Disease burden of schizophrenia patients visiting a Chinese regional mental health centre
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim & methods: A decision-analytic model was constructed to simulate a real-world cohort of Chinese patients visiting a Chinese regional mental health center for long-term health outcomes and direct medical costs. Results: When compared with age and gender-matched general population, the Chinese patients with schizophrenia were associated with reduced overall survival by 20.6 years (27.6 vs 48.2 years) and reduced quality-adjusted life years (QALY) by 18.4 QALY (18.4 vs 36.8 QALY), respectively, and increased lifetime direct medical costs by about three-times (US$84,324 vs 33,387 as of 31 December 2017) on average. Conclusion: The burden of schizophrenia was mainly driven by the mortality associated with relapsed schizophrenia and direct medical costs for schizophrenia in local mental health rehabilitation institutes.
Schizophrenia is a chronic mental disorder characterized by abnormal behaviors and confusion with reality. Schizophrenia affects approximately 0.3–0.7% of the global population and it is one of the leading causes of years lived with disability worldwide [1,2]. The manifestations of schizophrenia include positive symptoms, which are characterized by hallucinations and delusions and negative symptoms characterized by diminished emotional expression, lack of motivation and cognitive symptoms related to working memory and executive functions [1,3].
The latest epidemiological studies reported that the lifetime prevalence of schizophrenia in China increased from 0.39% in 1990 to 0.83% in 2010 [4]. Because schizophrenia disables patients, increase suicides and causes violence, the burden of schizophrenia on patients, families and societies is substantial. According to WHO’s estimation, schizophrenia is the leading contributor to the disease burden of psychiatric diseases, which will account for 15% of the overall healthcare expenditure in China [5].
The impact of schizophrenia on survival [6], quality of life [7] and costs [8] have been well studied. However, the disease burden of schizophrenia in Chinese patients over the entire life has remained unclarified and has not yet been quantified. There are many strategies that have been proven to be effective in controlling the disease burden of schizophrenia. These strategies include increasing the number of psychiatrists to closely manage patients [9], providing free drugs to improve patient access to treatment [10] and using community treatment order for better treatment compliance [11]. The current strategies for schizophrenia control in China have mainly focused on improving patient access to antipsychotic treatments [12], which have been proven effective in reducing the symptoms and functional impairment of schizophrenia [13]. Antipsychotic treatments are usually classified by treatment administration route (oral medications vs long-action injectable [LAI] formulations) due to its impact on treatment compliance [14], the key factor affecting treatment outcomes in schizophrenia patients [15]. There is well documented international evidence regarding the superiority of LAI treatment over oral antipsychotic treatments for treatment compliance and international practice guidelines have encouraged the use of LAI formulations for schizophrenia in routine clinical practices if the patients failed or did not comply to oral antipsychotics [16]. It has been over 5 years since the launch of the first LAI formulation, paliperidone palmitate injection, in China in 2012. However, the impact of introducing LAI formulations on the treatment landscape and the disease burden of schizophrenia in China has not yet been clarified.
Materials & methods
This study constructed a decision-analytic model to estimate the disease burden of schizophrenia by comparing the simulated health outcomes and direct medical costs associated with a created clinical cohort of Chinese patients with schizophrenia from a Chinese regional mental health center and the age and gender-matched Chinese general population. The Chinese healthcare system for mental diseases usually consists one regional mental health center in provincial capital city to provide tertiary care to schizophrenia patients at varied disease stages and community mental health rehabilitation institutes in the lower level cities and towns in the province for patients with relapsed disease. The created clinical cohort with schizophrenia from the regional mental health center in Hunan province was used to conduct a retrospective cohort study, which was used to develop the disease analytic model for the disease burden of schizophrenia. This regional mental health center provides tertiary care for schizophrenia patients with varied disease stages across Hunan province, which has over 60 million residents. A literature review and telephone interview of the relevant experts were conducted to estimate the model variables that could not be derived from the retrospective cohort study. The constructed decision-analytic model was used to perform base-case analysis and sensitivity analyses for the point estimations and uncertainty of the disease burden of schizophrenia, which was estimated using the differences in the simulated life years, quality-adjusted life years (QALY) and direct medical costs over lifetime between the created clinical cohort of schizophrenia patients and the age and gender-matched Chinese general population. The cost perspective in this study was healthcare payers. All costs in this study were converted to US dollars according to the currency exchange rate on 31 December 2017 (¥1 = US$0.15). This study was reviewed and approved by the ethics board of the Second Xiangya Hospital where the retrospective cohort study was conducted.
Model structure
The decision-analytic model was constructed to simulate two model cohorts: the schizophrenia cohort with patients admitted to a Chinese tertiary care hospital for active schizophrenia versus a hypothetical model cohort with age and gender-matched general Chinese population. According to the interview with Chinese psychiatrists, the newly diagnosed schizophrenia patients were mainly managed in a tertiary care hospital for the first two treatment relapses. Refractory schizophrenia, defined as three or more treatment relapses, was usually managed in local mental health rehabilitation institutes [17]. Thus, the decision-analytic model used two Markov models to simulate the management of these treatment relapses schizophrenia in the two settings. The Markov model simulating the management of treatment relapses in tertiary care hospital setting included health states for disease remission, disease relapse and death under the antipsychotic treatment pattern in the identified patients from the tertiary care hospital. The Markov model used two health states (i.e., refractory schizophrenia and death) to simulate the management of refractory schizophrenia in local mental health rehabilitation institutes. The Markov model used two health states, alive and dead, to simulate the model control cohort for age and gender-matched general Chinese population using reported lifetable [18], quality of life [19] and annual direct medical costs [20] in the Chinese general population. The cycle length of the created Markov models was set as a quarter, the time interval often used for regular follow-up schedule. The time horizon of the decision-analytic model was set to lifetime to estimate overall disease burden. To assess the external validity of the model outputs, the decision-analytic model did not discount the health outcomes and direct medical costs. The structure of the decision-analytic model measuring the disease burden of schizophrenia in China is illustrated in Figure 1.

Figure 1. The structure of the decision-analytic model estimating the disease burden of schizophrenia.
LAI: Long-action injectable.
