Cost-per-remitter for esketamine nasal spray versus quetiapine for treatment-resistant depression
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Estimate the cost-per-remitter with esketamine nasal spray plus an oral antidepressant (ESK NS + OAD) versus quetiapine extended release plus an oral antidepressant (QTP XR + OAD) among adults with treatment-resistant depression (TRD). Materials & methods: An Excel-based model was developed to estimate the cost-per-remitter for ESK NS + OAD and QTP XR + OAD from the perspective of a US commercial insurance plan and Medicaid. Remission and response rates were estimated in 4-week intervals over 32 weeks using data from the ESCAPE-TRD phase IIIb clinical trial comparing ESK NS + OAD versus QTP XR + OAD in adults with TRD. Direct healthcare costs were sourced from health economic literature and the RED BOOK® drug pricing database. Indirect costs were derived from a separate analysis of ESCAPE-TRD using the Work Productivity and Activity Impairment: Depression questionnaire. Adults not remitting/responding either stayed on current treatment or discontinued current treatment and initiated either augmented therapy with antipsychotics or repetitive transcranial magnetic stimulation. In a scenario analysis, all individuals who did not achieve response and discontinued treatment initiated repetitive transcranial magnetic stimulation. Results: The remission rate at 32 weeks was 50% for adults receiving ESK NS + OAD and 33% for adults receiving QTP XR + OAD. The cost-per-remitter for ESK NS + OAD compared with QTP XR + OAD was $3102.17 lower in the commercial setting and $456.12 lower in the Medicaid setting. Under the scenario analysis, the cost-per-remitter for ESK NS + OAD compared with QTP XR + OAD was $15,133.66 lower in the commercial setting and $12,487.62 lower in the Medicaid setting. Conclusion: The findings suggest that ESK NS + OAD is a cost-effective treatment for adults with TRD compared with QTP XR + OAD in the commercial and Medicaid settings.
Plain language summary: Comparison of cost and benefits of esketamine nasal spray versus quetiapine XR for treatment-resistant depression
What is this article about?
Esketamine nasal spray plus oral antidepressant (ESK NS + OAD) and quetiapine extended release plus oral antidepressant (QTP XR + OAD) are treatments for adults with treatment-resistant depression. This study uses an Excel-based model to determine whether treatment with ESK + OAD delivers more benefit for the money spent compared with treatment with QTP XR + OAD under commercial and Medicaid insurance coverage. Our model leveraged treatment efficacy results from the ESCAPE-TRD clinical trial and considered overall healthcare costs associated with treatment use, inpatient and outpatient visits and reduced work productivity.
What were the results?
We find that although ESK NS + OAD has higher annual costs, these are more than offset by the better clinical outcomes achieved by this treatment compared with QTP XR + OAD.
What do the results mean?
Our findings suggest that, under commercial or Medicaid insurance, more patients treated with ESK NS + OAD achieved remission compared with those on QTP XR + OAD, leading to lower related medical costs.
Major depressive disorder (MDD) is one of the most common mental health conditions in the USA today, with an estimated 8.3% of all US adults having experienced a major depressive episode in the past year [1]. MDD results in substantial clinical, economic and societal burden [2–4]. Treatment-resistant depression (TRD) is often defined as a condition in which adults with MDD do not respond to treatment after at least two trials of different medications of adequate dose and duration [5]. Recent research estimates the prevalence of TRD at 30.9% of medication-treated MDD patients [5]. Several studies report that adults with TRD have higher rates of relapse, lower rates of remission and disproportionately higher clinical, economic and societal burden than adults with nontreatment resistant MDD or no depression [5–7].
Current therapeutic options for TRD include treatments such as oral antidepressants, augmentation therapy (e.g., adding an antipsychotic to an antidepressant), esketamine and brain stimulation [8]. Brain stimulation via modalities that include electroconvulsive therapy, repetitive transcranial magnetic stimulation (rTMS) or vagus nerve stimulation is typically reserved for patients with persistent TRD after several lines of ineffective therapies [8], and these interventions are often clinically and economically burdensome [9]. Another treatment approach for patients experiencing TRD is augmentation with atypical antipsychotic agents, which includes treatment with a combination of oral antidepressants and medications such as quetiapine, aripiprazole, olanzapine and risperidone [8].
Unfortunately, augmentation therapy with antipsychotic medications can also present clinical and practical challenges that may undermine effectiveness. Adherence rates for augmentation therapy are low [10], and atypical antipsychotics (APS) are associated with side effects such as significant weight gain and hypertriglyceridemia, which in turn contribute to treatment noncompliance [11]. As such, there is a need for treatment options that are more clinically effective and less cumbersome on patients and insurers.
Esketamine nasal spray (ESK NS) is a treatment for adults with TRD that is self-administered under direct clinical supervision [12]. In the recently completed phase IIIb, randomized, open-label, rater-blinded, active-controlled, international, multicenter ESCAPE-TRD trial, the efficacy and safety of ESK NS plus an oral antidepressant (ESK NS + OAD) was compared with quetiapine extended release plus oral antidepressant therapy (QTP XR + OAD) in adults with TRD. ESCAPE-TRD included a screening phase of up to 2 weeks, an acute dosing phase of 8 weeks, a maintenance dosing phase of 24 weeks, and a follow-up phase of 2 weeks after the last dose. Adults included in this study were aged 18–74 years and met the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) criteria for single-episode or recurrent MDD, had a score at least 34 on the 30-item Inventory of Depressive Symptomatology–Clinician-Rated scale (IDS-C30), did not respond to at least two consecutive treatments from at least two different antidepressant classes with adequate dose and duration, and had been receiving a single selective serotonin reuptake inhibitor or serotonin–norepinephrine reuptake inhibitor prior to randomization that was continued throughout the study. Adults were excluded if they had their first episode of MDD when they were 55 years or older, had a DSM-5 MDD or psychotic disorder diagnosis with psychotic features, received current treatment with >50 mg of quetiapine or esketamine, did not show signs of minimal clinical improvement on current AD therapy, or had previously received vagal nerve or deep brain stimulation in the current depressive episode [13].
Results from ESCAPE-TRD demonstrated that ESK NS + OAD increased the probability of achieving remission (defined as Montgomery–Åsberg Depression Rating Scale (MADRS) score ≤10) and remaining relapse free compared with QTP XR + OAD [14].
