Meta-analysis of immunogenicity and safety of human rabies vaccination under Zagreb and Essen regimens
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To assess the immunogenicity and safety of rabies vaccination under the Zagreb and Essen regimens by performing a meta-analysis. Methods: Electronic databases were searched for eligible studies. Risk ratios and weighted mean differences with 95% CIs were used to calculate estimates. Results: A total of 18 studies were included. Rabies virus neutralizing antibody concentration was comparable between the two regimens at D7 and 14. No significant differences were observed in seroconversion rates from D14 and 42. Incidence of fever was higher in Zagreb group (risk ratio: 1.55 [1.37–1.76]); but no significant differences were present for other common adverse events. Conclusion: Rabies vaccination under the Zagreb regimen was noninferior to the Essen regimen in immunogenicity and had an acceptable safety profile.
Rabies is an acute zoonotic disease caused by rabies virus, which almost invariably results in deaths after the onset of clinical symptoms [1–3]. According to the WHO, rabies causes more than 55,000 deaths each year worldwide, particularly in developing countries in Asia and Africa [4]. The virus travels to the central nervous system and causes encephalopathy followed by rapid death. Although being a practically 100% fatal disease, the rabies infection in human can be prevented and controlled by timely active vaccination under a scientific regimen after exposure to the virus.
Nowadays, the WHO recommendation for intramuscular postexposure prophylaxis includes two different immunization regimens: the Essen regimen, which involves five injections administered on each of days 0, 3, 7, 14 and 28; or the Zagreb regimen, with two doses given on day 0 and one dose given on each of days 7 and 21. As the gold standard for all of the postexposure prophylaxis regimens, the traditional Essen regimen has been formally approved and widely used almost anywhere in the world since years, but the cost and duration of this regimen always leads to preventative interventions either not being adopted at all or not being completed, especially in economically disadvantaged countries where the rate of exposure to rabies is higher than other areas. Compared with Essen regimen, the Zagreb regimen has been shown to be equivalently effective and more economical. Moreover, it can be expected to significantly improve patient compliance and rabies vaccine coverage, as it involves fewer doses and visits within a shorter period [5,6].
Although the Zagreb schedule has been recommended for over 20 years by WHO, this intramuscular post-exposure prophylaxis can not be selected until recent years and starts to be approved for more rabies vaccines in some countries, such as China. Additionally, there are still some studies focusing on the comparison of the two kinds of regimens in the recent decade [7,8]. Therefore, additional information is needed to establish the immunogenicity and safety profile of this vaccination program. Here we conducted a meta-analysis to evaluate the immunogenicity and safety of rabies vaccination under the Zagreb regimen compared with the Essen regimen by combining previous studies.
Methods
Literature search
Eligible studies were identified by electronic search of databases and cross-checking references of related papers before 25 September 2019. The databases of PubMed, Sciencedirect, Elsevier and China National Knowledge Infrastructure were systematically searched using the following search terms: ‘rabies’, ‘vaccine’, ‘post-exposure prophylaxis’, ‘Zagreb regimen’, ‘Essen regimen’, ‘immunogenicity’ and ‘safety’. Two independent authors first retrieved potentially relevant papers according to titles and abstracts and then further screened the articles by reading full texts. Any disagreements were resolved by discussion.
Inclusion & exclusion criteria
Studies were included if they met the following selection criteria: clinical studies focused on the immunogenicity, efficacy or safety of rabies vaccination under Zagreb and Essen regimens; the rabies vaccines used are currently available in clinical practice, including human diploid cell vaccine, purified chick embryo cell (PCECV), purified Vero cell rabies vaccine (PVRV) and purified duck embryo cell vaccine; participants were given the same vaccines during the whole intervention; full-text articles written in English or Chinese are available; detailed clinical data were present. Except for original articles, other publications like letters, reviews, case reports or editorial articles were rejected.
Data extraction
Two reviewers independently extracted data from eligible papers into a standardized data collection form. The following data were collected: the first author’s name, year of publication, country, study design, subjects inclusion and exclusion criteria, number of participants, age, gender, vaccine type, administration of rabies immunoglobulin (yes or no), assay and date to test rabies virus neutralizing antibody (RVNA) response, the immunogenicity of vaccines in RVNA concentrations and the percentage of seroconverted subjects with RVNA ≥0.5 IU/ml (this antibody titer of ≥0.5 IU/ml is globally accepted, which was established by the WHO as evidence of an immune response in humans against the rabies virus) and adverse events (local and systemic symptoms). The two reviewers reached consensus on each items through discussion.
The RVNA responses measured on D42 and D45 after the first injection were considered as the same outcome measure. Adverse events reported in more than five studies were extracted and analyzed. Local symptoms include pain, induration, erythema, pruritus and swelling; systemic symptoms include fever, malaise, nausea, headache, myalgia and fatigue. For the study of Fang et al. assessing the safety and immunogenicity of PVRV and PCECV under Zagreb and Essen regimens, we extracted two sets of data for meta-analyses, namely data for PVRV and data for PCECV [8]. For the trial of Li et al. assessing the immune response and safety of PCECV in two age cohorts (children and older adults), we also extracted two sets of data for meta-analyses, namely data for children and data for older adults [9].
