A real-world, population-based study for the outcomes of patients with metastatic colorectal cancer to the liver with distant lymph node metastases treated with metastasectomy
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To assess the impact of metastasectomy on survival outcomes of patients with concurrent liver and distant nodal metastases. Materials & methods: Surveillance, Epidemiology, and End Results (SEER) database was accessed and patients with colorectal liver metastases (with or without distant lymph node involvement) were reviewed. Kaplan–Meier survival estimates were then used to assess the impact of the presence of distant lymph node metastases as well as the impact of metastasectomy on overall and cancer-specific survival. A propensity score matching was then conducted between patients with distant lymph node metastases who had surgery versus those who did not have surgery. Results: A total of 15,325 patients were included in the current analysis including 1603 patients who have liver and distant nodal metastases (10.5%) and 13,722 patients who have liver metastases only (89.5%). The following factors were associated with better overall survival (OS): younger age (hazard ratio [HR] with increasing age: 1.024; 95% CI: 1.022–1.025), white race (HR for African–American race vs white race: 1.233; 95% CI: 1.175–1.295), distal site of the primary (HR: 0.808; 95% CI: 0.778–0.840), absence of distant lymph nodes (HR: 0.697; 95% CI: 0.659–0.737), metastasectomy (HR for no metastasectomy vs metastasectomy: 1.954; 95% CI: 1.858–2.056). Within the postpropensity cohort, metastasectomy was associated with improved OS among patients with concurrent distant lymph node and liver metastases (median OS of 20 vs 11 months; p < 0.001). Conclusion: Metastasectomy seems to be associated with improved survival among patients with concurrent lymph node and liver metastases. It is unclear if improved survival is related to the surgical intervention or to the fact that surgically treated patients have a better baseline general condition and hence improved outcomes.
While metastasectomy is the current standard of care for patients with isolated resectable liver +/- lung metastases from colorectal cancer, the role of metastasectomy for patients with liver metastases plus concurrent distant lymph node metastases is less well-defined [1–3]. Given the uncommon nature of this clinical scenario and the reluctance of most surgical teams to perform aggressive surgical resections (including metastasectomy) among those patients, prospective studies are unfortunately not available to provide evidence for this clinical scenario [4,5]. Therefore, a population-based study seems to be the appropriate first step which can then be followed by a prospective study (if evidence of efficacy is observed within the population-based study) [6–10].
Surveillance, Epidemiology, and End Results (SEER) database is one of the largest and most well-studied cancer registries in the world. Given its size and rigorous quality assurance processes, it represents an ideal vignette to study the role of metastasectomy in treating this subset of patients.
Objective
To assess the impact of metastasectomy on survival outcomes of patients with concurrent liver and distant nodal metastases.
Materials & methods
Cohort selection
The current study is based on SEER 18 registries with a data cutoff value in December 2017 [11]. Selection criteria for the study cohort included: patients with metastatic colorectal adenocarcinoma; diagnosis year between 2010–2015 (the lower limit was 2010 as information about individual sites of distant metastases was not available before 2010, and the upper limit was 2015 to allow at least 2 years of follow-up following diagnosis); evidence of liver metastases with or without distant lymph nodes metastases; no evidence of other sites of distant metastases. For patients with more than one primary colorectal cancer, only the first cancer was included. It has to be noted that all included patients had de-novo synchronous metastatic disease (not metachronous metastases).
Data collection
The following information was extracted (where available) from each included patient: age at diagnosis, sex, race, primary tumor site, side of the primary (proximal: before splenic flexure; distal: starting from splenic flexure), year of diagnosis, sites of metastases, histology, grade, surgery to the primary as well as surgery to the distant metastases. Surgery to the distant metastases was identified by the variable ‘Rx-Summ-Surg Oth reg/dis’ which describes the status of surgery to the metastases as either: no ; unknown; or non primary surgical procedures to distant sites and/or lymph nodes. Information about chemotherapy and radiation therapy was not available in this release of SEER database. The extent of metastasectomy (liver-only or liver plus lymph nodes) was not clearly described within the SEER database. Distant (non regional) lymph node metastases that were considered in the current analysis were reported in SEER documentation [12]; but the exact site of these distant lymph nodal metastases (abdominal or extra-abdominal) was not reported within the SEER database.
