Cost-per-remitter with esketamine nasal spray versus standard of care for treatment-resistant depression
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Estimate the cost-per-remitter with esketamine nasal spray plus an oral antidepressant (ESK + oral AD) versus oral AD plus nasal placebo (oral AD + PBO) among patients with treatment-resistant depression. Patients & methods: An Excel-based model was developed to estimate the cost-per-remitter for ESK + oral AD versus oral AD + PBO over 52 weeks from multiple US payer perspectives. Clinical end points and cost inputs were derived from clinical trials and the literature, respectively. Results: Under the base-case scenario, the cost-per-remitter for ESK + oral AD and oral AD + PBO were as follows: Commercial: US$85,808 versus US$100,198; Medicaid: US$76,236 versus US$96,067; Veteran’s Affairs: US$77,765 versus US$104,519; and Integrated Delivery Network: US$103,924 versus US$142,766. Conclusion: The findings suggest that ESK + oral AD is a cost-efficient alternative treatment for treatment-resistant depression compared with oral AD + PBO.
Lay abstract
The US FDA recently approved esketamine nasal spray plus an oral antidepressant (AD) as a new treatment for adults with treatment-resistant depression. We developed an Excel-based model to understand whether esketamine + oral AD treatment offers better value for the money spent, compared with treatment with oral AD alone. We find that the higher annual costs of esketamine + oral AD treatment are more than offset by the better clinical outcomes achieved with this treatment. Specifically, in a given year, more people treated with esketamine + oral AD versus oral AD alone achieved and remained in remission, and as a result, they incurred fewer other medical costs.
The World Health Organization ranks major depressive disorder (MDD) as the second leading cause of disability in the USA (based on the severity and prevalence of the disease) [1]. MDD results in substantial clinical, economic and societal burden. For example, recent studies reported that presence of depression negatively affects patients’ quality of life and the impact increases with an increase in disease severity [2,3]. In another study of commercially insured patients in the USA, Amos et al. found that the annual per-patient costs for individuals with MDD were US$6700 higher than the costs of similar people without depression [4].
According to the American Psychiatry Association (APA) Guidelines for MDD, the primary goal of treatment for MDD is to achieve remission from the symptoms [5]. This, in turn, results in better outcomes for patients both in the short- and long-term. For example, in the pragmatic STAR*D trial, patients with MDD who achieved remission following treatment functioned better socially and at work, had a better chance of staying well and had significant improvements in quality of life compared with nonremitters [6,7]. Unfortunately, however, under the current standard of care, many patients with MDD do not achieve adequate response with multiple lines of therapy. Researchers typically define depression that does not respond to at least two courses of antidepressant treatment of adequate dose and duration as treatment-resistant depression (TRD) [8–10]. Effective treatment options for patients experiencing TRD are limited. In fact, studies have reported that even after failed responses to at least two adequate lines of antidepressant treatments, oral antidepressants (ADs) remain the most common treatment for patients with TRD and nonpharmacologic treatments such as electroconvulsive therapy (ECT), repeated transcranial magnetic stimulation (rTMS) are particularly limited [11]. As a result, TRD is associated with considerable economic and societal burden; above and beyond that imposed by MDD. For example, in the aforementioned study by Amos et al., the researchers found that the annual per-patient healthcare costs of TRD exceeded the costs of non-TRD MDD and healthy cohorts by US$3200 and US$9900, respectively [4]. Similar results have also been reported for a variety of different populations [11–15]. Indirect costs due to disability as well as medically related absenteeism and productivity loss are also higher among patients with MDD and TRD compared with non-depressed individuals and non-TRD patients, respectively [4,14,16,17].
The US FDA recently approved esketamine (ESK) nasal spray in conjunction with an oral AD (ESK + oral AD) as a new therapeutic alternative for adults with TRD [18]. Unlike standard of care for TRD, this novel therapy is self-administered under direct clinical supervision. In a flexibly dosed Phase III trial evaluating efficacy and tolerability of ESK + oral AD in the short-term (4 weeks), the proportions of patients achieving clinical response (defined as improvement from baseline in Montgomery-Åsberg Depression Rating Scale [MADRS] score ≥50%) or remission (defined as MADRS score ≤12) were statistically significantly higher among those treated with ESK + oral AD compared with oral AD + placebo (PBO) [19]. Additionally, fewer patients treated with ESK + oral AD experienced a relapse in the long-term as compared with those treated with oral AD + PBO [18,20].
Payers with constrained budgets need to understand the value of ESK compared with the standard of care for TRD. The cost–effectiveness and budget implications of ESK + oral AD relative to the standard of care have been estimated previously [21–23]. However, these approaches are either complex and sensitive to differences in modeling assumptions, or focus disproportionately on the budget impact. In addition, the long-term (often, lifetime) perspective considered in the published cost–effectiveness studies necessitates extrapolation of trial data, which compounds uncertainty and makes the interpretation of findings challenging for US decision-makers who do not rely on health technology assessment-type modeling frameworks. In this context, estimates of short-term costs associated with attaining clinically relevant outcomes with the different treatment options within the same therapeutic condition could provide additional valuable information to the payers.
Therefore, in this study, we complement existing modeling studies by implementing a simple and transparent economic evaluation approach consistent with the cost-per-episode framework proposed by the Agency of Healthcare Research and Quality (AHRQ), which allows healthcare plans to ‘identify variations in the amount of money spent on patients with similar health problems with the objective of reducing costs’ [24]. Specifically, we compare the annual per-patient direct costs associated with achieving clinically relevant outcome of remission between ESK + oral AD and oral AD + PBO in the treatment of patients with TRD. The goal of our analysis is to complement other modeling approaches such as the cost–effectiveness analysis and the budget impact analysis by facilitating benefit-per-dollar-spent comparisons across treatment options accounting for differential efficacy. These calculations offer an additional important perspective, over a time horizon that is highly relevant to the US payers. Similar approaches have been employed by studies in several therapeutic areas including TRD [25–31]. For example, using a similar modeling framework, Sussman et al. estimated the cost-per-remitter of brexpiprazole + antidepressant therapy to be US$27,196–US$71,839 higher compared with antidepressants alone [25].
Methods
Modeling framework & key modeling assumptions
Patient population
The target population included TRD patients meeting the eligibility criteria for two key Phase III clinical trials comparing outcomes with ESK + oral AD versus PBO + oral AD in the short-term (Study 1) and long-term (Study 2) [18–20].
Model perspective
Four separate US payer perspectives were considered, reflecting the different cost implications for various insurance providers: Commercial (i.e., employer-sponsored private health insurance); Medicaid; Veteran’s Affairs (VA); and full-risk Integrated Delivery Networks (IDNs; network of providers that provide both healthcare services and health insurance) or payers managing members who receive care at an IDN. Each payer perspective was modeled independently using payer-specific cost inputs (where available). Note that efficacy rates were assumed to be the same across all payers.
Key comparators & outcomes
The model considered two treatment arms consistent with the Phase III clinical trials for esketamine: ESK + oral AD and oral AD + PBO. The per-patient direct costs associated with achieving remission were assessed over a 52-week period and compared between the treatment arms. As a sensitivity analysis, total costs including treatment, healthcare and productivity costs were also considered.