Estimating model variables from the retrospective cohort study
This study conducted a retrospective cohort study in a tertiary care hospital that provided tertiary care for schizophrenia patients living in Hunan province, which is located in south-central China and has a population of 68.6 million [8]. This retrospective cohort study identified the patients who were hospitalized for schizophrenia from 1 January 2013 to 31 December 2017. The medical and billing records associated with the identified patients during the observation time were extracted to estimate model variables for patient demographics, antipsychotic treatment pattern, health resources utilization and direct medical costs in this hospital. To differentiate the impact of oral antipsychotic medications and LAI treatment on health resources utilization and direct medical costs, the included patients were stratified by the antipsychotic treatment administration route (oral vs LAI) to compare the health resources utilization and direct medical costs using regression analyses after adjusting for the collected patient baseline characteristics. The conducted regression analyses included logistic regression analysis for the treatment administration route, Poisson regression analysis for outpatient visits and hospital admissions, linear regression analysis for hospital stay length and generalized linear regression analysis with gamma distribution assumption for direct medical costs.
Estimating model variables from the literature review & telephone interview
To address the evidence needs in the development of the decision-analytic model, a literature review was conducted to identify published evidence for the risk of treatment relapse associated with identified antipsychotic treatments in the retrospective cohort study and hazard ratio of mortality associated with schizophrenia status (remission and relapse). A meta-analysis approach was used to synthesize the identified evidence for the point estimation and its 95% CI. This study also conducted a literature review to estimate the positive and negative syndrome scale psychopathology subscore (PANSS_PSY) associated with two schizophrenia statuses (remission and relapse) in Chinese patients. The pooled estimations of PANSS_PSY associated with the two schizophrenia statuses were applied to a developed utility prediction formula (QOL = 1.026055 - 0.0076876*PANSS_PSY + 0.0457537*sex - 0.0020646*age) [21], respectively, to estimate the quality of life in the decision-analytic model. The model variables for age and gender-adjusted annual mortality, quality of life and annual direct medical costs in the Chinese general population were taken from the literature. Additionally, a telephone interview was conducted in the three levels of local mental health rehabilitation institutes (provincial capital city, regional city and county) in Hunan province to obtain the estimation of direct medical costs associated with refractory schizophrenia in the community. The estimated model variables from the literature review and telephone interview are summarized in Table 1.
| Model variable | Baseline value | 95% CI | Data source | Number of included studies | Number of included patients | |
|---|---|---|---|---|---|---|
| Lower limit | Upper limit | |||||
| Quarterly risk of disease relapse | ||||||
| Paliperidone palmitate injection | 3.1% | 2.3% | 4.2% | Literature | 10 | 1545 |
| Oral antipsychotic medications | 9.4% | 4.5% | 14.3% | Literature | 52 | 3725 |
| Hazard ratio of mortality schizophrenia patients vs the Chinese general population | ||||||
| Disease remission | 3.301 | 2.476 | 6.133 | Literature | 2 | 141,395 |
| Relapsed disease | 7.719 | 3.087 | 9.529 | Literature | 4 | 10,655 |
| Utility ratio of schizophrenia patients relative to the Chinese general population | ||||||
| Disease remission | 0.904 | 0.902 | 0.906 | Literature | 65 | 4698 |
| Relapsed disease | 0.805 | 0.804 | 0.807 | Literature | 96 | 7317 |
| Quarterly medical costs associated with mental health rehabilitation institute | ||||||
| Provincial capital city | US$1395 | Telephone interview | ||||
| Regional city | US$1102 | Telephone interview | ||||
| County | US$638 | Telephone interview | ||||
Measuring disease burden of schizophrenia
The constructed decision-analytic model for the disease burden of schizophrenia was used to conduct a base-case analysis, one-way sensitivity analysis and probabilistic sensitivity analysis (PSA) regarding the outcome measures, which were presented as the differences in estimated average life years, QALY and lifetime direct medical costs between the included schizophrenia patients and the age and gender-matched general Chinese population. The base-case analysis was conducted using the baseline values of the model variables. The distributions of the estimated lifetime direct medical costs associated schizophrenia patients by care settings, including tertiary care hospital and three levels of local mental health rehabilitation institutes, were calculated to demonstrate the allocation of direct medical costs associated with the Chinese schizophrenia patients. One-way sensitivity analyses were conducted to assess the uncertainty associated with each model variable on the measured outcomes for the disease burden of schizophrenia by varying each model variable within its 95% CI or ±25% of its baseline values if its 95% CI was lacking. PSA was conducted by assessing the impact of overall uncertainty associated with model variables on the disease burden of schizophrenia according to 10,000 Monte Carlo simulations under the distributions of model variables, which included beta distribution for probability and utility variables and the gamma distribution for cost variables and the other variables with a range crossing 1. The generated estimations of the outcome measures from the Monte Carlo simulations were plotted to identify their median and 95% credible intervals. The decision-analytic model for schizophrenia in China was constructed in 2013 Microsoft Excel to perform the base-case analysis, one-way sensitivity analysis and PSA.
Results
This study first reported the patient characteristics, treatment pattern, health resources utilization and direct medical costs from the included schizophrenia in the retrospective cohort study. The results of the base-case analysis, one-way sensitivity analyses and PSA in the developed schizophrenia disease burden model were reported subsequently.
Creating a clinical cohort of schizophrenia patients
The retrospective cohort study identified 4637 patients hospitalized for schizophrenia from 1 January 2013 to 31 December 2017. According to the inclusion and exclusion criteria, 3296 patients were included to conduct the retrospective cohort study. To be consistent with the model simulations under the antipsychotic treatments classified by their administration route, this study stratified the included patients by the administration routes (oral group vs LAI group) to generate the following evidence that was needed to develop the decision-analytic model for the measurement of the disease burden of schizophrenia in China.
Patient characteristics of the included schizophrenia patients
The included patients in the LAI group and the oral group were characterized with relatively young age (mean ± standard deviation: 31.1 ± 10.3 vs 31.1 ± 11.3 years; p = 0.989) and evenly distributed gender (male proportion: 53.7 vs 52.9%; p = 0.873). The two groups also had a comparable and high unemployment rate (61.0 vs 62.5%; p = 0.741). However, the LAI group was associated with significantly higher proportions of residence in the provincial capital city (25.0 vs 15.3%; p = 0.002) and participation in the urban worker insurance plan (23.2 vs 14.6%; p = 0.005). Additionally, the LAI group was likely to have a better health status than the oral group by having a significantly high proportion of patients with normal total protein (68.2 vs 55.2%) but a significantly lower proportions of patients with comorbidities for mental and behavior disorders (9.1 vs 15.7%; p = 0.026) and never diseases (0 vs 3.0%; p = 0.014). The patient characteristics of the two groups are summarized in Table 2.