Quality assessment
Methodological quality of included studies was assessing with the Cochrane Collaboration tool [10]. The ‘risk of bias’ tool consists of seven items: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting and other bias. Risk of bias for each item was graded as ‘low’, ‘unclear’ and ‘high’. Two investigators appraised the study quality independently and discrepancies were resolved by discussion.
Data analysis
Our objectives were the seroconversion rate, RVNA concentration and adverse events. Risk ratios (RR) and 95% CIs were calculated for the seroconversion rate and adverse events; weighted mean differences (WMDs) and 95% CIs were calculated for RVNA concentration. CIs were used for statistical test and a 95% CI without 1 for RR or without 0 for WMD indicated a significant difference between the two regimens. RVNA levels per study that were expressed as error bars in 95% CIs were converted to standard deviation according to The Cochrane Handbook 7.7.3.2 [10]. In data synthesis, overall estimates were calculated by using a random-effects model based on Mantel–Haenszel method when significant heterogeneity was present, while a fixed-effects model was used when no significant heterogeneity was found. I2 was used as a measure of heterogeneity across studies. An I2 >50% suggests the presence of significant heterogeneity. In the case of significant heterogeneity, sensitivity analyses were done to explore the impact of an individual study by dropping one study each time; or subgroup analyses were conducted according to age cohorts. Begg’s and Egger’s test were performed to test publication bias, of which a p < 0.05 suggests the existence of publication bias. Stata version 15.0 and Review Manager version 5.3 were used to conduct the meta-analysis.
Results
Study selection
The database search yielded 1252 studies and manual search retrieved four studies, resulting in 1256 potentially relevant publications, of which 72 articles were included based on titles and abstracts and underwent full text review. According to the inclusion and exclusion criteria, 18 studies were considered eligible and finally used to meta-analyze [6,8,9,11–25]. The process of study selection is shown in Figure 1.

Figure 1. Flowchart of study selection.
CNKI: China National Knowledge Infrastructure.
Study characteristics
All the included studies were conducted in Asia (China, India, Turkey) over a period of 8 years (2011–2018). A total of 7369 and 22631 participants were included in immunogenicity analysis and safety analysis, respectively. The vaccines used were PCECV, PVRV and human diploid cell vaccine. Among 13 studies evaluating immunogenicity, the RVNA assessment was done by using rapid fluorescent focus inhibition test in 12 studies and ELISA in one study [6,8,9,11–16,18,20–22]. Table 1 shows detailed characteristics of the included studies.
| First author | Year | Country | Study design | Subjects in the Zagreb regimen | Subjects in the Essen regimen | Vaccine | RIG | Ref. | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Number | Age | Sex (M/F) | Number | Age | Sex (M/F) | |||||||
| Chen | 2015 | China | Prospective | 229 | 34.19 ± 7.88 | 131/98 | 199 | 33.45 ± 8.05 | 107/92 | PVRV | Yes | [11] |
| Chen | 2018 | China | Prospective | 273 | 10–60 | 136/137 | 256 | 10–60 | 178/178 | HDCV | No | [12] |
| Fang | 2014 | China | Prospective | 84 | – | – | 81 | – | – | PCECV | No | [8] |
| 111 | – | – | 111 | – | – | PVRV | No | |||||
| Hu | 2014 | China | Prospective | 132 | 38.13 ± 27.08 | 59/73 | 126 | 35.83 ± 26.48 | 61 / 65 | PCECV | No | [13] |
| Huang | 2014 | China | Retrospective | 986 | 0–83 | 502/484 | 878 | 0–82 | 452/426 | PVRV | Yes | [14] |
| Li | 2015 | China | Prospective | 121 | 11 ± 3 | 72/49 | 122 | 10.8 ± 2.9 | 46/76 | PCECV | No | [9] |
| 201 | 62.1 ± 6.5 | 83/118 | 200 | 61.9 ± 6.8 | 77/123 | |||||||
| Liu | 2011 | China | Prospective | 50 | 22–57 | 24/26 | 30 | 20–54 | 14/16 | PVRV | No | [6] |
| Ma | 2014 | China | Prospective | 69 | 38.2 ± 7.1 | 28/41 | 70 | 39.3 ± 6.9 | 37/33 | PCECV | No | [15] |
| Mahendra | 2015 | India | Prospective | 124 | 29.1 ± 8.8 | – | 121 | 27.2 ± 7.3 | – | PCECV | No | [16] |
| Mao | 2013 | China | Retrospective | 3950 | – | – | 2151 | – | – | PVRV | No | [17] |
| Miao | 2018 | China | Prospective | 598 | 33.96 ± 12.20 | – | 604 | 33.86 ± 11.91 | – | PVRV | No | [18] |
| Sari | 2014 | Turkey | Prospective | 607 | 1–98 | – | 154 | 1–98 | – | PVRV | Yes | [19] |
| Shao | 2013 | China | Prospective | 437 | 18–59 | 263/174 | 400 | 18–59 | 159/141 | PCECV | No | [20] |
| Shi | 2017 | China | Prospective | 4972 | 33.7 ± 19.8 | 2608/2364 | 5587 | 33.5 ± 20.4 | 2878/2709 | PVRV | No | [21] |
| Wang | 2017 | China | Prospective | 57 | 61.7 ± 8.2 | 27/30 | 50 | 59.6 ± 6.3 | 22/28 | PVRV | No | [22] |
| Xie | 2015 | China | Retrospective | 102 | 6–81 | 52/50 | 116 | 3–85 | 53 / 63 | PVRV | No | [23] |
| Xie | 2016 | China | Prospective | 450 | – | – | 450 | – | – | PVRV | No | [24] |
| Ye | 2017 | China | Prospective | 91 | 26.8 ± 8.2 | 91 | 47/44 | 27.4 ± 8.4 | 46/45 | PVRV | No | [25] |
F: Female; HDCV: Human diploid cell vaccine; M: Male; PCECV: Purified chick embryo cell; PVRV: Purified Vero cell rabies vaccine; RIG: Rabies immunoglobulin.