The clinical outcomes observed in ESCAPE-TRD have yet to be supplemented with research on the cost implications of ESK NS + OAD versus QTP XR + OAD. Previous research on the cost implications of treatment with ESK NS + OAD versus placebo + OAD demonstrates that, when considering the effects of treatment efficacy on medical and other costs, ESK NS + OAD treatment is associated with a lower cost-per-remitter compared with nasal placebo + OAD [15]. Building upon this prior analysis, in the present study, we compared the cost-per-remitter between ESK NS + OAD and QTP XR + OAD using an Excel-based model to calculate a 32-week cost-per-remitter in the commercial and Medicaid settings.
Materials & methods
An Excel-based model was used to calculate a 32-week cost-per-remitter in the commercial and Medicaid settings for both ESK NS + OAD and QTP XR + OAD, leveraging observable clinical trial data from the phase IIIb ESCAPE-TRD clinical trial in addition to direct healthcare and indirect economic cost estimates derived from the healthcare literature and a separate analysis using the Work Productivity and Activity Impairment: Depression (WPAI:D) questionnaire [16]. To account for variation in treatment regimens initiated upon discontinuation of ESK NS + OAD or QTP XR + OAD, an alternative modeling scenario in which individuals who stop receiving treatment in both comparator arms were assumed to have initiated rTMS was also tested. Finally, a probabilistic sensitivity analysis was conducted to examine how cost-per-remitter estimates change when random variation is introduced into different model specifications.
Data sources
Data on treatment efficacy (i.e., attainment of clinical end points) were sourced from the phase IIIb clinical trial ESCAPE-TRD comparing the efficacy and safety of ESK NS + OAD versus QTP XR + OAD and restricted to the subgroup of adults who received ESK NS + OAD or QTP XR + OAD consistent with US prescribing information [13,17]. Estimates of direct healthcare costs (including medical care and drug costs) were derived from health economic literature and the RED BOOK® drug pricing database [18]. Indirect costs attributed to work productivity loss from presenteeism and absenteeism were derived from a separate analysis of ESCAPE-TRD participants using the WPAI:D questionnaire [16] and US Bureau of Labor Statistics survey results [19,20].
Modeling framework & key modeling assumptions
An Excel-based cost model was developed using methods consistent with a previous model estimating the cost of ESK NS + OAD and nasal placebo + OAD [15]. This model provides cost estimates associated with achievement of response and remission for individuals on ESK NS + OAD and QTP XR + OAD by accounting for differences in these efficacy outcomes (remission and response) across the two active treatment arms in ESCAPE-TRD. Figure 1 shows the overall modeling framework used in the present study.
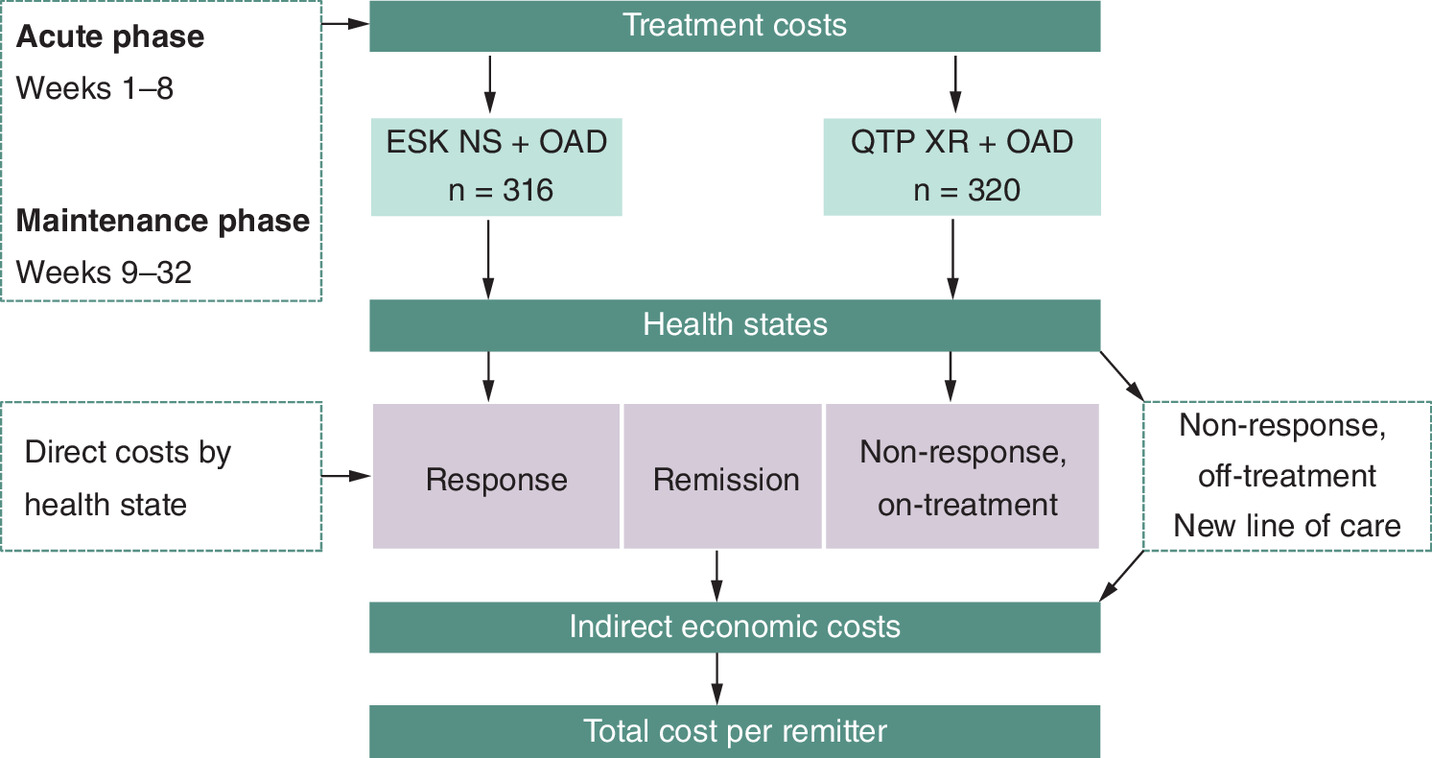
Figure 1. Model framework.
ESK NS: Esketamine nasal spray; OAD: Oral antidepressant; QTP XR: Quetiapine extended release.
