-based analysis assumed that the proportional hazards (PH) assumption was not violated, but this required further investigation.
Kaplan–Meier (KM) graphs (where available) for PFS and OS were digitized (via WebPlotDigitizer® software) to provide individual survival data. Survival proportions over time from these digitized data, total number of events, number of subjects and number of patients at risk by time point (where reported) were used in the algorithm developed by Guyot et al. [25] to estimate outcomes for each participant in the study (i.e., individual patient data [IPD]). The Guyot algorithm involved iteratively solving KM equations to estimate the event and censoring distribution over time to reconstruct the original KM intervals [25]. Estimated IPD were used to assess the PH assumption using log-cumulative hazard plots, Schoenfeld residual plots and the weighted residual test based on standardized Schoenfeld residuals [26]. An assessment of PH for PFS and OS end points was conducted and showed that the assumption was violated in certain studies included in the first-line-to-progression group.
To account for nonproportional hazards, the digitized KM curves were analyzed using a piecewise constant HR model following the approach developed by Lu et al. [27] This model used three time periods (0–3 months, 3–6 months and >6 months) within which the HRs were assumed to be constant. The time periods were selected based on trends observed in the studies, although the duration of the last period varied from trial to trial. A study reporting 5 months total follow-up used a piecewise constant hazard composed of 3 months of the 0–3 months period and 2 months of the 3–6 months period and did not contribute to the >6 month period. This method has been used in recent NMAs of survival data [28,29]. An additional sensitivity analysis was conducted to explore heterogeneity in the networks by analyzing a subgroup of patients considered high PD-L1 expressers (PD-L1 TPS ≥50%) in the first-line-to-progression group. The impact on the results was assessed by comparing the relative treatment effect estimates to those from the base cases.
A key assumption of NMA is that direct and indirect evidence are estimating the same parameters, meaning that the evidence is consistent. Inconsistency in an NMA occurs when the direct evidence informing a pairwise comparison differs from the indirect estimate informing the comparison. This can be caused by treatment effect modifiers or an imbalance in the distribution of treatment effect modifiers in direct and indirect evidence. Where there is a closed “loop” in the network, the indirect evidence obtained from the NMA can be compared with the direct evidence to assess inconsistency. Based on NICE DSU documents specifications, inconsistency was assessed in any given single loop using repeated application of the Bucher method [22]. This involved synthesizing the evidence for each pairwise contrast in the loop and then testing whether the direct and indirect evidence were consistent. The OS and PFS networks were assessed for inconsistency for the first-line-to-progression data. The indirect data from any two sides of a closed three-arm loop were compared with the direct evidence of the remaining side using the Bucher method since the estimate of inconsistency would be the same regardless of the sides chosen.
Results
Systematic literature review
Figure 1 summarizes the PRISMA flow diagram for the SLR. Overall, the SLR included 53 full-text articles and 13 conference abstracts, representing 50 unique studies and 16 secondary sources associated with these studies. These 50 studies comprised 29 studies that evaluated first-line-to-progression treatments and 21 studies that evaluated second-line treatments.
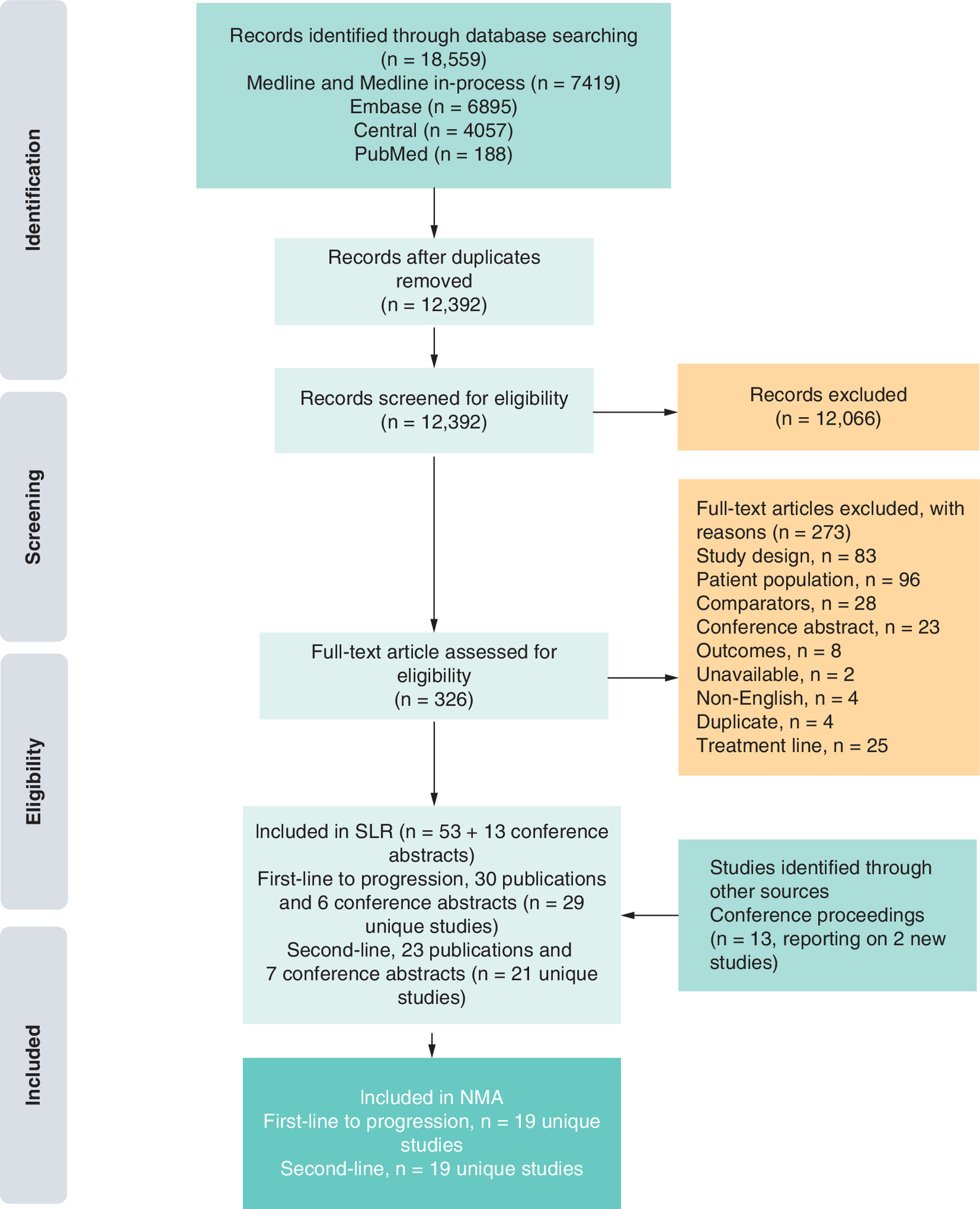
Figure 1. Preferred Reporting Items of Systematic reviews and Meta-Analyses publication screening and selection.
NMA: network meta-analysis.
First-line to progression
The characteristics of the studies in the SLR and analyzed in the NMA that evaluated first-line-to-progression treatments are presented in Table 1 [4,5,7,8,10,12–14,20,30–65]. Nineteen of the twenty-nine studies had PFS or OS data available and were connected to the network in this group (reasons for exclusion can be found in Supplementary Table 3); twelve were phase III studies and the remaining seven were phase II studies. The majority of the studies used an open-label trial design and blinding was not reported for three studies. Six studies included only patients with stage IV NSCLC, whereas the remainder included patients with stage IIIB or IV NSCLC. All studies included patients with Eastern Cooperative Oncology Group (ECOG) or WHO performance status (PS) of 0 or 1; patients with PS of 2 were included in three of the studies.
| Study ID | Primary publication | Associated publications | Clinical trial no. | Study location | Study phase | Study blinding | Eligible AJCC stage | Eligible ECOG/WHO PS | Ref. |
|---|---|---|---|---|---|---|---|---|---|
| First-line-to-progression | |||||||||
| 65Plus | 2017 | – | NCT00976456 | Germany | III | Open-label | IIIB or IV | 0–2 | [30] |
| BEYOND | 2015 | – | NCT01364012 | China | III | Double-blind | IIIB, IV or recurrent | 0–1 | [32] |
| CheckMate 227 | 2018 | – | NCT02477826 | International | III | Open-label | IV | 0–1 | [20,66] |
| Doebele | 2015 | – | NCT01160744 | Multicenter | II | Open-label | IV | 0–2 | [33] |
| ERACLE | 2015 | – | NCT01303926 | Italy | III | – | IIIB or IV | 0–1 | [34] |
| IMpower150 | 2018 | – | NCT02366143 | International | III | Open-label | IV | 0–1 | [13] |
| Johnson | 2004 | – | – | North America | II | Open-label | IIIB (pleural effusion), IV or recurrent | 0–2 | [36,67] |
| Karayama | 2016 | – | – | Japan | II | Open-label | IIIB or IV | 0–1 | [37] |
| KEYNOTE-021 | 2016 | – | NCT02039674 | US, Taiwan | II | Open-label | IIIB or IV | 0–1 | [10] |
| KEYNOTE-024 | 2016 | – | NCT02142738 | International | III | Open-label | IV | 0–1 | [8] |
| KEYNOTE-042 | 2018 | – | NCT02228094 | International | III | Open-label | – | 0–1 | [38] |
| KEYNOTE-189 | 2018 | – | NCT02578680 | International | III | Double-blind | – | 0–1 | [12,68] |
| Lee | 2016 | – | – | Korea | III | Open-label | – | 0–1 | [39,69] |
| Lynch | 2012 | – | – | International | II | Double-blind | IIIB or IV | 0–1 | [40,70] |
| Niho | 2012 | – | – | Japan | II | Open-label | IIIB (with pleural and/or pericardial effusion and/or pleural dissemination) or IV or recurrent | 0–1 | [41,71] |
| PointBreak | 2013 | – | NCT00762034 | US | III | Open-label | IIIB (with pleural effusion) or IV | 0–1 | [42] |
| PRONOUNCE | 2015 | – | NCT00948675 | US | III | Open-label | IV | 0–1 | [43,72] |
| Sandler | 2006 | – | NCT00021060 | US | III | – | IIIB or IV or recurrent | 0–1 | [44] |
| Spigel | 2018 | – | NCT00892710 | – | II | – | IV | – | [45,73] |
| Second-line | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| CheckMate 057 | 2015 | Paz-Ares ASCO 2015a | NCT01673867 | Multinational | III | Open-label | IIIB or IV or recurrent | 0–1 | [5,74,75] |
| CTONG0806 | 2014 | – | NCT00891579 | China | II | Open-label | IIIB or IV | 0–1 | [46] |
| DELTA | 2014 | – | – | Japan | III | Open-label | IIIB or IV | 0–2 | [47,76] |
| Dong | 2014 | – | – | China | II | IIIB or IV | <3 | [48] | |
| ISEL | 2005 | – | – | 28 countries across Europe, Asia, Central and South America, Australia and Canada | III | Double-blind | IIIB or IV | 0–2 | [49,77] |
| Juan | 2015 | – | – | Spain | II | Open-label | IIIB or IV | 0–2 | [50,78] |
| KEYNOTE-010 | 2016 | – | NCT01905657 | Multinational, 24 countries | II/III | Open-label | IIIB or IV | 0–1 | [4] |
| Kim | 2016 | – | NCT01783834 | Korea | II | Open-label | IIIB or IV | 0–2 | [51,79] |
| KSG-LU08-01 | 2012 | – | NCT01066195 | Korea | III | Open-label | IIIB or IV | 0–2 | [52] |
| Li | 2017 | – | NCT00950365 | US | II | – | – | 0–2 | [53] |
| LUX-Lung 5 | 2016 | Schuler ASCO 2014, Schuler ELCC 2015 | NCT01085136 | Multinational, 23 countries | III | Open-label | IIIB or IV | 0–2 | [55,56] |
| LUX-Lung 1 | 2012 | – | NCT00656136 | Multinational | IIb/III | Double-blind | IIIB or IV | 0–2 | [54] |
| OAK | 2016 | Fehrenbacher 2018 | NCT02008227 | International | III | Open-label | IIIB or IV | 0–1 | [7,57,80] |
| POPLAR | 2016 | Mazieres ELCC 2018 | NCT01903993 | International | II | Open-label | – | 0–1 | [58,59,81,82] |
| REVEL | 2014 | Paz-Ares ASCO 2015b | NCT01168973 | Multinational | III | Double-blind | IV | 0–1 | [14,83] |
| Smit | 2009 | – | – | – | II | – | IIIB or IV | 0–2 | [61] |
| TITAN | 2012 | – | NCT00556322 | Multinational, 24 countries | III | Open-label | IIIB or IV | 0–2 | [62] |
| Urata | Nishiyama ESMO 2014 | – | Multicenter; not specified | III | – | IIIB or IV or recurrent | 0–2 | [63,64,84] | |
| WJOG 5910L | 2016 | – | – | Japan | II | Open-label | IIIB or IV or recurrent | 0–2 | [65,85] |
AJCC: American Joint Committee on Cancer; ASCO: American Society of Clinical Oncology; ECOG: Eastern Cooperative Oncology Group; ELCC: European Lung Cancer Congress; ESMO: European Society for Medical Oncology; PS: Performance status.
