An impact evaluation of an education bundle for patients at risk of developing venous thromboembolism
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Among hospitalized patients, venous thromboembolism (VTE) is a preventable cause of morbidity and mortality. This study analyzed the effects of a large-scale adoption of a prompt response and education protocol to increase VTE prophylaxis adherence in the USA. Methods: A Markov model was developed that simulates outcomes and costs of delivering a VTE education bundle versus not, to hospitalized at-risk patients. Results: The education bundle could avert more than 134,000 VTEs, 552,000 hospital days and 19,000 deaths over 5 years. Patients could save 13 million hours in work absenteeism and travel time, valued at US$237 million. Total societal savings could amount to US$2.8 billion. In scenario analyses with assumed lower-effectiveness estimates, the bundle averts 16,000 VTEs, 67,000 hospital days and 2000 deaths. Conclusion: A nationwide rollout of an education bundle to reduce missed doses of prescribed prophylaxis could improve quality of care, resulting in a decline in VTEs and mortality.
Plain language summary
In a previous study, an education bundle was designed to increase administration of medication to prevent blood clotting among hospitalized patients at risk of venous thromboembolism (VTE). The education bundle led to a decrease in patients missing those needed doses of medication. The current study estimates the economic impacts of a nationwide rollout of the education bundle for patients at risk of VTE. The results show that if the education bundle were rolled out nationally, it could result in 134,000 fewer VTEs, 552,000 fewer days spent in the hospital and 19,000 fewer deaths over 5 years. As a result of reduced medical care, less time off work, and informal caregiving needed, societal cost savings could be as much as US$2.8 billion.
Background
Approximately 500,000 venous thromboembolism (VTE) events occur in the USA annually, half of which are associated with a recent hospitalization [1]. The economic burden and health consequences of VTEs are significant. Incident VTEs account for approximately US$7 billion to $10 billion in annual health spending [2]. The development of VTE is also associated with heightened mortality risk directly attributable to the VTE. Alotaibi and colleagues [3] found a 9.2% case fatality rate in the year following the formation of VTE. Other research points to much higher mortality rates as a result of VTE, suggesting that these data may underestimate mortality [4].
Physician guidelines note that hospital-acquired VTEs are preventable and strongly recommend the use of anticoagulants for prophylaxis for at-risk hospitalized patients [5]. Despite these guidelines, non administration is common and associated with VTE formation [6]. Non administration is defined here as any prescribed VTE prophylaxis dose that is not administered. Research has found that non administration of pharmacologic anticoagulants for prophylaxis increases alongside increased prescription of VTE prophylaxis, suggesting a need for interventions specifically targeting non administration of anticoagulants for prophylaxis [7]. A study of rates of adherence to VTE prophylaxis administration found patient refusal to be the most common reason for non administration [8]. This finding suggests the need for educational interventions aimed at reducing patient refusal and nurse non administration to improve adherence to guidelines [9], in which optimal VTE prevention care is delivered consistent with individual risk and patient preference.
The VTE education bundle
Haut and colleagues [10] studied the effect of real-time delivery of a patient-centered education bundle on non administration of low molecular weight heparins. The study consisted of 19,652 adult patient visits in medical and surgical units in the Johns Hopkins Hospital in Baltimore, Maryland. The intervention consisted of a real-time alert system that would page and email a health educator when a bedside nurse documented non administration of a prescribed dose of VTE prophylaxis. If the alert resulted from bedside nurse non administration, the bundle was delivered to the bedside nurse. The education bundle delivered information to patients via three methods, based on patient preference: a face-to-face discussion with the health educator, a two-page paper handout or a 10-minute educational video [11]. Each method provided patients with information about VTE, the mortality rate associated with VTE, its long-term complications, signs of its formation, tools to aid in its prevention and methods to handle VTE after formation.
A convenience sample of two surgical and two medical units was chosen to receive the intervention, and the hospital’s remaining five surgical and seven medical units did not receive the intervention. The overall proportion of VTE events decreased among all patients from the preintervention to postintervention periods; VTE events decreased by 40.0% in the intervention group and 16.6% in the comparison group, although neither decrease was statistically significant. The intervention did significantly decrease the conditional odds of VTE prophylaxis nonadministration from preintervention to postintervention periods: 9.1% (95% CI: 5.2–16.2%) versus 5.6% (95% CI: 3.1–9.9%; odds ratio [OR]: 0.57, 95% CI: 0.48–0.67) compared with no change on control units, 13.6% (95% CI: 9.8–18.7%) versus 13.3% (95% CI: 9.6–18.5%; OR: 0.98, 95% CI: 0.91–1.07); p < 0.001 for interaction. The intervention demonstrated improved quality of care and is in line with recommendations of a review of VTE prevention in emergency general surgery [12]. To reduce preventable harm, clinicians should ensure that patients receive all prescribed prevention therapies, or ‘defect-free care’ [13]. By reducing nonadministration, this education bundle aided defect-free care and aimed to improve adherence to guidelines.
Methods
An impact analysis was conducted to estimate the effects of a hypothetical national implementation of the real-time, patient-centered education bundle designed by Haut and colleagues [10]. A Markov model was constructed in Microsoft Excel (version 2012) to simulate patient outcomes and related medical and nonmedical costs of implementing the VTE education bundle compared with not implementing the bundle, referred to here as the control. Patients cycle through the six-state Markov model using transition probabilities informed by the literature; see Figure 1 for the model figure, Supplementary Table 1 for model inputs and the following section for a description of how patients cycle through the model.

Figure 1. Impact analysis model for the venous thromboembolism education bundle patient population.
Note: Patients can exit the model via death from any model state.
Hosp: Hospital; VTE: Venous thromboembolism.
State transition model overview
All patients start out hospitalized and at risk of developing VTE. The population modeled are those who would be prescribed anticoagulant prophylaxis for hospital-acquired VTE prevention and therefore are eligible to receive the education bundle intervention if a dose is missed. In the intervention group, patients receive the education bundle if they miss a dose of medication; in the control group, patients do not receive the bundle if they miss a dose, increasing their probability of developing VTE predischarge. If they develop VTE predischarge, surviving patients transition to the post-VTE health state, where they remain unless they have a recurrent VTE. If patients do not develop VTE predischarge, they transition to the no-VTE health state, where they remain unless they develop a hospital-related VTE (related to the initial hospitalization). If patients develop a hospital-related VTE, they transition to the hospital-related VTE health state, where they remain for one cycle; survivors then transition to the post-VTE health state as described previously (Figure 1). The probability of moving from the hospitalized at risk of VTE state to developing a VTE varies for surgical/trauma and medical patients. Mortality is modeled using background mortality (applied to all health states), hospital-related (applied to the initial hospitalization only), VTE-related (applied to those who develop a VTE) and post VTE-related (applied to the post-VTE health state) mortality rates.
