Biologic initiation rates in systemic-naive psoriasis patients after first-line apremilast versus methotrexate use
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To compare rates of biologic initiation after commencing treatment with apremilast (APR) versus methotrexate (MTX) in systemic-naive patients with psoriasis (PsO). Methods: This was a retrospective cohort study of systemic-naive patients with PsO who initiated treatment with APR or MTX between 1 January 2015 and 31 March 2018. Outcomes: Adjusted rates of biologic initiation during follow-up were compared by logistic and Cox regressions. Results: APR initiators had 58% lower likelihood of biologic initiation (odds ratio: 0.42; 95% CI: 0.37–0.48; p < 0.001), lower adjusted biologic initiation rate (14.4% [95% CI: 13.2–15.7%] vs 28.6% [95% CI: 26.8–30.5%]), lower risk of biologic initiation (hazard ratio: 0.45; 95% CI: 0.40–0.51; p < 0.001) compared with MTX initiators. Conclusion: Systemic-naive patients with PsO have a lower rate of biologic initiation over 1 year following APR initiation.
Psoriasis (PsO) is a chronic, systemic inflammatory skin disease that affects approximately 7.55 million adults in the USA [1]. This disease is associated with significant financial burden, increases the risk of serious comorbidities associated with systemic inflammation and negatively impacts quality of life. PsO is a life-long disease without a definitive cure requiring continued treatment, and in many patients, a sequence of consecutive pharmacological agents is necessary as the disease progresses.
Mild disease may be managed with topical corticosteroids and emollients, whereas more severe PsO requires phototherapy or systemic treatments including oral small molecule (OSM) therapies and biologics (anti-TNF inhibitors and IL-12, -23 and -17 inhibitors) [2–7]. Biologic therapies can be effective but require laboratory monitoring, have less convenient routes of administration, and may have high cost. Considering these factors, physicians and patients may decide to start treatment with OSM therapy and postpone the use of biologics as long as clinically indicated. A recently published commercial claims analysis using data from 2014–2016 found that about 60% of systemic-naive PsO patients initiate OSMs, whereas the remaining 40% start with biologics [8].
Apremilast (APR) and methotrexate (MTX) are both approved by the US FDA for the treatment of moderate-to-severe and severe PsO, respectively [9,10]. The safety and efficacy of APR and MTX in this space is confirmed by several randomized trials [11–13] and retrospective studies [14]. Unlike MTX and biologics, APR does not require laboratory monitoring, potentially making it more convenient to use. Some PsO treatment guidelines recommend MTX and other conventional OSMs before APR and biologics [5]; however real-world evidence shows that APR and MTX are common first-line therapies in the USA [8].
Evidence comparing APR with MTX in the treatment of systemic-naive (i.e., not previously been treated with OSM or biologics) PsO patients is limited. The objective of this study was to compare APR with MTX for the treatment of PsO in a real-world setting. In particular, it aimed to compare biologic initiation rates, length of time to biologic initiation, and index medication adherence and discontinuation between systemic-naive PsO patients who were newly initiating APR or MTX.
Materials & methods
This study employed a retrospective cohort design of administrative claims data (2014–2019) from the IBM® MarketScan® Commercial and Medicare Supplemental databases to examine biologic initiation rate in patients with PsO who newly initiated APR and MTX. The MarketScan data comprise health services for more than 39.7 million patients through privately insured fee-for-service, point-of-service or capitated health plans. This database contains enrollment information and administrative claims data with healthcare utilization information (e.g., inpatient and outpatient services, and prescription drug claims). This study used deidentified patient records and did not involve the collection, use or transmittal of individually identifiable data; therefore, institutional review board approval to conduct this study was not necessary.
