Safety and effectiveness of intranasal esketamine for treatment-resistant depression: a real-world retrospective study
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: There is limited real-world evidence for patients with treatment-resistant depression (TRD) receiving esketamine nasal spray. Methods: This retrospective cohort study used data collected from a psychiatric clinic's EHR system. Results: A total of 171 TRD patients received esketamine July 2019–June 2021. This predominantly female, white population had several mental health comorbidities and high exposure to psychiatric medications. We observed significant reductions (p < 0.001) in average PHQ-9 and GAD-7 scores from baseline (PHQ-9: mean: 16.7; SD: 5.8; GAD-7: mean: 12.0; SD: 5.8) to last available treatment (PHQ-9: mean: 12.0; SD: 6.4; GAD-7: mean: 8.7; SD: 5.6). There were no reports of serious adverse events. Conclusion: This study found a significant disease burden for patients with TRD. Esketamine appears to be well tolerated and effective in improving depression and anxiety.
Background: treatment-resistant depression
Major depressive disorder (MDD) is one of the most common mental health disorders in the US and is a major cause of disability [1]. In 2017, an estimated 17.3 million adults in the US had at least one major depressive episode, representing over 7% of all US adults [2]. Treatment-resistant depression (TRD) is broadly defined as failure to achieve response or remission to at least two antidepressant medications with adequate dosing and duration [1,3]. TRD patients account for approximately one third of MDD patients and this population disproportionally accounts for the burden of disease caused by depression [1,3–5].
Current pharmacotherapy strategies for TRD include switching antidepressants, combining antidepressants, using second-generation antipsychotics and augmentation with lithium [2,6]. However, most antidepressants take several weeks for patients to note symptom improvement, which is when TRD patients may be at imminent risk of suicidal ideation or suicide attempt [7–9]. Non-pharmacological treatments for TRD include somatic therapies such as transcranial magnetic stimulation (TMS), electroconvulsive therapy (ECT), vagal nerve stimulation (VNS) and deep brain stimulation (DBS) [10]. The clinical efficacy of ECT is well established, but this treatment is costly and is associated with acute cognitive impairment and amnesia. TMS is not fully supported by clinical trials for TRD, with small sample sizes, variable treatment schedules and high drop-out rates [10]. TMS is also time consuming, as TMS sessions, usually 30–60 min each, are given five-times a week for a period of 4 to 5 weeks for a total of 20 to 30 sessions [10]. Furthermore, TMS is costly and insurance companies are reluctant to reimburse for this treatment [10]. In 2005, VNS was approved by the FDA as an adjunctive treatment for TRD in patients who had failed four or more antidepressant medications [11,12]. However, there are perioperative risks involved with device implantation and response is not seen until 3 to 12 months after implantation, thus VNS is not recommended for acute treatment of TRD [12,13]. Furthermore, there is a lack of reimbursement by US insurance providers for VNS, namely Medicare/Medicaid [10]. DBS is an experimental surgical treatment for TRD with high cost and substantial risk associated with the surgical procedure [10]. Moreover, the effects of the stimulation can take weeks to months to begin working [10]. Thus, there is a significant unmet need for rapid acting treatment for patients with TRD.
Ketamine & esketamine for the treatment of depression
Ketamine was approved by the US FDA in 1970 as an anesthetic, but also has been observed to improve symptoms of depression and other mood disorders [9,14]. Hypothesized mechanism of actions of ketamine for depression include direct synaptic or extra-synaptic N-methyl-D-aspartate receptor (NMDAR) inhibition, selective inhibition of NMDARs localized on GABAergic interneurons and α-amino-3-hydroxy-5-methyl-4-isoxazole-propionic acid receptor (AMPAR) activation [15]. Downstream mechanisms regulating synaptic plasticity have also been hypothesized to affect the antidepressant response to ketamine, which include an increase in brain-derived neurotrophic factor (BDNF) protein levels, a decrease in eukaryotic elongation factor 2 kinase (eEF2k) activation, activation of mechanistic target of rapamycin (mTOR) and inhibition of glycogen synthase kinase-3 (GSK-3) [15,16]. These hypothesized mechanisms of action of ketamine are not mutually exclusive and may act harmoniously to produce an antidepressant response [15].
Ketamine is a racemic mixture of two stereoisomers, the S- and R-enantiomer [14,17]. Compared with the R-enantiomer, the S-enantiomer binds to the NMDA receptor with greater affinity and has stronger anesthetic and analgesic action, producing less lethargy and cognitive impairment [17]. Racemic ketamine can be administered via intravenous (IV), intranasal (IN), oral, sublingual (SL), anal, subcutaneous (SQ) and IM routes; however, the majority of research to date has been on IV administration with dose ranges of 0.5–0.75 mg/kg [18–20]. A meta-analysis of IV ketamine infusion for TRD found that patients experienced rapid reduction in depressive symptoms during the first 24 h after one infusion, and the effects decreased at 7 days post-infusion, showing how ketamine is promising for short-term treatment of TRD [19]. Sustained benefit from ketamine typically requires multiple infusions at a high-frequency during an induction period, typically six sessions over 2–3 weeks, followed by lower-frequency treatment during maintenance treatment [18,21]. While racemic ketamine is only prescribed for psychiatric disorders as an off-label indication, the S-enantiomer, esketamine (Spravato™), was approved by the FDA in March of 2019 as a rapid-acting treatment for TRD [9,17]. With its novel mechanism of action and rapid reduction of depressive symptoms as early as 24 h post-administration, esketamine has garnered interest for the treatment of TRD [1,9,17,22].
The FDA's approval of esketamine was based on the efficacy and safety results of four phase III clinical trials [23,24]. Three trials were short-term parallel-group designs (TRANSFORM-1 and TRANSFORM-2 with patients ages 18 to 64 years; TRANSFORM-3 with patients ages 65+ years) and one trial was a longer-term randomized withdrawal maintenance-of-effect design (SUSTAIN-1) [23]. The Montgomery-Åsberg Depression Rating Scale (MADRS) was used as the primary outcome measure to assess change in depressive symptoms in all trials. Patients enrolled were diagnosed with MDD and had failed two or more prior treatment lines. To assess esketamine efficacy, patients were randomly assigned to receive esketamine nasal spray (56 or 84 mg for TRANFORM-1 and TRANSFORM-2; 28, 56, or 84 mg for TRANSFORM-3) versus placebo. Additionally, all patients received a new oral antidepressant. Of the 421 patients randomly assigned to receive esketamine in the three short-term trials, 142 (34%) achieved remission and 199 (47%) responded. Of the 289 patients randomly assigned to receive placebo in the three short-term trials, 68 (24%) achieved remission and 102 (35%) responded. In the long-term SUSTAIN-1 trial, patients who had initially achieved remission or response while receiving esketamine in the short-term trials were randomly assigned to continue esketamine or replace with a placebo [23]. Two of the studies (TRANSFORM-2 and SUSTAIN-1) showed a statistically superior effect of esketamine versus placebo on the study's primary efficacy end point (i.e., MADRS total score change from baseline at day 28) [23]. In TRANSFORM-2, the treatment effect was apparent at day 2, which is an unusually rapid onset of effect for antidepressant medication [23]. In SUSTAIN-1, time to depressive relapse was significantly longer in patients who continued esketamine treatment than patients who switched to placebo, demonstrating evidence that esketamine is effective beyond one month for patients who initially responded [9,23]. Additionally, based on the safety data of these trials, the FDA approved esketamine with a Risk Evaluation and Mitigation Strategies (REMS) program to mitigate the risk associated with serious adverse outcomes and the potential for abuse and misuse [9,25,26]. The REMS program specifies that esketamine only be dispensed and administered to patients under direct observation of a healthcare provider where they can be monitored for at least 2 h post-administration [26].