| Patient group | LAI group | Oral treatment group | p-value | ||
|---|---|---|---|---|---|
| Sample size | 164 | 3132 | |||
| Variable | Mean/% | SD | Mean/% | SD | |
| Demographics | |||||
| Age (years) | 31.1 | 10.3 | 31.1 | 11.3 | 0.989 |
| Male gender | 53.70% | 52.90% | 0.873 | ||
| Employment status | |||||
| Full-time | 20.70% | 18.00% | 0.406 | ||
| Farmer | 4.90% | 7.10% | 0.346 | ||
| Unemployment | 61.00% | 62.50% | 0.741 | ||
| Retired | 2.40% | 2.30% | 0.79 | ||
| Student | 7.90% | 6.60% | 0.519 | ||
| Unknown | 3.00% | 3.50% | 1 | ||
| Residence | |||||
| County | 53.70% | 66.70% | 0.001 | ||
| Regional city | 20.70% | 15.60% | 0.099 | ||
| Provincial capital city | 25.00% | 15.30% | 0.002 | ||
| Insurance plan | |||||
| Urban workers | 23.20% | 14.60% | 0.005 | ||
| Urban residents | 15.90% | 7.50% | <0.001 | ||
| New-cooperation rural residents | 16.50% | 25.80% | 0.007 | ||
| Unclarified | 44.50% | 52.10% | 0.065 | ||
| Laboratory tests | |||||
| Normalization of total protein | 68.20% | 55.20% | 0.008 | ||
| Comorbidities | |||||
| Mental and behavior disorders | 9.10% | 15.70% | 0.026 | ||
| Neurological diseases | 0.00% | 3.00% | 0.014 | ||
Bold values indicate statistical significance.
LAI: Long-action injectable; SD: Standard deviation.
Antipsychotic treatments in the included schizophrenia patients
Among the identified oral antipsychotic medications, olanzapine and risperidone were prescribed for 35.5 and 22.4% of the included patients, respectively. The other prescribed oral antipsychotic medications included clozapine (10.8%), aripiprazole (6.1%), paliperidone (4.7%), amisulpride (4.6%), sulpiride (4.6%) and quetiapine (4.6%). A total of 5.0% of the included patients received LAI treatment, which was paliperidone palmitate injection. The mean treatment durations of LAI and oral antipsychotics were 8.1 and 12.3 months, respectively. Multiple logistic regression analysis with adjustment of the collected patient characteristics indicated that the prescription of LAI was independently and significantly associated with participation in the urban workers insurance plan (odds ratio [OR]: 1.742; p = 0.034), urban residents insurance plan (OR: 2.873; p < 0.001) and normal total protein (OR: 1.779; p = 0.006).
Direct medical costs associated with the included schizophrenia patients in the tertiary care hospital
Unadjusted comparisons of annual health resources utilization associated with the oral group and LAI group during the observation time identified significantly higher annual outpatient visits (median 9.4 vs 7.8; p = 0.025) but significantly fewer annual hospital admissions (median 1.4 vs 3.7; p < 0.001) and shorter annual hospital stay length (median 38.4 vs 82.0 days; p < 0.001) in the patients receiving LAI treatment. Additionally, the LAI group was associated with significantly lower annual medical costs (median: US$4964 vs 8145; p = 0.018) than the oral group because of significantly lower annual hospital costs associated with LAI (median: US$2997 vs 6822; p < 0.001). The health resources utilization and direct medical costs in the tertiary care hospital are summarized in Table 3. Multiple linear regression analysis with the adjustment for unbalanced patient characteristics confirmed that LAI was significantly associated with more annual outpatient visits (coefficient: 0.424; p < 0.001), lower annual hospital admissions (coefficient: -0.742, p < 0.001) and shorter hospital stay length (coefficient: -74.058; p < 0.001). The multiple generalized linear regression analysis indicated that the annual total medical costs associated with the two groups were highly comparable (coefficient: 0.002; p = 0.991).
| Patient group | LAI group | Oral treatment group | p-value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sample size | 164 | 3132 | |||||||||
| Variables | Mean | SD | Median | Q1 | Q3 | Mean | SD | Median | Q1 | Q3 | |
| Annual health resources utilization | |||||||||||
| Hospital admissions | 4.7 | 7.0 | 1.4 | 0.6 | 5.8 | 9.7 | 18.1 | 3.7 | 0.9 | 13.3 | <0.001 |
| Hospital stay days | 101.8 | 124.0 | 38.4 | 15.1 | 129.1 | 157.2 | 151.3 | 82.0 | 18.2 | 360.0 | <0.001 |
| Outpatient visits | 12.0 | 13.1 | 9.4 | 4.7 | 14.9 | 11.7 | 18.3 | 7.8 | 3.8 | 14.4 | 0.025 |
| Average medical costs/episode or visit | |||||||||||
| Hospitalization | US$2085 | US$1257 | US$1853 | US$1307 | US$2533 | US$2064 | US$2920 | US$1586 | US$1201 | US$2300 | 0.014 |
| Outpatient visit | US$218 | US$167 | US$197 | US$105 | US$281 | US$115 | US$115 | US$89 | US$29 | US$165 | <0.001 |
| Annual Medical costs | |||||||||||
| Hospitalization | US$8061 | US$10,591 | US$2997 | US$1145 | $11,428 | $16,698 | US$37,501 | US$6822 | US$1445 | US$22,666 | <0.001 |
| Outpatient visit | US$2487 | US$3207 | US$1669 | US$823 | US$3130 | US$1265 | US$2329 | US$788 | US$214 | US$1637 | <0.001 |
| Total | US$10,548 | US$11,897 | US$4964 | US$2696 | US$14,790 | US$17,962 | US$37,706 | US$8145 | US$2486 | US$24,071 | 0.018 |
Bold values indicate statistical significance.
LAI: Long-action injectable; SD: Standard deviation.
Disease burden of schizophrenia: base-case analysis
The included schizophrenia patients were associated with reduced survival by 20.6 years (27.6 vs 48.2 years) and reduced QALY by 18.4 QALY (18.4 vs 36.8 QALY) when compared with the model control cohort with age and gender-matched general Chinese population in the base-case analysis. Additionally, the average lifetime direct medical costs associated with the included schizophrenia patients were more than two-times of the lifetime medical costs associated with the model control cohort (US$84,324 vs 33,387). Further analysis of the distribution of the lifetime direct medical costs associated with schizophrenia patients indicated that 81% of the lifetime medical costs associated with schizophrenia patients were spent in the local mental health rehabilitation institutes. The county mental health rehabilitation institute spent the most direct medical costs, which accounted for 42% of the estimated lifetime direct medical costs in Chinese schizophrenia patients.
