Real-world evidence on clinical outcomes in immune thrombocytopenia treated with thrombopoietin receptor agonists
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Eltrombopag and romiplostim are US FDA approved for treatment of immune thrombocytopenia in patients with insufficient response to other treatments. Clinical or real-world data comparing outcomes of the two drugs are limited. Methods: This retrospective cross-sectional study sought information on bleeding-related episodes (BREs), adverse events (AEs) and other outcomes of eltrombopag or romiplostim treatment in immune thrombocytopenia. Results: Patients receiving eltrombopag experienced significantly reduced BREs, severe BREs, rescue medication use and platelet transfusions. Diarrhea and headache were significantly less frequent in patients receiving eltrombopag; other AEs occurred equally in both groups. Conclusion: There may be a potential advantage for the use of eltrombopag versus romiplostim in the practice settings studied, based on rates of BREs and AEs and rescue medication utilization.
Chronic immune thrombocytopenia (ITP) is an immune-mediated disease characterized by persistent low platelet counts that place patients at risk of uncontrolled bleeding [1]. The incidence of ITP in adults is between 16 and 39 cases per million adults per year, translating to 3900 to 9500 adults diagnosed with ITP in the USA each year [2,3]. The less severe symptoms of ITP include bruising, mucosal bleeding, petechiae and fatigue, all of which have an impact on health-related quality of life (HRQoL) [4,5]. More severe symptoms include serious bleeding-related episodes (BREs), such as gastrointestinal bleeding, intracranial hemorrhage (ICH) and intra- or post-operative hemorrhage, which are associated with morbidity, mortality and diminished HRQoL [4,6,7]. Patients with severe BREs may require whole blood transfusions and hospitalization, in addition to pharmacologic therapies, which can lead to substantial costs [8]. The risk of bleeding increases with age [9].
Population-based studies have found excess mortality in patients with ITP, with hazard ratios of death of 1.5 and 1.6 in two recent reports [10,11]; reasons include severe BREs, infection, cardiovascular disease and hematologic cancer [10–12]. Risk of ICH in ITP patients has been estimated at 1.5% for adults and 0.5% in children, and risk of severe (non-ICH) bleeding is estimated at 3–20% in children and approximately 10% in adults [9]. The risk of fatal hemorrhage has been estimated at 0.4% per year in patients <40 years, and 13% per year in patients >60 years [13].
The primary goal of ITP therapy is to lower the risk of bleeding or prevent recurrence. While bleeding risk is not strictly correlated with platelet count, and other variables (e.g., age, comorbidity, genetic factors) influence risk, practice guidelines from the American Society of Hematology recommend treatment initiation with first-line corticosteroids (longer courses preferred over shorter) with or without intravenous immune globulin (IVIG; depending on the desired rate of platelet increase), to prevent bleeding in patients with platelet count <30 × 109/l. However, it is also recognized that the risk of severe bleeding is much more substantial at platelet counts <10 × 109/l [14,15].
Newly diagnosed ITP patients receive corticosteroids and/or immunoglobulins, which are also used in chronic ITP to control emergent bleeding events [15]. Response to first-line corticosteroids can be variable, with initial response rates between 60 and 80%, but with relapses occurring after drug tapering in up to 80% of patients [16]. Prolonged treatment with corticosteroids is not advisable in many cases due to severe side effects [17]. First-line IVIG produces a rapid (1–3 days) response in 90% of patients, with response typically lasting for 2–4 weeks [15]. IVIG is usually considered a rescue treatment rather than therapy for patients with severe bleeding, as long-term IVIG is also inadvisable due to costs, inconvenience associated with infusions and debilitating headaches post infusion [16,18]. For patients with chronic ITP who do not respond to or tolerate first-line treatment, or who stop responding within 6 months, second-line treatment options include splenectomy, rituximab and thrombopoietin receptor agonists (TPO-RAs) [18]. Despite the potential for long-term remission with splenectomy, up to 20% of patients do not respond, and up to 20% will later relapse; risks include surgical complications, infections from long-term immunosuppression and thromboembolism [18–20]. Rituximab is an off-label option that depletes the B-cell pool, producing autoreactive antibodies that target platelets for destruction [21,22]. Eltrombopag and romiplostim are TPO-RAs that stimulate platelet production. Eltrombopag is a once-daily oral therapy, and romiplostim is subcutaneously injected [19,23]. In a recent US retrospective observational cohort study, in 2047 patients initiating second-line treatment between 2009 and 2016, rituximab was the most common treatment (72.7%), followed by splenectomy (12.7%), romiplostim (9.2%) and eltrombopag (5.4%) [24].
The end point to assess treatment effects in patients with ITP is often defined as a transient and/or sustained increase in platelet counts, while bleeding and quality of life have been assessed as secondary end points [9]. Thus, platelet counts may not capture the full burden of ITP for many patients who have reduced quality of life despite improvements in platelet count. Serious bleeding leading to hospitalization diminishes patients’ quality of life [4,25–27]. In the real-world practice setting, prevention or treatment of bleeding-related episodes (normal and severe), use of rescue medications, rates of AEs, quality of life, mortality and avoidance of other ITP agents are common factors included in clinical decision-making [9]. Despite growing use of these TPO-RAs, no large clinical studies have directly compared clinical outcomes with eltrombopag and romiplostim. A recently published meta-analysis of 13 randomized clinical trials (RCTs) analyzed data on any or severe bleeding events from ten of the included studies; pooled analysis of TPO-RAs indicated a significant reduction in incidence of any bleeding events compared with placebo [28]. Subgroup analysis indicated that eltrombopag, but not romiplostim, significantly reduced any or severe bleeding events compared with placebo [28]. To complement the meta-analysis approach with real-world evidence, here we provide data from US healthcare organizations (HCOs) that places into perspective clinical outcomes and risk of AEs associated with TPO-RA treatment of ITP.
Methods
Study setting & data
This study utilized a federated electronic health record (EHR) network of >39 million patients from 32 US HCOs (TriNetX), at the time the EHR network was accessed (3 April 2018). The HCOs contributing to the TriNetX data consisted at that time mostly of large academic health centers comprised main and satellite hospitals and outpatient clinics. TriNetX EHR data are aggregated results from de-identified patient records and can be queried in real time with an average of 5–6 years of retrospective data available from the time of query. The TriNetX EHR network provides information on patient demographics, International Classification of Diseases, Ninth Revision and Tenth Revision, Clinical Modification (ICD-9-CM; ICD-10-CM), procedure codes (ICD-9-CM, ICD-10-Procedure Coding systems, Current Procedural Terminology), medications, labs, oncology data, genomics and vital signs. Details on this network have previously been described [21,29]. When the network was accessed, the technology behind this approach had been primarily developed and used to facilitate real-time large-scale extraction of patient clinical data from HCO databases to help streamline enrollment in clinical trials. The technology and the various means used to ensure patient privacy using de-identified aggregated data thus allow access to patient characteristics and clinical features associated with different treatment groups, in this instance, patients with ITP who received either eltrombopag or romiplostim.