End points of this study include overall survival (OS; defined as the time from cancer diagnosis till death from any reason); and cancer-specific survival (defined as the time from colorectal cancer diagnosis till death from colorectal cancer). For cancer-specific survival, the variable cause-specific death classification was used and cases where death was attributed to this cancer diagnosis were considered as events, while other cases were considered as censored.
Statistical analysis
Two cohorts were initially recognized: patients with liver-only metastases and patients with liver and distant lymph node metastases. Chi-Squared testing was then used to compare categorical variables between both categories. An independent sample t-test was also used to compare baseline continuous variables.
Kaplan–Meier survival estimates were then used to compare survival outcomes according to the presence of distant lymph node metastases and according to the conduct of metastasectomy. Multivariable Cox regression analysis was then used to assess factors associated with overall and cancer-specific survival. Both models included age at diagnosis, race, sex, grade, sidedness, presence of distant lymph nodes and surgical removal of metastases (metastasectomy). Surgical resection of the primary was not included in these models because of concerns about collinearity between surgical resection of the primary versus metastases (i.e., it is unlikely for patients to undergo surgical removal of the metastases without resection of the primary tumor as well). All the above statistical analyses were conducted through SPSS (version 25.0; IBM, NY, USA).
Nearest neighbor, 1:1, propensity score matching was then done through R software to evaluate the outcomes of patients with liver and distant lymph node metastases treated with metastasectomy versus those treated without metastasectomy. This was adjusted for age, race, grade and side of the primary. Kaplan–Meier survival estimates were then used to compare OS in the postpropensity cohort.
Results
Patients’ characteristics
A total of 15,325 patients were included in the current analysis including 1603 patients who have liver and distant nodal metastases (10.5%) and 13,722 patients who have liver metastases only (89.5%). Comparing both categories together, patients with distant nodal metastases were more likely to be older (p < 0.001), have a distal primary site (p < 0.001), lower likelihood of radical surgery to the primary (p < 0.001) and lower likelihood of surgery to the metastases (p < 0.001) (Table 1).
| Variables | Patients with liver metastases plus distant lymph nodes (1603 patients), n (%) | Patients with liver metastases only (13,722 patients), n (%) | p-value |
|---|---|---|---|
| Age (mean; SD) | 61.00; 13.58 | 64.25; 13.43 | <0.001 |
| Sex Male Female | 915 (57.1%) 688 (42.9%) | 7901 (57.6%) 5821 (42.4%) | 0.702 |
| Race White African–American Asian/Pacific Islander American–Indian/Alaska native Unknown | 1247 (77.8%) 231 (14.4%) 111 (6.9%) 11 (0.7%) 3 (0.2%) | 10444 (76.1%) 2089 (15.2%) 1068 (7.8%) 99 (0.7%) 22 (0.2%) | 0.623 |
| Sidedness† Proximal Distal Unknown | 675 (42.1%) 821 (51.2%) 107 (6.7%) | 5208 (38%) 7753 (56.5%) 761 (5.5%) | <0.001 |
| Grade Grade I Grade II Grade III Grade IV Unknown | 49 (3.1%) 716 (44.7%) 348 (21.7%) 63 (3.9%) 427 (26.6%) | 529 (3.9%) 7974 (58.1%) 2189 (16%) 404 (2.9%) 2626 (19.1%) | <0.001 |
| Radical surgery to the primary Yes No Unknown | 603 (37.6%) 994 (62%) 6 (0.4%) | 8141 (59.3%) 5514 (40.2%) 67 (0.5%) | <0.001 |
| Metastasectomy Yes No Unknown | 226 (14.1%) 1374 (85.7%) 3 (0.2%) | 2700 (19.7%) 10982 (80.0%) 40 (0.3%) | <0.001 |
†
Proximal: before splenic flexure; and distal: splenic flexure and beyond.
SD: Standard deviation.
Survival outcomes within the overall cohort
Distant lymph node involvement was associated with worse OS (among patients who did or did not undergo metastasectomy). Median overall survival for patients with no distant lymphadenopathy was 37 months (for those who underwent metastasectomy) and 15 months (for those who did not undergo metastasectomy); while median OS for patients with distant lymphadenopathy was 20 months (for those who underwent metastasectomy) and 10 months for those who did not undergo metastasectomy (Figure 1A & B).