Prevalent patients with PsO were identified based on having at least one diagnosis code for PsO (International Classification of Diseases, 9th Revision, Clinical Modification [ICD-9-CM] code 696.1x or ICD-10-CM code L40.0, L40.8, L40.9) from a dermatologist or rheumatologist visit during the study period between 1 January 2014 to 31 March 2019 [15,16]. Patients were included if they initiated APR or MTX during the identification period (1 January 2015 to 31 March 2018). The date of the first claim for APR or MTX during the identification period was assigned as the index date. Patients were required to be at least 18 years of age on the index date, have continuous enrollment for at least 1 year prior to (baseline period) and 1 year after (follow-up period) the index date, and have at least one of the diagnosis claims for PsO in the baseline period or on the index date. Patients were excluded if they had claims for any systemic treatment agents (systemic-naive, including APR and MTX but not including symptomatic treatments) in the baseline period, biologic-indicated autoimmune conditions (ulcerative colitis, Crohn’s disease, rheumatoid arthritis and other inflammatory polyarthropathies, ankylosing spondylitis, juvenile idiopathic arthritis) or cancer (malignant neoplasms excluding nonmelanoma skin cancer) [17] in the baseline and follow-up periods, or had multiple systemic medications administered on the index date. A subset with 2 years of follow-up was also identified for a subgroup analysis.
Analyses were based on intention to treat, with individuals analyzed as part of their index treatment group regardless of subsequent changes in therapy. Demographic characteristics, prescriber specialty (defined as the specialty on the medical claim closest in time to the index date) and comorbidities, including the Charlson Comorbidity Index, as well as healthcare utilization and costs, were measured in the baseline period [18–20]. The primary outcomes were biologic initiation rate and time to biologic initiation, reported for the 1-year follow-up period in the main analysis and for the 2-year follow-up period in the subgroup analysis. Biologic initiation was defined as having a claim for a biologic therapy during the follow-up period, regardless of whether it was in addition to (add-on) or switch from the index therapy. The secondary outcomes were treatment patterns. Particularly, index therapy adherence was measured as the proportion of days covered during the follow-up period, defined as the number of days with index therapy available divided by the length of the observation period (365 days). Index treatment discontinuation was also reported for the follow-up period (defined as a ≥60-day gap in days’ supply). Restart of the index therapy was also measured (defined as reinitiating the index treatment following discontinuation). Descriptive statistics including means, standard deviations, and relative frequencies and percentages were reported for continuous and categorical data.
As the descriptive analyses used retrospective data rather than data from randomized trials, modeling was further performed to control for differences in observed characteristics of the two cohorts that may confound the findings. Logistic regression models were conducted to estimate the likelihood of biologic initiation during the 1-year follow-up period. Cox regression models were used to evaluate the risk of biologic initiation. All models were adjusted for the following: age group, gender, region, prescriber specialty, comorbid psoriatic arthritis (PsA), Charlson Comorbidity Index, index year, nonalcoholic fatty liver disease, serious infection, pain medication and glucocorticoid utilization, baseline healthcare utilization (in both inpatient and outpatient settings) and baseline healthcare costs (per US$1000). The odds ratio (OR) and 95% confidence interval (CI), as well as adjusted rates and 95% CI, were reported for the logistic regression model, whereas the hazard ratio (HR) and 95% CI were reported for the Cox regression model. In a subgroup analysis, estimations were replicated for a subgroup with 2 years of follow-up.
All data transformations and statistical analyses were performed using SAS© version 9.4.
Results
Among the total of 5860 systemic-naive PsO patients identified meeting the study criteria between 1 January 2015 and 31 December 2018, 3288 initiated APR and 2572 initiated MTX. Table 1 provides baseline characteristics for the study cohort. The mean age of APR initiators was 49.2 years versus 49.5 years for MTX initiators (p = 0.289). The percentage of females was similar among APR (53.9%) and MTX (55.1%) initiators (p = 0.36). Approximately 90% of each group was commercially insured. The prescriber specialty was significantly different between groups, with 22.2% of the MTX initiators receiving the index prescription from a rheumatologist compared with 2.5% of the APR initiators (p < 0.001). The mean number of Charlson comorbidities was similar among the two groups (APR vs MTX: 0.6 vs 0.5; p = 0.121), and 13.1% of APR users had a comorbid PsA diagnosis compared with 19.6% of the MTX group (p < 0.001). APR users were less likely than MTX users to have depression (9.9% vs 11.8%; p = 0.022) and hypertension (17.6% vs 20.0%; p = 0.017); however, for every other comorbidity of interest, the differences between the two groups were not statistically significant (Supplementary Table 2).