Efficacy end points & health states
Table 1 describes the efficacy inputs for the model. Under the base-case scenario, the efficacy inputs were derived from the short- and long-term clinical trials comparing ESK + oral AD to oral AD + PBO (Study 1 and Study 2, respectively) [19,20].
| Parameter | ESK + Oral AD | Oral AD + PBO |
|---|---|---|
| Base-case estimates | ||
| – Response rate (1st 4 weeks) | 69% | 52% |
| – Remission rate (1st 4 weeks) | 52% | 31% |
| – Cumulative relapse rate – responder (over subsequent 48 weeks) | 26% | 58% |
| – Cumulative relapse rate – remitter (over subsequent 48 weeks) | 27% | 45% |
| STAR*D sensitivity | ||
| – Response rate (1st 4 weeks) | 69% | 17% |
| – Remission rate (1st 4 weeks) | 52% | 14% |
AD: Antidepressant; ESK: Esketamine; PBO: Placebo.
It should be noted that the response and remission rates for oral AD + PBO in the ESK clinical trials are higher than the efficacy rates observed in other studies for TRD [32–37]. This may be attributed to the systematic assessments of the treatment protocols, including prior and concomitant therapies, as well as the frequent and intensive clinical contact that was necessary to maintain blinding in the Phase III trials comparing ESK + oral AD versus oral AD + PBO [38]. Because of the delivery model of ESK, clinical contact will remain frequent among patients receiving ESK in the real world. However, unlike in the ESK clinical trials, in a real-world setting, oral AD treatment is not implemented with the additional level of clinical supervision. Therefore, for a deterministic sensitivity analysis, efficacy rates for the oral AD + PBO arm were derived from the STAR*D study, a real-world effectiveness trial for depression, which may provide a better approximation for real-world outcomes associated with oral AD treatment at different lines of therapy [6]. The efficacy rates observed in the STAR*D study were comparable to other studies evaluating the effectiveness of various treatments for TRD (Supplementary Material 1).
In order to account for changes in the efficacy measures over time as observed in the clinical trials [18–20], remission rates, response rates and relapse rates were assessed in 4-week intervals and patients were categorized as remitters, responders or nonresponders at each interval (Figure 1). Consistent with the clinical trials, remission was defined as MADRS score ≤12 and response was defined as improvement from baseline in MADRS score ≥50% [19]. Patients not achieving either response or remission during the acute phase (i.e., first 4 weeks) were considered nonresponders. In addition, among patients achieving response or remission during the acute phase, rates of relapse during the maintenance phase (i.e., weeks 5–52) were also considered. Relapse was defined as a MADRS total score ≥22 for two consecutive weeks or hospitalization for worsening depression or any other clinically relevant event indicative of relapse [18,20]. Note that patients experiencing a relapse during the maintenance phase were considered as nonresponders during the remainder of the assessment period.

Figure 1. Model framework.
AD: Antidepressants; ESK: Esketamine; PBO: Placebo.
Cost inputs
Table 2 describes the base-case payer-specific cost inputs for the different health states.
| Parameter | Commercial | Medicaid† | VA† | IDN | ||||
|---|---|---|---|---|---|---|---|---|
| ESK + Oral AD | Oral AD + PBO | ESK + Oral AD | Oral AD + PBO | ESK + Oral AD | Oral AD + PBO | ESK + Oral AD | Oral AD + PBO | |
| Treatment costs ($US)‡ | ||||||||
| – Cost per ESK device | 295 | n/a | 226.86 | n/a | 226.86 | n/a | 295 | n/a |
| – Cost per ESK administration (weeks 1–4)§ | 240.59 | n/a | 229.14 | n/a | 229.14 | n/a | 240.59 | n/a |
| – Cost per ESK administration (weeks 5–52)§ | 226.62 | n/a | 214.63 | n/a | 214.63 | n/a | 226.62 | n/a |
| – Avg. weekly costs – all patients (weeks 1–4) | 1961.73 | 5.56 | 1597.39 | 4.83 | 1597.39 | 4.83 | 1961.73 | 5.56 |
| – Avg. weekly costs – before relapse (weeks 5–52) | 969.67 | 5.56 | 786.61 | 4.83 | 786.61 | 4.83 | 969.67 | 5.56 |
| – Avg. weekly costs – after relapse (weeks 5–52) | 21.13 | 19.38 | 19.38 | 18.22 | ||||
| Healthcare costs (weekly; US$) | ||||||||
| – Nonresponder | 368.01 | 342.11 | 386.11 | 517.14 | ||||
| – Responder | 224.97 | 252.09 | 267.76 | 327.19 | ||||
| – Remitter | 156.58 | 171.73 | 148.19 | 288.04 | ||||
†
The prices for esketamine and oral AD were adjusted to reflect the most recent statutory mandate provisions.
‡
During the first 4 weeks, patients on ESK + oral AD received ESK twice weekly. During weeks 5–52, 23.3% of remitters and 54.8% of responder-nonremitters received ESK once a week; the remaining received ESK once every other week. The cost inputs for weeks 5–52 reflect the cost of a single weekly administration of ESK for patients receiving the treatment. Throughout the assessment period, patients were assumed to receive 2.5 devices per administration (to account for the flexible dosing schedule [i.e., 56 or 84 mg; i.e., 2 or 3 devices]). Average weekly costs for ESK also include costs for oral AD.
§
Administration cost includes medical costs due to the administration of the treatment and monitoring post-treatment (e.g., presence of adverse event). For the first administration, all patients were assigned costs for prolonged – monitoring by a physician (CPT codes 99204 and 99354) – US$338 for Commercial and IDNs and US$331 for Medicaid and VA. For all subsequent visits, patients were assumed to receive prolonged monitoring by nonphysician providers (e.g., nurse practitioner) as indicated by CPT codes 99213 and 99354. The resulting administration costs for subsequent visits were US$227 for Commercial and IDNs, and US$215 for Medicaid and VA.
AD: Antidepressant; ESK: Esketamine; IDN: Integrated delivery network; n/a: Not applicable; PBO: Placebo; VA: Veteran’s Affairs.
Treatment costs
Treatment costs for the ESK + oral AD arm include the price of the device used for the administration (US$295/device for Commercial plans and IDNs; US$226.86 for Medicaid and VA to reflect the 23.1% statutory rebates [39,40]) as well as the administration and monitoring costs associated with the esketamine Risk Evaluation and Mitigation Strategy program. Administration costs were derived from the IBM MarketScan Commercial and Medicaid databases [41] using the appropriate CPT codes to indicate whether the patient was monitored by the physician or non-MD provider such as a nurse practitioner (Supplementary Material 2). Throughout the assessment period, patients were assumed to receive 2.5 devices per administration (to account for the flexible dosing schedule [i.e., 56 or 84 mg; i.e., 2 or 3 devices]) [18]. During the acute phase (i.e., first 4 weeks), all patients received ESK twice weekly. Consistent with Study 2, during the maintenance phase (i.e., weeks 5–52), 54.8% of responders and 23.3% of remitters received ESK once a week, whereas the remaining patients received ESK once every 2 weeks [20]. Under the base case, patients were assumed to receive ESK treatment until the first occurrence of relapse, attainment of remission for 7 months to approximate the real-world treatment persistence patterns (only for patients achieving remission during the acute phase) [5,42], or the end of 52 weeks.