Disease burden of schizophrenia: one-way sensitivity analysis
One-way sensitivity analyses indicated that the hazard ratio of mortality associated with relapsed schizophrenia had the largest impact on the reduced life years and QALY associated with schizophrenia. Varying this model variable within its 95% CI could change the reduced life years and QALY associated with schizophrenia by 2.792 years and 1.680 QALY, respectively. The key model variable driving lifetime direct medical costs associated with schizophrenia patients was the direct medical costs spent in the county mental health rehabilitation institute, which could vary the increased lifetime direct medical costs by US$17,903, about 21.2% of the point estimation in the base-case analysis (US$84,324). Additionally, varying the LAI treatment rate from 5 to 100% in the model cohort of schizophrenia patients could increase life years and QALY by 0.3 years and 0.2 QALY, respectively, and reduce lifetime medical costs by US$818. The results of the one-way sensitivity analyses are illustrated in Figure 2 by the three outcome measures used to estimate the disease burden of schizophrenia in this study.
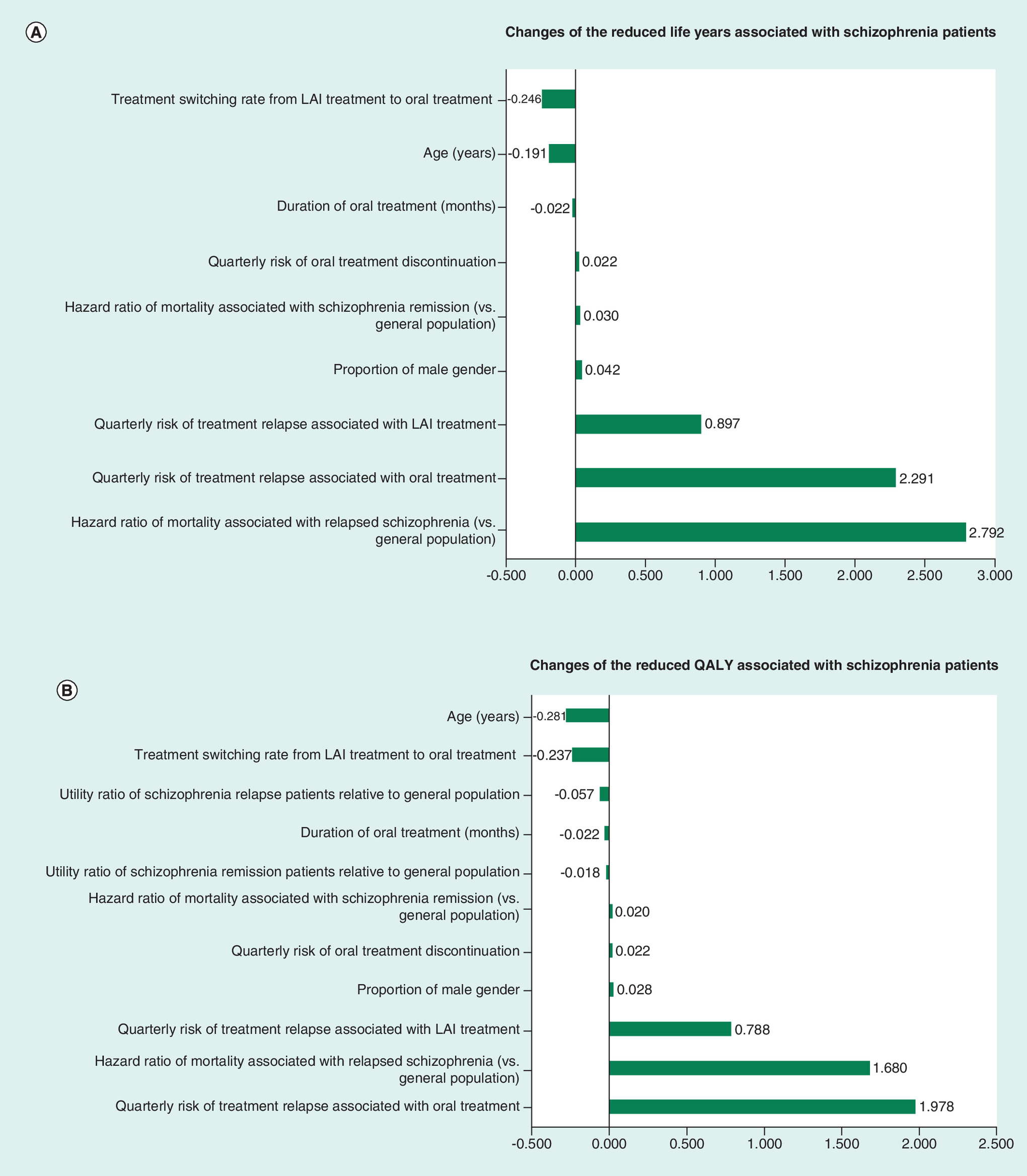
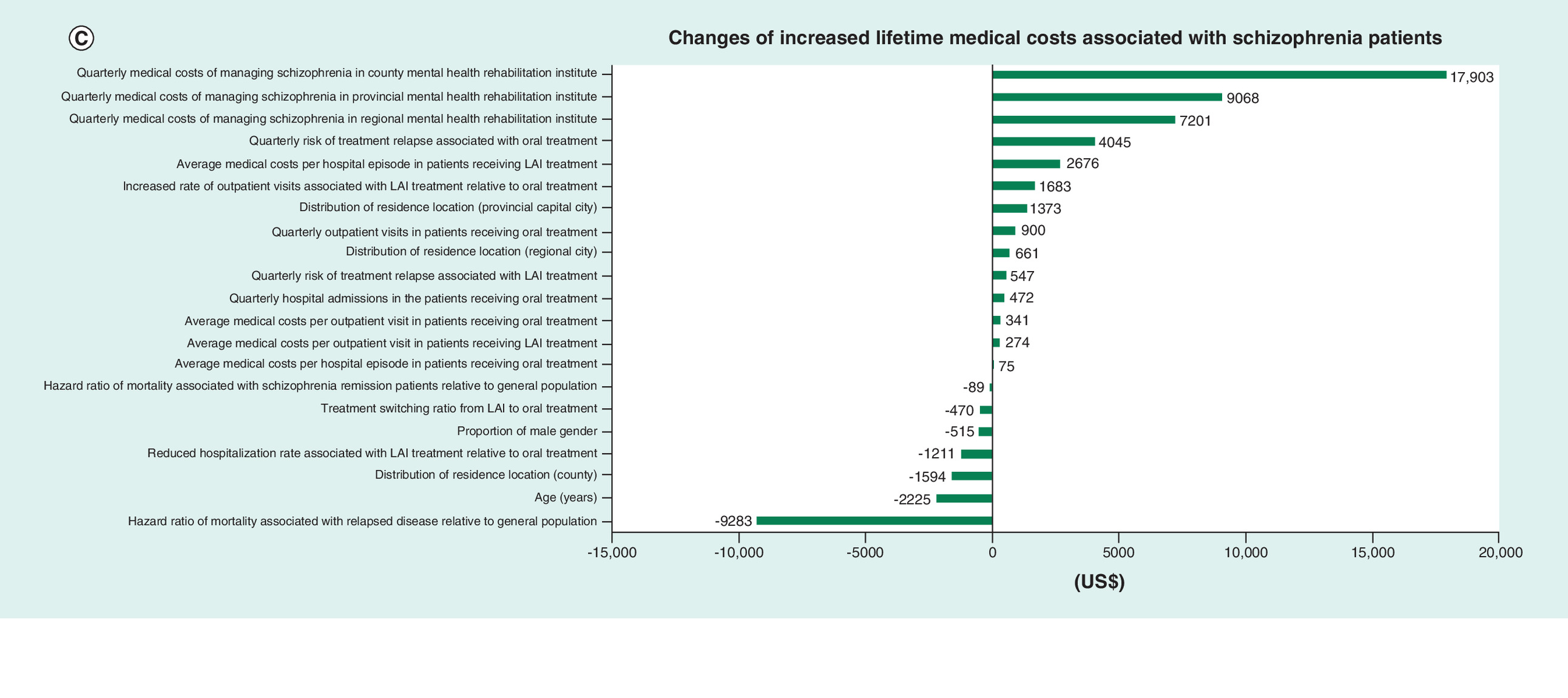
Figure 2. The impact of uncertainty associated with the main model variables on the measured outcomes for the disease burden of schizophrenia in the one-way sensitivity analyses.