Outcomes such as VTE events, hospital days and mortality were included, as were medical, nonmedical, patient, family and employer costs. The base-case analysis took a societal perspective, which incorporates patient and caregiver time and out-of-pocket expenses, an estimate of absenteeism costs from the employer’s perspective, and payer and provider costs. The model took a 5-year time horizon using 3-month cycle lengths. All costs are reported using 2020 prices. Healthcare cost estimates from earlier years were inflated using a price index for health expenditures [14]. This research was conducted according to the principles in the Declaration of Helsinki.
Model parameters
Model inputs were collected from publicly available data sources, peer-reviewed literature and clinical expert input. Supplementary Table 1 provides a full list of these inputs.
Population parameters
The model follows a single cohort over a 5-year time horizon. The cohort represents the hospitalized US population at risk for developing VTE. An estimated 12 million patients a year experience a procedure or medical event during hospitalization that puts them at risk of VTE [15]; these 12 million patients cycle through the model and accumulate costs and outcomes. These 12 million patients were split into two risk groups of 4.3 million surgical patients and 7.7 million medical patients [15]. Patients in these risk groups were subsequently assigned differing VTE risk estimates, following the literature. Because the study was modeling patients at increased risk of VTE, more potential VTEs could be prevented by the intervention than would be present in the general hospitalized population. Patients entered at age 55 years, which was the average age of patients participating in the VTE education bundle study [10].
Healthcare utilization parameters
For patients who received the intervention, the average reduction in pharmacologic missed doses was calculated as 0.632 doses per patient using estimates from Haut and colleagues [10], and the cost of the additional dose per participant receiving the intervention was modeled. The decrease in VTE events as measured by administrative codes (PSI-12, Perioperative Pulmonary Embolism or Deep Vein Thrombosis Rate) observed by Haut and colleagues [10] was not found to be statistically significant.
Although Haut and colleagues [10] were significantly powered to observe a statistically significant change in the rate of prophylaxis administration, the study was underpowered to observe a significant decline in VTEs within and across VTE risk groups, and few VTEs were observed in the trial. Louis and colleagues found a statistically significant association between missed doses of prophylaxis and VTEs among trauma and general surgery patients, in which 23.5% of trauma and general surgery patients who missed at least one dose of prophylaxis experienced a VTE compared with 4.8% of patients who missed zero doses [6]. Estimates from Louis and colleagues [6] were applied to the 4.3 million general surgery patients in the at-risk for VTE population, and estimates from Haut and colleagues [10] were applied to the rest of the at risk for VTE population to estimate the rates of patients experiencing VTEs across risk groups in the intervention and control. Total hospital days, VTE events and VTE follow-up visits made up the remaining outcome parameters. A shorter length of stay (LOS) was modeled for patients not experiencing VTE during initial hospitalization. Patients experience an estimated 2.89 additional follow-up visits per VTE event [16]. Supplementary Table 1 provides the full list of model parameters.
Mortality
Patients can die at any point as they transition through the model. Background mortality was applied to all health states, and event-specific mortality was applied to the relevant health state. Event-specific mortality rates included a general hospital-related rate (for initial hospitalization that did not result in VTE), VTE-specific rate (for all initial hospitalization VTEs and future VTEs) and increased risk of mortality following VTE applied to the post-VTE health state.
Healthcare cost parameters
Direct medical costs include cost of hospitalization, post-VTE medical costs, and cost of the additional pharmacologic prophylaxis dose in the intervention arm. Out-of-pocket costs for inpatient stays were estimated by creating an out-of-pocket cost to total cost ratio, constructed from the ratio of total costs to out-of-pocket costs for all medical events in the Medical Expenditure Panel Survey (MEPS). This ratio was multiplied by the total cost of inpatient stays found by Cohoon and colleagues [17].
Provider (intervention) cost parameters
The original Haut and colleagues study [10] had a dedicated health educator who delivered the intervention. In a later dissemination study [18], all floor nurses received training and delivered the intervention, because most hospitals would not hire a new health educator just to deliver this intervention. It was assumed that removing the dedicated health educator did not affect the observed decrease in VTE events used in the model. The responsibility of delivering the intervention was assumed to be split by all nurses providing care for the at-risk population (see all other assumptions in Supplementary Table 2). Nurses would be required to undergo a one-time, 30 min online training to deliver this intervention. Material costs modeled included the cost of printing the paper handout given as an option for the education bundle. The other options for providing the intervention were assumed not to incur any costs because face-to-face discussion was assumed to be a standard nurse responsibility and the educational video was made freely available on the internet. Intervention costs include nurses’ wages (for the time spent in training), the cost of the online training, and the paper and printing costs for the education bundle. The cost of the training module for providers was estimated to be approximately US$11 per nurse. Other intervention costs included the cost of implementing the real-time alert system in hospitals. These costs were calculated based on author’s assumptions of time to implement the real-time alert system at the wage of a software developer [19]. Maintenance costs were also included for each subsequent year. These costs were assumed across all US hospitals [20].
Patient time, travel & productivity cost parameters
Patient time, travel and employer productivity cost parameters were estimated between the control and intervention arms. Patient time included time spent receiving VTE-related medical care, including time in the hospital and follow-up visits. Patient total time and absenteeism time were estimated from average LOS for VTE and non-VTE hospitalization. Absenteeism time was estimated as a 5-day workweek of 40 h. Productivity loss to employers was estimated by multiplying the labor force participation rate among Americans aged 55 years and older [10] by the estimated absenteeism hours resulting from hospitalization and follow-up visits and an average patient wage of US$35.96 [21]. A similar estimate was created for productivity losses to patients’ families and friends serving as caregivers. The caregiver wage rate used was an estimate of the median wage for nursing and home health aides [21]. Travel costs were estimated using a nationwide median distance between patients’ homes and the closest hospital [22], a standard mileage rate of 59 cents per mile for 2020 from the Internal Revenue Service [23] and the number of follow-up visits for patients who experience VTE (estimated from the work of Spyropoulos and Lin [16]). Please see Supplementary Table 1 for a table of all parameter values and their sources.