Design & study population
In this cross-sectional observational study, the inclusion and exclusion criteria were built into the data extraction parameters. Patients were included if they had any diagnosis code of ITP defined with an ICD-10-CM of D69.3, D69.4, D69.5 or D69.6 (Supplementary data) and were ≥18 years of age at the time of extraction (3 April 2018). Once adult ITP patients were identified, medication data were queried to identify ITP patients on eltrombopag or romiplostim. To ensure the eltrombopag and romiplostim patient groups were mutually exclusive (i.e., no patients counted in both treatment groups), we excluded romiplostim patients with any prior history of eltrombopag, and eltrombopag patients with any prior history of romiplostim from each treatment group. Therefore, patients in the eltrombopag group had no prior history of romiplostim use, and patients in the romiplostim group had no prior use of eltrombopag. In building an initial set of patients, age and gender were captured in the query search, as well as splenectomy and co-morbidities related to hepatitis virus B and C, HIV, severe aplastic anemia, myelodysplastic syndrome and myelofibrosis, among others. The initial patient characteristics from this set are listed in Table 1. Since this study used a real-time EHR network, we applied additional criteria to help mitigate the confounding factors arising from patient selection bias. Prevalence of acute hepatitis C with hepatic coma, prothrombin gene mutation, systemic lupus erythematosus, essential (hemorrhagic) thrombocythemia and myelodysplastic syndrome was significantly different (p < 0.01) between the two treatment groups (Table 1), Therefore, patients with these co-morbidities were excluded to prevent imbalance due to these characteristics. Patients with a history of rituximab treatment and those with ongoing (i.e., not rescue) corticosteroid treatment during the study period were excluded.
| Characteristic | Eltrombopag n = 1617 | Romiplostim n = 1140 | p-value |
|---|---|---|---|
| Age (mean ± SD) | 53 (23) | 56 (22) | 0.1196 |
| Gender (male %) | 49% | 51% | 0.3011 |
| Splenectomy | 67 (4) | 85 (7) | 0.0002† |
| Co-morbidities, n (%) | |||
| Acute hepatitis B without δ-agent with hepatic coma | 10 (1) | 10 (1) | 0.4305 |
| Acute hepatitis B without δ-agent and without hepatic coma | 21 (1) | 20 (2) | 0.3305 |
| Acute hepatitis C without mention of hepatic coma | 35 (2) | 21 (2) | 0.5546 |
| Acute hepatitis C with hepatic coma | 10 (1) | 0 (0) | 0.0079† |
| Chronic viral hepatitis C | 183 (11) | 112 (10) | 0.2120 |
| Unspecified viral hepatitis B without hepatic coma | 31 (2) | 30 (3) | 0.2093 |
| Unspecified viral hepatitis B with hepatic coma | 10 (1) | 10 (1) | 0.4305 |
| Unspecified viral hepatitis C without hepatic coma | 183 (11) | 102 (9) | 0.0443 |
| Prothrombin gene mutation | 31 (2) | 36 (3) | 0.0374† |
| Other primary thrombophilia | 60 (4) | 44 (4) | 0.8397 |
| Lupus anticoagulant syndrome | 37 (2) | 40 (4) | 0.0556 |
| Systemic lupus erythematosus | 41 (3) | 53 (5) | 0.0026† |
| Cachexia | 39 (2) | 27 (2) | 0.9414 |
| Essential (hemorrhagic) thrombocythemia | 59 (4) | 71 (6) | 0.0017† |
| Myelodysplastic syndrome | 283 (18) | 149 (13) | 0.0017† |
| Thrombotic microangiopathy | 26 (2) | 19 (2) | 0.9046 |
| Defibrination syndrome | 51 (3) | 44 (4) | 0.3173 |
| Acquired hemolytic anemias | 153 (9) | 105 (9) | 0.8234 |
| Hemolytic-uremic syndrome | 10 (1) | 10 (1) | 0.4305 |
| HIV disease | 17 (1) | 14 (1) | 0.6648 |
| Asymptomatic HIV infection status | 14 (1) | 10 (1) | 0.9747 |
| Malignant neoplasm of lymphatic and hematopoietic tissue | 83 (5) | 56 (5) | 0.7943 |
| Malignant neoplasm | 641 (40) | 487 (43) | 0.1057 |
| Malignant neoplasm of ill-defined, other secondary | 167 (10) | 134 (12) | 0.2370 |
| Malignant neoplasm of digestive organs | 88 (5) | 78 (7) | 0.1283 |
| Malignant neoplasm of breast | 46 (3) | 43 (4) | 0.1752 |
| Malignant neoplasm of lymphoid, hematopoietic and related tissue | 447 (28) | 298 (26) | 0.3815 |
| Malignant neoplasm of respiratory and intrathoracic organs | 30 (2) | 30 (3) | 0.1691 |
| Malignant neoplasm of male genital organs | 37 (2) | 35 (3) | 0.2050 |
| Malignant neoplasm of female genital organs | 26 (2) | 21 (2) | 0.6400 |
†
Patients with co-morbidities that were distributed significantly differently (p < 0.01) were excluded from further analysis.
SD: Standard deviation.
Prevalence of splenectomy was also significantly different between eltrombopag (4%) and romiplostim (7%; p = 0.0017) treatment groups; we did not, however, initially exclude these patients because splenectomy is a procedure indicated in some ITP patients. Instead, we conducted an exploratory analysis to determine the descriptive rates of splenectomy prior to treatment initiation with TPO-RAs, and rates following treatment initiation. There was a significant difference between patients who underwent splenectomy after eltrombopag initiation (2%) versus after romiplostim initiation (4%; p = 0.0039); these patients were further excluded from both the treatment groups to prevent imbalance due to splenectomy following TPO-RA treatment initiation. After applying this exclusion, the two treatment groups selected for further analysis were eltrombopag (n = 1281) and romiplostim (n = 930; Figure 1). The two patient groups were well balanced and not significantly different with respect to age, proportion of males and platelet volumes.

Figure 1. Patient flow.
EMR: Electronic medical record; EPAG: Eltrombopag; ITP: Immune thrombocytopenia; ROMI: Romiplostim.
Outcomes
Clinical outcomes related to benefit and risks were identified retrospectively in the TriNetX patient records within a 6-month period following treatment initiation with eltrombopag or romiplostim. While data were collected for a 6-month period from treatment initiation, the availability of 6 months of data was not a specific inclusion criterion, that is, if <6 months of data were available for a patient, then <6 months of data were used.