All patients in both comparator arms were assumed to receive one of the four oral AD used in the trial (duloxetine, escitalopram, sertraline or extended-release venlafaxine) [18] until the first occurrence of relapse or the end of 52 weeks. The average price of oral AD treatment was estimated to be US$5.56 per week for Commercial and IDN channels [39] and US$4.83 per week for Medicaid and VA channels (to reflect the statutory rebates [40]).
Furthermore, patients who experienced a relapse following an initial response or remission were assumed to cease treatment altogether (in either arm) and were assigned a new treatment initiation cost. The treatment costs of new initiation were assumed to be the average cost of treatment in the population of TRD patients weighted by frequency of various non-ESK treatments as observed in the real world. The treatments considered include oral AD, oral AD-augmented therapies (e.g., with atypical antipsychotics), ECT and rTMS (Table 2) [11,43,44].
Direct healthcare costs
Direct healthcare costs include all costs associated with medical services, such as inpatient and outpatient visits, as well as pharmacy costs. Healthcare costs were assigned to each health state (i.e., remitter, responder and nonresponder) based on the published literature evaluating the average overall healthcare costs associated with treating TRD [4,11–13]: nonresponding/relapsing patients in the model were assumed equivalent to TRD patients in the literature, responding patients were assumed equivalent to ‘Non-treatment resistant MDD’ patients, and patients in remission were assumed equivalent to ‘Non MDD’ patients. The decreases in cost among responders and remitters were based on the adjusted cost differences from patients with TRD after matching on baseline demographics and adjusting for differences in baseline costs and co-morbidities. All costs were converted from annual to weekly figures and inflated to 2019 dollars [45].
Estimating cost-per-remitter
For each comparator arm, the total cost for each category (i.e., treatment and healthcare, and lost productivity [for the sensitivity analysis]) was calculated for a given 4-week interval as the average of the costs for a given health state weighted by the share of patients in that health state. To estimate cost-per-remission, the model accounted for the fact that while all remitters also achieve response, a fraction of responders do not achieve remission. Therefore, the average cost for each comparator arm was calculated as the weighted average of costs for patients achieving remission, those achieving response but not remission, and those not achieving a response, where the weights were the fractions of remitters, responders but not remitters, and non-responders in the population, respectively.
Following this, the cost-per-remitter for each arm was calculated by dividing the average cost for the cohort by the estimated cumulative relapse-free remission rate (at the end of 52 weeks) for that arm.
Sensitivity analyses
Several sensitivity analyses were conducted to test the robustness of the base case results to various modeling assumptions. As with the base case, separate sensitivity analyses were conducted for each payer perspective.
Deterministic sensitivity analysis
Three separate one-way sensitivity analyses were conducted.
First, as already discussed previously, in order to consider alternative efficacy rates associated with oral AD in a real-world setting, sensitivity analyses estimated the cost-per-remitter using the efficacy rates found in the STAR*D study [6]. For this sensitivity analysis, we assumed the response and remission rates observed at line 3 (16.8 and 13.7%, respectively) to represent the outcomes with oral AD + PBO during the acute phase (Table 1). All other parameters were held constant at the base-case values.
Second, the costs-per-remitter were estimated allowing for up to 52 weeks of ESK treatment among patients who attain remission throughout that period to represent a more conservative ceiling cost if, in the real world, the remitters continue and maintain the treatment for more than the base case assumption of 7 months to receive clinical benefits.
Third, the costs-per-remitter were estimated using total costs including direct treatment and healthcare costs as well as indirect costs. Costs due to lost productivity associated with different levels of depression were derived from the literature [14]. Both costs due to absenteeism (i.e., percentage of time missed from work due to health in the past 7 days) and presenteeism (i.e., percentage of impairment while at work in the past 7 days) were considered. Given that lost productivity costs are only applicable for employed people, an employment assumption was included to reflect the employment rate typical for the populations covered by the respective payers. Specifically, for all payers other than Medicaid, the employment rate was assumed 100%. For Medicaid, the employment rate was assumed to be 76% [46].
Probabilistic sensitivity analysis
A Monte Carlo simulation technique was used for this analysis, allowing simultaneous variation of multiple efficacy (remission, response and relapse rates for the two comparators) and medical cost inputs. For each payer perspective, the model was run 5000-times using sets of input parameters that were drawn at random from prespecified distributions representing the expected uncertainty surrounding the mean estimate for a given parameter. The efficacy inputs were assumed to have a binomial distribution and the costs inputs were assumed to have a gamma distribution, all defined with a mean equal to the base case value and a standard deviation of 0.2 [11]. For cost categories, only the nonresponder/relapse cost was drawn for the underlying distribution, and the responder and remitter costs were adjusted proportionally to ensure a logical and consistent ordering of costs among the cohorts.
See Supplementary Exhibits 3–7 for distributions of efficacy and cost inputs considered in these analyses.
Results
Base case
Under the base-case scenario, the cumulative relapse-free remission rates at the end of 52 weeks were 38% for ESK + oral AD and 17% for oral AD + PBO. Correspondingly, the annual cost-per-remitter was lower for ESK + oral AD relative to oral AD + PBO, with differences ranging from US$14,391 for Commercial insurers to US$38,842 for IDNs (Figure 2A–D).

Figure 2. Base case results – cost per remitter with esk+oral AD and oral AD+PBO.
(A) Commercial Insurance. (B) Medicaid. (C) VA. (D) IDN.
AD: Antidepressant; ESK: Esketamine; IDN: Integrated delivery network; PBO: Placebo; VA: Veteran’s Affairs.
Deterministic sensitivity analyses
Under the STAR*D scenario, the cumulative relapse-free remission rates at the end of 52 weeks were 38% for ESK + oral AD and 7% for oral AD + PBO (Table 3). This scenario resulted in higher cost-per-remitter for the oral AD + PBO arm, which in turn increased the cost-per-remitter advantage for ESK + oral AD (e.g., US$161,744 for Medicaid to US$250,354 for IDNs).
| Parameter | Commercial | Medicaid | VA | IDN | ||||
|---|---|---|---|---|---|---|---|---|
| ESK + Oral AD | Oral AD + PBO | ESK + Oral AD | Oral AD + PBO | ESK + Oral AD | Oral AD + PBO | ESK + Oral AD | Oral AD + PBO | |
| Clinical end points | ||||||||
| – Cumulative relapse-free remission rate [A] | 38% | 7% | 38% | 7% | 38% | 7% | 38% | 7% |
| Total annual per-patient costs (US$) | ||||||||
| – Treatment costs† | 19,584 | 963 | 15,964 | 881 | 15,964 | 881 | 19,521 | 837 |
| – Healthcare costs | 13,437 | 18,053 | 13,373 | 16,937 | 13,962 | 18,893 | 20,470 | 25,688 |
| – Total treatment and healthcare costs [B] | 33,021 | 19,016 | 29,337 | 17,818 | 29,925 | 19,774 | 39,992 | 26,526 |
| Cost-per-remitter [B]/[A] (US$) | 85,808 | 253,978 | 76,236 | 237,980 | 77,766 | 264,106 | 103,925 | 354,279 |
| Difference (Oral AD + PBO − ESK + Oral AD) | 168,169 | 161,744 | 186,340 | 250,354 | ||||
†
Includes average weekly costs for new line of treatment after relapse – estimated to be US$21.13 for Commercial, US$18.22 for IDN, and US$19.38 for Medicaid and VA. During the first 4 weeks, patients received ESK twice weekly. During weeks 5–52, 23.3% of remitters and 54.8% of responder-nonremitters received ESK once a week; the remaining received ESK once every other week. The duration of ESK treatment was the minimum of time to relapse, nonresponse, end of 7 months (for remitters only) or end of 52 weeks. All patients in both arms received oral AD until they relapsed or reached end of the 52-week period, whichever occurred first.