Key comparators & outcomes
This model considered two treatment arms consistent with the phase IIIb ESCAPE-TRD clinical trial for esketamine: ESK NS + OAD and QTP XR + OAD. The percentage of patients who achieved response and remission in 4-week intervals between week 8 and week 32 was directly observed from the ESCAPE-TRD trial among the subgroup of adults treated in accordance with US prescribing label information [13,17]. Remission was defined by a MADRS score ≤10 and response was defined as an improvement in MADRS by at least 50% or a MADRS score of ≤10. Table 1 shows the percentage of patients who achieved response and remission, as well as the percentage of patients who continued treatment and the percentage of patients who transitioned off treatment, by comparator arm at week 8 and week 32.
| Parameter | ESK NS + OAD | QTP XR + OAD |
|---|---|---|
| Individuals, n | 316 | 320 |
| Response rate including remission (8 weeks) | 51.9% | 37.2% |
| Remission rate (8 weeks) | 26.3% | 18.1% |
| Non-response, on-treatment rate (8 weeks) | 37.3% | 40.9% |
| Non-response, off-treatment rate (8 weeks) | 10.8% | 21.9% |
| Response rate including remission (32 weeks) | 66.8% | 47.2% |
| Remission rate (32 weeks) | 50.3% | 32.5% |
| Non-response, on-treatment rate (32 weeks) | 11.1% | 13.1% |
| Non-response, off-treatment rate (32 weeks) | 22.2% | 39.7% |
ESK NS: Esketamine nasal spray; OAD: Oral antidepressant; QTP XR: Quetiapine extended release.
Per-patient costs associated with achieving remission over a 32-week period were compared between the treatment arms. Both direct (treatment and healthcare) and indirect (productivity) costs were considered.
Model perspective
Two US payer perspectives were considered, reflecting the different cost implications for different insurance providers: Commercial (i.e., employer-sponsored private health insurance) and Medicaid. Each payer perspective was modeled independently using payer-specific cost inputs where available.
Patient population
The analysis focused on adults with TRD who were defined according to the eligibility criteria of the US label subgroup for the ESCAPE-TRD trial. Participants were required to be 18–74 years old, and to have had a history of non-response to at least two consecutive and adequately dosed treatments from at least two different antidepressant classes during the current episode of depression [17].
Efficacy end points & health states
Table 1 describes key efficacy inputs for the model. Efficacy inputs were derived directly from the results of the ESCAPE-TRD clinical trial [13,17]. Rates of remission, response and non-response in individuals discontinuing and remaining on initial treatment were extracted from ESCAPE-TRD in 4-week intervals from week 8 to week 32. As seen in Table 1, the response and remission rates for ESK NS + OAD are higher than the efficacy rates observed for QTP XR + OAD in the ESCAPE-TRD trial. Efficacy rates were assumed to be the same for both the commercial and Medicaid settings.
Cost inputs
Table 2 describes the payer-specific cost inputs for the different health states. Costs for individuals who transitioned off initial treatment were assumed to be equal across both arms and both payer settings. Direct healthcare costs differed by efficacy results (i.e., individuals who did not achieve response had greater direct healthcare costs compared with individuals who achieved response) and payer setting (i.e., individuals who did not achieve response in the Medicaid setting had lower direct healthcare costs compared with individuals who did not achieve response in a commercial setting). Indirect healthcare costs varied by treatment arm. Further discussion of model cost parameter differences follows.
| Parameter | Commercial | Medicaid | ||
|---|---|---|---|---|
| ESK NS + OAD | QTP XR + OAD | ESK NS + OAD | QTP XR + OAD | |
| Treatment costs | ||||
| Treatment costs | ||||
| Cost per ESK NS device | $342 | n/a | $263 | n/a |
| Average cost per administration | $271 | n/a | $271 | n/a |
| Average weekly costs (weeks 1–8) | $1585 | $11 | $1314 | $10 |
| Average weekly costs (weeks 9–32) | $956 | $12 | $799 | $11 |
| Off-treatment non-responder – new treatment initiation cost (base-case) | $600 | $600 | ||
| Off-treatment non-responder – new treatment initiation cost (scenario analysis) | $1172 | $1172 | ||
| Direct healthcare costs (weekly) | ||||
| Non-responder | $408 | $380 | ||
| Responder | $250 | $280 | ||
| Remitter | $174 | $191 | ||
| Indirect economic costs (weekly) | ||||
| Non-responder | $529 | $607 | $529 | $607 |
| Responder | $529 | $607 | $529 | $607 |
| Remitter | $529 | $607 | $529 | $607 |
ESK NS: Esketamine nasal spray; OAD: Oral antidepressant; QTP XR: Quetiapine extended release.
Treatment costs
Individuals in both treatment arms were assumed to have an average weekly OAD cost of $6.16 in the commercial setting based on average wholesale acquisition costs of a basket of reference drugs [18]. For Medicaid, the 13.0% statutory rebate for noninnovator multiple source drugs was applied to yield an average weekly OAD cost of $5.36 [21].
In the acute phase (first 8 weeks), individuals receiving ESK NS + OAD were assumed to receive 1.5 ESK NS administrations per week with 2.29 devices administered per session based on the average observation in the ESCAPE-TRD trial [22]. ESK NS device cost was estimated to be $341.83 ($262.87 for Medicaid with a 23.1% rebate) [18,23]. In addition, treatment administration cost was assumed to be $271.48 based on an analysis of relevant claims observed in the data provided by Merative MarketScan Commercial Claims and Encounters [22]. Overall, drug and administration cost for individuals receiving ESK NS + OAD in the acute phase was assumed to be $1585.35 per week ($1313.82 per week for Medicaid).
In the maintenance phase (weeks 9–32), individuals receiving ESK NS + OAD were assumed to receive one ESK NS administration per week and 1.99 devices per administration [22]. The overall drug and administration cost for individuals receiving ESK NS + OAD in the maintenance phase was assumed to be $956.39 per week ($798.80 per week for Medicaid).
A proportion of individuals receiving ESK NS + OAD in the maintenance phase were modeled to receive ESK NS + OAD once every 2 weeks while the remaining share received a weekly dose to represent variation in weekly and bi-weekly administration in actual maintenance phase use. 76.7% of remitters and 45.2% of non-remitting responders were assumed to have received ESK NS + OAD administration bi-weekly in the maintenance phase (weeks 9–32).