Having a new treatment for TRD is important given the substantial burden of the disease coupled with the unmet clinical need. However, the efficacy, safety, patient profile and use of esketamine in the real world may differ from that reported in the clinical trial data for esketamine. For instance, patients treated in real-world settings may have more severe depressive symptoms, a less rigorous or regular treatment schedule than observed dose-frequency data in the RCTs, or other co-occurring psychiatric conditions that were excluded from the RCTs; therefore, the efficacy and safety of treating these populations with esketamine is unknown [17].
The current study
Given the limited real-world and long-term data for patients with TRD receiving esketamine treatment, the aim of our study is to better understand the demographic and clinical characteristics, treatment patterns, clinical outcomes and adverse events of patients with TRD receiving esketamine therapy in a private outpatient psychiatric clinic setting.
Methods
This retrospective analysis was conducted in accordance with International Society for Pharmacoepidemiology (ISPE) Guidelines for Good Pharmacoepidemiology Practices (GPP) and received approval from the University of Utah human subject protection review board.
We evaluated patients receiving esketamine treatment at a private integrative psychiatric clinic that provides outpatient mental health treatment, specializing in ketamine and esketamine treatment. The services provided include diagnostic evaluations, medication management, psychotherapy, TMS, and esketamine and ketamine treatment. This clinic is a certified esketamine treatment center and has been administering esketamine since 2019 when the FDA approved the medication for treatment of TRD.
Study design & population
This retrospective observational cohort study was conducted using data from an electronic health record (EHR) system that contains clinical and administrative data. All adults 18 years or older with a diagnosis of major depressive disorder, recurrent without psychotic features (ICD-10 code F33.2) and who received esketamine nasal spray from July 2019 to June 2021 were included. Individuals who received other forms of ketamine, including intravenous, oral, sublingual, or intramuscular, were excluded.
Data collection
Data were collected through customized reports from the EHR and by medical chart review. Variables extracted electronically included demographics, history questionnaires (physical and mental medical history, social history and family history of mental illness), diagnoses, concomitant medications, treatment dates and clinical outcomes. History questionnaires were provided to patients to complete before their first visit; however, not all patients completed these questionnaires. Some variables were not available as structured data, so reviews of medical charts were conducted to extract information pertinent to this study. These data include data elements required by the REMS program (i.e., adverse events, blood pressure, time following administration for monitoring) and vital signs consisting of blood pressure, pulse, respiration rate and temperature.
Outcomes
The primary outcomes of interest were the Patient Health Questionnaire (PHQ-9) depression score, the Generalized Anxiety Disorder (GAD-7) score and the suicidal ideation (SI) score (PHQ-9 item 9). The PHQ-9 and GAD-7 are valid and reliable tools to screen for depression and generalized anxiety disorder in clinical practice and research [27,28]. The PHQ-9 scores for each of the 9 DSM-5 criteria for depression as ‘0’ (not at all) to ‘3’ (nearly every day) over the last 2 weeks [27]. The PHQ-9 total score ranges from 0 to 27 and scores represent minimal depression (0–4), mild depression (5–9), moderate depression (10–14), moderately severe depression (15–19), and severe depression (20–27). Previous research has defined a clinically meaningful improvement in PHQ-9 score as a 3-point reduction, while a clinically substantial improvement has been defined as a 6-point reduction [29]. The GAD-7 scores the 7 criteria for anxiety based on the DSM-5 criteria as ‘0’ (not at all) to ‘3’ (nearly every day) over the last 2 weeks [28]. The GAD-7 total score ranges from 0 to 21 and scores represent mild anxiety (0–5), moderate anxiety (6–10), moderately severe anxiety (11–15), and severe anxiety (15–21) [28].
Statistical analyses
Descriptive statistics were used to describe the study sample characteristics, treatment patterns, clinical outcomes and adverse events. To compare outcome measures from baseline to the last dosing session, the cohort was stratified by number of treatments received and two-sample paired t-tests were conducted. Correlation analyses were performed to determine the association between the number of treatment sessions and outcome measures.
Multiple linear regression analyses were performed to determine the relationship between number of treatments and change in depression and anxiety measures from baseline to the last treatment session available. Covariates with missing data were not included in the multivariable analysis. We utilized forward selection with an entry significance level at 0.15 to determine the final models for predicting change in PHQ-9 score and change in GAD-7 score. The models were each evaluated for outliers with standardized residuals and influential values were assessed with Cook's distance. Collinearity was assessed using the variance inflation factor (VIF) and the condition index (CI). Residual plots were used to assess linearity and heteroskedasticity assumptions. Normality was assessed graphically with a histogram and Q-Q plot of the residuals. The R2 value was assessed to evaluate how much variability in the change in PHQ-9 score or change in GAD-7 score is accounted for by the regression models. Analyses were performed using STATA 16.1. Levels of significance in this study were defined as p < 0.05.
Results
A total of 171 patients were treated with esketamine therapy from July 2019–June 2021 and met all inclusion/exclusion criteria. The patient population had an average age of 36 (±12) years, included a higher proportion of females (60%) and were predominantly white (92%) (Table 1).
| Demographic characteristics | Total (n = 171) | |
|---|---|---|
| Mean or n | SD or (%) | |
| Age (years) | 36 | 12 |
| Sex, female | 103 | 60% |
| Race | ||
| White | 157 | 92% |
| Black or African–American | 2 | 1.2% |
| Asian | 1 | 0.58% |
| American–Indian | 1 | 0.58% |
| Other race | 4 | 2% |
| Patient declined | 6 | 4% |
| Utah residence | 168 | 98% |
| Psychiatric diagnoses | ||
|---|---|---|
| Major depressive disorder (MDD) | 171 | 100% |
| Generalized anxiety disorder (GAD) | 67 | 39% |
| Attention-deficit hyperactivity disorder (ADHD) | 43 | 25% |
| Insomnia | 43 | 25% |
| Other mental disorder† | 33 | 19% |
| Post-traumatic stress disorder (PTSD) | 20 | 12% |
| Panic disorder (PD) | 12 | 7% |
| Bipolar disorder (BD) | 11 | 6% |
| Psychiatric medications | ||
|---|---|---|
| All psychiatric medications | 168 | 98% |
| Prescriptions per patient | 5.8 | 4.0 |
| Antidepressant | 160 | 94% |
| Prescriptions per patient | 2.3 | 1.4 |
| Tricyclic antidepressant | 10 | 6% |
| Antipsychotic | 79 | 46% |
| Stimulant | 71 | 42% |
| Benzodiazepine | 74 | 43% |
| Anticonvulsant | 59 | 35% |
| Sedative/hypnotic | 40 | 23% |
| Anticonvulsant/mood stabilizer | 39 | 23% |
| Mood stabilizer | 12 | 7% |
| Opiate antagonist | 11 | 6% |
| Other‡ | 19 | 11% |
†
Other mental disorder includes the following: Anxiety disorder, unspecified (n = 9); Sleep disorder, unspecified (n = 6); Obsessive-compulsive disorder (n = 4); Eating disorder (n = 4); Suicidal ideations (n = 3); Unspecified mood disorder (n = 2); Alcohol use disorder (n = 1); Attention and concentration deficit (n = 1); Opioid use disorder (n = 1); Personality disorder (n = 1); Social phobia (n = 1).