Treatment outcomes: rescue medications & BREs
Key treatment outcomes in ITP included use of rescue medications (intravenous immunoglobulin, corticosteroid injections or platelet transfusions) and occurrence of BREs. BREs were identified using ICD-10 diagnosis codes, and severe BREs were defined as having a BRE plus rescue medication use. The ICD-10 codes used to identify these outcomes are provided in Supplementary data.
Adverse events
AEs were defined from a list of ICD-10 diagnosis codes (Supplementary data). Relevant AEs were selected based on FDA prescribing information for eltrombopag and romiplostim, with input from clinical experts [30,31]. AEs included arthralgia, confusion, diarrhea, epistaxis, fatigue, headache, pain in extremities, petechiae and upper respiratory tract infection.
Statistical analysis
Incidence proportions of patient characteristics and outcomes were compared using unadjusted descriptive statistics; 95% CIs were compared for each outcome using two-tailed Z-tests with α of 0.05. Risk ratios were calculated using probabilities of observing a given event in each group: risk ratios = (probability with eltrombopag)/(probability with romiplostim). Probabilities were derived from incidence proportions of events in each group. Forest plots graphically display results obtained for each event measured in this study (Figures 2 & 3).
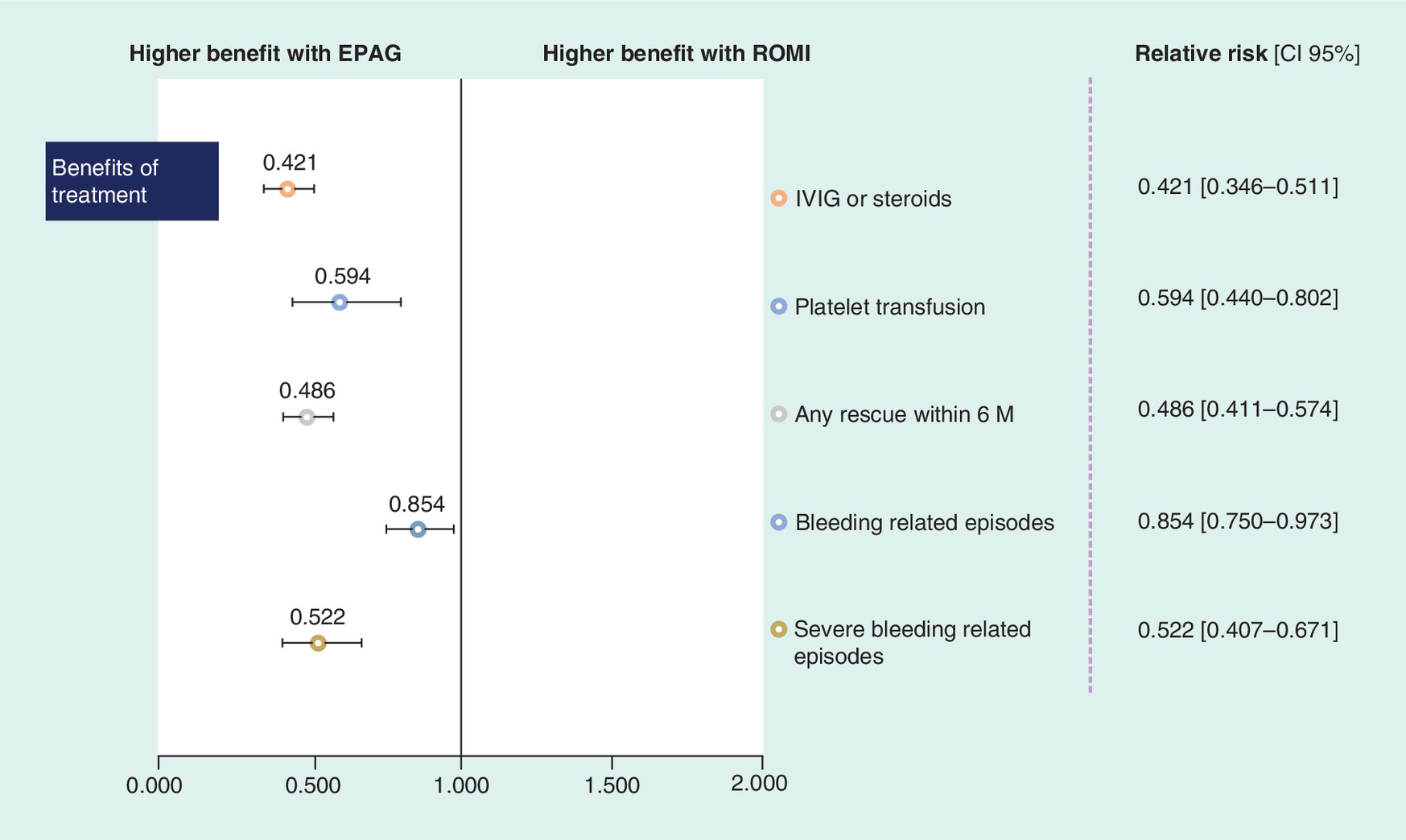
Figure 2. Forest plot comparing outcomes of treatment between eltrombopag and romiplostim.
EPAG: Eltrombopag; IVIG: Intravenous immune globulin; ROMI: Romiplostim.