Individuals receiving QTP XR were assumed to receive a daily dose of 185.87 mg in the acute phase and 219.62 mg in the maintenance phase based on data from the ESCAPE-TRD trial [22], with a generic price of $0.00361 per mg based on RED BOOK® pricing data [18]. Overall, drug costs for individuals receiving QTP XR + OAD were assumed to be $10.86 per week ($10.06 per week for Medicaid) in the acute phase and $11.72 per week ($10.92 per week for Medicaid) in the maintenance phase.
At each 4-week interval, a proportion of individuals did not achieve response and transitioned off ESK NS or QTP XR. In the base case model, 50% of individuals that transitioned off initial treatment were assumed to initiate augmentation therapy with APS while the other 50% initiated rTMS to simulate expected alternative care scenarios. The average weekly cost of an individual that transitioned off initial treatment was estimated to be $600.44, based on estimates of average weekly APS and rTMS treatment costs reported in the health economic literature [24,25].
An alternative scenario in which 100% of individuals who did not achieve response transitioned off the initial treatment were assumed to have initiated rTMS was also modeled. The average cost for such individuals was $1172.06 based on average weekly rTMS treatment costs reported in the health economic literature [24,25].
Direct healthcare costs
Direct all-cause healthcare costs included medical services costs, such as inpatient and outpatient visits, and treatment costs. Healthcare costs were assigned to each health state (i.e., remission, response and non-response) based on published literature evaluating the average overall healthcare costs associated with treating adults with TRD with different levels of depression severity [26,27]. All costs were converted from annual to weekly figures and inflated to 2023 dollars.
Indirect costs
An analysis was conducted to assess the indirect economic cost of work productivity loss due to absenteeism (i.e., percentage of time missed from work due to health in the past 7 days) and presenteeism (i.e., percentage of impairment while at work in the past 7 days). The average weekly cost of work productivity loss was estimated using responses to the WPAI:D questionnaire from individuals enrolled in the ESCAPE-TRD trial [16] and survey results from the US Bureau of Labor Statistics [19,20].
Consistent with the WPAI:D analysis of participants in the ESCAPE-TRD trial, indirect economic costs varied by treatment arm and were held constant across efficacy states. Based on a Kaiser Family Foundation analysis of 2021 federal survey data, 61% of nonelderly adults with Medicaid who are also not covered by Medicare are employed full or part-time [28]. This employment rate was applied to the indirect costs in the Medicaid setting. The average weekly indirect economic cost was $528.78 for individuals receiving ESK NS + OAD and $606.51 for individuals receiving QTP XR + OAD. The average weekly indirect economic costs were assumed to be the same in the Medicaid setting.
Estimating cost-per-remitter
For each comparator arm, the total per-patient cost for each category (treatment, direct healthcare and indirect economic) was calculated for a given 4-week interval as the average of the costs for a given health state weighted by the share of individuals in that health state. To estimate cost-per-remitter for each arm, the total per-patient cost in each arm was then divided by the remission rate at week 32 for each arm.
Probabilistic sensitivity analysis
A probabilistic sensitivity analysis was conducted to test the robustness of the base case results under alternative efficacy and cost inputs for the commercial setting. This probabilistic sensitivity analysis used a Monte Carlo simulation technique, allowing for simultaneous variation in efficacy and cost inputs. The model was run 5000-times using sets of input parameters that were randomly drawn from prespecified distributions representing the expected uncertainty surrounding the mean estimate for a given parameter. The efficacy inputs were assumed to have a binomial distribution and the cost inputs were assumed to have a gamma distribution, all defined with a mean equal to the baseline value and a normalized standard deviation of 0.2. This approach is similar to the one conducted in a previous cost-per-remitter analysis of ESK NS + OAD treatment compared with nasal placebo + OAD treatment [15]. See Supplementary Figure 1 for the distribution of efficacy inputs considered in these analyses.
Results
Base case
The remission rate at week 32 was 50.3% for individuals receiving ESK NS + OAD and 32.5% for individuals receiving QTP XR + OAD. For individuals receiving ESK NS + OAD at 32 weeks, per-patient treatment cost was $28,337 ($24,117 for Medicaid), direct healthcare costs were $8992 ($9076 for Medicaid) and indirect economic costs were $16,921 ($10,322 for Medicaid). For individuals receiving QTP XR + OAD at 32 weeks, per-patient treatment cost was $6404 ($6387 for Medicaid), direct healthcare costs were $10,236 ($10,029 for Medicaid), and indirect economic costs were $19,408 ($11,839 for Medicaid).
In the base case scenario, where equal proportions of individuals who did not achieve response and who discontinued initial treatment received rTMS or APS augmentation as alternative treatment, ESK NS + OAD treatment was associated with a lower cost-per-remitter over 32 weeks compared with QTP XR + OAD in both the commercial and Medicaid settings. The cost-per-remitter for individuals receiving ESK NS + OAD in the commercial setting at 32 weeks was $107,817 ($86,483 for Medicaid). The cost-per-remitter for individuals receiving QTP XR + OAD in the commercial setting at 32 weeks was $110,919 ($86,939 for Medicaid). In the base case scenario, therefore, the cost-per-remitter for ESK NS + OAD was $3102 lower than that of QTP XR + OAD in the commercial setting and $456 lower than that of QTP XR + OAD in the Medicaid setting. Figure 2 indicates that, despite ESK NS + OAD being associated with higher treatment cost, improved efficacy and lower direct healthcare and indirect economic costs produced an overall lower cost-per-remitter compared with QTP XR + OAD.