Regarding methodological quality, a majority of included studies had a low risk of bias. Several studies that did not mention randomization or allocation were assessed as unclear or high risk of bias in the category ‘selection bias’. Because we judged that the outcomes are not likely to be influenced by lack of blinding, performance bias and detection bias remained at low risk of bias in all cases. Our ratings of the risk of bias in each studies are displayed in Figure 2.
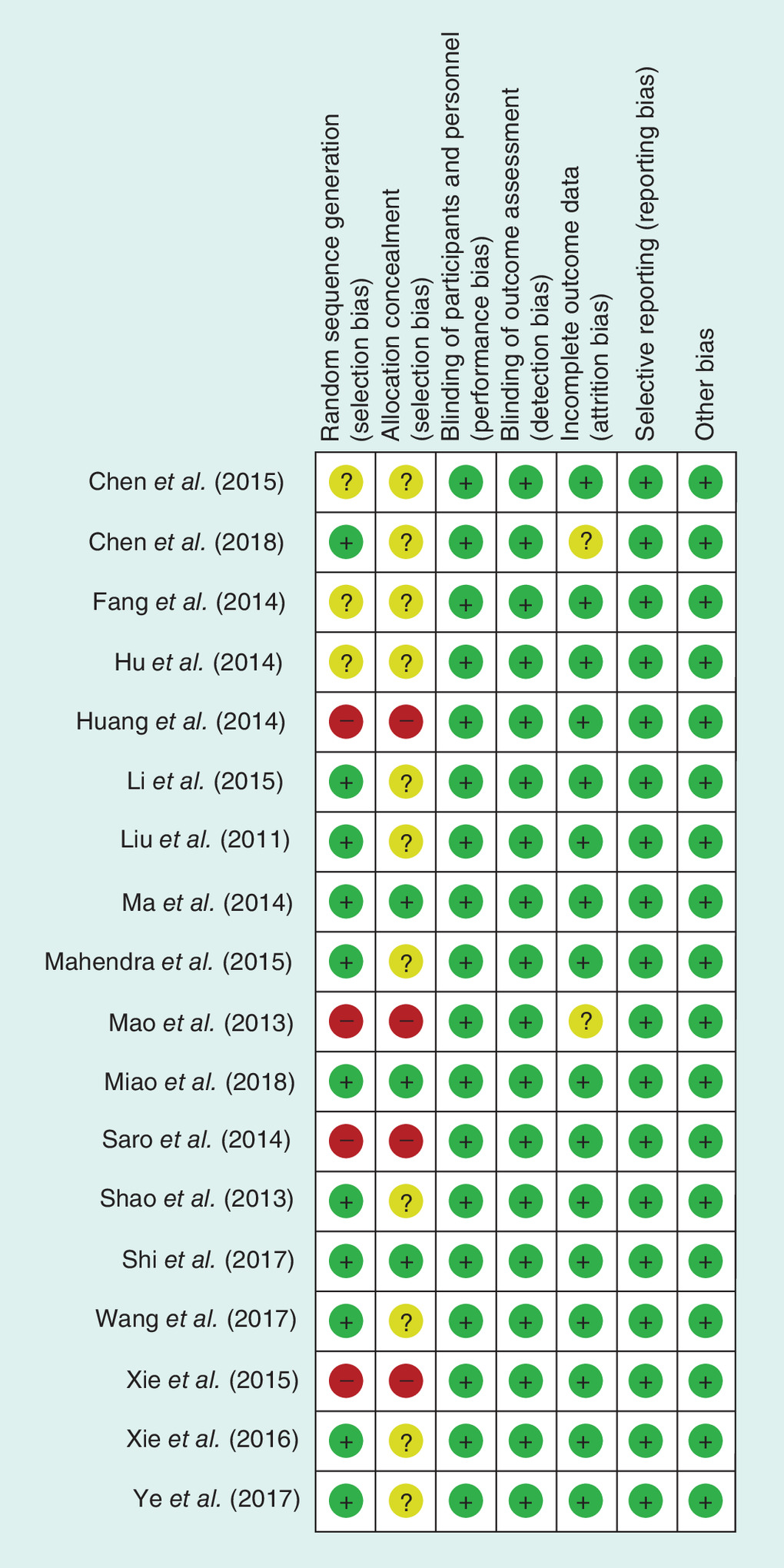
Figure 2. Quality assessment of included studies.
‘+’ represents low risk of bias; ‘?’ represents unclear risk of bias; ‘-’ represents high risk of bias.