‡
Other psychiatric medications include the following: Dopamine agonist (n = 7); Triptan (n = 4); Alcohol antagonist (n = 3); CNS depressant (n = 2); MAOI (n = 2); NMDA receptor antagonist (n = 2); Sedative (n = 2); Marijuana (n = 1).
Several common psychiatric diagnoses were generalized anxiety disorder (GAD) (39%; n = 67), attention-deficit hyperactivity disorder (ADHD) (25%; n = 43), insomnia (25%; n = 43) and post-traumatic stress disorder (PTSD) (12%; n = 20) (Table 1). There were 168 (98%) patients with recorded use of other psychiatric medications besides esketamine, with an average of 5.8 (SD: 4.0) psychiatric medications per patient. There were 160 (94%) patients with a recorded prescription for an oral antidepressant and each of these patients were taking on average 2.3 (SD: 1.4) oral antidepressants (Table 1). For all other psychiatric medication classes listed, patients were taking one to two medications each.
The patient self-reported medical, social and family history questionnaires are summarized in Tables 2 & 3. The number for each question changes based on whether the patient completed the questionnaire and/or the individual question. The number of respondents is shown for each question and percentages are based on available data. The majority of patients reported a history of acute or chronic pain (55% [38/69]) and high blood pressure (32% [17/53]). Regarding mental health history, 45% of respondents reported one or more prior psychiatric hospitalizations (35/78), 48% of respondents reported self-harm behavior (31/64) and 46% of respondents reported one or more prior suicide attempts (28/61). Most patients with available data did not have a history of heavy alcohol use (5% [5/107]), daily tobacco use (6% [9/146]), recreational cocaine/amphetamine use (18% [24/134]), or psychedelic/entheogenic drug use (19% [25/134]). Several patients had a history of opiate use (including prescription opiates and/or heroin) but denied current use (78% [105/137]). Of the 135 respondents with data on family history of mental illness, 70% (n = 120) reported a family history of mental illness. The majority of patients reported having one or more family members with a history of depressive disorder (71% [96/135]) or anxiety disorder (57% [77/135]).
| Medical history – physical | Patients with available data (n) | n (%) |
|---|---|---|
| Acute or chronic pain | 69 | 38 (55.1%) |
| High blood pressure | 53 | 17 (32.0%) |
| Thyroid disease | 52 | 15 (28.9%) |
| Cancer | 45 | 7 (15.6%) |
| Traumatic brain injury | 47 | 6 (12.8%) |
| Cardiovascular issues | 45 | 5 (11.1%) |
| Stroke TIA | 41 | 3 (7.3%) |
| Diabetes | 43 | 3 (7.0%) |
| Seizures/epilepsy | 45 | 3 (6.7%) |
| Medical history – mental | ||
|---|---|---|
| Any prior psychiatric hospitalizations | 78 | 35 (44.9%) |
| Any self-harm behavior | 64 | 31 (48.4%) |
| Prior suicide attempts | 61 | 28 (45.9%) |
| Prior ketamine use | 48 | 8 (16.7%) |
| Social history | ||
|---|---|---|
| Alcohol use | 107 | |
| Denies history of use | 53 (49.5%) | |
| Heavy | 5 (4.7%) | |
| Moderate | 14 (13.1%) | |
| Occasional (2–3-times monthly or less) | 35 (32.7%) | |
| Blackouts/delirium tremens/seizures related to alcohol | 135 | |
| No | 123 (91.1%) | |
| Yes | 12 (8.9%) | |
| Ever attended any alcohol or drug treatment centers | 138 | |
| No | 128 (92.8%) | |
| Yes | 10 (7.3%) | |
| Do you or have you ever smoked tobacco | 146 | |
| Never | 101 (69.2%) | |
| Formerly | 26 (17.8%) | |
| Currently some days | 9 (6.2%) | |
| Currently every day | 9 (6.2%) | |
| Current status unknown | 1 (0.7%) | |
| Cannabis use | 134 | |
| Denies history of use | 63 (47.0%) | |
| Previous use – denies current use | 37 (27.6%) | |
| Recreational use | 24 (17.9%) | |
| Currently prescribed medicinal cannabis | 10 (7.5%) | |
| Cocaine/amphetamines use | 139 | |
| Denies history of use | 126 (90.7%) | |
| Previous use – denies current use | 9 (6.5%) | |
| Currently uses | 4 (2.9%) | |
| Opiate (pain pills/heroin) use | 137 | |
| Denies history of use | 9 (6.6%) | |
| Previous use – denies current use | 105 (76.6%) | |
| Currently uses | 23 (16.8%) | |
| Psychedelic/entheogenic drug use (e.g. LSD, DMT, Psilocybin, MDMA) | 134 | |
| Denies history of use | 109 (81.3%) | |
| Admits history of use | 25 (18.7%) | |
| Family history of mental illness (n = 171) | n | % |
|---|---|---|
| Yes | 120 | 70.2 |
| No current problems or disability | 2 | 1.2 |
| Unknown | 13 | 7.6 |
| No data | 36 | 21.1 |
| Mental illness/substance use condition of patient family members (n = 135) | n† | % |
|---|---|---|
| Depressive disorder | 96 | 71 |
| Anxiety disorder | 77 | 57 |
| Alcohol abuse | 53 | 39 |
| Attention deficit hyperactivity disorder | 44 | 33 |
| Substance abuse | 34 | 25 |
| Panic disorder | 25 | 19 |
| History of attempted suicide | 28 | 21 |
| Posttraumatic stress disorder | 23 | 17 |
| Bipolar disorder | 24 | 18 |
| Obsessive-compulsive disorder | 18 | 13 |
| Personality disorder | 14 | 10 |
| Schizophrenia | 3 | 2 |
| Schizoaffective disorder | 2 | 1 |
| Alcohol dependence | 1 | 1 |
| Cocaine abuse | 1 | 1 |
†
N represents count of patients with 1+ family members with the specified mental health/substance use condition history.
Depression & anxiety outcome measurements – PHQ-9 & GAD-7 survey scores
Figure 1 presents the mean PHQ-9 (depression) and GAD-7 (anxiety) scores for treatment sessions 1–28. For treatment sessions 1–8, the average PHQ-9 and GAD-7 scores steadily decrease, reflecting improvements in depression severity. The average survey scores increase at treatment session 9, decrease from treatment sessions 9–12 and increase at treatment session 14. After treatment session 14, the survey score trends become variable but do not increase to scores above those seen at treatment session 14 – PHQ-9 mean: 12.8 (SD: 5.7), GAD-7 mean: 9.6 (SD: 5.7).