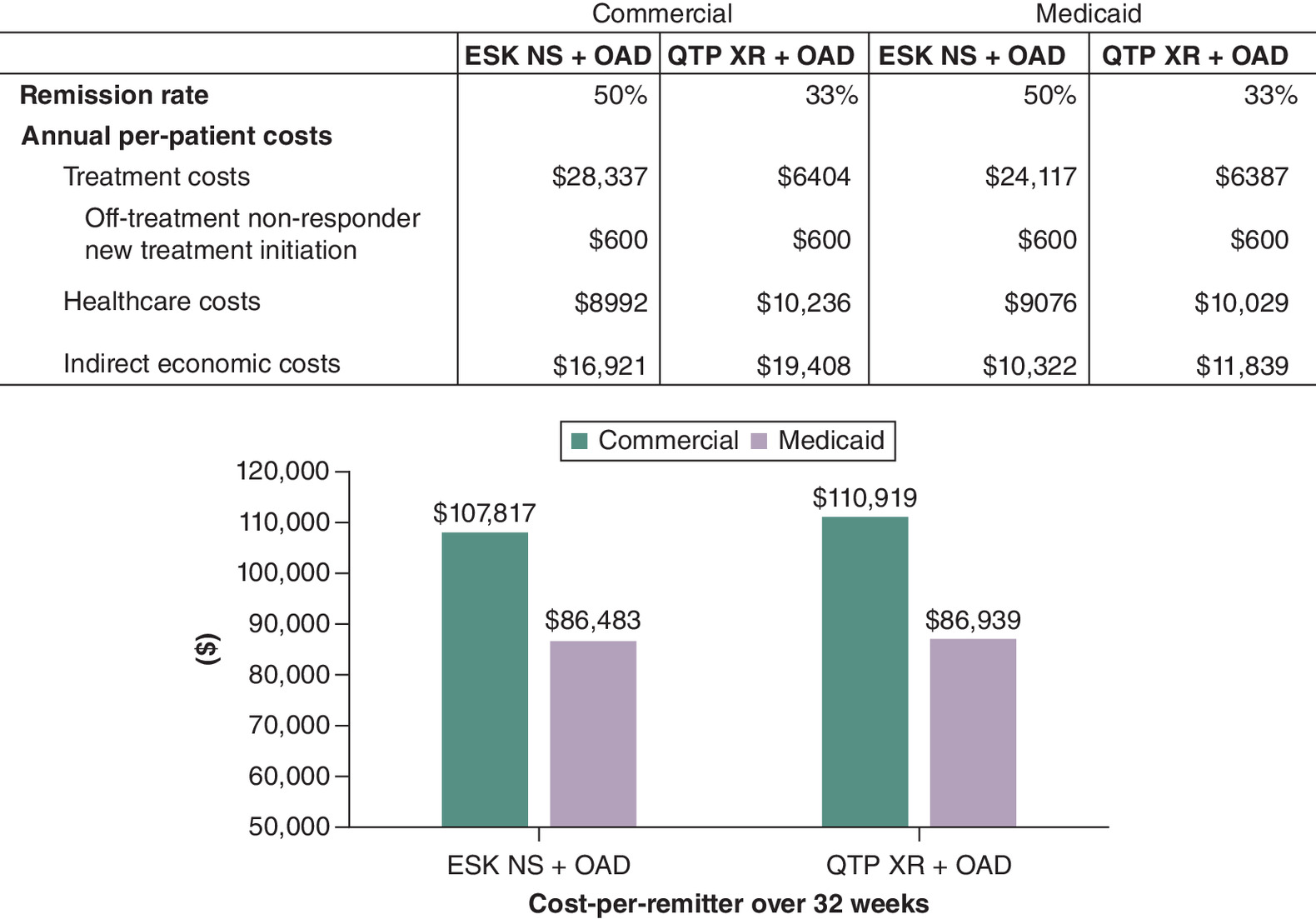
Figure 2. Base case results.
ESK NS: Esketamine nasal spray; OAD: oral antidepressant; QTP XR: Quetiapine extended release.
Alternative off-treatment care scenario
In the alternative scenario where 100% of individuals who went off initial treatment initiated rTMS treatment, the cost-per-remitter difference between ESK NS + OAD and QTP XR + OAD was more pronounced. For individuals receiving ESK NS + OAD, per-patient treatment cost was $31,354 ($27,135 for Medicaid). For individuals receiving QTP XR + OAD, per-patient treatment cost was $12,263 ($12,246 for Medicaid). Direct and indirect healthcare costs for both treatment arms and payer perspectives remained the same as they were in the base case scenario.
The cost-per-remitter for individuals receiving ESK NS + OAD in the commercial setting at 32 weeks was $113,813 ($92,479 for Medicaid). The cost-per-remitter for individuals receiving QTP XR + OAD in the commercial setting at 32 weeks was $128,947 ($104,967 for Medicaid). In the alternative off-treatment care scenario, the cost-per-remitter for ESK NS + OAD was $15,134 lower compared with QTP XR + OAD in the commercial setting and $12,488 lower than that of QTP XR + OAD in the Medicaid setting. Figure 3 demonstrates that the difference in cost-per-remitter between ESK NS + OAD and QTP XR + OAD is even more pronounced in the alternative care scenario than in the base case scenario.

Figure 3. Alternative off-treatment care scenario results.
ESK NS: Esketamine nasal spray; OAD: Oral antidepressant; QTP XR: Quetiapine extended release.
Probabilistic sensitivity analyses
Of 5000 runs of the probabilistic sensitivity analysis, each with randomly simulated efficacy and cost parameters under prespecified distribution assumptions, 2706 (54%) produced a result where the cost-per-remitter for ESK NS + OAD was more favorable than the cost-per-remitter for QTP XR + OAD. Figure 4 illustrates the full Monte Carlo distribution of the difference in cost-per-remitter between ESK NS + OAD treatment and QTP XR + OAD treatment.
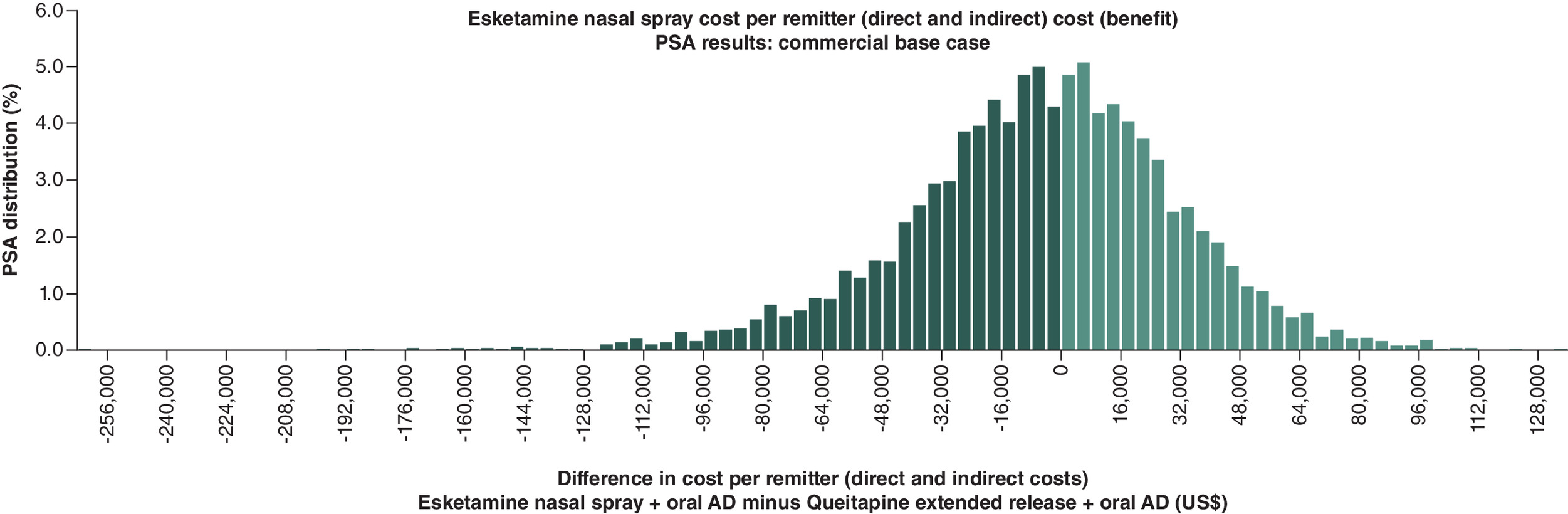
Figure 4. Probability sensitivity analysis results (cost per remission using direct and indirect costs) with commercial insurance.