Immunogenicity
The immunogenicity as measured by the proportion of participants with RVNA titers ≥0.5 IU/ml was analyzed at 7, 14, 42 and 365 days postimmunization. Summarized outcomes among 13 studies regarding the seroconversion rate are shown in Figure 3. At day 7, the percentage of individual with adequate RVNA titers under the Zagreb regimen was significantly higher than the Essen regimen (RR: 1.22; 95% CI: 1.15–1.30; I2 = 0%). One week after the third vaccine dose (day 14), almost all subjects under both regimens reached to positive for rabies antibody and no difference between two groups was found (RR: 1.00; 95% CI: 0.99–1.01; I2 = 0%); this result remained at day 42, 3 weeks after the last injection in Zagreb and 2 weeks in Essen (RR: 1.00; 95% CI: 0.99–1.00; I2 = 0%). For long-term efficacy, the overall estimate at day 365 showed that possibly the Zagreb regimen was again noninferior to the Essen regimen (RR: 0.95; 95% CI: 0.90–1.00; I2 = 0%).
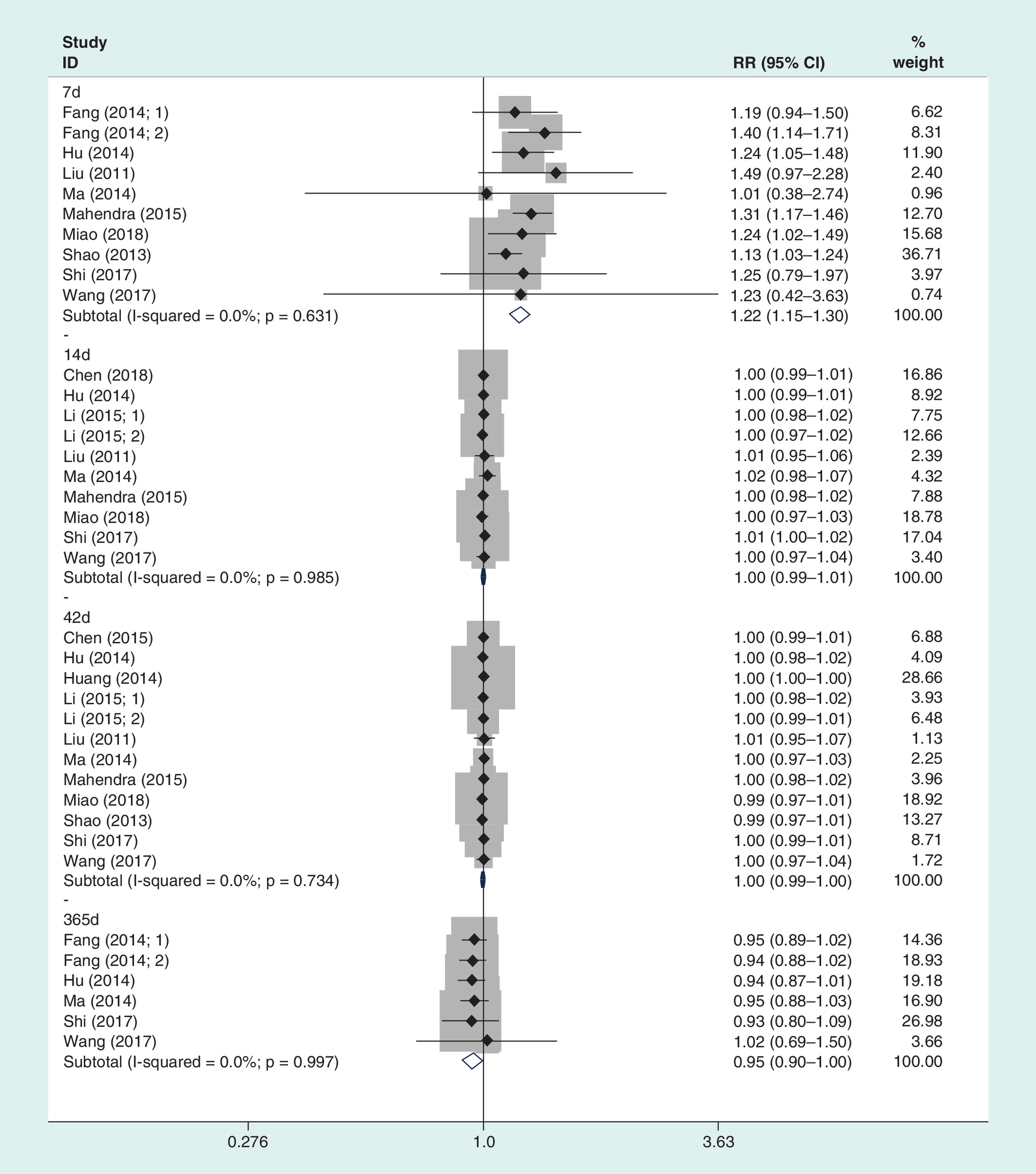
Figure 3. Forest plots of the overall pooled seroconversion rates at D7, 14, 42 and 365.
RR: Risk ratio.
