SPECT/CT versus planar imaging to determine treatment strategy for non-small-cell lung cancer: a cost–effectiveness analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: SPECT/CT has been found to improve predicted postoperative forced expiratory volume in one second (ppoFEV1) assessments in patients with non-small-cell lung cancer (NSCLC). Methods: An economic simulation was developed comparing the cost–effectiveness of SPECT/CT versus planar scintigraphy for a US payer. Clinical outcomes and cost data were obtained through review of the published literature. Results: SPECT/CT increased the accuracy ppoFEV1 assessment, changing the therapeutic decision for 1.3% of nonsurgical patients to a surgical option, while 3.3% of surgical patients shifted to more aggressive procedures. SPECT/CT led to an expected cost of $4694 per life year gained, well below typical thresholds. Conclusion: SPECT/CT resulted in substantially improved health outcomes and was found to be highly cost-effective.
According to American Cancer Society estimates, there will be about 228,820 new cases of lung cancer in the USA in 2020, with an estimated 135,720 deaths, or approximately 22% of all cancer deaths [1]. Non-small-cell lung cancer (NSCLC) comprises about 80–85% of all lung cancer cases. NSCLC presents a substantial burden on quality of life, both from the disease itself along with the side effects associated with chemo- and radiation therapy, or potentially invasive surgeries.
Surgical resection of the tumor remains the best and most consistent therapeutic option to improve survival in NSCLC patients, despite the advances made in radiation therapy and chemotherapy [2]. Lung cancer resection with curative intent may require removal of an entire lung (pneumonectomy), entire lobe (lobectomy) or a portion of a lobe (sublobar) since potential cure remains predicated on achieving a complete resection. The decision to proceed to lung resection surgery relies on the preoperative assessment of its risks and feasibility, in order to avoid postoperative respiratory failure and other cardiopulmonary complications. Among several indicators predicting the risks involved, predicted postoperative pulmonary function expressed as predicted postoperative forced expiratory volume in 1 s (ppoFEV1) has emerged as the most critical determinant when evaluating the feasibility of lung resection surgery [3–5].
In current medical practice, measurement of baseline lung function combined with ventilation-perfusion or perfusion-only planar lung scintigraphy is the most widely used imaging examination for preoperative prognostic calculation of ppoFEV1 [6]. However, planar scintigraphy only estimates relative regional lung perfusion, as it is limited by its nonanatomic nature of imaging, for example, inability to measure the impact of nonuniform and oblique pulmonary fissures and, therefore, cannot accurately assess the perfusion contribution of an individual lobe [7]. Consequently, planar scintigraphy's low accuracy in estimating the differential contribution of pulmonary lobes or segments leads to underestimation of ppoFEV1 [6–9], with correlation coefficients of predicted versus actual ppoFEV1 ranging from 0.51 to 0.92 [6]. Depending on the extent of this underestimation, it is plausible that patients are either erroneously excluded from potentially curative resection surgery that they could have tolerated from a pulmonary function perspective.
Given this premise, investigators have suggested more effective alternatives than planar perfusion scintigraphy for the prediction of ppoFEV1 [6–9]. One such recent alternative is single-photon emission computed tomography (SPECT) perfusion scintigraphy combined with conventional computed tomography (CT; SPECT/CT). The integrated CT images (delineating lung lobes and segments) and attenuation correction SPECT imaging (measuring lobar perfusion) together provide a more accurate estimation of ppoFEV1 [7–9]. Toney et al. first showed that SPECT/CT provided an anatomically more accurate assessment of lobar perfusion and ppoFEV1 than planar imaging, and could thus more accurately define resectability and improve the rate of appropriate and potentially curative surgical resection in NSCLC patients [7]. Given these findings, we sought to investigate the economics of migrating from planar scintigraphy to SPECT/CT for the purposes of preoperative assessment of ppoFEV1 in NSCLC patients, and the potential impact on clinical decision-making around appropriate treatment choices. The study objective was therefore to quantify the economics of the diagnostic impact of SPECT/CT versus planar scintigraphy on ppoFEV1 for the preoperative assessment of NSCLC patients for lung resection surgery and assess its cost–effectiveness as an intervention from a payer perspective.
Materials & methods
Model structure
A cohort-level decision tree model was built and validated using Microsoft Excel 2016 to estimate the total costs, cost–effectiveness, and impact on treatment selection of using hybrid SPECT/CT versus planar imaging for NSCLC patients. A depiction of this model is shown in Figure 1. The model assumes a hypothetical cohort of 1000 early stage (stage I or II) potentially resectable NSCLC patients, potentially with typical co-morbidities, for example, coronary artery disease, chronic obstructive pulmonary disease, other pulmonary diseases. Costs, in USD, and benefits, in deaths avoided/life years gained, were evaluated over a 1-year time horizon. Due to the short time horizon, no discounting was applied.
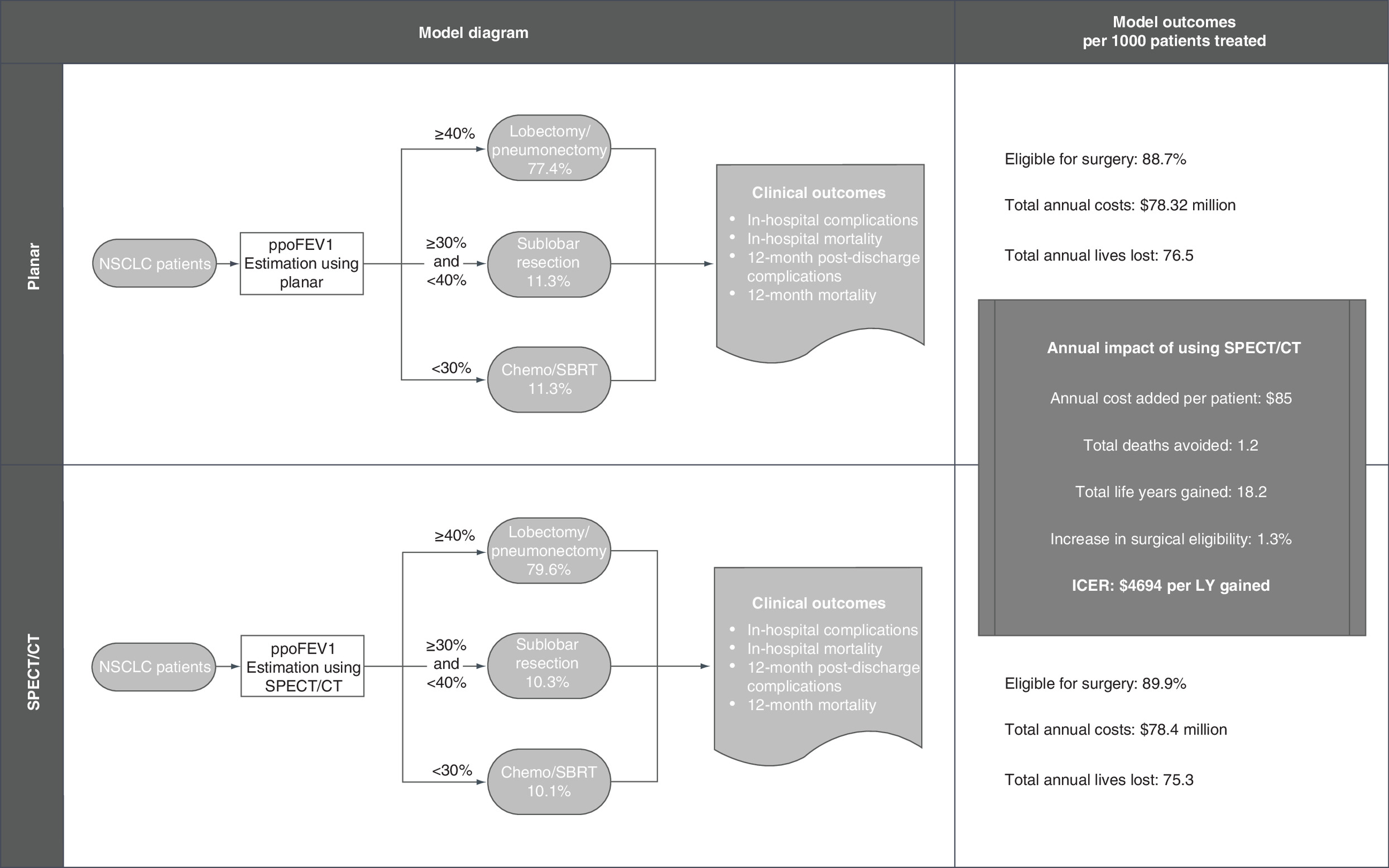
Figure 1. Model overview.