AD: Antidepressant; PSA: Probability sensitivity analysis.
Discussion
In the ESCAPE-TRD trial, treatment with ESK NS + OAD resulted in higher response and remission rates compared with QTP XR + OAD among adults with TRD [13,17]. We find that these improved clinical efficacy outcomes are associated with a lower cost-per-remitter for ESK NS + OAD treatment compared with QTP XR + OAD. Under the base case scenario from a US commercial payer perspective, the cost-per-remitter for ESK NS + OAD was $3102 lower than that of QTP XR + OAD. Under the base case scenario from a Medicaid perspective, the cost-per-remitter for ESK NS + OAD was $456 lower than that of QTP XR + OAD.
The results also held under alternative modeling assumptions. In a scenario where 100% of individuals who did not achieve response and discontinued initial treatment were assumed to have initiated rTMS, the cost-per-remitter for ESK NS + OAD was $15,134 lower ($12,488 lower in Medicaid) than that of QTP XR + OAD. Additionally, a Monte Carlo simulation was performed with 5000 model runs under varying direct healthcare costs, indirect economic costs, response rates and remission rates in the commercial setting. The simulation yielded 2706 runs (54%) where ESK NS + OAD had a lower cost-per-remitter than QTP XR + OAD.
A previous cost-per-remitter study comparing ESK NS + newly initiated OAD to newly initiated OAD found that the superior clinical efficacy expected with ESK NS + newly initiated OAD would result in a lower cost-per-remitter than the placebo comparator [15]. Our results are consistent with this previous study when comparing ESK NS + OAD with an active treatment alternative (QTP XR + OAD), both in combination with ongoing OAD, although the gap in cost-per-remitter between ESK NS + OAD and QTP XR + OAD was smaller in this study compared with the previous one. This is unsurprising given that QTP XR + OAD is more likely to be effective at treating adults with TRD than nasal placebo; as corroborated by the clinical efficacy outcomes observed in the ESCAPE-TRD trial comparing the two treatments [13].
Our study provides important evidence to payers as they consider coverage policies for ESK NS for adults with TRD. Specifically, we leveraged and built upon a previous Excel-based approach to estimate the cost-per-remitter for adults with TRD undergoing esketamine treatment compared with a common alternative treatment in augmentation therapy with antipsychotic medication. The efficacy rates used in the cost-per-remitter model were directly observed in the ESCAPE-TRD clinical trial, and the estimates of direct and indirect costs used in this study were based on analyses of real-world databases. Additionally, the study assessed an alternative treatment scenario and employed a probabilistic sensitivity analysis to account for uncertainty associated with the model parameters.
There are a few limitations to consider in evaluating this model. First, this analysis was limited to the population included in the ESCAPE-TRD trial evaluating the efficacy and safety of ESK NS compared with quetiapine extended release and may not be representative of the overall US population. Additionally, individuals in ESCAPE-TRD were not located in the US despite a subgroup being treated according to US prescribing information, which limits the generalizability of our findings to a US population. Moreover, differences in treatment adherence and routes of administration could potentially introduce bias in the results. Additionally, since ESK NS must be administered under the supervision of a healthcare professional, trial participants in the ESK NS + OAD arm had twice-weekly visits for the first 4 weeks of the study whereas individuals receiving QTP XR + OAD were seen once weekly, introducing a potential confounding influence of visit frequency. While our study examined clinical efficacy rates directly in ESCAPE-TRD, the treatment costs do not reflect actual commercial arrangements with payers, and the productivity costs do not reflect potential differences in the rate of re-engagement in the labor force due to the improved clinical outcomes among individuals in each treatment arm. This model also assumes that indirect costs varied only by treatment arm and were the same regardless of health state within each arm, which may not represent differences in actual indirect costs. Patient deaths were not addressed in this model, though one death occurred in the ESCAPE-TRD trial from ‘an undetermined cause’. Finally, the model did not evaluate adverse event rates or their associated costs given the focus on short-term outcomes, as observed within the ESCAPE-TRD trial population. Consideration of adverse event rates and their associated costs could be expected to increase the cost-per-remitter for augmentation with antipsychotic treatment due to these treatments being associated with adverse events such as weight gain and hypertriglyceridemia. In contrast, a recent study using the US Food and Drug Adverse Event Reporting System found that long-term use of ESK NS may be correlated with additional adverse events such as addiction risks and suicidal risks [29]. A post hoc analysis found that common treatment-emergent adverse events in ESCAPE-TRD include nervous system, gastrointestinal, and psychiatric disorders, which may also increase the costs associated with ESK NS treatment. However, this study also found that these treatment-emergent adverse events were typically mild/moderate in severity and resolved within the same day [30]. Finally, our study did not assess the cost-per-remitter for other treatments used in the TRD population. For instance, racemic ketamine, a formulation of ketamine delivered intravenously, has been used in the US as an off-label treatment for several psychiatric disorders (e.g., depression, anxiety, suicidal ideation) and might have different cost implications with a similar mechanism of action to ESK NS. A previous study exploring the cost-effectiveness of ESK NS compared with intravenous ketamine using clinical trial efficacy and real-world effectiveness estimates suggested that while ESK NS may not be cost-effective from a healthcare sector perspective, ESK NS may provide similar effectiveness to ketamine with less cost to patients due to insurance coverage [31]. Future studies should assess the cost implications of ESK NS + OAD treatment relative to other accepted therapies.