(A) Changes of the differences in life years between schizophrenia patients and the general population (positive values indicating the increase of the disease burden of schizophrenia on lost life years). (B) Changes of the differences in QALY between schizophrenia patients and the general population (positive values indicating the increase of the disease burden of schizophrenia on lost QALY). (C) Changes of the differences in lifetime direct medical costs between schizophrenia patients and the general population (positive values indicating the increase of the disease burden of schizophrenia on lifetime direct medical costs).
LAI: Long-action injectable; QALY: Quality-adjusted life years.
Disease burden of schizophrenia: PSA
The 10,000 Monte Carlo simulations of the constructed decision-analytic model with the distributions of model variables identified that the median and 95% credible interval of reduced life years associated with schizophrenia were 20.5, 18.7 to 22.1 years; the median and 95% credible interval of reduced QALY associated with schizophrenia were 18.4, 17.0 to 19.4 QALY; and the median and 95% credible interval of increased lifetime direct medical costs associated with schizophrenia were US$51,171, 46,014 to 56,668 The distributions of the 10,000 simulations for the three outcome measures indicating the disease burden of schizophrenia are plotted in Figure 3.
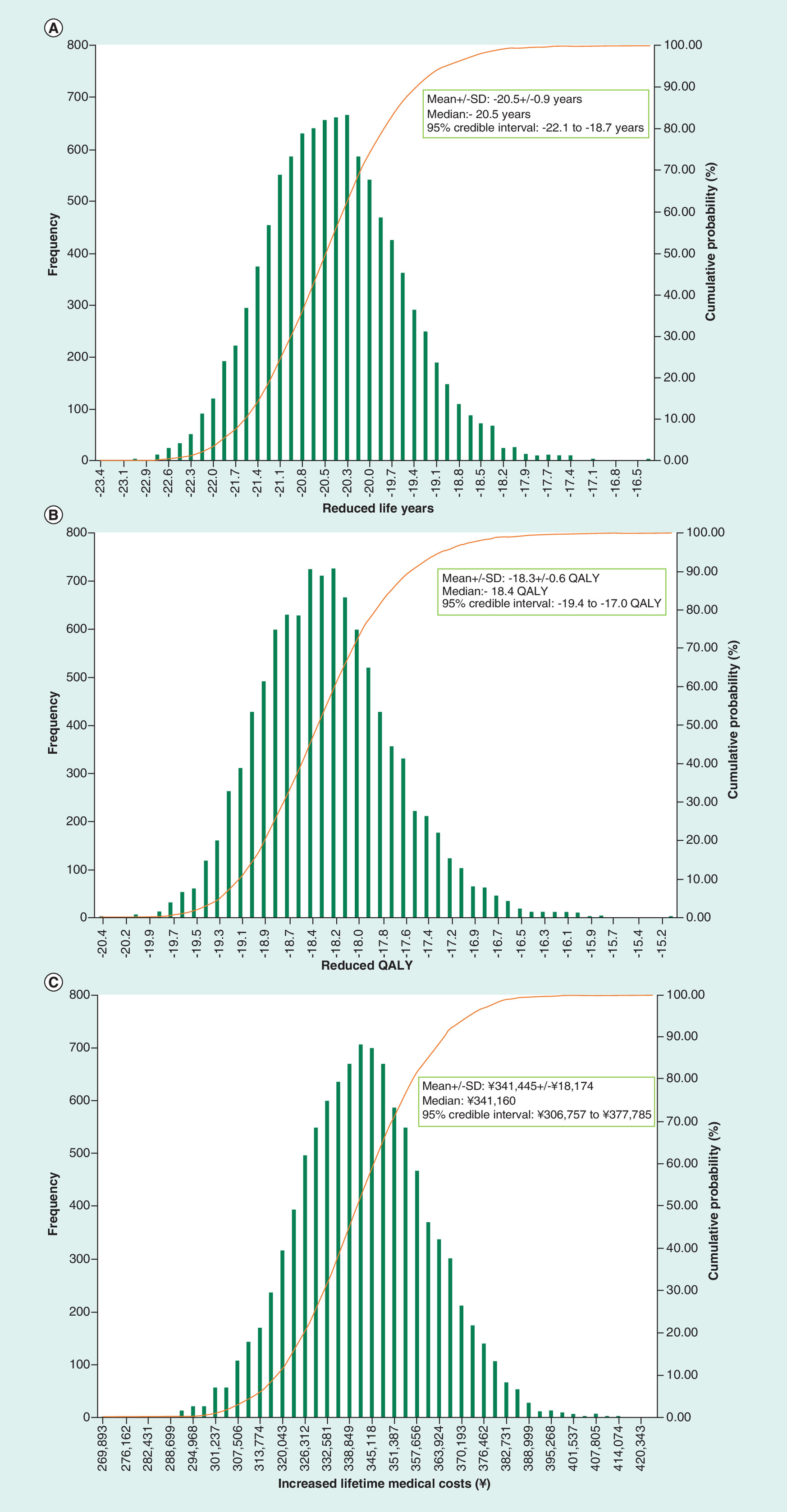
Figure 3. The distributions of the measured outcomes for the disease burden of schizophrenia based on the 10,000 Montel Carlo simulations.