Figure 1 depicts the model design and flow of patients. A cohort of 1000 potentially resectable early-stage NSCLC patients enters the model and use either SPECT/CT or planar imagining to estimate the ppoFEV1 for patients. Based on this value, the treatment option is chosen for the various patients. Ultimately, SPECT/CT led to an additional 1.2% of patients eligible for surgery, 18.2 life years gained, and an ICER of $4694 per life year gained.
ICER: Incremental cost–effectiveness ratio; LY: Life year; NSCLC: Non-small-cell lung cancer; ppoFEV1: Predicted postoperative forced expiratory volume in 1 s; SBRT: Stereotactic body radiation therapy; SPECT/CT: Single-photon emission computed tomography perfusion scintigraphy combined with conventional computed tomography.
The study's premise is based on the assumption that, when all other clinical factors are held constant, a patient's ppoFEV1 can be used to determine the most appropriate treatment strategy for NSCLC. Based on the consensus of expert clinicians in field of nuclear medicine and oncology, it was assumed that patients with a ppoFEV1 ≥40% underwent either a lobectomy or pneumonectomy (latter in 13–26% of all resected lung cancer cases [10–13]), while a sublobar resection (wedge resection or segmentectomy) was performed for patients with ppoFEV1 between 30 and <40%. Patients with a value <30% were not assumed to be surgical candidates due to their increased risk of perioperative morbidity and mortality. For this group, patients underwent nonsurgical treatment, specifically chemotherapy and/or stereotactic body radiation therapy (SBRT).
All data used to perform this analysis were de-identified and accessed in compliance with the Health Insurance Portability and Accountability Act. As a model using a collection of publicly available data, the research was exempt from IRB review under 45 CFR 46.101(b)(4).
Data sources
The primary data source for this model was a ‘best-evidence’ literature review. The National Library of Medicine's PubMed database was the source for the electronic search. The selection criteria included English language studies in an adult population published between January 2005 and February 2017 that containing data relevant to the clinical and imaging application(s) in question. This search was supplemented with publicly available government reports and databases.
Where multiple data points (from multiple data sources) existed for any given model parameter, sample size weighted pooled estimates were calculated. This allowed for a single, pooled estimate for the base case value that is reflective of all the available evidence, minimizing potential bias associated with using data from any one source.
Clinical parameters
The model's key parameter is the average discrepancy between the actual and predicted ppoFEV1 value for SPECT/CT and planar imaging. This represents the diagnostic accuracy of the two imaging techniques, the results of which influence the treatment plan and, thus, ultimately affect the patients expected clinical outcomes. The estimated difference in actual and predicted ppoFEV1 was pooled from multiple sources and weighted by their corresponding sample sizes, similar to calculation of other model parameters. Assuming all other factors were equal, the treatment assignment in the model was based entirely on the ppoFEV1 values generated by the imaging modalities.
The general lung cancer population distribution across the study's ppoFEV1 values thresholds was derived from published literature and assumed to be generated by the standard planar lung scintigraphy. Similarly, all clinical parameters including in-hospital and 12-month post-discharge complication and mortality rates related to the study's treatment choices are estimated from published literature. The values for each of the clinical parameters are shown in Table 1.
| Parameter description | Base case | Range | Study | Ref. |
|---|---|---|---|---|
| Patient population | ||||
| <65 years of age (therefore commercial coverage) | 56.92% | 54–64% | Billmeier 2011, Gopaldas 2010, Swanson 2012 | [14–16] |
| Medicare to private payer reimbursement conversion | 1.62 | 1.22–2.03 | American Hospital Association 2016 | [17] |
| Predicted postoperative forced expiratory volume in 1 second (ppoFEV1) | ||||
| ≥40% | 77.4% | 1–100% | Linden 2014, Varlotto 2013 | [18,19] |
| 30–39% | 11.3% | 1–100% | Expert Opinion | |
| <30% | 11.3% | 1–100% | Expert Opinion | |
| Imaging scans | ||||
| SPECT/CT | ||||
| Scan cost | $390 | $295–487.5 | CPT #78597 | [20] |
| Underestimated mean difference between preoperative and actual ppoFEV1 (%) | 6.4% | 2.65–10.24% | Ohno 2007, Toney 2014, Sudoh 2006, Yoshimoto 2009 | [6–9] |
| Planar | ||||
| Scan cost | $390 | $295–487.5 | CPT #78597 | [20] |
| Underestimated mean difference between preoperative and actual ppoFEV1 (%) | 11.9% | 7.95–15.78% | Ohno 2007, Toney 2014, Sudoh 2006, Yoshimoto 2009 | [6–9] |
| Treatment | ||||
| Pneumonectomy/lobectomy | ||||
| Surgery + hospitalization cost | $33,866 | $17,336–40,212 | Gopaldas 2010, Swanson 2012, Louie 2014, Medbery 2014, Shah 2013, Smith 2015 | [15,16,21–24] |
| In-hospital complication rate | 34.2% | 3.6–43.2% | Billmeier 2011, Gopaldas 2010, Burfeind 2010, Landreneau 2014, Lin 2016, Linden 2014, Ludwig 2005, Martin-Ucar 2002, Medbery 2014, Paul 2013, Shapiro 2010 | [14,15,18,22,25–31] |
| In-hospital mortality rate | 3.0% | 0–9.9% | Billmeier 2011, Gopaldas 2010, Landreneau 2014, Linden 2014, Ludwig 2005, Medbery 2014, Shapiro 2010, Stolz 2014, Strand 2007, Zhang 2012 | [14,15,18,22,26,28,31–34] |
| Post-discharge complication rate | 14.1% | 1.8–8.6% | Farjah 2014, Landreneau 2014, Martin-Ucar 2002, Ren 2014, Shapiro 2009, Sugi 2010, Yang 2012 | [26,29,35–39] |
| 12-month follow-up mortality rate | 3.7% | 1.8–54% | Billmeier 2011, Cerfolio 2006, Gudbjartsson 2008, Kim 2005, Landreneau 2014, Ludwig 2005, Stolz 2014, Varlotto 2013, Whitson 2011, Zhang 2012 | [14,19,26,28,32,34,40–43] |
| Sublobar resection | ||||
| Surgery + hospitalization cost | $36,870 | $27,964–49,652 | Kwan 2014, Shah 2013, Smith 2015, Yendamuri 2007 | [23,24,44,45] |
| In-hospital complication rate | 27.98% | 4.5–36.9% | Billmeier 2011, Deen 2014, Landreneau 2014, Lin 2016, Linden 2014, Yendamuri 2007 | [14,18,26,27,45,46] |
| In-hospital mortality rate | 1.5% | 0.0–7.1% | Billmeier 2011, Kwan 2014, Landreneau 2014, Linden 2014, Yang 2012, Yendamuri 2007 | [14,18,26,39,44,45] |