| Apremilast | Methotrexate | All | p-value | ||
|---|---|---|---|---|---|
| N (%) | 3288 (56.1) | 2572 (43.9) | 5860 (100) | ||
| Age, years | Mean (SD) | 49.2 (12.9) | 49.5 (13.2) | 49.3 (13.1) | 0.289 |
| Female | No. (%) | 1772 (53.9) | 1417 (55.1) | 3189 (54.4) | 0.360 |
| Insurance type | |||||
| Commercial | No. (%) | 2956 (89.9) | 2311 (89.9) | 5267 (89.9) | 0.949 |
| Medicare supplemental | No. (%) | 332 (10.1) | 261 (10.1) | 593 (10.1) | |
| Prescriber specialty | |||||
| Dermatologist | No. (%) | 1542 (46.9) | 1183 (46.0) | 2725 (46.5) | <0.001 |
| Rheumatologist | No. (%) | 83 (2.5) | 572 (22.2) | 655 (11.2) | |
| Primary care/PA/NP | No. (%) | 400 (12.2) | 196 (7.6) | 596 (10.2) | |
| Other/Unknown | No. (%) | 1263 (38.4) | 621 (24.1) | 1884 (32.2) | |
| Charlson Comorbidity Index | Mean (SD) | 0.6 (1.2) | 0.5 (1.1) | 0.6 (1.1) | 0.121 |
| No. of chronic conditions | Mean (SD) | 3.6 (2.1) | 3.7 (2.1) | 3.7 (2.1) | 0.077 |
| Psoriatic arthritis | No. (%) | 438 (13.3) | 505 (19.6) | 943 (16.1) | <0.001 |
| Pain medications | No. (%) | 1354 (41.2) | 1259 (49.0) | 2613 (44.6) | <0.001 |
| Glucocorticoids | No. (%) | 866 (26.3) | 935 (36.4) | 1801 (30.7) | <0.001 |
| Baseline total healthcare costs ($) | Mean (SD) [median] | 10,509 (26,679.6) [4324] | 8882 (17,296.8) [3845] | 9795 (23,049.3) [4123] | 0.005 |
NP: Nurse practitioner; PA: Physician assistant; SD: Standard deviation.
APR users were less likely than MTX users to be on pain medications (41.2% vs 49.0%; p < 0.001) and glucocorticoids (26.3% vs 36.4%; p < 0.001) at baseline (Table 1 & Supplementary Table 3). Last, mean baseline healthcare costs were higher among APR users than among MTX users (US$10,509 vs $8882; p = 0.005).