There were totally six studies reporting RVNA concentration. In these studies, subjects having previously received any rabies vaccine were excluded and no rabies immunoglobulin was involved in the whole vaccination treatment. Estimates of RVNA concentration at 7, 14, 42 and 365 days postimmunization were tested in 4, 6, 5 and 3 studies, respectively. On day 7, the results showed that both regimens attained comparable RVNA concentration (WMD: -0.25; 95% CI: -0.67–0.17; I2 = 93%); omitting the study of Mahendra et al. decreased the heterogeneity to 7% but did not affect the result and the reason for this may be a few subjects enrolled in this study exhibited RVNA concentration ≥0.5 IU/ml before vaccination. Antibody concentration remained comparable from D14 (WMD: -0 .71; 95% CI: -1.53–0.10; I2 = 26%), but there was a trend of lower concentration in the Zagreb group according to the higher 95% CI. Expectedly, 3 weeks later (D42) patients with rabies vaccination under the Zagreb regimen achieved significantly lower RVNA concentration compared with those in the Essen regimen (WMD: -3.40, 95% CI: from -6.24 to -0 .56; I2 = 81%). In the interpretation of heterogeneity of concentration on day 42, sensitivity analysis revealed that data of Li et al. from children group had an impact on the heterogeneity but did not change the result. One year after the first dose (day 365), RVNA concentration in both regimens returned to comparable levels (WMD: -0 .03; 95% CI: -0.54–0.48; I2 = 0%).
Safety
In order to evaluate the safety of rabies vaccination under the Zagreb and the Essen regimens, both the most common local and systemic adverse events were extracted and meta-analyzed. No deaths related to rabies virus were reported among 14 analyzed studies [6,8,9,13,15–17,19–25]. Table 2 showed the summary of the safety comparison between the two groups. When comparing local symptoms in the overall population, incidences of pain, induration, pruritus and swelling were comparable among subjects following either regimen; however, erythema was more frequently in the Essen regimen than in the Zagreb regimen. The overall estimates of systemic adverse events, irrespective of population, showed that a significant difference was only found in fever and there were no differences in other systemic symptoms (malaise, nausea, headache, myalgia and fatigue). When analyzing fever, an I2 of 50% was found. Subgroup analyses stratified by age showed that the difference in the incidence of fever became less significant in the adults group (>18 years old) based on its RR of 1.31 (95% CI: 1.10–1.57) and heterogeneity decreased to 8%, while in the children group (<18 years old), the difference becomes more significant according to its RR of 1.75 (95% CI: 1.46–2.10) and heterogeneity decreased to 32%.
| Adverse events | Number of study | Analysis model | RR | 95% CI (%) | I2 value (%) | Significant difference† |
|---|---|---|---|---|---|---|
| Local symptoms | ||||||
| – Pain | 13 | RE | 1.11 | 0.98–1.25 | 11 | No |
| – Induration | 11 | FE | 0.92 | 0.74–1.14 | 0 | No |
| – Erythema | 7 | FE | 0.67 | 0.50–0.88 | 0 | Yes |
| – Pruritus | 7 | FE | 1.01 | 0.82–1.24 | 45 | No |
| – Swelling | 8 | FE | 0.99 | 0.94–1.05 | 24 | No |
| Systemic symptoms | ||||||
| – Fever | 12 | FE | 1.55 | 1.37–1.76 | 50 | Yes |
| – Malaise | 6 | FE | 1.27 | 0.90–1.80 | 0 | No |
| – Nausea | 14 | FE | 1.03 | 0.85–1.24 | 9 | No |
| – Headache | 9 | FE | 1.12 | 0.93–1.33 | 5 | No |
| – Myalgia | 7 | FE | 0.87 | 0.57–1.33 | 0 | No |
| – Fatigue | 8 | FE | 1.02 | 0.91–1.15 | 40 | No |
†
Significant differences of outcomes between the Zagreb and the Essen regimens.
FE: Fixed-effects model; RE: Random-effects model; RR: Risk ratio.
Evaluation of publication bias
Begg’s and Egger’s test were performed based on studies with data on the seroconversion rate at 42 days, local symptoms and systemic symptoms, which suggested no publication bias among the included studies (p = 0.279, p = 0.388 and p = 0.253, respectively).
Discussion
Rabies is an acute neurological disease with almost 100% of fatality rate [26]. Postexposure prophylaxis is the most important method to prevent and control rabies, including timely vaccination with full doses [1]. Intramuscular rabies vaccination after exposure to the virus has been established for several decades and the traditional five-dose Essen regimen recommended by the WHO had been widely adopted in the world [4,27]. However, exposed individuals often withdrew midway and failed to complete the vaccine schedule and thus remained a high risk of rabies virus infection, especially in low-income areas. In order to reduce costs and develop simpler regimens, WHO started to recommend an abbreviated four-dose Zagreb regimen in 1992 [28]. Since then, this Zagreb scheme has been intensively investigated from aspects of immunogenicity and safety.
This meta-analysis was conducted to compare the immunogenicity and safety for the use of rabies vaccination administered intramuscularly under the Zagreb and Essen regimens. Our results showed that the Zagreb schedule is noninferior in terms of immunogenicity to the conventional Essen schedule by day 14 and 42 as far as the rates of seroconversion concerned; regarding safety, this four-dose regimen causes slightly more fever, especially in children, which may be due to a double dose at first time vaccination and physiological responses to primary immunization, but noninferiority is demonstrated in other adverse events.
In immunogenicity analysis, data synthesis revealed a significant difference between the two groups on D7 in terms of seroconversion, indicating that the Zagreb induces much earlier antibody comparing with the Essen regimen, which might be more suitable for seriously exposed patients to develop protective antibodies as soon as possible and thus decrease the risk of human rabies. In the analysis of RVNA concentration, the estimates in the Zagreb group were comparable with the Essen group at D7 and 14 after the first injection, but were significantly lower from D42. However, no significant differences were observed in the seroconversion rates between the two regimens from D14 and 42 and these results are in line with the meta-analysis by Scott et al. examining the immunogenicity of PCECV under four- or five-dose regimens [29]. Furthermore, we meta-analyzed the antibody persistence at D365 postimmunization and again found no significant difference between the two groups, but the higher 95% CI of 1.00 precluded us to make a conclusion and thus further studies are needed to provide more robust evidence on this issue.