| Post-discharge complication rate | 14.74% | 0–25.8% | Landreneau 2014, Ren 2014, Shapiro 2009, Sugi 2010, Yang 2012 | [26,36–39] |
| 12-month follow-up mortality rate | 6.54% | 2.7–20% | Billmeier 2011, Kwan 2014, Landreneau 2014, Linden 2014, Varlotto 2013 | [14,18,19,26,44] |
| SBRT and/or chemotherapy | ||||
| Treatment cost | $29,791 | $16,322–49,120 | Cipriano 2011, Puri 2012, Shah 2013, Smith 2015, Yendamuri 2007 | [23,24,45,47,48] |
| Post-discharge complication rate | 12.54% | 0–34.6% | Puri 2012, Shah 2013, Yu 2015 | [23,48,49] |
| 12-month follow-up mortality rate | 15.05% | 11.5–19.5% | Puri 2012, Speicher 2014, Varlotto 2013, Yu 2015 | [19,48–50] |
| In-hospital complication cost | $14,319 | $5395–23,242 | Medbery 2014, Paul 2013 | [22,30] |
| In-hospital mortality cost | $27,698 | $4509–50,877 | Medbery 2014, Puri 2012 | [22,48] |
| Post discharge complication cost (surgical treatment) | $13,676 | $12,586–20,976 | Farjah 2014, Kwan 2014 | [35,44] |
| Post discharge complication cost (SBRT treatment) | $23,008 | $1870–43,860 | Cipriano 2011, Shah 2013 | [23,47] |
| 12-month follow-up cost (surgical treatment) | $15,669 | $11,752–19,586 | Kwan 2014 | [44] |
| 12-month follow-up cost (SBRT treatment) | $0 | ≥0 | Assumption | |
| One-time oxygen equipment cost | $1742 | $1262–2103 | Billmeier 2011, Shah 2013 | [14,23] |
| – Monthly cost | $346 | $251–418 | Billmeier 2011, Shah 2013 | [14,23] |
| Terminal care cost | $50,203 | $20,321–97,971 | Cipriano 2011, Louie 2014, Shah 2013, Tangka 2015 | [21,23,47,51] |
Cost parameters
The expected cost of any given event (complication or mortality) was calculated by multiplying the event rate with the treatment cost. Follow-up costs also included the cost of oxygen equipment for those with ppoFEV1 ≤50%. For the imaging scans, reimbursement amounts were calculated based on the 2019 Medicare total payments for technical and professional components for the code 78582 (nuclear medicine scans) as reported by the CMS [20]. All literature-derived costs were converted to 2019 USD using the Bureau of Labor Statistics' US Medical Care Consumer Price Index to adjust for inflation [52]. Based on the demographic distribution of the lung cancer population in USA, slightly more than half of the model cohort is assumed to be insured by commercial (non-Medicare) payers [14–16]. Therefore, all Medicare payments were adjusted by a conservative multiplier of 1.6 to appropriately represent a private payer's reimbursement amount for the corresponding portion of the hypothetical cohort [17]. The final clinical and economic parameters in the model are shown in Table 1 [18,19,21–51].
Model outcomes
The model compares the downstream differential impact of ppoFEV1 values as generated by SPECT/CT versus planar by estimating the total direct cost of the care pathway under consideration. The cost calculation includes the cost of imaging, surgery, peri- and postoperative 12-month complications, mortality, and follow-up between the different surgical and nonsurgical groups as deemed by the ppoFEV1 thresholds (described above).
The primary clinical outcome that was estimated in the model is the difference in lung resection rates i.e., if differences in the mean underestimation of ppoFEV1 from their actual values impact their preoperative surgical eligibility, then the model calculates the difference in proportion of patients receiving any of the treatment options between the SPECT/CT and planar cohorts.
Effectiveness is expressed as the number of patient life years gained across the different treatment options, assuming that patients surviving at the end of the study time frame are free from tumors and remain in remission until the end of their natural life. The latter is estimated using the mean US life expectancy [53]. The average age of a commercial and Medicare patient in the model is assumed to be 56.2 and 73.9 years, respectively [16]. The incremental cost–effectiveness ratio (ICER) is the cost per life year gained and is calculated as the net difference in total 1-year costs divided by the difference in life years gained/lost between SPECT/CT and planar.
Sensitivity analysis
A one-way deterministic sensitivity analysis was conducted by varying each model parameter individually and observing the effect on the results in order to assess the impact of the individual model parameters and the robustness of the findings. Each model parameter was varied by ±25% of its base value. The top three parameters found to be most critical to the model are reported, along with a tornado diagram that graphically shows the results of the sensitivity analysis.
As the relative underestimation in ppoFEV1 using SPECT/CT versus planar is a particularly important parameter in the model, a separate deterministic sensitivity analysis was performed. In this analysis, the difference in the underestimation between SPECT/CT versus planar was varied across the maximum and minimum values found for each imaging modality in the literature (range: -2.29–13.13%, calculated as Planar–SPECT/CT). The impact on the ICER and annual cost difference was assessed.
Scenario analysis
The presence and severity of emphysema in individual patients is modestly correlated with the degree of airflow obstruction as assessed by reduction in predicted FEV1 (r = 0.65–0.71) [54,55]. It has been suggested that SPECT/CT's benefits could be more pronounced in NSCLC patients with emphysema because of planar imaging's inability to accurately demarcate lobar boundaries and assess lobar and segmental perfusion [7,8]. Thus, we used a scenario analysis to evaluate the imaging modalities in two NSCLC cohorts with either mild–moderate or moderate–severe emphysema. To this end, the distribution of the model's ppoFEV1 values was adjusted to reflect this group with emphysema, while all other study parameters were kept constant. Two distinct ppoFEV1 thresholds were modeled, including ≤80% predicted (likely mild–moderate emphysema) and ≤60% predicted (moderate–severe emphysema) [56]. The percentage of patients with ppoFEV1 values over the thresholds (≤80 and ≤60%) was uniformly distributed across the remaining ppoFEV1 value ranges to form new patient ppoFEV1 distributions for the scenario analysis. ppoFEV1 distributions (measured using the standard planar) are shown in Table 2.