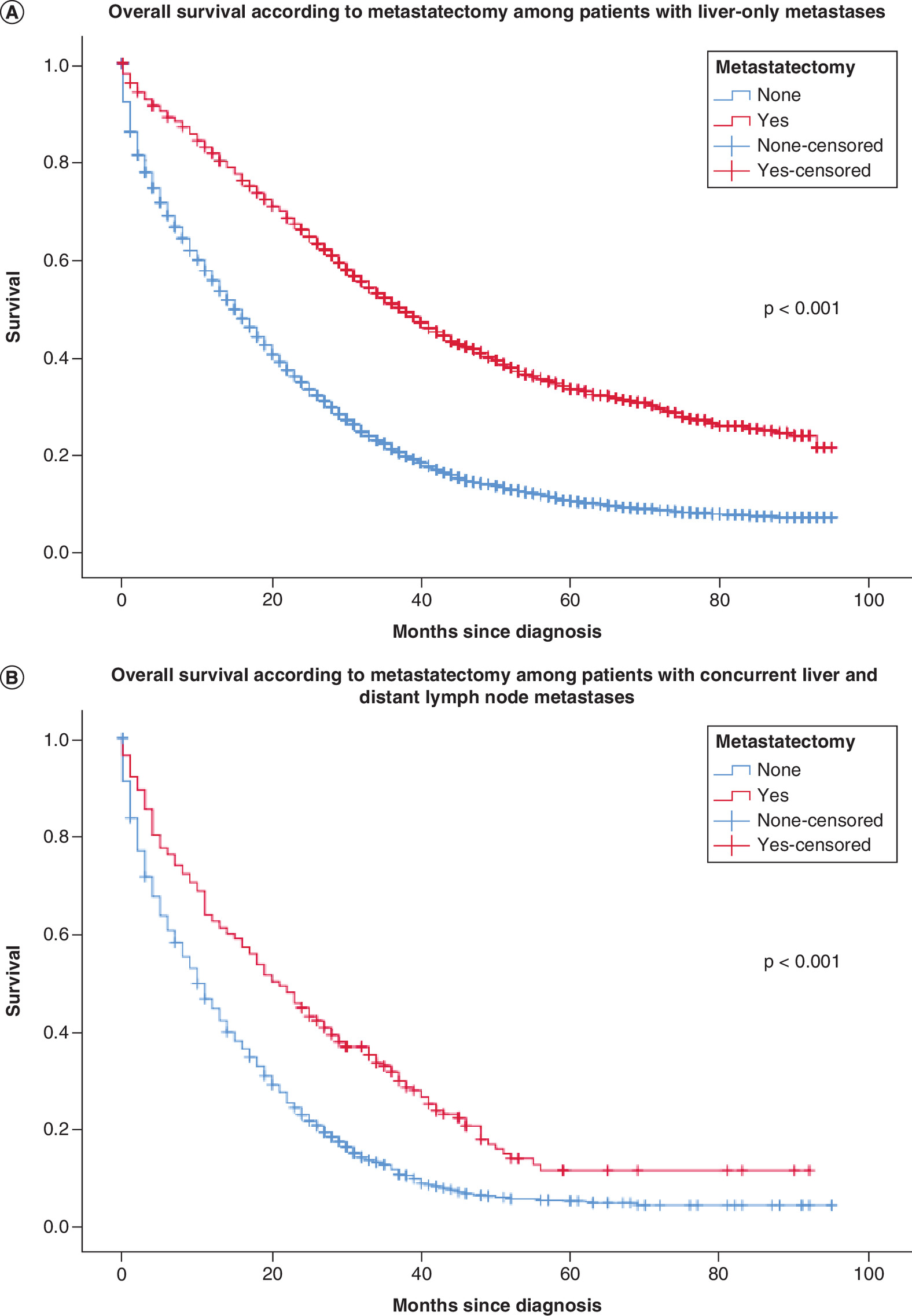
Figure 1. Kaplan-Meier overall survival estimates.
Kaplan–Meier overall survival estimates within the overall cohort according to surgery to metastatic sites among patients with (A) isolated liver metastasis and (B) concurrent liver and distant lymph node metastases.