Patient baseline characteristics were generally similar between treatment arms (Table 2). The median age at baseline ranged from 56 to 74 years. The majority of patients were men across the studies with two exceptions [11,36]. A greater proportion of patients had stage IV disease compared with stage IIIB disease in studies that included both stage IIIB and IV patients. The proportions of patients with EGFR-positive status ranged from 25.5 to 27.3% in the two studies that enrolled these patients and reported on the proportion who tested positive.
| Study ID | Interventions | n | Median age, years (range) | Female (%) | Current/previous smoker (%) | AJCC stage IV (%) | EGFR+ (%) |
|---|---|---|---|---|---|---|---|
| 65Plus | BEVc + PEMc | 135 | 71 (65–86) | 38 | 73 | 95 | – |
| BEVc + PEMc + PLATi | 136 | 72 (65–86) | 36 | 81 | 96 | – | |
| BEYOND | BEVc + PACi + PLATi | 138 | 57 (30–75) | 46 | – | 91 | 27 |
| PACi + PLATi | 138 | 56 (23–74) | 44 | – | 91 | 26 | |
| CheckMate 227 | IPIc + NIVc | – | 64 (41–87) | 30 | 94 | – | – |
| PEMc + PLATi | – | 64 (29–80) | 34 | 91 | – | – | |
| Doebele (2015) | PEMc + PLATi | 71 | – | 37 | 78 | 100 | – |
| PEMc + PLATi + RAMc | 69 | – | 48 | 84 | 100 | – | |
| ERACLE | PEMc + PLATi | 60 | 60 (35–72) | 30 | 70 | 95 | 0 |
| BEVc + PACi + PLATi | 58 | 62 (41–71) | 22 | 60 | 93 | 0 | |
| IMpower150 | ATEZc + BEVc + PACi + PLATi | 400 | 63 (31–89) | 40 | 80 | – | – |
| BEVc + PACi + PLATi | 400 | 63 (31–90) | 40 | 81 | – | – | |
| Johnson (2004) | PACi + PLATi | 32 | – | 25‡ | – | – | – |
| BEVc +PACi + PLATi | 32 | – | 38‡ | – | – | – | |
| BEVc + PACi + PLATi | 35 | – | 54‡ | – | – | – | |
| Karayama (2016) KEYNOTE-021 | BEVc + PEMc + PLATi | 55 | 65 (39–75) | 36 | 66 | 86 | 27 |
| BEVi + PEMc + PLATi | 55 | 66 (50–75) | 29 | 76 | 87 | 26 | |
| PEMc + PEMBROc + PLATi | 60 | 61.8 | 63 | 75 | 98 | 0 | |
| PEMc + PLATi | 63 | – | 59 | 86 | 95 | 0 | |
| KEYNOTE-024 | PEMBROc | 154 | – | 40 | 97 | – | – |
| (GEMi or PACi or PEMc) + PLATi | 151 | – | 37 | 87 | – | – | |
| KEYNOTE-042 | PEMBROc | – | 63 (25–89) | 29 | 78 | – | – |
| PEMc + PLATi | – | 63 (31–90) | 29 | 78 | – | – | |
| KEYNOTE-189 | PEMc + PEMBROc + PLATi | 410 | 65 (34–84) | 38 | 88 | – | – |
| PEMc + PLATi | 206 | 64 (34–84) | 47 | 88 | – | – | |
| Lee (2016) | PEMc + PLATi | – | 74‡ (70–86) | 35‡ | – | – | – |
| PEMc | – | 74‡ (70–86) | 35‡ | – | – | – | |
| Lynch (2012) | PACi + PLATi | 66 | – | 54 | – | 74 | – |
| IPIc + PACi + PLATi | 70 | – | 58 | – | 84 | – | |
| IPIc + PACi + PLATi | 68 | – | 56 | – | 90 | – | |
| Niho (2012) | PACi + PLATi | 59 | 60 (30–73) | 36 | 68 | 71 | – |
| BEVc + PACi + PLATi | 121 | 61 (34–74) | 36 | 69 | 69 | – | |
| PointBreak | BEVc + PEMc + PLATi | 472 | 65 | 47 | 89 | 90 | – |
| BEVc + PACi + PLATi | 467 | 65 | 47 | 88 | 90 | – | |
| PRONOUNCE | PEMc + PLATi | 182 | 66§ (38–84) | 42 | 90 | 100 | – |
| BEVc + PACi + PLATi | 179 | 65 (41–86) | 47 | 96 | 100 | – | |
| Sandler (2006) | PACi + PLATi | 444 | – | 42 | – | 78 | – |
| BEVc + PACi + PLATi | 434 | – | 50 | – | 74 | – | |
| Spigel (2018) | PEMc | 48 | 72 (51–84) | 38 | 96 | 90 | – |
| BEVc + PEMc | 63 | 72 (50–90) | 43 | 95 | 92 | – | |
| BEVc + PEMc + PLATi | 61 | 73 (48–90) | 44 | 91 | 97 | – |
Carboplatin and cisplatin were pooled as PLAT as their efficacies were considered similar.
†
Baseline characteristics for whole study population including squamous and nonsquamous NSCLC.
‡
Calculated figure.
§
Some patients had missing values.
AJCC: American Joint Committee on Cancer; ATEZ: Atezolizumab; BEV: Bevacizumab; c: Continuous; GEM: Gemcitabine; i: Induction; IPI: Ipilimumab; NIV: Nivolumab; PAC: Paclitaxel; PEM: Pemetrexed; PEMBRO: Pembrolizumab; PLAT: Platinum; RAM: Ramucirumab.
Second-line
Characteristics of the studies in the SLR and analyzed in the NMA that evaluated second-line treatments are presented in Table 1. Nineteen of the twenty-one studies identified had available PFS or OS data and were connected to the network in this group (reasons for exclusion can be found in Supplementary Table 4). Eight studies were phase III, nine were phase II and two were phase II/III. Of the 14 studies that reported the blinding status of the study, 11 had an open-label design and three were double-blinded. All studies included patients with stage IIIB or IV NSCLC except the REVEL trial [14], which included only patients with stage IV NSCLC. Only patients with ECOG/WHO PS of 0 or 1 were eligible for inclusion in six studies, whereas all other studies included patients with PS of 0–2. The ISEL trial [49] also included patients with a PS of 3 if the investigator believed that the poor PS was not predominantly due to comorbidities.
Patient baseline characteristics were generally comparable between treatment arms (Table 3). The median age at baseline was similar across studies ranging between 56 and 68 years. The majority of participants were male in all studies except four. All studies that included stage IIIB and IV patients had a higher proportion of patients with stage IV (69–96%) than stage IIIB disease. The REVEL trial was the only study that included only stage IV patients [14]. The EGFR status of patients was reported in the majority of studies; the LUX-Lung 1 [54] and WJOG 5108L [63] studies had >66% of patients with EGFR-positive mutations. Only the CheckMate 057 [5] and KEYNOTE-010 [4] trials reported the number of patients with ALK-positive mutations (1–4%).
| Study ID | Interventions | n | Median age, years (range) | Female (%) | Current/previous smoker (%) | AJCC stage IV (%) | EGFR+ (%) |
|---|---|---|---|---|---|---|---|
| CheckMate 057 | NIV | 292 | 61 (37–84) | 48 | 79 | 93 | 15 |
| DOC | 290 | 64 (21–85) | 42 | 78 | 92 | 13 | |
| CTONG0806 | PEM | 80 | 56 (24–75) | 38 | 42 | 87 | 0 |
| GEF | 81 | 58 (27–78) | 33 | 59 | 95 | 0 | |
| DELTA | ERL | 150 | 68 (37–82) | 28 | 74 | 80 | – |
| DOC | 151 | 67 (31–85) | 29 | 76 | 81 | – | |
| Dong (2014) | PEM | 54 | – | 57 | – | 89 | – |
| DOC | 55 | – | 58 | – | 91 | – | |
| ISEL | GEF | 1129 | 62 (28–90) | 33 | 78 | 93 | – |
| PCB | 563 | 61 (31–87) | 33 | 78 | 79 | – | |
| Juan (2015) | DOC + ERL | 34 | 58 | 6 | 94 | 80 | – |
| ERL | 36 | 64 | 17 | 94 | 91 | – | |
| KEYNOTE-010 | PEMBRO | 345 | 63 | 38† | 81 | 83 | – |
| PEMBRO | 346 | 63 | 38† | 82 | – | 8 | |
| DOC | 343 | 62 | 39† | 78 | – | 9 | |
| Kim (2016) | PEM | 47 | 64 (31–81) | 30 | 70 | 94 | 2 |
| GEF | 48 | 67 (42–82) | 27 | 69 | 96 | 2 | |
| KSG-LU08-01 | GEF | 71 | 58 (40–77) | 85 | – | 91 | – |
| PEM | 70 | 64 (30–78) | 85 | – | 91 | – | |
| Li (2017) | PEM | 27 | 64 (47–91) | 48 | – | – | 8 |
| PEM + ERL | 52 | 62 (37–86) | 55 | – | – | 0 | |
| LUX-Lung 1 | AFT | 390 | 58 (30–85) | 59 | 37 | – | 14 |
| PCB | 195 | 59 (32–82) | 60 | 38 | 96 | 67 | |
| NVALT-10 | ERL | 115 | 64 (38–81) | 35 | 85 | 96 | – |
| ERL + PEM | 116 | 63 (40–82) | 37 | 84 | 75 | – | |
| OAK | ATEZ | 613 | 63 (33–82) | 39 | 80 | 81 | 0 |
| DOC | 612 | 64 (34–85) | 39 | 83 | – | 10 | |
| POPLAR | ATEZ | 144 | 62 (42–82) | 35 | 81 | – | 10 |
| DOC | 143 | 62 (36–84) | 47 | 80 | – | 12 | |
| REVEL | DOC + RAM | 628 | 62 (21–85) | 37 | 81 | – | 10 |
| DOC + PCB | 625 | 61 (25–86) | 63 | 74 | 100 | 2 | |
| Smit (2009) | PEM | 121 | 59 (36–78) | 36 | – | 100 | 3 |
| PEM + PLAT | 119 | 59 (39–84) | 38 | – | 77 | – | |
| TITAN | ERL | 203 | 59 (36–80) | 21 | 85 | 77 | – |
| DOC or PEM | 221 | 59 (22–79) | 28 | 80 | 80 | 4 | |
| Urata (2016) | ERL | 281 | 67 (39–85) | 54 | 50 | 77 | 8 |
| GEF | 280 | 68 (34–91) | 55 | 50 | 69 | 65 | |
| WJOG 5910L | DOC | 50 | - (40–84) | 34 | 76 | 88 | 16 |
| DOC+BEV | 50 | - (36–78) | 36 | 78 | 82 | 10 |
Carboplatin and cisplatin were pooled as PLAT as their efficacies were considered similar.