| Predicted postoperative forced expiratory volume in a single second using planar scintigraphy (ppoFEV1) distributions | |||
|---|---|---|---|
| ppoFEV1 range | |||
| ≥40% | 30–39% | <30% | |
| Base case model | 77.4 | 11.3 | 11.3 |
| Mild–moderate emphysema | 64.5 | 17.8 | 17.8 |
| Moderate–severe emphysema | 57.1 | 21.5 | 21.5 |
Results
Base case model
In this construct, where decisions around preoperative surgical eligibility and the specific procedure rely solely on ppoFEV1 values, 77.6, 11.3 and 11.3% receive pneumonectomy/lobectomy, sublobar resection and SBRT, respectively, in the planar cohort. Conversely, 79.7, 10.3 and 10.0% of the SPECT/CT cohort would undergo pneumonectomy/lobectomy, sublobar resection procedures or receive SBRT, respectively (Figure 1). For every 1000 potentially resectable NSCLC patients, using SPECT/CT in place of planar perfusion scintigraphy is expected to be associated with an estimated cost of $78.40 million versus $78.32 million, respectively. This represents $85,466 in total, or $85.5 per patient, in additional costs for a payer per year (Table 3). After accounting for lives lost due to treatment-related complications and lack of successful surgical resection during the 1-year study period, SPECT/CT is associated with a gain of 18.2 patient life years versus planar perfusion scintigraphy. The expected ICER per life year gained for SPECT/CT is estimated at $4694.
| Population | SPECT/CT | Planar | Difference | Incremental cost–effectiveness ratio per life year gained for SPECT/CT ($) |
|---|---|---|---|---|
| NSCLC | ||||
| Total costs ($) | 78,400,543 | 78,315,078 | 85,466 | 4694 |
| per patient | 78,401 | 78,316 | 85 | |
| Total life years | 13,858.5 | 13,840.3 | 18.2 | |
| Treatment type (%) | ||||
| Pneumonectomy/lobectomy | 79.7 | 77.4 | 2.3 | NA |
| Sublobar resection | 10.3 | 11.3 | -1.0 | |
| SBRT | 10.0 | 11.3 | -1.3 | |
| Mild–moderate emphysema | ||||
| Total costs ($) | 78,162,777 | 78,028,765 | 134,012 | 4694 |
| Per patient | 78,163 | 78,029 | 134 | |
| Total life years | 13,801.4 | 13,776.3 | 28.5 | |
| Treatment type (%) | ||||
| Pneumonectomy/lobectomy | 68.0 | 64.5 | 3.6 | NA |
| Sublobar resection | 16.2 | 17.8 | -1.6 | |
| SBRT | 15.8 | 17.8 | -2.0 | |
| Moderate–severe emphysema | ||||
| Total costs ($) | 78,025,959 | 77,864,013 | 161,947 | 4694 |
| Per patient | 78,026 | 77,864 | 162 | |
| Total life years | 13,723.3 | 13,688.7 | 34.5 | |
| Treatment type (%) | ||||
| Pneumonectomy/lobectomy | 61.3 | 57.1 | 4.3 | NA |
| Sublobar resection | 19.6 | 21.5 | -1.9 | |
| SBRT | 19.1 | 21.5 | -2.4 | |
Sensitivity analysis
One-way sensitivity analysis indicates that the cost–effectiveness results of this model are most sensitive to the following three parameters: lobectomy/pneumonectomy treatment costs, SPECT/CT and Planar scan costs and the treatment costs for SBRT. The impact of each parameter on the cost–effectiveness (ICER) between SPECT/CT versus planar approaches can be seen in Figure 2.
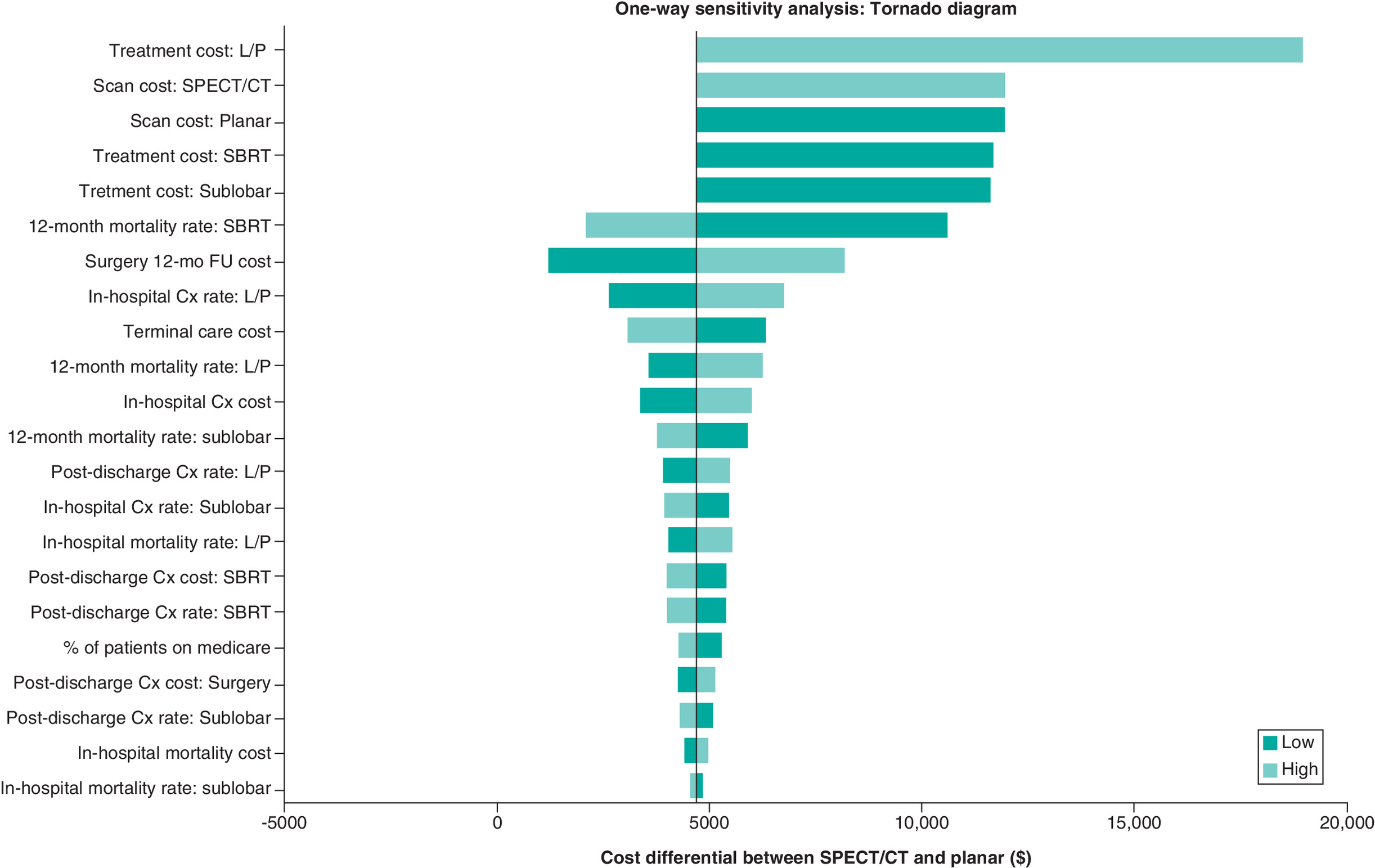
Figure 2. One-way sensitivity analysis results: tornado diagram.
In the sensitivity analysis, each model parameter was varied individually by ±25% to observe the effect on the results, assessing the impact of the individual model parameters and the robustness of the findings. The most influential variables on the total costs were the ppoFEV1 underestimation, treatment costs and scan costs.
Cx: Complication; FU: Follow-up; L/P: Lobectomy/pneumonectomy; SBRT: Stereotactic body radiation therapy.