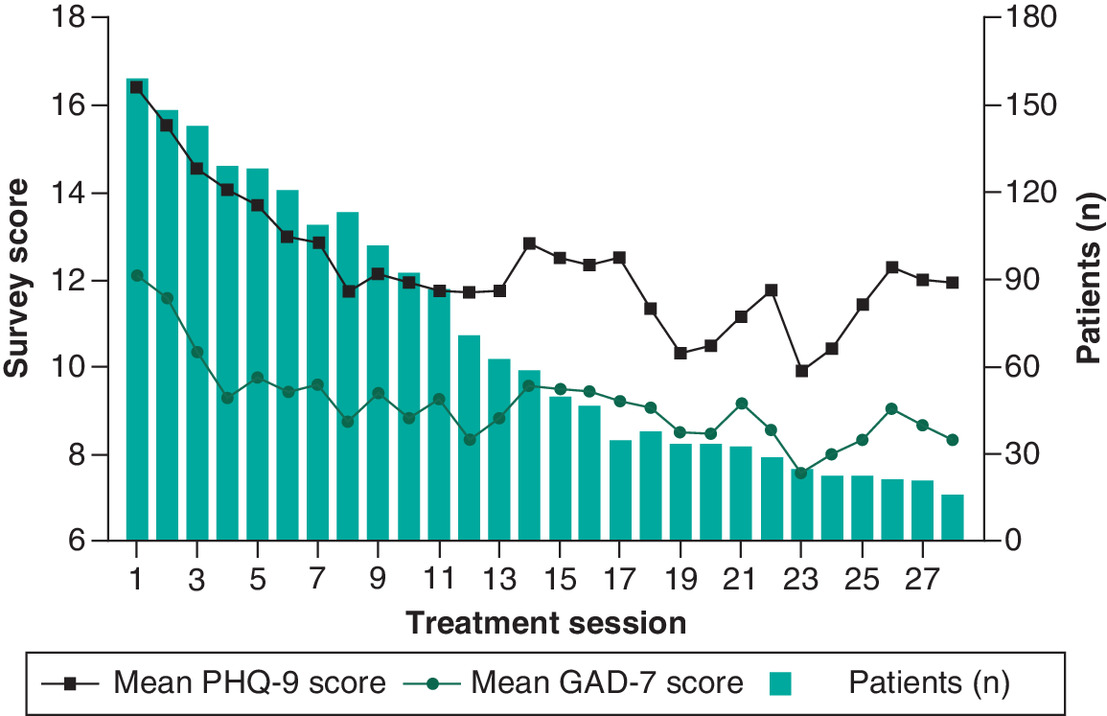
Figure 1. Outcome measures for patients receiving esketamine therapy, treatment sessions 1–28.
PHQ-9 survey instrument scores may range from 0–27; GAD-7 survey instrument scores may range from 0–21. Higher scores indicate more severe depression or anxiety symptoms.
Figure 2 displays the mean SI score for treatment sessions 1–28. Similar to the PHQ-9 total score, the average SI score steadily decreased from treatment sessions 1–9, increased at treatment session 10, decreased sharply at session 11 and was variable thereafter. After treatment session 13, the average SI score for the cohort becomes variable but does not increase to scores above those seen at session 13 (SI mean: 0.81; SD: 0.95).
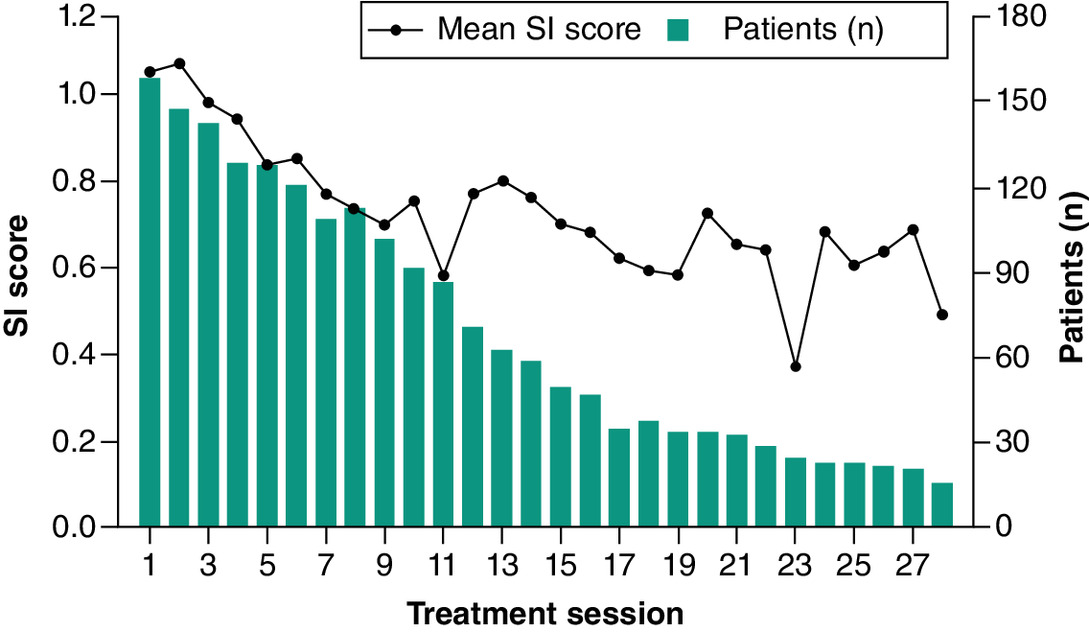
Figure 2. SI scores for patients receiving esketamine therapy, treatment sessions 1–28.
SI scores (PHQ-9 item 9) range from 0 to 3. Higher score indicates more severe suicidal ideation.
The cohort of patients had a median of 11 treatments (IQR 10.5). The median days between treatments ranges from 3–6 days for treatment sessions 1–9, increases to 7 days at treatment session 10 and remains at a median of 7 days for treatment sessions 10–28.
Table 4 provides the summary of PHQ-9 and GAD-7 scores taken at baseline versus the patients' last available esketamine treatment. The summaries are stratified by number of treatments the patients received. There were 148 patients of the 171 patients that had a baseline PHQ-9 score and a PHQ-9 score at a follow-up esketamine treatment greater than 2 weeks after the first treatment. These patients had an average baseline PHQ-9 score of 16.7 (SD: 5.8) and an average last treatment PHQ-9 score of 12 (SD: 6.4) and these scores were significantly different (p < 0.001). For the subgroup analysis of PHQ-9 scores stratified by number of treatments, baseline scores were significantly higher than last available treatment scores for all comparisons except for patients that received 2–5 treatments. We observed that the baseline PHQ-9 score is higher for patients that had more treatments.
| Depression – PHQ-9 | n | Score at baseline | Last available treatment | p-value† |
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | |||
| All patients with baseline and >2 survey scores and/or >2 weeks of treatment | 148 | 16.7 (5.82) | 12 (6.38) | <0.001 |
| Patients with 1 treatment | 7 | 13 (6.72) | N/A | |
| Patients with 2–5 treatments | 31 | 15.8 (6.85) | 14.6 (6.67) | 0.202 |
| Patients with 6–10 treatments | 36 | 15.1 (5.77) | 11 (6.46) | <0.001 |
| Patients with 11–15 treatments | 39 | 16.7 (5.60) | 11.2 (6.42) | <0.001 |
| Patients with 16–30 treatments | 33 | 18.5 (5.00) | 11.6 (5.73) | <0.001 |
| Patients with 31–71 treatments | 13 | 17.5 (5.87) | 11.9 (5.50) | 0.001 |
| Suicidal ideation – PHQ-9 item 9 | ||||
|---|---|---|---|---|
| All patients with baseline and >2 survey scores and/or >2 weeks of treatment | 140 | 1.09 (1.06) | 0.79 (0.94) | <0.001 |
| Patients with 1 treatment | 5 | 0.80 (1.17) | N/A | |
| Patients with 2–5 treatments | 25 | 1.12 (1.11) | 1.04 (1.11) | 0.603 |
| Patients with 6–10 treatments | 30 | 0.97 (0.98) | 0.67 (0.83) | 0.071 |
| Patients with 11–15 treatments | 22 | 1.17 (1.09) | 0.77 (0.99) | 0.043 |
| Patients with 16–30 treatments | 27 | 0.96 (1.07) | 0.74 (0.84) | 0.227 |
| Patients with 31–71 treatments | 11 | 1.36 (1.07) | 0.64 (0.98) | 0.012 |
| Anxiety – GAD-7 | ||||
|---|---|---|---|---|
| All patients with baseline and >2 survey scores and/or >2 weeks of treatment | 120 | 12.0 (5.80) | 8.7 (5.62) | <0.001 |
| Patients with 1 treatment | 7 | 11.3 (6.97) | N/A | |
| Patients with 2–5 treatments | 28 | 11.6 (6.29) | 10.1 (6.14) | 0.023 |
| Patients with 6–10 treatments | 29 | 11.3 (5.93) | 8.38 (5.20) | 0.004 |
| Patients with 11–15 treatments | 34 | 12.0 (6.01) | 8.5 (6.04) | 0.001 |
| Patients with 16–30 treatments | 31 | 13.80 (5.15) | 9.58 (5.81) | <0.001 |
| Patients with 31–71 treatments | 9 | 10.67 (5.81) | 7.11 (3.48) | 0.049 |
†
2-sample paired t-tests were conducted.