In conclusion, the findings from this study suggest that when accompanied by oral antidepressant use, ESK NS is a cost-efficient treatment for adults with TRD compared with quetiapine extended release, as higher treatment costs are offset by improved clinical outcomes. The advantages associated with ESK NS are particularly pronounced under the assumption that all individuals who did not achieve response and who discontinued initial treatment subsequently initiated alternative treatment with rTMS. Furthermore, these findings remain robust in the context of a probabilistic sensitivity analysis where variation is introduced to model parameters.
Summary points
•
Many adults with major depressive disorder do not respond to at least two courses of adequate medication dose and duration, experiencing treatment-resistant depression (TRD).
•
Studies have shown that adults with TRD have lower chance of remission, higher risk of relapse, greater clinical burden, utilize significantly more healthcare resources and experience lower quality of life compared with adults without depression or adults with non-treatment-resistant major depressive disorder.
•
Esketamine nasal spray in conjunction with oral antidepressant therapy (ESK NS + OAD) previously demonstrated improved short- and long-term efficacy outcomes compared with quetiapine extended release plus oral antidepressant therapy (QTP XR + OAD) among adult patients with TRD who received treatment in accordance with US prescribing information in ESCAPE-TRD, a randomized, multicenter, phase IIIb, open-label, active-controlled, rater-blinded trial.
•
In this study, we utilize and build upon a previous cost-per-remitter model to quantify the economic benefit of treating adults with TRD with ESK NS + OAD versus QTP XR + OAD.
•
Clinical inputs were derived from ESCAPE-TRD comparing the efficacy and safety of ESK NS + OAD to QTP XR + OAD among the subgroup of adults receiving treatment according to US prescribing information, and cost inputs were derived from health economic literature and prior cost analyses.
•
We find that improved efficacy outcomes of adults taking ESK NS + OAD are associated with lower cost-per-remitter compared with QTP XR + OAD in both the base case and alternative care scenarios.
•
These findings complement previous modeling evaluations of ESK NS and provide additional information for payers and physicians as they make treatment decisions for adults with TRD.
Acknowledgments
Preliminary results from the study were presented during the poster sessions at Neuroscience Education Institute (NEI) Congress; CO, USA 9–10 November 2023.
Author contributions
U Desai and N Kirson contributed to the conception and design, interpretation of the data and drafting of the paper. J Doran, D Eid and A Qu contributed to the analysis and interpretation of the data and drafting of the paper. K Clemens, A Teeple, B Rive, H Bowrey and K Joshi contributed to the conception and design, interpretation of the data and critical revisions to the manuscript for intellectual content. All authors have reviewed and approved the manuscript and agree to be accountable for all aspects of the work.
Financial disclosure
Funding for this research was provided by Janssen Scientific Affairs. Authors from Janssen reviewed the manuscript and made critical revisions for intellectual content. The authors have received no other financial and/or material support for this research or the creation of this work apart from that disclosed.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Competing interests disclosure
N Kirson, U Desai, J Doran, D Eid and A Qu are employees of Analysis Group, Inc., a company that received funding for this study from Janssen Scientific Affairs. A Teeple, B Rive, H Bowrey and K Joshi are employees of Janssen Scientific Affairs. The authors have no other competing interests or relevant affiliations with any organization/entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Data sharing statement
The authors certify that this manuscript reports the secondary analysis of clinical trial data that have been shared with them, and that the use of this shared data is in accordance with the terms agreed upon their receipt. The source of this data is Jassen Scientific Affairs.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 54.58 KB
References
Papers of special note have been highlighted as: • of interest
1.
National Institute of Mental Health. Major Depression Definitions. (2023). Accessed: 28 November 2023: https://www.nimh.nih.gov/health/statistics/major-depression
2.
Jain S, Gupta S, Li VW, Suthoff E, Arnaud A. Humanistic and economic burden associated with depression in the United States: a cross-sectional survey analysis. BMC Psychiatry 22(1), 542 (2022).
3.
Greenberg PE, Fournier AA, Sisitsky T et al. The economic burden of adults with major depressive disorder in the United States (2010 and 2018). Pharmacoeconomics 39(6), 653–665 (2021).
4.
Chow W, Doane MJ, Sheehan J, Alphs L, Le H. Economic burden among patients with major depressive disorder: an analysis of healthcare resource use, work productivity, and direct and indirect costs by depression severity. Am. J. Manag. Care (2019). (Supplements and Featured Publications. February 2019). Available at: https://www.ajmc.com/view/economic-burden-mdd
5.
Zhdanava M, Pilon D, Ghelerter I et al. The prevalence and national burden of treatment-resistant depression and major depressive disorder in the United States. J. Clin. Psychiatry 82(2), 20m13699 (2021).
• Reports the prevalence of treatment-resistant depression (TRD) and the considerable economic, clinical and societal burden of individuals with TRD in the USA.
6.
Sussman M, O'Sullivan AK, Shah A, Olfson M, Menzin J. Economic burden of treatment-resistant depression on the U.S. Health care system. J. Manag. Care Spec. Pharm. 25(7), 823–835 (2019).
7.
Mrazek DA, Hornberger JC, Altar CA, Degtiar I. A review of the clinical, economic, and societal burden of treatment-resistant depression: 1996–2013. Psychiatr. Serv. 65(8), 977–987 (2014).
8.
Voineskos D, Daskalakis ZJ, Blumberger DM. Management of treatment-resistant depression: challenges and strategies. Neuropsychiatr. Dis. Treat. 16, 221–234 (2020).
9.
Delaloye S, Holtzheimer PE. Deep brain stimulation in the treatment of depression. Dialogues Clin. Neurosci. 16(1), 83–91 (2014).
10.
Forma F, Liberman JN, Rui P, Ruetsch C. Adherence to augmentation therapy for the treatment of major depressive disorder. Expert Rev. Pharmacoecon Outcomes Res. 23(3), 327–335 (2023).
11.
Simpson GM. Atypical antipsychotics and the burden of disease. Am. J. Manag. Care 11(Suppl. 8), S235–S241 (2005).
12.