Multivariable Cox regression analysis suggested that the following factors were associated with better OS: younger age (HR with increasing age: 1.024; 95% CI: 1.022–1.025), white race (HR for African–American race vs white race: 1.233; 95% CI: 1.175–1.295), distal site of the primary (HR: 0.808; 95% CI: 0.778–0.840), absence of distant lymph nodes (HR: 0.697; 95% CI: 0.659–0.737), metastasectomy (HR for no metastasectomy vs metastasectomy: 1.954; 95% CI: 1.858–2.056). Likewise, the following factors were associated with better cancer-specific survival: younger age (HR with increasing age: 1.021; 95% CI: 1.020–1.023), white race (HR for African–American race vs white race: 1.220; 95% CI: 1.160–1.284), distal site of the primary (HR: 0.801; 95% CI: 0.769–0.834), absence of distant lymph nodes (HR: 0.677; 95% CI: 0.639–0.718), metastasectomy (HR for no metastasectomy vs metastasectomy: 1.978; 95% CI: 1.876–2.085) (Table 2).
| Variables | OS, HR (95% CI) | Cancer-specific survival, HR (95% CI) |
|---|---|---|
| Age (continuous) | 1.024 (1.022–1.025) | 1.021 (1.020–1.023) |
| Sex Male Female | Reference 1.004 (0.968–1.040) | Reference 1.026 (0.988–1.965) |
| Race White African–American Asian/Pacific Islander American–Indian/Alaska native | Reference 1.233 (1.175–1.295) 0.931 (0.869–0.997) 0.888 (0.713–1.107) | Reference 1.220 (1.160–1.284) 0.919 (0.855–0.988) 0.849 (0.671–1.074) |
| Sidedness Proximal Distal | Reference 0.808 (0.778–0.840) | Reference 0.801 (0.769–0.834) |
| Grade Grade I Grade II Grade III Grade IV | Reference 1.039 (0.944–1.143) 1.499 (1.354–1.660) 1.718 (1.501–1.965) | Reference 1.063 (0.960–1.176) 1.570 (1.410–1.749) 1.801 (1.564–2.074) |
| Distant lymph nodes Yes No | Reference 0.697 (0.659–0.737) | Reference 0.677 (0.639–0.718) |
| Metastasectomy Yes No | Reference 1.954 (1.858–2.056) | Reference 1.978 (1.876–2.085) |
†
Patients with unknown race, side or grade were included in the analysis but not reported in this table.
HR: Hazard ratio; OS: Overall survival.
Survival analysis in the postpropensity cohort
A total of 226 patients with liver and distant lymph node metastases who underwent surgery were matched to 226 patients who did not undergo surgery (Supplementary Figure 1). There were no significant differences in the baseline characteristics of both groups (Table 3). Kaplan–Meier survival estimates suggested that metastasectomy is associated with improved OS in this postpropensity cohort (median OS of 20 vs 11 months; p < 0.001).
| Variables | Patients who underwent metastasectomy (226 patients), n (%) | Patients who did not undergo metastasectomy (226 patients), n (%) | p-value |
|---|---|---|---|
| Age <40 years 40–69 years ≥70 years | 17 (7.5%) 148 (65.5%) 61 (27%) | 18 (8%) 147 (65%) 61 (27%) | 0.984 |
| Race White African–American Asian/Pacific Islander American–Indian/Alaska native | 181 (80.1%) 31 (13.7%) 13 (5.8%) 1 (0.4%) | 182 (80.5%) 31 (13.7%) 13 (5.8%) 0 (0%) | 0.801 |
| Sidedness Proximal Distal Unknown | 107 (47.3%) 106 (36.9%) 13 (5.8%) | 107 (47.3%) 106 (36.9%) 13 (5.8%) | 1.000 |
| Grade Grade I Grade II Grade III Grade IV Unknown | 6 (2.7%) 115 (50.9%) 61 (27%) 10 (4.4%) 34 (15%) | 7 (3.1%) 115 (50.9%) 61 (27%) 8 (3.5%) 35 (15.5%) | 0.989 |
Discussion
The current study evaluates the impact of metastasectomy on the outcomes of patients with liver and distant lymph node metastases. It suggested that metastasectomy is associated with improved survival in this cohort of patients. It also suggested that distant lymph node involvement is associated with worse survival regardless of whether metastasectomy was attempted.
Metastasectomy has traditionally been recommended for individuals with isolated resectable colorectal liver and/or lung metastases [13]. More recently, cytoreductive surgery (+/-) hyperthermic intraperitoneal chemotherapy has been advocated among selected patients with peritoneal metastases as well [14]. The presence of concurrent distant lymphadenopathy with liver metastases has traditionally been considered a contraindication for surgical resection of the metastases [15]. However, there has generally been a lack of evidence to support this recommendation.