AD: Antidepressant; ESK: Esketamine; IDN: Integrated delivery network; PBO: Placebo; VA: Veteran’s Affairs.
Under the 12-month ESK treatment scenario, the cumulative relapse-free remission rates at the end of 52 weeks was same as the base case scenario (i.e., 38% for ESK + oral AD and 17% for oral AD + PBO) (Table 4). However, the remitters in ESK + oral AD treatment arm incurred higher costs for continuing ESK treatment beyond 7 months of remission, resulting in higher cost-per-remitter compared with the base-case scenario. Despite this, ESK + oral AD treatment was associated with lower cost-per-remitter than the oral AD + PBO treatment for all non-Commercial payers, with direct cost-per-remitter advantages ranging from US$8148 for Medicaid to US$24,433 for IDNs.
| Parameter | Commercial | Medicaid | VA | IDN | ||||
|---|---|---|---|---|---|---|---|---|
| ESK + Oral AD | Oral AD + PBO | ESK + Oral AD | Oral AD + PBO | ESK + Oral AD | Oral AD + PBO | ESK + Oral AD | Oral AD + PBO | |
| Clinical end points | ||||||||
| – Cumulative relapse-free remission rate [A] | 38% | 17% | 38% | 17% | 38% | 17% | 38% | 17% |
| Total annual per-patient costs (US$) | ||||||||
| – Treatment costs† | 25,189 | 821 | 20,460 | 748 | 20,460 | 748 | 25,066 | 722 |
| – Healthcare costs | 13,437 | 16,154 | 13,373 | 15,527 | 13,962 | 16,959 | 20,471 | 23,465 |
| – Total treatment and Healthcare costs [B] (US$) | 38,565 | 16,975 | 33,833 | 16,276 | 34,422 | 17,707 | 45,537 | 24,187 |
| Cost-per-remitter [B]/[A] | 100,217 | 100,198 | 87,920 | 96,067 | 89,449 | 104,519 | 118,333 | 142,766 |
| Difference (Oral AD + PBO − ESK + Oral AD) | (19) | 8148 | 15,070 | 24,433 | ||||
†
Includes average weekly costs for new line of treatment after relapse – estimated to be US$21.13 for Commercial, US$18.22 for IDN, and US$19.38 for Medicaid and VA. During the first 4 weeks, patients received ESK twice weekly. During weeks 5–52, 23.3% of remitters and 54.8% of responder-nonremitters received ESK once a week; the remaining received ESK once every other week. The duration of ESK treatment was the minimum of time to relapse, nonresponse, end of 7 months (for remitters only) or end of 52 weeks. All patients in both arms received oral AD until they relapsed or reached end of the 52-week period, whichever occurred first.
AD: Antidepressant; ESK: Esketamine; IDN: Integrated delivery network; PBO: Placebo; VA: Veteran’s Affairs.
For the scenario including costs due to lost productivity, the cumulative relapse-free remission rates at the end of 52 weeks were also the same as the base-case scenario. However, compared with the base case scenario, the cost-per-remitter advantages with ESK + oral AD treatment in this scenario were greater by up to 300%, depending on the plan type (Table 5).
| Parameter | Commercial | Medicaid | VA | IDN | ||||
|---|---|---|---|---|---|---|---|---|
| ESK + Oral AD | Oral AD + PBO | ESK + Oral AD | Oral AD + PBO | ESK + Oral AD | Oral AD + PBO | ESK + Oral AD | Oral AD + PBO | |
| Clinical end points | ||||||||
| – Cumulative relapse-free remission rate [A] | 38% | 17% | 38% | 17% | 38% | 17% | 38% | 17% |
| Total annual per-patient costs (US$) | ||||||||
| – Treatment costs† | 19,584 | 821 | 15,964 | 748 | 15,964 | 748 | 19,521 | 722 |
| – Healthcare costs | 13,437 | 16,154 | 13,373 | 15,527 | 13,962 | 16,959 | 20,471 | 23,465 |
| – Productivity costs‡ | 18,020 | 21,266 | 13,695 | 16,162 | 18,020 | 21,266 | 18,020 | 21,266 |
| – Total treatment, healthcare, productivity costs [B] (US$) | 51,041 | 38,242 | 43,032 | 32,438 | 47,946 | 38,974 | 58,012 | 45,454 |
| Cost-per-remitter [B]/[A] | 132,636 | 225,724 | 111,825 | 191,467 | 124,593 | 230,045 | 150,752 | 268,292 |
| Difference (Oral AD + PBO − ESK + Oral AD) | 93,088 | 79,642 | 105,452 | 117,540 | ||||
†
Includes average weekly costs for new line of treatment after relapse – estimated to be US$21.13 for Commercial, US$18.22 for IDN, and $19.38 for Medicaid and VA. During the first 4 weeks, patients received ESK twice weekly. During weeks 5–52, 23.3% of remitters and 54.8% of responder-nonremitters received ESK once a week; the remaining received ESK once every other week. The duration of ESK treatment was the minimum of time to relapse, nonresponse, end of 7 months (for remitters only) or end of 52 weeks. All patients in both arms received oral AD until they relapsed or reached end of the 52-week period, whichever occurred first.
‡
For productivity cost estimates, for all payers other than Medicaid, the employment rate was assumed to be 100%. For Medicaid, the employment rate was assumed to be 76%. The weekly costs for nonresponders, responders and remitters were US$478.29, US$297.62 and US$226.91.
AD: Antidepressant; ESK: Esketamine; IDN: Integrated delivery network; PBO: Placebo; VA: Veteran’s Affairs.
Probabilistic sensitivity analyses
Probabilistic sensitivity analysis found a cost-per-remitter advantage for ESK + oral AD across 54–68% of input specifications, depending on the plan type (Figure 3A–D). Among the scenarios resulting in lower cost-per-remitter for ESK + oral AD relative to oral AD + PBO, the magnitudes of these advantages ranged from approximately US$40 to over US$500,000, depending on the input specifications and plan type. Among the scenarios resulting in higher cost-per-remitter for ESK + oral AD relative to oral AD + PBO, the magnitudes of cost-per-remitter disadvantages ranged from approximately US$20 up to US$70,000.