Johnson & Johnson. Spravato important safety information. (2023). Accessed: 28 November 2023: https://www.spravato.com/?&utm_source=google&utm_medium=cpc&utm_campaign=GO-USA-ENG-PS-Spravato-BC-PH-RN-DTC_Core_HV&utm_content=Spravato+-+HV&utm_term=spravato&gclid=CjwKCAiAmZGrBhAnEiwAo9qHiUIgdFyx45wROgSCx0MrK5N0PWtHWH6LZnpUUqUNVagqkN1h9KfuqxoCcpAQAvD_BwE&gclsrc=aw.ds
13.
Reif A, Bitter I, Buyze J et al. Esketamine nasal spray versus quetiapine for treatment-resistant depression. N. Engl. J. Med. 389(14), 1298–1309 (2023).
• Clinical trial of esketamine nasal spray (ESK NS) versus extended-release quetiapine for individuals with TRD showing superior efficacy in ESK NS compared to extended-release quetiapine. Results from this trial were used as clinical inputs for our study.
14.
National Library of Medicine. A long-term comparison of esketamine nasal spray versus quetiapine extended release, both in combination with a selective serotonin reuptake inhibitor/serotonin-norepinephrine reuptake inhibitor, in participants with treatment resistant major depressive disorder (ESCAPE-TRD). (2023). Accessed: 28 November 2023: https://clinicaltrials.gov/study/NCT04338321
15.
Desai U, Kirson NY, Guglielmo A et al. Cost-per-remitter with esketamine nasal spray versus standard of care for treatment-resistant depression. J. Comp. Eff. Res. 10(5), 393–407 (2021).
• Used an approach similar to ours and reported the superior cost-efficiency of ESK NS in conjunction with an oral antidepressant for individuals with TRD compared to standard of care.
16.
Teeple A, Zhdanava M, Shah A et al. Costs associated with work productivity loss of patients with treatment-resistant depression treated with esketamine nasal spray versus quetiapine extended release: ESCAPE-TRD subgroup analysis [poster presentation]. Psych Congress, Nashville, TN, USA (6–10 September 2023).
• Examined the productivity costs associated with clinical outcomes for ESK NS and extended-release quetiapine from the ESCAPE-TRD trial. Productivity loss results from this study were considered economic costs in the model of this study.
17.
McIntyre RS, Mattingly G, Godinov Y et al. Esketamine nasal spray versus quetiapine XR in adults with treatment-resistant depression: A secondary analysis of the ESCAPE-TRD randomized clinical trial. CNS Spectr. 30(1), e26 (2025).
• Presented the efficacy results from the ESCAPE-TRD clinical trial using the same subgroup population as this study.
18.
Merative. Micromedex REDBOOK. https://www.micromedexsolutions.com/micromedex2/librarian. (Accessed: 28 November 2023).
19.
United States Census Bureau. Current Population Survey (CPS). 2022. (2022). Accessed: 28 November 2023: https://www.census.gov/programs-surveys/cps.html.
20.
Bureau of Labor Statistics, U.S. Department of Labor. American Time Use Survey — 2021 results. (2022). Accessed: 28 November 2023
21.
Centers for Medicare & Medicaid Services. Unit rebate amount calculation for non-innovator multiple source drugs. Accessed: 20 December 2023: https://www.medicaid.gov/medicaid/prescription-drugs/medicaid-drug-rebate-program/unit-rebate-calculation/unit-rebate-amount-calculation-for-non-innovator-multiple-source-drugs/index.html
22.
Johnson & Johnson Innovative Medicine Scientific Affairs. Data on File.
23.
Centers for Medicare & Medicaid Services. Unit rebate amount calculation for single source or innovator multiple source drugs. Accessed: 20 December 2023: https://www.medicaid.gov/medicaid/prescription-drugs/medicaid-drug-rebate-program/unit-rebate-calculation/unit-rebate-amount-calculation-for-single-source-or-innovator-multiple-source-drugs/index.html
24.
Ross EL, Zivin K, Maixner DF. Cost-effectiveness of electroconvulsive therapy vs pharmacotherapy/psychotherapy for treatment-resistant depression in the United States. JAMA Psychiatry 75(7), 713–722 (2018).
25.
Voigt J, Carpenter L, Leuchter A. Cost effectiveness analysis comparing repetitive transcranial magnetic stimulation to antidepressant medications after a first treatment failure for major depressive disorder in newly diagnosed patients – a lifetime analysis. PLoS ONE 12(10), e0186950 (2017).
26.
Amos TB, Tandon N, Lefebvre P et al. Direct and indirect cost burden and change of employment status in treatment-resistant depression: a matched-cohort study using a US commercial claims database. J. Clin. Psychiatry 79(2), 17m11725 (2018).
• Shows that individuals with TRD have greater costs compared to individuals with non-TRD major depressive disorder (MDD) and non-MDD.
27.
Pilon D, Sheehan JJ, Szukis H et al. Medicaid spending burden among beneficiaries with treatment-resistant depression. J. Comp. Eff. Res. 8(6), 381–392 (2019).
• Supports similar conclusions as Amos (2018) within the Medicaid population.
28.
Guth M, Drake P, Rudowitz R, Mohamed M. Understanding the intersection of Medicaid & work: a look at what the data say. (2023). Accessed: 28 November 2023: https://www.kff.org/medicaid/issue-brief/understanding-the-intersection-of-medicaid-work-a-look-at-what-the-data-say/
29.
Jiang Y, Du Z, Shen Y, Zhou Q, Zhu H. The correlation of esketamine with specific adverse events: a deep dive into the FAERSdatabase.Eur. Arch. Psychiatry Clin. Neurosci. (2023).
30.
McIntyre RS, Bitter I, Buyze J et al. Safety and tolerability of esketamine nasal spray versus quetiapine extended release in patients with treatment resistant depression. Eur. Neuropsychopharmacol. 85, 58–65 (2024).
31.
Brendle M, Robison R, Malone DC. Cost-effectiveness of esketamine nasal spray compared to intravenous ketamine for patients with treatment-resistant depression in the US utilizing clinical trial efficacy and real-world effectiveness estimates. J. Affect. Disord. 319, 388–396 (2022).
Information & Authors
Information
Published In
Copyright
© 2025 J&J Innovative Medicines (formerly Janssen Scientific Affairs). This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 25 May 2024
Accepted: 14 April 2025
Published online: 9 June 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost-per-remitter for esketamine nasal spray versus quetiapine for treatment-resistant depression. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0092
Export citation
Select the citation format you wish to export for this article or chapter.