(A) Reduced life years. (B) Reduced QALY. (C) Increased lifetime direct medical costs.
QALY: Quality-adjusted life years; SD: Standard deviation.
Discussion
To our knowledge, this study was the first research to quantify the disease burden of schizophrenia in China by simulating a real-world clinical cohort of schizophrenia patients over the entire lifetime in a decision-analytic model. Through comparisons with the age and gender-matched model control cohort with general Chinese population, the Chinese patients with schizophrenia could expect to lose about 18 years survival time and triple the lifetime direct medical costs under current treatment pattern, which mainly included oral antipsychotic medications. Thus, this study confirmed that schizophrenia has become a major health problem with a heavy disease burden that requires attention and actions to address the unmet medical needs of Chinese schizophrenic patients.
As the provincial mental healthcare center, our hospital received referred schizophrenia patients across the Hunan province with a population of over 68 million. The schizophrenia patients managed in our hospital had highly comparable demographics (young age and evenly distributed gender) and socioeconomic status (high unemployment rate and more patients living in the county) as the Chinese schizophrenia patients included in previous observational studies [22,23]. Thus, the schizophrenia cohort in this study should well represent the Chinese schizophrenia patients and the estimated disease burden of schizophrenia from the simulation of the created schizophrenia cohort should be comparable as the disease burden of the schizophrenia patients living in other Chinese provinces.
The estimated disease burden of Chinese schizophrenia was extremely heavy as the reduced survival time was as much as 20.6 years. After the review of the patient characteristics, treatment pattern and disease natural history, the heavy disease burden of schizophrenia in Chinese patients was likely to strongly correlated with the following factors. First, the Chinese schizophrenia patients were relatively young with a mean age of 31.1 years. Since schizophrenia is not curable, the longer duration of schizophrenia increases mortality. Second, the longer duration of schizophrenia increases the risk of treatment relapse, which reduces the quality of life and increases hospitalizations, the two main contributors to the disease burden of schizophrenia. Third, the current treatment pattern was predominated by oral antipsychotic medications that were associated with poor treatment compliance [24]. Thus, the high risk of treatment relapse due to poor treatment compliance could further worsen the disease burden of schizophrenia by increasing both mortality and direct medical costs. Because the demographics of schizophrenia patients could not be changed, how to reduce the risk of treatment relapse in schizophrenia patients could be the main direction to reduce the disease burden of schizophrenia in China.
Changing the current antipsychotic treatment pattern could be an effective solution to address the heavy disease burden of schizophrenia. Even though LAI treatment was introduced in China in 2012, LAI was only prescribed in 5% of the included patients in this study. Thus, the introduction of LAI treatment did not substantially change the treatment landscape of schizophrenia in China. Based on the synthesized evidence on the treatment effects of identified main oral antipsychotic medications and paliperidone palmitate injection, which was the only LAI identified in the included patients, the hazard ratio of treatment relapse associated with LAI relative to oral antipsychotic medications was 0.367. The superiority of LAI over oral antipsychotic medications for the reduced risk of treatment relapse was expected to substantially reduce the disease burden of schizophrenia. However, the reduction of the disease burden associated with the increased treatment rate of LAI was modest in the one-way sensitivity analysis likely due to the short treatment duration of LAI. The treatment duration of LAI in our real-world patient cohort was only 8.1 months because of the lack of reimbursement support. None of LAIs were listed for reimbursement in China during the study observation time. The schizophrenia patients and their families in China usually have limited income and they were unlikely to afford the high drug acquisition costs of the approved LAI. Thus, the improving the patient access to LAI through reimbursement could be an effective solution to improve health outcomes in Chinese schizophrenia patients.
The estimated lost survival time associated with our schizophrenic patients in the base-case analysis was 20.6 years, which was in the range of the reported lost life years associated with schizophrenia in the literature (14.5–25 years) [25,26]. Different from other chronic diseases, the impact of schizophrenia on survival was not well recognized and previous disease burden studies for schizophrenia have mainly focused on disability and costs. Our study estimated the mortality risk associated with schizophrenia in Chinese patients irrespective of residence location. In a real-world setting, the schizophrenia patients living in the rural area could be associated with much higher mortality risk than those living in the urban cities because of higher suicide rates [27], higher prevalence of other mental diseases and poorer management [28]. Given the fact that over half of our patients could live in a rural area, the lost life years associated with our schizophrenic patients could be even higher than our estimates.
Similar to previous economic burden studies, our study confirmed the substantial economic burden of schizophrenia from the perspective of healthcare payers. Our retrospective cohort study reported that the medical costs associated with one hospital episode were ¥13,769, which was 55% above the average costs of one hospital episode in China in 2017 [20]. According to the one-way sensitivity analyses, the economic burden of schizophrenia in China was mainly driven by the direct medical costs associated with the local mental health rehabilitation institutes, which have been well established across China to control the violence and threaten of mental diseases to the society [29]. The telephone interviews with these institutes found that LAI treatment was not used in the community at all due to the lack of access. Thus, the lack of LAI treatment in the community care for schizophrenia patients could further increase the risk of disease relapse and cause patients to heavily use local mental health rehabilitation institutes.
Even though this study leveraged real-world patient characteristics, treatment pattern and direct medical costs associated with over 3000 schizophrenia patients from a Chinese tertiary care hospital to maximize the robustness of the data sources for the development of schizophrenia disease burden model, the challenges and limitations associated with model development could still damage the reliability and validity of the estimated disease burden of schizophrenia. First, selection bias could be associated with the created study cohort, which could include more patients with newly diagnosed schizophrenia and patients living in the provincial city where the hospital located. The younger age associated with newly diagnosed schizophrenia patients could overestimate the disease burden because they would have a longer disease duration. Additionally, the higher medical costs associated with mental health rehabilitation institutes in the provincial city could overestimate the economic burden of schizophrenia. Second, reimbursement coverage had a substantial impact on treatment selection. LAI was not listed for reimbursement during the observation time defined in the retrospective cohort study. Recently, LAI has been listed for national reimbursement formula and the use of LAI for schizophrenia could be much improved. Thus, the measured disease burden of schizophrenia in our study should be interpreted under the treatment pattern without reimbursement coverage of LAI. Third, this study did not conduct chart review to extract more patient clinical characteristics, such as disease history and previous treatments, which could impact our data analysis regarding the differences in the measured outcomes associated with LAI and oral treatment. Third, the model assumptions in the decision analytic model could have a strong impact on the measured disease burden. For example, our study assumed that patients with more than two treatment relapses were managed in local mental health rehabilitation institutes. This assumption could underestimate the direct medical costs associated with tertiary care as some included patients had more than two hospital episodes in the retrospective cohort study. The management pathways associated with schizophrenia patients in real-world settings should be investigated in the future to further improve the robustness of our decision-analytic model. Fourth, our study still used a large amount of non-Chinese evidence to estimate the model variables that could drive the disease burden of schizophrenia. For example, the treatment efficacies of antipsychotic treatments were mainly based on studies from high-income countries. The quality of life associated with Chinese schizophrenia patients was based on a utility formula developed from a French study. Even though this study used conversion methods to improve the validity of these estimations in Chinese patients, future studies are still needed to validate these conversions and further confirm these estimations. Finally, the medical costs associated with local mental health rehabilitation institutes were based on the rough estimation from the telephone interview. These cost estimations might not take into account the additional medical costs associated with managing other mental disorders, which were prevalent in our study cohort as well. Thus, the economic burden of our schizophrenia patients could be underestimated. Future studies are still needed to obtain real-world cost data from those institutes to improve the accuracy of the estimated economic burden of schizophrenia.