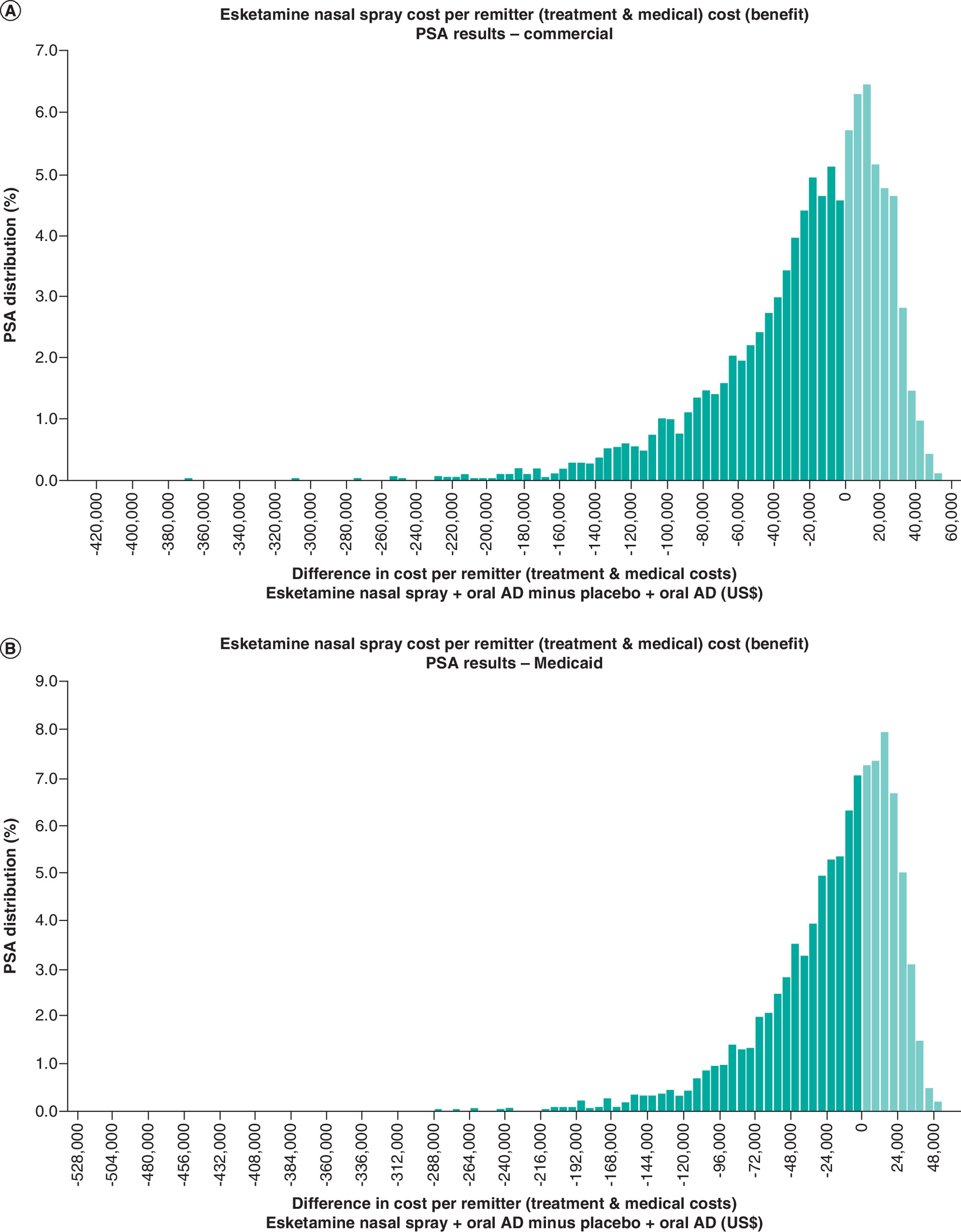

Figure 3. Probability Sensitivity Analysis Results (Cost per remission using direct costs).
(A) Commercial Insurance. (B) Medicaid. (C) VA. (D) IDN.
IDN: Integrated delivery network; VA: Veteran’s Affairs.
Discussion
In Phase III clinical trials, treatment with ESK in conjunction with oral antidepressants resulted in significantly higher response and remission rates as well as significantly lower relapse rates compared with oral antidepressants alone among patients with TRD [18,19]. In our study, we find that these improved efficacy outcomes are associated with a lower cost-per-remitter for ESK + oral AD treatment compared with oral antidepressants alone. For example, the costs-per-remitter from the Commercial insurer’s perspective were US$85,808 for ESK + oral AD compared with US$100,198 for oral AD + PBO. The results were robust to the underlying modeling assumptions. For example, 54–68% of the input specifications for the probabilistic sensitivity analysis resulted in a cost-per-remitter advantage for ESK + oral AD. Similarly, ESK + oral AD treatment was associated with smaller, yet meaningful cost-per-remitter advantages under a scenario that allowed for up to 12 months of the more expensive ESK + oral AD treatment for patients who continue to be in remission after initial treatment (as opposed to 7 months under the base-case scenario) for all but Commercial payers. The cost-per-remitter advantages with ESK increased when accounting for productivity changes or the potential overestimation of oral AD efficacy in the context of the more frequent clinical contact during the ESK trial.
Taken together, these findings suggest that treatment with ESK, inclusive of administration and monitoring costs, could result in improved cost efficiency – a dollar spent on ESK nasal spray yields more clinical benefits on average than a dollar spent on oral AD. This finding stems from better short- and long-term treatment efficacy and lower medical costs compared with oral AD alone.
Our study provides important additional evidence to payers as they contemplate the appropriate coverage of ESK nasal spray for TRD. Specifically, we used a simple but effective approach consistent with the cost per episode framework proposed by AHRQ to assess economic value associated with the higher clinical efficacy observed with ESK nasal spray relative to oral AD from a variety of payer perspectives, in order to complement the information generated from other economic evaluations related to ESK nasal spray. While this framework does not estimate an incremental cost–effectiveness ratio or facilitate comparisons against established thresholds of cost–effectiveness, it does provide payers and physicians information about the value of using ESK + oral AD relative to oral AD alone for treating patients with TRD in an intuitive manner. Specifically, unlike the typical cost–effectiveness or cost-utility analyses that rely on projected quality-adjusted life years gained over a patient’s lifetime, the dichotomous outcomes considered in this study represent the most relevant end points from a physician and payer’s perspective: whether or not a patient attained remission from TRD treatment during a year. Relatedly, the more traditional economic evaluations often involve a complex set of underlying modeling assumptions and calculations making the interpretation of findings difficult. For example, the differences in time horizons and other methodological assumptions employed in the cost–effectiveness analyses by Hernandez et al. and Agboola et al. resulted in a wide range of incremental cost–effectiveness ratio estimates [21,23]. Consequently, it is difficult to understand the true value of ESK + oral AD treatment. In contrast, this cost-per-remitter analysis uses inputs gathered directly from the clinical trials for ESK and published literature and can be easily replicated and updated in case of emerging clinical or economic evidence.