Both the ICER and the annual cost difference vary based on the mean difference in ppoFEV1 underestimation between SPECT/CT and planar (Figure 3). As the mean difference in underestimation increases (greater underestimation by planar relative to SPECT/CT), more patients become eligible for surgery or for more aggressive surgery, thus increasing costs, as shown by the rising cost difference between SPECT/CT and planar. Despite this, the ICER remains relatively constant, indicating that the life years gained are increasing nearly proportionately to costs. In summary, assuming all other model inputs are held constant, the life years gained are a direct result of SPECT/CT being associated with a higher surgical rate versus planar imaging.
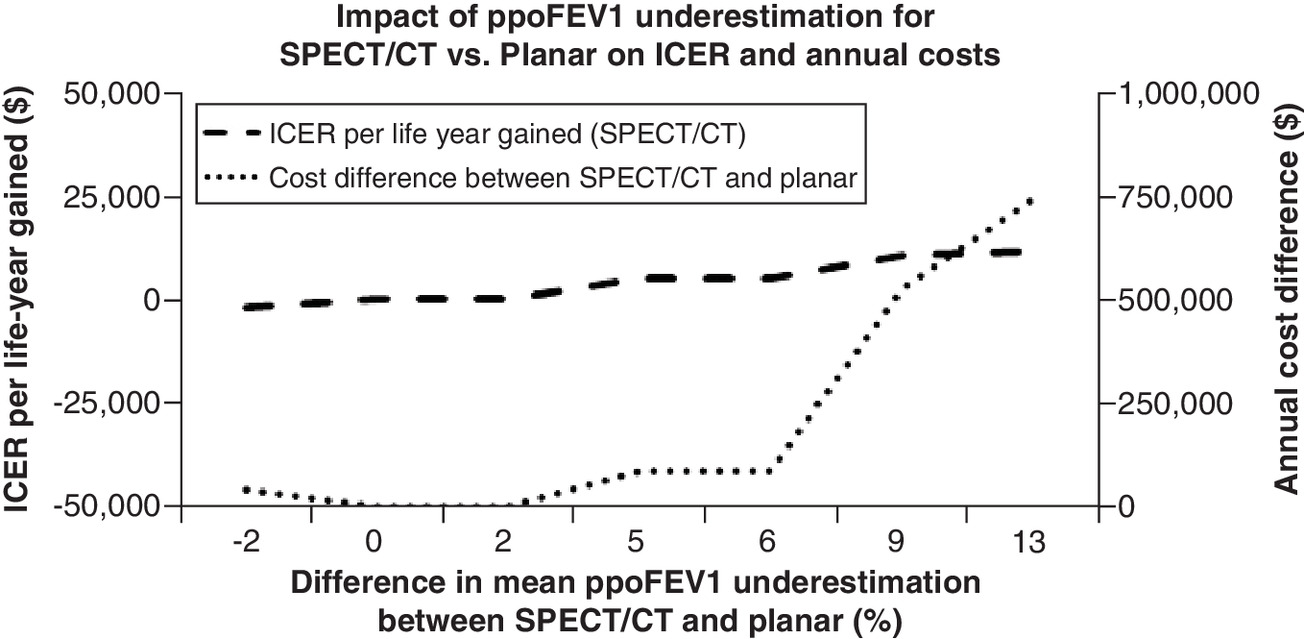
Figure 3. Impact of percentage difference in underestimated ppoFEV1 on total lung cancer-related costs and ICER.
The degree of underestimation for each imaging technology was varied within a defined range and the change in results observed. With the mean difference in underestimation increasing (planar underestimating more relative to SPECT/CT), more patients are becoming eligible for surgery, or a more aggressive surgery, thus increasing costs as shown by the rising cost difference between SPECT/CT and planar. The ICER remains relatively constant, indicating that the life years gained are increasing nearly proportionate to costs.
ICER: Incremental cost–effectiveness ratio; ppoFEV1: Predicted postoperative forced expiratory volume in 1 s; SPECT/CT: Single-photon emission computed tomography perfusion scintigraphy combined with conventional computed tomography.
Scenario analysis
For a hypothetical scenario modeling, 1000 NSCLC patients with mild–moderate emphysema, using SPECT/CT (rather than planar) perfusion scintigraphy for preoperative eligibility is expected to lead to $134,012 in excess costs and a gain of 28.5 life years with 68.1% (vs 64.5%), 16.2% (vs 17.8%) and 15.8% (vs 17.8%) of the SPECT/CT (vs planar) cohort receiving pneumonectomy/lobectomy, sublobar resection and SBRT, respectively. The ICER per life year gained is calculated to be $4694.
For the NSCLC with moderate–severe emphysema, switching to SPECT/CT is expected to lead to $161,947 in additional cost, and 34.5 life years. Thus, the ICER per life year gained is $4694. In this scenario, using SPECT/CT under the model assumption leads to 61.4,19.5 and 19.1% of the cohort receiving pneumonectomy/lobectomy, sublobar resection, and SBRT, respectively. Correspondingly, 57.1, 21.5 and 21.5% of the planar group would be assigned the above three treatment options in that order.
Discussion
The American Cancer Society recognizes surgical resection is the cornerstone of therapy in individuals with localized NSCLC who are medically fit and suitable for treatment [57]. Given the poorer prognosis when surgery is not an option, it is critical to identify all those who can safely tolerate surgery that maximizes the margins of resection, and potentially lowers the risk of local recurrence. SPECT/CT's fusion technology can provide anatomic and functional information in a single examination and allows for attenuation correction of the perfusion SPECT emission data using CT. Clinical studies have shown this hybrid technology provides an anatomically more accurate assessment of lobar perfusion, which in turn, leads to a relatively more accurate ppoFEV1 [7,8].
To the authors' knowledge, this is the first study attempting to evaluate the economic impact of SPECT/CT in planning NSCLC treatment. This study found that using SPECT/CT to estimate ppoFEV1 as opposed to Planar imaging lead to a gain of 18.2 life years, and $85,466 in annual costs, for every 1000 potentially resectable NSCLC patients. The estimated ICER was $4694 for every life year gained. Using a threshold of $50,000, which is common for cost–utility analysis, or even the more current inflation-adjusted value of $100,000–$150,000 [58], SPECT/CT can be considered as highly ‘cost-effective’. SPECT/CT shifted 1.3% of the model patients from a nonsurgical care pathway toward a surgical option and, in addition, 3.3% of SPECT/CT patients underwent a more extensive surgical lung resection procedure than would have been recommended using planar imaging alone. While this led to increased costs, health outcomes were also greatly improved, as demonstrated in the ICER.
Cost–effectiveness was also shown to be consistent in both mild–moderate emphysema, as well as moderate–severe emphysema. The ICER remained the same in the scenario analyses due to the fact that shift in patients toward surgical eligibility occurred proportionately for both imaging cohorts, so therefore while the total costs and life years gained changed, the ICER did not as the changes were proportionate.
Limitations
We acknowledge that this model has limitations, given that every economic analysis is a simplistic representation of the real world. The major limitation is the study assumption that other factors that could potentially decide the care pathway for a NSCLC patient (e.g., tumor size, location, age, etc.), do not play any differential role in the estimated outcomes and therefore are not included in the model. Additionally, the clinical studies underlying the extent of ppoFEV1 estimations are of small sample size and therefore cannot be fully generalized.