Adverse events were considered as the biggest challenge for rabies vaccination under the Zagreb regimen due to the administration of a double-dose vaccine on the first day. In the present study, local adverse events were reported as pain, induration, erythema, pruritus and swelling. The Zagreb was found noninferior to the Essen regimen in these local symptoms and even can decrease the possibility of erythema. Systemic adverse events were analyzed as fever, malaise, nausea, headache, myalgia and fatigue. It is observed that the Zagreb schedule induces more fever, especially in <18-year-old patients, which may be associated with more rapid stimulus in a short time and the relatively low immunity of children. However, equivalences were demonstrated between the two schedules in other systemic symptoms. Therefore, the four-dose Zagreb vaccination regimen having an acceptable safety profile is evidence based, as reported by many previous studies [9,15,16]. However, in order to avoid serious side effects caused by fever, particular care needs to be well-prepared and exercised when clinical rabies immunization under the Zagreb regimen is used in children and adolescents.
As a simpler vaccination schedule, the Zagreb regimen was shown to be as effective as the conventional Essen regimen for preventing human rabies and to have a quick response to immunization. Furthermore, this regimen cuts the whole vaccination period from 28 to 21 days, which can greatly reduce workload and improve patients’ compliance [9,14,30]. The findings of this study may provide more information to vaccinees and medical personnel and authorities to have confidence in the four-dose Zagreb regimen. To our knowledge, this is the first meta-analysis specially comparing the Zagreb and the Essen regimens in terms of immunogenicity and safety. The present study, however, may have some limitations. First, rare adverse events were not covered in our analysis due to limited data, even if the safety population was larger than the immunogenicity population. Second, significant heterogeneity in the estimate of RVNA concentration on D42 was caused by the study analyzing children, which suggests that age may be a factor influencing the antibody response, but further analyses were unavailable because of lack of data. Third, for the reason that all the selected studies were conducted in Asian countries and most in China, geographical factor could bring some bias in the final analysis.
Conclusion
The immunogenicity analysis showed that the Zagreb regimen was noninferior to the Essen regimen in preventing rabies in human and had an acceptable safety profile. This more practical vaccination schedule shows fewer doses and lower cost, which is worth promoting. However, given a double dose at the first injection, this four-dose Zagreb regimen might induce more fever. Close attention should be paid, particularly in children, when adopting the Zagreb regimen for rabies immunization. Further studies are encouraged to provide more robust evidence.
•
Rabies is a fetal zoonotic disease but can be prevented and controlled by timely active vaccination under a scientific regimen after exposure to the virus.
•
The Essen regimen and the Zagreb regimen are two immunization regimens for intramuscular postexposure prophylaxis recommended by WHO.
•
This is the first meta-analysis specially comparing the Zagreb and the Essen regimens in terms of immunogenicity and safety.
•
A total of 18 studies were included in this meta-analysis. For immunogenicity, seroconversion rate and rabies virus neutralizing antibody concentration were examined. For safety, local and systemic adverse events were analyzed.
•
The meta-analysis found that the Zagreb regimen and the Essen regimen had similar immunogenicity, with the comparable seroconversion rates at D7 and 14.
•
The Zagreb regimen induced more fever, especially in children, but was noninferior to the Essen regimen in other adverse events (pain, induration, erythema, pruritus, swelling, malaise, nausea, headache, myalgia and fatigue).
•
The Zagreb regimen was noninferior to the Essen regimen in preventing rabies in human and had an acceptable safety profile.
•
Close attention should be paid, particularly in children, when adopting the Zagreb regimen for rabies immunization.
Author contributions
T Li made contribution to work conception, data interpretation and manuscript writing; X Wang and HB Cheng were responsible for study identification, data extraction and analysis. All authors have read and approved the manuscript.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest
1.
Hemachudha T, Wacharapluesadee S, Mitrabhakdi E, Wilde H, Morimoto K, Lewis RA. Pathophysiology of human paralytic rabies. J. Neurovirol. 11(1), 93–100 (2005).
2.
McGettigan JP. Experimental rabies vaccines for humans. Expert Rev. Vaccines 9, 1177–1186 (2010).
3.
Nandi S, Kumar M. Development in immunoprophylaxis against rabies for animals and humans. AJMB 2, 3–21 (2010).
4.
WHO. WHO Expert consultation on rabies: first report. World Health Organ. Tech. Rep. Ser. 931, 1–88 (2005).
5.
Rupprecht CE, Briggs D, Brown CM et al. Use of a reduced (4-dose) vaccine schedule for postexposure prophylaxis to prevent human rabies: recommendations of the advisory committee on immunization practices. MMWR Recomm. Rep. 59(RR-2), 1–9 (2010).
6.
Liu H, Huang G, Tang Q et al. The immunogenicity and safety of vaccination with purified Vero cell rabies vaccine (PVRV) in China under a 2-1-1 regimen. Hum. Vaccin. 7(2), 220–224 (2011).
• A relatively high-quality clinical trial used for this meta-analysis.