Our study findings take on added relevance to US payers as the estimates of direct healthcare costs used in this study were based on robust and recent analyses of real-world databases that represent populations typically served by that payer. Relatedly, the indirect costs considered as part of the sensitivity analyses are particularly relevant for large self-insured employers, or entities who serve employers, whose businesses may be adversely affected because of reduced productivity among employees with TRD. Additionally, the study employed rigorous techniques to account for uncertainty around the inputs and found robust results.
There are a number of limitations to this model that may affect the real-world applicability of its results. First, the analysis is based on the population included in the Phase III clinical trials of ESK nasal spray and may not be representative of the overall TRD population. Relatedly, consistent with the Phase III clinical trials for ESK, the study only compared the outcomes relative to oral AD. However, in the real-world, some patients with TRD may receive other treatments such as antipsychotic augmentation, ECT and rTMS. Future studies should compare the clinical and cost outcomes associated with ESK + oral AD treatment relative to these other therapeutic alternatives. Second, given the double-blind randomization approach in the clinical trials for ESK, all patients in the oral AD + PBO arm were also required to take their medication under medical supervision, which does not reflect the real-world practice. Indeed, the observed remission/response rates in the oral AD + PBO arm are substantially higher than other reported estimates for oral ADs, including the STAR*D study [6,32]. Using the efficacy rates from the STAR*D study, which may provide a more realistic estimate of the efficacy of oral ADs as used in clinical practice, the cost-per-remitter advantages of ESK + oral AD were even greater. Therefore, our estimates under the base-case assumptions may understate the true cost-per-remitter advantage with ESK nasal spray. Third, direct and indirect cost assumptions for this study were derived from the published literature and may not fully represent the real-world costs. In addition, while the model used payer-specific costs where possible, the treatment costs do not reflect actual commercial arrangements with payers. Fourth, with the exception of Medicaid, the indirect cost estimates assume 100% employment for patients and do not reflect potential differences in the rate of re-engagement in the labor force due to the improved clinical outcomes among patients with ESK + oral AD versus oral AD + PBO. Relatedly, the model does not consider productivity gains among the informal labor force (e.g., unpaid caregivers) that may be achieved with improved clinical outcomes among patients with ESK + oral AD. Finally, all patients were assumed to follow a similar, and consistent, pattern of initiating a new line of therapy following a relapse, which may not represent the actual treatment among these patients. For example, patients may be more likely to initiate an adjunctive atypical antipsychotic following ESK + oral AD failure than with oral AD + PBO failure. Similarly, patients experiencing a relapse/nonresponse could initiate a new line of treatment at any point during the assessment period, not necessarily immediately after relapse/nonresponse to treatment. Relatedly, the model does not account for potential differences in adherence and persistence to treatment between the clinical trials and the real world.
Conclusion
In conclusion, the estimates from this study show that esketamine nasal spray in conjunction with an oral antidepressant is a cost-efficient alternative for patients with TRD, as higher treatment costs are more than offset by improved clinical outcomes. The cost-per-remitter advantages for esketamine are particularly pronounced when considering the costs associated with lost productivity or the potential over-estimation of oral AD efficacy due to the more frequent clinical contact during esketamine trials relative to the real-world medical practice. These results provide important information to decision-makers as they contemplate the value of esketamine nasal spray as a treatment for TRD patients.
•
Many patients with major depressive disorder do not achieve adequate response with multiple lines of therapy.
•
People who do not respond to at least two courses of antidepressant treatment of adequate dose and duration are considered to have treatment-resistant depression (TRD).
•
Under the current standard of care, effective treatment options for people with TRD are limited, resulting in considerable economic and societal burden; above and beyond that imposed by major depressive disorder.
•
The US FDA recently approved esketamine (ESK) nasal spray in conjunction with an oral antidepressant (AD) as a new therapeutic alternative for adults with TRD.
•
In this study, we use a simple and intuitive modeling approach to quantify the benefit-per-dollar-spent for treating patients with TRD with ESK plus oral AD versus oral AD alone.
•
The clinical inputs were derived directly from the pivotal trials for ESK nasal spray, whereas the cost inputs were derived from the published literature.
•
We find that the higher annual costs associated with ESK treatment are more than offset by the better clinical outcomes achieved with this treatment.
•
These findings complement other existing economic evaluations for ESK nasal spray and provide additional evidence to payers and physicians as they contemplate the value of ESK as a treatment for TRD patients.
Author contributions
U Desai and NY Kirson contributed to the conception and design, interpretation of the data and drafting of the paper. A Guglielmo, T Spittle and J Tseng-Tham contributed to the analysis and interpretation of the data and drafting of the paper. M Shawi, HH L and JJ Sheehan contributed to the conception and design, interpretation of the data and critical revisions to the manuscript for intellectual content. All the authors have reviewed and approved the manuscript and agree to be accountable for all aspects of the work.
Acknowledgments
Preliminary results from the study were presented during the poster sessions at ISPOR 2019 Annual Meeting, 20–23 May 2019, New Orleans, LA, USA.
Financial & competing interests disclosure
Funding for this research was provided by Janssen Scientific Affairs. The authors from Janssen reviewed the manuscript and made critical revisions for intellectual content. U Desai, NY Kirson, T Spittle and J Tseng-Tham are employees of Analysis Group, Inc., a company that received funding for this study from Janssen Scientific Affairs. M Shawi, HH L and JJ Sheehan are employees of Janssen Scientific Affairs. A Guglielmo was an employee of Analysis Group, Inc. at the time of this study. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_file.docx)
- Download
- 65.24 KB
References
Papers of special note have been highlighted as: • of interest
1.
The US Burden of Disease Collaborators. The State of US Health, 1990–2016: burden of diseases, injuries, and risk factors among US states. JAMA 319(14), 1444–1472 (2018).
2.
Mitchell PM, Al-Janabi H, Richardson J, Iezzi A, Coast J. The relative impacts of disease on health status and capability wellbeing: a multi-country study. PLoS ONE 10(12), e0143590 (2015).
3.
Salomon J, Vos T, Hogan D et al. Common values in assessing health outcomes from disease and injury: disability weights measurement study for the Global Burden of Disease Study 2010. Lancet 380(9859), 2129–2143 (2012).
4.
Amos T, Tandon N, Lefebvre P et al. Direct and indirect cost burden and change of employment status in treatment-resistant depression. J. Clin. Psych. 79(2), 1–9 (2018).
• Exemplifies the considerable economic and societal burden imposed by treatment-resistant depression (TRD) in the real-world, above and beyond that of major depressive disorder.
5.
American Psychiatry Association. Practice Guideline for the Treatment of Patients with Major Depressive Disorder, 3rd Edition. (2010). https://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/mdd.pdf
6.
Rush J, Trivedi M, Wisniewski S et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR* D report. Am. J. Psych. 163(11), 1905–1917 (2006).
7.
Steiner AJ, Boulus N, Wright SM et al. Major depressive disorder in patients with doctoral degrees: patient-reported depressive symptom severity, functioning, and quality of life before and after initial treatment in the STAR*D study. J. Psychiatr. Pract. 23(5), 328–341 (2017).