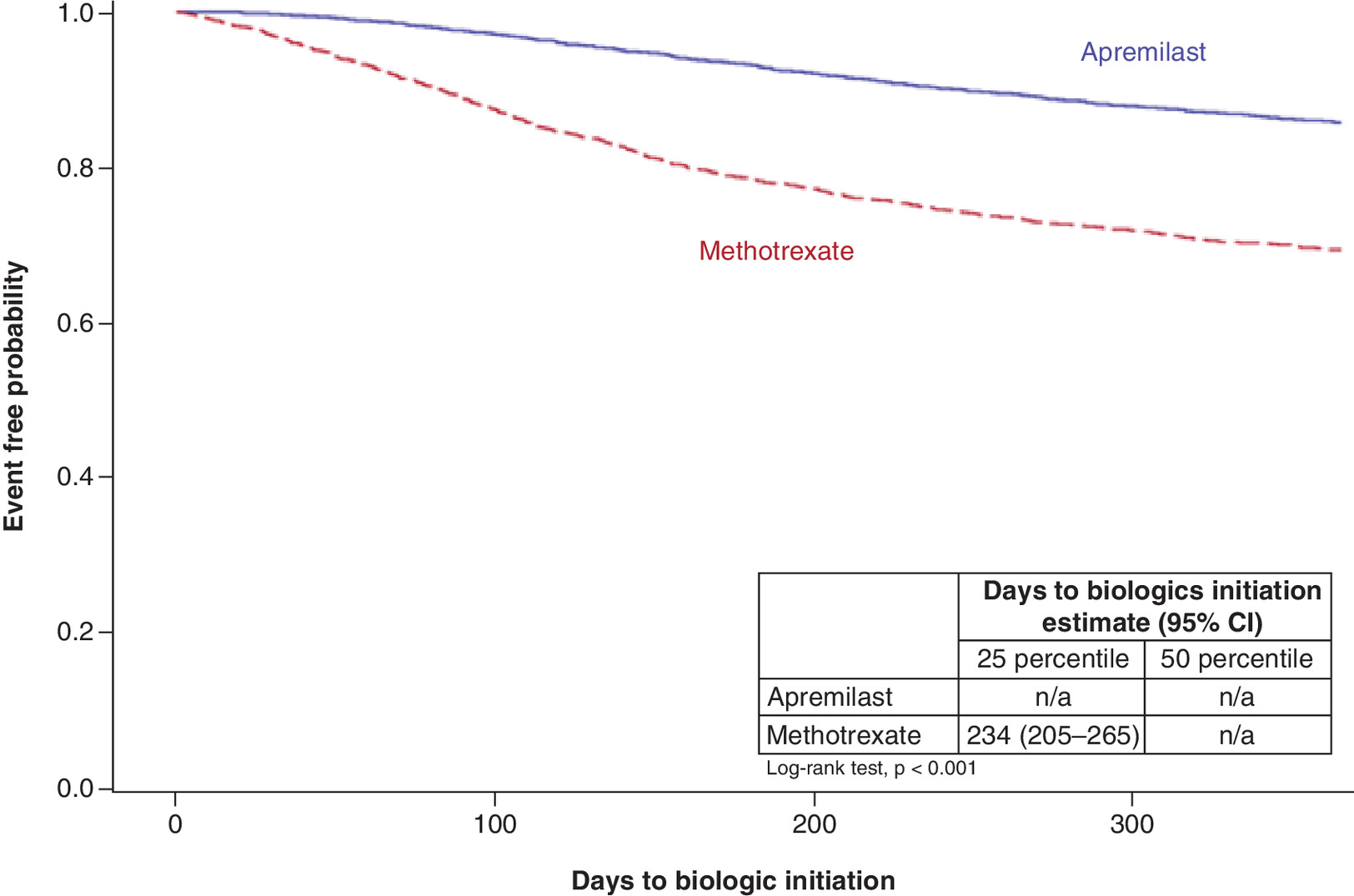
Fewer APR users initiated biologic treatment than MTX users throughout the 1-year follow-up period (Figure 1). During the first 3 and 6 months of follow-up, the unadjusted biologic initiation rates in the APR and MTX cohorts were 2.4% versus 10.7% (p < 0.001) and 6.8% versus 21.3% (p < 0.001), respectively. At the end of the 1-year follow-up, fewer APR patients (14.2%) than MTX patients (30.5%) initiated biologic treatment (Table 2).