†
Calculated figure.
AFT: Afatinib; AJCC: American Joint Committee on Cancer; ATEZ: Atezolizumab; BEV: Bevacizumab; DOC: Docetaxel; ERL: Erlotinib; GEF: Gefitinib; NIV: Nivolumab; PCB: Placebo; PEM: Pemetrexed; PEMBRO: Pembrolizumab; PLAT: Platinum; RAM: Ramucirumab.
Network meta-analysis
All studies from the SLR that investigated first-line-to-progression or second-line treatments were considered for inclusion in the NMA. However, stricter eligibility criteria for the NMA around the PFS definition resulted in several further exclusions (Supplementary Tables 3 & 4). In addition, studies that were included in the SLR but were not connected to the evidence network were not included in the NMA. Input data used for the NMA are presented in Supplementary Tables 5–10. For both RE and FE models, the DICs and point estimates were similar; however, wider credible intervals were observed for the RE model. Convergence of RE models was poor based on visual assessment of trace, Gelman–Rubin and autocorrelation diagnostic plots. Under the RE model, the heterogeneity standard deviation in the overall population OS was 0.08 and PFS was 0.18 on the log-hazard ratio scale, indicating very low heterogeneity (Supplementary Table 11). Fixed effects results are therefore presented in this paper and random effects results are available in Supplementary Tables 12–13, 17, 19–21.
First-line to progression
The network for the 18 studies included in the OS analysis for first-line-to-progression treatment is illustrated in Supplementary Figure 1. The pairwise HR data for all treatments show that the combination of PEM plus PEMBRO plus platinum chemotherapy in the induction phase, followed by PEM and PEMBRO until progression (PEMc + PEMBROc + PLATi) was associated with a lower hazard of death compared with all included treatments (Table 4).
| PEMc + PLATi | ATEZc + BEVc + PACi + PLATi | BEVc + PACi + PLATi | BEVc + PEMc | BEVc + PEMc + PLATi | BEVi + PEMc + PLATi | IPIc + PACi + PLATi | PACi + PLATi | PEMBROc | PEMc | PEMc + PEMBROc + PLATi | PEMc + PLATi + RAMc | (GEMi or PACi or PEMc) + PLATi | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PEMc + PLATi | 1.29 (0.97,1.72) | 1.01 (0.83,1.23) | 0.89 (0.63,1.24) | 1 (0.79,1.26) | 0.87 (0.47,1.61) | 0.75 (0.45,1.25) | 0.79 (0.63,1.01) | 1.16 (0.97,1.39) | 0.92 (0.69,1.21) | 1.99 (1.57,2.52) | 0.97 (0.7,1.35) | 0.73 (0.51,1.06) | |
| ATEZc + BEVc + PACi + PLATi | 0.77 (0.58,1.03) | 0.78 (0.64,0.96) | 0.69 (0.48,0.98) | 0.77 (0.6,0.99) | 0.67 (0.36,1.25) | 0.58 (0.35,0.97) | 0.62 (0.48,0.78) | 0.9 (0.64,1.26) | 0.71 (0.5,1.02) | 1.54 (1.07,2.23) | 0.75 (0.49,1.16) | 0.57 (0.36,0.91) | |
| BEVc + PACi + PLATi | 0.99 (0.81,1.21) | 1.28 (1.05,1.57) | 0.88 (0.65,1.18) | 0.99 (0.85,1.14) | 0.86 (0.48,1.55) | 0.74 (0.46,1.19) | 0.79 (0.69,0.9) | 1.15 (0.88,1.51) | 0.91 (0.68,1.22) | 1.98 (1.45,2.69) | 0.96 (0.66,1.41) | 0.73 (0.48,1.11) | |
| BEVc + PEMc | 1.13 (0.81,1.58) | 1.46 (1.02,2.08) | 1.14 (0.85,1.53) | 1.12 (0.86,1.47) | 0.98 (0.52,1.84) | 0.85 (0.48,1.48) | 0.9 (0.65,1.24) | 1.31 (0.9,1.92) | 1.03 (0.73,1.47) | 2.25 (1.5,3.38) | 1.1 (0.69,1.75) | 0.83 (0.5,1.36) | |
| BEVc + PEMc + PLATi | 1 (0.79,1.27) | 1.3 (1.01,1.66) | 1.01 (0.88,1.17) | 0.89 (0.68,1.16) | 0.87 (0.49,1.54) | 0.75 (0.46,1.24) | 0.8 (0.66,0.97) | 1.17 (0.87,1.57) | 0.92 (0.68,1.24) | 2 (1.43,2.79) | 0.98 (0.65,1.46) | 0.74 (0.47,1.14) | |
| BEVi + PEMc + PLATi | 1.15 (0.62,2.14) | 1.49 (0.8,2.78) | 1.16 (0.64,2.09) | 1.02 (0.54,1.92) | 1.15 (0.65,2.03) | 0.86 (0.41,1.83) | 0.92 (0.5,1.68) | 1.34 (0.71,2.55) | 1.06 (0.55,2.02) | 2.3 (1.19,4.44) | 1.12 (0.56,2.26) | 0.85 (0.41,1.74) | |
| IPIc + PACi + PLATi | 1.34 (0.8,2.23) | 1.73 (1.03,2.89) | 1.35 (0.84,2.16) | 1.18 (0.68,2.07) | 1.33 (0.81,2.18) | 1.16 (0.55,2.47) | 1.06 (0.67,1.68) | 1.55 (0.9,2.68) | 1.22 (0.7,2.14) | 2.66 (1.51,4.68) | 1.3 (0.71,2.38) | 0.98 (0.52,1.84) | |
| PACi + PLATi | 1.26 (0.99,1.59) | 1.63 (1.28,2.07) | 1.27 (1.11,1.44) | 1.11 (0.81,1.54) | 1.25 (1.03,1.52) | 1.09 (0.6,1.99) | 0.94 (0.6,1.49) | 1.46 (1.09,1.97) | 1.15 (0.83,1.59) | 2.5 (1.79,3.5) | 1.22 (0.82,1.83) | 0.92 (0.59,1.43) | |
| PEMBROc | 0.86 (0.72,1.03) | 1.11 (0.79,1.55) | 0.87 (0.66,1.13) | 0.76 (0.52,1.11) | 0.86 (0.64,1.15) | 0.75 (0.39,1.42) | 0.64 (0.37,1.11) | 0.68 (0.51,0.92) | 0.79 (0.57,1.1) | 1.71 (1.27,2.3) | 0.84 (0.58,1.21) | 0.63 (0.46,0.87) | |
| PEMc | 1.09 (0.83,1.44) | 1.41 (0.98,2.02) | 1.1 (0.82,1.48) | 0.97 (0.68,1.37) | 1.09 (0.81,1.47) | 0.95 (0.5,1.81) | 0.82 (0.47,1.43) | 0.87 (0.63,1.2) | 1.27 (0.91,1.77) | 2.17 (1.51,3.13) | 1.06 (0.69,1.63) | 0.8 (0.5,1.27) | |
| PEMc + PEMBROc + PLATi | 0.5 (0.4,0.64) | 0.65 (0.45,0.94) | 0.51 (0.37,0.69) | 0.45 (0.3,0.67) | 0.5 (0.36,0.7) | 0.44 (0.22,0.84) | 0.38 (0.21,0.66) | 0.4 (0.29,0.56) | 0.58 (0.43,0.79) | 0.46 (0.32,0.66) | 0.49 (0.33,0.73) | 0.37 (0.24,0.57) | |
| PEMc + PLATi + RAMc | 1.03 (0.74,1.43) | 1.33 (0.86,2.05) | 1.04 (0.71,1.52) | 0.91 (0.57,1.45) | 1.02 (0.69,1.53) | 0.89 (0.44,1.8) | 0.77 (0.42,1.42) | 0.82 (0.55,1.23) | 1.2 (0.83,1.74) | 0.94 (0.61,1.44) | 2.05 (1.37,3.06) | 0.75 (0.46,1.24) | |
| (GEMi or PACi or PEMc) + PLATi | 1.36 (0.94,1.98) | 1.76 (1.1,2.81) | 1.37 (0.9,2.1) | 1.21 (0.73,1.99) | 1.36 (0.88,2.11) | 1.18 (0.58,2.43) | 1.02 (0.54,1.93) | 1.08 (0.7,1.69) | 1.59 (1.15,2.2) | 1.25 (0.79,1.98) | 2.71 (1.75,4.21) | 1.32 (0.81,2.17) |
HRs are provided for treatments specified in column 1 (in rows) vs the treatments in subsequent columns; HRs <1 show better survival of the treatments in column 1; carboplatin and cisplatin were pooled as PLAT as their efficacies were considered similar.
ATEZ: Atezolizumab; BEV: Bevacizumab; c: Continuous; GEM: Gemcitabine; HR: Hazard ratio; i: Induction; IPI: Ipilimumab; PAC: Paclitaxel; PEM: Pemetrexed; PEMBRO: Pembrolizumab; PLAT: Platinum; RAM: Ramucirumab.
The network for the 18 studies in the PFS analysis for first-line-to-progression treatment is illustrated in Supplementary Figure 2. The pairwise HR results showed that treatment with PEMc + PEMBROc + PLATi had a lower hazard of progression or death compared with all included treatments except the following three regimens: ATEZ + BEV + PAC + platinum chemotherapy in the induction phase followed by ATEZ and BEV until progression (ATEZc + BEVc + PACi + PLATi); IPI + NIV until progression (IPIc + NIVc); and PEM + platinum chemotherapy + RAM in the induction phase followed by PEM and RAM until progression (PEMc + PLATi + RAMc; Table 5).