Model assumptions
The model required several assumptions, listed in Supplementary Table 2.
Sensitivity analyses
One-way & probabilistic sensitivity analyses
To explore uncertainty in the model estimates, one-way analysis and probabilistic sensitivity analysis (PSA) were performed. One-way sensitivity analysis involved varying each model input, one at a time, to determine how each input affected total costs. The results are presented graphically as a tornado diagram identifying primary cost drivers in the model. PSA was conducted to allow for uncertainty in the estimation of all parameters within the model. Each input parameter was assigned a probability distribution and a range for which the default input would vary in PSA. The range was informed by 95% CIs found in the literature, a credible range, or a 20% increase and decrease in the default input. PSA jointly varied model inputs over 1000 simulations from these distributions to estimate the average VTE events, hospital days, mortality, medical costs and nonmedical costs for each group. Then, 95% credible range estimates were calculated for each model outcome based on these results. Additional analyses examined time horizons from 1 to 10 years.
Scenario analyses
There is a dearth of evidence surrounding the quantitative relationship between missed doses and the effectiveness of VTE prophylaxis. Only two studies examining this relationship were identified: a case–control study [24] and a prospective study [6]. Potential upper and lower bound scenario analyses were performed using effectiveness estimates from the prospective study [6], where a significant decline in VTEs was observed for those who did not miss any doses of pharmacologic VTE prophylaxis. Louis and colleagues [6] observed VTEs in 23.5% of participants who missed one or more doses versus 4.8% who did not miss any doses (p < 0.01). These estimates were used to inform an upper bound effectiveness scenario for the population at risk for VTE over a 1-year time horizon (risk of in-hospital VTE of 23.5% applied to control and 4.8% applied to intervention). A lower bound effectiveness scenario was modeled to reflect minimal difference between surgical/trauma and medical patients (6.0% risk in control vs 5.0% risk in intervention).
Results
Model results show a decline in hospital-related VTE events from 1,500,000 to 1,365,000 (a 9% decrease) over 5 years as a result of nationwide implementation of the education bundle. This decline in VTE events results in more than 552,000 fewer days spent in the hospital (95% CI: 402,000–1,049,000) and 19,000 fewer deaths (95% CI: 14,000–38,000) over 5 years. The intervention reduces total missed pharmacologic doses by 7,641,609. Total societal costs decrease by US$2.8 billion (95% CI: $1.5 billion–$4.5 billion) in health-related spending. Of this decrease in societal cost, approximately US$2.7 billion is attributable to decreased direct medical costs (Table 1).
| Outcome | Control group | Intervention group | Difference (control minus intervention) | Per patient |
|---|---|---|---|---|
| Outcomes | ||||
| – Number of VTE events | 1,500,733 | 1,365,853 | 134,880 | 0.00 |
| – Number of hospital days (post initial hospitalization) | 45,520,670 | 44,968,680 | 551,990 | 0.00 |
| – Number of deaths | 1,823,942 | 1,804,956 | 18,986 | 0.00 |
| – Increase in doses | 0 | 7,641,608 | N/A | 0.632 |
| Provider perspective (intervention only) | ||||
| – Nurse training costs ($) | 0 | 204,820,000 | -204,820,000 | -17 |
| – Printing costs ($) | 0 | 73,142 | -73,142 | 0 |
| – Real-time alert system costs ($) | 0 | 116,421,165 | -116,421,165 | -10 |
| – Total costs ($) | 0 | 321,314,307 | -321,314,307 | -27 |
| Patient perspective | ||||
| – Total hours of lost time | 1,096,829,500 | 1,083,192,275 | 13,637,225 | 1.13 |
| – Indirect costs (travel) ($) | 69,343,965 | 67,693,479 | 1,650,486 | 0.14 |
| – Direct medical costs ($) | 14,048,250,046 | 13,813,255,333 | 234,994,713 | 19.44 |
| – Additional prophylaxis cost (intervention) ($) | 0 | 46,528,034 | -46,528,034 | -3.85 |
| – Total costs ($) | 14,117,594,011 | 13,880,948,812 | 236,645,199 | 19.57 |
| Payer perspective | ||||
| – Direct medical costs ($) | 163,104,537,885 | 159,914,691,304 | 3,189,846,581 | 263.82 |
| – Additional prophylaxis cost (intervention) ($) | 0.00 | 313,296,857 | -313,296,857 | -25.91 |
| – Medicare costs ($) | 91,827,854,829 | 90,031,971,204 | 1,795,883,625 | 148.53 |
| – Medicaid costs ($) | 8,909,585,382 | 8,735,340,012 | 174,245,370 | 14.41 |
| – Other payer costs ($) | 62,367,097,674 | 61,147,380,087 | 1,219,717,587 | 100.88 |
| – Total costs ($) | 163,104,537,885 | 60,227,988,161 | 2,876,549,725 | 237.91 |
| Family perspective | ||||
| – Hours of absenteeism | 131,857,596 | 130,652,756 | 1,204,840 | 0.10 |
| – Total absenteeism cost ($) | 2,083,350,014 | 2,064,313,538 | 19,036,476 | 1.57 |
| Employer perspective | ||||
| – Hours of absenteeism | 140,975,408 | 139,687,255 | 1,288,154 | 0.00 |
| – Total absenteeism cost ($) | 5,069,475,683 | 5,023,153,676 | 46,322,007 | 3.83 |
| Societal perspective | ||||
| – Total direct medical costs ($) | 177,152,787,931 | 174,362,557,800 | 2,790,230,131 | 230.77 |
| – Total additional prophylaxis cost (intervention) ($) | 0 | 359,824,891 | -359,824,891 | -29.76 |
| – Total costs ($) | 184,374,957,593 | 181,517,718,493 | 2,857,239,100 | 236.31 |
N/A: Not applicable; VTE: Venous thromboembolism.
Provider (intervention) costs total an additional US$321 million (95% CI: $456 million–$215 million) over 5 years. Most of these costs come from implementing the alert system (US$116 million), nurse training (US$205 million) and printing (US$73,000), equating to approximately US$27 per patient. From the patient perspective, patients save 13 million hours (95% CI: 9,935,000–25,626,000) of lost time, equating to 1.3 million fewer hours absent from work. Decreased travel costs from fewer follow-up post-VTE visits save patients approximately US$1.6 million. Patients in the intervention also experience fewer total costs as a result of reduced hospitalization, with savings of about US$235 million, or US$20 per patient.