There were 140 patients with an SI score that also had a baseline PHQ-9 score sheet in their records and a PHQ-9 at a follow-up esketamine treatment greater than 2 weeks after the first treatment. These patients had an average baseline SI score of 1.09 (SD: 1.06) and an average last treatment SI score of 0.79 (SD: 0.94) and these scores were significantly different (p < 0.001). For the subgroup analysis of SI scores stratified by number of treatments, baseline scores were significantly higher than last treatment scores for patients with 6–10, 11–15 and 31–71 treatments.
There were 120 patients that had a baseline GAD-7 score and a GAD-7 score at a follow-up esketamine treatment greater than 2 weeks after the first treatment. These patients had an average baseline GAD-7 score of 12.0 (SD: 5.8) and an average last treatment GAD-7 score of 8.7 (5.6), a reduction that was significant (p < 0.001). For the subgroup analysis of GAD-7 scores, there was a significant reduction in GAD-7 values from baseline to last treatment for all subgroups of number of esketamine treatments received.
The change in PHQ-9 scores from baseline to last available treatment was negatively correlated with number of treatments patients received, so additional treatments was correlated with a decrease in depressive symptoms (Spearman's rho = -0.2645; p = 0.001). The change in GAD-7 scores from baseline to last available treatment was also negatively correlated with number of treatments received, thus additional treatments is correlated with a decrease in anxiety severity (Spearman's rho = -0.1871; p = 0.04).
Results from the multiple linear regression analyses are summarized in Table 5. The predictors in the final model predicting change in PHQ-9 score were as follows: patient age, patient sex, baseline PHQ-9 score, diagnosis of generalized anxiety disorder (GAD), diagnosis of insomnia and treatment duration. Four variables were statistically significant in the multivariate model predicting change in PHQ-9 score from baseline to last available treatment. Increase in age (p = 0.021), increase in baseline PHQ-9 score (p < 0.001) and increase in treatment duration (p = 0.034) were associated with a decrease in PHQ-9 score from baseline to last available treatment. In contrast, being female (p = 0.021) was associated with an increase in PHQ-9 score from baseline to last treatment date. The average change in PHQ-9 score within this cohort (n = 137) included significant variability (mean: -4.7; SD: 6.2) and the R2 value was 29%. The predictors in the final model predicting change in GAD-7 score were as follows: patient sex, baseline GAD-7 score, diagnosis of GAD and treatment duration. Two variables were statistically significant in the multivariate model predicting change in GAD-7 score from baseline to last available treatment. An increase in baseline GAD-7 (p < 0.001) was associated with a decrease in GAD-7 score whereas a diagnosis of GAD (p = 0.026) was associated with an increase in GAD-7 score from baseline to last treatment date available. Similar to the model predicting change in PHQ-9 score, the model predicting change in GAD-7 score in this cohort (n = 120) included significant variability (mean: -3.32; SD: 4.68) and the R2 value was 27%.
| Variable | Coefficient (β) | 95% CI | p-value | |
|---|---|---|---|---|
| Predicting change in PHQ-9 score (n = 137) | ||||
| Constant | 4.74 | (0.721, 0.876) | 0.021 | |
| Demographic characteristics | ||||
| Age (year) | -0.0988 | (-0.169, -0.0285) | 0.006 | |
| Female sex | 2.19 | (0.339, 4.03) | 0.021 | |
| Clinical characteristics | ||||
| Baseline PHQ-9 score | -0.451 | (-0.609, -0.293) | <0.001 | |
| Diagnosis of generalized anxiety disorder | 1.59 | (-0.306, 3.48) | 0.100 | |
| Diagnosis of insomnia | 1.10 | (-0.385, 0.398) | 0.106 | |
| Treatment patterns | ||||
| Treatment duration (days) | -0.00890 | (-0.0171, -0.000671) | 0.034 |
| Predicting change in GAD-7 score (n = 120) | ||||
|---|---|---|---|---|
| Constant | 0.246 | (-1.82, 2.31) | 0.814 | |
| Demographic characteristics | ||||
| Female sex | 1.34 | (-0.240, 2.928) | 0.096 | |
| Clinical characteristics | ||||
| Baseline GAD-7 score | -0.376 | (-0.507, -0.244) | <0.001 | |
| Diagnosis of Generalized Anxiety Disorder | 1.80 | (0.224, 3.38) | 0.026 | |
| Treatment patterns | ||||
| Treatment duration (days) | -0.00733 | (-0.0156, 0.000911) | 0.081 |
Safety
Table 6 summarizes REMS information, stratified by dose of esketamine administered (56 or 84 mg). Adverse events of esketamine include transient increases in blood pressure and possible dissociation and sedation lasting 1–2 h [30]. On average, sedation was experienced less frequently than dissociation during treatments for the entire cohort, 8% (SD: 22%) of treatments versus 48% (SD: 41%) of treatments, respectively. Of the patients who experienced sedation (22%; n = 38), 74% experienced sedation onset within the first 30 min or the first hour (63% of treatments) after esketamine administration and most had symptoms resolve within 2 h (97%). Of the patients who experienced dissociation (73%; n = 125), the majority experienced dissociation onset within the first 30 min (94% of treatments), but most patients had dissociation symptoms resolve within 2 h (99%). There was one reported serious adverse event where the patient experienced prolonged dissociation/sedation with nausea/vomiting 2 h post-administration of esketamine 84 mg; however, this AE had unknown cause or risk and the patient had previously tolerated the 84 mg dose well. The case was fully resolved the same day before the patient left the clinic, with no ongoing related symptoms thereafter. Blood pressure decreased throughout each session from baseline (mean systolic (mmHg) 124; SD: 14; mean diastolic (mmHg) 83; SD: 9) to 40 min after esketamine administration (mean systolic (mmHg) 122; SD: 14; mean diastolic (mmHg) 81; SD: 9) and prior to session completion (mean systolic (mmHg) 119; SD: 15; mean diastolic (mmHg) 80; SD: 10). Patients were reported as ready to leave by approximately 90 min post administration of esketamine for both the 56 mg and 84 mg dosages.