| PEMc + PLATi | ATEZc + BEVc + PACi + PLATi | BEVc + PACi + PLATi | BEVc + PEMc | BEVc + PEMc + PLATi | BEVi + PEMc + PLATi | IPIc + NIVc | IPIc + PACi + PLATi | PACi + PLATi | PEMBROc | PEMc | PEMc + PEMBROc + PLATi | PEMc + PLATi + RAMc | (GEMi or PACi or PEMc) + PLATi | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PEMc + PLATi | 1.61 (1.25,2.09) | 1 (0.83,1.21) | 0.96 (0.71,1.3) | 1.22 (0.97,1.53) | 0.89 (0.51,1.54) | 1.82 (1.25,2.64) | 0.71 (0.44,1.15) | 0.6 (0.48,0.76) | 0.93 (0.82,1.06) | 0.82 (0.65,1.04) | 1.92 (1.6,2.3) | 1.33 (0.97,1.83) | 0.51 (0.36,0.73) | |
| ATEZc + BEVc + PACi + PLATi | 0.62 (0.48,0.8) | 0.62 (0.52,0.74) | 0.59 (0.43,0.82) | 0.75 (0.6,0.95) | 0.55 (0.32,0.95) | 1.13 (0.72,1.78) | 0.44 (0.27,0.71) | 0.37 (0.3,0.46) | 0.58 (0.43,0.77) | 0.51 (0.37,0.7) | 1.19 (0.87,1.63) | 0.83 (0.55,1.24) | 0.32 (0.21,0.49) | |
| BEVc + PACi+ PLATi | 1 (0.83,1.21) | 1.61 (1.35,1.92) | 0.96 (0.74,1.25) | 1.22 (1.05,1.41) | 0.89 (0.53,1.49) | 1.82 (1.2,2.76) | 0.71 (0.46,1.11) | 0.6 (0.53,0.68) | 0.93 (0.74,1.17) | 0.82 (0.63,1.07) | 1.92 (1.47,2.49) | 1.33 (0.92,1.92) | 0.51 (0.34,0.77) | |
| BEVc + PEMc | 1.04 (0.77,1.41) | 1.68 (1.22,2.31) | 1.04 (0.8,1.36) | 1.27 (1.01,1.6) | 0.93 (0.54,1.61) | 1.9 (1.17,3.06) | 0.74 (0.44,1.25) | 0.63 (0.47,0.84) | 0.97 (0.7,1.35) | 0.86 (0.62,1.18) | 2 (1.4,2.85) | 1.39 (0.9,2.15) | 0.54 (0.34,0.86) | |
| BEVc + PEMc + PLATi | 0.82 (0.66,1.03) | 1.33 (1.05,1.66) | 0.82 (0.71,0.95) | 0.79 (0.63,0.99) | 0.73 (0.44,1.2) | 1.49 (0.96,2.31) | 0.59 (0.37,0.93) | 0.49 (0.41,0.6) | 0.77 (0.59,0.99) | 0.68 (0.51,0.89) | 1.57 (1.18,2.1) | 1.1 (0.74,1.61) | 0.42 (0.28,0.64) | |
| BEVi + PEMc + PLATi | 1.12 (0.65,1.94) | 1.81 (1.05,3.13) | 1.12 (0.67,1.89) | 1.08 (0.62,1.87) | 1.37 (0.83,2.25) | 2.04 (1.05,3.96) | 0.8 (0.4,1.59) | 0.68 (0.4,1.15) | 1.05 (0.6,1.84) | 0.92 (0.52,1.63) | 2.15 (1.21,3.84) | 1.5 (0.8,2.82) | 0.58 (0.3,1.11) | |
| IPIc + NIVc | 0.55 (0.38,0.8) | 0.89 (0.56,1.4) | 0.55 (0.36,0.84) | 0.53 (0.33,0.85) | 0.67 (0.43,1.04) | 0.49 (0.25,0.95) | 0.39 (0.21,0.72) | 0.33 (0.21,0.51) | 0.51 (0.35,0.76) | 0.45 (0.29,0.7) | 1.06 (0.7,1.6) | 0.73 (0.45,1.19) | 0.28 (0.17,0.47) | |
| IPIc + PACi + PLATi | 1.4 (0.87,2.28) | 2.26 (1.4,3.65) | 1.4 (0.9,2.19) | 1.35 (0.8,2.26) | 1.71 (1.07,2.73) | 1.25 (0.63,2.47) | 2.55 (1.38,4.69) | 0.84 (0.55,1.29) | 1.31 (0.8,2.16) | 1.15 (0.69,1.94) | 2.69 (1.6,4.51) | 1.87 (1.05,3.33) | 0.72 (0.4,1.31) | |
| PACi + PLATi | 1.66 (1.32,2.09) | 2.68 (2.16,3.33) | 1.66 (1.46,1.89) | 1.59 (1.19,2.14) | 2.02 (1.67,2.45) | 1.48 (0.87,2.52) | 3.02 (1.95,4.68) | 1.18 (0.77,1.81) | 1.55 (1.2,2.02) | 1.37 (1.02,1.84) | 3.19 (2.38,4.27) | 2.22 (1.5,3.27) | 0.85 (0.56,1.3) | |
| PEMBROc | 1.07 (0.94,1.21) | 1.73 (1.29,2.31) | 1.07 (0.85,1.35) | 1.03 (0.74,1.42) | 1.3 (1.01,1.69) | 0.95 (0.54,1.67) | 1.95 (1.31,2.88) | 0.76 (0.46,1.26) | 0.64 (0.5,0.84) | 0.88 (0.68,1.15) | 2.05 (1.64,2.57) | 1.43 (1.02,2) | 0.55 (0.39,0.77) | |
| PEMc | 1.22 (0.96,1.53) | 1.96 (1.42,2.7) | 1.22 (0.93,1.58) | 1.17 (0.85,1.6) | 1.48 (1.13,1.94) | 1.08 (0.61,1.91) | 2.21 (1.42,3.43) | 0.87 (0.52,1.45) | 0.73 (0.54,0.98) | 1.14 (0.87,1.48) | 2.33 (1.73,3.14) | 1.62 (1.09,2.4) | 0.62 (0.41,0.96) | |
| PEMc+ PEMBROc+ PLATi | 0.52 (0.43,0.63) | 0.84 (0.61,1.16) | 0.52 (0.4,0.68) | 0.5 (0.35,0.71) | 0.63 (0.48,0.85) | 0.46 (0.26,0.83) | 0.95 (0.63,1.43) | 0.37 (0.22,0.62) | 0.31 (0.23,0.42) | 0.49 (0.39,0.61) | 0.43 (0.32,0.58) | 0.7 (0.48,1) | 0.27 (0.18,0.4) | |
| PEMc + PLATi + RAMc | 0.75 (0.55,1.03) | 1.21 (0.8,1.82) | 0.75 (0.52,1.08) | 0.72 (0.47,1.11) | 0.91 (0.62,1.34) | 0.67 (0.35,1.25) | 1.36 (0.84,2.21) | 0.53 (0.3,0.95) | 0.45 (0.31,0.67) | 0.7 (0.5,0.98) | 0.62 (0.42,0.91) | 1.44 (1,2.07) | 0.39 (0.24,0.62) | |
| (GEMi or PACi or PEMc) + PLATi | 1.94 (1.36,2.78) | 3.14 (2.02,4.87) | 1.95 (1.3,2.91) | 1.87 (1.17,2.97) | 2.37 (1.55,3.61) | 1.73 (0.9,3.32) | 3.54 (2.11,5.91) | 1.39 (0.76,2.53) | 1.17 (0.77,1.78) | 1.82 (1.3,2.54) | 1.6 (1.04,2.45) | 3.73 (2.5,5.57) | 2.59 (1.61,4.17) |
HRs are provided for treatments specified in column 1 (in rows) vs the treatments in subsequent columns; HRs <1 shows better survival of the treatments in column 1; carboplatin and cisplatin were pooled as PLAT as their efficacies were considered similar.
ATEZ: Atezolizumab; BEV: Bevacizumab; c: Continuous; GEM: Gemcitabine; HR: Hazard ratio; i: Induction; IPI: Ipilimumab; NIV: Nivolumab; PAC: Paclitaxel; PEM: Pemetrexed; PEMBRO: Pembrolizumab; PLAT: Platinum; RAM: Ramucirumab.
Second-line
Thirteen studies for OS and nine studies for PFS contributed to the analyses for second-line treatment. The pairwise HR results for OS showed a benefit for ATEZ, NIV and PEMBRO monotherapies compared with DOC. Additionally, PEMBRO monotherapy resulted in longer OS compared with AFT monotherapy (Table 6). PFS benefit was observed for PEM + PLAT compared with PEM monotherapy and GEF monotherapy. PEMBRO monotherapy also showed lower PFS compared with GEF monotherapy (Table 7).
| PEM | AFT | ATEZ | BEV + DOC | DOC | DOC/PEM | ERL | ERL + PEM | GEF | NIV | PCB | PEMBRO | RAM + DOC | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PEM | 0.7 (0.47,1.02) | 1.39 (0.78,2.42) | 1.37 (0.66,2.79) | 1.01 (0.58,1.72) | 0.88 (0.57,1.36) | 0.93 (0.68,1.27) | 1.27 (0.84,1.91) | 0.9 (0.7,1.15) | 1.35 (0.75,2.37) | 0.75 (0.55,1.03) | 1.61 (0.88,2.86) | 1.22 (0.69,2.12) | |
| AFT | 1.43 (0.98,2.11) | 1.99 (1,3.94) | 1.96 (0.87,4.42) | 1.45 (0.74,2.81) | 1.26 (0.79,2.03) | 1.33 (0.92,1.91) | 1.82 (1.13,2.94) | 1.28 (0.96,1.72) | 1.94 (0.97,3.84) | 1.08 (0.86,1.35) | 2.31 (1.14,4.63) | 1.75 (0.88,3.44) | |
| ATEZ | 0.72 (0.41,1.28) | 0.5 (0.25,1) | 0.99 (0.6,1.63) | 0.73 (0.62,0.86) | 0.63 (0.31,1.31) | 0.67 (0.35,1.29) | 0.91 (0.46,1.85) | 0.65 (0.35,1.21) | 0.97 (0.76,1.25) | 0.54 (0.29,1.04) | 1.16 (0.87,1.54) | 0.88 (0.7,1.11) | |
| BEV + DOC | 0.73 (0.36,1.51) | 0.51 (0.23,1.16) | 1.01 (0.61,1.68) | 1 (1,1) | 0.74 (0.46,1.19) | 0.64 (0.28,1.5) | 0.68 (0.31,1.49) | 0.93 (0.41,2.13) | 0.65 (0.31,1.41) | 0.99 (0.59,1.64) | 0.55 (0.25,1.21) | 1.17 (0.69,1.99) | 0.89 (0.54,1.47) |
| DOC | 0.99 (0.58,1.71) | 0.69 (0.36,1.35) | 1.37 (1.16,1.62) | 1.35 (0.84,2.17) | 1 (1,1) | 0.87 (0.44,1.76) | 0.91 (0.49,1.73) | 1.25 (0.64,2.49) | 0.88 (0.49,1.63) | 1.33 (1.11,1.6) | 0.74 (0.4,1.4) | 1.59 (1.26,2) | 1.2 (1.03,1.41) |
| DOC/PEM | 1.14 (0.73,1.76) | 0.79 (0.49,1.27) | 1.58 (0.76,3.21) | 1.55 (0.67,3.6) | 1.15 (0.57,2.3) | 1 (1,1) | 1.05 (0.78,1.43) | 1.44 (0.91,2.29) | 1.02 (0.7,1.48) | 1.53 (0.74,3.14) | 0.85 (0.56,1.3) | 1.83 (0.87,3.79) | 1.39 (0.67,2.82) |
| ERL | 1.08 (0.79,1.48) | 0.75 (0.52,1.08) | 1.5 (0.78,2.85) | 1.48 (0.67,3.22) | 1.09 (0.58,2.03) | 0.95 (0.7,1.29) | 1 (1,1) | 1.37 (0.97,1.93) | 0.97 (0.78,1.2) | 1.46 (0.75,2.78) | 0.81 (0.61,1.08) | 1.74 (0.88,3.36) | 1.32 (0.69,2.5) |
| ERL + PEM | 0.79 (0.52,1.19) | 0.55 (0.34,0.89) | 1.09 (0.54,2.19) | 1.08 (0.47,2.46) | 0.8 (0.4,1.57) | 0.69 (0.44,1.1) | 0.73 (0.52,1.03) | 1 (1,1) | 0.71 (0.48,1.03) | 1.07 (0.52,2.14) | 0.59 (0.39,0.91) | 1.27 (0.61,2.59) | 0.96 (0.48,1.92) |
| GEF | 1.12 (0.87,1.44) | 0.78 (0.58,1.04) | 1.55 (0.83,2.85) | 1.53 (0.71,3.25) | 1.13 (0.61,2.03) | 0.98 (0.68,1.43) | 1.03 (0.84,1.28) | 1.42 (0.97,2.07) | 1 (1,1) | 1.51 (0.8,2.79) | 0.84 (0.7,1.01) | 1.8 (0.94,3.37) | 1.36 (0.73,2.5) |
| NIV | 0.74 (0.42,1.32) | 0.52 (0.26,1.03) | 1.03 (0.8,1.32) | 1.01 (0.61,1.69) | 0.75 (0.62,0.9) | 0.65 (0.32,1.35) | 0.69 (0.36,1.33) | 0.94 (0.47,1.91) | 0.66 (0.36,1.25) | 1 (1,1) | 0.56 (0.29,1.08) | 1.19 (0.89,1.6) | 0.9 (0.71,1.15) |
| PCB | 1.33 (0.97,1.82) | 0.93 (0.74,1.16) | 1.84 (0.96,3.5) | 1.82 (0.83,3.95) | 1.35 (0.71,2.5) | 1.17 (0.77,1.77) | 1.23 (0.93,1.64) | 1.69 (1.1,2.58) | 1.19 (0.99,1.44) | 1.79 (0.93,3.42) | 1 (1,1) | 2.13 (1.09,4.13) | 1.62 (0.85,3.07) |
| PEMBRO | 0.62 (0.35,1.13) | 0.43 (0.22,0.88) | 0.86 (0.65,1.15) | 0.85 (0.5,1.44) | 0.63 (0.5,0.79) | 0.55 (0.26,1.15) | 0.58 (0.3,1.13) | 0.79 (0.39,1.63) | 0.56 (0.3,1.07) | 0.84 (0.63,1.13) | 0.47 (0.24,0.92) | 1 (1,1) | 0.76 (0.58,1) |
| RAM + DOC | 0.82 (0.47,1.45) | 0.57 (0.29,1.14) | 1.14 (0.9,1.43) | 1.12 (0.68,1.85) | 0.83 (0.71,0.97) | 0.72 (0.35,1.49) | 0.76 (0.4,1.46) | 1.04 (0.52,2.1) | 0.73 (0.4,1.37) | 1.11 (0.87,1.41) | 0.62 (0.33,1.18) | 1.32 (1,1.74) | 1 (1,1) |
HRs are provided for treatments specified in column 1 (in rows) vs the treatments in subsequent columns; HRs <1 show better survival of the treatments in column 1.