7.
Rahimi P, Vahabpour R, Shirzadi MR, Bahramali G, Aghasadeghi MR. Rabies prophylaxis strategy in Iran, a need for an alternative strategy: would the Essen regimen be replaced by Zagreb protocol? Clin. Lab. 65(1), 10.7754 (2019).
8.
Fang Y, Chen L, Liu MQ, Zhu ZG, Zhu ZR, Hu Q. Comparison of safety and immunogenicity of PVRV and PCECV immunized in patients with WHO category II animal exposure: a study based on different age groups. PLoS Negl. Trop. Dis. 8(12), e3412 (2014).
• A relatively high-quality clinical trial used for this meta-analysis.
9.
Li R, Li Y, Wen S et al. Immunogenicity and safety of purified chickembryo cell rabies vaccine under Zagreb 2-1-1 or 5-dose Essen regimen in Chinese children 6 to 17 years old and adults over 50 years: a randomized open-label study. Hum. Vaccin. Immunother. 11(2), 435–442 (2015).
• A relatively high-quality clinical trial used for this meta-analysis.
10.
Higgins J, Green S. Cochrane Handbook for Systematic Reviews of Interventions: Cochrane Book Series. John Wiley & Sons, Ltd, Chichester, UK, 1–649 (2008).
11.
Chen ZQ. Clinical study of rabies vaccine administered with 5-dose immunization program and 2-1-1 immunization program. Med. Aesthe. Cosm. 2, 224 (2015).
12.
Chen ZP, Lv HK, Wang SY, Li YH. Immunogenicity of human diploid cell rabies vaccine vaccinated with Zagreb regimen. Chin. J. Emerg. Resusc. Disaster Med. 13(11), 1069–1071 (2018).
13.
Hu Q, Liu MQ, Zhu ZG, Zhu ZR, Lu S. Comparison of safety and immunogenicity of purified chick embryo cell vaccine using Zagreb and Essen regimens in patients with category II exposure in China. Hum. Vaccin. Immunother. 10(6), 1645–1649 (2014).
14.
Huang F, Xie L, Yi T. Effect and nursing intervention of “2-1-1” rabies vaccine immunization program and ‘5-dose’ immunization program. Prac. Clin. Med. 15(3), 103–104 (2014).
15.
Ma J, Wang H, Li J et al. A randomized open-labeled study to demonstrate the non-inferiority of purified chick-embryo cell rabies vaccine administered in the Zagreb regimen (2-1-1) compared with the Essen regimen in Chinese adults. Hum. Vaccin. Immunother. 10(10), 2805–2812 (2014).
• A relatively high-quality clinical trial used for this meta-analysis.
16.
Mahendra BJ, Narayana DA, Agarkhedkar S et al. Comparative study on the immunogenicity and safety of a purified chick embryo cell rabies vaccine (PCECV) administered according to two different simulated post exposure intramuscular regimens (Zagreb versus Essen). Hum. Vaccin. Immunother. 11(2), 428–434 (2015).
• A relatively high-quality clinical trial used for this meta-analysis.
17.
Mao R, Jin AB, Cao JS. Comparison of different immunization procedures for rabies exposure prophylaxis. Chin. J. Public Health 29(9), 1403–1404 (2013).
18.
Miao L, Shi L, Yang Y et al. Immunological effect of aGV rabies vaccine administered using the Essen and Zagreb regimens: a double-blind, randomized clinical trial. Viral Immunol. 31(3), 242–248 (2018).
• A relatively high-quality clinical trial used for this meta-analysis.
19.
Sari T, Tulek N, Bulut C, Oral B, Tuncer EG. Adverse events following rabies post-exposure prophylaxis: a comparative study of two different schedules and two vaccines. Travel Med. Infect. Dis. 12, 659–666 (2014).
20.
Shao W, Zheng YS, Zhang J, Jiang YZ, Jiang XY. Observation on efficacy and side effects of “2-1-1” Needle injection rabies vaccine in patients exposed. Chin. J. Gen. Prac. 11(11), 1768–1769 (2013).
21.
Shi N, Zhang Y, Zheng H et al. Immunogenicity, safety and antibody persistence of a purified vero cell cultured rabies vaccine (Speeda) administered by the Zagreb regimen or Essen regimen in post-exposure subjects. Hum. Vaccin. Immunother. 13(6), 1–8 (2017).
• A relatively high-quality clinical trial used for this meta-analysis.
22.
Wang J, Luo F, Feng Z et al. Immunogenicity and safety of purified vero cell rabies vaccine (PVRV) produced by Liaoning Cheng Da Co. under Zagreb 2-1-1 or 5-dose Essen regimen in Chinese adults aged 50 and above. Hum. Vaccin. Immunother. 13(1), 144–150 (2017).
• A relatively high-quality clinical trial used for this meta-analysis.
23.
Xie FX, Qiu T. Comparative study of safety of rabies vaccine between 4 and 5 dose immune procedures. J. Prev. Med. Inf. 31(1), 65–68 (2015).
24.
Xie ZW, Chen YN, Liao XW, Wang MC. Safety assessment of different age groups using 2-1-1 vaccination. J. Trop. Med. 16(2), 249–251 (2016).
25.
Ye WM. Comparative analysis on safety of rabies vaccine Phases IV and V immunization for exposed persons. Chin. J. Mod. Drg. Appl. 11(11), 189–191 (2017).