| Total (n = 171) | Esketamine 56 mg (n = 146) | Esketamine 84 mg (n = 154) | |
|---|---|---|---|
| Treatment summary | Mean (SD) | Mean (SD) | Mean (SD) |
| Treatments per patient | 13.6 (11.2) | 2.28 (2.01) | 12.9 (11.0) |
| Percentage of treatments each patient experienced sedation | 8.2% (21.5%) | 14.9% (33%) | 6.6% (19.5%) |
| Percentage of treatments each patient experienced dissociation | 47.7% (41.4%) | 44.7% (45.4%) | 47.9% (41.9%) |
| Sedation | n (%) | n (%) | n (%) |
|---|---|---|---|
| Patient experienced sedation (n = 171) | 38 (22%) | 28 (19%) | 29 (19%) |
| Symptoms resolved within 2 h (n = 38) | 37 (97%) | 25 (89%) | 28 (97%) |
| Dissociation | n (%) | n (%) | n (%) |
|---|---|---|---|
| Patient experienced dissociation (n = 171) | 125 (73%) | 79 (54%) | 110 (64%) |
| Symptoms resolved within 2 h (n = 125) | 124 (99%) | 77 (97%) | 109 (99%) |
| Serious AE† | n (%) | n (%) | n (%) |
|---|---|---|---|
| Patient experienced prolonged dissociation/sedation with nausea and vomiting (n = 171) | 1 (1%) | 0 | 1 (1%) |
| Event resolved (n = 1) | 1 (100%) | N/A | 1 (100%) |
| Blood Pressure | Mean (SD) | Mean (SD) | Mean (SD) |
|---|---|---|---|
| Prior to administration | |||
| Systolic (mm Hg) | 124 (14) | 124 (14) | 124 (14) |
| Diastolic (mm Hg) | 83 (9) | 82 (10) | 83 (9) |
| 40 min after administration | |||
| Systolic (mm Hg) | 122 (14) | 123 (14) | 122 (14) |
| Diastolic (mm Hg) | 81 (9) | 81 (10) | 81 (9) |
| Prior to session completion | |||
| Systolic (mm Hg) | 119 (15) | 120 (15) | 119 (15) |
| Diastolic (mm Hg) | 80 (10) | 79 (10) | 80 (10) |
| Min patient was ready to leave | Mean (SD) | Mean (SD) | Mean (SD) |
|---|---|---|---|
| min | 90 (15) | 90 (16) | 90 (15) |
†
Spravato given at 1:33 pm, nausea/vomiting at 3:30 pm, prolonged sedation/dissociation until 4:30–5 pm; Unknown cause/risk, previously tolerated 84 mg dosing well.
SD: Standard deviation.
Discussion
Using data from a real-world setting, this study demonstrates esketamine therapy was efficacious in relieving depressive and anxious symptoms without major safety concerns. We observed clinically meaningful improvements in depressive symptoms in this population. In this study, patients receiving between 6–10 treatments had an average reduction of 4.1 points in PHQ-9 score from baseline to last treatment session. For patients with 11–15, 16–30 and 31–71 treatments, reduction in PHQ-9 score ranged from 5.5 to 6.9 points from baseline to last treatment session. These clinically meaningful improvements in PHQ-9 scores suggest a reduction in the risk of relapse and recurrence of depressive symptoms [29,31]. Furthermore, the change in PHQ-9 scores observed in this population are larger than what was observed in the esketamine short-term RCTs, which ranged from -2.2 to -2.8 per study [23]. Thus, the results of this study support esketamine's consistent benefit and clinically meaningful efficacy in real-world practice [23,32].
In terms of potential relapse risk, decreasing dose frequency to once weekly does not seem to be problematic because average depression, anxiety and SI scores did not increase to levels above those measured at session 14. This finding aligns with data from the long-term SUSTAIN-1 trial [23]. The results of SUSTAIN-1 showed that continuation of esketamine significantly reduced the risk of relapse by 51% for patients who achieved stable remission and 70% for patients who achieved stable response compared with patients that switched to a placebo [23]. However, these relapse prevention results should be considered in the context of relapse rates for oral antidepressants, because these results do not indicate that patients who respond to esketamine had lower relapse risk than patients who respond to oral antidepressants. The Sequenced Treatment Alternatives to Relieve Depression (STAR*D) trial was a randomized trial where outpatients with MDD were followed across 4 treatment steps [4]. The STAR*D trial reported relapse rates of 65% for patients at treatment step 3 and 71% for step 4 [4]. These relapse rates were much higher than rates in the esketamine continuation group in the SUSTAIN-1 trial – 27% of remitters relapsed and 26% of responders relapsed [4,23]. Thus, our study and the SUSTAIN-1 trial provide important evidence that esketamine is effective beyond the first month of treatment for patients who initially experience improvement in depressive symptoms [9,23].
The population received esketamine treatment in accordance with the manufacturer's recommended dosing – twice per week for weeks 1–4 (i.e., the induction phase), weekly for weeks 5–8 (i.e., maintenance phase) and weekly or every other week for weeks 9+ [33]. At session 9 we observed a transient increase and variability thereafter in PHQ-9 and GAD-7 scores. This is the instance where the time between sessions began to increase substantially – a median of 4 days since the last treatment at session 8, a median of 6 days at session 9 and a median of 7 days thereafter. The increase in days between treatment is one possible explanation for the plateau in depression score improvement since esketamine is a rapid acting medication with transient effects. The rapid reduction of depression and anxiety symptoms is a key benefit of esketamine and continued administration may be necessary to relieve depressive symptoms. Additionally, it is important to note that clinical contact is frequent for esketamine therapy compared with oral antidepressant treatment because of the delivery model of esketamine, which likely aids in patients' improvement in depression/anxiety symptoms [34].
Population
We found that in this relatively young, predominantly female and white population with TRD, patients had several physical and mental health comorbidities. Our study had higher rates of chronic pain, GAD, ADHD and insomnia compared with previous analyses of TRD populations [5,35]. For example, an insurance claims analysis of 6,411 patients with TRD reported that 17.8% of patients were diagnosed with GAD, compared with 39% in this population [5]. This population also had higher rates of comorbidities compared with a TRD population in an insurance claims analysis conducted by Cepeda et al. [35]. However, a sub-group analysis of an esketamine-treated TRD group in the Cepeda et al. study had higher rates of comorbidities and exposure to psychiatric medications than the esketamine-treated TRD cohort in our analysis. This may be explained by the study's larger sample size (n = 418 esketamine-treated patients) or including a Medicaid patient database, as Medicaid patients have been shown to be older, sicker and more disabled than privately-insured patients [36,37]. Hence, this population was representative of a TRD population with a high disease burden of mental illness.
We observed a high exposure to psychiatric medications in this population (98%), with an average of 5.8 psychiatric prescriptions per patient and 2.3 antidepressant prescriptions per patient. This demonstrates that future studies evaluating medication management of patients receiving esketamine therapy is warranted. Prospective research tracking medication management could help determine if TRD patients may benefit from changing or reducing their psychiatric medications, particularly oral antidepressants, as their depressive symptoms improve with esketamine therapy. Oral antidepressants have unpleasant side effects and the potential for drug–drug interactions, leading to poor adherence [38].
Safety
For the patients included in these analyses, we did not observe documentation of significant tolerability issues with esketamine treatment. Only one patient (0.58%) experienced a serious AE of prolonged dissociation/sedation; however, the AE was reported to have been resolved during the clinic visit. Dissociation occurred during the majority of patient treatments. However, most patients (99%) had their dissociative symptoms resolve within two h, suggesting that the two-hour monitoring requirement of the REMS program is sufficient and ensures safe utilization of this medication. Most patients were ready to leave the clinic within 90 min post administration. This data can help determine the time commitment necessary for administering esketamine, a noted concern and barrier to access to the treatment [17].