AFT: Afatinib; ATEZ: Atezolizumab; BEV: Bevacizumab; DOC: Docetaxel; ERL: Erlotinib; GEF: Gefitinib; HR: Hazard ratio; NIV: Nivolumab; PEM: Pemetrexed; PEMBRO: Pembrolizumab; RAM: Ramucirumab.
| NIV | DOC | DOC + ERL | ERL | PEM | GEF | PEM + PLAT | DOC + RAM | ERL + PEM | PEMBRO | BEV + DOC | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| NIV | 0.8908 (0.7453, 1.058) | 1.345 (0.5181, 3.408) | 0.7813 (0.56, 1.089) | 0.7338 (0.4821, 1.117) | 0.6898 (0.477, 0.9989) | 1.083 (0.6238, 1.867) | 1.157 (0.9248, 1.435) | 1.115 (0.7155, 1.714) | 1.035 (0.8004, 1.327) | 1.256 (0.7921, 1.946) | |
| DOC | 1.123 (0.9384, 1.332) | 1.511 (0.59, 3.762) | 0.8776 (0.6605, 1.161) | 0.8247 (0.5619, 1.204) | 0.7746 (0.5585, 1.072) | 1.215 (0.7212, 2.042) | 1.299 (1.133, 1.48) | 1.252 (0.831, 1.852) | 1.163 (0.9633, 1.391) | 1.41 (0.9245, 2.115) | |
| DOC + ERL | 0.7433 (0.2817, 1.857) | 0.6617 (0.2555, 1.624) | 0.5801 (0.2368, 1.374) | 0.5442 (0.2123, 1.337) | 0.5114 (0.2042, 1.233) | 0.8065 (0.2951, 2.115) | 0.8585 (0.3285, 2.141) | 0.8288 (0.32, 2.033) | 0.7682 (0.2936, 1.929) | 0.934 (0.3291, 2.502) | |
| ERL | 1.28 (0.9051, 1.765) | 1.14 (0.8517, 1.496) | 1.724 (0.7033, 4.088) | 0.9381 (0.723, 1.208) | 0.8826 (0.7427, 1.042) | 1.387 (0.8872, 2.132) | 1.48 (1.075, 2.005) | 1.426 (1.065, 1.892) | 1.325 (0.9395, 1.836) | 1.606 (0.9594, 2.615) | |
| PEM | 1.363 (0.8807, 2.047) | 1.213 (0.8184, 1.753) | 1.837 (0.7199, 4.525) | 1.066 (0.8193, 1.369) | 0.9413 (0.755, 1.159) | 1.479 (1.028, 2.102) | 1.574 (1.042, 2.331) | 1.519 (1.099, 2.068) | 1.41 (0.9131, 2.127) | 1.71 (0.9556, 2.957) | |
| GEF | 1.45 (0.9868, 2.067) | 1.291 (0.9201, 1.768) | 1.956 (0.7818, 4.718) | 1.133 (0.9529, 1.337) | 1.062 (0.8555, 1.313) | 1.571 (1.032, 2.357) | 1.677 (1.165, 2.366) | 1.615 (1.183, 2.174) | 1.501 (1.023, 2.161) | 1.818 (1.06, 3.047) | |
| PEM + PLAT | 0.9235 (0.5232, 1.565) | 0.8232 (0.4796, 1.361) | 1.24 (0.4535, 3.257) | 0.721 (0.4605, 1.108) | 0.676 (0.4682, 0.9578) | 0.6365 (0.4169, 0.953) | 1.068 (0.6112, 1.796) | 1.026 (0.6324, 1.637) | 0.9563 (0.5379, 1.629) | 1.157 (0.585, 2.205) | |
| DOC + RAM | 0.8641 (0.6905, 1.072) | 0.7698 (0.6721, 0.8777) | 1.165 (0.4497, 2.926) | 0.6756 (0.4924, 0.9195) | 0.6351 (0.4224, 0.9443) | 0.5961 (0.4164, 0.8464) | 0.936 (0.546, 1.598) | 0.9646 (0.6264, 1.459) | 0.8954 (0.7117, 1.117) | 1.085 (0.6959, 1.662) | |
| ERL + PEM | 0.8968 (0.5726, 1.373) | 0.7987 (0.5309, 1.184) | 1.207 (0.4714, 2.999) | 0.7011 (0.523, 0.9284) | 0.6584 (0.4775, 0.8983) | 0.6193 (0.4544, 0.8346) | 0.9751 (0.599, 1.549) | 1.037 (0.6725, 1.569) | 0.9288 (0.5908, 1.435) | 1.127 (0.625, 1.981) | |
| PEMBRO | 0.966 (0.747, 1.236) | 0.86 (0.7129, 1.029) | 1.302 (0.4999, 3.281) | 0.7548 (0.5365, 1.049) | 0.709 (0.462, 1.076) | 0.6662 (0.4563, 0.9625) | 1.046 (0.6008, 1.811) | 1.117 (0.8868, 1.393) | 1.077 (0.6844, 1.662) | 1.212 (0.7606, 1.884) | |
| BEV + DOC | 0.7961 (0.5043, 1.238) | 0.7094 (0.4652, 1.064) | 1.071 (0.3828, 2.918) | 0.6226 (0.3746, 1.022) | 0.5848 (0.3297, 1.021) | 0.55 (0.3214, 0.9246) | 0.8646 (0.4427, 1.663) | 0.9213 (0.5898, 1.412) | 0.8876 (0.4938, 1.565) | 0.8254 (0.5211, 1.289) |
HRs are provided for treatments specified in column 1 (in rows) vs the treatments in subsequent columns; HRs <1 show better survival of the treatments in column 1; carboplatin and cisplatin were pooled as PLAT as their efficacies were considered similar.
BEV: Bevacizumab; DOC: Docetaxel; ERL: Erlotinib; GEF: Gefitinib; HR: Hazard ratio; NIV: Nivolumab; PEM: Pemetrexed; PEMBRO: Pembrolizumab; PLAT: Platinum; RAM: Ramucirumab.
Sensitivity analyses of first-line-to-progression studies
Piecewise constant hazard ratio
All studies except Lee [39] and Lynch [40] were included in the piecewise constant HR analyses comparing first-line-to-progression treatments; the reason for exclusion was a lack of published KM curves. The exclusion of these two studies did not alter the structure of the OS or PFS networks compared with the base case, as the comparators were represented by studies included in the analyses (Supplementary Figures 1 & 2). Model assessment results strongly preferred RE models (Supplementary Table 11). HR data compared with PEMc + PLATi for OS and PFS are shown in Supplementary Tables 14 & 15. The HR results showed that treatment with PEMc + PEMBROc + PLATi had a lower hazard of death compared with PEMc + PLATi during the longest-term follow-up (>6 months). No other treatment showed a difference in hazards of death at any time period. Lower hazards of progression or death were also observed for PEMc + PEMBROc + PLATi compared with PEMc + PLATi for the longest follow-up period. Increased hazards of progression or death were observed for PACi + PLATi compared with the reference. Similar to frequentist measures such as the Akaike information criterion, the DIC can only be used to compare models that have been fitted to the same dataset [86]. It is therefore not possible to use this to compare the fit of the Woods models, which are fit to aggregate data, and piecewise constant models, which are fit to KM data, and this is a limitation of the multimodel approach.
PD-L1 ≥50%
The OS and PFS network illustrating first-line-to-progression treatments for a subgroup of patients with PD-L1 TPS ≥50% tumors from the KEYNOTE-024, -042 and -189 studies is shown in Supplementary Figure 3. Pairwise HR results for OS showed that treatment with PEMc + PEMBROc + PLATi had a lower hazard of death compared with the other three treatments in the network: PEMc + PLATi (HR: 0.42); PEMBROc monotherapy (HR: 0.61); and investigator's choice of chemotherapy (GEMi or PACi or PEMc) + PLATi (HR: 0.38; Supplementary Tables 16 & 17). Improvement in OS was also observed in patients treated with PEMBROc monotherapy compared with PEMc + PLATi (HR: 0.69) and (GEMi or PACi or PEMc) + PLATi (HR:0.63). The pairwise data for PFS also demonstrated that treatment with PEMc + PEMBROc + PLATi had a lower hazard of progression or death compared with the other three treatments (HRs: 0.36, 0.44 and 0.24, respectively; Supplementary Tables 18 & 19). Treatment with PEMBROc monotherapy also showed a lower hazard of progression or death compared with PEMc + PLATi (HR: 0.81) and (GEMi or PACi or PEMc) + PLATi (HR: 0.55).