In the control group, payers spend approximately US$163 billion in direct medical costs for patients with or at risk of VTE. In the intervention group, this amount decreases by approximately US$2.9 billion as a result of decreased VTEs, despite an increase of about US$313 million in VTE prevention medication costs. In total, direct medical costs from the payer perspective decrease by about US$2.8 billion, or $238 per patient.
Employers experience 1.3 million reduced absenteeism hours, equaling approximately US$46 million, or $4 per patient. Families and caregivers of patients also experience fewer hours of absenteeism as a result of decreased VTEs: approximately 1.2 million (95% CI: 910,000–2,200,000) in absenteeism hours for family caregivers and more than US$19 million (95% CI: $14 million–$37 million) in caregiving costs, or $2 per patient caregiver.
One-way sensitivity analysis
Figures 2 & 3 show the ranges of potential savings, costs and distributional assumptions for each input parameter. Tornado diagrams were produced to visualize the sensitivity of model outcomes. Figure 2 displays one-way sensitivity analysis results from the societal perspective, whereas Figure 3 illustrates these results from the patient perspective. The control estimate for surgical/trauma patients demonstrates the most societal cost uncertainty, with a range of potential savings from US$1.7 billion to $3.9 billion. The control estimate for surgical/trauma patients also demonstrates the most uncertainty for patient total costs, with potential savings ranging from US$151 million to $322 million, depending on how this measure is varied (Figures 2 & 3).
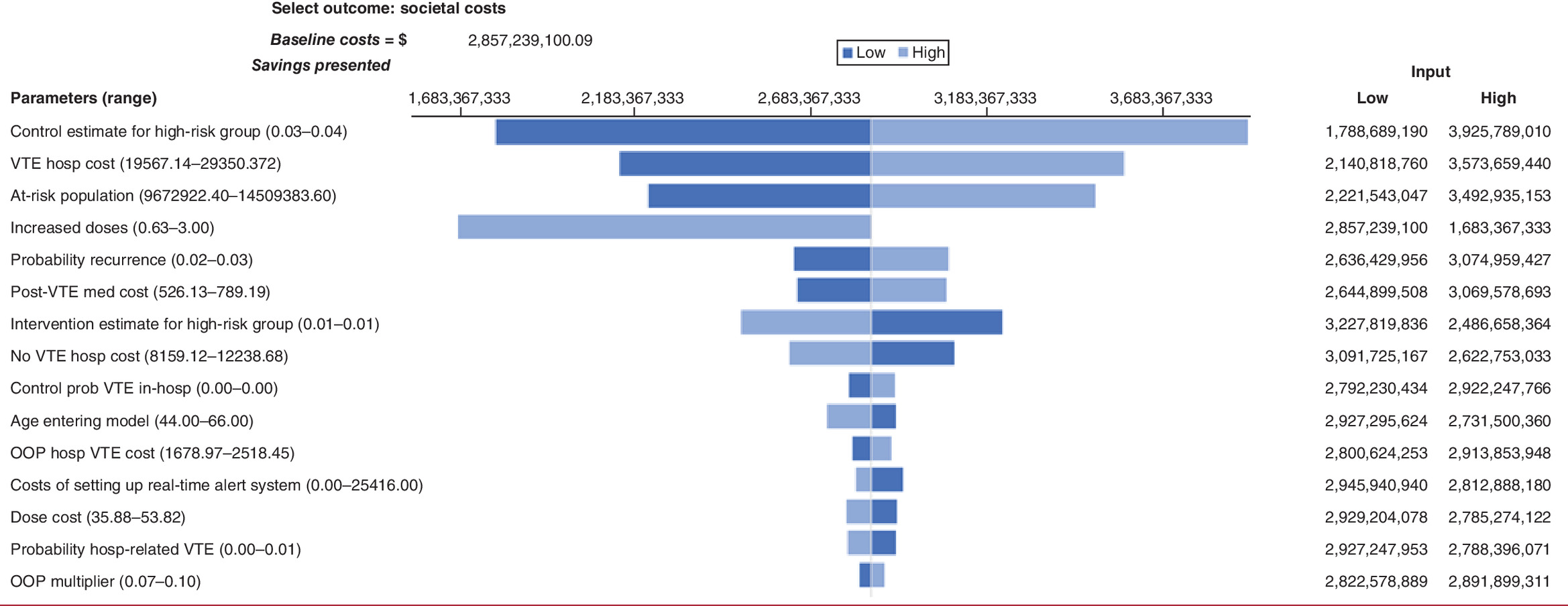
Figure 2. Tornado diagram of total societal costs.
Hosp: Hospitalization; MR: Mortality rate; OOP: Out-of-pocket; Prob: Probability; VTE: Venous thromboembolism.