The model does not account for specific differences across the different study treatment options in terms of peri- and postoperative complications (e.g., respiratory failure, infections, cardiovascular, etc.), and post-discharge ancillary healthcare resource use including hospital re-admissions, rehabilitation, etc., due to paucity of published evidence. As well, due to the lack of incorporation of specific clinical features, eg. lobar/lung collapse, in the imaging estimation of ppoFEV1, the approach taken in this model may not apply to such clinical situations.
In addition, the average age/life expectancy for the US general population (78.8 years) was used to determine the remaining life years that were lost due to a death. It is very possible that the life expectancy is reduced in NSCLC patients, however, it is difficult to determine exactly by how much, given that the prognosis is largely dependent on age, stage when identified, comorbidities and several other factors. As this model specifically evaluates early-stage NSCLC patients with anatomically resectable tumors, the authors feel that this was a reasonable simplifying assumption to make.
Lack of strong literature evidence required us to seek clinical expertise and input to inform care pathways and resource utilization parameters. Last, the model does not assess the long-term impact of the treatment decisions, nor does it assess the quality of life of these patients.
Conclusion
The results indicate that SPECT/CT is highly cost-effective compared with planar imaging in the assessment of NSCLC patients for potentially curative lung resection surgery. SPECT/CT's additional costs are primarily driven by patients being shifted from a nonsurgical care pathway toward a relatively expensive but potentially curative surgical option. This identification of a more refined treatment strategy subsequently increased the cohort's survival. Assuming all other factors are held constant, the life years gained are a direct function of a more accurate prediction of ppoFEV1 values by SPECT/CT, which in turn lead to a slightly larger resection rate versus planar and improved patient survival. Most importantly, SPECT/CT provides the Thoracic Surgeon a greater level of confidence in proceeding with cancer resection in the borderline respiratory compromised patient.
Future perspective
Despite advances made in radiation therapy and chemotherapy, surgical resection of the tumor remains the best and most consistent therapeutic option to improve survival in NSCLC patients, with ppoFEV1 being the most critical determinant when evaluating the feasibility of lung resection surgery. Traditional methods of planar scintigraphy have been found to have limitations in terms of accurately assessing the differential contribution of pulmonary lobes or segments, leading to patients being denied potentially curative surgery. The current economic model indicates that the integrated information in the SPECT/CT scans may provide increased accuracy, leading to more confidence in surgeons' decision to operate and, ultimately, more patients correctly undergoing lung-resection surgery, that would otherwise have been ruled out. We expect that SPECT/CT will become the standard of care in the NSCLC diagnostic process, and this analysis predicts that patient outcomes, including survival, will improve and that the investment in SPECT/CT technology will prove cost-effective.
•
This study compared the cost–effectiveness of lung single-photon emission computed tomography combined with conventional computed tomography (SPECT/CT) to planar lung scintigraphy in the treatment determination for patients with non-small-cell lung cancer (NSCLC).
•
An Excel-based economic model was developed from a US payer perspective. Associated clinical outcomes and costs were obtained through a review of published literature.
•
The primary clinical outcome estimated in the model was the difference in lung resection rates between the SPECT/CT and planar cohorts. Effectiveness is expressed as the number of patient life years gained across the different treatment options, assuming patients surviving at the end of the study time frame are free from tumor and remain in remission until the end of their natural life.
•
When compared with planar scintigraphy, it was determined that SPECT/CT is expected to lead to $85,466 ($85.5 per patient) in increased cost for a payer per 1000 patients per year, with an increased survival of 18.2 patient life years. The incremental cost–effectiveness ratio (ICER) was determined to be $4694.
•
Furthermore, SPECT/CT increased the ppoFEV1, and thus changed the therapeutic decision in 1.3% of nonsurgical patients, moving them to a surgical option, while 3.3% of surgical patients were shifted to a more aggressive surgical procedure.
•
Sensitivity analysis showed that the model was most sensitive to three parameters: ppoFEV1 underestimation for SPECT/CT, lobectomy/pneumonectomy treatment costs and ppoFEV1 underestimation for planar imaging.
•
The results indicate that lung SPECT/CT is highly cost-effective compared with planar imaging for NSCLC patients. While the resulting accuracy in imaging shifted some patients from a nonsurgical care path, resulting in overall increased costs, there was an even more significant increase in patient life years.
Author contributions
Ryan J Imhoff and Swetha R Palli were responsible for the design, execution and interpretation of the analysis, along with drafting the manuscript. Jonathan Romsa, Richard Inculet and Sanjay Mehta contributed to the design and interpretation of the analysis, and reviewed and revised the manuscript.
Acknowledgments
GE Healthcare provided financial support for the study performed by CTI Clinical Trial and Consulting Services. Although the funding for the project was provided by GE Healthcare, the authors had freedom of investigation and full control of the design of the study, methods used, outcome parameters and results, analysis of data and production of the written report.
Financial & competing interests disclosure
This study was funded by GE Healthcare. RJ Imhoff is, and SR Palli is a former, employee of CTI Clinical Trial and Consulting Services, which is a consultant to GE Healthcare, the study sponsor. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest
1.
2.
Molina JR, Yang P, Cassivi SD, Schild SE, Adjei AA. Non-small-cell lung cancer: epidemiology, risk factors, treatment, and survivorship. Mayo Clin. Proc. 83(5), 584–594 (2008).
3.
Markos J, Mullan BP, Hillman DR et al. Preoperative assessment as a predictor of mortality and morbidity after lung resection. Am. Rev. Respir. Dis. 139(4), 902–910 (1989).
4.
Kearney DJ, Lee TH, Reilly JJ, Decamp MM, Sugarbaker DJ. Assessment of operative risk in patients undergoing lung resection. Importance of predicted pulmonary function. Chest 105(3), 753–759 (1994).
5.
Brunelli A, Kim AW, Berger KI, Addrizzo-Harris DJ. Physiologic evaluation of the patient with lung cancer being considered for resectional surgery: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 143(Suppl. 5), e166S–e190S (2013).
6.
Ohno Y, Koyama H, Takenaka D et al. Coregistered ventilation and perfusion SPECT using krypton-81m and Tc-99m-labeled macroaggregated albumin with multislice CT utility for prediction of postoperative lung function in non-small-cell lung cancer patients. Acad. Radiol. 14(7), 830–838 (2007).
• This study was used to estimate the difference in underestimation of FEV1 between the imaging techniques, which is the primary driver of the model results.
7.
Toney LK, Wanner M, Miyaoka RS, Alessio AM, Wood DE, Vesselle H. Improved prediction of lobar perfusion contribution using technetium-99m-labeled macroaggregate of albumin single photon emission computed tomography/computed tomography with attenuation correction. J. Thoracic Cardiovasc. Surg. 148(5), 2345–2352 (2014).
• This study was used to estimate the difference in underestimation of FEV1 between the imaging techniques, which is the primary driver of the model results.
8.
Sudoh M, Ueda K, Kaneda Y et al. Breath-hold single-photon emission tomography and computed tomography for predicting residual pulmonary function in patients with lung cancer. J. Thoracic Cardiovasc. Surg. 131(5), 994–1001 (2006).
• This study was used to estimate the difference in underestimation of FEV1 between the imaging techniques, which is the primary driver of the model results.
9.
Yoshimoto K, Nomori H, Mori T et al. Prediction of pulmonary function after lung lobectomy by subsegments counting, computed tomography, single photon emission computed tomography and computed tomography: a comparative study. Eur. J. Cardio. Thoracic Surg. 35(3), 408–413 (2009).