Inconsistency checking
For inconsistency checking, closed loops in the OS and PFS networks for first-line-to-progression treatment were identified and assessed. For the first-line-to-progression network for OS and PFS, one closed loop was identified between comparators PEMc versus BEVc + PEMc versus BEVc + PEMc + PLATi. This loop consisted of one three-arm trial (Spigel [45]) and one two-arm trial (65Plus [30]) for the BEVc + PEMc versus BEVc + PEMc + PLATi comparison. The Bucher method was used to compare the indirect estimate for BEVc + PEMc versus BEVc + PEMc + PLATi for inconsistency with the pooled estimate for BEVc + PEMc versus BEVc + PEMc + PLATi from the fixed-effects NMA. The results of the inconsistency assessment for first-line-to-progression OS and PFS networks are presented in Tables 8 & 9. The p-values for the inconsistency estimates for these loops were all above 0.9, indicating no evidence of inconsistencies in the loops.
| Direct and indirect estimates | Study | Comparison | log(HR) | SE, log(HR) | p-value |
|---|---|---|---|---|---|
| Indirect estimate | Spigel 2018 (3-arm trial) | BEVc + PEMc vs BEVc + PEMc + PLATi | 0.12 | 0.29 | 0.668 |
| Direct estimate | 65Plus | BEVc + PEMc vs BEVc + PEMc + PLATi | 0.09 | 0.16 | 0.591 |
| Inconsistency assessment results | |||||
|---|---|---|---|---|---|
| Comparison | Inconsistency estimate, w | SE(w) | p-value | ||
| Inconsistency estimate | BEVc + PEMc vs BEVc + PEMc + PLATi | -0.04 | 0.33 | 0.914 | |
| BEV: Bevacizumab; c: Continuous; HR: Hazard ratio; i: Induction; PEM: Pemetrexed; PLAT: Platinum; SE: Standard error. | |||||
| Direct and indirect estimates | Study | Comparison | log(HR) | SE, log(HR) | p-value |
|---|---|---|---|---|---|
| Indirect estimate | Spigel 2018 (3-arm trial) | BEVc + PEMc vs BEVc + PEMc + PLATi | 0.24 | 0.28 | 0.395 |
| Direct estimate | 65Plus | BEVc + PEMc vs BEVc + PEMc + PLATi | 0.25 | 0.14 | 0.06 |
| Inconsistency assessment results | |||||
|---|---|---|---|---|---|
| Comparison | Inconsistency estimate, w | SE(w) | p-value | ||
| Inconsistency estimate | BEVc + PEMc vs BEVc + PEMc + PLATi | 0.02 | 0.31 | 0.953 | |
BEV: Bevacizumab; c: Continuous; HR: Hazard ratio; i: Induction; PEM: Pemetrexed; PLAT: Platinum; SE: Standard error.
Discussion
In this comprehensive NMA, the comparative efficacy of treatments in first-line and second-line settings for locally advanced or metastatic nonsquamous NSCLC was systematically reviewed and evaluated. Immunotherapies have been associated with a greater gain in survival compared with traditional chemotherapy in the first-line setting; specifically, PEMc + PEMBROc + PLATi had the highest PFS and OS benefit compared with PEMc + PLATi in first-line treatment until progression for advanced nonsquamous NSCLC for both the overall population and PD-L1 TPS ≥50% subgroup. PEMBRO monotherapy is efficacious in the PD-L1 ≥1% population, with greater efficacy benefit in the PD-L1 TPS ≥50% subgroup [38]. This was supported by the analyses wherein PEMBROc monotherapy showed a PFS and OS benefit compared with PEMc + PLATi. When comparing PEMBROc monotherapy to PEMc + PEMBROc + PLATi, the triplet showed no difference in OS and a PFS benefit compared with PEMBROc monotherapy in the PD-L1 TPS ≥50% subgroup. For second-line studies, favorable OS was observed for PEMBRO monotherapy compared with AFT and DOC monotherapies. Immunotherapy monotherapies ATEZ and NIV also showed improved OS compared with DOC. Treatment with PEM + PLAT showed favorable PFS when compared with PEM and GEF monotherapies. Of note, this was the only treatment regimen that included a platinum agent. For the included immunotherapies in this analysis, only PEMBRO monotherapy showed improved PFS compared with GEF.
In interpreting these findings, one must note certain exceptions made in these analyses. In seeking to include all available data on immunotherapies, specifically NIV and PEMBRO, some exceptions to the inclusion criteria were made that resulted in heterogeneity across studies. Among these exceptions is the inclusion of the CheckMate 227 study [20] in which patients with a tumor mutational burden of at least 10 mutations per megabase, a subpopulation of the larger trial, were assessed. Additionally, the KEYNOTE-024 trial [8], which only enrolled patients with PD-L1 ≥50% tumors and included mixed histologies, was analyzed. Lastly, the KEYNOTE-042 trial [38], which included mixed histologies and patients with PD-L1 TPS>1%, was pooled in this analysis. For these two trials with mixed histology, the majority of patients were nonsquamous.
In an effort to include all available data, it was necessary to use median survival estimates to inform inputs for the survival NMAs for studies not reporting HRs or KM data from which the underlying IPD could be reconstructed. There were only three such studies across the analyses, all of which evaluated second-line treatments (Dong, Li and Kim) [48,51,53]. The use of median survival estimates relies on the assumption that the rate of events is constant over time. However, the assumption of a constant rate of events may not hold for treatments for which median survival estimates were used. It should also be noted as a limitation that these analyses were conducted from data collected in an SLR conducted in 2018 and trials published since then were not included in the analyses. The analyses may therefore be missing some newer therapies that may have relevant data to further inform these analyses.
Here, the base case NMA employing the Woods methodology had to assume PHs, and this assumption may have been violated [87]. The sensitivity analysis allowing different HRs over 0–3, 3–6 and >6 months, but constant for each interval, gave results consistent with the base case. It is feasible to use other nonproportional hazards methods, such as fractional polynomial or spline-based NMA [88,89]. The less flexible piecewise constant models with only three time periods were selected to avoid overfitting the data. The residual deviance of these models was close to the number of data points, suggesting sufficient flexibility to capture the pattern of hazards in the underlying data. The evidence networks were often limited to only one study informing any particular treatment arm. As the credible intervals for the RE models span implausible ranges for the Woods models, results from the FE models were presented with RE models in the Supplementary Materials for comparison.
An NMA evaluating the efficacy of PEMc + PEMBROc + PLATi by Frederickson [90] et al. differed in the classification of treatment line and treatment pooling. To reduce heterogeneity introduced by pooling all studies conducted in first-line patients, this study considered first-line to be patients receiving treatment until progression and did not include those that received only four cycles of induction treatment. This definition of first-line treatment reflected the treatment-until-progression indications of newer immunotherapies, a fundamental difference in dosing compared with traditional chemotherapies. These differences in study design did not impact conclusions, with results from both studies suggesting a survival benefit of PEMc + PEMBROc + PLATi compared with other included treatments.
The addition of the current study to existing evidence elucidates the prognostic role of PD-L1 expression. The subgroup analyses of patients with PD-L1 TPS ≥50% revealed a more pronounced survival benefit specifically with PEMc + PEMBROc + PLATi compared with the base case. The PFS benefit of PEMc + PEMBROc + PLATi was maintained compared with PEMBROc monotherapy in this subgroup. Further study of stratified PD-L1 expression levels where relevant data are available will aid in physician treatment selection between PEMBROc monotherapy and PEMc + PEMBROc + PLATi given the lack of head-to-head randomized trials between the two regimens.
Conclusion
The findings from this NMA consistently demonstrated that treatment with immunotherapy bolsters survival benefits when combined with standard platinum-based chemotherapies across different treatment modalities in first-line populations. Specifically, PEMc + PEMBROc + PLATinum had the highest PFS and OS benefit compared with PEMc + PLATinum. This combination also showed a PFS and OS benefit compared with PEMBROc monotherapy. PFS and OS differences between PEMc + PEMBROc + PLATinum and PEMc + PLATinum were even greater in the PD-L1 TPS ≥50% subgroup. Further investigations are warranted to elucidate full treatment benefits; however, these findings lend support to the consideration of immunochemotherapy combinations as optimal first-line treatment options for locally advanced or metastatic nonsquamous NSCLC.
•
A systematic literature review (SLR) and network meta-analysis (NMA) were conducted to compare the efficacy of immunotherapies for advanced nonsquamous non-small-cell lung cancer (NSCLC).
•
Treatments used for first-line to progression and second-line in advanced NSCLC were analyzed in terms of overall survival (OS) and progression-free survival (PFS).
•
Fifty studies were identified in the SLR, however, 19 out of 29 studies that evaluated first-line-to-progression treatments and 19 out of 21 studies that evaluated second-line treatments were included in the NMA.
•
Among first-line-to-progression treatments, pembrolizumab + pemetrexed + platinum showed the greatest OS benefit versus other regimens and a PFS benefit versus all but three regimens.
•
Among second-line treatments, an OS benefit was seen for atezolizumab, nivolumab and pembrolizumab versus docetaxel.
•
PFS benefit was observed for pemetrexed + platinum compared with pemetrexed monotherapy and gefitinib monotherapy.
•
In the PD-L1 ≥50% group of patients, pembrolizumab + pemetrexed + platinum had a lower hazard of death compared with the other three treatments in the network, pemetrexed + platinum, pembrolizumab monotherapy and investigator's choice of chemotherapy + platinum.
•
The NMA demonstrated that treatment with immunotherapy improves survival benefit when combined with standard platinum-based chemotherapies across different treatment modalities in first-line populations.
Financial & competing interests disclosure
H Thom has received personal consulting fees from ICON Plc, Pfizer Inc, Novartis Pharma AG, Roche Holding AG, Eisai Co Ltd, Lundbeck and Janssen. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
File (supplementary appendix.pdf)
- Download
- 732.51 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
WHO. Cancer Fact Sheet. Secondary Cancer Fact Sheet (2018). www.who.int/news-room/fact-sheets/detail/cancer
2.
Planchard D, Popat S, Kerr K et al. ESMO Guidelines Committee. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 29(Suppl. 4), iv192–iv237 (2018).
3.
Massarelli E, Papadimitrakopoulou V, Welsh J, Tang C, Tsao AS. Immunotherapy in lung cancer. Transl. Lung Cancer Res. 3(1), 53–63 (2014).
4.
Herbst RS, Baas P, Kim DW et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): a randomised controlled trial. Lancet 387(10027), 1540–1550 (2016).
5.
Borghaei H, Paz-Ares L, Horn L et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N. Engl. J. Med. 373(17), 1627–1639 (2015).
6.
Brahmer J, Reckamp KL, Baas P et al. Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N. Engl. J. Med. 373(2), 123–135 (2015).
7.
Rittmeyer A, Barlesi F, Waterkamp D et al. OAK Study Group. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a phase 3, open-label, multicentre randomised controlled trial. Lancet 389(10066), 255–265 (2017).
8.
Reck M, Rodríguez-Abreu D, Robinson AG et al. KEYNOTE-024 Investigators. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N. Engl. J. Med. 375(19), 1823–1833 (2016).
9.
Mok TSK, Wu YL, Kudaba I et al. KEYNOTE-042 Investigators. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, phase 3 trial. Lancet 393(10183), 1819–1830 (2019).
10.
Langer CJ, Gadgeel SM, Borghaei H et al. KEYNOTE-021 investigators. Carboplatin and pemetrexed with or without pembrolizumab for advanced, non-squamous non-small-cell lung cancer: a randomised, phase 2 cohort of the open-label KEYNOTE-021 study. Lancet Oncol. 17(11), 1497–1508 (2016).
11.
Borghaei H, Langer CJ, Gadgeel S et al. 24-month overall survival from KEYNOTE-021 cohort G: pemetrexed and carboplatin with or without pembrolizumab as first-line therapy for advanced nonsquamous non-small cell lung cancer. J. Thorac. Oncol. 14(1), 124–129 (2019).
12.
Gandhi L, Rodríguez-Abreu D, Gadgeel S et al. KEYNOTE-189 Investigators. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N. Engl. J. Med. 378(22), 2078–2092 (2018).
13.
Socinski MA, Jotte RM, Cappuzzo F et al. IMpower150 Study Group. Atezolizumab for first-line treatment of metastatic nonsquamous NSCLC. N. Engl. J. Med. 378(24), 2288–2301 (2018).
14.
Garon EB, Ciuleanu TE, Arrieta O et al. Ramucirumab plus docetaxel versus placebo plus docetaxel for second-line treatment of stage IV non-small-cell lung cancer after disease progression on platinum-based therapy (REVEL): a multicentre, double-blind, randomised phase 3 trial. Lancet 384(9944), 665–673 (2014).
15.
Hanna N, Shepherd FA, Fossella FV et al. Randomized phase III trial of pemetrexed versus docetaxel in patients with non-small-cell lung cancer previously treated with chemotherapy. J. Clin. Oncol. 22(9), 1589–1597 (2004).