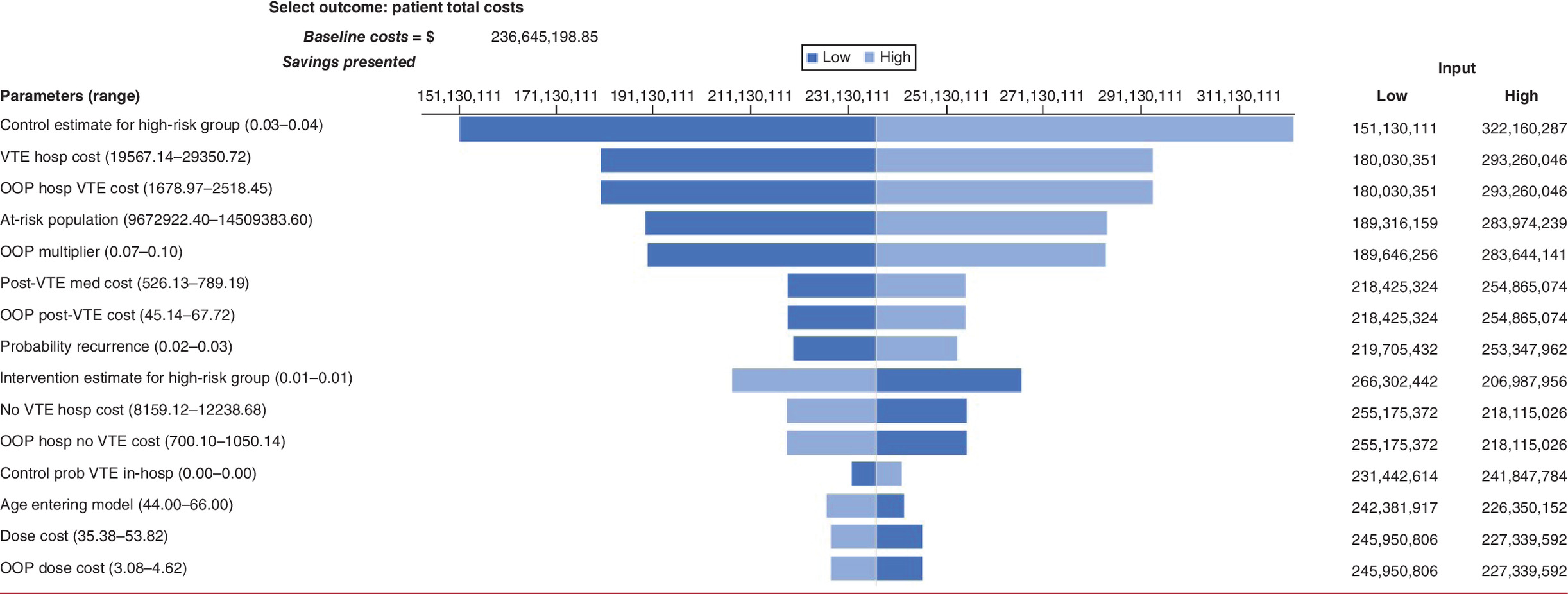
Figure 3. Tornado diagram of patient total costs.
Hosp: Hospital; MR: Mortality rate; OOP: Out-of-pocket; Prob: Probability; VTE: Venous thromboembolism.
Ranges for the cost of setting up the real-time alert system were set between US$0 and $25,416 for 5235 US hospitals [20]. The lower bound of zero was chosen for the possibility that hospitals would already have real-time alert systems implemented in their existing systems. The input parameter and upper bound were based on potential time estimates to complete the implementation of the real-time alert system [19]. Varying these costs ranges total societal cost savings between US$2.8 billion and $2.9 billion. Annual maintenance costs following the initial setup of the real-time alert system vary between US$0 and $3177. The lower and upper ranges of these annual maintenance costs causes total societal costs to vary between US$2.801 billion and $2.885 billion.
Results of the PSA based on 1000 iterations of the model are shown in Table 2. Total societal cost estimates of implementing the education bundle versus not implementing it range from US$1.3 billion to $4.7 billion in savings.
| Outcome | Impacts avoided or cost savings | Credible range lower bound | Credible range upper bound |
|---|---|---|---|
| Outcomes | |||
| – Number of VTE events | 134,880 | 87,541 | 197,331 |
| – Hospital days | 551,990 | 309,312 | 885,354 |
| – Deaths | 18,986 | 11,959 | 28,244 |
| Patient perspective | |||
| – Patient time (h) | 13,637,225 | 7,728,197 | 21,809,045 |
| – Indirect costs (transportation) ($) | 1,650,486 | 839,208 | 2,829,105 |
| – Direct medical costs ($) | 281,522,747 | 158,175,871 | 454,142,458 |
| – Total costs ($) | 236,645,199 | 115,175,871 | 405,446,724 |
| Provider perspective | |||
| – Intervention costs ($) | -321,314,307 | -443,998,613 | -214,665,977 |
| Payer perspective | |||
| – Direct medical costs ($) | 2,876,549,725 | 1,455,346,606 | 4,551,938,990 |
| Family perspective | |||
| – Unpaid caregiving time (h) | 1,204,840 | 736,164 | 1,767,342 |
| – Total cost of unpaid caregiving ($) | 19,036,476 | 11,064,758 | 29,187,344 |
| Employer perspective | |||
| – Productivity loss (h) | 1,288,154 | 741,036 | 1,815,148 |
| – Total cost of productivity loss ($) | 46,322,007 | 25,238,035 | 66,770,039 |
| Societal perspective | |||
| – Total direct medical costs ($) | 2,790,230,131 | 1,271,387,707 | 4,556,494,386 |
| – Total costs ($) | 2,857,239,100 | 1,316,280,209 | 4,645,687,732 |
VTE: Venous thromboembolism.
Savings as a result of the intervention increased as the time horizon increased (Table 3). For example, going from 5 to 10 years increases the savings of the intervention by about US$1.1 billion, or $94.64 per patient.
| Time horizon | Control ($) | Intervention ($) | Difference (control minus intervention) ($) | Per patient ($) |
|---|---|---|---|---|
| Societal perspective | ||||
| 1 year | 146,424,255,761 | 145,087,628,416 | 1,336,627,346 | 110.55 |
| 2 years | 154,939,522,444 | 153,162,426,508 | 1,777,095,937 | 146.97 |
| 3 years | 164,189,591,182 | 162,013,964,367 | 2,175,626,815 | 179.94 |
| 4 years | 174,043,122,051 | 171,508,297,493 | 2,534,824,558 | 209.64 |
| 5 years | 184,374,957,593 | 181,517,718,493 | 2,857,239,100 | 236.31 |
| 6 years | 195,065,987,564 | 191,920,639,222 | 3,145,348,342 | 260.14 |
| 7 years | 206,002,902,617 | 202,601,355,462 | 3,401,547,155 | 281.33 |
| 8 years | 217,078,663,463 | 213,450,505,089 | 3,628,158,374 | 300.07 |
| 9 years | 228,193,449,927 | 224,366,004,515 | 3,827,445,411 | 316.55 |
| 10 years | 239,255,480,708 | 235,253,867,040 | 4,001,613,668 | 330.95 |
Scenario analysis
Based on findings from Louis and colleagues [6], two additional scenarios were explored varying the rate of VTE for patients receiving the education bundle. These included upper and lower bound effectiveness scenarios (Table 4).