| Apremilast | Methotrexate | All | p-value | ||
|---|---|---|---|---|---|
| N (%) | 3288 (56.1) | 2572 (43.9) | 5860 (100) | ||
| Biologic initiation rate during the 1-year follow-up period | No. (%) | 467 (14.2) | 785 (30.5) | 1252 (21.4) | <0.001 |
| Days to biologic initiation among patients who initiated biologic in 1 year | Mean (SD) | 188.4 (91.6) | 138.7 (92.2) | 157.2 (95.0) | <0.001 |
| Biologic initiation rate within 3 months | No. (%) | 79 (2.4) | 276 (10.7) | 355 (6.1) | <0.001 |
| Biologic initiation rate within 6 months | No. (%) | 222 (6.8) | 548 (21.3) | 770 (13.1) | <0.001 |
| PDC of index therapy during the 1-year follow-up period | Mean (SD) [median] | 0.574 (0.319) [0.575] | 0.458 (0.334) [0.384] | 0.523 (0.331) [0.493] | <0.001 |
| Duration of index therapy (60-day gap) during the 1-year follow-up period | Mean (SD) [median] | 226.5 (135.4) [241] | 178.3 (134.9) [142] | 205.3 (137.3) [189] | <0.001 |
| Discontinuation (≥60-day gap) | No. (%) | 1865 (56.7) | 1845 (71.7) | 3710 (63.3) | <0.001 |
| Restart following discontinuation | No. (%) | 235 (12.6) | 110 (6.0) | 345 (9.3) | <0.001 |
PDC: Proportion of days covered; SD: Standard deviation.
The mean time to biologic initiation during the 1-year follow-up was 188.4 days in the APR cohort compared with 138.7 days in the MTX cohort (p < 0.001) (Table 2). The most frequently used first biologic treatment was adalimumab for both the APR and MTX cohorts (Supplementary Tables 6 & 7).
APR users were more compliant to their index therapies. The mean proportion of days covered for the index therapy was 0.57 for the APR cohort and 0.46 for the MTX cohort (p < 0.001). The discontinuation rate of the index therapy was 56.7% for APR users and 71.7% for MTX users during the 1-year follow-up period (p < 0.001). Among patients who discontinued their index therapy, 12.6% of APR users and 6.0% of MTX users restarted after an index treatment gap of more than 60 days within the follow-up period (p < 0.001) (Table 2).
After adjusting for potential confounders, patients treated with APR maintained a lower risk of biologic initiation when compared with patients treated with MTX (hazard ratio: 0.45; 95% CI: 0.40–0.51; p < 0.001) (Table 3 & Supplementary Table 8).
| Cox regression (risk of biologic initiation during follow-up) | Logistic regression (any biologic use during follow-up) | |||
|---|---|---|---|---|
| HR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Patients with 1-year follow-up | 0.45 (0.40–0.51) | <0.001 | 0.42 (0.37–0.48) | <0.001 |
| Patients with 2-year follow-up | 0.56 (0.49–0.64) | <0.001 | 0.54 (0.46–0.63) | <0.001 |
HR: Hazard ratio; OR: Odds ratio.
The logistic model showed that the likelihood of biologic initiation was statistically significantly lower with APR treatment even after adjusting for potential confounders (odds ratio: 0.42; 95% CI: 0.37–0.48; p < 0.001) (Supplementary Table 4) with adjusted rates of biologic initiation being 14.4% (95% CI: 13.2–15.7%) for the APR cohort compared with 28.6% (95% CI: 26.8–30.5%) for the MTX cohort.
To evaluate the robustness of the findings, the analyses were repeated for a subgroup of patients who had at least 2 years of continuous enrollment after their index date. Findings were similar in this subgroup to ones in the main analysis.
Discussion
This study in an adult, systemic-naive PsO population with primary commercial or Medicare supplemental insurance found that patients treated with APR had a lower rate of, as well as longer time to, biologic initiation when compared with patients treated with MTX. These results were robust in patients with 1 and 2 years of follow-up after APR or MTX initiation, with differences being observed as early as 3 months post-index.
APR and MTX are both indicated for PsO, and real-world evidence shows that they are common first-line treatments for that disease. However, there are no randomized trials directly comparing APR to MTX in PsO. An indirect comparison based on data from clinical trials did not find a statistically significant difference in the efficacy of APR versus MTX [21].
Biologic initiation as an outcome may serve as a suitable proxy for suboptimal disease control in PsO, and it can easily be assessed from administrative claims databases. Previous studies demonstrated that higher disease activity is a predictor for biologic therapy initiation in PsO [22] and other autoimmune diseases such as rheumatoid arthritis [23–25].