16.
Shepherd FA, Dancey J, Ramlau R et al. Prospective randomized trial of docetaxel versus best supportive care in patients with non-small-cell lung cancer previously treated with platinum-based chemotherapy. J. Clin. Oncol. 18(10), 2095–2103 (2000).
17.
Centre for Reviews and Dissemination. Systematic Reviews – CRD's Guide for undertaking reviews in health care. www.york.ac.uk/media/crd/Systematic_Reviews.pdf
18.
Hutton B, Salanti G, Caldwell DM et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann. Intern. Med. 162(11), 777–784 (2015).
19.
Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0. The Cochrane Collaboration (2011).
20.
Hellmann MD, Ciuleanu TE, Pluzanski A et al. Nivolumab plus ipilimumab in lung cancer with a high tumor mutational burden. N. Engl. J. Med. 378(22), 2093–2104 (2018).
21.
Dias S, Welton NJ, Sutton AJ, Ades AE. NICE DSU Technical Support Document 2: A Generalised Linear Modelling Framework for Pairwise and Network Meta-Analysis of Randomised Controlled Trials. National Institute for Health and Care Excellence (NICE), UK (2014). www.ncbi.nlm.nih.gov/books/NBK310366/
22.
Lunn D, Jackson C, Best N, Thomas A, Spiegelhalter D. The BUGS Book: A Practical Introduction to Bayesian Analysis. CRC Press, UK (2012).
23.
Woods BS, Hawkins N, Scott DA. Network meta-analysis on the log-hazard scale, combining count and hazard ratio statistics accounting for multi-arm trials: a tutorial. BMC Med Res Methodol. (2010).
24.
Spiegelhalter DJ, Best NG, Carlin BP, Van Der Linde A. Bayesian measures of model complexity and fit. J. Royal Stat. Soc. B 64(4), 583–639 (2002).
25.
Guyot P, Ades AE, Ouwens MJ, Welton NJ. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC Med. Res. Methodol. 12, 9 (2012).
26.
Schoenfeld D. Partial residuals for the proportional hazards regression model. Biometrika 69(1), 239–241 (1982).
27.
Lu G, Ades AE, Sutton AJ, Cooper NJ, Briggs AH, Caldwell DM. Meta-analysis of mixed treatment comparisons at multiple follow-up times. Stat. Med. 26(20), 3681–3699 (2007).
28.
López-López JA, Humphriss RL, Beswick AD et al. Choice of implant combinations in total hip replacement: systematic review and network meta-analysis. BMJ 359, j4651 (2017).
29.
Thom H, Ender F, Samavedam S et al. Effect of AcrySof versus other intraocular lens properties on the risk of Nd:YAG capsulotomy after cataract surgery: a systematic literature review and network meta-analysis. PLOS ONE 14(8), e0220498 (2019).
30.
Schuette W, Schneider CP, Engel-Riedel W et al. 65Plus: open-label study of bevacizumab in combination with pemetrexed or pemetrexed/carboplatin as first-line treatment of patients with advanced or recurrent nonsquamous non-small-cell lung cancer. Lung Cancer (Auckl.) 8, 217–229 (2017).
31.
Reck M, von Pawel J, Zatloukal P et al. Overall survival with cisplatin-gemcitabine and bevacizumab or placebo as first-line therapy for nonsquamous non-small-cell lung cancer: results from a randomised phase III trial (AVAiL). Ann. Oncol. 21(9), 1804–1809 (2010).
32.
Zhou C, Wu YL, Chen G et al. BEYOND: a randomized, double-blind, placebo-controlled, multicenter, phase III study of first-line carboplatin/paclitaxel plus bevacizumab or placebo in Chinese patients with advanced or recurrent nonsquamous non-small-cell lung cancer. J. Clin. Oncol. 33(19), 2197–2204 (2015).
33.
Doebele RC, Spigel D, Tehfe M et al. Phase 2, randomized, open-label study of ramucirumab in combination with first-line pemetrexed and platinum chemotherapy in patients with nonsquamous, advanced/metastatic non-small cell lung cancer. Cancer 121(6), 883–892 (2015).
34.
Galetta D, Cinieri S, Pisconti S et al. Cisplatin/pemetrexed followed by maintenance pemetrexed versus carboplatin/paclitaxel/bevacizumab followed by maintenance bevacizumab in advanced nonsquamous lung cancer: the GOIM (Gruppo Oncologico Italia Meridionale) ERACLE phase III randomized trial. Clin. Lung Cancer 16(4), 262–273 (2015).
35.
Georgoulias V, Samonis G, Papadakis E et al. Comparison of docetaxel/cisplatin to docetaxel/gemcitabine as first-line treatment of advanced non-small cell lung cancer: early results of a randomized trial. Lung Cancer 34(Suppl. 4), S47–S51 (2001).
36.
Johnson DH, Fehrenbacher L, Novotny WF et al. Randomized phase II trial comparing bevacizumab plus carboplatin and paclitaxel with carboplatin and paclitaxel alone in previously untreated locally advanced or metastatic non-small-cell lung cancer. J. Clin. Oncol. 22(11), 2184–2191 (2004).
37.
Karayama M, Inui N, Fujisawa T et al. Maintenance therapy with pemetrexed and bevacizumab versus pemetrexed monotherapy after induction therapy with carboplatin, pemetrexed, and bevacizumab in patients with advanced non-squamous non small cell lung cancer. Eur. J. Cancer 58, 30–37 (2016).
38.
Lopes G, Wu Y-L, Kudaba I et al. Pembrolizumab (pembro) versus platinum-based chemotherapy (chemo) as first-line therapy for advanced/metastatic NSCLC with a PD-L1 tumor proportion score (TPS) ≥1%: Open-label, phase 3 KEYNOTE-042 study. J. Clin. Oncol. 36(Suppl. 18), LBA4 (2018).
••A key study demonstrating that pembrolizumab monotherapy is efficacious in the PD-L1 ≥1% population, with greater efficacy benefit in the PD-L1 tumor proportion score ≥50% subgroup, a key finding validated by this network meta-analysis.
39.
Lee DH, Cho EK, Ahn JS et al. Open-label, multicenter, randomized phase III trial of pemetrexed/carboplatin doublet vs pemetrexed singlet in chemotherapy-naïve elderly patients aged 70 or more with advanced non-squamous non-small cell lung cancer and good performance status. J. Clin. Oncol. 34(Suppl. 15), 9081 (2016).
40.
Lynch TJ, Bondarenko I, Luft A et al. Ipilimumab in combination with paclitaxel and carboplatin as first-line treatment in stage IIIB/IV non-small-cell lung cancer: results from a randomized, double-blind, multicenter phase II study. J. Clin. Oncol. 30(17), 2046–2054 (2012).
41.
Niho S, Kunitoh H, Nokihara H et al. Randomized phase II study of first-line carboplatin-paclitaxel with or without bevacizumab in Japanese patients with advanced non-squamous non-small-cell lung cancer. Lung Cancer 76(3), 362–367 (2012).
42.
Patel JD, Socinski MA, Garon EB et al. PointBreak: a randomized phase III study of pemetrexed plus carboplatin and bevacizumab followed by maintenance pemetrexed and bevacizumab versus paclitaxel plus carboplatin and bevacizumab followed by maintenance bevacizumab in patients with stage IIIB or IV nonsquamous non-small-cell lung cancer. J. Clin. Oncol. 31(34), 4349–4357 (2013).
43.
Zinner RG, Obasaju CK, Spigel DR et al. PRONOUNCE: randomized, open-label, phase III study of first-line pemetrexed + carboplatin followed by maintenance pemetrexed versus paclitaxel + carboplatin + bevacizumab followed by maintenance bevacizumab in patients with advanced nonsquamous non-small-cell lung cancer. J. Thoracic Oncol. 10(1), 134–142 (2015).
44.
Sandler A, Gray R, Perry MC et al. Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer. N. Engl. J. Med. 355(24), 2542–2550 (2006).
45.
Spigel DR, Hainsworth JD, Joseph MJ et al. Randomized phase 2 trial of pemetrexed, pemetrexed/bevacizumab, and pemetrexed/carboplatin/bevacizumab in patients with stage IIIB/IV non-small cell lung cancer and an Eastern Cooperative Oncology Group performance status of 2. Cancer 124(9), 1982–1991 (2018).
46.
Zhou Q, Cheng Y, Yang JJ et al. Pemetrexed versus gefitinib as a second-line treatment in advanced nonsquamous nonsmall-cell lung cancer patients harboring wild-type EGFR (CTONG0806): a multicenter randomized trial. Ann. Oncol. 25(12), 2385–2391 (2014).
47.
Kawaguchi T, Ando M, Asami K et al. Randomized phase III trial of erlotinib versus docetaxel as second- or third-line therapy in patients with advanced non-small-cell lung cancer: Docetaxel and Erlotinib Lung Cancer Trial (DELTA). J. Clin. Oncol. 32(18), 1902–1908 (2014).
48.
Dong L, Han ZF, Feng ZH, Jia ZY. Comparison of pemetrexed and docetaxel as salvage chemotherapy for the treatment for nonsmall-cell lung cancer after the failure of epidermal growth factor receptor-tyrosine kinase inhibitors. J. Int. Med. Res. 42(1), 191–197 (2014).
49.
Thatcher N, Chang A, Parikh P et al. Gefitinib plus best supportive care in previously treated patients with refractory advanced non-small-cell lung cancer: results from a randomised, placebo-controlled, multicentre study (Iressa Survival Evaluation in Lung Cancer). Lancet 366(9496), 1527–1537 (2005).
50.
Juan Ó, Aparisi F, Sánchez-Hernández A et al. Intercalated dosing schedule of erlotinib and docetaxel as a therapeutic strategy to avoid antagonism and optimize its benefits in advanced non-small-cell lung cancer. a randomized phase II clinical trial. Clin. Lung Cancer 16(3), 193–199 (2015).
51.
Kim YS, Cho EK, Woo HS et al. Randomized phase II study of pemetrexed versus gefitinib in previously treated patients with advanced non-small cell lung cancer. Cancer Res. Treat. 48(1), 80–87 (2016).
52.
Sun JM, Lee KH, Kim SW et al. Gefitinib versus pemetrexed as second-line treatment in patients with nonsmall cell lung cancer previously treated with platinum-based chemotherapy (KCSG-LU08-01): an open-label, phase 3 trial. Cancer 118(24), 6234–6242 (2012).
53.
Li T, Piperdi B, Walsh WV et al. Randomized phase 2 trial of pharmacodynamic separation of pemetrexed and intercalated erlotinib versus pemetrexed alone for advanced nonsquamous, non-small-cell lung cancer. Clin. Lung Cancer 18(1), 60–67 (2017).
54.
Miller VA, Hirsh V, Cadranel J et al. Afatinib versus placebo for patients with advanced, metastatic non-small-cell lung cancer after failure of erlotinib, gefitinib, or both, and one or two lines of chemotherapy (LUX-Lung 1): a phase 2b/3 randomised trial. Lancet Oncol. 13(5), 528–538 (2012).
55.
Schuler M, Yang JC, Park K et al. Afatinib beyond progression in patients with non-small-cell lung cancer following chemotherapy, erlotinib/gefitinib and afatinib: phase III randomized LUX-Lung 5 trial. Ann. Oncol. 27(3), 417–423 (2016).
56.
Schuler MH, Yang C-H, Park K et al. Continuation of afatinib beyond progression: results of a randomized, open-label, phase III trial of afatanib plus paclitaxel (P) versus investigator's choice chemotherapy (CT) in patients (pts) with metastatic non-small cell lung cancer (NSCLC) progressed on erlotinib/gefitinib (E/G) and afatanib—LUX-Lung 5 (LL5). J. Clin. Oncol. 32(Suppl. 15), 8019 (2014).