Limitations
The results of this study must be interpreted in the context of its limitations. First, this is a descriptive, real-world observational cohort study. Thus, the findings from this study represent routine clinical practice and support other studies that have examined the use of these agents for TRD. Second, data in medical charts is subject to missing data and coding errors. Third, the outcome measures utilized have limitations that must be considered. We did not have data on outcome measurements (PHQ-9, GAD-7 and SI score) between treatments. Thus, our conclusions on the trends in outcome measurements should be interpreted in the context of not knowing fluctuations between esketamine treatment sessions. Additionally, the PHQ-9 and GAD-7 survey instruments asked respondent about the preceding two weeks to assess depression and anxiety symptom criteria. Thus, these tools are limited in measuring rapid reduction of depression and anxiety symptomatology as well as measuring changes in symptoms when treatment visits are frequent. Also, clinical trials of esketamine used the MADRS as the primary outcome for measuring severity of depression [23]. Thus, comparisons between clinical trial data and the results presented in this study need to consider the differences and limitations of these two instruments for measuring depression severity. Fourth, patients were encouraged to seek psychotherapy in addition to esketamine treatment. However, it was not feasible to report the number of patients receiving psychotherapy since some patients sought psychotherapy from other clinics, and patients that did receive psychotherapy from the same clinic they received esketamine treatment received varying number of visits and modalities of psychotherapy dependent upon their provider. Finally, because the study was conducted in an outpatient psychiatric clinic setting, the population studied may not be representative of TRD patients in other healthcare settings or other areas of the US.
Conclusion
Using novel data, this study demonstrates the significant disease burden of TRD and the effectiveness esketamine therapy has in relieving depressive and anxious symptoms without major safety concerns. Esketamine and ketamine are fundamentally changing how researchers and clinicians study and treat depression, and this study provides new evidence for esketamine use in clinical practice. Further research is warranted to continue studying the long-term and real-world benefits of esketamine therapy for TRD.
•
There is currently limited real-world and long-term data for patients with treatment-resistant depression (TRD) receiving esketamine treatment.
•
This retrospective cohort study utilized data collected from a private outpatient psychiatric clinic's electronic health record system.
•
A total of 171 patient with TRD received esketamine therapy from July 2019–June 2021.
•
We found that in this relatively young, predominantly female and white population with TRD, patients had several physical and mental health comorbidities.
•
We observed a high exposure to psychiatric medications in this population.
•
We observed significant reductions (p < 0.001) in average PHQ-9 and GAD-7 scores from baseline to last available treatment.
•
We did not observe documentation of significant tolerability issues with esketamine treatment.
•
Using novel real-world data, this study demonstrates the significant disease burden of TRD and the effectiveness esketamine therapy has in relieving depressive and anxious symptoms without major safety concerns.
Author contributions
All the authors have equal contribution towards conceptualizing and designing the study. M Brendle extracted and analyzed data and completed the manuscript writeup. S Ahuja and M Della Valle extracted and formatted data. P Thielking, R Robison and DC Malone reviewed the data analysis and critically reviewed/revised the manuscript writeup. All authors have read and approved the final article.
Financial & competing interests disclosure
R Robison and P Thielking are employed by Numinus and have stock ownership in Numinus. R Robison is on the Janssen Speakers Bureau for esketamine. Janssen Pharmaceuticals did not financially support this research. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
This paper is received approval from the University of Utah institutional review board on 14 July 2021 as non-human subject research (IRB 00145104). These data do not contain any information that could identify subjects. Informed consent was not required for this study.
Data sharing statement
The data that support the findings of this study are available on request from the corresponding author, M Brendle. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
References
1.
Hough D. Esketamine. Janssen Pharmaceutical Companies of Johnson and Johnson (2019).
2.
3.
Ionescu DF, Rosenbaum JF, Alpert JE. Pharmacological approaches to the challenge of treatment-resistant depression. Dialogues Clin. Neurosci. 17(2), 111–126 (2015).
4.
Rush AJ, Trivedi MH, Wisniewski SR et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am. J. Psychiatry 163(11), 1905–1917 (2006).
5.
Amos TB, Tandon N, Lefebvre P et al. Direct and indirect cost burden and change of employment status in treatment-resistant depression: a matched-cohort study using a US commercial claims database. J. Clin. Psychiatry 79(2), 17m1172 (2018).
6.
Luan S, Wan H, Wang S, Li H, Zhang B. Efficacy and safety of olanzapine/fluoxetine combination in the treatment of treatment-resistant depression: a meta-analysis of randomized controlled trials. Neuropsych. Dis. Treat. 13, 609–620 (2017).
7.
Hasin DS, Sarvet AL, Meyers JL et al. Epidemiology of adult DSM-5 major depressive disorder and its specifiers in the United States. JAMA Psychiatry 75(4), 336–346 (2018).
8.
Jakuszkowiak-Wojten K, Gałuszko-Węgielnik M, Wilkowska A et al. Suicidality in treatment resistant depression: perspective for ketamine use. Psychiatr. Danub. 31(Suppl. 3), 258–260 (2019).
9.
Kim J, Farchione T, Potter A, Chen Q, Temple R. Esketamine for treatment-resistant depression – first FDA-approved antidepressant in a new class. N. Engl. J. Med. 381(1), 1–4 (2019).
10.
Cusin C, Dougherty DD. Somatic therapies for treatment-resistant depression: ECT, TMS, VNS, DBS. Biol. Mood Anxiety Disord. 2, 14 (2012).
11.
Cusin C, Sakurai H, Bentley K et al. All suicidal ideation is not created equal: two cases of suicide attempts during maintenance ketamine treatment. Am. J. Psychiatry 177(2), 173–174 (2020).
12.
Carreno FR, Frazer A. Vagal nerve stimulation for treatment-resistant depression. Neurotherapeutics 14(3), 716–727 (2017).
13.
Yap JYY, Keatch C, Lambert E, Woods W, Stoddart PR, Kameneva T. Critical review of transcutaneous vagus nerve stimulation: challenges for translation to clinical practice. Front. Neurosci. 14, 284 (2020).
14.
Moghaddam B. Ketamine. MIT Press, USA (2021).
15.
Zanos P, Gould TD. Mechanisms of ketamine action as an antidepressant. Mol. Psych. 23(4), 801–811 (2018).
16.
Costi S, Soleimani L, Glasgow A et al. Lithium continuation therapy following ketamine in patients with treatment resistant unipolar depression: a randomized controlled trial. Neuropsychopharmacology 44(10), 1812–1819 (2019).
17.
Agboola F, Atlas SJ, Touchette DR, Fazioli K, Pearson SD. The effectiveness and value of esketamine for the management of treatment-resistant depression. J. Manag. Care Spec. Pharm. 26(1), 16–20 (2020).
18.
Sanacora G, Frye MA, Mcdonald W et al. A consensus statement on the use of ketamine in the treatment of mood disorders. JAMA Psychiatry 74(4), 399–405 (2017).
19.
Marcantoni WS, Akoumba BS, Wassef M et al. A systematic review and meta-analysis of the efficacy of intravenous ketamine infusion for treatment resistant depression: january 2009–January 2019. J. Affect. Disord. 277, 831–841 (2020).
20.
Andrade C. Ketamine for Depression, 4: in what dose, at what rate, by what route, for how long, and at what frequency? J. Clin. Psychiatry 78(7), e852–e857 (2017).
21.
Dore J, Turnipseed B, Dwyer S et al. Ketamine assisted psychotherapy (KAP): patient demographics, clinical data and outcomes in three large practices administering ketamine with psychotherapy. J. Psychoactive Drugs 51(2), 189–198 (2019).
22.
Moghadam B. Ketamine. MIT Press, USA (2021).
23.
FDA. Psychopharmacologic Drugs Advisory Committee (PDAC) and Drug Safety and Risk Management (DSaRM) Advisory Committee Meeting; agenda topic: the committees will discuss the efficacy, safety, and risk-benefit profile of new drug application (NDA) 211243, esketamine 28mg single-use nasal spray device, submitted by Janssen Pharmaceuticals, Inc., for the treatment of treatment-resistant depression (2019). www.fda.gov/media/121376/download
24.