| Outcome | Control | Intervention | Difference (control minus intervention) | Per patient |
|---|---|---|---|---|
| Upper bound outcomes | ||||
| – Number of VTE events | 1,634,928 | 1,368,778 | 266,150 | 0 |
| – Number of hospital days (post initial hospitalization) | 46,069,854 | 44,980,649 | 1,089,205 | 0 |
| – Number of deaths | 1,842,831 | 1,805,367 | 37,464 | 0 |
| Upper bound societal perspective | ||||
| – Total direct medical costs ($) | 180,606,511,584 | 174,437,827,679.32 | 6,168,683,904.46 | 510.18 |
| – Total additional prophylaxis cost (intervention) ($) | 0.00 | 359,824,891 | -359,824,891 | -29.76 |
| – Total costs ($) | 187,895,349,595 | 181,594,441,331.16 | 6,300,908,263.75 | 521.12 |
| Lower bound outcomes | ||||
| – Number of VTE events | 1,385,229 | 1,368,778 | 16,451 | 0 |
| – Number of hospital days (post initial hospitalization) | 45,047,974 | 44,980,649 | 67,326 | 0 |
| – Number of deaths | 1,807,683 | 1,805,367 | 2,316 | 0 |
| Lower bound societal perspective | ||||
| – Total direct medical costs ($) | 174,180,087,202 | 174,437,827,679.32 | -257,740,476.92 | -21.32 |
| – Total additional prophylaxis cost (intervention) ($) | 0.00 | 359,824,891 | -359,824,891 | -29.76 |
| – Total costs ($) | 181,344,873,857 | 181,594,441,331.16 | -249,567,473.95 | -20.64 |
The upper bound effectiveness scenario used a predischarge VTE rate of 23.5% for patients not receiving any intervention and 5% for patients receiving the education bundle. This scenario suggested cost savings of approximately US$6.3 billion after 5 years (95% CI: $3.6 billion–$9.4 billion) and included 266,000 fewer VTE events (95% CI: 185,000–367,000) and more than 37,000 fewer deaths (95% CI: 24,000–52,000).
The lower bound effectiveness scenario assumed more similar predischarge VTE rates between the intervention and control groups. In this scenario, 6% of patients who did not receive any intervention experienced VTE versus 5% of patients who received the education bundle. The lower bound effectiveness scenario outcomes suggested costs of approximately US$249 million after 5 years (95% CI: -$1 billion–$619 million). This includes 16,000 fewer VTE events (95% CI: -6,000–40,600) and 2316 fewer deaths (95% CI: -801–5,684).
The results for the lower bound scenario showed wide ranges that cross zero, indicating uncertainty about the costs and savings of the intervention when effectiveness decreased for the hypothetical subset of high-risk patients under the lower bound effectiveness scenario conditions.
Discussion
A variety of interventions to improve appropriate prescription of VTE prophylaxis have been developed [25], including ones aimed at improving prescription of pharmacologic prophylaxis by increasing pharmacists’ and doctors’ ability to identify at-risk patients. Other interventions create electronic alerts to warn attending physicians when their at-risk patients do not receive prophylaxis. A common thread throughout these interventions is that they attempt to improve prescription of pharmacologic prophylaxis but do not necessarily focus on the administration of prophylaxis following prescription. Haut and colleagues [10] provide an intervention aimed at improving prophylaxis administration to optimize adherence to VTE prophylaxis regimens. The analysis in this study estimates costs of and savings from this intervention. Much of the work on the economic burden of VTE has focused on immediate and long-term complications as a result of VTE and VTE recurrence, with comparatively little research on the economic effects of hospital-acquired VTE prevention interventions [2].
This study further characterizes potential uncertainty (in costs and outcomes) of bundle implementation. The main cost of implementing the education bundle is training all nurses in a unit to deliver the intervention. Per nurse, these training costs are minimal; a 30-minute online training costs about US$11. However, the costs of training all nurses are considerable compared with the bundle’s uncertain effect on significantly reducing VTEs.
Limitations
This study has several limitations. First, evidence surrounding the decline in VTEs following increased administration of prescribed doses of VTE prophylaxis is limited and mixed [24]. Louis and colleagues [6] found a correlation between missed doses and increased incidence of deep vein thrombosis (DVT) in surgery and trauma patients. DVTs occurred in 23.5% of patients who missed at least one dose and in 4.8% of patients who did not (p < 0.01). This study also observed the same association between LOS and increased DVT odds; however, the correlation observed between the increasing number of missed doses and DVT did not control for LOS. As a conservative assumption, midpoint estimates from Louis and colleagues (2014) were applied only to the surgical/trauma subset of the overall hospitalized population at risk of VTE, which is a much lower rate than was used for nonsurgical patients. The decline in VTE rate for the surgical/trauma group may be too optimistic to apply to the education bundle because the most common reason for interruption of prophylaxis is a pending invasive procedure or concern for bleeding [6]. This may lead to an overestimate of base-case VTEs prevented and costs saved. Readers should reference the range of estimates reported in the sensitivity and scenario analyses.
Most hospital-related VTEs occur posthospitalization [1]. This finding may suggest that addressing pharmacologic prophylaxis non administration prior to discharge has little overall impact on VTE formation. One study found that VTE rates remained unchanged despite near-universal administration of pharmacologic VTE prophylaxis for those at risk [1]. The authors suggest that these unchanged rates may be the result of patients only receiving prophylaxis while in the inpatient setting. They also suggest that 50% of VTEs are unrelated to current or recent hospitalization. Therefore, efforts to identify and target those at highest risk in inpatient and outpatient settings with longer duration of primary and secondary prophylaxis would broaden prevention efforts to reach those outside the hospital setting [1].
The relationship between increased doses and prevention of VTE is not well established. The evidence in the literature for the link between missed doses of prophylactic antithrombotic medications and development of DVT is mixed. A case–control study [24] did not demonstrate any evidence of a relationship between any missed dose and development of DVT but found an association between increased LOS in the hospital and odds of developing DVT. Further research to establish the relationship between medication adherence and VTE prevention is needed and could strengthen model assumptions around the education bundle’s effectiveness in preventing VTE. The evidence gathered only stratified between missing one or more doses versus none, and our model reflects this binary stratification. There is reason to believe that missing one dose is less impactful on VTE formation than missing all doses for example, but this dosing effect is not currently reflected in our model. However, to clarify, the effectiveness is not modeled based on increased doses but rather reduction in VTE, and dosing only factors into pharmacologic resource utilization cost calculations.