A previous systematic review has evaluated the role of para-aortic lymph node dissection among patients with para-aortic lymph node metastases and it did suggest that dissection confers a survival advantage compared with palliative chemotherapy alone [16]. However, this systematic review did not specifically address the question of the role of metastasectomy in the treatment of patients with concomitant liver and distant lymph node metastases. Previous studies have reviewed the accidental discovery of lymph node metastases as well during pulmonary metastasectomy (reported in 20% of patients) and they did suggest that this is associated with decreased survival. The optimal surgical approach of this scenario (sampling vs dissection) is; however, unclear [17–20]. Surgical treatment has been associated with a doubling of OS in the current study compared with no surgery (among individuals with concurrent liver and distant lymph nodes). Whether this improvement is related to the impact of surgery or related to an understandably higher fitness/more chemotherapy treatment for surgically treated patients is unclear.
The current study has some limitations that need to be discussed. First, the absence of information about performance status and comorbidities is a possible source of bias (patients with higher comorbidities are less likely to undergo aggressive surgical resection and they are also more likely to have worse survival outcomes because of their comorbidities). To limit the impact of this limitation, both OS and cancer-specific survival were evaluated. While OS is likely to be affected by noncancer comorbidities, cancer-specific survival is less likely to be affected by comorbidities. Additionally, propensity score matching was done to adjust for some baseline characteristics within the study cohort. Second, the absence of information about systemic chemotherapy is another limitation. It has to be remembered; however, that several prospective studies suggested that postmetastasectomy chemotherapy does not affect the OS of patients with resected metastatic colorectal cancer [21–23]. Third, details of surgical treatment (particularly whether it involved a formal lymph node dissection or not) are not available. This likely affected the veracity of the conclusions of the current study. Fourth, the site of distant lymph nodes is not reported within the SEER database. While lymph node dissection can be contemplated for selected patients with abdominal/pelvic nodal disease; it is difficult to contemplate a similarly aggressive strategy for other sites of distant lymph nodes. Fifth, the method of diagnosis of distant lymph node metastases are not described within the SEER database. One of the possibilities is that some patients with surgically resected distant lymph nodes have negative preoperative imaging (for the presence of distant lymphadenopathy) but were just discovered to have distant lymph node involvement intraoperatively or as a histological surprise. These patients would have a lower burden of metastatic disease compared with patients clinically diagnosed with bulky distant lymphadenopathy that did obviate surgical removal of the metastases. Sixth, the inability to gauge the true burden of the metastatic disease within the liver/lymph nodes. Clearly, patients who do not undergo surgery due to extensive liver metastases or conversely extensive distant nodal disease, are different from patients with very limited disease who do undergo surgery. The results of the current study thus inform association rather than causation; and further prospective studies are needed to confirm these results. These weaknesses should be assessed against clear strengths of the current study including relatively large size and contemporaneous data collection.
Further research questions in this field would include assessment of the outcomes of patients with limited distant lymphadenopathy in surgically resectable locations versus those with bulky, widespread lymphadenopathy or those with lymph nodes in surgically challenging locations. Additionally, we need to separate the outcomes of patients with microscopically diagnosed distant lymph node metastases versus those with clinically evident bulky lymphadenopathy within preoperative staging (as these should be two distinct groups of patients). Another important question is related to weighing the potential benefits of any surgical intervention versus its harms (which include immediate surgical and anesthetic complications, delay in the start of effective anticancer therapy and possible deterioration in the quality of life because of an aggressive surgery). We need, thus, to identify the best surgical (and nonsurgical approach) that would maximize the chances of long-term disease control for those patients with no or minimal detrimental effect on their quality of life. Multidisciplinary management is key to improve outcomes of cancer patients in general, but in particular those with colorectal liver metastases [24]. These cases need to be discussed among different specialists to reach out to the best treatment course. Additionally direct and indirect costs have to be considered when recommending liver-directed therapies for those patients [25].
In conclusion, metastasectomy seems to be associated with improved survival among patients with concurrent lymph node and liver metastases. It is not clear if improved survival is related to the surgical intervention, or it might be also related to the fact that surgically treated patients have a better general condition and hence improved outcomes. These findings need to be confirmed in a larger cohort of patients; preferably collected prospectively with complete documentation of surgical and nonsurgical treatments received.