In summary, this study used a real-world clinical cohort of Chinese patients with schizophrenia and a decision-analytic model to demonstrate the disease burden of schizophrenia under treatments, mainly oral antipsychotic medications. Based on the model simulation of these real-world patients, schizophrenia was associated with substantial disease burden by reducing survival time over 20 years and tripling the lifetime direct medical costs when compared with age and gender-matched general Chinese population. Because the mortality and high medical costs associated with relapsed schizophrenia mainly drove up to the disease burden of schizophrenia, improving patient access and compliance to treatment with the least risk of treatment relapse, such as LAI, could be an effective method to reduce the disease burden of schizophrenia in Chinese patients.
•
Oral antipsychotic treatments were predominate treatments in Chinese schizophrenia patients. Long-action injectable treatment was used only in 5% of the Chinese schizophrenia patients.
•
The utilization of long-action injectable treatment in the Chinese real-world setting was associated with reduced hospital admissions and did not increase overall medical costs.
•
The Chinese schizophrenia patients were associated with heavy loss of life years and quality-adjusted life years likely due to poor treatment compliance to oral antipsychotic treatments.
•
The economic burden of schizophrenia in China was heavy as well likely due to heavy use of local mental rehabilitation institutes for the management of relapsed schizophrenia patients.
•
Improving patient access to long-action injectable treatment could be an effective method to reduce the disease burden of schizophrenia in China because long-action injectable treatment was associated with better treatment compliance, which reduced disease relapse and the utilization of local mental rehabilitation institutes.
Author contributions
Q Zhong, W Chen, J Chen and H Tang formulated the research idea and developed the study protocol. Q Zhong, Y Tana, H Huang, J Huang, S Li, Z Teng, M Shen, C Wu, L Wang, S Cao, H Wu and H Tang conducted patient identification and data extraction at the study site. H Huang conducted the data analysis and developed the disease burden model of schizophrenia under the supervision of W Chen, J Chen and H Tang. Q Zhong, W Chen, J Chen and H Tang developed the manuscript. The submitted manuscript has been critically reviewed and approved by all authors.
Financial & competing interests disclosure
This study was sponsored by Xian Janssen Pharmaceutical Ltd. W Chen owns a consulting firm receiving industry funds to conduct health economics and outcomes research. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
This study was reviewed and approved by the ethics board of the Second Xiangya Hospital where the retrospective cohort study was conducted.
References
1.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (5th Edition). American Psychiatric Association, Washington DC, USA (2013).
2.
Whiteford HA, Degenhardt L, Rehm J et al. Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. Lancet 382(9904), 1575–1586 (2013).
3.
National Institute for Clinical Excellence. Psychosis and schizophrenia in adults: prevention and management. National Clinical Practice Guidelines number CG178 (2014). www.nice.org.uk/guidance/cg178
4.
Chan KY, Zhao FF, Meng S et al. Prevalence of schizophrenia in China between 1990 and 2010. J. Glob. Health 5(1), 010410 (2015).
5.
Xu J, Wang J, Wimo A, Qiu C. The economic burden of mental disorders in China, 2005–2013: implications for health policy. BMC Psych. 16(1), 137 (2016).
6.
Brown S. Excess mortality of schizophrenia: a meta-analysis. Brit. J. Psych. 171(6), 502–508 (1997).
7.
Eack SM, Newhill CE. Psychiatric symptoms and quality of life in schizophrenia: a meta-analysis. Schizophr. Bull. 33(5), 1225–1237 (2007).
8.
Knapp M, Mangalore R, Simon J. The global costs of schizophrenia. Schizophr. Bull. 30(2), 279–293 (2004).
9.
Andrews G, Henderson S. (Eds). Unmet Need in Psychiatry: Problems, Resources, Responses. Cambridge University Press, UK (2000).
10.
Yan F, Yang Y, Huang Q et al. Cost–effectiveness of a free drug program for schizophrenia in Beijing, China. Int. J. Social Psych. 65(1), 28–37 (2019).
11.
Muirhead D, Harvey C, Ingram G. Effectiveness of community treatment orders for treatment of schizophrenia with oral or depot antipsychotic medication: clinical outcomes. Aus. NZ J. Psych. 40(6–7), 596–605 (2006).
12.
Liu J, Ma H, He YL et al. Mental health system in China: history, recent service reform and future challenges. World Psych. 10(3), 210–216 (2011).
13.
Lieberman JA, Stroup TS, Mcevoy JP et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N. Engl. J. Med. 353(12), 1209–1223 (2005).
14.
Leucht C, Heres S, Kane JM, Kissling W, Davis JM, Leucht S. Oral versus depot antipsychotic drugs for schizophrenia--a critical systematic review and meta-analysis of randomised long-term trials. Schizophr. Res. 127(1–3), 83–92 (2011).
15.
Ascher-Svanum H, Faries DE, Zhu B, Ernst FR, Swartz MS, Swanson JW. Medication adherence and long-term functional outcomes in the treatment of schizophrenia in usual care. J. Clin. Psych. 67(3), 453–460 (2006).
16.
Kane JM, Garcia-Ribera C. Clinical guideline recommendations for antipsychotic long-acting injections. Brit. J. Psych. 195(Suppl. 52), S63–S67 (2009).
17.
Liu J, Ma H, He YL et al. Mental health system in China: history, recent service reform and future challenges. World Psych. 10(3), 210–216 (2011).
18.
China Banking and Insurance Regulatory Commission. China life insurance lifetable (2016). www.cbirc.gov.cn/cn/view/pages/ItemDetail.html?docId=372677&itemId=925&generaltype=0
19.