• This study was used to estimate the difference in underestimation of FEV1 between the imaging techniques, which is the primary driver of the model results.
10.
Ferguson MK, Karrison T. Does pneumonectomy for lung cancer adversely influence long-term survival? J. Thoracic Cardiovasc. Surg. 119(3), 440–448 (2000).
11.
Alexiou C, Beggs D, Onyeaka P et al. Pneumonectomy for stage I (T1N0 and T2N0) nonsmall cell lung cancer has potent, adverse impact on survival. Ann. Thoracic Surg. 76(4), 1023–1028 (2003).
12.
Ferguson MK, Siddique J, Karrison T. Modeling major lung resection outcomes using classification trees and multiple imputation techniques. Eur. J. Cardio. Thoracic Surg. 34(5), 1085–1089 (2008).
13.
Powell HA, Tata LJ, Baldwin DR, Stanley RA, Khakwani A, Hubbard RB. Early mortality after surgical resection for lung cancer: an analysis of the English National Lung cancer audit. Thorax 68(9), 826–834 (2013).
14.
Billmeier SE, Ayanian JZ, Zaslavsky AM, Nerenz DR, Jaklitsch MT, Rogers SO. Predictors and outcomes of limited resection for early-stage non-small-cell lung cancer. J. Natl Cancer Inst. 103(21), 1621–1629 (2011).
• This study was used to estimate the distribution of patient's ages, as well as the complication and mortality rates for the surgical treatments and the rate and cost of oxygen usage.
15.
Gopaldas RR, Bakaeen FG, Dao TK, Walsh GL, Swisher SG, Chu D. Video-assisted thoracoscopic versus open thoracotomy lobectomy in a cohort of 13,619 patients. Ann. Thoracic Surg. 89(5), 1563–1570 (2010).
16.
Swanson SJ, Meyers BF, Gunnarsson CL et al. Video-assisted thoracoscopic lobectomy is less costly and morbid than open lobectomy: a retrospective multiinstitutional database analysis. Ann. Thoracic Surg. 93(4), 1027–1032 (2012).
17.
TrendWatch Chartbook 2016. Trends Affecting Hospitals and Health Systems. https://www.aha.org/system/files/research/reports/tw/chartbook/2016/table4-4.pdf (July 24).
• This report was used to estimate the difference in reimbursement for commercial versus Medicare payers.
18.
Linden PA, D'amico TA, Perry Y et al. Quantifying the safety benefits of wedge resection: a society of thoracic surgery database propensity-matched analysis. Ann. Thoracic Surg. 98(5), 1705–1711; discussion 1711–1702 (2014).
• Used to estimate the distribution of patient's FEV1 values, as well as the complication and mortality rates for the surgical treatments.
19.
Varlotto J, Fakiris A, Flickinger J et al. Matched-pair and propensity score comparisons of outcomes of patients with clinical stage I non-small-cell lung cancer treated with resection or stereotactic radiosurgery. Cancer 119(15), 2683–2691 (2013).
20.
Medicare Physician Fee Schedule. https://www.cms.gov/apps/physician-fee-schedule/search/search-criteria.aspx
• The CMS fee schedule was used to determine the national payment amounts for many of the line item costs in this analysis.
21.
Louie AV, Rodrigues GB, Palma DA, Senan S. Measuring the population impact of introducing stereotactic ablative radiotherapy for stage I non-small-cell lung cancer in Canada. Oncologist 19(8), 880–885 (2014).
22.
Medbery RL, Perez SD, Force SD et al. Video-assisted thoracic surgery lobectomy cost variability: implications for a bundled payment era. Ann. Thoracic Surg. 97(5), 1686–1692; discussion 1692–1683 (2014).
23.
Shah A, Hahn SM, Stetson RL, Friedberg JS, Pechet TT, Sher DJ. Cost–effectiveness of stereotactic body radiation therapy versus surgical resection for stage I non-small-cell lung cancer. Cancer 119(17), 3123–3132 (2013).
• This study was used to estimate the surgical costs, cost of SBRT, SBRT complication rate and cost and oxygen usage and cost.
24.
Smith BD, Jiang J, Chang JY et al. Cost–effectiveness of stereotactic radiation, sublobar resection, and lobectomy for early non-small-cell lung cancers in older adults. J. Geriatric Oncol. 6(4), 324–331 (2015).
• This study was used to estimate the distribution of patient's FEV1 values as well as the mortality rates for the surgical treatments.
25.
Burfeind WR Jr, Jaik NP, Villamizar N, Toloza EM, Harpole DH Jr, D'amico TA. A cost-minimisation analysis of lobectomy: thoracoscopic versus posterolateral thoracotomy. Eur. J. Cardio. Thoracic Surg. 37(4), 827–832 (2010).
26.
Landreneau RJ, Normolle DP, Christie NA et al. Recurrence and survival outcomes after anatomic segmentectomy versus lobectomy for clinical stage I non-small-cell lung cancer: a propensity-matched analysis. J. Clin. Oncol. 32(23), 2449–2455 (2014).
27.
Lin Y, Zheng W, Zhu Y, Guo Z, Zheng B, Chen C. Comparison of treatment outcomes between single-port video-assisted thoracoscopic anatomic segmentectomy and lobectomy for non-small-cell lung cancer of early-stage: a retrospective observational study. J. Thoracic Dis. 8(6), 1290–1296 (2016).
28.
Ludwig C, Stoelben E, Olschewski M, Hasse J. Comparison of morbidity, 30-day mortality, and long-term survival after pneumonectomy and sleeve lobectomy for non-small-cell lung carcinoma. Ann. Thoracic Surg. 79(3), 968–973 (2005).
29.
Martin-Ucar AE, Chaudhuri N, Edwards JG, Waller DA. Can pneumonectomy for non-small-cell lung cancer be avoided? An audit of parenchymal sparing lung surgery. Eur. J. Cardio. Thoracic Surg. 21(4), 601–605 (2002).
30.
Paul S, Andrews WG, Nasar A et al. Outcomes of lobectomy in patients with severely compromised lung function (predicted postoperative diffusing capacity of the lung for carbon monoxide % </= 40%). Ann. Am. Thoracic Soc. 10(6), 616–621 (2013).
31.
Shapiro M, Swanson SJ, Wright CD et al. Predictors of major morbidity and mortality after pneumonectomy utilizing the Society for Thoracic Surgeons General Thoracic Surgery Database. Ann. Thoracic Surg. 90(3), 927–934; discussion 934–925 (2010).
32.
Stolz AJ, Harustiak T, Simonek J, Schutzner J, Lischke R. Pneumonectomy for non-small-cell lung cancer: predictors of early mortality and morbidity. Acta Chirurgica Belgica 114(1), 25–30 (2014).
33.
Strand TE, Rostad H, Damhuis RA, Norstein J. Risk factors for 30-day mortality after resection of lung cancer and prediction of their magnitude. Thorax 62(11), 991–997 (2007).
34.
Zhang P, Jiang C, He W, Song N, Zhou X, Jiang G. Completion pneumonectomy for lung cancer treatment: early and long term outcomes. J. Cardiothoracic Surg. 7, 107 (2012).
35.
Farjah F, Backhus LM, Varghese TK et al. Ninety-day costs of video-assisted thoracic surgery versus open lobectomy for lung cancer. Ann. Thoracic Surg. 98(1), 191–196 (2014).