Turner EH. Esketamine for treatment-resistant depression: seven concerns about efficacy and FDA approval. Lancet Psychiatry 6(12), 977–979 (2019).
25.
WHO. Fact file on ketamine (2016). https://sa1s3.patientpop.com/assets/docs/55947.pdf
26.
Janssen. SPRAVATO® REMS Program Overview (Risk Evaluation and Mitigation Strategy) (2019).
27.
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J. Gen. Intern. Med. 16(9), 606–613 (2001).
28.
Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch. Intern. Med. 166(10), 1092–1097 (2006).
29.
Turkoz I, Alphs L, Singh J et al. Clinically meaningful changes on depressive symptom measures and patient-reported outcomes in patients with treatment-resistant depression. Acta Psychiatr. Scand. 143(3), 253–263 (2021).
30.
Wilkinson ST, Howard DH, Busch SH. Psychiatric practice patterns and barriers to the adoption of esketamine. JAMA 322(11), 1039–1040 (2019).
31.
Mcmillan D, Gilbody S, Richards D. Defining successful treatment outcome in depression using the PHQ-9: a comparison of methods. J. Affect. Disord. 127(1), 122–129 (2010).
32.
Mathews M, Daly EJ, Popova V, Heerlein K, Canuso C, Drevets WC. Comment to Drs Gastaldon, Papola, Ostuzzi and Barbui. Epidemiol. Psychiatr. Sci. 29, e124 (2020).
33.
Janssen. Spravato (esketamine) nasal spray prescribing information (2019).
34.
Desai U, Kirson NY, Guglielmo A et al. Cost-per-remitter with esketamine nasal spray versus standard of care for treatment-resistant depression. J. Comp. Eff. Res. 10(5), 393–407 (2021).
35.
Cepeda MS, Kern DM, Canuso CM. At baseline patients treated with esketamine have higher burden of disease than other patients with treatment resistant depression: learnings from a population based study. Depress. Anxiety 38(5), 521–527 (2021).
36.
Foundation KF. Medicaid enrollees are sicker and more disabled than the privately-insured. Kaiser Family Foundation (2013).
37.
Ryan J, Abrams MK. Medicaid cuts would affect older, sicker Americans. The Commonwealth Fund (2017).
38.
Al-Harbi KS. Treatment-resistant depression: therapeutic trends, challenges, and future directions. Patient Prefer. Adher. 6, 369–388 (2012).
Information & Authors
Information
Published In
Pages: 1323 - 1336
PubMed: 36331048
Copyright
© 2022 Future Medicine Ltd.
History
Received: 15 August 2022
Accepted: 21 October 2022
Published online: 4 November 2022
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Safety and effectiveness of intranasal esketamine for treatment-resistant depression: a real-world retrospective study. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0149
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Allan H. Young, Bernhard T. Baune, Beatrice Benatti, Djamila Bennabi, Sven Estercam, Philip Gorwood, Luis Gutiérrez-Rojas, Vassilis Martiadis, Patricio Molero, Claus Normann, Richard Perry, William Pitchot, Andreas Reif, Gianluca Rosso, Eduard Vieta, Andrea Fagiolini, Clinical guidance on the use of esketamine nasal spray for patients with treatment resistant depression: A European Delphi consensus report, European Neuropsychopharmacology, 10.1016/j.euroneuro.2026.112907, 113, (112907), (2026).
- Hongwei Zhang, Feng Yin, Lantao Li, Xuefei Li, Weiwei Xu, Yi Zhou, Liang Jin, Hongyan Lin, Xihua Lu, Jianjun Yang, Hai Yu, Effects of low-dose esketamine on early quality of recovery following minimally invasive esophagectomy: a multicenter, randomized controlled study, Annals of Medicine, 10.1080/07853890.2026.2704297, 58, 1, (2026).
- Ludovic Samalin, Maud Rothärmel, Lila Mekaoui, Anne Sauvaget, Clotilde Wicart, Emeline Gaudre-Wattine, Vanessa Cohignac, Andrés Malatesta, Julien Dupin, Effectiveness and factors associated with esketamine response during the 4-week induction period for treatment-resistant depression: post-hoc analysis of the real-world ESKALE study, Journal of Psychiatric Research, 10.1016/j.jpsychires.2026.03.011, 197, (298-302), (2026).
- Trisha Menon, Andy Lu, Akhilan Arulmozhi, Christine E. Dri, Sabrina Wong, Kayla M. Teopiz, Gia Han Le, Serene Lee, Cory R. Weissman, Roger S. McIntyre, The use of repetitive transcranial magnetic stimulation (rTMS), electroconvulsive therapy (ECT), ketamine, and esketamine in reducing suicidality in major depressive disorder: A comprehensive narrative review, Psychiatry Research, 10.1016/j.psychres.2026.117036, 359, (117036), (2026).
- Clara de Oliveira Lapa, Thiago Viola, Rodrigo Delfino, Luiza Dutra, Gabriela Rubira, Rafaela Jung Kurtz Rodrigues, Sayra Catalina Coral, J. Antoni Ramos-Quiroga, Lucas Spanemberg, Systematic review and meta-analysis of intranasal esketamine for treatment-resistant depression: Evidence from real-world studies, Journal of Affective Disorders, 10.1016/j.jad.2026.121257, 401, (121257), (2026).
- Juan An, Xuejing Li, Zhiqi Li, Jinghui Wang, Yuanming Pan, Intranasal administration in modulating depressive-like behavior and reconstructing treatment paradigms through neuroinflammation and neurotrophic pathways, Journal of Nanobiotechnology, 10.1186/s12951-026-04417-y, 24, 1, (2026).
- Rocío Gómez-Juanes, Guillermo Mompaler Lázaro, Adoración Castro, Guillem Navarra-Ventura, Josep Antoni Mestre Quetglas, Ana Bolon Marset, Julia Van der Walt Monasterio, Jaume Andreu Garcias Trullols, Miquel Roca, Margalida Gili, Joan Salvà, Mauro Garcia-Toro, Intranasal esketamine for treatment-resistant depression: real-world effectiveness in electroconvulsive therapy non-responders, The European Journal of Psychiatry, 10.1016/j.ejpsy.2026.100349, 40, 2, (100349), (2026).
- J. García-Jiménez, D. Nuñez-Arias, G. Carretero Merelo, A. Miller, A. Martínez Romero, L. Gutiérrez-Rojas, J. E. Mesones Peral, Esketamine nasal spray for treatment-resistant depression: A retrospective multicenter real-world cohort study on effectiveness and suicidal outcomes, Journal of Psychopharmacology, 10.1177/02698811261430495, 40, 6, (914-924), (2026).
- Bernhard T. Baune, Kevin Rosemann, Dimitri Hefter, Mustafa Tonkul, Erhan Kavakbasi, Intranasal esketamine: real-world clinical practice in treatment-resistant depression and factors associated with treatment response, BMC Psychiatry, 10.1186/s12888-026-07980-8, 26, 1, (2026).
- Jin-Ming Liu, Yan-Lin Zhang, Fang Guo, Bin-Wu Li, Hu Chen, Yuye Mo, Jiangwei Kong, Xiaohui Tan, Weibin Wu, Xiong Cao, Treatment with perampanel alleviates depression-like behavior in mice via modulating GluN2B expression to improve excitatory synaptic transmission, Translational Psychiatry, 10.1038/s41398-026-03874-1, 16, 1, (2026).
- See more