Use of biologic initiation in PsO can be particularly helpful. Fluctuating symptoms, frequent dose adjustments and medication hoarding are typical in this condition. Therefore, other traditional treatment pattern measures used in claims studies, such as adherence or persistence, may be harder to interpret. Although low adherence is usually negatively associated with adequate control of disease, it is possible that patients with PsO experience periods of symptom control and temporarily pause treatment. This is consistent with the higher restart rate observed with APR.
In a cohort of patients with PsO, this study found that treatment with APR was associated with extended time to biologic initiation – the next line of treatment – when compared with MTX treatment. Future research using clinical measures could investigate whether biologic initiation is associated with disease progression, suboptimal disease control or toxicity in PsO. Research could also examine patient-specific and clinical factors associated with progression to biologic therapies.
Our study has several limitations. First, this study was a retrospective, observational analysis using large administrative claims data, thus randomized treatment assignment was not possible. Generally, administrative claims data lack possibly important clinical details providing information on disease severity and symptoms and thus does not allow to control for all potentially confounding variables. In particular, it is plausible that MTX users in our cohort have more severe disease than APR users and thus are more likely to switch to biologics. However, the modeling analyses included several measurable proxies of disease severity, such as prescriber specialty, pre-index healthcare costs and resource utilization, use of glucocorticoids and pain medications, and comorbidities/PsA. In addition, administrative claims data do not reflect whether medications are taken as prescribed. Thus, in studying adherence, only information regarding medication fills was considered. Finally, this study is limited to patients with commercial and Medicare supplemental insurance. Results may not be generalizable to other populations.
Conclusion
Systemic-naive adult PsO patients who initiated APR were more adherent to their index therapy and had a lower rate of biologic initiation when compared with patients initiating MTX. In addition, considering only patients who initiated a biologic during the follow-up period, the time to biologic initiation was longer among APR users than MTX users. APR use may delay biologic initiation in patients with PsO, suggesting better symptom control and outcome relative to MTX.
Future perspective
Direct clinical comparisons between APR and MTX in the treatment of PsO could be an important area of future research to better improve patient outcomes.
•
Apremilast (APR) and methotrexate (MTX) are oral small molecule (OSM) therapies approved by the US FDA for adult patients with psoriasis (PsO).
•
Some treatment guidelines recommend MTX and other conventional OSMs before APR and biologics; however, real-world evidence shows that APR and MTX are similarly used as first-line systemic therapies.
Materials & methods
•
We used 2014–2019 claims data from the IBM® MarketScan® Commercial and Medicare Supplemental databases.
•
The study population comprised of systemic-naive patients with PsO who started treatment with either APR or MTX between 1 January 2015 and 31 March 2018. PsO patients were identified via diagnosis codes; the first prescription date for APR or MTX was the index date. Patients were categorized by index treatment: APR or MTX.
•
Rates of biologic initiation during follow-up were compared between APR and MTX users by logistic and Cox regressions.
•
Models were adjusted for baseline covariates: age group, gender, region, prescriber specialty, comorbid PsA, Charlson Comorbidity Index, index year, nonalcoholic fatty liver disease, serious infection, pain medication and glucocorticoid utilization, healthcare utilization and healthcare costs.
Results
•
The likelihood of biologic initiation during follow-up was 58% lower (odds ratio: 0.42; 95% CI: 0.37–0.48; p < 0.001) for APR compared with MTX users.
•
APR users had a significantly lower adjusted rate of biologic initiation among APR versus MTX users (14.4% [95% CI: 13.2–15.7%] vs 28.6% [95% CI: 26.8–30.5%]).
•
APR users had lower risk of biologic initiation compared with MTX users (hazard ratio: 0.45; 95% CI: 0.40–0.51; p < 0.001) at any point in time during the 1-year follow-up.
Conclusion
•
In adults with primary commercial or Medicare supplemental insurance, systemic-naive patients with PsO on APR had a delay in biologic initiation compared with patients on MTX. Additionally, in patients who initiated a biologic during the follow-up period, the time to biologic initiation was longer among APR users than MTX users.