8.
Gaynes BN, Asher G, Gartlehner G et al. Definition of treatment-resistant depression in the Medicare population (2018). www.ncbi.nlm.nih.gov/books/NBK526366/pdf/Bookshelf_NBK526366.pdf
9.
Mrazek D, Hornberger J, Altar CA, Degtiar I. A review of the clinical, economic, and societal burden of treatment-resistant depression: 1996–2013. Psychiatr. Serv. 65(8), 977–987 (2014).
10.
Little A. Treatment-resistant depression. Am. Fam. Physician 80, 167–172 (2009).
11.
Pilon D, Szukis H, Joshi K et al. US Integrated Delivery Networks perspective on economic burden of patients with treatment-resistant depression: a retrospective matched-cohort Study. Pharmacoecon Open. 4(1), 119–131 (2020).
• Finds that despite guidelines recommending otherwise, in the real-world, oral antidepressants remain the mainstay treatment among people with TRD and that use of nonpharmacological treatments such as electroconvulsive therapy and repeated transcranial magnetic stimulation is extremely limited.
12.
Szukis H, Benson C, Huang A et al. Economic burden of illness among US veterans with treatment-resistant depression. Presented at: Psych Congress. FL, USA, 25–28 October 2018.
13.
Pilon D, Sheehan JJ, Szukis H et al. Medicaid spending burden among beneficiaries with treatment-resistant depression. J. Comp. Eff. Res. 8(6), 381–392 (2019).
14.
Chow W, Doane M, Sheehan J, Alphs L, Le H. Economic burden among patients with major depressive disorder: an analysis of health care resource use, work productivity, and direct and indirect costs by depression severity. Presented at: AMCP Nexus Meeting. FL, USA, 22–25 October 2018.
15.
Shrestha A, Roach M, Joshi K et al. Incremental health care burden of treatment-resistant depression among Commercial, Medicaid, and Medicare payers. Psychiatr. Serv. 71(6), 593–601 (2020).
16.
Clark M, DiBenedetti D, Perez V. Cognitive dysfunction and work productivity in major depressive disorder. Expert Rev. Pharmacoecon. Outcomes Res. 16(4), 455–463 (2016).
17.
Ivanova J, Birnbaum H, Kidolezi Y, Subramanian G, Khan SA, Stensland MD. Direct and indirect costs of employees with treatment-resistant and non-treatment-resistant major depressive disorder. Curr. Med. Res. Opin. 26(10), 2475–2484 (2010).
18.
Janssen. Full prescribing information for SPRAVATOTM. www.janssenlabels.com/package-insert/product-monograph/prescribing-information/SPRAVATO-pi.pdf
19.
Popova V, Daly EJ, Trivedi M et al. Efficacy and safety of flexibly dosed esketamine nasal spray combined with a newly initiated oral antidepressant in treatment-resistant depression: a randomized double-blind active-controlled study. Am. J. Psych. 176(6), 428–438 (2019).
20.
Daly EJ, Trivedi M, Janik A et al. Efficacy of esketamine nasal spray plus oral antidepressant treatment for relapse prevention in patients with treatment-resistant depression. JAMA Psych. 76(9), 893–903 (2019).
21.
Hernandez LG, Li S, Toro-Diaz H, Zhang Q, Sheehan J, Le H. Cost-effectiveness analysis of esketamine in treatment-resistant depression in the United States. Value Health 22(Suppl. 2), S228–S229 (2019).
22.
Le HH, Zhang Q, Sheehan JJ. Budget impact analysis of esketamine in treatment-resistant depression in the United States. Value Health. 22(Suppl. 2), S229–S230 (2019).
23.
Agboola F, Atlas S, Touchette DR, Fazioli K, Pearson SD. The effectiveness and value of esketamine for the management of treatment-resistant depression: a summary from the Institute for Clinical and Economic Review’s Midwest Comparative Effectiveness Public Advisory Council. J. Manag. Care Spec. Pharm. 26(1), 16–20 (2020).
24.
Agency for Healthcare Research and Quality. Identifying, categorizing, and evaluating health care efficiency measures. AHRQ Publication No. 08-0030 (2008). www.ahrq.gov/research/findings/final-reports/efficiency/hcemch2.html
25.
Sussman M, Yu J, Kamat SA et al. Cost-effectiveness of brexpiprazole adjunctive treatment for major depressive disorder. J. Affect. Disord. 207, 54–62 (2017).
• Used an evaluation approach similar to ours and in the same therapeutic area of TRD.
26.
Malone DC. A budget-impact and cost-effectiveness model for second-line treatment of major depression. J. Manag. Care 13, S8–S18 (2007).
27.
Ektare VU, Lopez J, Martin SC, Patel DA, Rupnow MFT, Botteman MF. Cost efficiency of canagliflozin versus sitagliptin for type 2 diabetes mellitus. Am. J. Manag. Care 20(Suppl. 10), S204–S215 (2014).
28.
Cannon AJ, Bargiota A, Billings L et al. Evaluation of the short-term cost-effectiveness of IDegLira versus basal insulin and basal-bolus therapy in patients with type 2 diabetes based on attainment of clinically relevant treatment targets. J. Manag. Care Spec. Pharm. 26(2), 143–153 (2020).
29.
Ueno F, Doi M, Kawai Y, Ukawa N, Cammarota J, Betts KA. Number needed to treat and cost per remitter for biologic treatments of Crohn’s disease in Japan. J. Med. Econ. 23(1), 80–85 (2020).
• Used an evaluation approach similar to ours.
30.
Teeple A, Muser E. Cost per response for guselkumab versus adalimumab in the United States using data from a head-to-head trial in moderate-to-severe plaque psoriasis. J. Med. Econ. 22(12), 1268–1273 (2019).
31.
Afonso M, Ryan F, Pitcher A, Lew E. Evaluating drug cost per responder and number needed to treat associated with lixisenatide on top of glargine when compared to rapid-acting insulin intensification regimens on top of glargine, in patients with type 2 diabetes in the UK, Italy, and Spain. J. Med. Econ. 20(6), 633–639 (2017).
32.
Papakostas GI, Fava M, Thase ME. Treatment of SSRI-resistant depression: a meta-analysis comparing within- versus across-class switches. Biol. Psych. 63(7), 699–704 (2008).
33.
Shelton RC, Williamson DJ, Corya SA et al. Olanzapine/fluoxetine combination for treatment-resistant depression: a controlled study of SSRI and nortriptyline resistance. J. Clin. Psych. 66(10), 1289–1297 (2005).
34.
Thase ME, Corya SA, Osuntokun O et al. A randomized, double-blind comparison of olanzapine/fluoxetine combination, olanzapine, and fluoxetine in treatment-resistant major depressive disorder. J. Clin. Psych. 68(2), 224–236 (2007).
35.
Thase ME, Youakim JM, Skuban A. Efficacy and safety of adjunctive brexpiprazole 2 mg in major depressive disorder: a Phase III, randomized, placebo-controlled study in patients with inadequate response to antidepressants. J. Clin. Psych. 76, 1224–1231 (2015).
36.