36.
Ren M, Meng Q, Zhou W et al. Comparison of short-term effect of thoracoscopic segmentectomy and thoracoscopic lobectomy for the solitary pulmonary nodule and early-stage lung cancer. OncoTargets Ther. 7, 1343–1347 (2014).
37.
Shapiro M, Weiser TS, Wisnivesky JP, Chin C, Arustamyan M, Swanson SJ. Thoracoscopic segmentectomy compares favorably with thoracoscopic lobectomy for patients with small stage I lung cancer. J. Thoracic Cardiovasc. Surg. 137(6), 1388–1393 (2009).
38.
Sugi K, Kobayashi S, Sudou M, Sakano H, Matsuda E, Okabe K. Long-term prognosis of video-assisted limited surgery for early lung cancer. Eur. J. Cardio. Thoracic Surg. 37(2), 456–460 (2010).
39.
Yang CF, D'amico TA. Thoracoscopic segmentectomy for lung cancer. Ann. Thoracic Surg. 94(2), 668–681 (2012).
40.
Cerfolio RJ, Bryant AS. Survival and outcomes of pulmonary resection for non-small-cell lung cancer in the elderly: a nested case-control study. Ann. Thoracic Surg. 82(2), 424–429; discussion 429–430 (2006).
41.
Gudbjartsson T, Gyllstedt E, Pikwer A, Jonsson P. Early surgical results after pneumonectomy for non-small-cell lung cancer are not affected by preoperative radiotherapy and chemotherapy. Ann. Thoracic Surg. 86(2), 376–382 (2008).
42.
Kim YT, Kang CH, Sung SW, Kim JH. Local control of disease related to lymph node involvement in non-small-cell lung cancer after sleeve lobectomy compared with pneumonectomy. Ann. Thoracic Surg. 79(4), 1153–1161; discussion 1153–1161 (2005).
43.
Whitson BA, Groth SS, Andrade RS, Maddaus MA, Habermann EB, D'cunha J. Survival after lobectomy versus segmentectomy for stage I non-small-cell lung cancer: a population-based analysis. Ann. Thoracic Surg. 92(6), 1943–1950 (2011).
44.
Kwan SW, Mortell KE, Hippe DS, Brunner MC. An economic analysis of sublobar resection versus thermal ablation for early-stage non-small-cell lung cancer. J. Vasc. Interv. Radiol. 25(10), 1558–1564; quiz 1565 (2014).
45.
Yendamuri S, Komaki RR, Correa AM et al. Comparison of limited surgery and three-dimensional conformal radiation in high-risk patients with stage I non-small-cell lung cancer. J. Thoracic Oncol. 2(11), 1022–1028 (2007).
46.
Deen SA, Wilson JL, Wilshire CL et al. Defining the cost of care for lobectomy and segmentectomy: a comparison of open, video-assisted thoracoscopic, and robotic approaches. Ann. Thoracic Surg. 97(3), 1000–1007 (2014).
47.
Cipriano LE, Romanus D, Earle CC et al. Lung cancer treatment costs, including patient responsibility, by disease stage and treatment modality, 1992 to 2003. Value Health 14(1), 41–52 (2011).
48.
Puri V, Crabtree TD, Kymes S et al. A comparison of surgical intervention and stereotactic body radiation therapy for stage I lung cancer in high-risk patients: a decision analysis. J. Thoracic Cardiovasc. Surg. 143(2), 428–436 (2012).
49.
Yu JB, Soulos PR, Cramer LD, Decker RH, Kim AW, Gross CP. Comparative effectiveness of surgery and radiosurgery for stage I non-small-cell lung cancer. Cancer 121(14), 2341–2349 (2015).
50.
Speicher PJ, Ganapathi AM, Englum BR, Onaitis MW, D'amico TA, Berry MF. Survival in the elderly after pneumonectomy for early-stage non-small-cell lung cancer: a comparison with nonoperative management. J. Am. Coll. Surg. 218(3), 439–449 (2014).
51.
Tangka FK, Subramanian S, Sabatino SA et al. End-of-life medical costs of medicaid cancer patients. Health Serv. Res. 50(3), 690–709 (2015).
52.
US Medical Care Consumer Price Index. https://data.bls.gov/timeseries/CUUR0000SAM?output_view=pct_12mths
53.
Life Expectancy. https://www.cdc.gov/nchs/fastats/life-expectancy.htm
54.
Xie X, De Jong PA, Oudkerk M et al. Morphological measurements in computed tomography correlate with airflow obstruction in chronic obstructive pulmonary disease: systematic review and meta-analysis. Eur. Radiol. 22(10), 2085–2093 (2012).
55.
Thomsen LH, Shaker SB, Dirksen A et al. Correlation between emphysema and lung function in healthy smokers and smokers with COPD. Chronic Obstr. Pulm. Dis. 2(3), 204–213 (2015).
56.
Edwards JG, Duthie DJ, Waller DA. Lobar volume reduction surgery: a method of increasing the lung cancer resection rate in patients with emphysema. Thorax 56(10), 791–795 (2001).
57.
Surgery for non-small-cell Lung Cancer. https://www.cancer.org/cancer/non-small-cell-lung-cancer/treating/surgery.html
58.
Ubel PA, Hirth RA, Chernew ME, Fendrick AM. What is the price of life and why doesn't it increase at the rate of inflation? Arch. Intern. Med. 163(14), 1637–1641 (2003).
Information & Authors
Information
Published In
Pages: 229 - 241
PubMed: 35006007
Copyright
© 2022 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 10 June 2021
Accepted: 30 November 2021
Published online: 10 January 2022
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
SPECT/CT versus planar imaging to determine treatment strategy for non-small-cell lung cancer: a cost–effectiveness analysis. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0139
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Pablo Mínguez Gabiña, Katarina Sjögreen Gleisner, Nicolas Chouin, Johannes Tran-Gia, Michel Koole, Marta Cremonesi, Ana M. Denis-Bacelar, Bartolomeo Cassano, Frederik Verburg, Julia Brosch-Lenz, Massimiliano Pacilio, Jonathan Gear, Caroline Stokke, EANM recommendations for dosimetry in targeted radionuclide therapy with alpha-emitters, EANM Innovation, 10.1016/j.eanmi.2025.100018, 2, (100018), (2026).
- Daniel M. Seraphim, Katia H. Koga, Antoine Vacavant, Diana R. de Pina, How anatomical impairments found on CT affect perfusion percentage assessed by SPECT/CT scan?, Annals of Nuclear Medicine, 10.1007/s12149-024-01969-7, 38, 12, (960-970), (2024).
- Sarah C. CADE, Richard N. GRAHAM, Technical concepts on blood pool phase SPECT (acquisition, reconstruction), The Quarterly Journal of Nuclear Medicine and Molecular Imaging, 10.23736/S1824-4785.23.03506-9, 67, 3, (2023).
- Subapriya Suppiah, Mohd Fazrin Mohd Rohani, Ahmad Zaid Zanial, Ahmad Danial Ahmad Shahrir, Khairul Aliff Khairuman, Sobhan Vinjamuri, A Review on the Usage of Bone Single-Photon Emission Computed Tomography/Computed Tomography in Detecting Skeletal Metastases in the Post-COVID-19 Era, Indian Journal of Nuclear Medicine, 10.4103/ijnm.ijnm_142_22, 38, 2, (191-200), (2023).