•
This study aims to assess the impact of metastasectomy on survival outcomes of patients with concurrent liver and distant nodal metastases.
•
SEER database was accessed and patients with colorectal liver metastases (with or without distant lymph node involvement) were reviewed.
•
Kaplan–Meier survival estimates were then used to assess the impact of the presence of distant lymph node metastases as well as the impact of metastasectomy on overall and cancer-specific survival.
•
A propensity score matching was then conducted between patients with distant lymph node metastases who had surgery versus those who did not have surgery.
•
A total of 15,325 patients were included in the current analysis including 1603 patients who have liver and distant nodal metastases (10.5%) and 13,722 patients who have liver metastases only (89.5%).
•
The following factors were associated with better overall survival (OS): younger age (HR with increasing age: 1.024; 95% CI: 1.022–1.025), white race (HR for African–American race vs white race: 1.233; 95% CI: 1.175–1.295), distal site of the primary (HR: 0.808; 95% CI: 0.778–0.840), absence of distant lymph nodes (HR: 0.697; 95% CI: 0.659–0.737), metastasectomy (HR for no metastasectomy vs metastasectomy: 1.954; 95% CI: 1.858–2.056).
•
Within the postpropensity cohort, metastasectomy is associated with improved OS among patients with concurrent distant lymph node and liver metastases (median OS of 20 vs 11 months; p < 0.001).
•
These findings need to be confirmed in a larger cohort of patients; preferably collected prospectively with complete documentation of surgical and nonsurgical treatments received.
Financial & competing interests disclosure
The author is on the advisory board with Eisai, Roche and Lilly. The author has no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
This article does not contain any studies with human participants or animals performed by the author. As this study is based on a publicly available database without identifying patient information, informed consent was not needed.
Supplementary Material
File (supplementary figure 1.png)
- Download
- 5.93 KB
{kind=link}
References
Papers of special note have been highlighted as: • of interest
1.
Abdel-Rahman O, Karachiwala H. Impact of age on toxicity and efficacy of 5-FU-based combination chemotherapy among patients with metastatic colorectal cancer; a pooled analysis of five randomized trials. Int. J. Colorectal Dis. 34(10), 1741–1747 (2019).
2.
Abdel-Rahman O. Effect of body mass index on 5-FU-based chemotherapy toxicity and efficacy among patients with metastatic colorectal cancer; a pooled analysis of 5 randomized trials. Clin. Colorectal Cancer (2019) (Epub ahead of print).
3.
Abdel-Rahman O. Impact of sex on chemotherapy toxicity and efficacy among patients with metastatic colorectal cancer: pooled analysis of 5 randomized trials. Clin. Colorectal Cancer 18(2), 110–115.e112 (2019).
4.
Primrose J, Falk S, Finch-Jones M et al. Systemic chemotherapy with or without cetuximab in patients with resectable colorectal liver metastasis: the New EPOC randomised controlled trial. Lancet Oncol. 15(6), 601–611 (2014).
5.
Nordlinger B, Sorbye H, Glimelius B et al. Perioperative FOLFOX4 chemotherapy and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC 40983): long-term results of a randomised, controlled, Phase III trial. Lancet Oncol. 14(12), 1208–1215 (2013).
6.
Ampollini L, Gnetti L, Goldoni M et al. Pulmonary metastasectomy for colorectal cancer: analysis of prognostic factors affecting survival. J. Thorac. Dis. 9(Suppl. 12), S1282–S1290 (2017).
7.
Beppu T, Sakamoto Y, Hayashi H, Baba H. Perioperative chemotherapy and hepatic resection for resectable colorectal liver metastases. Hepatobiliary Surg. Nutrition 4(1), 72–75 (2015).
8.
Cokmert S, Ellidokuz H, Demir L et al. Survival outcomes of liver metastasectomy in colorectal cancer cases: a single-center analysis in Turkey. Asian Pac. J. Cancer Prev. 15(13), 5195–5200 (2014).
9.
Shah SA, Haddad R, Al-Sukhni W et al. Surgical resection of hepatic and pulmonary metastases from colorectal carcinoma. J. Am. Coll. Surg. 202(3), 468–475 (2006).
• Evaluates surgical resection of liver and lung metastases from colorectal carcinoma.
10.