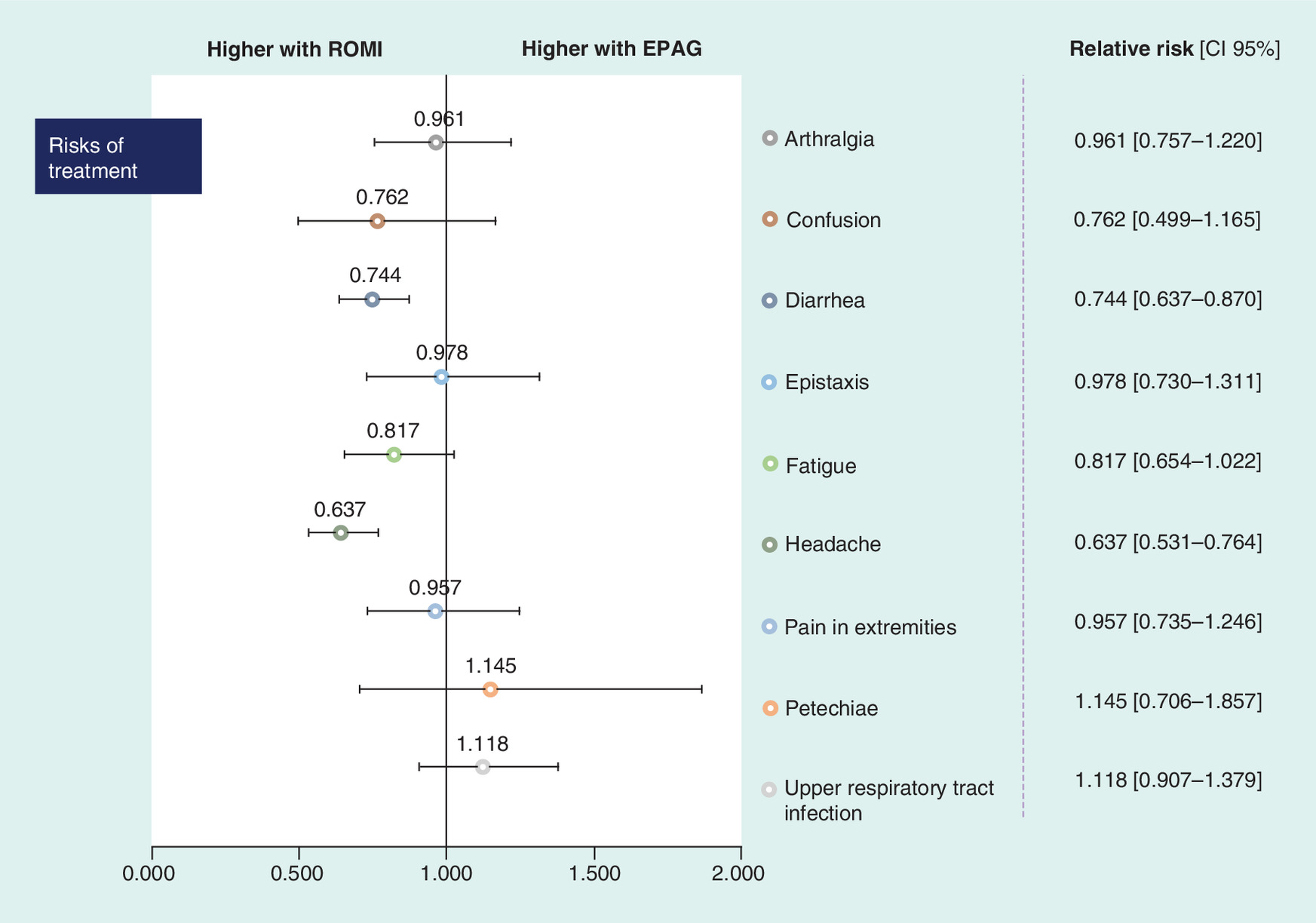
Figure 3. Forest plot comparing adverse events between eltrombopag and romiplostin.
EPAG: Eltrombopag; ROMI: Romiplostim.
Results
Of 671,909 patients (≥18 years) diagnosed with ITP in the EHR network on 3 April 2018, 1617 patients were on eltrombopag (with no prior romiplostim) and 1140 patients were on romiplostim (with no prior eltrombopag) (Table 1). The patient flow is displayed in Figure 1. To analyze patient outcomes from matched samples, we excluded patients with the following co-morbidities/characteristics as there were significant differences (p < 0.01) in prevalence between the two groups: acute hepatitis C, prothrombin gene mutation, systemic lupus erythematosus, essential (hemorrhagic) thrombocythemia, myelodysplastic syndrome and splenectomy post treatment. Following these exclusions, there were 1281 patients treated with eltrombopag and 930 patients treated with romiplostim available for analysis. Mean ages of patients included in the subsequent analysis of clinical outcomes and AEs were: eltrombopag, 50 years (standard deviation: 23) and romiplostim, 55 years (standard deviation: 23). There were 48% males in the eltrombopag group and 51% in the romiplostim group, and mean platelet volumes were 10.24 ± 1.94 fL (eltrombopag) and 10.43 ± 1.84 fL (romiplostim). Differences in distribution between the two groups for these three parameters were nonsignificant.
Treatment patterns & clinical outcomes
Significantly fewer eltrombopag patients received IVIG or corticosteroids compared with romiplostim patients within 6 months of treatment initiation (eltrombopag 11% vs romiplostim 25%; p < 0.0001; Table 2 & Figure 2).
| Clinical outcome | Eltrombopag n = 1281 | Romiplostim n = 930 | p-value |
|---|---|---|---|
| Treatment outcomes (n, %) | |||
| IVIG or corticosteroids | 135 (11) | 233 (25) | 0.0000† |
| Platelet transfusion | 72 (6) | 88 (9) | 0.0006† |
| Any rescue within 6 months | 182 (14) | 272 (29) | < 0.0001† |
| Bleeding-related episodes | 346 (27) | 294 (32) | 0.0186† |
| Severe bleeding-related episodes | 95 (7) | 132 (14) | 0.0000† |
| Selected adverse events (n, %) | |||
| Arthralgia | 139 (11) | 105 (11) | 0.7448 |
| Confusion | 42 (3) | 40 (4) | 0.2094 |
| Diarrhea | 247 (19) | 241 (26) | 0.0002† |
| Epistaxis | 97 (8) | 72 (8) | 0.8821 |
| Fatigue | 143 (11) | 127 (14) | 0.0774 |
| Headache | 179 (14) | 204 (22) | < 0.0001† |
| Pain in extremities | 116 (9) | 88 (9) | 0.7442 |
| Petechiae | 41 (3) | 26 (3) | 0.5836 |
| Upper respiratory tract infection | 191 (15) | 124 (13) | 0.2952 |
†
Statistically significant difference (p < 0.05).
IVIG: Intravenous immunoglobulin.
Platelet transfusions were also significantly lower in the eltrombopag group compared with romiplostim (eltrombopag 6% vs romiplostim 9%; p = 0.0006; Table 2 & Figure 2). Eltrombopag patients also experienced significantly fewer BREs (eltrombopag 27% vs romiplostim 32%; p = 0.0186) and fewer severe BREs (eltrombopag 7% vs romiplostim 14%; p < 0.0001; Table 2 & Figure 2). Risks were also evaluated within 6 months of treatment initiation, using selected AEs. Eltrombopag and romiplostim patients experienced similar rates of AEs, except for diarrhea and headache, which were significantly different in prevalence (Table 2 & Figure 3). Diarrhea was reported in 19% of eltrombopag-treated patients compared with 26% of romiplostim-treated patients (p = 0.0002), and headache was reported in 14% of eltrombopag-treated patients compared with 22% of romiplostim-treated patients (p < 0.0001; Table 2 & Figure 3).
Discussion
The use of TPO-RAs for treatment of ITP has expanded over the past decade and improved therapeutic options for patients in whom first-line treatment fails to provide clinical improvement, namely reductions in bleeding risk based on improved platelet counts [14,35]. The original indications for these treatments were limited to adult patients who had relapsed after splenectomy (and those in whom splenectomy was contraindicated) and those in whom first-line treatments were ineffective [36]. The RCT data that initially led to approval of both the treatments included patient populations in which 34–67% had previously undergone splenectomy [37–41]. One RCT included no splenectomized patients [42] and one RCT examined safety and efficacy of romiplostim versus placebo separately in splenectomized and nonsplenectomized patients [23]. Both eltrombopag and romiplostim are now FDA approved in the USA for ITP patients who have had an insufficient response to corticosteroids, immunoglobulins or splenectomy (i.e., patients who may or may not have had a splenectomy) [30,31]. These improved responses reported in clinical trials are known to translate into reduced bleeding and decreased necessity of providing concomitant or rescue medication [32,35].