Thase ME, Youakim JM, Skuban A. Adjunctive brexpiprazole 1 and 3 mg for patients with major depressive disorder following inadequate response to antidepressants: a Phase III, randomized, double-blind study. J. Clin. Psych. 76, 1232–1240 (2015).
37.
Blumberger DM, Mulsant BH, Fitzgerald PB et al. A randomized double-blind sham-controlled comparison of unilateral and bilateral repetitive transcranial magnetic stimulation for treatment-resistant major depression. World J. Biol. Psych. 13(6), 423–435 (2012).
38.
Posternak MA, Zimmerman M. Therapeutic effect of follow-up assessments on antidepressant and placebo response rates in antidepressant efficacy trials: meta-analysis. Br. J. Psych. 190, 287–292 (2007).
39.
Red Book Online [database online]. Truven Health Analytics, Inc, CO, USA. www.ibm.com/products/micromedex-red-book
40.
Medicaid Drug Rebate Program (2020). www.medicaid.gov/medicaid/prescription-drugs/medicaid-drug-rebate-program/index.html
41.
Janssen. Data on File.
42.
Keyloun KR, Hansen RN, Hepp Z, Gillard P, Thase ME, Devine EB. Adherence and persistence across antidepressant therapeutic classes: a retrospective claims analysis among insured US patients with major depressive disorder (MDD). CNS Drugs 31, 421–432 (2017).
43.
Ross E, Zivin K, Maixner D. Cost–effectiveness of electroconvulsive therapy vs pharmacotherapy/psychotherapy for treatment-resistant depression in the United States. JAMA Psych. 75(7), 713–722 (2018).
44.
Voigt J, Carpenter L, Leuchter A. Cost effectiveness analysis comparing repetitive transcranial magnetic stimulation to antidepressant medications after a first treatment failure for major depressive disorder in newly diagnosed patients – a lifetime analysis. PLoS ONE 12, 10 (2017).
45.
United States Bureau of Labor Statistics. Consumer Price Index for Medical Care (2020). www.bls.gov/cpi/factsheets/medical-care.htm
46.
Kaiser Family Foundation. Distribution of the nonelderly with Medicaid by family work status. State Health Facts. (2017). www.kff.org/medicaid/state-indicator/distribution-by-employment-status-4/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D
Information & Authors
Information
Published In
Pages: 393 - 407
PubMed: 33565893
Copyright
© 2021 Janssen Scientific Affairs, LLC. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 9 December 2020
Accepted: 13 January 2021
Published online: 10 February 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost-per-remitter with esketamine nasal spray versus standard of care for treatment-resistant depression. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0276
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Sajan Gunarathna, Yongha Hwang, Jung-Seok Lee, Existing Evidence from Economic Evaluations of Antimicrobial Resistance—A Systematic Literature Review, Antibiotics, 10.3390/antibiotics14111072, 14, 11, (1072), (2025).
- Mary Lou Chatterton, Johana Kevin Perez, Thao Thai, Jan Faller, Colleen K. Loo, Nick Glozier, David Barton, Bernhard T. Baune, Natalie T. Mills, Paul B. Fitzgerald, Paul Glue, Shanthi Sarma, Dusan Hadzi-Pavlovic, Vanessa Dong, Donel Martin, Philip B. Mitchell, Michael Berk, Gregory Carter, Maree Hackett, Sean Hood, Andrew A. Somogyi, Anthony Rodgers, Cathrine Mihalopoulos, Economic evaluation of subcutaneous ketamine injections for treatment resistant depression: A randomised, double-blind, active-controlled trial – The KADS study, Journal of Affective Disorders, 10.1016/j.jad.2025.119502, 387, (119502), (2025).
- J. Antoni Ramos-Quiroga, Fernando Mora, Silvia Arostegui, Narcís Cardoner, Jon-Inaki Etxeandia-Pradera, Rocío Gómez-Juanes, Marcos Gómez-Revuelta, José Manuel Montes, Eduard Vieta, Treatment-resistant depression and intranasal esketamine: Spanish clinical consensus on practical aspects, The European Journal of Psychiatry, 10.1016/j.ejpsy.2025.100313, 39, 3, (100313), (2025).
- Lucio N. Gordan, Arielle G. Bensimon, Fan Mu, Nina Kim, Bingcao Wu, Dee Lin, Agne Paner, Jessica Fowler, Alex Marshall, Suzy Van Sanden, Eric Ammann, Joe Goble, Xinke Zhang, Hoa H. Le, Elissa E. Min, Louis P. Garrison, Cost per responder for teclistamab and elranatamab in relapsed or refractory multiple myeloma in the United States, Journal of Medical Economics, 10.1080/13696998.2025.2514909, 28, 1, (910-920), (2025).
- Kristin Clemens, Amanda Teeple, Benoit Rive, Noam Kirson, Urvi Desai, Jason Doran, Diab Eid, Alice Qu, Hannah Bowrey, Kruti Joshi, Cost-per-remitter for esketamine nasal spray versus quetiapine for treatment-resistant depression, Journal of Comparative Effectiveness Research, 10.57264/cer-2024-0092, 14, 7, (2025).
- Masayuki Saruta, Isao Kawaguchi, Yuji Ogawa, Yuri Sanchez Gonzalez, Naoki Numajiri, Xiaohe Tang, Russell Miller, Assessing the economics of biologic and small molecule therapies for the treatment of moderate to severe ulcerative colitis in Japan: a cost per responder analysis of upadacitinib, Journal of Medical Economics, 10.1080/13696998.2024.2333683, 27, 1, (566-574), (2024).
- Isaure Estrade, Anne-Cécile Petit, Vincent Sylvestre, Michel Danon, Sylvain Leroy, Rebecca Perrain, Fabien Vinckier, Lila Mekaoui, Raphaël Gaillard, Emmanuelle Advenier-Iakovlev, Rossella Letizia Mancusi, Daphnée Poupon, Pierre De Maricourt, Philip Gorwood, Early effects predict trajectories of response to esketamine in treatment-resistant depression, Journal of Affective Disorders, 10.1016/j.jad.2023.09.030, 342, (166-176), (2023).
- Laura A. Hannah, Cathy M. Walsh, Louise Jopling, Jesus Perez, Rudolf N. Cardinal, Rory A. Cameron, Economic evaluation of interventions for treatment-resistant depression: A systematic review, Frontiers in Psychiatry, 10.3389/fpsyt.2023.1056210, 14, (2023).
- Madeline Brendle, Reid Robison, Daniel C. Malone, Cost-effectiveness of esketamine nasal spray compared to intravenous ketamine for patients with treatment-resistant depression in the US utilizing clinical trial efficacy and real-world effectiveness estimates, Journal of Affective Disorders, 10.1016/j.jad.2022.09.083, 319, (388-396), (2022).
- Madeline Brendle, Sachin Ahuja, Maisa Della Valle, Claire Moore, Paul Thielking, Daniel C Malone, Reid Robison, Safety and effectiveness of intranasal esketamine for treatment-resistant depression: a real-world retrospective study, Journal of Comparative Effectiveness Research, 10.2217/cer-2022-0149, 11, 18, (1323-1336), (2022).