Sun S, Chen J, Johannesson M et al. Population health status in China: EQ-5D results, by age, sex and socio-economic status, from the National Health Services Survey 2008. Qual. Life Res. 20(3), 309–320 (2011).
20.
National Health Commission of P.R. China. 2017 China health care development annual report (2018). www.nhc.gov.cn/guihuaxxs/s10743/201806/44e3cdfe11fa4c7f928c879d435b6a18.shtml
21.
Hunan Provincial Bureau of Statistics. Main data bulletin of the national sampling survey of 1% population in Hunan province in 2015 (2016). http://tjj.hunan.gov.cn/tjfx/tjgb/rkpc/201605/t20160524_3800859.html
22.
Siani C, De Peretti C, Millier A, Boyer L, Toumi M. Predictive models to estimate utility from clinical questionnaires in schizophrenia: findings from EuroSC. Qual. Life Res. 25(4), 925–934 (2016).
23.
Xiang Y-T, Wang C-Y, Weng Y-Z et al. Predictors of relapse in Chinese schizophrenia patients: a prospective, multi-center study. Soc. Psych. Psychiatr. Epidemiol. 46(12), 1325–1330 (2011).
24.
Byerly MJ, Nakonezny PA, Lescouflair E. Antipsychotic medication adherence in schizophrenia. Psychiatr. Clin. North Am. 30(3), 437–452 (2007).
25.
Hjorthøj C, Stürup AE, Mcgrath JJ, Nordentoft M. Years of potential life lost and life expectancy in schizophrenia: a systematic review and meta-analysis. Lancet Psych. 4(4), 295–301 (2017).
26.
Tiihonen J, Lönnqvist J, Wahlbeck K et al. 11-year follow-up of mortality in patients with schizophrenia: a population-based cohort study (FIN11 study). Lancet 374(9690), 620–627 (2009).
27.
Ma X, Xiang Y-T, Cai Z-J et al. Lifetime prevalence of suicidal ideation, suicide plans and attempts in rural and urban regions of Beijing, China. Aust. NZ J. Psych. 43(2), 158–166 (2009).
28.
Ran M. A study of schizophrenic patients' treatment compliance in a rural community. J. Ment. Health 4(1), 85–90 (1995).
29.
Xiang Y-T, Yu X, Sartorius N, Ungvari GS, Chiu HF. Mental health in China: challenges and progress. Lancet 380(9855), 1715–1716 (2012).
Information & Authors
Information
Published In
Pages: 469 - 481
PubMed: 32301625
Copyright
© 2020 Future Medicine Ltd.
History
Received: 22 August 2019
Accepted: 24 February 2020
Published online: 17 April 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Disease burden of schizophrenia patients visiting a Chinese regional mental health centre. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0129
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Yan Gu, Yong He, Yingying Xie, Wenqian Lu, Hao Liu, Yan Li, Gangqin Li, Distinctive and common risk factors contributing to violent offending in patients with schizophrenia compared to people without a mental illness, International Journal of Law and Psychiatry, 10.1016/j.ijlp.2026.102192, 105, (102192), (2026).
- Hong Ma, Jun Cai, Fujun Jia, Jiansong Zhou, Bo Zhou, Wanyi Zhang, Chong Ye, Miaomiao Jia, Tianmei Si, Clinical Practice Recommendations for Switching from Once-Monthly to Longer-Interval Paliperidone Palmitate Injectable in Schizophrenia Patients: A Modified Delphi Study in China, Neuropsychiatric Disease and Treatment, 10.2147/NDT.S579943, Volume 22, (1-14), (2026).
- Hua Ren, Qin Yang, Changjiu He, Jian Jiao, Zaiquan Dong, Community management: An effective model to reduce medication discontinuation rate in patients with schizophrenia, PLOS One, 10.1371/journal.pone.0324114, 21, 1, (e0324114), (2026).
- Sihan Zhao, Yonghou Zhao, Ming Yu, Jianbo Chai, Xinhui Yao, A Systematic Review of Traditional Uses, Phytochemistry, and Pharmacology of Chinese Herb Medicine for Schizophrenia, Journal of Clinical Pharmacy and Therapeutics, 10.1155/jcpt/9996801, 2025, 1, (2025).
- Xiao Liu, Xiao-yu Wang, Bing-zhe Chen, Yu-mei Su, Run-hui Pang, Risk prediction model development for requiring unplanned psychiatric readmission in bipolar disorder, Scientific Reports, 10.1038/s41598-025-17142-7, 15, 1, (2025).
- Yuting Tan, Guiling Chen, Shuge Wang, Xingxin Zhan, Rong Cheng, Linru Qiao, Zhixia Zhang, Yaping Liu, Machine Learning and Interpretability Study for Predicting 30-Day Unplanned Readmission Risk of Schizophrenia: A Retrospective Study, Neuropsychiatric Disease and Treatment, 10.2147/NDT.S522675, Volume 21, (1509-1521), (2025).
- Hong Cai, Pan Chen, Qinge Zhang, Mei Ieng Lam, Tong Leong Si, Yu-Fei Liu, Wan-Ying Zheng, Zhaohui Su, Teris Cheung, Todd Jackson, Gabor S. Ungvari, Zhihong Ren, Xinyue Li, Xiao-Hong Li, Yu-Tao Xiang, Global prevalence of major depressive disorder in LGBTQ+ samples: A systematic review and meta-analysis of epidemiological studies, Journal of Affective Disorders, 10.1016/j.jad.2024.05.115, 360, (249-258), (2024).
- Mingru Hou, Yuqing Wu, Jianhua Xue, Qiongni Chen, Yan Zhang, Ruifen Zhang, Libo Yu, Jun Wang, Zhenhe Zhou, Xianwen Li, A predictive model for readmission within 1-year post-discharge in patients with schizophrenia, BMC Psychiatry, 10.1186/s12888-024-06024-3, 24, 1, (2024).
- Yujing Sun, Hong Yu, Zhengjun Wang, Jing Zhang, Yuqiu Zhou, Wenming Cui, Wenlong Jiang, Relationship between medication burden and medication experience in stable patients with schizophrenia: the mediating effect of medication belief, BMC Nursing, 10.1186/s12912-024-01882-4, 23, 1, (2024).
- Xu Yang, Haidong Yang, Na Li, Chunyu Li, Weiye Liang, Xiaobin Zhang, Increased serum homocysteine in first episode and drug-naïve individuals with schizophrenia: sex differences and correlations with clinical symptoms, BMC Psychiatry, 10.1186/s12888-022-04416-x, 22, 1, (2022).