We sought to quantify the responses – clinical outcomes and AEs – to TPO-RAs in a real-world setting utilizing de-identified aggregated patient data from a federated EHR network with access to multiple US HCOs. In this study of 2211 ITP patients, eltrombopag’s use was associated with subsequent significantly lower rates of BREs (including severe BREs), decreased use of rescue medications (including IVIG or corticosteroid injections) and platelet transfusions compared with romiplostim. We sought to avoid potential sources of bias that might affect our results; notably, the patient populations included here were mutually exclusive and comparable with respect to TPO-RA treatment. Patients on romiplostim at the time of data capture were excluded if they had previously been on eltrombopag, and vice-versa. Second, we assessed 20 co-morbidities for imbalances between the two patient groups. Five of these, acute hepatitis C with hepatic coma, prothrombin gene mutation, systemic lupus erythematosus, essential (hemorrhagic) thrombocythemia and myelodysplastic syndrome, had significantly different (p < 0.01) prevalence rates between the two treatment groups. Consequently, all patients with these co-morbidities were excluded. Third, although a minority of patients were reported to have undergone splenectomy, either before or after treatment initiation, we found that higher rates of patients treated with romiplostim subsequently underwent splenectomy (4%) compared with eltrombopag-treated patients (2%; p = 0.0039). To prevent bias, patients from both the groups were excluded if they underwent splenectomy following TPO-RA initiation. As for exclusion of patients who previously underwent splenectomy, this was considered not necessary, given the indications for both the treatments and given that the majority of clinical trials for TPO-RA enrolled patients both with and without prior splenectomy. Data from clinical trials are not uniformly consistent with respect to splenectomy prior to treatment. For example, multivariate analysis from one study that separately analyzed patients with and without splenectomy showed baseline weight <70 kg (p = 0.0106) and no splenectomy (p = 0.0306) were the only two variables significantly associated with increased rates of durable response [23]. In a separate study, previously splenectomized patients responded equally well to romiplostim compared with non-splenectomized patients [38].
The results presented here are comparable with a recently published meta-analysis of 13 RCTs that analyzed data on any or severe bleeding events from ten of the included studies. Pooled analysis of TPO-RAs indicated a significant reduction in incidence of any bleeding events compared with placebo [28]. Subgroup analysis indicated that eltrombopag, but not romiplostim, significantly reduced any or severe bleeding events compared with placebo [28].
In this real-world evidence study, we also captured data on selected nonbleeding AEs in both the patient groups. AEs, which are arthralgia, fatigue, headache and diarrhea, with >10% prevalence were the same in both the groups. In this study, the latter two AEs were present at a significantly lower rate in eltrombopag-treated patients compared with romiplostim. These AE results are in contrast with results obtained from a French Pharmacovigilance database indicating higher risk of gastrointestinal and hematologic AEs with romiplostim versus eltrombopag [50]. The reasons for differences in AE patterns between these two studies are not immediately clear but may involve a susceptibility to under-reporting in such databases, along with lower power to detect differences in AE signals between treatments [50].
While current US guidelines include TPO-RAs as appropriate second-line treatment options for ITP, it is recognized that not all patients will have a clinically meaningful response to TPO-RA treatment, and some patients discontinue TPO-RA because of the lack of response [15,43]. For example, in the EXTEND study of eltrombopag treatment, of the 302 patients enrolled, 14% withdrew from the study due to AEs, 13% due to patient decision, 11% due to lack of efficacy and 17% due to other reasons [44]. In one long-term romiplostim study, 8.5% of the 292 enrolled patients discontinued because of withdrawn consent, 3.8% due to AEs or alternative therapy, and 24% for other reasons [45].
In this respect, it is quite interesting that the recognized benefits of TPO-RAs have led to studies where switching from one to the other has proven beneficial following inadequate response to initial romiplostim or eltrombopag [46–49]. A retrospective pooled analysis of 18 switching studies (including 401 patients) estimated a relatively high response rate (improved platelet counts) of 65% when patients switched due to lack of efficacy with the first TPO-RA [49]. These differential effects of TPO-RAs in different patients demonstrating a lack of cross-resistance are consistent with known differences in activation of downstream signaling pathways between eltrombopag and romiplostim [35]. These studies raise the theoretical possibility that molecular and/or genetic markers may eventually be identified to personalize treatment decisions to select the most appropriate TPO-RA option for each patient.
Differential effects between TPO-RAs were also noted in a recent study that compared response rates (defined as platelet counts ≥50 × 109/l and ≥20 × 109/l higher than the pretreatment baseline) as a function of baseline TPO levels [51]. This retrospective chart review of patients on eltrombopag (n = 37) or romiplostim (n = 46) concluded that patients with normal (or lower) baseline TPO were equally likely to benefit from either TPO-RA, and those with moderate TPO levels were more likely to benefit from romiplostim than eltrombopag, whereas those with more substantial elevated baseline TPO were unlikely to respond to TPO-RA [51].
Improving platelet count is the most practical clinical end point in randomized trials, but the other key goal of treatment is to prevent bleeding, as this feature of ITP is the most worrisome for patients and clinicians [52,53], and associated costs for treatment of BREs are high. Factoring in fear of bleeding, fatigue, restriction in daily activities, altered immune responses and treatment-related side effects, there is the potential for diminished HRQoL in ITP patients [16]. Though our results did not include formal HRQoL assessments, our real-world findings suggest that patients may have fewer disruptions on eltrombopag compared with romiplostim, based on the potential reduction in platelet transfusions, fewer BREs and fewer severe BREs, along with lower rates of diarrhea and headache. Recent analyses directly link higher rates of BREs to increased healthcare resource use and elevated costs [33,34]. Reducing BREs is critical to the cost–effectiveness of ITP treatment [32].
In this respect, the type of real-world evidence presented in this study is directly relevant to potential cost savings and potential improved QoL attributable to TPO-RAs in general, and further research is warranted to investigate these issues in ITP patients on TPO-RA treatments.
Limitations
This study utilized a federated EHR network (TriNetX) incorporating data from various HCOs providing statistical results, that is, aggregated data and frequency calculations, on variables of interest. Without access to individual patient-level data, regression-aided matching of cohorts cannot be carried out, and patient characteristics cannot be identified with date or time. Regression is preferred when a researcher wants to make inferences about causal relationships and predictions (e.g., using the regression coefficients to predict how changes in the covariates affect the outcome of interest); therefore, this is an important limitation. The imbalances and potential confounding factors introduced by the nonrandomized nature of the study were thus not fully accounted for. However, we believe the methods employed in this analysis are reasonable for the goals of the analysis.