Next, the model did not account for other long-term complications of VTE, such as post thrombotic syndrome and pulmonary hypertension, although medical cost estimates applied to the post-VTE health state may partially account for these complications [17,26]. To the best of the authors’ knowledge, no sources estimate the costs of the real-time alert bundle. These real-time alert setup estimates are based on author assumptions of time and cost to implement in all hospitals nationwide. Those looking to implement this bundle should examine existing hospital infrastructure to determine feasibility of implementing a real-time alert system when prescribed doses of VTE prophylaxis go unfilled. Expert opinion indicated that the range in cost could vary widely and is highly dependent on existing information technology infrastructure within the hospital. Finally, in modeling a nationwide implementation of the VTE education bundle, it is assumed that every hospital would implement the intervention uniformly, which includes decreasing the average number of non administered doses of prophylaxis by 0.632 and decreasing VTE events by the same rate as observed in the work of Haut and colleagues [10] and Louis and colleagues [6], which is a strong assumption (as are all assumptions around the study’s model inputs) because regional variation and compliance are likely to differ. This model may be overestimating the effects and overestimating or underestimating the costs of implementing the intervention.
Conclusion
An estimated 134,000 VTEs and 19,000 deaths could potentially be averted with nationwide implementation of the education bundle. The use of the education bundle results in increased provider (intervention) costs for nurse training, materials and costs of setting up the real-time alert system of US$321 million. Averted VTEs would result in more than 13 million fewer hours of lost patient time, leading to US$46 million in savings in employee absenteeism costs, US$19 million in savings in caregiving costs and US$237 million in savings in patient costs. The implementation of the education bundle is estimated to reduce societal costs by approximately US$2.8 billion. As such, a nationwide rollout of the VTE education bundle could result in a decline in VTEs and mortality with savings to society. Evidence suggests that half of annual VTEs occur unrelated to current or recent hospitalization; therefore, efforts to identify at-risk individuals outside the healthcare system should supplement efforts to decrease VTE medication nonadministration.
•
Venous thromboembolism (VTE) is a common hospital-acquired condition that can be fatal but is treatable with medical prophylaxis. Non administration of VTE prophylaxis is common.
•
Research comparing an education bundle intervention with standard care finds significantly lower levels of VTE non administration among patients receiving education on VTE risks and VTE prophylaxis.
•
This article constructed a population-level Markov model to estimate the effects of a national rollout of a VTE education bundle for patients at risk of developing VTE.
•
The article examined costs and outcomes from a societal perspective, which included patient, family, provider, payer and employer perspectives.
•
Model parameters were identified from publicly available data sources and the literature.
•
Uncertainty was explored through a series of one-way probabilistic sensitivity and scenario analyses.
•
Model results estimate that a nationwide rollout of VTE education bundles could result in a reduction of VTEs and deaths, with societal savings of approximately US$2.8 billion over 5 years compared with standard care.
•
Limitations include uncertainty in model parameters and possible nonaccounting for long-term complications as a result of VTE. Nationwide rollout of the education bundle may also be uneven.
Author contributions
A Breck was responsible for study conception. N Boyer was responsible for model conceptualization and design. R Skinner was responsible for literature review, model input identification, and drafting the manuscript. All authors were responsible for model programming, data analysis, and manuscript revision.
Acknowledgments
The authors gratefully acknowledge funding for this study from the Patient-Centered Outcomes Research Institute. The authors also thank J Heit and D Esposito for their valuable guidance, expertise and thoughtful review of this manuscript, and E Haut and B Lau for their expertise and feedback related to the VTE education bundle.
Financial & competing interests disclosure
This work was funded by the Patient-Centered Outcomes Research Institute (PCORI) under contract IDIQ-SOW #16-INSIGHT-AOSEPP-ENG. The contents of this work are solely the responsibility of the authors and do not necessarily represent the views of PCORI, its Board of Governors or its Methodology Committee. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing assistance in terms of editing and formatting of this manuscript was provided in house within the terms of the contract.
Supplementary Material
File (supplementary materials (2).docx)
- Download
- 29.56 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Heit JA, Crusan DJ, Ashrani AA, Petterson TM, Bailey KR. Effect of a near-universal hospitalization-based prophylaxis regimen on annual number of venous thromboembolism events in the US. Blood 130(2), 109–114 (2017).
2.
Grosse SD, Nelson RE, Nyarko KA, Richardson LC, Raskob GE. The economic burden of incident venous thromboembolism in the United States: a review of estimated attributable healthcare costs. Thromb. Res. 137, 3–10 (2016).
•• Demonstrates the economic burden of venous thromboembolism.
3.
Alotaibi GS, Wu C, Senthilselvan A, McMurtry MS. Secular trends in incidence and mortality of acute venous thromboembolism: the AB-VTE population-based study. Am. J. Med. 129(8), 879.e19–879.e25 (2016).
4.
Heit JA, Silverstein MD, Mohr DN, Petterson TM, O’Fallon WM, Melton LJ 3rd. Predictors of survival after deep vein thrombosis and pulmonary embolism: a population-based, cohort study. Arch. Intern. Med. 159(5), 445–453 (1999).
5.
Schünemann HJ, Cushman M, Burnett AE et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: prophylaxis for hospitalized and nonhospitalized medical patients. Blood Adv. 2(22), 3198–3225 (2018).
6.
Louis SG, Sato M, Geraci T et al. Correlation of missed doses of enoxaparin with increased incidence of deep vein thrombosis in trauma and general surgery patients. JAMA Surg. 149(4), 365–370 (2014).
• Finds a link between missed doses of prophylaxis and deep vein thrombosis.
7.
Lau BD, Wang J, Hobson DB et al. Missed doses of venous thromboembolism prophylaxis: a growing problem without an active management strategy. J. Gen. Intern. Med. 36(2), 540–542 (2021).
8.
Fanikos J, Stevens LA, Labreche M et al. Adherence to pharmacological thromboprophylaxis orders in hospitalized patients. Am. J. Med. 123(6), 536–541 (2010).
9.
Streiff MB, Lau BD, Hobson DB et al. The Johns Hopkins Venous Thromboembolism Collaborative: multidisciplinary team approach to achieve perfect prophylaxis. J. Hosp. Med. 11(Suppl. 2), 8–14 (2016).
10.
Haut ER, Aboagye JK, Shaffer DL et al. Effect of real-time patient-centered education bundle on administration of venous thromboembolism prevention in hospitalized patients. JAMA Netw. Open 1(7), e184741 (2018).
•• Demonstrating an increase in prophylaxis administration due to decreased patient refusal because of the education bundle.
11.