Author contributions
All authors made substantial contributions to the conception or design of the work, or the acquisition, analysis or interpretation of data for the work; drafted the work or revised it critically for important intellectual content; provided final approval of the version to be published; and made agreement to be accountable for all aspects of the work.
Financial & competing interests disclosure
The study was funded by Amgen, Inc. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed. E Chang, M Broder, C Paydar and K Bognar are employees of PHAR, which was hired by Amgen to conduct this study. J Yan was an employee of PHAR at the time of this study. S Richter was an employee of Amgen at the time of this study. P Desai was an employee of Amgen at the time of this study and owned stock in the company. I Khilfeh was an employee of Amgen at the time of this study.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
This study used deidentified patient records and did not involve the collection, use or transmittal of individually identifiable data; therefore, institutional review board approval to conduct this study was not necessary.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
References
Papers of special note have been highlighted as: • of interest
1.
Armstrong AW, Mehta MD, Schupp CW, Gondo GC, Bell SJ, Griffiths CEM. Psoriasis prevalence in adults in the United States. JAMA Dermatol. 157(8), 940 (2021).
• The current prevalence estimates of psoriasis, showing that the disease remains common, affecting 3.0% of the US adult population.
2.
Feldman SR, Goffe B, Rice G et al. The challenge of managing psoriasis: unmet medical needs and stakeholder perspectives. Am. Health Drug. Benefits 9(9), 504–513 (2016).
• This article highlights the complexity of psoriasis and unmet needs of patients afflicted by the disease.
3.
Menter A, Strober BE, Kaplan DH et al. Joint AAD-NPF guidelines of care for the management and treatment of psoriasis with biologics. J. Am. Acad. Dermatol. 80(4), 1029–1072 (2019).
• These guidelines cover the use of oral-systemic and nonbiologic medication in the treatment of psoriasis.
4.
Menter A, Gelfand JM, Connor C et al. Joint American Academy of Dermatology – National Psoriasis Foundation guidelines of care for the management of psoriasis with systemic nonbiologic therapies. J. Am. Acad. Dermatol. 82(6), 1445–1486 (2020).
• These guidelines cover the use of biologic agents in the treatment of psoriasis in adults.
5.
National Institute for Health and Care Excellence. Psoriasis: Assessment and Management (2017). www.nice.org.uk/guidance/cg153
6.
Amatore F, Villani A-P, Tauber M, Viguier M, Guillot B. The Psoriasis Research Group of the French Society of Dermatology (Groupe de Recherche sur le Psoriasis de la Société Française de Dermatologie). French guidelines on the use of systemic treatments for moderate-to-severe psoriasis in adults. J. Eur. Acad. Dermatol. Venereol. 33(3), 464–483 (2019).
7.
Kim WB, Jerome D, Yeung J. Diagnosis and management of psoriasis. Can. Fam. Physician 63(4), 278–285 (2017).
8.
Higa S, Devine B, Patel V, Baradaran S, Wang D, Bansal A. Psoriasis treatment patterns: a retrospective claims study. Curr. Med. Res. Opin. 35(10), 1727–1733 (2019).
• This study indicates that approximately 60% of patients with psoriasis initiated treatment with oral small molecules during the study period, whereas more than 40% initiated a TNF-α biologic therapy. Furthermore, more than 50% of the study population used concomitant topical therapy.
9.
US Food and Drug Administration. Reditrex Drug Label (2019). www.accessdata.fda.gov/drugsatfda_docs/label/2019/210737s000lbl.pdf
10.
UF Food and Drug Administration. Otezla Drug Label (2014). www.accessdata.fda.gov/drugsatfda_docs/label/2014/205437s000lbl.pdf
11.
Papp K, Reich K, Leonardi CL et al. Apremilast, an oral phosphodiesterase 4 (PDE4) inhibitor, in patients with moderate to severe plaque psoriasis: results of a phase III, randomized, controlled trial (Efficacy and Safety Trial Evaluating the Effects of Apremilast in Psoriasis [ESTEEM] 1). J. Am. Acad. Dermatol. 73(1), 37–49 (2015).