While our inclusion criteria used codes for primary ITP, and we excluded patients with codes for secondary ITP, we cannot exclude the possibility that some patients had ITP secondary to malignancy, infection or other conditions. The co-morbidities (Table 1) suggest that there was a fraction of patients receiving either of the drugs who had co-morbid malignancies or infections.
As romiplostim is administered as a weekly injection and eltrombopag is an oral suspension or tablet, the difference in therapeutic setting may have contributed to differences in documentation. This may especially be applicable to the AEs of diarrhea and headache as typical outpatient complaints; likewise, minor bleeding events that do not require additional follow-up may be more likely to be recorded for patients who have more frequent clinic visits. Unlike adjudicated or audited claims, data from EHR are subject to change as patients progress through episodes of care, and this process introduces an opportunity for error as new data and older conflicting data should ideally be reconciled. This cross-sectional method does not capture duration of disease, duration of therapy, or various other clinical details that may provide additional insights. This study examined events from treatment initiation and the ensuing 6 months, while perhaps a longer duration of follow-up would identify more clinical outcomes. However, since bleeding episodes are severe occurrences, these incidences are mostly captured in the hospital setting, suggesting that there may be minimal impact to the underestimation of these clinical outcomes.
Conclusion
This is the first direct (real-world evidence based) comparison of clinical outcomes and AEs in patients with ITP treated with eltrombopag or romiplostim that suggests there may be a potential advantage for the use of eltrombopag, based on lower rates of BREs (normal and severe), lower utilization of rescue medications and fewer AEs versus romiplostim in the practice settings studied. Further research is warranted in more patients, and in a variety of different settings to arrive at more definitive understanding of the real-world relative risks and benefits of the two TPOs.
•
Chronic immune thrombocytopenia is an immune-mediated disease characterized by persistent low platelet counts that place patients at risk of uncontrolled bleeding.
•
Eltrombopag is a US FDA-approved second-line treatment for immune thrombocytopenia.
•
A retrospective cross-sectional study was conducted to examine treatment outcomes and adverse events associated with eltrombopag or romiplostim treatment in immune thrombocytopenia patients.
•
In the practice settings studied using electronic health records, patients receiving eltrombopag experienced significantly lower instances of diarrhea and headache – and significantly reduced bleeding-related episodes, rescue medication use and platelet transfusions – compared with those receiving romiplostim.
•
Some studies have seen that switching between thrombopoietin receptor agonists after lack of response results in improved platelet counts.
•
More research is warranted into the relative risks and benefits of eltrombopag and romiplostim.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material. Some preliminary results from this study were presented at the American Society of Hematology 2017 Congress. The associated abstract is available at: http://www.bloodjournal.org/content/130/Suppl_1/3409?sso-checked=true
Author contributions
A Forsythe and A Roy made substantial contributions to study conception/design, data acquisition and critically revising the article for important intellectual content. CS Kwon, J Schneider and A Allepuz substantially contributed to data analyzed and critical article revision. T Pham, M Bhor, Q Said and MSO Portella were substantial contributors to study design and data analysis, as well as to the critical review of the article. All authors approved the final version to be published and agreed to be accountable for all aspects of the work.
Financial & competing interests disclosure
This study was conducted with support from Novartis. A Allepuz, T Pham, M Bhor, Q Said, MSO Portella and A Roy are employees of Novartis. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
The authors would like to acknowledge that this paper was written and edited with assistance from N Merritt and C Crotty of Purple Squirrel Economics, with support from Novartis.
Supplementary Material
File (supplementary data_cer-2019-0177.docx)
- Download
- 25.35 KB
References
1.
Rodeghiero F, Stasi R, Gernsheimer T et al. Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children: report from an international working group. Blood 113(11), 2386–2393 (2009).
2.
Altomare I, Cetin K, Wetten S, Wasser JS. Rate of bleeding-related episodes in adult patients with primary immune thrombocytopenia: a retrospective cohort study using a large administrative medical claims database in the US. Clin. Epidemiol. 8, 231–239 (2016).
3.
Terrell DR, Beebe LA, Vesely SK, Neas BR, Segal JB, George JN. The incidence of immune thrombocytopenic purpura in children and adults: a critical review of published reports. Am. J. Hematol. 85(3), 174–180 (2010).
4.
Mathias SD, Gao SK, Miller KL et al. Impact of chronic immune thrombocytopenic purpura (ITP) on health-related quality of life: a conceptual model starting with the patient perspective. Health Qual. Life Outcomes 6, 13 (2008).
5.
McMillan R, Bussel JB, George JN, Lalla D, Nichol JL. Self-reported health-related quality of life in adults with chronic immune thrombocytopenic purpura. Am. J. Hematol. 83(2), 150–154 (2008).
6.
McMillan R. Therapy for adults with refractory chronic immune thrombocytopenic purpura. Ann. Intern. Med. 126(4), 307–314 (1997).
7.
Lin J, Zhang X, Li X et al. Cost of bleeding-related episodes in adult patients with primary immune thrombocytopenia: a population-based retrospective cohort study of administrative claims data for commercial payers in the United States. Clin. Ther. 39(3), 603.e1–609.e1 (2017).
8.
Saleh MN, Fisher M, Grotzinger KM. Analysis of the impact and burden of illness of adult chronic ITP in the US. Curr. Med. Res. Opin. 25(12), 2961–2969 (2009).
9.
Arnold DM. Bleeding complications in immune thrombocytopenia. Hematology Am. Soc. Hematol. Educ. Program 2015, 237–242 (2015).
10.
Schoonen WM, Kucera G, Coalson J et al. Epidemiology of immune thrombocytopenic purpura in the General Practice Research Database. Br. J. Haematol. 145(2), 235–244 (2009).
11.
Frederiksen H, Maegbaek ML, Norgaard M. Twenty-year mortality of adult patients with primary immune thrombocytopenia: a Danish population-based cohort study. Br. J. Haematol. 166(2), 260v267 (2014).
12.
Portielje JE, Westendorp RG, Kluin-Nelemans HC, Brand A. Morbidity and mortality in adults with idiopathic thrombocytopenic purpura. Blood 97(9), 2549–2554 (2001).
13.
Cohen YC, Djulbegovic B, Shamai-Lubovitz O, Mozes B. The bleeding risk and natural history of idiopathic thrombocytopenic purpura in patients with persistent low platelet counts. Arch. Intern. Med. 160(11), 1630–1638 (2000).
14.
Lambert MP, Gernsheimer TB. Clinical updates in adult immune thrombocytopenia. Blood 129(21), 2829–2835 (2017).
15.
Neunert C, Terrell DR, Arnold DM et al. American Society of Hematology 2019 guidelines for immune thrombocytopenia. Blood Adv. 3(23), 3829–3866 (2019).
16.
Bohn JP, Steurer M. Current and evolving treatment strategies in adult immune thrombocytopenia. Memo 11(3), 241–246 (2018).