Johns Hopkins Medicine. How do I prevent blood clots? YouTube [Video]. (2015). www.youtube.com/watch?v=0o3yadu4DFw
12.
Murphy PB, Vogt KN, Lau BD et al. Venous thromboembolism prevention in emergency general surgery: a review. JAMA Surg. 153(5), 479–486 (2018).
13.
Haut ER, Lau BD, Kraus PS et al. Preventability of hospital-acquired venous thromboembolism. JAMA Surg. 150(9), 912–915 (2015).
•• Attempts to measure the preventability of venous thromboembolism by measuring patients with defect-free care.
14.
U.S. Bureau of Economic Analysis. Personal consumption expenditures: health (chain-type price index). FRED, Federal Reserve Bank of St. Louis [Web page] (2021). https://fred.stlouisfed.org/series/DHLTRG3A086NBEA
15.
Anderson FAJ, Zayaruzny M, Heit JA, Fidan D, Cohen AT. Estimated annual numbers of US acute-care hospital patients at risk for venous thromboembolism. Am. J. Hematol. 82(9), 777–782 (2007).
16.
Spyropoulos AC, Lin J. Direct medical costs of venous thromboembolism and subsequent hospital readmission rates: an administrative claims analysis from 30 managed care organizations. J. Manag. Care Spec. Ph. 13(6), 475–486 (2007).
17.
Cohoon KP, Leibson CL, Ransom JE et al. Direct medical costs attributable to venous thromboembolism among persons hospitalized for major operation: a population-based longitudinal study. Surgery 157(3), 423–431 (2015).
18.
Owodunni OP, Haut ER, Shaffer DL et al. Using electronic health record system triggers to target delivery of a patient-centered intervention to improve venous thromboembolism prevention for hospitalized patients: is there a differential effect by race? PLoS One 15(1), e0227339 (2020).
19.
Bureau of Labor Statistics. Software Developers, Quality Assurance Analysts, and Testers (2020). www.bls.gov/ooh/computer-and-information-technology/software-developers.htm
20.
Quality, Certificationand Oversight Reports. Hospitals: Active Provider and Supplier Counts Report. https://qcor.cms.gov/hospital_wizard.jsp?which=3&report=active.jsp
21.
Bureau of Labor Statistics. Labor Force Statistics from the Current Population Survey (2020). www.bls.gov/cps/
22.
Bliss RL, Katz JN, Wright EA, Losina E. Estimating proximity to care: are straight line and zipcode centroid distances acceptable proxy measures? Med. Care 50(1), 99–106 (2012).
23.
Internal Revenue Service. Standard Mileage Rates www.irs.gov/tax-professionals/standard-mileage-rates
24.
Voils SA, Carlson A. Association of deep-vein thrombosis (DVT) with missed doses of prophylactic antithrombotic medications in ICU patients: a case-control study. Ann. Pharmacother. 48(10), 1294–1297 (2014).
25.
Lau BD, Haut ER. Practices to prevent venous thromboembolism: a brief review. BMJ Qual. Saf. 23(3), 187–195 (2014).
26.
Ginsberg JS, Hirsh J, Julian J et al. Prevention and treatment of postphlebitic syndrome: results of a 3-part study. Arch. Intern. Med. 161(17), 2105–2109 (2001).
27.
Spencer FA, Gore JM, Lessard D, Douketis JD, Emery C, Goldberg RJ. Patient outcomes after deep vein thrombosis and pulmonary embolism: the Worcester venous thromboembolism study. Arch. Intern. Med. 168(4), 425–430 (2008).
28.
Healthcare Cost and Utilization Project. Free Health Care Statistics (2014). https://hcupnet.ahrq.gov
29.
Tsai J, Abe K, Boulet SL, Beckman MG, Hooper WC, Grant AM. Predictive accuracy of 29-comorbidity index for in-hospital deaths in US adult hospitalizations with a diagnosis of venous thromboembolism. PLoS One 8(7), e70061 (2013).
30.
Centers for Medicare & Medicaid Services. Medicare Part D Drug Spending Dashboard [Dataset] (2020). https://data.cms.gov/summary-statistics-on-use-and-payments/medicare-medicaid-spending-by-drug/medicare-part-d-spending-by-drug
31.
Shahi A, Chen AF, Tan TL, Maltenfort MG, Kucukdurmaz F, Parvizi J. The incidence and economic burden of in-hospital venous thromboembolism in the United States. J. Arthroplasty 32(4), 1063–1066 (2017).
32.
Agency for Health Research and Quality. MEPS HC-201: 2017 Full Year Consolidated Data File [Dataset] (2019). https://meps.ahrq.gov/mepsweb/data_stats/download_data_files_detail.jsp?cboPufNumber=HC-201
33.
Wolff JL, Roter DL. Family presence in routine medical visits: a meta-analytical review. Soc. Sci. Med. 72(6), 823–831 (2011).
Information & Authors
Information
Published In
Pages: 563 - 574
PubMed: 35593109
Copyright
© 2022 Future Medicine Ltd.
History
Received: 21 October 2021
Accepted: 25 March 2022
Published online: 20 May 2022
Keywords:
Topics
Authors
Funding Information
Patient-Centered Outcomes Research Institute: IDIQ-SOW #16-INSIGHT-AOSEPP-ENG
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
An impact evaluation of an education bundle for patients at risk of developing venous thromboembolism. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0260
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Thanh Lu, Sophia D'Angelo, Zohra Tayebali, Matthew Dempsey, Kristen Giombi, Olga Khavjou, Impact analysis of expanded access to ketamine for treatment-resistant depression, Journal of Comparative Effectiveness Research, 10.57264/cer-2024-0233, 14, 6, (2025).
- Nilgün Özbaş, The Status of Nurses Working in Surgical Units in Delivering Patient Education on Venous Thromboembolism, Journal of Nursology, 10.17049/jnursology.1507222, 28, 1, (56-63), (2025).
- Mujtaba Khalil, Selamawit Woldesenbet, Muhammad Musaab Munir, Muhammad Muntazir Mehdi Khan, Zayed Rashid, Abdullah Altaf, Erryk Katayama, Yutaka Endo, Mary Dillhoff, Susan Tsai, Timothy M. Pawlik, Healthcare utilization and expenditures among patients with venous thromboembolism following gastrointestinal cancer surgery, Journal of Gastrointestinal Surgery, 10.1016/j.gassur.2024.05.012, 28, 7, (1151-1157), (2024).