12.
Reich K, Gooderham M, Green L et al. The efficacy and safety of apremilast, etanercept and placebo in patients with moderate-to-severe plaque psoriasis: 52-week results from a phase IIIb, randomized, placebo-controlled trial (LIBERATE). J. Eur. Acad. Dermatol. Venereol. 31(3), 507–517 (2017).
13.
West J, Ogston S, Foerster J. Safety and efficacy of methotrexate in psoriasis: a meta-analysis of published trials. PLoS One 11(5), e0153740 (2016).
14.
Zweegers J, Otero M, Reek J et al. Effectiveness of biologic and conventional systemic therapies in adults with chronic plaque psoriasis in daily practice: a systematic review. Acta Derm. Venerol. 96(4), 453–458 (2016).
15.
Li X, Andersen KM, Chang H-Y, Curtis JR, Alexander GC. Comparative risk of serious infections among real-world users of biologics for psoriasis or psoriatic arthritis. Ann. Rheum. Dis. 79(2), 285–291 (2019).
16.
Asgari MM, Wu JJ, Gelfand JM et al. Validity of diagnostic codes and prevalence of psoriasis and psoriatic arthritis in a managed care population, 1996-2009. Pharmacoepidemiol. Drug Saf. 22(8), 842–849 (2013).
17.
Wu JJ, Pelletier C, Ung B, Tian M. Real-world treatment patterns and healthcare costs among biologic-naive patients initiating apremilast or biologics for the treatment of psoriasis. J. Med. Econ. 22(4), 365–371 (2019).
18.
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J. Chronic. Dis. 40(5), 373–383 (1987).
19.
Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J. Clin. Epidemiol. 45(6), 613–619 (1992).
20.
Agency for Healthcare Research and Quality. HCUP Chronic Condition Indicator (CCI) for ICD-9-CM. (2015). www.hcup-us.ahrq.gov/toolssoftware/chronic/chronic.jsp
21.
Armstrong AW, Betts KA, Sundaram M, Thomason D, Signorovitch JE. Comparative efficacy and incremental cost per responder of methotrexate versus apremilast for methotrexate-naïve patients with psoriasis. J. Am. Acad. Dermatol. 75(4), 740–746 (2016).
22.
Geale K, Henriksson M, Schmitt-Egenolf M. Evaluating equality in psoriasis healthcare: a cohort study of the impact of age on prescription of biologics. Br. J. Dermatol. 174(3), 579–587 (2016).
• This study highlights that increased disease activity is a predictor of biologic initiation.
23.
DeWitt EM, Lin L, Glick HA, Anstrom KJ, Schulman KA, Reed SD. Pattern and predictors of the initiation of biologic agents for the treatment of rheumatoid arthritis in the United States: an analysis using a large observational data bank. Clin. Ther. 31(8), 1871–1880 (2009).
24.
Verstappen SMM, Lunt M, Bunn DK, Scott DGI, Symmons DPM. In patients with early inflammatory polyarthritis, ACPA positivity, younger age and inefficacy of the first non-biological DMARD are predictors for receiving biological therapy: results from the Norfolk Arthritis Register. Ann. Rheum. Dis. 70(8), 1428–1432 (2011).
25.
Png WY, Kwan YH, Lim KK et al. A systematic review of the factors associated with the initiation of biologicals in patients with rheumatological conditions. Eur. J. Hosp. Pharm. 26(3), 163–169 (2019).
Information & Authors
Information
Published In
Pages: 575 - 582
PubMed: 35514324
Copyright
© 2022 Amgen Inc. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 27 December 2021
Accepted: 12 April 2022
Published online: 6 May 2022
Keywords:
Topics
Authors
Funding Information
Amgen Inc.
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Biologic initiation rates in systemic-naive psoriasis patients after first-line apremilast versus methotrexate use. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0311
Export citation
Select the citation format you wish to export for this article or chapter.