26.
Wang LY, Sun MP, Zhang XC et al. Safety and immunogenicity of two freeze-dried vero cell rabies vaccines for human use in post-exposure prophylaxis. Vaccine 29, 2679–2681 (2011).
27.
Ashwath Narayana DH, Madhusudana SN, Sampath G et al. Safety and immunogenicity study of a new purified chick embryo cell rabies vaccine Vaxirab-N (Pitman-Moore strain) manufactured in India. Hum. Vaccin. Immunother. 10, 120–125 (2014).
28.
WHO Expert Committee on Rabies. World Health Organ. Tech. Rep. Ser. 824, 1–84 (1992).
29.
Scott P, Chanthavanich P, Chen LH et al. Post-exposure prophylaxis (PEP) for rabies with purified chick embryo cell vaccine: a systematic literature review and meta-analysis. Expert Rev. Vaccines 17(6), 525–545 (2018).
30.
Wang CL, Zhang XW, Yu YX. Study on the compliance and economic cost of rabies vaccination. Zhongguo Yi Miao He Mian Yi 16, 254–257 (2010).
Information & Authors
Information
Published In
Pages: 459 - 468
PubMed: 32374178
Copyright
© 2020 Future Medicine Ltd.
History
Received: 23 December 2019
Accepted: 25 February 2020
Published online: 6 May 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Meta-analysis of immunogenicity and safety of human rabies vaccination under Zagreb and Essen regimens. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0202
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Hua-Kun Lv, Xu Chen, Bo Xing, Xiao-Song Hu, Xin-Pei Zhang, Yu-Gang Shen, Yan Wang, Miao-Miao Liu, Ying-Ping Chen, Zhen-Zhen Liang, Yu Mao, A phase 3 clinical trial on the immunogenicity and safety of booster vaccination after Zagreb or Essen regimens, Scientific Reports, 10.1038/s41598-025-88361-1, 15, 1, (2025).
- Zhenzhen Liang, Xu Chen, Bo Xing, Xiaosong Hu, Miaomiao Liu, Xinpei Zhang, Yugang Shen, Yan Wang, Yingping Chen, Huakun Lv, Yu Mao, Safety, immunogenicity and immune-persistence of a lyophilized human rabies vaccine (Vero cells) under Zagreb and Essen regimens: a randomized, open-label, controlled phase III clinical trial in healthy participants aged 10–60 years in China, Frontiers in Immunology, 10.3389/fimmu.2024.1444686, 15, (2024).
- Danaya Chansinghakul, Terapong Tantawichien, Kriengsak Limkittikul, Winai Ratanasuwan, Yuancheng Wang, Celine Petit, Francoise Guinet-Morlot, Carina Frago, Andrea-Clemencia Pineda-Peña, Randomized Controlled Trial of the Immunogenicity and Safety of a Serum-Free Purified Vero Rabies Vaccine (PVRV-NG2) Using a Simulated Postexposure Zagreb Regimen With Human Rabies Immunoglobulin in Adults in Thailand, Open Forum Infectious Diseases, 10.1093/ofid/ofae633, 11, 11, (2024).
- Pavle Banović, Dragana Mijatović, Verica Simin, Nenad Vranješ, Eleftherios Meletis, Polychronis Kostoulas, Dasiel Obregon, Alejandro Cabezas-Cruz, Real-world evidence of rabies post-exposure prophylaxis in Serbia: Nation-wide observational study (2017–2019), Travel Medicine and Infectious Disease, 10.1016/j.tmaid.2024.102697, 58, (102697), (2024).
- Ruiqi Lu, Jinsheng Lin, Yang Zhou, Qian Chen, Zaiying Fan, Shuning Wu, Pei Qin, Liping Li, Rabies vaccination adherence and associated factors among rabies-exposed patients in Shenzhen, China: a hospital-based cross-sectional study, Epidemiology and Infection, 10.1017/S0950268824000049, 152, (2024).
- Tianren Shen, Susan Christina Welburn, Long Sun, Guo-Jing Yang, Progress towards dog-mediated rabies elimination in PR China: a scoping review, Infectious Diseases of Poverty, 10.1186/s40249-023-01082-3, 12, 1, (2023).
- Kanika Gupta, Management of Animal Bite, Infections and Pregnancy, 10.1007/978-981-16-7865-3_31, (491-506), (2022).
- Shi-Yuan Wang, Jin-Fang Sun, Pei Liu, Li Luo, Jing-Xin Li, Feng-Cai Zhu, Xu-Xiang Shen, Fan-Yue Meng, Immunogenicity and safety of human diploid cell vaccine (HDCV) vs. purified Vero cell vaccine (PVRV) vs. purified chick embryo cell vaccine (PCECV) used in post-exposure prophylaxis: a systematic review and meta-analysis, Human Vaccines & Immunotherapeutics, 10.1080/21645515.2022.2027714, 18, 1, (2022).
- Tauseef Ahmad, undefined Haroon, Muhammad Khan, Manal Abdulaziz Murad, Mukhtiar Baig, Bibi Nazia Murtaza, Muhammad Mumtaz Khan, Harapan Harapan, Jin Hui, Research trends in rabies vaccine in the last three decades: a bibliometric analysis of global perspective, Human Vaccines & Immunotherapeutics, 10.1080/21645515.2021.1910000, 17, 9, (3169-3177), (2021).