Zabaleta J, Aguinagalde B, Fuentes MG et al. Survival after lung metastasectomy for colorectal cancer: importance of previous liver metastasis as a prognostic factor. Eur. J. Surg. Oncol. 37(9), 786–790 (2011).
11.
NCI-SEER. Surveillance, Epidemiology, and End Results (SEER) program. http://www.seer.cancer.gov
13.
Oweira H, Mehrabi A, Reissfelder C, Abdel-Rahman O. A real-world, population-based analysis of the outcomes of colorectal cancer patients with isolated synchronous liver or lung metastases treated with metastasectomy. World J. Surg. 44(5), 1604–1611 (2020).
14.
Abdel-Rahman O. A real-world, population-based study of the outcomes of patients with metastatic colorectal cancer to the peritoneum treated with or without cytoreductive surgery. Int. J. Colorectal Dis. 35(4), 719–725 (2020).
15.
Fujii T, Tabe Y, Yajima R et al. Process of distant lymph node metastasis in colorectal carcinoma: implication of extracapsular invasion of lymph node metastasis. BMC Cancer 11, 216 (2011).
16.
Wong JS, Tan GH, Teo MC. Management of para-aortic lymph node metastasis in colorectal patients: a systemic review. Surg. Oncol. 25(4), 411–418 (2016).
17.
Sihag S, Muniappan A. Lymph node dissection and pulmonary metastasectomy. Thorac. Surg. Clin. 26(3), 315–323 (2016).
18.
Reinersman JM, Wigle DA. Lymphadenectomy during pulmonary metastasectomy. Thorac. Surg. Clin. 26(1), 35–40 (2016).
19.
Shiono S, Matsutani N, Okumura S et al. The prognostic impact of lymph-node dissection on lobectomy for pulmonary metastasis. Eur. J. Cardiothorac. Surg. 48(4), 616–621 (2015).
20.
Renaud S, Falcoz PE, Olland A et al. The intrathoracic lymph node ratio seems to be a better prognostic factor than the level of lymph node involvement in lung metastasectomy of colorectal carcinoma. Interact. Cardiovasc. Thorac. Surg. 20(2), 215–221 (2015).
21.
Portier G, Elias D, Bouche O et al. Multicenter randomized trial of adjuvant fluorouracil and folinic acid compared with surgery alone after resection of colorectal liver metastases: FFCD ACHBTH AURC 9002 trial. J. Clin. Oncol. 24(31), 4976–4982 (2006).
22.
Langer B, Bleiberg H, Labianca R et al. Fluorouracil (FU) plus l-leucovorin (l-LV) versus observation after potentially curative resection of liver or lung metastases from colorectal cancer (CRC): results of the ENG (EORTC/NCIC CTG/GIVIO) randomized trial. Presented at: Proc. Am. Soc. Clin. Oncol. Chicago, IL, USA (2002).
23.
Portier G, Elias D, Bouche O et al. Multicenter randomized trial of adjuvant fluorouracil and folinic acid compared with surgery alone after resection of colorectal liver metastases: FFCD ACHBTH AURC 9002 trial. J. Clin. Oncol. 24(31), 4976–4982 (2006).
24.
Giuliani J, Marzola M. Multidisciplinary approach as the key factor in the management of liver metastases from colorectal cancer. J. Gastrointest. Cancer 44(4), 486–488 (2013).
25.
Giuliani J, Bonetti A. The pharmacological costs of complete liver resections in unselected advanced colorectal cancer patients: focus on targeted agents. A review of randomized clinical trials. J. Gastrointest. Cancer 47(4), 341–350 (2016).
Information & Authors
Information
Published In
Pages: 243 - 250
PubMed: 35075916
Copyright
© 2022 Future Medicine Ltd.
History
Received: 5 June 2021
Accepted: 1 December 2021
Published online: 25 January 2022
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
A real-world, population-based study for the outcomes of patients with metastatic colorectal cancer to the liver with distant lymph node metastases treated with metastasectomy. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0133
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Saira Sanjida, Gail Garvey, Roxanne Bainbridge, Abbey Diaz, Federica Barzi, Sherry Holzapfel, Michael Y. Chen, Harry Collin, Yaqoot Fatima, Xiang-Yu Hou, James Ward, Prevalence of surgery in Indigenous people with cancer: a systematic review and meta-analysis, The Lancet Regional Health - Western Pacific, 10.1016/j.lanwpc.2025.101527, 57, (101527), (2025).