57.
Fehrenbacher L et al. Updated efficacy analysis including secondary population results for OAK: a randomized phase III study of atezolizumab versus docetaxel in patients with previously treated advanced non-small cell lung cancer. J. Thorac. Oncol. 13(8), 1156–1170 (2018).
58.
Fehrenbacher L, von Pawel J, Park K et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): a multicentre, open-label, phase 2 randomised controlled trial. Lancet 387(10030), 1837–1846 (2016).
59.
Mazières J, Park K, Lewanski C et al. 136PD_PR 3-year survival and duration of response in randomized phase II study of atezolizumab (atezo) vs docetaxel (doc) in 2L+ NSCLC (POPLAR). J. Thorac. Oncol. 13(4), S79 (2018).
60.
Paz-Ares L, Perol M, Ciuleanu T-E et al. Exploratory analysis of safety by histology and efficacy in a nonsquamous NSCLC subgroup in REVEL: a randomized phase III study of ramucirumab (RAM) plus docetaxel (DOC) vs DOC for second-line treatment of stage IV non-small-cell lung cancer (NSCLC). J. Clin. Oncol. 33(Suppl. 15), 8055 (2015).
61.
Smit EF, Burgers SA, Biesma B et al. Randomized phase II and pharmacogenetic study of pemetrexed compared with pemetrexed plus carboplatin in pretreated patients with advanced non-small-cell lung cancer. J. Clin. Oncol. 27(12), 2038–2045 (2009).
62.
Ciuleanu T, Stelmakh L, Cicenas S et al. Efficacy and safety of erlotinib versus chemotherapy in second-line treatment of patients with advanced, non-small-cell lung cancer with poor prognosis (TITAN): a randomised multicentre, open-label, phase 3 study. Lancet Oncol. 13(3), 300–308 (2012).
63.
Urata Y, Katakami N, Morita S et al. Randomized phase III study comparing gefitinib with erlotinib in patients with previously treated advanced lung adenocarcinoma: WJOG 5108L. J. Clin. Oncol. 34(27), 3248–3257 (2016).
64.
Nishiyama A, Katakami N, Morita S et al. Randomized phase III study comparing gefitinib (G) with erlotinib (E) in patients (pts) with previously treated advanced lung adenocarcinoma (LA): WJOG 5108L. Ann. Oncol. 25(Suppl. 4), IV447 (2014).
65.
Takeda M, Yamanaka T, Seto T et al. Bevacizumab beyond disease progression after first-line treatment with bevacizumab plus chemotherapy in advanced nonsquamous non–small cell lung cancer (West Japan Oncology Group 5910L): An open-label, randomized, phase 2 trial. Cancer 122(7), 1050–1059 (2016).
66.
Hellmann MD, Ciuleanu TE, Pluzanski A et al. Nivolumab plus ipilimumab in lung cancer with a high tumor mutational burden. N. Engl. J. Med. 378(22), 2093–2104 (2018).
67.
Johnson DH, Fehrenbacher L, Novotny WF et al. Randomized phase II trial comparing bevacizumab plus carboplatin and paclitaxel with carboplatin and paclitaxel alone in previously untreated locally advanced or metastatic non-small-cell lung cancer. J. Clin. Oncol. 22(11), 2184–2191 (2004).
68.
Gandhi L, Rodríguez-Abreu D, Gadgeel S et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N. Engl. J. Med. 378(22), 2078–2092 (2018).
69.
Lee DH, Cho EK, Ahn JS et al. Open-label, multicenter, randomized phase III trial of pemetrexed/carboplatin doublet vs pemetrexed singlet in chemotherapy-naive elderly patients aged 70 or more with advanced non-squamous non-small cell lung cancer and good performance status. J. Clin. Oncol. 34(Suppl. 15), (2016).
70.
Lynch TJ, Bondarenko I, Luft A et al. Ipilimumab in combination with paclitaxel and carboplatin as first-line treatment in stage IIIB/IV non-small-cell lung cancer: results from a randomized, double-blind, multicenter phase II study. J. Clin. Oncol. 30, 2046–2054 (2012).
71.
Niho S, Kunitoh H, Nokihara H et al. Randomized phase II study of first-line carboplatin-paclitaxel with or without bevacizumab in Japanese patients with advanced non-squamous non-small-cell lung cancer. Lung Cancer 76(3), 362–367 (2012).
72.
Zinner RG, Obasaju CK, Spigel DR et al. PRONOUNCE: randomized, open-label, phase III study of first-line pemetrexed + carboplatin followed by maintenance pemetrexed versus paclitaxel + carboplatin + bevacizumab followed by maintenance bevacizumab in patients with advanced nonsquamous non-small-cell lung cancer. J. Thorac. Oncol. 10(1), 134–142 (2015).
73.
Spigel DR, Hainsworth JD, Joseph MJ et al. Randomized phase 2 trial of pemetrexed, pemetrexed/bevacizumab, and pemetrexed/carboplatin/bevacizumab in patients with stage IIIB/IV non-small cell lung cancer and an Eastern Cooperative Oncology Group performance status of 2. Cancer 124(9), 1982–1991 (2018).
74.
Borghaei H, Paz-Ares L, Horn L et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N. Engl. J. Med. 373(17), 1627–1639 (2015).
75.
Paz-Ares L, Horn L, Borghaei H et al. Phase III, randomized trial (CheckMate 057) of nivolumab (NIVO) versus docetaxel (DOC) in advanced non-squamous cell (non-SQ) non-small cell lung cancer (NSCLC). J. Clin. Oncol. 33(Suppl. 18), (2015).
76.
Kawaguchi T, Ando M, Asami K et al. Randomized phase III trial of erlotinib versus docetaxel as second-or third-line therapy in patients with advanced non-small-cell lung cancer: Docetaxel and Erlotinib Lung Cancer Trial (DELTA). J. Clin. Oncol. 32(18), 1902–1908 (2014).
77.
Thatcher N, Chang A, Parikh P et al. Gefitinib plus best supportive care in previously treated patients with refractory advanced non-small-cell lung cancer: results from a randomised, placebo-controlled, multicentre study (Iressa Survival Evaluation in Lung Cancer). Lancet 366(9496), 1527–1537 (2005).
78.
Juan Ó, Aparisi F, Sánchez-Hernández A et al. Intercalated dosing schedule of erlotinib and docetaxel as a therapeutic strategy to avoid antagonism and optimize its benefits in advanced non-small-cell lung cancer. a randomized phase II clinical trial. Clin. Lung Cancer 16(3), 193–199 (2015).
79.
Kim YS, Cho EK, Woo HS et al. Randomized phase II study of pemetrexed versus gefitinib in previously treated patients with advanced non-small cell lung cancer. Cancer Res. Treat. 48(1), 80–87 (2016).
80.
Fehrenbacher L, von Pawel J, Park K et al. Updated efficacy analysis including secondary population results for OAK: a randomized phase III study of atezolizumab vs docetaxel in patients with previously treated advanced non-small cell lung cancer. J. Thorac. Oncol. 16, 16 (2018).
81.
Fehrenbacher L, Spira A, Ballinger M et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): a multicentre, open-label, phase 2 randomised controlled trial. Lancet 387, 1837–1846 (2016).
82.
Mazieres J, Park K, Lewanski C et al. 3-year survival and duration of response in randomized phase II study of atezolizumab (atezo) vs docetaxel (doc) in 2L+ NSCLC (POPLAR). J. Thorac. Oncol. 13(1 Suppl. 4), S79 (2018).
83.
Paz-Ares L, Perol M, Ciuleanu T et al. Exploratory analysis of safety by histology and efficacy in a nonsquamous NSCLC subgroup in REVEL: a randomized phase III study of ramucirumab (RAM) plus docetaxel (DOC) vs DOC for second-line treatment of stage IV non-small-cell lung cancer (NSCLC). J. Clin. Oncol. 33(Suppl. 18), (2015).
84.
Nishiyama A, Katakami N, Morita S et al. Randomized phase III study comparing gefitinib (G) with erlotinib (E) in patients (pts) with previously treated advanced lung adenocarcinoma (LA): WJOG 5108L. Ann. Oncol. 25(Suppl. 4), iv447 (2014).
85.
Takeda M, Yamanaka T, Seto T et al. Bevacizumab beyond disease progression after first-line treatment with bevacizumab plus chemotherapy in advanced nonsquamous non-small cell lung cancer (West Japan Oncology Group 5910L): an open-label, randomized, phase 2 trial. Cancer 122, 1050–1059 (2016).
86.
Thom HH, Jackson CH, Commenges D et al. State selection in Markov models for panel data with application to psoriatic arthritis. Stat. Med. 34(16), 2456–2475 (2015).
87.
Wiksten A, Hawkins N, Piepho HP, Gsteiger S. Nonproportional hazards in network meta-analysis: efficient strategies for model building and analysis. Value Health 23(7), 918–927 2020).
88.
Jansen JP. Network meta-analysis of survival data with fractional polynomials. BMC Med. Res. Methodol. 11, 61 (2011).
89.
Freeman SC, Carpenter JR. Bayesian one-step IPD network meta-analysis of time-to-event data using Royston-Parmar models. Res. Synth. Methods 8(4), 451–464 (2017).
90.
Frederickson AM, Arndorfer S, Zhang I et al. Pembrolizumab plus chemotherapy for first-line treatment of metastatic nonsquamous non-small-cell lung cancer: a network meta-analysis. Immunotherapy 11(5), 407–428 (2019).
• A similar network meta-analysis in the first-line setting. Despite the difference in the inclusion criteria for the studies analyzed, this study found similar results (i.e., a survival benefit of pemetrexed + pembrolizumab + platinum compared with other included treatments).
Information & Authors
Information
Published In
Copyright
© 2023 Becaris Publishing Ltd.
History
Received: 27 January 2022
Accepted: 29 September 2022
Published online: 9 January 2023
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
A network meta-analysis of immunotherapy-based treatments for advanced nonsquamous non-small cell lung cancer. (2023) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0016
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Mikhail Fedyanin, Nikolai Zhukov, Fedor Moiseenko, Olga Mironenko, Kirill Sapozhnikov, Natalia Sableva, Andrei Lazarev, Daria Tolkacheva, Efficacy of immune checkpoint inhibitors in the first line therapy of non-squamous non-small cell lung cancer: A systematic review and network meta-analysis, Critical Reviews in Oncology/Hematology, 10.1016/j.critrevonc.2026.105216, 221, (105216), (2026).
- Tim Reason, Yunchou Wu, Cheryl Jones, Emma Benbow, Kasper Johannesen, Bill Malcolm, The “Artificial Intelligence Statistician”: Utilizing Generative Artificial Intelligence to Select an Appropriate Model and Execute Network Meta-Analyses, Value in Health, 10.1016/j.jval.2025.08.001, 28, 11, (1646-1654), (2025).
- Nicolas Girard, Ji-Youn Han, Ross A. Soo, Kaijun Wang, Wenxi Tang, Georgios F. Nikolaidis, Anastasios Tasoulas, Ifigeneia Barouma, JeanPierre Coaquira Castro, Zheyuan Yang, Tanushree Chaudhary, Lin Zhan, Comparative effectiveness and safety of tislelizumab versus other anti–PD-(L)1 agents in first- and subsequent lines in locally advanced or metastatic non–small cell lung cancer: Systematic literature review and network meta-analysis, Lung Cancer, 10.1016/j.lungcan.2025.108450, 201, (108450), (2025).
- 颖 李, Progress in the Study of Serum Markers to Predict the Efficacy of Immune Checkpoint Inhibitors in the Treatment of Advanced Non-Small Cell Lung Cancer, Advances in Clinical Medicine, 10.12677/acm.2024.1492547, 14, 09, (917-924), (2024).