17.
Harris E, Tiganescu A, Tubeuf S, Mackie SL. The prediction and monitoring of toxicity associated with long-term systemic glucocorticoid therapy. Curr. Rheumatol. Rep. 17(6), 513 (2015).
18.
Cuker A. Transitioning patients with immune thrombocytopenia to second-line therapy: challenges and best practices. Am. J. Hematol. 93(6), 816–823 (2018).
19.
Cheng G, Saleh MN, Marcher C et al. Eltrombopag for management of chronic immune thrombocytopenia (RAISE): a 6-month, randomised, Phase III study. Lancet 377(9763), 393–402 (2011).
20.
Chaturvedi S, Arnold DM, McCrae KR. Splenectomy for immune thrombocytopenia: down but not out. Blood 131(11), 1172–1182 (2018).
21.
Stasi R, Cooper N, Del Poeta G et al. Analysis of regulatory T-cell changes in patients with idiopathic thrombocytopenic purpura receiving B cell-depleting therapy with rituximab. Blood 112(4), 1147–1150 (2008).
22.
Rituxan (Rituximab). Prescribing information. Genentech, Inc, CA, USA (2016).
23.
Kuter DJ, Bussel JB, Lyons RM et al. Efficacy of romiplostim in patients with chronic immune thrombocytopenic purpura: a double-blind randomised controlled trial. Lancet 371(9610), 395–403 (2008).
24.
Said Q, Lal LS, Nezami B. Evaluation of treatment outcomes after second-line treatment among patients with immune thrombocytopenia. Blood 132, P3765 (2018).
25.
Michel M. Immune thrombocytopenic purpura: epidemiology and implications for patients. Eur. J. Haematol. Suppl. 71, 3–7 (2009).
26.
Zhou Z, Yang L, Chen Z et al. Health-related quality of life measured by the Short Form 36 in immune thrombocytopenic purpura: a cross-sectional survey in China. Eur. J. Haematol. 78(6), 518–523 (2007).
27.
Provan D, Stasi R, Newland AC et al. International consensus report on the investigation and management of primary immune thrombocytopenia. Blood 115(2), 168–186 (2010).
28.
Wang L, Gao Z, Chen XP et al. Efficacy and safety of thrombopoietin receptor agonists in patients with primary immune thrombocytopenia: a systematic review and meta-analysis. Sci. Rep. 6, 39003 (2016).
29.
Stapff M. Use of electronic health data in clinical development. ECV Editio Cantor Verlag 79(2), 204–210 (2017).
30.
NPlate. Package insert. Amgen Inc, CA, USA.
31.
Promacta. Package Insert. Novartis Pharmaceuticals, NJ, USA.
32.
Tremblay G, Bhor M, Roy A et al. Cost-consequence model comparing eltrombopag and romiplostim for pediatric patients with previously-treated chronic immune thrombocytopenia. Blood 130(Suppl. 1), 2146–2146 (2017).
33.
Forsythe A, Bhor M, Roy A, Socorro O Portella M, Kwon C, Tremblay G. Economic burden of immune thrombocytopenia (ITP) in patients receiving eltrombopag (EPAG) and romiplostim (ROMI): real world evidence from 26 US institutions. Value Health 20(9), A552 (2017).
34.
Kwon C, Forsythe A, Roy A, Bhor M, Socorro O Portella M, Tremblay G. Health care resource use (HCRU) due to bleeding related episodes (BRE) in patients with immune thrombocytopenic purpura (ITP) receiving eltrombopag (EPAG), romiplostim (ROMI), or rituximab (RITUX): real world evidence (RWE) from 27 US institutions. Value Health 20(9), A558 (2017).
35.
Ghanima W, Cooper N, Rodeghiero F, Godeau B, Bussel JB. Thrombopoietin receptor agonists: ten years later. Haematologica 104(6), 1112–1123 (2019).
36.
Gonzalez-Porras JR, Bastida JM. Eltrombopag in immune thrombocytopenia: efficacy review and update on drug safety. Ther. Adv. Drug Saf. 9(6), 263–285 (2018).
37.
Bussel JB, Kuter DJ, George JN et al. AMG 531, a thrombopoiesis-stimulating protein, for chronic ITP. N. Engl. J. Med. 355(16), 1672–1681 (2006).
38.
Shirasugi Y, Ando K, Miyazaki K et al. Romiplostim for the treatment of chronic immune thrombocytopenia in adult Japanese patients: a double-blind, randomized Phase III clinical trial. Int. J. Hematol. 94(1), 71–80 (2011).
39.
Bussel JB, Provan D, Shamsi T et al. Effect of eltrombopag on platelet counts and bleeding during treatment of chronic idiopathic thrombocytopenic purpura: a randomised, double-blind, placebo-controlled trial. Lancet 373, 641–648 (2009).
40.
Bussel JB, Cheng G, Saleh MN et al. Eltrombopag for the treatment of chronic idiopathic thrombocytopenic purpura. N. Engl. J. Med. 357, 2237–2247 (2007).
41.
Tomiyama Y, Miyakawa Y, Okamoto S et al. A lower starting dose of eltrombopag is efficacious in Japanese patients with previously treated chronic immune thrombocytopenia. J. Thromb. Haemost. 10, 799–806 (2012).
42.
Kuter DJ, Rummel M, Boccia R et al. Romiplostim or standard of care in patients with immune thrombocytopenia. N. Engl. J. Med. 363(20), 1889–1899 (2010).
43.
Bussel JB, Kuter DJ, Pullarkat V, Lyons RM, Guo M, Nichol JL. Safety and efficacy of long-term treatment with romiplostim in thrombocytopenic patients with chronic ITP. Blood 113(10), 2161–2171 (2009).
44.
Wong RSM, Saleh MN, Khelif A et al. Safety and efficacy of long-term treatment of chronic/persistent ITP with eltrombopag: final results of the EXTEND study. Blood 130(23), 2527–2536 (2017).
45.
Kuter DJ, Bussel JB, Newland A et al. Long-term treatment with romiplostim in patients with chronic immune thrombocytopenia: safety and efficacy. Br. J. Haematol. 161(3), 411–423 (2013).
46.
Kuter DJ, Macahilig C, Grotzinger KM et al. Treatment patterns and clinical outcomes in patients with chronic immune thrombocytopenia (ITP) switched to eltrombopag or romiplostim. Int. J. Hematol. 101(3), 255–263 (2015).
47.
Khellaf M, Viallard JF, Hamidou M et al. A retrospective pilot evaluation of switching thrombopoietic receptor-agonists in immune thrombocytopenia. Haematologica 98(6), 881–887 (2013).
48.
Cantoni S, Carpenedo M, Mazzucconi MG et al. Alternate use of thrombopoietin receptor agonists in adult primary immune thrombocytopenia patients: a retrospective collaborative survey from Italian hematology centers. Am. J. Hematol. 93(1), 58–64 (2018).
49.
González-Porras JR, Godeau B, Carpenedo M. Switching thrombopoietin receptor agonist treatments in patients with primary immune thrombocytopenia. Ther. Adv. Hematol. 10, 20406207198379062019 (2019).
50.
Moulis G, Bagheri H, Sailler L et al. Are adverse drug reaction patterns different between romiplostim and eltrombopag? 2009–2013 French PharmacoVigilance assessment. Eur. J. Intern. Med. 25(8), 777–780 (2014).
51.
Al-Samkari H, Kuter DJ. Thrombopoietin level predicts response to treatment with eltrombopag and romiplostim in immune thrombocytopenia. Am. J. Hematol. 93(12), 1501–1508 (2018).
52.
Arnold DM. Platelet count or bleeding as the outcome in ITP trials? Am. J. Hematol. 87(10), 945–946 (2012).
53.
Trotter P, Hill QA. Immune thrombocytopenia: improving quality of life and patient outcomes. Patient Relat. Outcome Meas. 9, 369–384 (2018).
Information & Authors
Information
Published In
Pages: 447 - 457
PubMed: 32175766
Copyright
© 2020 Future Medicine Ltd.
History
Received: 22 November 2019
Accepted: 11 February 2020
Published online: 16 March 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Real-world evidence on clinical outcomes in immune thrombocytopenia treated with thrombopoietin receptor agonists. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0177
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Serhat Çelik, Zeynep Tuğba Karabulut, Cem Selim, Rafiye Çiftçiler, Abdulkerim Yıldız, Samet Yaman, İbrahim Ethem Pınar, Ayşe Hilal Eroğlu Küçükdiler, Nuray Gül Açar, Aysun Şentürk Yıkılmaz, Vehbi Demircan, Dilek Keskin, İbrahim Halil Açar, Ekin Kırcalı, Meltem Kurt Yüksel, Original Versus Generic Eltrombopag in Patients with Immune Thrombocytopenia: A Prospective Multi-Center Experience on Efficacy and Safety, Journal of Clinical Medicine, 10.3390/jcm15020634, 15, 2, (634), (2026).
- Jaap Zwaginga, Srikanth Nagalla, Marie Linden, Marjo Lindberg, Caroline Kruse, Mervyn Morgan, Cecilie Yssing, Donatella Decise, Milica Putnik, Carly Rich, Impact of Primary Chronic Immune Thrombocytopenia and Thrombopoietin Receptor Agonists Treatment Instructions on Daily Living: Results of a Multinational Cross-Sectional Survey, Patient Preference and Adherence, 10.2147/PPA.S505337, Volume 19, (2445-2458), (2025).
- S. G. Zakharov, Immune thrombocytopenia: literature review, Oncohematology, 10.17650/1818-8346-2024-19-3-34-44, 19, 3, (34-44), (2024).
- Yi Liang, Karen Rascati, Jamie C. Barner, Kenneth A. Lawson, Radhika Nair, Treatment patterns and outcomes among adults with immune thrombocytopenia receiving pharmaceutical second-line therapies: a retrospective cohort study using administrative claims data, Current Medical Research and Opinion, 10.1080/03007995.2024.2328653, 40, 5, (781-788), (2024).
- O. Yu. Vinogradova, M. M. Pankrashkina, Anna Leonidovna Neverova, M. V. Chernikov, L. A. Mukha, D. I. Shikhbabaeva, V. V. Ptushkin, Primary Immune Thrombocytopenia and Thrombopoietin Receptor Agonists: Feasibilities of Treatment Discontinuation upon Achieving Stable Complete Platelet Response, Clinical Oncohematology, 10.21320/2500-2139-2023-16-4-413-425, 16, 4, (413-425), (2024).
- T. I. Ionova, O. Yu. Vinogradova, T. V. Shelekhova, D. G. Sherstnev, A. V. Proidakov, E. V. Lyyurova, M. M. Pankrashkina, L. A. Mukha, E. E. Markova, N. V. Novitskaya, T. I. Pospelova, T. N. Babaeva, N. B. Bulieva, G. B. Kuchma, E. A. Andreevskaya, E. E. Zinina, M. V. Frolova, K. B. Trizna, I. L. Shestopalova, T. V. Shneider, S. A. Volkova, S. G. Zakharov, I. I. Mulina, I. E. Solov’eva, A. A. Myasnikov, A. A. Kuchin, L. B. Khvorostenko, N. M. Porfirieva, Tatyana Pavlovna Nikitina, V. V. Ptushkin, S. V. Gritsaev, Quality of Life Changes in Patients with Chronic Immune Thrombocytopenia in the Process of Romiplostim Therapy, its Efficacy and Safety in the Real-World Setting: Results of a Multi-Center Observational Study, Clinical Oncohematology, 10.21320/2500-2139-2023-16-2-154-165, 16, 2, (154-165), (2024).
- Raymond Siu Ming Wong, İrfan Yavaşoğlu, Mohamed A. Yassin, Pınar Tarkun, Sung-Soo Yoon, Xie Wei, Ashraf Elghandour, Pantep Angchaisuksiri, Mehmet Ozcan, Renchi Yang, Mervat Mattar, Masiur Rahman, Sara Ingles, Michael Goldbrunner, Jennifer A. Frueh, Jun Ho Jang, Eltrombopag in patients with chronic immune thrombocytopenia in Asia-Pacific, the Middle East, and Turkey: final analysis of CITE, Blood Advances, 10.1182/bloodadvances.2022008287, 7, 17, (4773-4781), (2023).
- Ji Yun Lee, Ju-Hyun Lee, Sang-A Kim, Koung Jin Suh, Ji-Won Kim, Se Hyun Kim, Jeong-Ok Lee, Jin Won Kim, Yu Jung Kim, Keun-Wook Lee, Jee Hyun Kim, Jong Seok Lee, Soo-Mee Bang, Treatment patterns of thrombopoietin receptor agonists among adults with primary immune thrombocytopenia: A Korean nationwide population-based study, Thrombosis Research, 10.1016/j.thromres.2022.03.015, 213, (114-118), (2022).
- Michael Fillitz, Barbara Dixer, Felix Keil, Practical considerations for the management of immune thrombocytopenic purpura, memo - Magazine of European Medical Oncology, 10.1007/s12254-021-00771-9, 14, 4, (350-354), (2021).
- Hafiz Abdul Waqas Ahmed, Ahmed Taher Masoud, Jia Han, Ahmed Adel Sofy, Ahmed Saeed Ahmed, Ahmed Taha Abdesattart, Emmanuel Kwateng Drokow, Kai Sun, Eltrombopag Effectiveness and Tolerability in Chronic Immune Thrombocytopenia: A Meta-Analysis, Clinical and Applied Thrombosis/Hemostasis, 10.1177/10760296211005555, 27, (2021).